Quick guide
Diagnostic approach
- ABCDE survey
- Targeted clinical evaluation
- CBC
- BMP
- Blood cultures
- Bacterial culture of abscess aspirate
- CT neck with IV contrast
Red flag features
- Clinical features of sepsis
- Signs of respiratory distress
- Signs of airway obstruction
- Trismus
- Torticollis
Management checklist
- Perform emergency airway management of deep neck infections.
- Start empiric antibiotic therapy for deep neck infections.
- Consider corticosteroids (e.g., dexamethasone ).
- Provide supportive care (e.g., pain management, antipyretic therapy, IV fluid therapy).
- Consult ENT and/or oral maxillofacial surgery for abscess drainage.
- Consult dentistry for abscesses with an odontogenic source.
Summary
Deep neck infections include peritonsillar abscess, parapharyngeal abscess (PPA), and retropharyngeal abscess (RPA). While uncommon, deep neck infections are clinically significant because of their potentially life-threatening complications, including the spread of infection to vital nearby structures and airway compromise. Consultation with airway specialists is recommended if there are clinical features of airway compromise. Early recognition, aggressive airway management, broad-spectrum IV antibiotic therapy, and urgent ENT consultation for abscess drainage and/or other surgical interventions reduce the risk of complications and death from sepsis or airway compromise.
Overview
| Overview of deep neck infections [1][2] | |||
|---|---|---|---|
| Peritonsillar abscess | Parapharyngeal abscess | Retropharyngeal abscess | |
| Definition |
|
|
|
| Epidemiology |
|
|
|
| Etiology |
|
|
|
| Clinical Features |
|
|
|
| Diagnosis |
|
|
|
| Treatment |
|
||
Emergency airway management of deep neck infections
Anticipate a difficult airway as a result of anatomical distortion caused by the infection. [4][5]
- Assess the airway: Check for signs of airway compromise.
-
If the airway must be secured: Consult an airway specialist urgently.
- Preferred method: awake fiberoptic intubation in the operating room [4][6]
- Prepare for a difficult intubation, e.g., ensure intubation adjuncts are immediately available.
- Exercise caution with direct laryngoscopy, as it can precipitate airway compromise. [5]
- Anticipate the need for an emergency surgical airway; see “Cricothyrotomy” for detailed procedural guidance. [5]
- No immediate concern for airway compromise: Reassess the airway regularly.
Direct laryngoscopy can worsen airway edema, rupture the abscess, and/or precipitate complete airway obstruction.
Peritonsillar abscess
Peritonsillar abscess, also known as quinsy, is the most common deep neck infection.
Epidemiology [3]
- Most frequently occurs in adults aged 20–40 years
- Increased risk of airway obstruction in children with peritonsillar abscess
Etiology [7][8]
- Pathogens: Streptococcus pyogenes (most common), Streptococcus anginosus, viridans streptococci, Staphylococcus aureus, and Haemophilus species, often in a polymicrobial environment
- Acute bacterial tonsillitis (see acute tonsillitis)
Clinical features [8][9]
- Features of tonsillitis: fever, malaise, severe sore throat, dysphagia, and odynophagia
- “Hot potato” voice (muffled speech), drooling, or halitosis
- Trismus
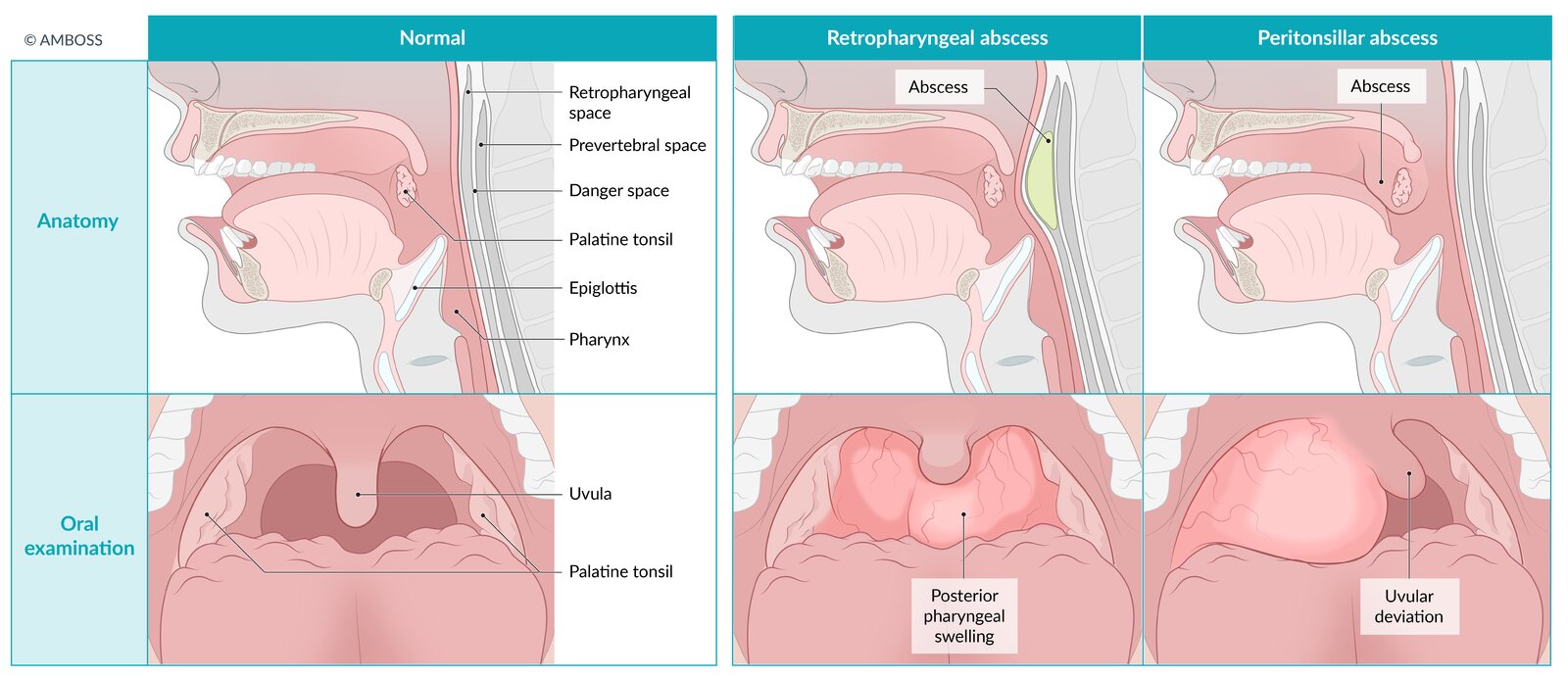
- Uvula shifted to the contralateral side, with inferior and medial displacement of tonsil
- Unilateral fluctuant, swollen, erythematous tonsil with exudates (ipsilateral bulging of the palatine arch)
- Ipsilateral ear pain
- Ipsilateral cervical lymphadenopathy (and neck swelling)
Palpate with a gloved index finger for peritonsillar fluctuance to distinguish an abscess from cellulitis. [10]


Diagnostics [3][11]
Peritonsillar abscess is typically a clinical diagnosis; obtain imaging if there is diagnostic uncertainty and/or concern for complications.
Microbiological studies
- Bacterial culture of abscess aspirate can help to direct therapy for the causative pathogen.
- Obtain a rapid group A streptococcus antigen detection test. [12]
- Consider obtaining EBV serology to rule out infectious mononucleosis.
Evidence of pus on needle aspiration confirms the diagnosis.
Imaging [3]
-
Ultrasound neck (intraoral or transcutaneous) [13]
- Indication: diagnostic uncertainty
- Findings: irregular hypoechoic cavity with a defined circumference
-
CT or MRI neck with IV contrast [14]
- Indication: clinical suspicion of other diagnoses or complications
- Findings
- Fluid collection adjacent to tonsil with rim enhancement
- Uvula deviation
- May show extension of abscess beyond the peritonsillar space [3]
- May show complications (e.g., internal jugular thrombosis, carotid sheath abscess erosion)

Treatment [3][11]
- Patients with respiratory distress: prompt airway management
- Systemic antibiotics (IV or oral) with abscess drainage are the mainstay of therapy.
- Consult ENT and/or oral maxillofacial surgery for consideration of abscess drainage.
- Provide supportive care (e.g., pain management, antipyretic therapy, IV fluid therapy)
- Consider corticosteroids (e.g., dexamethasone ) to reduce inflammation. [3][15]
Antibiotic therapy [3]
- Start empiric antibiotic therapy for deep neck infections.
- Target coverage for aerobes (e.g., Streptococcus spp.) and anaerobes.
- E.g., clindamycin or ampicillin/sulbactam ) [3]
- Tailor to culture and sensitivity results.
- Duration: 10–14 days
Abscess drainage [3]
-
Indications [10]
- Obvious abscess (unless it is < 1 cm and there is no drooling, trismus, or muffled voice)
- Suspected abscess with signs of sepsis or signs of airway compromise
- Lack of rapid response to medical therapy
- Contraindications: severe trismus, coagulopathy [10]
-
Method
- Preferred: needle aspiration or incision and drainage
- Tonsillectomy: may be indicated in certain groups of children and/or for recurrent or treatment-resistant abscesses [3][16]
Complications [17][18]
- Can become life-threatening due to airway compromise
- Further spread of infection into the parapharyngeal space (PPA), retropharyngeal space (RPA), mediastinum (mediastinitis), or fascia (necrotizing fasciitis)
- Aspiration pneumonia
- Internal jugular vein thrombosis or thrombophlebitis
- Bacteremia and sepsis
Disposition [15][19]
- Outpatient management may be appropriate, unless there are risks for complications or previous outpatient therapy was unsuccessful.
- Consider admission for patients who, e.g.: [6]
- Have sepsis, immunocompromise, and/or signs of airway compromise
- Have evidence of abscess extension beyond the peritonsillar region on CT
© AMBOSS
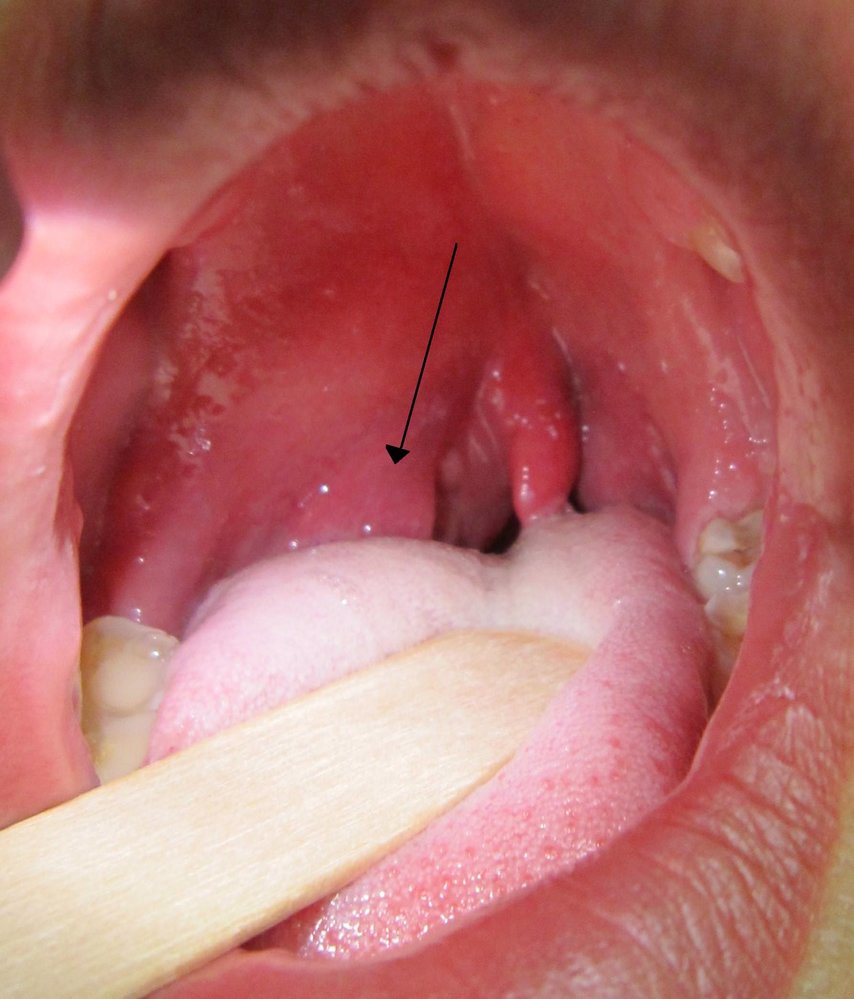
Redness and swelling can be seen on the right side of the anterior palatal arch and of the soft palate. There is a slight left-sided deviation of the soft palate. The uvula shows a distinct redness and is slightly swollen.
These findings are suggestive of a peritonsillar abscess on the right side.
Source: “PeritonsilarAbsess” by James Heilman, MD, Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}
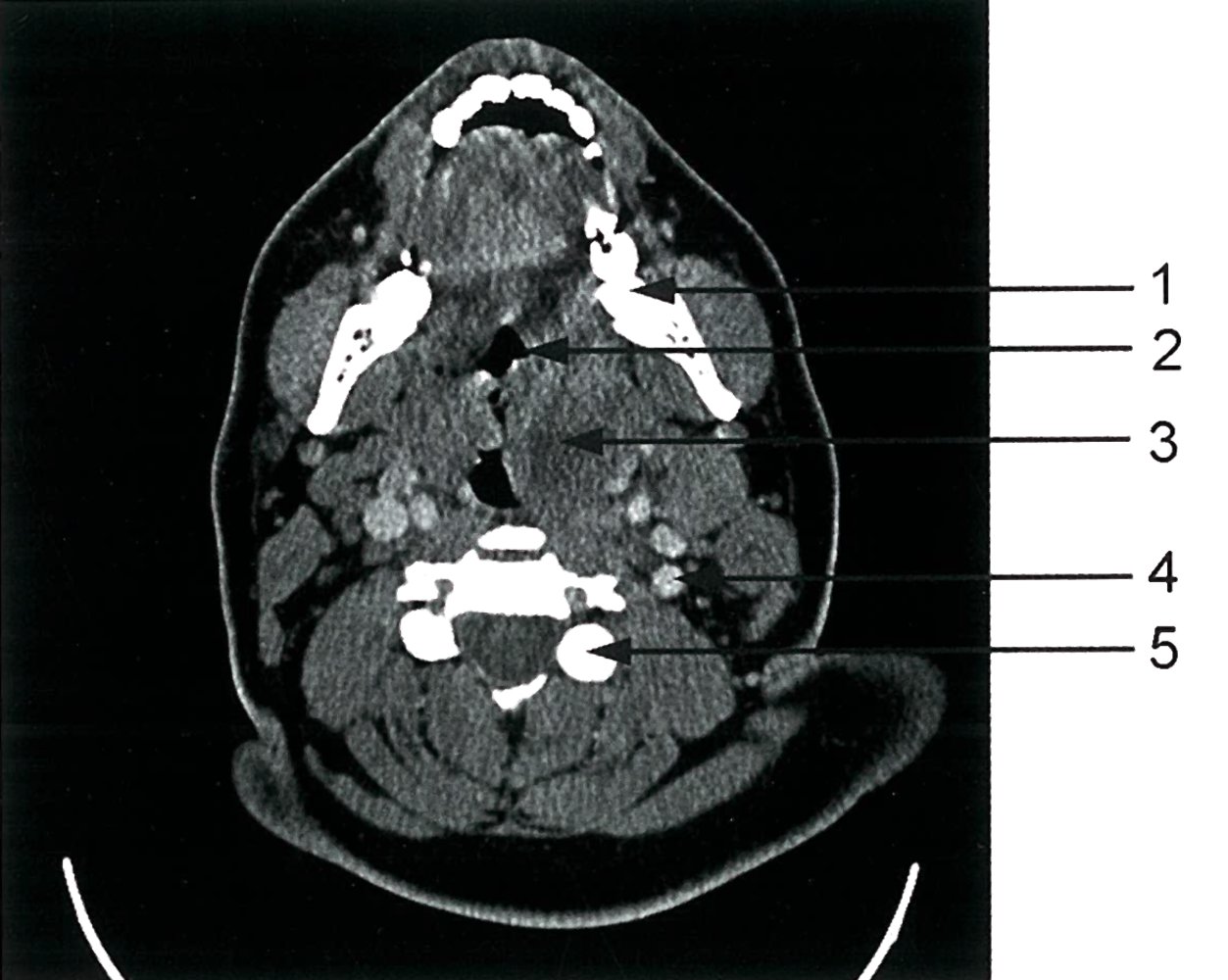
CT neck (with contrast; axial plane) of patient with acute history of progressive dysphagia, odynophagia and subfebrile temperature
A hypodense left peritonsillar mass (blue overlay) with ill-defined borders exerts mass effect that compresses the airway. There is no rim enhancement.
Peritonsillar abscesses typically show a peripheral rim of contrast enhancement corresponding to the abscess capsule. In this case, the diagnosis of a phlegmon should be considered since no rim enhancement is seen.
1: molar; 2: oropharynx; 3: peritonsillar mass; 4; left internal carotid artery; 5: articular process of cervical vertebra
Source: © IMPP
Parapharyngeal abscess
Epidemiology [20]
- Most common in children < 5 years of age
- ♂ > ♀
Etiology [7]
- Pathogens: streptococci (viridans streptococci, S. pneumoniae), staphylococci (including MRSA), Haemophilus influenzae, oral anaerobes (peptostreptococci, Bacteroides species), often in a polymicrobial environment
-
Oropharyngeal infections
- Dental infections (most commonly)
- Acute tonsillitis
- Peritonsillar abscess through the superior constrictor muscle into the parapharyngeal space
- Pharyngeal or salivary gland infections
Clinical features [21]
- Features of peritonsillar abscess, especially trismus
- Posterior space abscess: medial displacement of the lateral pharyngeal wall and tonsil
- Anterior space abscess: indurated swelling below the angle of the mandible down to the hyoid bone
- Respiratory distress: dyspnea, stridor
- Limited cervical neck extension
Diagnostics [2][15]
-
Imaging: required for diagnostic confirmation [22]
- CT neck with IV contrast (preferred) may show: [22][23]
- Hypodense collection with rim enhancement in the lateral pharyngeal space
- Single or multiloculated lesion with central fluid and/or air
-
MRI neck [2]
- Indication: concern for complications
- Findings: similar to CT but with better visualization of soft tissue (e.g., for cellulitis) [15]
- CT neck with IV contrast (preferred) may show: [22][23]
- Microbiological studies (e.g., bacterial culture of abscess aspirate): can help to direct therapy for the causative pathogen


Treatment [23][24]
Systemic IV antibiotics with abscess drainage and supportive care are the mainstays of therapy.
- Patients with respiratory distress: prompt airway management
- Start empiric IV broad-spectrum antibiotics: see “Empiric antibiotic therapy for deep neck infections” for more detail and dosing.
- Switch to targeted antibiotics based on culture and sensitivity results.
- Most patients require surgical drainage or image-guided drainage: Consult ENT and/or oral maxillofacial surgery.
- Provide supportive care (e.g., pain management, antipyretic therapy, IV fluid therapy)
- Consider corticosteroids (e.g., dexamethasone ) to reduce inflammation. [3][15]
- Consult dentistry for abscesses with an odontogenic source for possible removal of the infected tooth.
- Patients should be managed as inpatients.
Conservative treatment with IV antibiotics alone may be considered in select patients (e.g., clinically stable patients with a small abscess).
Complications [7]
- Airway obstruction
- Spread of infection to retropharyngeal space, carotid sheath (presents with torticollis) and then mediastinum (internal carotid artery erosion jugular vein thrombophlebitis, and mediastinitis), or cranial nerves (Horner syndrome, hoarseness, unilateral paresis of the tongue, and other neurologic deficits)
- Aspiration pneumonia with spontaneous pus drainage
- Bacteremia and sepsis
Parapharyngeal infections can become life-threatening because of their proximity to the retropharyngeal space, carotid sheath, and airway!
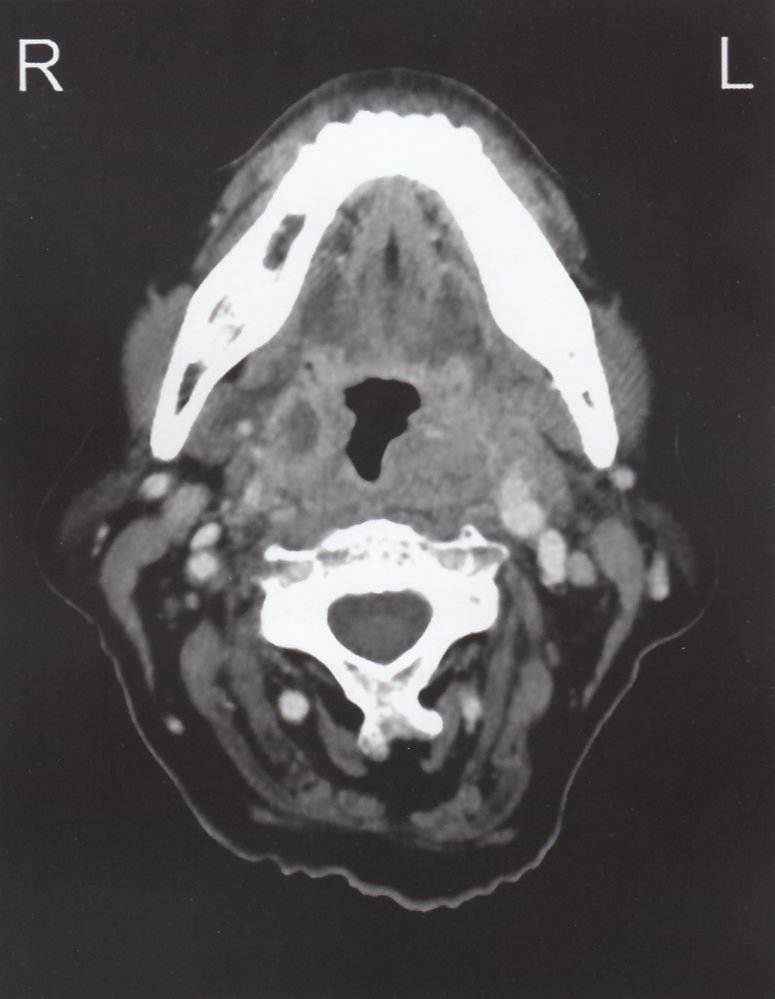
CT neck (with contrast; axial plane) of patient with history of fever and progressive dysphagia for two days
The parapharyngeal soft tissues (green overlay) show contrast enhancement and mass effect narrowing the airway. On the right, a hypodense fluid collection (red overlay) with rim enhancement (white overlay) indicates an abscess.
Blue overlay: carotid artery; green hatched overlay: sternocleidomastoid muscle; M: mandible; red hatched overlay: jugular vein; yellow overlay: lymph node
Source: © IMPP
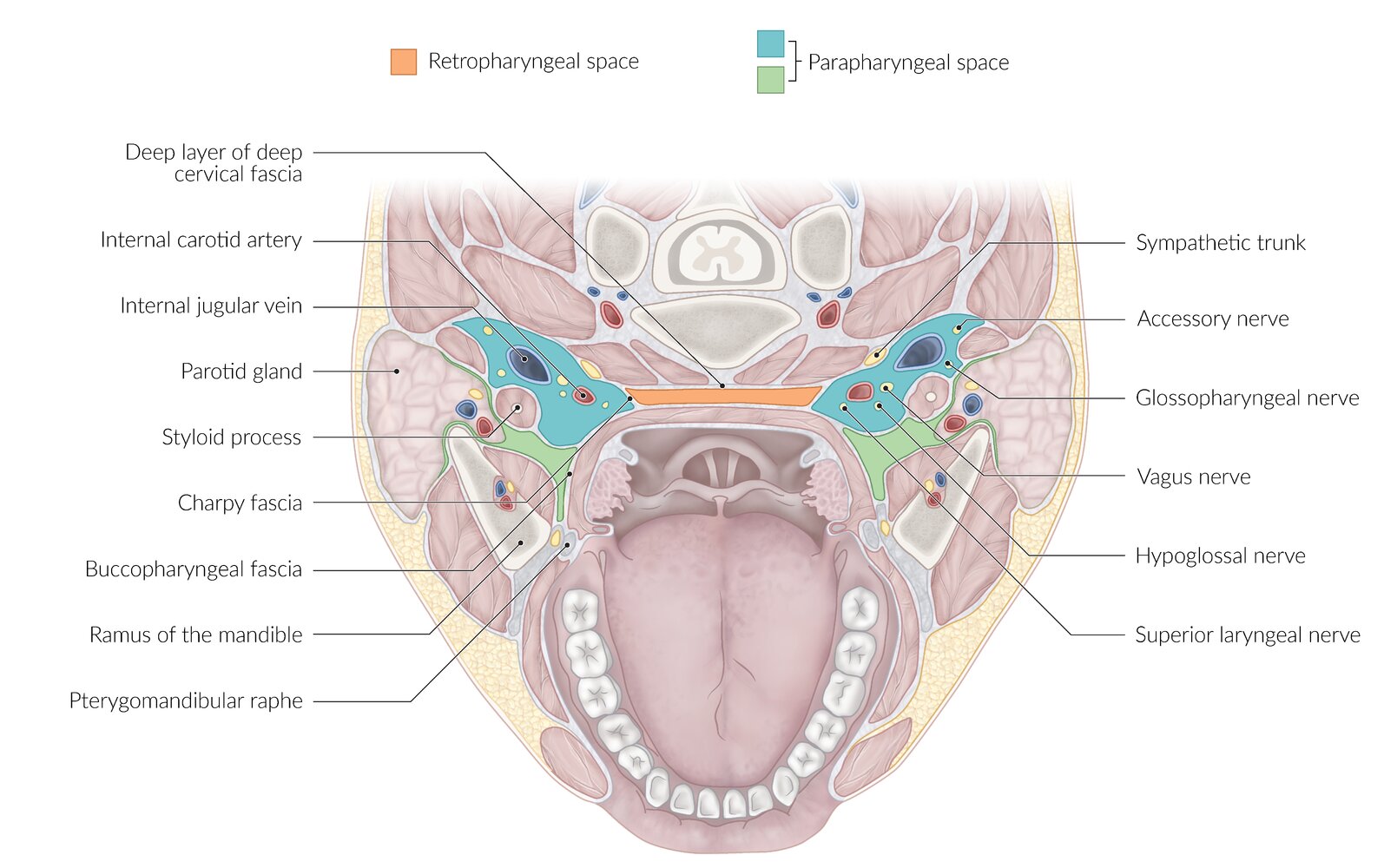
The peripharyngeal space is divided into two parts: the retropharyngeal space and the parapharyngeal space.
© AMBOSS
Retropharyngeal abscess
Epidemiology [20][25]
- Generally the most dangerous deep neck infection
- Most common in children < 5 years of age
- ♂ > ♀
- Overall incidence in the U.S. has increased.
Etiology [26]
- Pathogen: streptococci (viridans streptococci, S. pneumoniae), staphylococci (including MRSA), Haemophilus influenzae, oral anaerobes (peptostreptococci, Bacteroides species), often in a polymicrobial environment
- Direct or indirect causes
- Contiguous or lymphatic spread from oral (most common) or upper respiratory tract infections
- Local penetrating pharyngeal trauma; (e.g., from small bones such as of fish or chicken, or medical instruments)
- Spread from other deep neck infections (nasopharynx, sinuses, adenoids)
Clinical features [27]
- Features of tonsillitis and trismus (minimal)
- Neck asymmetry with unilateral swelling of the posterior pharyngeal wall; (possible fluctuance) → inability to extend neck
- Torticollis
- Anterior cervical lymphadenopathy
- Respiratory distress
- Infants may also present with lethargy, cough, poor intake, rhinorrhea, and agitation.
Diagnostics [28]
Imaging is required for diagnostic confirmation. Microbiological studies can help identify the causative pathogen.
-
CT neck with IV contrast (preferred study) [22]
- Indication: suspicion of RPA with a negative x-ray
- Findings [29]
- Hypodense fluid collection with ring enhancement in the retropharyngeal space
- Posterior pharynx wall with anterior displacement
- May detect spread of infection to other spaces and the presence of foreign bodies
- Differentiates between cellulitis and abscess
-
Lateral x-ray neck ; [29][30]
- Indication: initial screening study in patients with airway compromise or if there is a low level of suspicion for RPA
- Findings
- Widened prevertebral (soft tissue) space with gas or air-fluid levels
- Lordosis
- Evidence of foreign body, if present
-
MRI neck [2][15]
- Indication: contraindication to CT
- Findings are similar to CT with improved detection of:
- Soft tissue changes (e.g., necrosis)
- Complications (e.g., extension of abscess to prevertebral space)
- Microbiological studies (e.g., bacterial culture of abscess aspirate): can help to direct therapy for the causative pathogen

Treatment [15][19][28]
Systemic IV antibiotics with abscess drainage and supportive care are the mainstays of therapy.
- Patients with respiratory distress: prompt airway management
- Start broad-spectrum empiric antibiotics (e.g., clindamycin or ampicillin/sulbactam ): See “Empiric antibiotic therapy for deep neck infections.”
- Switch to targeted antibiotics based on culture and sensitivity results. [28]
- Adult patients usually require needle aspiration or surgical drainage: Consult ENT and/or maxillofacial surgery. [15][28][31]
- Consult dentistry for abscesses with an odontogenic source for possible removal of the infected tooth.
- Provide supportive care (e.g., pain management, antipyretic therapy, IV fluid therapy)
- Consider corticosteroids (e.g., dexamethasone ) to reduce inflammation. [3][15]
- Patients should be managed as inpatients.
Airway management is always the first step if the patient has signs of respiratory distress.
Complications [32]
- Airway obstruction
- Spread of infection to carotid sheath including internal carotid artery erosion and jugular vein thrombophlebitis (Lemierre syndrome)
- Descending mediastinitis (acute necrotizing mediastinitis); . May be visible on chest x-ray as a widened mediastinum +/- bilateral pleural effusions
- Infection can spread and enter the skull base (epidural abscess) or the posterior mediastinum (pericarditis).
- Aspiration pneumonia
- Atlantoaxial dislocation
- Bacteremia and sepsis
© AMBOSS

X-ray neck (lateral view) of a patient with a retropharyngeal abscess
Retropharyngeal soft tissue swelling has produced widening (indicated by left-right arrows) of the prevertebral soft tissues.
Source: “Retroabscess10” by James Heilman, MD, Wikimedia Commons, licensed under CC BY-SA 3.0. Modifications: Original arrow removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
Differential diagnoses
-
Throat pain
- Tonsillitis
- Pharyngitis
- Epiglottitis
-
Painful neck mass [33]
- Cervical adenitis
- Cat-scratch disease
- Acute purulent sialadenitis
-
Neck swelling or respiratory distress
- Anaphylaxis or angioedema
- Retropharyngeal tumors
-
Neck stiffness
- Meningitis
- Cervical spine osteomyelitis
- Dystonia
The differential diagnoses listed here are not exhaustive.
Empiric antibiotic therapy for deep neck infections
General principles
- Infections are typically polymicrobial. [6]
- There is a lack of consensus on the optimal empiric antibiotic regimen and duration. [34]
- Treatment should be individualized in consultation with an infectious disease specialist. [35]
- Switch to targeted antibiotics once culture and sensitivity results are available. [34]
Tailor empiric antibiotic therapy to local antibiograms, suspected pathogen, prior antibiotic use, and disease severity.
Most common pathogens [36]
- Gram-positive: e.g., Staphylococcus aureus, Streptococcus spp., viridans streptococci
- Gram-negative: e.g., Haemophilus influenzae
- Anaerobic: e.g., Porphyromonas, Fusobacterium, Prevotella, Bacteroides, and Peptostreptococcus spp.
Example regimens (for adults) [3]
- Immunocompetent patients
- Amoxicillin/clavulanic acid [3]
- Ampicillin/sulbactam [3]
- Ceftriaxone PLUS metronidazole [3]
- Penicillin allergy: clindamycin
-
Suspected MRSA infection [3]
- Vancomycin OR linezolid
- PLUS metronidazole
- Severe disease, concern for MDRO, and/or immunocompromised patients [3][36]
- Vancomycin
- PLUS piperacillin/tazobactam OR meropenem
Empiric antibiotic regimen for children [35][37]
- Suspected tonsillar or pharyngeal source: [35]
- Clindamycin (off-label) [37]
- Ampicillin-sulbactam (off-label)
- Suspected odontogenic source:
- Penicillin G (off-label)
- PLUS metronidazole (off-label) OR clindamycin (off-label) [35][38]
- Severe disease or suspected MRSA: Add vancomycin (off-label) OR linezolid (off-label). [6][35]
References
- Galioto NJ. "Peritonsillar Abscess". Am Fam Physician. 95(8). :501-506. (2017)
- Long SS, Pickering LK, Prober CG. "Principles and Practice of Pediatric Infectious Disease". Elsevier. (2012). ISBN: 9781437727029
- Kilty SJ, Gaboury I. "Clinical predictors of peritonsillar abscess in adults". J Otolaryngol Head Neck Surg. 37(2). :165-168. (2008)
- Galioto NJ. "Peritonsillar abscess". Am Fam Physician. 77(2). :199-202. (2008)
- Roberts JR. "Roberts and Hedges' Clinical Procedures in Emergency Medicine and Acute Care". Elsevier. (2018). ISBN: 9780323354783
- Klug TE. "Peritonsillar abscess: clinical aspects of microbiology, risk factors, and the association with parapharyngeal abscess.". Dan Med J. 64(3). (2017)
- Choby BA. "Diagnosis and treatment of streptococcal pharyngitis.". Am Fam Physician. 79(5). :383-90. (2009)
- Steyer TE. "Peritonsillar abscess: diagnosis and treatment". Am Fam Physician. 65(1). :93-6. (2002)
- Winegar B, Kabul WS. "Acute neck infections". Imaging in the ED. (2018)
- Esposito S, De Guido C, Pappalardo M, et al. "Retropharyngeal, Parapharyngeal and Peritonsillar Abscesses". Children. 9(5). :618. (2022)
- Baugh RF, Archer SM, Mitchell RB, et al. "Clinical Practice Guideline: Tonsillectomy in Children". Otolaryngol Head Neck Surg. 144(1_suppl). :S1-S30. (2011)
- Bluestone CD, Casselbrant ML, Yellon RF et al. "Pediatric Otolaryngology". Mcgraw-Hill Professional. (2013). ISBN: 9781607950189
- Goldenberg NA, Knapp-clevenger R, Hays T, Manco-johnson MJ. "Lemierre's and Lemierre's-like syndromes in children". Pediatrics. 116(4). :e543-548. (2005)
- Megwalu UC, Shin EJ. "Deep Neck Space Infections & Parapharyngeal Space Neoplasms". McGraw Hill Professional. (2012). ISBN: 9780071624398
- Walls R, Hockberger R, Gausche-Hill M, Erickson TB, Wilcox SR. "Rosen's Emergency Medicine 10th edition- Concepts and Clinical Practice E-Book". Elsevier Health Sciences. (2022). ISBN: 9780323757904
- Woods CR, Cash ED, Smith AM, et al. "Retropharyngeal and Parapharyngeal Abscesses Among Children and Adolescents in the United States: Epidemiology and Management Trends: 2003-2012". J Pediatric Infect Dis Soc. 5(3). :259-268. (2015)
- "Parapharyngeal Abscess". http://www.merckmanuals.com/professional/ear,-nose,-and-throat-disorders/oral-and-pharyngeal-disorders/parapharyngeal-abscess. [2016-10-01]
- Orzell S, Suryadevara A. "Pharyngitis and Pharyngeal Space Infections". Springer International Publishing. :53-66. (2018). ISBN: 9783319910796
- Bou-Assaly W. "Computed tomography imaging of acute neck inflammatory processes". World J Radiol. 2(3). :91. (2010)
- Tubachi J, Hakeem A, Pradeep D, Nayak P. "Surgical Management of Parapharyngeal Abscess". Int J Otorhinolaryngol Clin. 4(3). :122-124. (2012)
- Heim N, Warwas FB, Wiedemeyer V, et al. "The role of immediate versus secondary removal of the odontogenic focus in treatment of deep head and neck space infections. A retrospective analysis of 248 patients". Clin Oral Investig. 23(7). :2921-2927. (2019)
- Qureshi HA, Ference EH, Tan BK, et al. "National trends in retropharyngeal abscess among adult inpatients with peritonsillar abscess". Otolaryngol Head Neck Surg. 152(4). :661-666. (2015)
- Philpott CM, Selvadurai D, Banerjee AR. "Paediatric retropharyngeal abscess". J Laryngol Otol. 118(12). :919-926. (2004)
- Page NC, Bauer EM, Lieu JE. "Clinical features and treatment of retropharyngeal abscess in children". Otolaryngol Head Neck Surg. 138(3). :300-306. (2008)
- Reilly BK, Reilly SJ. "Retropharyngeal Abscess: Diagnosis and Treatment Update". Infect Disord Drug Targets. 12(4). :291-296. (2012)
- Kumar N. "Adult Retropharyngeal Abscess: A Retrospective Case Series". Int J Otorhinolaryngol Clin. 7(2). :100-103. (2015)
- Harkani A, Hassani R, Ziad T, et al. "Retropharyngeal Abscess in Adults: Five Case Reports and Review of the Literature". ScientificWorldJournal. 11. :1623-1629. (2011)
- Khudan A, Jugmohansingh G, Islam S, Medford S, Naraynsingh V. "The effectiveness of conservative management for retropharyngeal abscesses greater than 2 cm". Ann Med Surg. 11. :62-65. (2016)
- Thompson JW, Cohen SR, Reddix P. "Retropharyngeal abscess in children: a retrospective and historical analysis". Laryngoscope. 98(6 Pt 1). :589-592. (1988)
- Chang L, Chi H, Chiu NC, Huang FY, Lee KS. "Deep neck infections in different age groups of children". J Microbiol Immunol Infect. 43(1). (2010)
- Kharel B, Shahi K, Gurung U. "Antibiotic Resistance Pattern in Pediatric Deep Neck Space Infection". Int Arch Otorhinolaryngol.. 26(4). :e585-e591. (2022)
- Kavanagh KR, Valdez TA. "Deep Neck Space Infections in Children: Has Anything changed?". Int J of Head and Neck Surgery. 7(2). :77-82. (2016)
- Brook I. "Microbiology and Principles of Antimicrobial Therapy for Head and Neck Infections". Infect Dis Clin North Am. 21(2). :355-391. (2007)
- McGann KA, Long SS. "Respiratory Tract Symptom Complexes". Elsevier. :164-172.e2. (2017). ISBN: 9780323401814
- AAP Committee on Infectious Diseases. "Red Book: 2021–2024 Report of the Committee on Infectious Diseases". American Academy of Pediatrics. (2021). ISBN: 9781610025218
- Haynes J, Arnold KR, Aguirre-Oskins C, Chandra S. "Evaluation of neck masses in adults.". Am Fam Physician. 91(10). :698-706. (2015)
- Patel VA, Sedeek KA, Wilson MN. "Airway management principles in complex cervicofacial infections". Oper Tech Otolaryngol Head Neck Surg. 31(2). :144-155. (2020)
- Karkos PD, Leong SC, Beer H, Apostolidou MT, Panarese A. "Challenging airways in deep neck space infections". Am J Otolaryngol. 28(6). :415-418. (2007)
- Siewert JR. "Chirurgie". Springer Verlag (2006). ISBN: 9783540304500
- de Virgilio C, Frank PN, Grigorian A. "Surgery: A Case Based Clinical Review". Springer. (2015). ISBN: 9781493917259
- Schlossberg D. "Clinical Infectious Disease". Cambridge University Press. (2015). ISBN: 9781107038912
- Walls R, Hockberger R, Gausche-Hill M. "Rosen's Emergency Medicine - Concepts and Clinical Practice". Elsevier Health Sciences. (2013). ISBN: 9780323390163
- Marx J, Walls R, Hockberger R. "Rosen's Emergency Medicine - Concepts and Clinical Practice E-Book". Elsevier Health Sciences. (2013). ISBN: 9781455749874
- Ferri FF. "Ferri's Clinical Advisor". Elsevier Health Sciences. (2013). ISBN: 0323084311
- Jameson JL, Fauci AS, Kasper DL, et al. "Harrison's Principles of Internal Medicine, Twentieth Edition (Vol.1 & Vol.2)". McGraw-Hill Education / Medical. (2018). ISBN: 9781259644030
- Maroldi R, Farina D, Ravanelli M, Lombardi D, Nicolai P. "Emergency Imaging Assessment of Deep Neck Space Infections". Seminars in Ultrasound, CT and MRI. 33(5). :432-442. (2012)
- Tabas, J & Reynolds, T. "High Risk Emergencies: Emergency Medicine Clinics of North America". Saunders. :121. (2010). ISBN: 9781437718140
- Van TT, Naccache SN, Dien Bard J. "The Brief Case: Retropharyngeal Abscess in a 14-Year-Old Caused by Fusobacterium necrophorum". J Clin Microbiol. 56(12). (2018)
- Allegrini D, Autelitano A, Nocerino E, et al. "Grisel’s syndrome, a rare cause of anomalous head posture in children: a case report". BMC Ophthalmol. 16(1). (2016)
- Corsten MJ, Shamji FM, Odell PF, et al. "Optimal treatment of descending necrotising mediastinitis". Thorax. 52(8). :702-708. (1997)
- McLeod C, Stanley KA. "Images in emergency medicine: retropharyngeal abscess.". West J Emerg Med. 9(1). :55. (2008)
- Zaoutis, LB & Chiang VW. "Comprehensive pediatric hospital medicine". Elselvier Health Sciences. (2007). ISBN: 9780323030045
- Reid, J; Lee, E; Angelisa Paladin, A; Davros, W & Carrico C. "Pediatric Radiology". OUP USA. :13. (2014). ISBN: 9780199755325
- Tanaka K, Inokuchi R, Namai Y, Yahagi N. "Retropharyngeal cellulitis in adolescence". BMJ Case Rep. 2013(may17 1). :bcr2013009684-bcr2013009684. (2013)
- Hansen BW, Ryndin S, Mullen KM. "Infections of Deep Neck Spaces". Semin Ultrasound CT MR. 41(1). :74-84. (2020)
- Smith MM, Heubi CH. "Infections of the Neck and Pharynx in Children". Curr Treat Options Pediatr. 4(2). :211-220. (2018)
- Schott CK, Counselman FL, Ashe AR. "A Pain in the Neck: Non-traumatic Adult Retropharyngeal Abscess". J Emerg Med. 44(2). :329-331. (2013)
- Lander L, Lu S, Shah RK. "Pediatric retropharyngeal abscesses: A national perspective". Int J Pediatr Otorhinolaryngol. 72(12). :1837-1843. (2008)
- Hochstim CJ, Messner AH. "Pediatric Inflammatory Neck Mass". Current Treatment Options in Pediatrics. 2(3). :216-223. (2016)
- Sudhanthar S, Garg A, Gold J, Napolova O. "Parapharyngeal abscess: A difficult diagnosis in younger children". Clinical Case Reports. 7(6). :1218-1221. (2019)
- Duval M, Daniel SJ. "Retropharyngeal and parapharyngeal abscesses or phlegmons in children". Int J Pediatr Otorhinolaryngol. 72(12). :1765-1769. (2008)
- Klug TE, Fischer ASL, Antonsen C, et al. "Parapharyngeal abscess is frequently associated with concomitant peritonsillar abscess". European Archives of Oto-Rhino-Laryngology. 271(6). :1701-1707. (2013)
- Alaani A, Griffiths H, Minhas SS, Olliff J, Drake Lee AB. "Parapharyngeal abscess: diagnosis, complications and management in adults". Eur Arch Otorhinolaryngol. 262(4). :345-350. (2004)
- Blumberg JM, Judson BL. "Surgical management of parapharyngeal space infections". Oper Tech Otolayngol Head Neck Surg. 25(3). :304-309. (2014)
- Johnston J, Stretton M, Mahadevan M, Douglas RG. "Peritonsillar abscess: A retrospective case series of 1773 patients". Clin Otolaryngol. 43(3). :940-944. (2018)
- Marom T, Cinamon U, Itskoviz D, Roth Y. "Changing trends of peritonsillar abscess". Am J Otolaryngol. 31(3). :162-167. (2010)
- Allen DZ, Rawlins K, Onwuka A, Elmaraghy CA. "Comparison of inpatient versus outpatient management of pediatric peritonsillar abscess outcomes". Int J Pediatr Otorhinolaryngol. 123. :47-50. (2019)
- Sowerby LJ, Hussain Z, Husein M. "The epidemiology, antibiotic resistance and post-discharge course of peritonsillar abscesses in London, Ontario". J Otolaryngol Head Neck Surg. 42(1). :5. (2013)
- Chin RL, Frazee BW, Coralic Z. "Emergency Management of Infectious Diseases". Cambridge University Press. (2018). ISBN: 9781107153158
- Powell J, Wilson JA. "An evidence-based review of peritonsillar abscess". Clin Otolaryngol. 37(2). :136-145. (2012)
- Rao M, Linga R., Vishwanathan P. "Anaesthetic management of difficult airway due to retropharyngeal abscess". Indian J Anaesth. 54(3). :246. (2010)
- Cho SY, Woo JH, Kim YJ, et al. "Airway management in patients with deep neck infections". Medicine. 95(27). :e4125. (2016)
- Tansey JB, Hamblin J, Mamidala M, et al. "Dexamethasone Use in the Treatment of Pediatric Deep Neck Space Infections". Ann Otol Rhinol Laryngol. 129(4). :376-379. (2019)
- Anand H Kulkarni, Swarupa D Pai, Basant Bhattarai, Sumesh T Rao, M Ambareesha. "Ludwig's angina and airway considerations: a case report". Cases J. 1(1). (2008)
- Hegenbarth MA. "Preparing for Pediatric Emergencies: Drugs to Consider". Pediatrics. 121(2). :433-443. (2008)
- Pluijms WA, van Mook WN, Wittekamp BH, Bergmans DC. "Postextubation laryngeal edema and stridor resulting in respiratory failure in critically ill adult patients: updated review". Crit Care. 19(1). (2015)
- Duprey K, Rose J, Fromm C. "Ludwig’s angina". Int J Emerg Med. 3(3). :201-202. (2010)
- Jamiela A. McDonnough, Deawodi A. Ladzekpo, Iasson Yi, et al. "Epidemiology and resource utilization of ludwig's angina ED visits in the United States 2006–2014". Laryngoscope. 129(9). :2041-2044. (2019)
- Nicholas Costain, Thomas J. Marrie. "Ludwig's Angina". Am J Med. 124(2). :115-117. (2011)
- N. P L, V. N S, B. Jenkins. "Ludwig's angina: need for including airways and larynx in ultrasound evaluation". BMJ Case Rep. 2014(nov09 1). :bcr2014206506-bcr2014206506. (2014)
- Arslan Fatma Zeynep, Altunkeser Ayşegul, Turgut Bekir, Erdogan Hasan. "Ludwig's Angina: A Rapid Radiological and Clinical Nightmare". Clin Med Img Lib. 3(3). (2017)
- Wael Hasan, David Leonard, John Russell. "Ludwig's Angina—A Controversial Surgical Emergency: How We Do It". Int J Otolaryngol. 2011. :1-4. (2011)
- Edetanlen BE, Saheeb BD. "Comparison of Outcomes in Conservative versus Surgical Treatments for Ludwig’s Angina". Med Princ Pract. 27(4). :362-366. (2018)
- Fleisher LA, Roizen MF. "Essence of Anesthesia Practice E-Book". Elsevier Health Sciences. (2010). ISBN: 9781455700868
- Maharaj S, Ahmed S, Pillay P. "Deep Neck Space Infections: A Case Series and Review of the Literature". Clin Med Insights Ear Nose Throat. 12. :117955061987127. (2019)
- Flint PW, Haughey BH, Robbins KT, et al. "Cummings Otolaryngology - Head and Neck Surgery E-Book". Elsevier Health Sciences. (2014). ISBN: 9780323278201
- Wang B, Gao B-L, Xu G-P, Xiang C. "Images of deep neck space infection and the clinical significance". Acta radiol. 55(8). :945-951. (2014)
- McGahan JP, Schick MA, Mills L. "Fundamentals of Emergency Ultrasound". Elsevier Health Sciences. (2019). ISBN: 9780323596510
- Kalmovich LM, Gavriel H, Eviatar E, Kessler A. "Accuracy of Ultrasonography Versus Computed Tomography Scan in Detecting Parapharengeal Abscess in Children". Pediatr Emerg Care. 28(8). :780-782. (2012)
- Simard RD, Socransky S, Chenkin J. "Transoral Point-of-Care Ultrasound in the Diagnosis of Parapharyngeal Space Abscess". J Emerg Med. 56(1). :70-73. (2019)
- Capps EF, Kinsella JJ, Gupta M, Bhatki AM, Opatowsky MJ. "Emergency Imaging Assessment of Acute, Nontraumatic Conditions of the Head and Neck". Radiographics. 30(5). :1335-1352. (2010)
- Lawrence R, Bateman N. "Controversies in the management of deep neck space infection in children: an evidence-based review". Clin Otolaryngol. 42(1). :156-163. (2016)
- Cheng J, Elden L. "Children with Deep Space Neck Infections". Otolaryngol Head Neck Surg. 148(6). :1037-1042. (2013)
- Kanekar S, Mannion K. "Imaging of Head and Neck Spaces for Diagnosis and Treatment, An Issue of Otolaryngologic Clinics, E-Book". Elsevier Health Sciences. (2012). ISBN: 9781455758692
- Flint PW, Haughey BH, Niparko JK, et al. "Cummings Otolaryngology - Head and Neck Surgery E-Book". Elsevier Health Sciences. (2010). ISBN: 9780323080873
- Bailey BJ, Johnson JT, Newlands SD. "Head & Neck Surgery--otolaryngology". Lippincott Williams & Wilkins. (2006). ISBN: 9780781755610
- Bluestone, CD. "Pediatric Otolaryngology". Gulf Professional Publishing. (2003). ISBN: 9789997619846