CME information and disclosures
To see contributor disclosures related to this article, hover over this reference: [1]
Physicians may earn CME/MOC credit by reading information in this article to address a clinical question, and then completing a brief evaluation, in which they will identify their question and report the impact of any information learned on their clinical practice.
AMBOSS designates this Internet point-of-care activity for a maximum of 0.5 AMA PRA Category 1 Credit(s)™. Physicians should claim only credit commensurate with the extent of their participation in the activity.
For answers to questions about AMBOSS CME, including how to redeem CME/MOC credit, see “Tips and Links” at the bottom of this article.
Summary
Decubitus ulcers or pressure ulcers are preventable injuries frequently encountered in older, malnourished, and immobilized individuals, especially those with multiple comorbidities. These injuries typically develop over bony prominences when local pressure-induced hypoperfusion and necrosis can lead to the loss of several or all skin layers. Diagnosis is primarily clinical but laboratory studies and imaging are required to evaluate for complications or risk factors that may delay healing (e.g., uncontrolled blood sugars, hypoalbuminemia). Treatment includes adequate analgesia, pressure relief (e.g., regular position changes, alternating pressure mattresses), frequent wound dressings, and nutritional support. Infectious complications (e.g., osteomyelitis, sepsis) should be treated with appropriate antibiotic therapy. Large, deep ulcers may require surgical debridement, especially if there is an inadequate response to conservative management. Preventive measures should be taken for all at-risk individuals and include pressure relief, rigorous skin care, and treatment of comorbidities and other risk factors such as malnutrition and systemic infection.
Definitions
A decubitus ulcer or pressure injury is a focal area of unrelieved pressure resulting in ischemia, cell death, and necrotic injury of the epidermis and soft tissue.
Etiology
The development of decubitus ulcers is multifactorial. Decubitus ulcers are prone to secondary infection, which is often polymicrobial.
Predisposing factors [2][3]
- Old age
- Cachexia or malnourishment
- Multimorbidity
- Diabetes mellitus
-
Prolonged reduction in any of the following:
- Mobility (e.g., secondary to illness, frailty, or paralysis)
- Perception of pain (e.g., due to polyneuropathy, cognitive impairment, or anesthesia)
- Skin perfusion (e.g., in peripheral artery disease, heart failure, vasoconstriction, or shock)
- Skin breakdown (maceration) due to urinary or fecal incontinence
- Certain medications (e.g., immunosuppressants, steroids, or vasopressors) [2][4]
- Prolonged pressure from medical devices such as feeding tubes, oxygen delivery devices, or tracheostomy tubes [2][4]
Pressure ulcers can develop within hours in an immobilized individual. Critically ill patients are at especially high risk and must be monitored carefully. [3]
Microbiology [5]
The most commonly isolated bacteria include:
- Staphylococcus aureus
- Proteus mirabilis
- Pseudomonas aeruginosa
- Enterococcus faecalis
Pathophysiology
Mechanical stress → local hypoperfusion → ischemic necrosis [3]
Clinical features
- Typical location: over bony prominences, such as the sacrum, ischium, heel, greater trochanter, lateral malleolus, elbows
-
Initial presentation
- Focal area of nonblanchable erythema with/without edema
- Evidence of decreased skin perfusion (increased capillary refill time)
- Painful, unless there is sensory loss (e.g., due to spinal cord injury) [6]
-
Advanced ulcers: loss of several or all skin layers and/or subcutaneous tissue
- Eschar and/or slough may cover the wound bed.
- Exposure of underlying tissue, including muscle and bone
- Signs of wound infection (e.g., purulent drainage or unpleasant odor) may be present.
- See also “Etiology” for predisposing factors and “Staging of decubitus ulcers” for further information.
")
Reference [4]
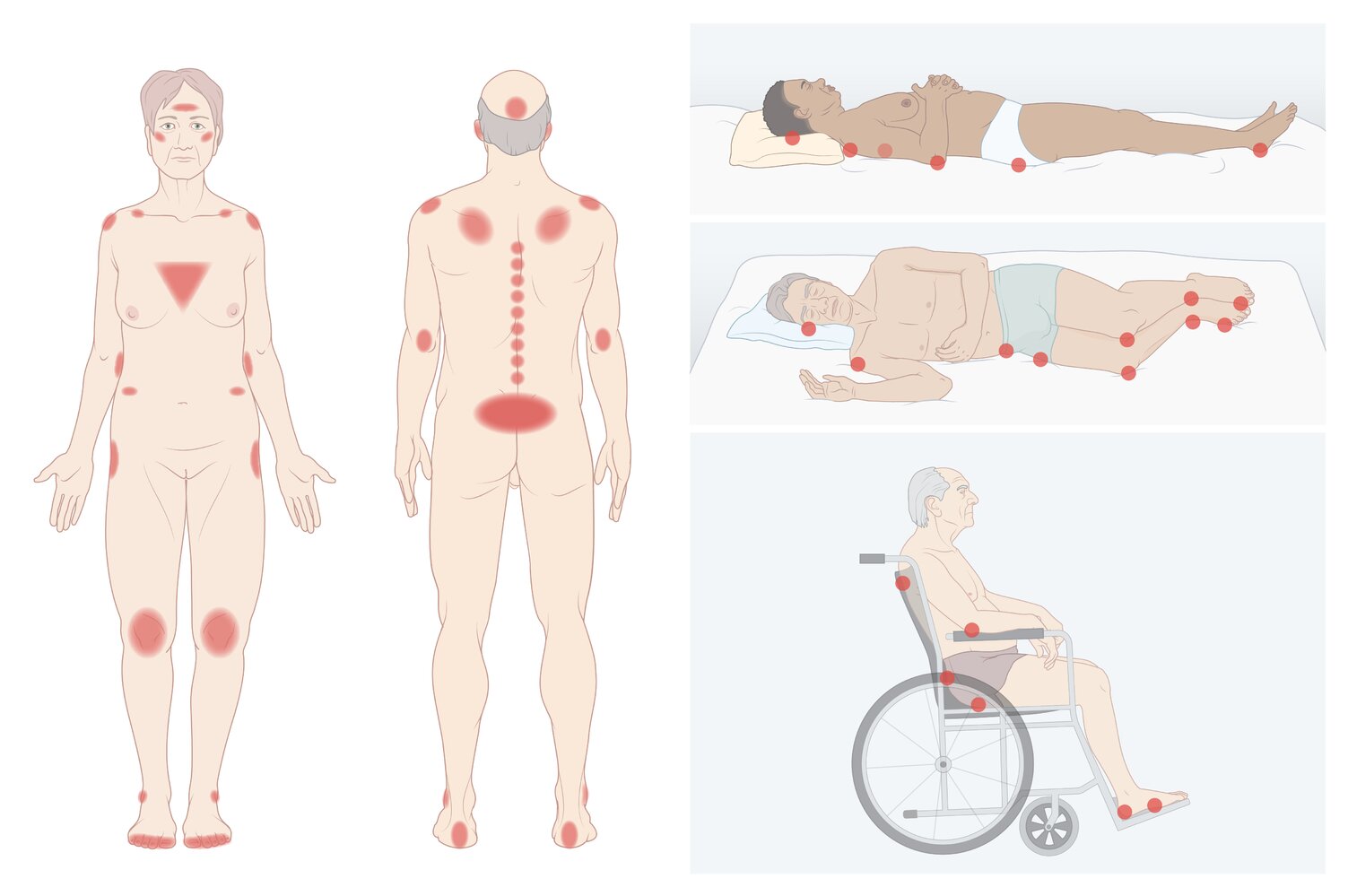
Pressure ulcers typically develop over bony prominences.
© AMBOSS
Classification
- Decubitus ulcers should be staged in order to plan management. [4]
- The wound bed should be cleaned before staging to ensure accurate assessment.
- The stage is determined by the deepest extent of the ulcer.
| Staging of decubitus ulcers [4] | |
|---|---|
| Stage | Clinical features |
| 1 |
|
| 2 |
|
| 3 |
|
| 4 |
|
| Unstageable |
|
 ulcer")
 ulcer")
 ulcer")
 ulcer")

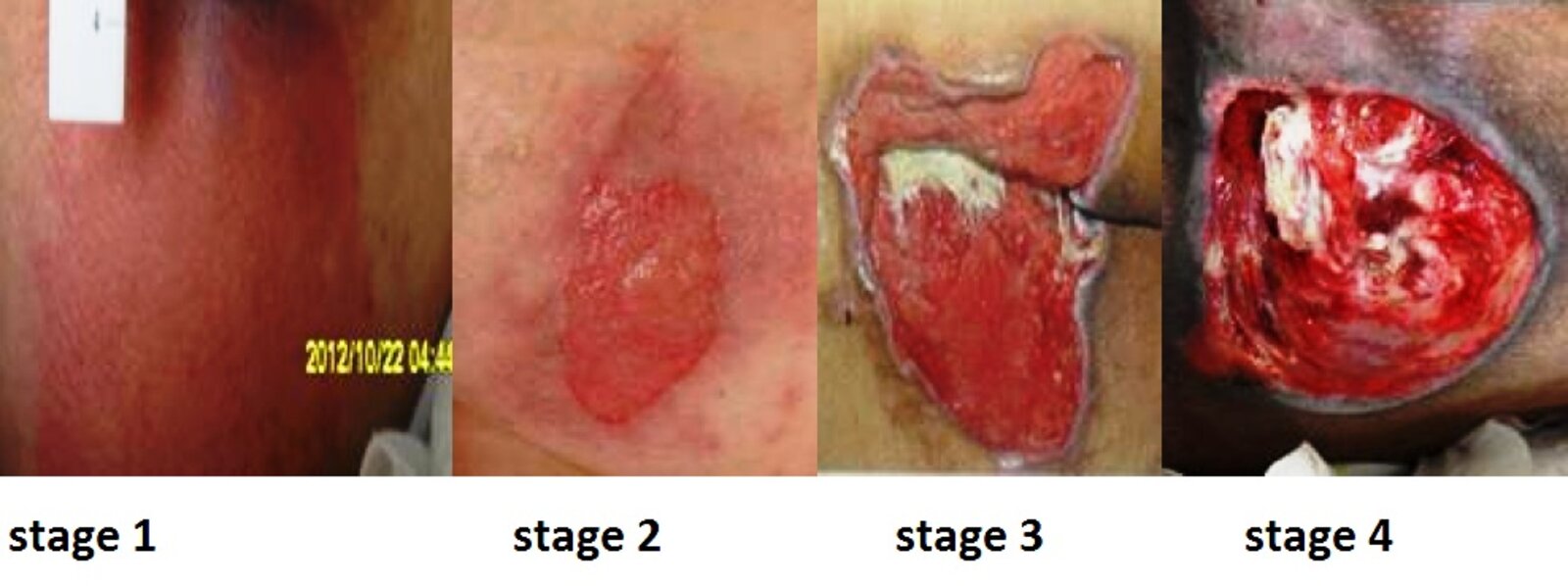
Source: “Wound stage” by Babagolzadeh, Wikimedia commons, licensed under CC BY-SA 3.0.
{kind=link}
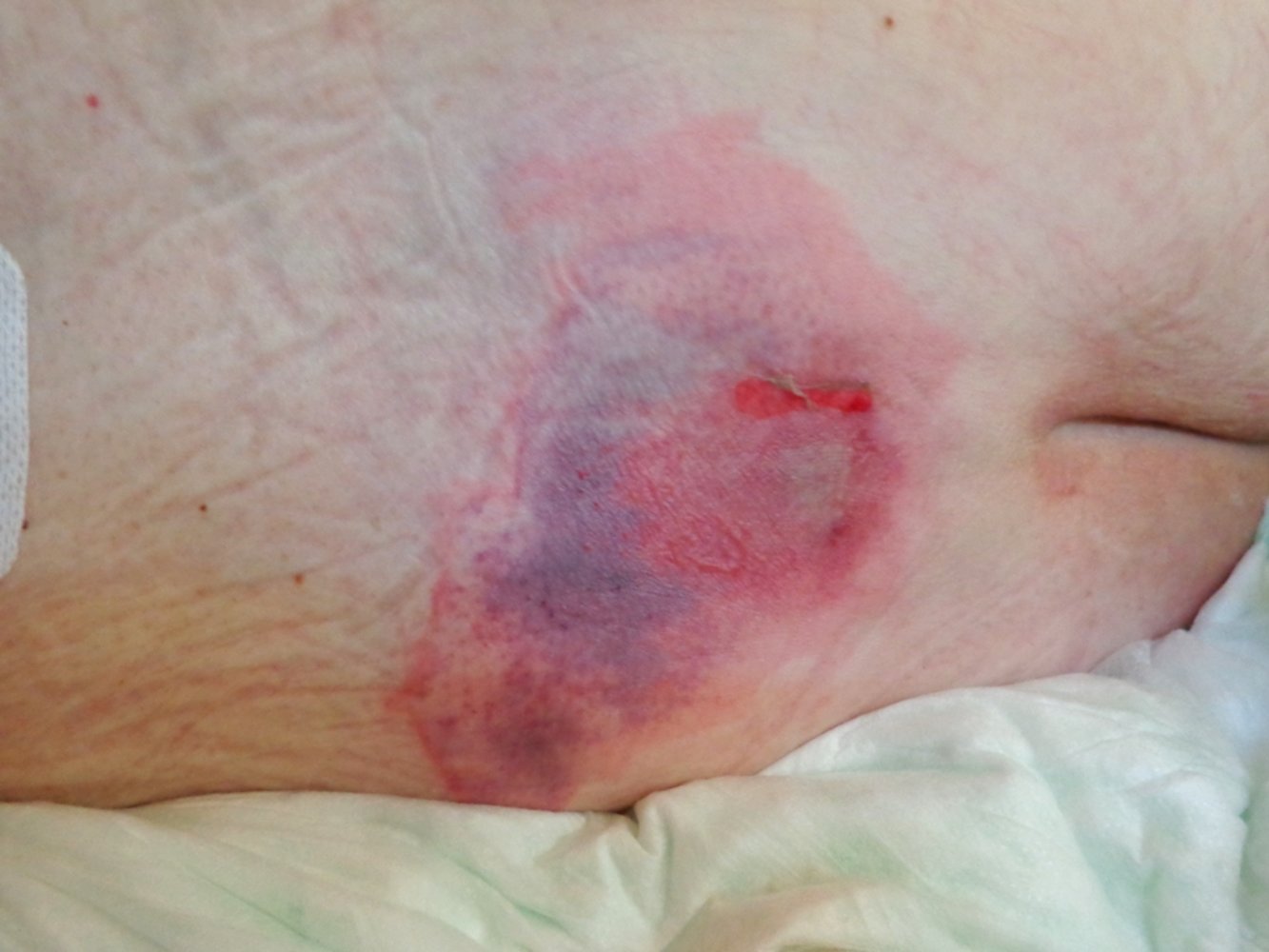
An erythematous, blue-purple area of skin measuring approx. 10 cm x 5 cm is visible over the sacrum with a small area of superficial (epidermal) skin loss near the lower edge.
Source: “Decubitus 01” by AfroBrazilian, Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}

A decubitus ulcer with loss of all skin layers and subcutaneous involvement is visible to the right of the intergluteal cleft.
Source: © IMPP

There is an extensive circular lesion over the right hip with loss of all skin layers, resulting in exposure and damage to deeper structures, including the right gluteus medius muscle.
Source: “Imagen Bob 108” by Bobjgalindo, Wikimedia Commons, licensed under CC BY-SA 4.0.
{kind=link}

Buttocks of a 42-year-old male patient with morbid obesity after prolonged hospitalization
A decubital ulcer is visible, partially covered with black eschar and surrounded by erythema. The ulcer was described as having a foul smell, indicating bacteremia. Blood culture and surgical sample confirmed the involvement of Escherichia coli, Enterococcus faecalis, and P. loescheii.
Source: “Figure 1, in: Bacteremic skin and soft tissue infection caused by Prevotella loescheii” by Mansoor Mehmood, Nabil A Jaffar, Muhammad Nazim, Faisal A Khasawneh, BMC Infectious Diseases, licensed under CC BY 2.0.

A decubitus ulcer with full-thickness skin and tissue loss is visible over the sacrum, exposing the bone. The ulcer is partly covered by eschar and surrounded by erythema.
Source: © IMPP
Diagnosis
Initial assessment
- Identify predisposing factors (see “Etiology”) and assess nutritional status and skin condition, especially in other at-risk areas.
- Confirm that the injury is secondary to prolonged focal pressure. [4]
- Determine the onset of the ulcer and if it has changed in size or depth.
- Assess for undermining and tunneling into surrounding tissue, as well as the presence of necrotic tissue and drainage.
- Document the stage of the decubitus ulcer.
- Consider differential diagnoses of decubitus ulcers that may need additional workup.
Diagnostics
- Evaluate for predisposing factors, such as:
- Blood glucose and HbA1C to assess for diabetes
- Serum albumin to assess for malnutrition
- Screen for complications
- CBC, CRP: Leukocytosis and ↑ CRP suggest an infectious complication.
- Wound swab: not routinely recommended ; consider in patients with suspected MRSA infection/colonization. [7]
- Blood cultures: Consider in patients with deep ulcers and signs of sepsis.
- Imaging (e.g., x-ray, CT, or MRI): Consider if osteomyelitis or an underlying bony involvement is suspected.
- For further information see “Skin and soft tissue infections” and “Diagnosis of osteomyelitis”.
Differential diagnoses
- Venous ulcer
- Arterial ulcer
- Malum perforans
- Ulcerated skin tumor (e.g., basal cell carcinoma)
The differential diagnoses listed here are not exhaustive.
Complications
- Soft tissue infection (e.g., cellulitis, abscess)
- Osteomyelitis
- Bacteremia, sepsis
- Marjolin ulcer [8]
Reference [9]
We list the most important complications. The selection is not exhaustive.
Treatment
Approach
- Ensure adequate analgesia (see “Pain management” for details on drugs and dosages).
- Consult a wound care specialist, general surgery, and/or plastic surgery.
- Urgently consult surgery for advanced and/or infected ulcers, especially if they are suspected to be the source of sepsis.
- Initiate treatment depending on the stage of the ulcer and whether an infection is present.
- Superficial, clean wound: supportive care alone may be appropriate
- Extensive and/or infected wound, wet eschar: debridement, antibiotic therapy, and/or surgical management in addition to supportive care
- Optimize management of comorbidities that may affect healing (e.g., uncontrolled diabetes mellitus).
- Ensure proper follow-up. [10]
- The wound should be cleaned and freshly dressed regularly.
- Repeated debridements might be necessary.
Supportive care [2][10][11]
The following are also important preventive measures for patients at risk of developing a decubitus ulcer.
Redistribute pressure
Pressure relief over the affected or vulnerable area is one of the most important aspects of management.
-
Immobile patients and patients with several or refractory ulcers: [3]
- Frequent position changes (every 2 hours)
- Pad all pressure points.
- Alternating pressure mattress
- Mobile patients
- Optimize bedding with a foam mattress or overlay.
- Assist with movement for patients with limited mobility.
- All at-risk patients: pad pressure points on devices such as CPAP masks and physical restraints.
Rigorous skin care
- Keep the skin clean and moisturized in order to prevent skin erosion and laceration.
- Advise caregivers to regularly inspect other at-risk areas to identify early stages of decubitus ulcers.
- Catheterization, bowel programs, and/or highly absorbent incontinence products (e.g., diapers, pads) may be helpful for patients with incontinence.
Nutrition
- Ensure adequate hydration and nutrition in all patients, preferably in consultation with a nutritionist.
- Protein supplementation is recommended. [12]
- Consider increasing daily calorie requirement and supplementing micronutrients to facilitate healing.
Pressure relief and regular skin care are the most important steps for the prevention and treatment of decubitus ulcers.
Wound management [2][10][12]
-
Cleaning
- Perform frequently to reduce the bacterial load.
- Normal saline is a suitable cleaning agent.
- Limit the use of antiseptic fluids, because they inhibit the formation of granulation tissue. [10]
- Dressings (e.g., hydrocolloids, foam dressings ): Perform frequently to absorb excess exudate while keeping the wound moist
-
Debridement
- Used to remove devitalized tissue or biofilms to prevent or treat infection and enable healing
- Modalities: sharp (surgical), mechanical, biological, enzymatic, and autolytic
- In patients with suspected infection, obtain a swab or tissue for culture following debridement.
- Adjunctive treatment options: electrical stimulation, negative pressure wound therapy, and administration of platelet-derived growth factor [12]
 wound therapy: materials and application")
 wound therapy: principles")
Systemic antibiotic treatment [2]
- Indication: evidence of localized or systemic infection (e.g., cellulitis, underlying osteomyelitis, sepsis)
-
Options
- The choice of antibiotic should be directed by local microbiological guidance or, if a wound swab was obtained, by the culture results.
- See “Empiric antibiotic therapy for skin and soft tissue infections”, “Treatment of osteomyelitis”, or "Antibiotics for sepsis” as needed.
Surgical management [2][10]
-
Indications and options
-
Surgical debridement, ulcer/eschar excision
- Extensive ulcers with undermining of adjacent tissue, cavity formation, or large necrotic areas
- Management of associated infection (e.g., extensive cellulitis, abscess, or osteomyelitis)
- Stage 3 or 4 wounds refractory to conservative management
- Secondary closure (e.g., tissue flap reconstruction): clean, healing ulcers.
-
Surgical debridement, ulcer/eschar excision
- Important consideration: Conservative management may be more appropriate for patients who are not good candidates for surgery (e.g., multiple comorbidities, limited life-expectancy).
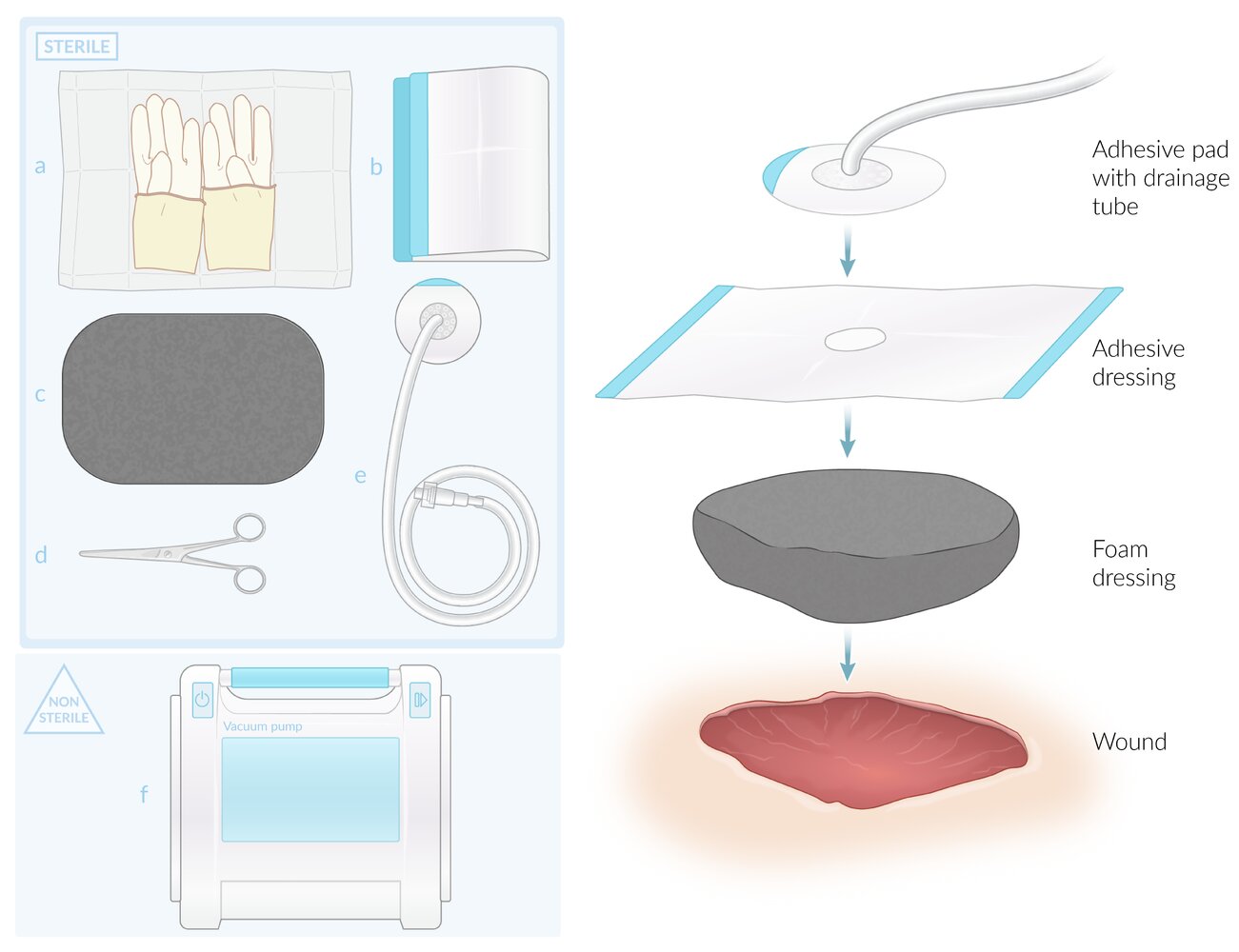
Sterile equipment (top left)
(a) Sterile gloves
(b) Adhesive dressing
(c) Foam dressing
(d) Scissors
(e) Adhesive pad with drainage tube
Nonsterile equipment (bottom left)
(f) Vacuum pump
Not illustrated are materials for antisepsis and wound debridement.
Application (right)
After wound cleaning and debridement (if required), the foam dressing is cut to fill the entire cavity and placed in the wound. The adhesive dressing is placed over the foam dressing and surrounding skin. If the dressing does not have a preexisting opening, a hole is cut into it following placement over the foam dressing. The adhesive pad with drainage tube is placed over this opening and the tube connected to the vacuum pump. After switching on the pump, the dressing should be assessed for air leaks.
© AMBOSS
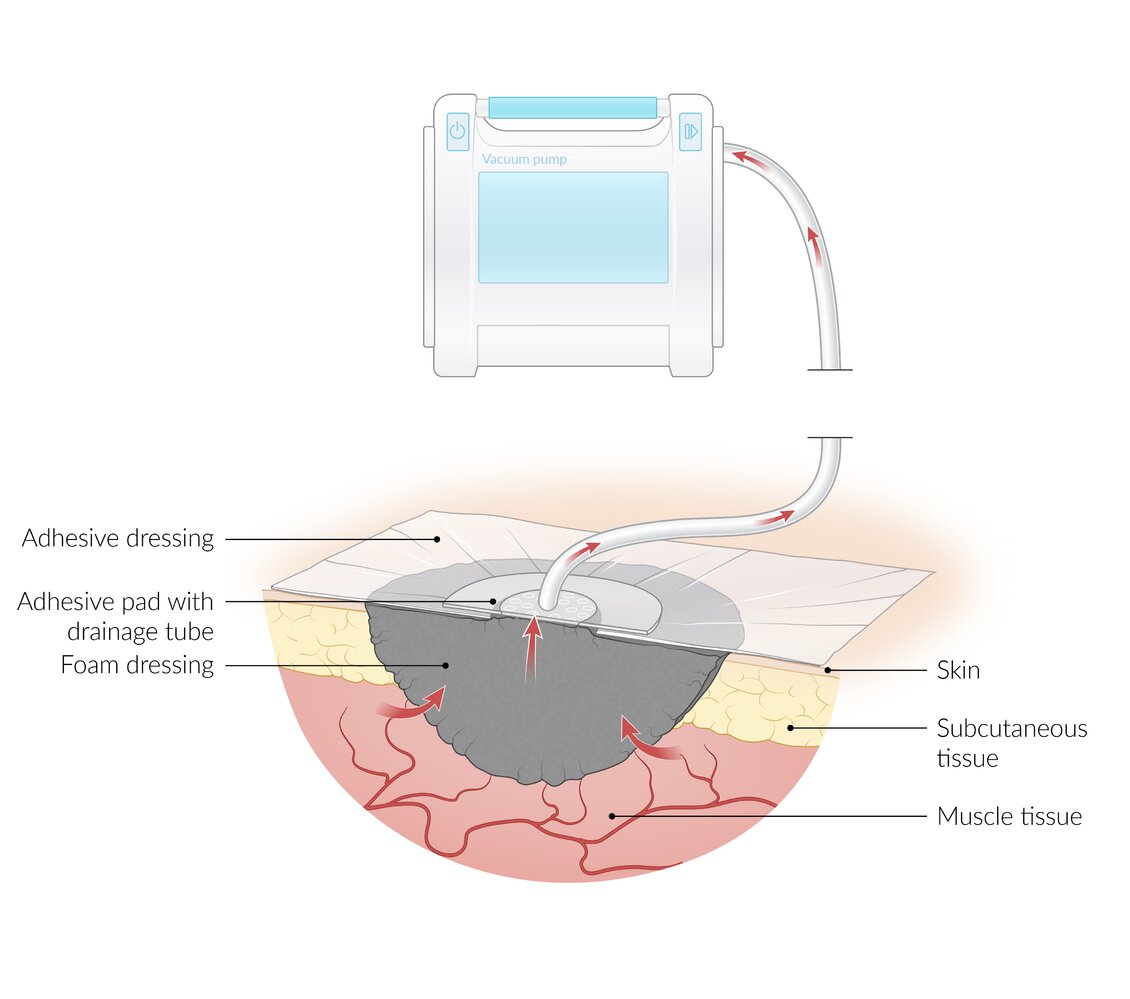
Cross-section of a vacuum dressing
The wound cavity is filled with a foam dressing. (The cavity shown here extends into muscle tissue; cavities may also be limited to subcutaneous tissue or extend to the bone.) An airtight adhesive dressing covers the foam dressing and surrounding skin. The adhesive dressing is perforated centrally and the opening covered by an adhesive pad, which is connected via a drainage tube to the vacuum pump. The pump creates negative pressure, drawing off wound exudate (red arrows) via the foam dressing and drainage tube into a collection device.
© AMBOSS
Prevention
- Identify patients at high risk of developing a decubitus ulcer (e.g., use scoring systems such as the Braden scale and Norton scale).
- Initiate measures to prevent decubitus ulcers from forming, such as pressure relief, skin care, regular skin inspection of at-risk areas, and good nutrition. (see “Supportive care” in “Treatment” for details).
Ensure regular screening and preventative measures in high-risk care settings (e.g., overcrowded emergency departments) where pressure ulcer incidence is high and development can be rapid. [13][14]
External Resources
- 2016 NPUAP Pressure Injury Staging System
- 2015 Wound Healing Society Update on Guidelines for Pressure Ulcers
- 2015 ACP Guideline for Risk Assessment and Prevention of Pressure Ulcers
- 2015 ACP Guideline for the Treatment of Pressure Ulcers
- 2019 NPIAP Prevention and Treatment of Pressure Ulcers/Injuries: Quick Reference Guide
- CME Program Overview
- Internet Point-of-Care CME
References
- Gould L, Stuntz M, Giovannelli M, et al. "Wound healing society 2015 update on guidelines for pressure ulcers". Wound Repair Regen. 24(1). :145-162. (2016)
- "Prevention and Treatment of Pressure Ulcers/Injuries: Quick Reference Guide". http://www.internationalguideline.com/static/pdfs/Quick_Reference_Guide-10Mar2019.pdf. [2019-03-10]
- Qaseem A, Mir TP, Starkey M, Denberg TD. "Risk Assessment and Prevention of Pressure Ulcers: A Clinical Practice Guideline From the American College of Physicians". Ann Intern Med. 162(5). :359. (2015)
- Bansal C, Scott R, Stewart D, Cockerell CJ. "Decubitus ulcers: A review of the literature". Int J Dermatol. 44(10). :805-810. (2005)
- Qaseem A, Humphrey LL, Forciea MA, Starkey M, Denberg TD. "Treatment of Pressure Ulcers: A Clinical Practice Guideline From the American College of Physicians". Ann Intern Med. 162(5). :370. (2015)
- "Contributor Disclosures - Decubitus ulcers. None of the individuals in control of the content for this article reported relevant financial relationships with ineligible companies. For details, please review our full conflict of interest (COI) policy:"
- Edsberg LE, Black JM, Goldberg M, et al. "Revised National Pressure Ulcer Advisory Panel Pressure Injury Staging System". J Wound Ostomy Continence Nurs. 43(6). :585-597. (2016)
- Khan K, Giannone AL, Mehrabi E, Khan A, Giannone RE. "Marjolin's Ulcer Complicating a Pressure Sore: The Clock is Ticking.". The American journal of case reports. 17. :111-4. (2016)
- Espejo E, Andrés M, et al. "Bacteremia associated with pressure ulcers: a prospective cohort study". European Journal of Clinical Microbiology & Infectious Diseases. 37(5). :969-975. (2018)
- Raetz JG, Wick KH. "Common Questions About Pressure Ulcers". Am Fam Physician. 92(10). :888-94. (2015)
- Dana AN, Bauman WA. "Bacteriology of pressure ulcers in individuals with spinal cord injury: What we know and what we should know.". J Spinal Cord Med. 38(2). :147-60. (2015)
- Girouard K, Harrison MB, VanDenKerkof E. "The symptom of pain with pressure ulcers: a review of the literature.". Ostomy Wound Manage. 54(5). :30-40, 42. (2008)
- Naccarato MK, Kelechi T. "Pressure Ulcer Prevention in the Emergency Department". Advanced Emergency Nursing Journal. 33(2). :155-162. (2011)
- Liu P, Shen WQ, Chen HL. "The Incidence of Pressure Ulcers in the Emergency Department: A Metaanalysis.". Wounds. 29(1). :14-19. (2017)