Quick guide
Diagnostic approach
- Assess for clinical features of DVT.
- Calculate Wells score for DVT.
- Low PTP: D-dimer
- High PTP or positive D-dimer: DVT POCUS and/or lower extremity venous US

Red flag features
- Signs of pulmonary embolism
- Phlegmasia cerulea dolens
- Limb-threatening ischemia
Management checklist
- Assess for pulmonary embolism.
- Estimate bleeding risk with anticoagulation.
- Start anticoagulation for DVT (e.g., rivaroxaban , apixaban ).

© AMBOSS
© AMBOSS
Summary
Deep vein thrombosis (DVT) is the formation of a blood clot within the deep veins, most commonly those of the lower extremities. The main risk factors for DVT are vascular endothelial damage (e.g., surgery or trauma), venous stasis (e.g., immobility), and hypercoagulability (e.g., thrombophilia), collectively referred to as the Virchow triad. Symptoms include edema, warmth, and dull pain of the affected extremity. Patients may also present with features of pulmonary embolism (PE), a severe complication of DVT. The Wells criteria for DVT are used to determine the pretest probability (PTP) of DVT in nonpregnant adults. The initial test of choice for DVT in nonpregnant adults is D-dimer in patients with a low PTP and venous ultrasound (US) in patients with moderate or high PTP. A negative D-dimer assay (i.e., levels < 500 ng/mL) allows DVT to be ruled out, while a positive D-dimer (levels ≥ 500 ng/mL) is nonspecific and requires a venous ultrasound to confirm the diagnosis. Noncompressibility of the affected vein is the most important sonographic feature of DVT. Long-term anticoagulation for 3–6 months is recommended in all patients with DVT, except for isolated asymptomatic distal DVT, for which expectant management with serial ultrasound may be considered, as the risk of postthrombotic sequelae is low. Prevention of recurrent DVT (i.e., anticoagulation extended indefinitely after completion of primary treatment) is recommended for select patients, depending on the extent and etiology of the DVT and the patient's bleeding risk. Catheter-directed thrombolysis or thrombectomy may be considered for limb-threatening ischemia, acute iliofemoral DVT, and patients with contraindications to anticoagulation. Primary prevention of VTE is recommended in patients at risk of DVT or PE (e.g., seriously ill medical patients, most surgical patients, and long-distance travelers with additional risk factors for VTE) and includes mechanical and pharmacological measures.
Definitions
-
Deep vein thrombosis (DVT): the formation of one or more blood clots in a deep vein, typically of the lower extremities [1][2][3]
- Proximal DVT: DVT of the lower extremity affecting the femoral vein, profunda femoris vein, and/or the popliteal vein (up to the calf vein trifurcation) [4]
- Distal DVT: DVT of the lower extremity that is confined to the veins beyond the calf vein trifurcation (i.e., below the knee joint)
-
Venous thromboembolism (VTE): an umbrella term that encompasses DVT and pulmonary embolism (PE)
- Recurrent VTE: VTE that recurs in a patient after the completion of the first 2 weeks of antithrombotic therapy. [5]
- Provoked VTE: VTE in an individual with ≥ 1 risk factor for VTE
- Unprovoked VTE (idiopathic VTE): VTE in an individual without risk factors for VTE
Etiology
Any factor that causes hypercoagulability, endothelial damage, and/or venous stasis can cause DVT (see “Virchow triad”).
| Risk factors for venous thromboembolism [6][7] | |
|---|---|
| Transient risk factors | Chronic risk factors |
|
|
Remember DVT risk factors using the mnemonic “THROMBOSIS”: Travel, Hypercoagulable/HRT, Recreational drugs, Old (> 60), Malignancy, Blood disorders, Obesity/Obstetrics, Surgery/Smoking, Immobilization, Sickness (CHF/MI, IBD, nephrotic syndrome, vasculitis)!
References:[11]
Pathophysiology
The Virchow triad
The Virchow triad refers to the three main pathophysiological components of thrombus formation.
- Hypercoagulability: increased platelet adhesion, thrombophilia (e.g., factor V Leiden mutation), use of oral contraceptives, pregnancy
- Endothelial damage: Inflammatory or traumatic vessel injuries can lead to activation of clotting factors through contact with exposed subendothelial collagen.
- Venous stasis: varicosis, external pressure on the extremity, immobilization (e.g., hospitalization, bed rest, long flights or bus rides), local application of heat
To remember the three pathophysiological components of thrombus formation, think: “HE'S Virchow”: H-Hypercoagulability, E-Endothelial damage, S-Stasis.
References:[12]
Clinical features
Deep vein thrombosis may be asymptomatic.
-
Localized unilateral symptoms
- Typically affects deep veins of the legs, thighs, or pelvis
- Swelling, feeling of tightness or heaviness
- Warmth, erythema, and possibly livid discoloration
-
Progressive tenderness, dull pain
- Homans sign: calf pain on dorsal flexion of the foot
- Meyer sign: Compression of the calf causes pain.
- Payr sign: pain when pressure is applied over the medial part of the sole of the foot
- Distention of superficial veins
- Distal pulses are normal.
- General symptoms: : fever [13]
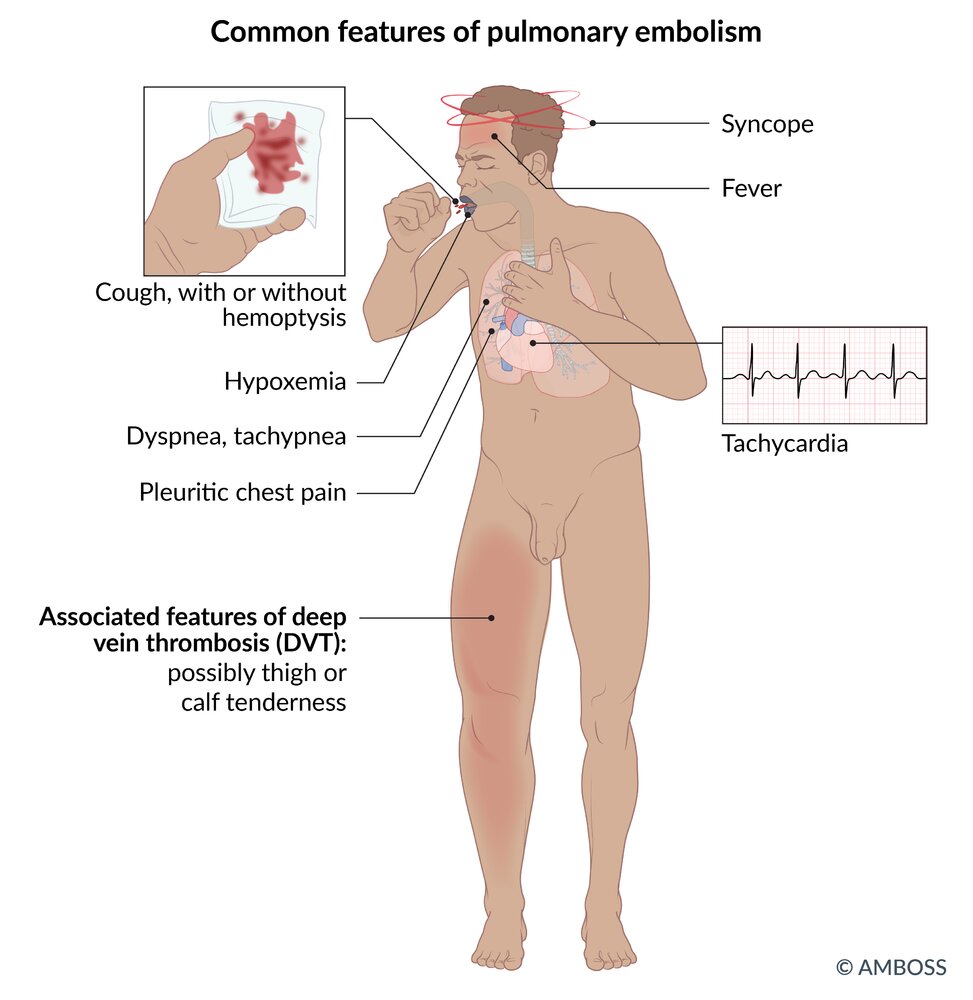
- Possible signs of pulmonary embolism: dyspnea, chest pain, dizziness, weakness
- See also “Clinical features of UEDVT.”
")

There is diffuse edema and erythema of the right leg and foot. The diameter of the right calf is visibly greater than that of the left.
These features are typical of DVT. Clinical history and investigations (e.g., Doppler ultrasonography, D-dimer levels) help distinguish between DVT and cellulitis, which also manifests with a painful, warm, erythematous, and edematous leg.
Source: “Deep vein thrombosis of the right leg” by James Heilman, MD, Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}
Subtypes and variants
Upper extremity deep vein thrombosis (UEDVT) [14]
Definitions
- Proximal UEDVT: thrombosis of the axillary or subclavian vein
- Distal UEDVT: thrombosis of the brachial, radial, ulnar, or interosseus veins
- Primary UEDVT (Paget-Schroetter syndrome): UEDVT due to an underlying anatomical abnormality, repetitive injury to the vein, or an unknown cause
- Secondary UEDVT: UEDVT due to an indwelling device in the vein or a hypercoagulable state
Epidemiology
- UEDVT is less common than lower extremity DVT.
- Primary UEDVT typically occurs in young individuals, while secondary UEDVT typically occurs in older adults.
- Secondary UEDVT is more common than primary UEDVT.
- Proximal UEDVT is more common than distal UEDVT with the subclavian vein being the most commonly affected.
- Multiple vein involvement occurs in approx. 60% of patients with UEDVT.
Etiology
-
Primary UEDVT
- Venous thoracic outlet syndrome due to increased muscle bulk, fibrotic connective tissue, abnormal ligamentous insertion, or osseous abnormalities (e.g., cervical rib)
- Effort-induced thrombosis: repetitive strenuous activity involving the upper extremities (e.g., weight-lifting, gymnastics, operation of a jackhammer)
-
Secondary UEDVT
-
Venous devices
- Central venous catheters and port systems
- Pacemaker leads
-
Hypercoagulable states
- Malignancy
- Hereditary thrombophilia
- Pregnancy
- Oral contraceptive use
- Prolonged upper extremity immobilization
-
Venous devices
Clinical features of UEDVT
- Symptoms tend to be more severe with proximal UEDVT than with distal UEDVT.
-
Acute thrombosis
- Discoloration, swelling, and/or pain in the affected arm
- Superficial venous engorgement
-
Chronic thrombosis
- Often asymptomatic until complete occlusion occurs
- Even with complete occlusion, symptoms are often nonspecific or minimal as drainage through collateral veins can partially compensate for occlusion.
Management [15][16][17]
-
Initial evaluation
-
Calculate the pretest probability of UEDVT using the dichotomized Constans score. [18]
- One point is given for each of the following:
- The presence of a device in the vein
- Unilateral edema
- Localized pain
- One point is subtracted if another diagnosis is at least equally plausible.
- A score of ≥ 2 indicates a high likelihood of UEDVT.
- One point is given for each of the following:
- UEDVT likely (dichotomized Constans score ≥ 2): perform duplex ultrasonography or measure D-dimers
- UEDVT unlikely (dichotomized Constans score < 2): measure D-dimers
- If D-dimers are negative: UEDVT can be ruled out.
- If D-dimers are positive: perform duplex ultrasonography
-
Calculate the pretest probability of UEDVT using the dichotomized Constans score. [18]
-
Further evaluation
- If initial duplex ultrasonography is negative but clinical suspicion remains high:
- Consider repeating duplex ultrasonography.
- Consider alternative imaging modalities such as CT or MR venography.
- If primary UEDVT is suspected: Consider a chest x-ray to screen for bone abnormalities (see “Diagnostics” in “Thoracic outlet syndrome”).
- If secondary UEDVT due to a hypercoagulable state is suspected: Consider screening for occult malignancy or inherited thrombophilia (see “Diagnostics” in “Hypercoagulable states”).
- If initial duplex ultrasonography is negative but clinical suspicion remains high:
-
Initial treatment
-
Proximal UEDVT
- First-line: anticoagulation therapy
- Second-line: catheter-directed thrombolysis in patients with limb-threatening or severe symptoms despite anticoagulation and no contraindications for thrombolytic therapy
-
Distal UEDVT
- Symptomatic patients: anticoagulation therapy
- Asymptomatic patients: typically expectant management with repeat duplex ultrasonography to monitor the clot
-
Proximal UEDVT
-
Anticoagulation therapy in UEDVT
- Initiate parenteral anticoagulation using unfractionated heparin or low molecular weight heparin (LMWH)
- Continue long-term anticoagulation for at least 3 months with LMWH, vitamin K antagonists, or direct oral anticoagulants.
-
Further treatment based on the underlying cause
- Primary UEDVT: Consider thoracic outlet decompression surgery if symptoms persist despite anticoagulation and thrombolysis.
-
Secondary UEDVT due to a venous device
- Leave the device in situ if the patient has proximal UEDVT and does not have an indication for device removal.
- Indications for device removal
- Failure of symptoms to resolve with anticoagulation
- Contraindication to anticoagulation
- Evidence of a central line-associated blood stream infection (see “Indications for intravascular catheter removal”)
- The device is no longer needed.
Differential diagnosis
- Neurologic or arterial thoracic outlet syndrome
- Superior vena cava syndrome
- Complex regional pain syndrome
- Secondary lymphedema
- Brachial neuritis
- Quadrilateral pain syndrome
- Cervical nerve root compression
- Peripheral nerve compression
Complications
- Pulmonary embolism
- Superior vena cava syndrome
- Postthrombotic syndrome
- Recurrence of a UEDVT

Phlegmasia cerulea dolens
- Definition: : a severe form of DVT characterized by obstruction of all veins of one extremity, with subsequent restriction of arterial flow; associated with high mortality
-
Symptoms
- Severe swelling, edema, and pain
- Coldness, cyanosis, and pulselessness
-
Treatment
- Emergency surgery: venous thrombectomy, fasciotomy
- Fibrinolysis if surgery fails
- Amputation as last resort
- Complications: shock, gangrene, acute renal failure (due to rhabdomyolysis)
Click on the overlay icon below the taskbar on the left to toggle the overlay on and off.
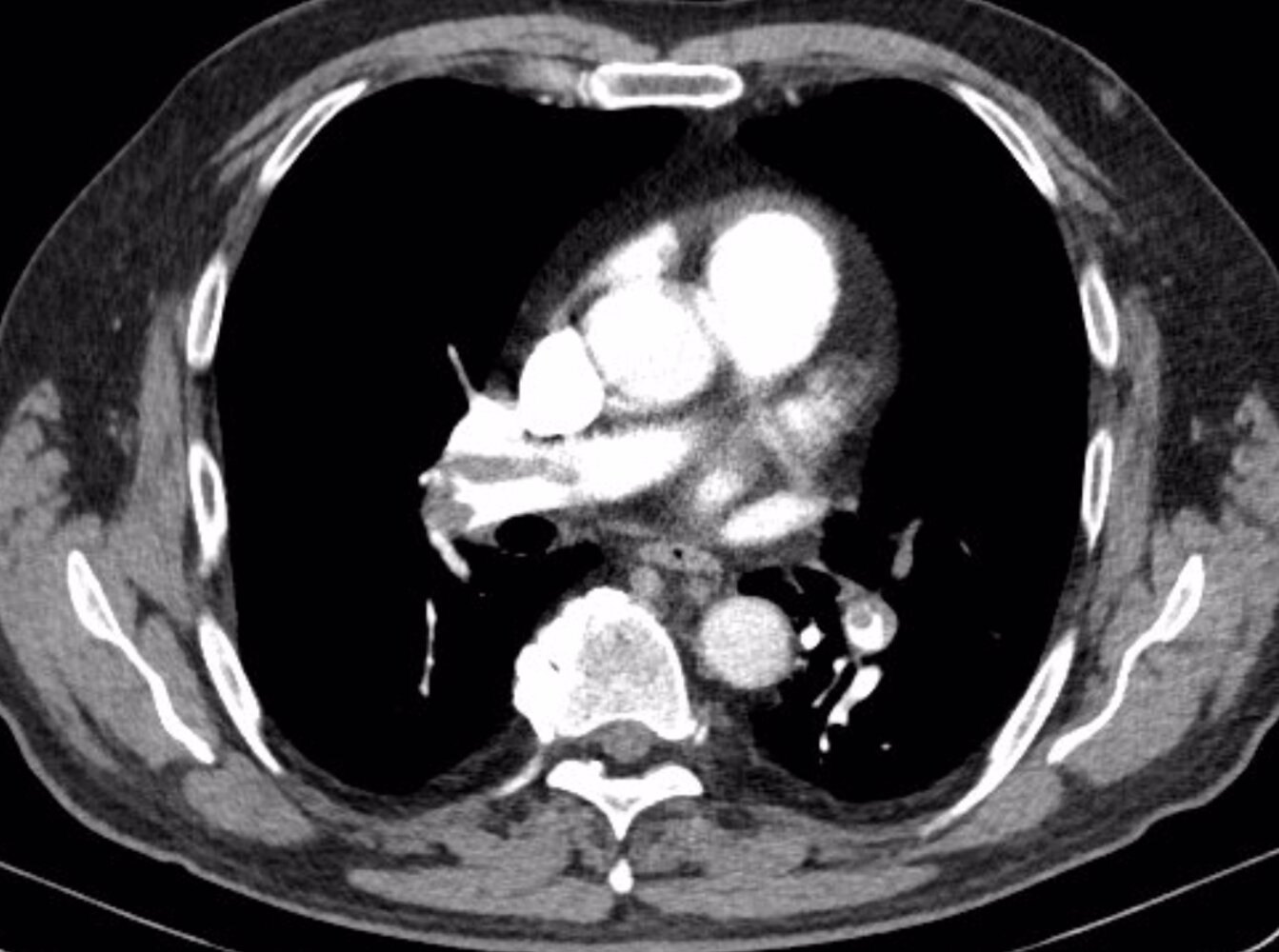
CT chest (with contrast; axial plane, lung window; axial plane, mediastinal window; coronal plane, mediastinal window) of a patient with shortness of breath, post-circulatory collapse, elevated D-dimer (5,086 ug/L; normal < 5), and normal C-reactive protein (CRP; < 3.0 mg/L)
Multiple intraluminal filling defects in the right and left pulmonary arteries and their lobar, segmental, and subsegmental branches represent pulmonary emboli of different age. The acute emboli are seen as central filling defects, whereas the older emboli are eccentric and show irregular thickening of the arterial wall.
Right ventricular and atrial enlargement, septal flattening, and contrast reflux into the hepatic veins are evidence of right ventricular strain. The causes of ground glass opacification in the left upper lobe and misty mesentery with nodes in the upper abdomen are not readily evident. Incidental findings include a hypodense cyst within a small, irregular left kidney and slight deformity of the right sixth rib from a previous fracture.
Our great thanks to Nándor Faluhelyi (University of Pécs, Medical School) for kindly providing this image.
Wells score
- The Wells score for DVT, also known as the Wells criteria, is used to calculate the pretest probability of DVT of the lower extremities in nonpregnant adults. [19][20]
- A different version of the score is used to determine the probability of PE (see “Wells criteria for PE”).
| Modified Wells criteria for deep vein thrombosis [19][20][21] | ||
|---|---|---|
| Criteria | Score | |
| Medical history | Active cancer | + 1 |
| Previously documented DVT | + 1 | |
| Immobilization | Paralysis, paresis, or recent (cast) immobilization of lower extremity | + 1 |
| Recently bedridden for ≥ 3 days OR underwent major surgery within the past 12 weeks under general/local anesthesia | + 1 | |
| Clinical features | Tenderness localized along the deep venous system | + 1 |
| Swelling of the entire leg | + 1 | |
| Calf swelling ≥ 3 cm compared to the contralateral leg | + 1 | |
| Pitting edema confined to the symptomatic leg | + 1 | |
| Distended collateral superficial veins (nonvaricose) | + 1 | |
| Differential diagnosis | Alternative diagnosis as likely as or more likely than DVT | - 2 |
Interpretation (pretest probability for DVT) [15]
| ||
The Wells score can overestimate the probability of DVT in patients with concomitant signs of lower extremity cellulitis due to overlap in the clinical manifestations. [22]

This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
Diagnosis
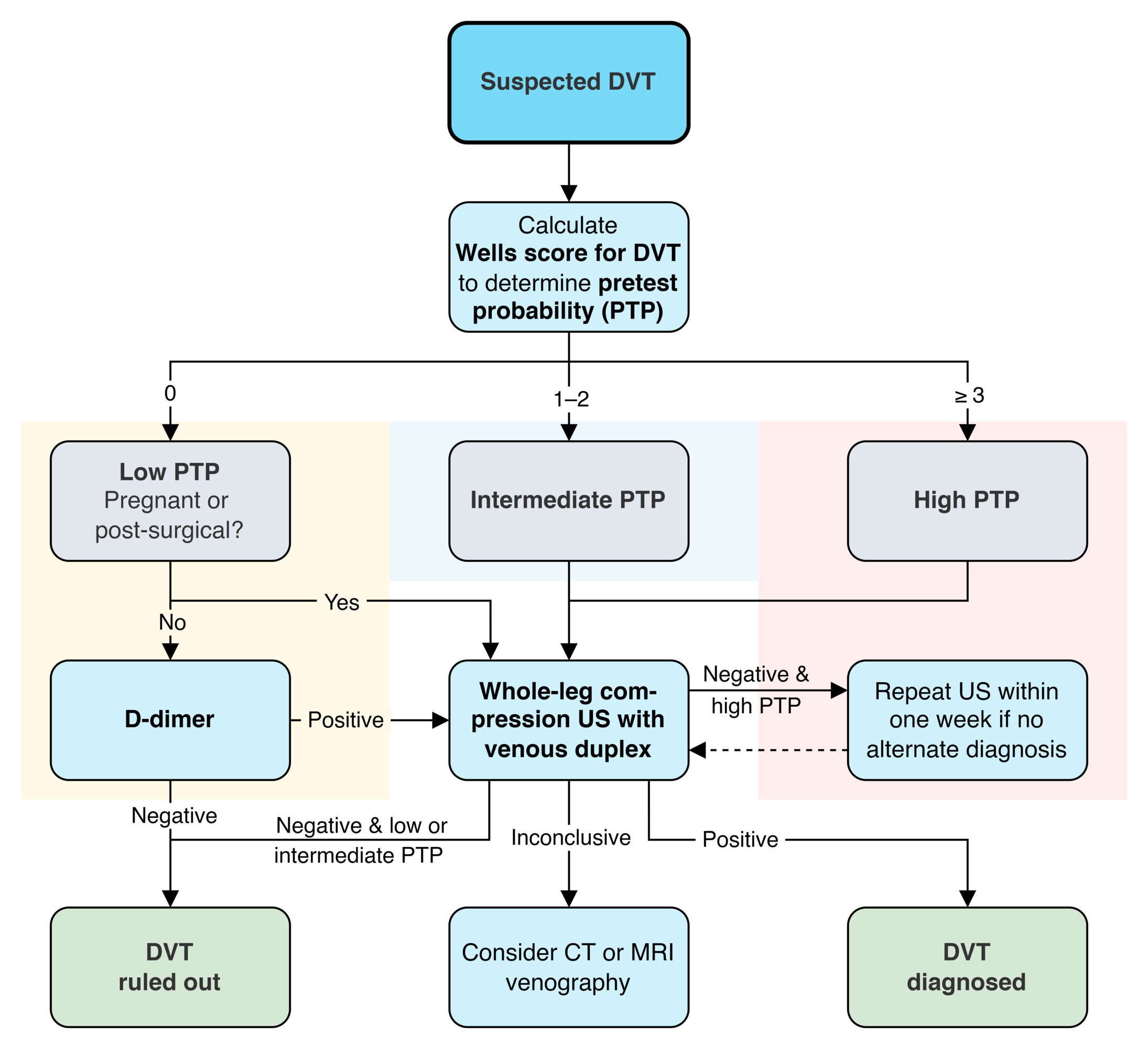
Diagnostic approach for suspected lower-extremity DVT [4][15][23]
This approach is valid for evaluating a first-episode or recurrent lower extremity DVT. [15]
- Calculate the pretest probability (PTP) using Wells criteria for DVT.
-
Check D-dimer first for low PTP (initial D-dimer is not diagnostically helpful for intermediate and high PTP). ; [24]
- Negative (< 500 ng/mL): DVT ruled out
- Positive (≥ 500 ng/mL): Possible DVT; Proceed to venous US.
- Obtain venous ultrasound (US) for intermediate or high PTP, or low PTP with positive D-Dimer [23]
- Negative US
- Intermediate and low PTP: DVT ruled out
- High PTP: Repeat venous US within a week if no alternate diagnosis. [4]
- Positive US: DVT confirmed; Screen for an underlying cause if no risk factors for DVT are identified on initial evaluation.
- Inconclusive US: Consider venography, CT venography, or MR venography.
- Negative US
A negative D-dimer can help rule out DVT without venous ultrasound in patients with low pretest probability. It is not helpful for patients with intermediate or high pretest probability.
The positive yield of investigations for concomitant DVT (i.e., using the Wells score, D-Dimer, and/or venous ultrasound) is low for patients with a high likelihood of lower extremity cellulitis. A selective rather than routine approach to evaluating for DVT is preferred in these patients to avoid unnecessary testing. [22]
Initial evaluation of DVT
Based on the patient's pretest probability, the initial test to evaluate for DVT may be either D-dimer or compression ultrasound.
Severe swelling and edema with concomitant coldness, cyanosis, and pulselessness should raise concern for phlegmasia cerulea dolens, which requires emergency surgery.
D-dimer [15][23]
- Indication: preferred initial test for nonpregnant patients with a low PTP of DVT (Wells score = 0)
-
Interpretation
- Cutoff for normal range is typically 500 ng/mL
- Some centers use age-adjusted D-dimer cutoffs (See also “Diagnostics” in “Pulmonary embolism”) [25][26][27]
-
Accuracy
- High sensitivity (∼ 96%)
- Low specificity (∼ 36%) [4]
- Not reliable for ruling out DVT in patients with intermediate or high PTP
In patients with a low pretest probability of DVT, a negative D-dimer (< 500 ng/mL) rules out DVT. [15]
A positive D-dimer alone does not confirm DVT. [15]
Lower extremity venous ultrasound [4][15][23][28]
-
Indications
- Preferred initial test for patients with moderate or high PTP of lower extremity DVT (Wells score ≥ 1)
- Preferred initial test for pregnant or postsurgical patients even if the PTP of DVT is low
- Next diagnostic step in patients with a low PTP of lower extremity DVT but a positive D-dimer
-
Procedures [23]
-
Compression ultrasound: The vein is identified and external pressure is directly applied over it with the probe.
- Proximal leg: allows for evaluation of the femoral and popliteal veins up to the trifurcation
- Whole leg: allows for evaluation of the proximal leg PLUS distal calf veins (beyond the trifurcation)
-
Venous duplex ultrasound: can be added to compression ultrasound
- Involves the addition of color Doppler
- Allows for better evaluation of noncompressible deep veins [29]
- Point-of-care ultrasound for DVT: Consider if formal ultrasound cannot be promptly obtained. [23]
-
Compression ultrasound: The vein is identified and external pressure is directly applied over it with the probe.
-
Supportive ultrasound findings of DVT [29]
- Noncompressibility of the obstructed vein
- Intraluminal hyperechoic mass
- Distention of the affected vein
-
On Doppler imaging
- Absent venous flow (complete obstruction) or abnormal venous flow (partial obstruction)
- Inadequate augmentation of venous flow on distal calf compression or Valsalva maneuver
- Of recurrent DVT: thrombosis in a new venous segment or a > 4 mm increase in noncompressibility of the obstructed vein
-
Accuracy: operator- and technique-dependent
- Whole leg study by radiology: high sensitivity and specificity (∼ 95%) for proximal DVT; lower sensitivity and specificity (∼ 65%) for distal DVT [28]
- Point of care ultrasound study (POCUS) by trained nonradiologists: equivalent accuracy for detection of proximal DVT, but distal DVT may be missed [30][31]
Compression ultrasound of the whole leg with color Doppler (i.e., duplex scanning) is the most accurate test for diagnosing DVT. [23]
If appropriately trained, consider performing a POCUS study to quickly rule in a proximal DVT. If the study is negative, further investigations (e.g., a whole leg ultrasound study by radiology) may be necessary. [30][31]

Additional evaluation
Routine laboratory studies
These are recommended to assess organ function and bleeding risk prior to anticoagulation.
- CBC
- BMP
- Liver chemistries
-
Coagulation studies
- Assess the patient's baseline coagulation status.
- Screen for subtherapeutic INR in patients on VKA therapy with suspected recurrent DVT.
Venography, CT venography, or MR venography [4][28]
-
Indications
- Inconclusive findings on compression US
- Inability to perform compression US due to, e.g., obesity, significant lower limb edema, immobilization cast
- Finding: intraluminal filling defect
Screening for an underlying cause
Patients with the following may require additional evaluation: unprovoked DVT, unexplained recurrent VTE, and/or a history suggestive of a hypercoagulable state or occult malignancy. [2]
-
Thrombophilia screening [2]
- Thrombosis in patients < 45 years
- Unusual thrombus localization
- Positive family history
- Recurrent or multiple thromboses
- Recurrent pregnancy loss
- See “Diagnostics” in “Hypercoagulable states.”
-
Screening for occult malignancy [2][32][33]
- Indications: unprovoked VTE (esp. patients > 50 years), recurrent VTE, unusual thrombus location
-
Investigations: routine age-appropriate cancer screening recommended [32][33]
- In addition to routine laboratory studies: consider e.g., urinalysis, FOBT, serum calcium levels
- Consider CXR, colonoscopy, mammogram, digital rectal examination, Pap smear
© AMBOSS
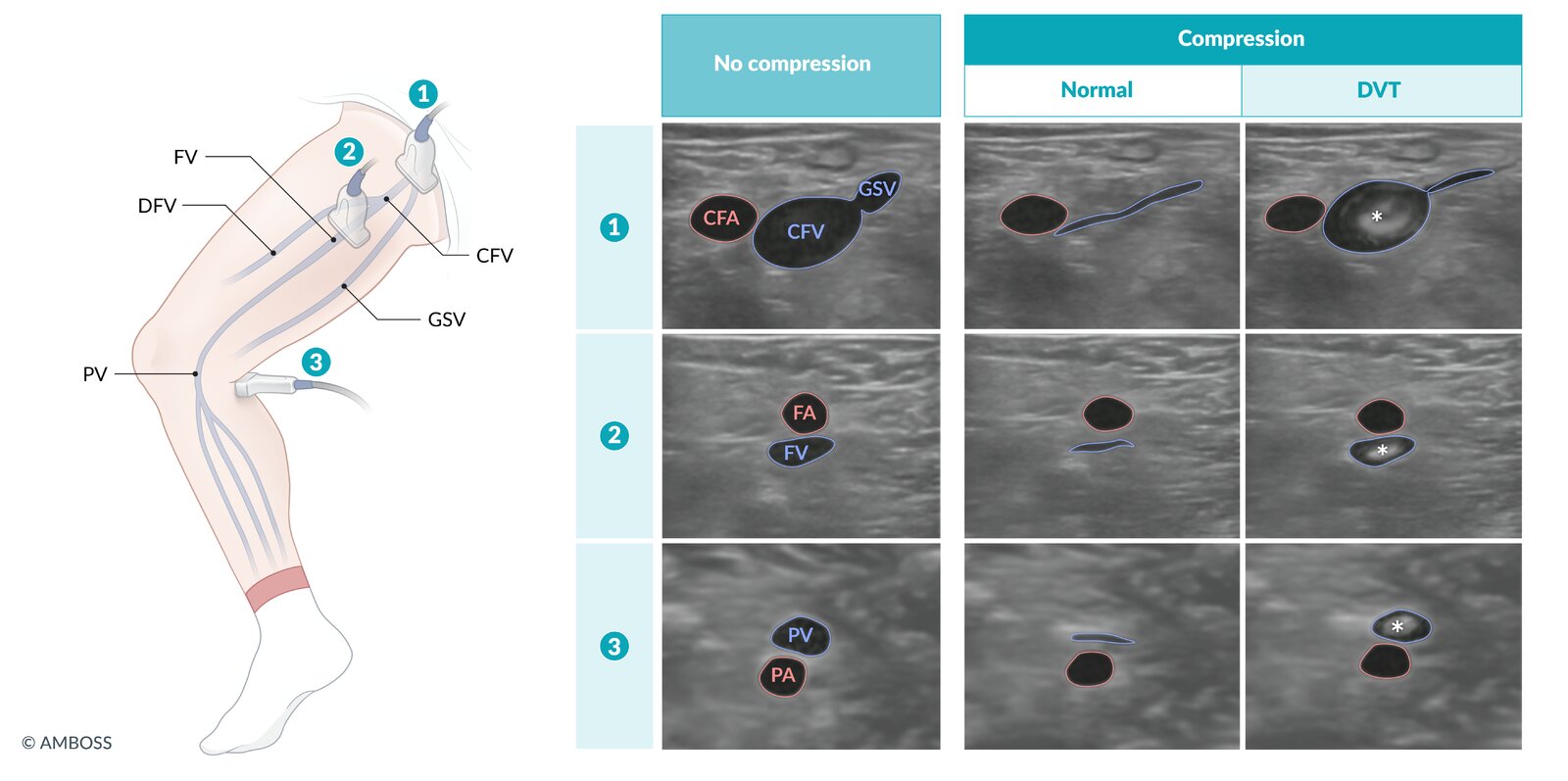
Various POCUS (point of care ultrasound) protocols exist for the detection of lower extremity DVT (deep vein thrombosis). In contrast to the whole-leg scans performed by radiology departments, POCUS protocols typically use only 2 or 3 points of compression along the femoral and popliteal veins.
– Preferred probe: linear
– Patient positioning: supine; leg rotated laterally at the hip and knee bent ∼ 30º
– Compression technique: Holding the probe perpendicular to the skin, apply enough downward pressure to slightly compress the pulsatile artery.
– Interpretation: The pressure needed to slightly compress the artery should completely collapse a non-thrombosed vein. A non-collapsible vein is highly suggestive of a DVT. Direct visualization of an intraluminal hyperechoic mass (asterisk) confirms the diagnosis.
Three-point protocol steps:
1. Locate the CFV and CFA at the branch point of the GSV from the CFV. Compress.
2. Move the transducer distally along the CFV, just past the branch point of the FV and DFV, where the FA is superficial to the FV. Compress.
3. Reposition the probe behind the knee and locate the PV superficial to the PA. Compress.
CFA: common femoral artery; CFV: common femoral vein; DFV: deep femoral vein; GSV: great saphenous vein; FA: femoral artery; FV: femoral vein; PA: popliteal artery; PV: popliteal vein
© AMBOSS
Differential diagnoses
- Superficial thrombophlebitis
- Muscle or soft tissue injury (i.e., posttraumatic swelling or hematoma)
- Lymphedema
- Venous insufficiency
- Ruptured popliteal cyst
- Cellulitis
- Compartment syndrome
In patients with suspected cellulitis AND risk factors for DVT or no response to antibiotics, consider compression ultrasound to rule out DVT. [22]
The differential diagnoses listed here are not exhaustive.
Superficial thrombophlebitis
Definition
- Inflammation and thrombosis of a superficial vein
- Variants
- Thrombophlebitis migrans (Trousseau syndrome)
- Superficial thrombophlebitis of the breast
Risk factors
- Risk factors for VTE
- Varicose veins [34]
- Venous cannulation, IV drug administration
- Behçet disease
- Thromboangiitis obliterans [35]
Risk factors for concomitant DVT [17][36]
- Age ≥ 75 years
- Past history of VTE
- Superficial thrombophlebitis affecting nonvaricose veins or veins above the knee [17][37]
- Recent immobilization, surgery, or trauma
- Pregnancy, recent childbirth, use of estrogen therapy
- Obesity, autoimmune disease, thrombophilia, CHF, or active cancer
Clinical features
- Pain, tenderness, induration, and erythema overlying a superficial vein, often with a palpable cord (the thrombosed vein)
- Most commonly affects the superficial veins of the leg
- Concomitant DVT and/or PE present in ∼ 25% of patients (see “Clinical features of DVT” and “Clinical features of PE”) [36][37][38]
Diagnostics
Superficial thrombophlebitis is typically a clinical diagnosis. The primary differential diagnoses are localized skin or soft tissue inflammation (e.g., cellulitis, vasculitis) [36][39]
-
Compression ultrasound with/without Doppler
- Indication: presence of any risk factor for concomitant DVT or if the clinical diagnosis is unclear
- Findings: thickened, edematous, noncompressible superficial vein with/without an intraluminal thrombus, with/without extension into a deep vein
- Evaluation for the underlying cause: same as that for DVT (see “Diagnostics" above)
Treatment [17][40]
All patients should be evaluated and treated for concomitant pulmonary embolism or DVT.
-
Symptomatic care: indicated for all patients [17]
- Oral and/or topical analgesics: See “Pain management.”
- Compression therapy with graduated compression stockings
-
Anticoagulation: : to consider based on thrombus length (e.g., ≥ 5 cm), location (i.e., proximity to the deep venous system), and risk factors for DVT
- Not required in the following circumstances: (i.e., provide symptomatic care only)
- Superficial thrombophlebitis caused by venous cannulation
- Thrombus length < 5 cm without risk factors for concomitant DVT
-
Prophylactic regimen (for 45 days)
- Indications
- Thrombus length ≥ 5 cm located > 3 cm away from the SFJ
- Thrombus length < 5 cm with any risk factors for concomitant DVT
-
Options
- Rivaroxaban [41]
- Fondaparinux [42]
- LMWH, such as enoxaparin : preferred in pregnant patients
- Indications
- Therapeutic regimen (for at least 3 months)
- Indication: any length thrombus located < 3 cm from the SFJ
- Options: See “Long-term anticoagulation” in “Treatment.”
- Not required in the following circumstances: (i.e., provide symptomatic care only)
Complications
- DVT
- Pulmonary embolism
- Infection (septic thrombophlebitis)
Treatment
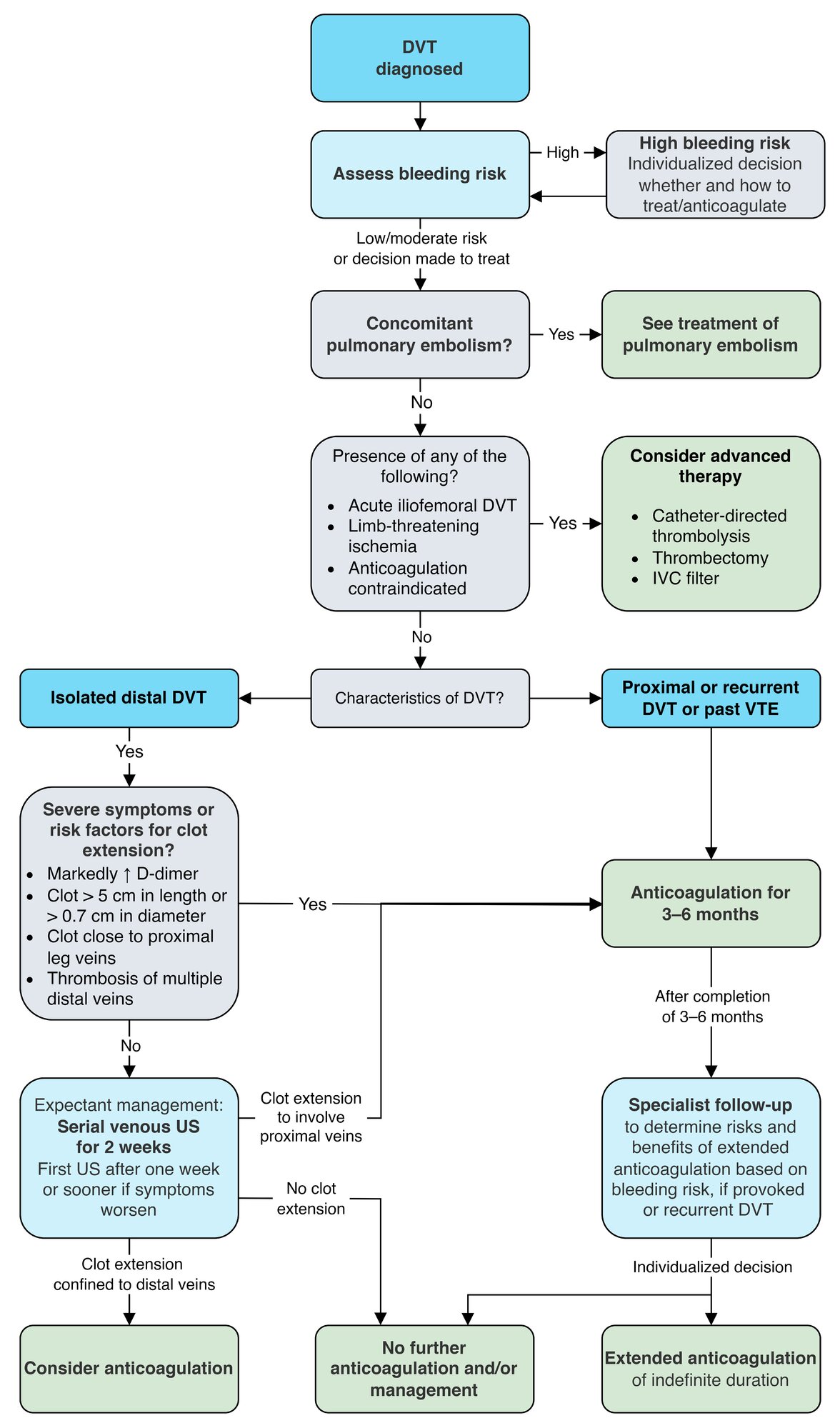
Approach [7][24]
- Evaluate and treat concomitant pulmonary embolism and stabilize the patient as needed.
- Assess bleeding risk on anticoagulation for VTE.
- Initiate anticoagulation therapy based on the extent and etiology of DVT.
- Expectant management: serial venous ultrasound without anticoagulation
- Primary treatment: anticoagulation for 3–6 months in patients not being managed expectantly
- Prevention of recurrent DVT: extended anticoagulation after completion of primary treatment; should be individualized (e.g., patients with chronic risk factors)
- Treat the underlying cause, if feasible.
Consider empirical management of pulmonary embolism in unstable or pulseless patients with obvious signs of DVT. [17][43]
Expectant management of DVT [7][23][24]
- Indication: asymptomatic or only mildly symptomatic isolated distal DVT without risk factors for clot extension
-
Relative contraindications
- Severe symptoms
-
Risk factors for clot extension in DVT
- Markedly elevated D-dimer levels
- Thrombosis > 5 cm in length and/or > 0.7 cm in diameter
- Thrombosis of multiple distal veins
- Thrombosis in close proximity to the proximal leg veins
- Past history of VTE
-
Measures
- Serial venous US for 2 weeks after symptom onset to identify clot extension
- If evidence of clot extension is:
- Absent: No further management is required.
- Confined to distal veins: Consider anticoagulation.
- Involves proximal veins: Initiate anticoagulation.
Anticoagulation for DVT [7][24][44]
Patients with acute DVT may require temporary parenteral anticoagulation initially (bridging anticoagulation) followed by long-term (typically 3–6 months) oral anticoagulation.
Initial parenteral anticoagulation
-
Indications
- Bridging anticoagulation for VKAs: Parenteral anticoagulation overlaps with oral anticoagulation until therapeutic INR is maintained.
- Parenteral lead-in therapy for dabigatran and edoxaban: These DOACs are started after completion of lead-in parenteral therapy without overlapping.
- Duration: first 5–10 days
-
Options
- Low molecular weight heparin (LMWH) (e.g., enoxaparin ); : preferred in pregnant patients and patients with normal renal function, liver disease, or active cancer [17][45][46]
- Fondaparinux (factor Xa inhibitor); : preferred in patients with a history of heparin-induced thrombocytopenia
- Unfractionated heparin (UFH) bolus plus infusion; : preferred in patients with renal failure, inadequate subcutaneous absorption (i.e., morbid obesity), and those at a high risk of bleeding [44][47]
Treatment with heparin (especially UFH) can cause heparin-induced thrombocytopenia. For early detection, perform regular CBCs.
Long-term anticoagulation for DVT
-
Indication: all patients with DVT who cannot be managed expectantly and have no contraindications to anticoagulation
- Isolated distal DVT with severe symptoms and/or risk factors for clot extension
- Any of the following in a patient with high bleeding risk:
- Proximal DVT (provoked or unprovoked)
- Recurrent DVT (provoked or unprovoked)
- DVT provoked by a transient risk factor
- Duration: : 3–6 months
-
Direct oral anticoagulants (DOACs): first-line therapy in nonpregnant patients, including patients with active cancer (preferred over VKAs) [46][48][49]
- Regular monitoring of coagulation parameters is not required.
- Associated with a lower risk of major bleeding
- Options (any of the following)
- Direct factor Xa inhibitors: rivaroxaban , apixaban , or edoxaban
- Direct thrombin inhibitors: dabigatran
- Dabigatran and edoxaban require parenteral lead-in therapy while rivaroxaban and apixaban can be started immediately. [48]
-
Vitamin K antagonists (VKAs): warfarin
-
Bridging anticoagulation is required.
- Initiate simultaneously with initial parenteral anticoagulation.
- Continue parenteral anticoagulation with warfarin for at least 5 days and until therapeutic INR has been maintained for 48 hours. [49][50]
- Second-line therapy in nonpregnant patients, including patients with active cancer [46]
- Requires dose adjustment to maintain a target INR of 2–3
-
Bridging anticoagulation is required.
- LMWH: : preferred in pregnant individuals; , e.g., enoxaparin [46][48]
Initial parenteral anticoagulation (with LMWH, fondaparinux, or UFH) should be initiated at the same time as warfarin and before dabigatran and edoxaban. Initial parenteral anticoagulation is not required for patients receiving rivaroxaban or apixaban. [7][24]
Extended anticoagulation for DVT [7][24][44]
The decision to extend anticoagulation indefinitely after primary treatment is typically made after balancing the risk of recurrent DVT (e.g., for patients with chronic risk factors) with the bleeding risk on anticoagulation for VTE.
-
Indications
- Any of the following in a patient with low or moderate bleeding risk:
- Unprovoked proximal DVT
- Unprovoked recurrent DVT
- DVT provoked by chronic risk factors (e.g., active cancer with additional risk factors, thrombophilia)
- Any of the following in a patient with low or moderate bleeding risk:
- Duration: indefinite
-
Options [24]
- First episode of DVT: Continue the same anticoagulant used for long-term anticoagulation (e.g., warfarin, or DOACs).
-
Recurrent DVT while appropriately anticoagulated
- On an oral anticoagulant: Switch to LMWH; either temporarily or for the remaining duration of therapy (e.g., enoxaparin ).
- On LMWH: Increase LMWH dose by 25–33%.
- Patients wishing to discontinue anticoagulation : Consider aspirin (unless there are contraindications).
- Monitoring: Reassess bleeding risk periodically (e.g., annually).
Extended anticoagulation is usually not required in patients with a provoked DVT due to a transient or reversible risk factor (e.g., surgery, intravascular catheter). [24][44]
Anticoagulation for DVT in active cancer [46]
-
Approach to management
- Initiate LMWH (e.g., enoxaparin), UFH, fondaparinux, rivaroxaban, or apixaban.
-
Continue anticoagulation for at least 6 months.
- First line: LMWH (e.g., enoxaparin), edoxaban, rivaroxaban, or apixaban (preferred over VKAs) [46]
- Alternative : VKAs, e.g., warfarin (bridging anticoagulation required)
- Consider indefinite anticoagulation for patients with active metastatic cancer and/or receiving chemotherapy. [46]
- For dosages, see “Anticoagulation.”
-
Additional considerations
- No alterations are required for patients with primary or metastatic CNS malignancy. [46]
- Incidental PE or DVT should be treated in the same way as symptomatic VTE. [46]
Patients with active cancer and VTE should receive anticoagulation for at least 6 months. [46]
Advanced therapy for DVT
These interventions are not routinely indicated. Consider in patients with acute iliofemoral DVT, limb-threatening ischemia, or DVT and contraindications to anticoagulation.
-
Catheter-directed thrombolysis (CDT) [7][24]
- Indications
- Limb-threatening ischemia (phlegmasia cerulea dolens)
- Consider in acute (< 14 days) iliofemoral DVT in patients with low risk of bleeding and life expectancy ≥ 1 year [24][51]
- Agents: streptokinase, urokinase, rtPA [51]
- Indications
-
Thrombectomy
- Indications: same as for CDT; consider as an alternative to CDT in patients with absolute contraindications to thrombolysis [51]
-
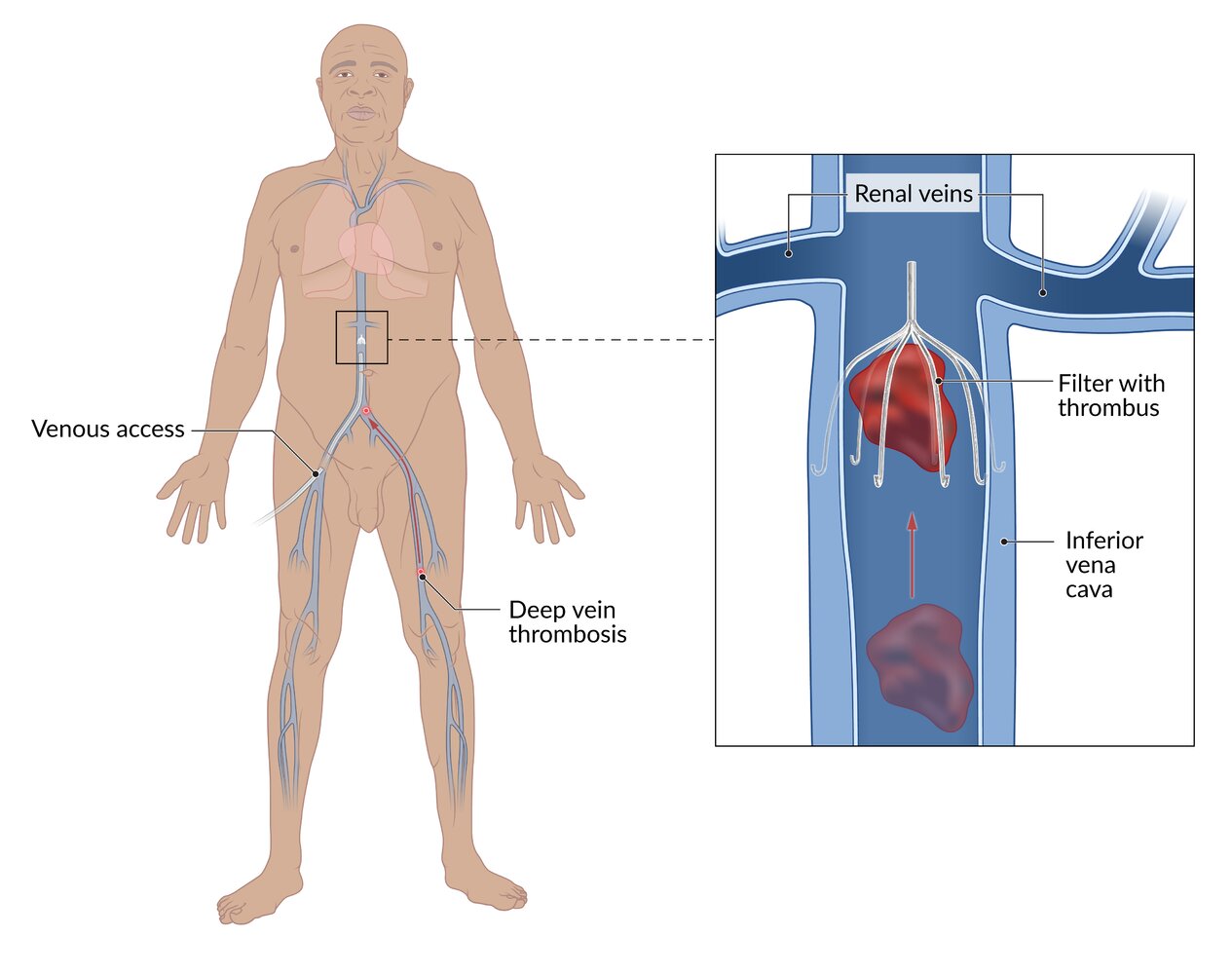
Inferior vena cava filter (Greenfield filter)
- Indications [24][46][52]
- DVT with a high risk of PE (e.g., proximal DVT) in patients with contraindications for anticoagulation, absolute contraindications to thrombolysis, and contraindications to thrombectomy (e.g., patients with active bleeding, recent major surgery, recent intracranial hemorrhage) [53]
- Consider in anticoagulated patients with severe PE to prevent subsequent PE. [24][52]
- Indications [24][46][52]

Supportive care [24]
- Encourage early ambulation; minimize bed rest. [54][55][56]
-
Graduated compression stockings
- Consider only for symptomatic relief (i.e., reduction of edema and pain)
- No longer routinely recommended to prevent postthrombotic syndrome. [24][44]
- Analgesics for pain relief: See “ Pain management ”; avoid NSAIDs if the patient is receiving anticoagulation or thrombolytics. [57]
- Delay any elective surgery for at least 3 months after initiation of anticoagulation therapy. [44]
Disposition [7][24][44]
- Outpatient therapy is preferred for patients with uncomplicated DVT. [58]
- Educate the patient regarding prescribed anticoagulation and the recognition of warning signs.
- Ensure outpatient follow-up within 1–2 weeks.
- Hospital admission during the acute phase is recommended for patients with:
- Suspected limb ischemia
- High bleeding risk
- Inability or unwillingness to self-administer parenteral anticoagulant therapy
- Significant comorbidities
- Limited social supports
- Pain requiring IV analgesia
Prior to discharge, educate patients regarding prescribed anticoagulation and advise them to immediately seek medical attention if they develop worsening pain or swelling, shortness of breath, chest pain, or signs of bleeding.
© AMBOSS
© AMBOSS
Estimation of bleeding risk with anticoagulation
Risk factors for bleeding in patients with VTE [24]
-
Patient characteristics
- Age > 65 years
- Decreased functional capacity and comorbidity
- Frequent falls
-
Past medical history
- Prior history of bleeding
- Prior history of stroke
- Recent surgery
-
Chronic conditions
- Cancer
- Renal failure
- Liver failure
- Diabetes
- Alcohol use disorder
-
Medication history
- Poor anticoagulant control
- Antiplatelet therapy
- NSAID use
-
Laboratory abnormalities
- Low platelets
- Anemia
Risk assessment
| Risk of major bleeding on anticoagulant therapy in patients with VTE [24] | ||
|---|---|---|
| Risk category | First 3 months of therapy | After 3 months of therapy |
| Low (No risk factors) | 1.6% | 0.8%/year |
| Moderate (1 risk factor) | 3.2% | 1.6%/year |
| High (≥ 2 risk factors) | 12.8% | ≥ 6.5%/year |
Complications
- Pulmonary embolism: Pulmonary emboli most commonly originate in the proximal deep veins of the lower extremities (e.g., iliac, femoral, or popliteal veins).
- Postthrombotic syndrome (chronic venous insufficiency)
- Septic thrombophlebitis: may occur in patients with a history of IV drug use using nonsterile needles
-
Venous gangrene (rare complication) [59]
- The development of ischemic necrosis of a distal extremity despite palpable or doppler pulses, occurring as a complication of deep vein thrombosis
- Often associated with the use of warfarin in patients with acquired hypercoagulability (e.g., in malignancy, heparin-induced thrombocytopenia, antiphospholipid syndrome).


We list the most important complications. The selection is not exhaustive.
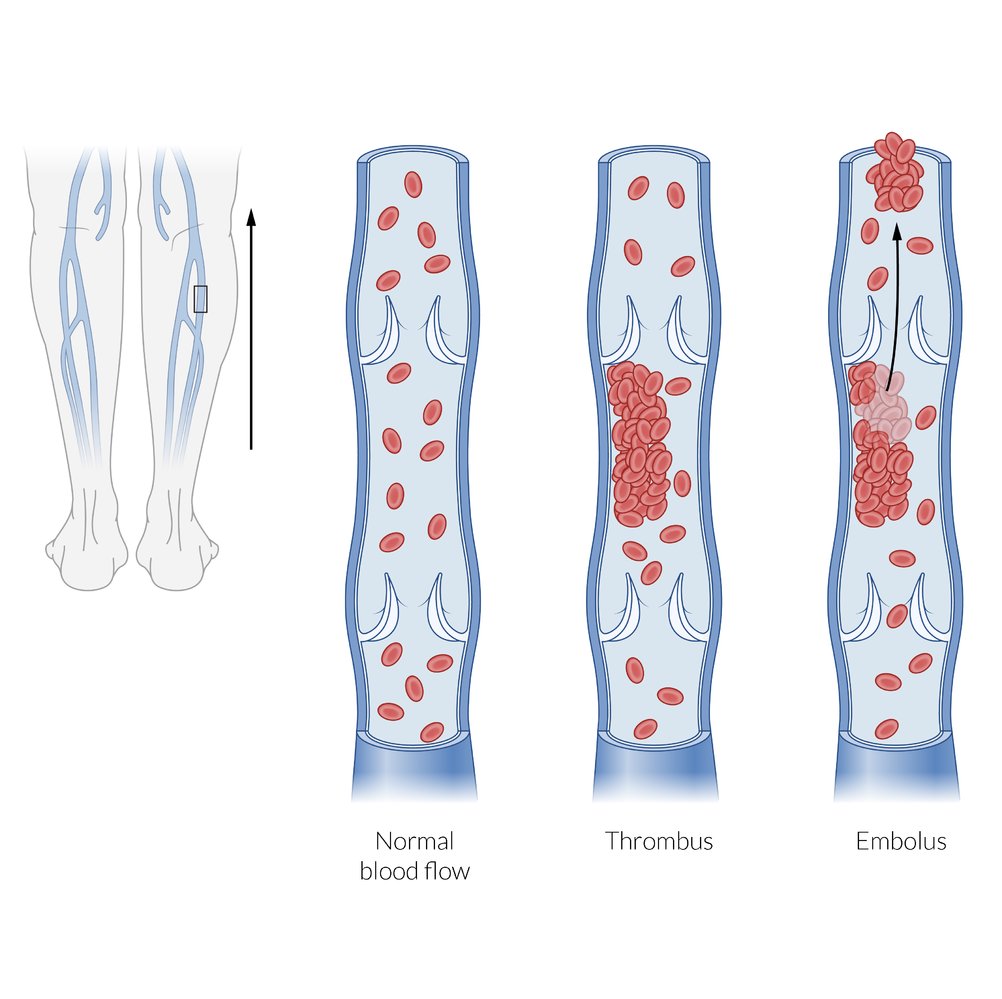
Deep vein thrombosis typically occurs in the deep veins of the lower extremity, most commonly the calf veins. Pulmonary embolism occurs when a thrombus is dislodged and carried to the lungs by the venous blood flow returning to the heart.
© AMBOSS
© AMBOSS
Click on the overlay icon below the taskbar on the left to toggle the overlay on and off.
CT chest (with contrast; axial plane, lung window; axial plane, mediastinal window; coronal plane, mediastinal window) of a patient with shortness of breath, post-circulatory collapse, elevated D-dimer (5,086 ug/L; normal < 5), and normal C-reactive protein (CRP; < 3.0 mg/L)
Multiple intraluminal filling defects in the right and left pulmonary arteries and their lobar, segmental, and subsegmental branches represent pulmonary emboli of different age. The acute emboli are seen as central filling defects, whereas the older emboli are eccentric and show irregular thickening of the arterial wall.
Right ventricular and atrial enlargement, septal flattening, and contrast reflux into the hepatic veins are evidence of right ventricular strain. The causes of ground glass opacification in the left upper lobe and misty mesentery with nodes in the upper abdomen are not readily evident. Incidental findings include a hypodense cyst within a small, irregular left kidney and slight deformity of the right sixth rib from a previous fracture.
Our great thanks to Nándor Faluhelyi (University of Pécs, Medical School) for kindly providing this image.
Prevention
VTE prophylaxis
VTE prophylaxis should be chosen based on the presence of risk factors for VTE and estimated risk of bleeding on anticoagulation therapy. [60]
-
General preventive measures
- Regular exercise
- Early postoperative mobilization
- Physiotherapy
- Avoid certain medications (e.g., OCPs) in patients with thrombophilias (e.g., factor V Leiden).
- Pharmacological VTE prophylaxis: (antithrombotics): LMWH, low-dose UFH, and DOACs are recommended.
-
Mechanical VTE prophylaxis
- Graduated compression stockings: preferred in long-distance travelers
-
Intermittent pneumatic compression device
- Preferred in seriously ill medical patients and in surgical patients
- Alternating inflation and deflation of the compression device improve venous return by simulating the calf pump mechanism.
-
Duration of prophylaxis in hospitalized patients [60]
- Mechanical VTE prophylaxis: until the patient is mobile
-
Pharmacological VTE prophylaxis
- Seriously ill medical patients: at least 7 days; extend to span the duration of hospitalization
- Surgical patients: consider extended therapy for > 3 weeks [61]
| Approach to VTE prophylaxis [60][61][62] | ||
|---|---|---|
| Indications | Choice of prophylaxis [63][64] | |
| Low-risk patients |
|
|
| At-risk outpatients |
|
|
| Medical inpatients |
|
|
|
|
|
| Surgical patients |
|
|
|
|
|
|
|
|
|
|
|
Prophylaxis is usually indicated in seriously ill patients who are hospitalized, patients undergoing major surgery, patients with major trauma, and long-distance travelers with additional risk factors for VTE.
In surgical patients, the first dose of the antithrombotic should be administered within 12 hours of completing the surgery. [61]
LMWH or low-dose UFH is recommended for postoperative anticoagulation in patients who have undergone major surgery.
VTE prophylaxis in active cancer [46]
The preferred agent for VTE prophylaxis depends on the patient's setting and risk factors. Always assess bleeding risk.
Outpatients [46]
- Patients receiving selected cancer therapy (e.g., hormonal therapy, thalidomide, or lenalidomide) and those with a high risk of thrombosis who are starting systemic cancer therapy [46]
- LMWH, e.g., enoxaparin
- Apixaban (off-label) OR rivaroxaban [69][70]
- Patients traveling for > 4 hours: See “Approach to VTE prophylaxis.” [60]
Pharmacological VTE prophylaxis is not routinely recommended for outpatients with cancer or those admitted for minor procedures, chemotherapy, or stem cell or bone marrow transplantation unless other risk factors are present.
Hospitalized patients [46]
- Medical patients (i.e., patients with an acute medical illness or reduced mobility) [46]
- First line: LMWH, e.g., enoxaparin
- Alternative: low-dose UFH
- Surgical patients
- Begin VTE prophylaxis preoperatively with UFH or LMWH (unless contraindicated).
- Continue for at least 7–10 days after major cancer surgery. [46]
Special patient groups
The approach to suspected DVT differs in children and in pregnant and postpartum individuals.
DVT in pregnancy and postpartum
Overview [71][72]
- Individuals are at increased risk of VTE during pregnancy and the postpartum period. [71]
- Highest risk: postpartum, particularly in the first week
- During pregnancy: Risk is highest in the third trimester.
- Common risk factors for VTE in pregnancy include:
- Previous history of DVT (most significant risk factor)
- Cesarean delivery [71]
- DVT is more commonly proximal in pregnant than nonpregnant individuals.
Diagnostics of DVT in pregnancy and postpartum [71]
Modifications to the standard diagnostic approach to DVT are as follows:
-
Initial evaluation [71]
- Use clinical suspicion to determine whether imaging is required.
- Avoid using the Wells score, as it is not validated in pregnancy or the postpartum period. [4][73]
- Initial imaging: lower extremity venous ultrasound [71]
-
Further studies: required when compression ultrasound is negative or equivocal [71][71]
- When iliac vein thrombosis is suspected, obtain one of the following:
- Doppler ultrasound, including the iliac vein, if not already performed
- Venography
- MRI
- When iliac vein thrombosis is not suspected, repeat lower extremity venous ultrasound on days 3 and 7. [71]
- When further imaging is not available, consider empiric management.
- When iliac vein thrombosis is suspected, obtain one of the following:
Calf swelling of > 2 cm compared to the contralateral leg suggests DVT in pregnant individuals. [71]
D-dimer is unreliable in pregnancy and is generally not indicated. [71]
Management of DVT in pregnancy and postpartum [71][74]
Modifications to the standard treatment of DVT are as follows:
-
Indications for inpatient management [71]
- Significant comorbidities
- Large clots
-
Diagnosed during pregnancy
- Start LMWH.
- For management of anticoagulation during delivery, consult obstetrics, anesthesia, and hematology.
- Continue anticoagulation for at least 6 weeks postpartum, and 3–6 months in total. [71]
- If anticoagulation is used for > 6 weeks postpartum, consider changing to:
- Warfarin [71]
- A DOAC if not breastfeeding [71]
-
Diagnosed during the postpartum period
- Follow standard treatment of DVT.
- Avoid DOACs in individuals who are breastfeeding.
Avoid warfarin and DOACs in pregnancy. [71]
Prevention of DVT in pregnancy and postpartum
- Assess all patients, at least once, for risk factors for VTE, including: [71][72]
- Known thrombophilia or history of venous thromboembolism
- Multiple pregnancy
- Hypertensive pregnancy disorders
- Heart disease
- Obesity
- Hyperemesis gravidarum
- Ovarian hyperstimulation syndrome (first trimester only)
- Cesarean delivery
- Consider prophylactic anticoagulation with LMWH based on risk factors and shared decision-making. [72]
DVT in children
DVT in children is rare, with an estimated incidence of 10–14 per 10,000 hospitalized children annually. [75][76][77]
Risk factors for pediatric VTE [75][76]
- Central venous catheters (most common cause) [75][76]
- Malignancy
- Congenital heart disease
- Active infection
- Oral contraceptives
- Obesity
- Hereditary thrombophilia
- Congenital anomalies (e.g., IVC atresia or occlusion)
- See also “Risk factors for VTE.”
Unprovoked VTE is rare in otherwise healthy children. [75]
Clinical features [76][77]
- Extremity DVTs commonly manifest with swelling, pain, and/or erythema.
- Catheter-related DVTs may manifest with catheter malfunction.
- Infants may present with signs of thrombocytopenia. [78]
- See also “Clinical features of DVT.”
Clinical features of DVT are often less pronounced in children than in adults. [76]
Diagnosis [76][78]
-
Venous imaging: recommended in all children with suspected DVT
- Duplex compression ultrasound
- Usually preferred as initial imaging modality [76][78]
- See “Supportive ultrasound findings of DVT.”
-
MR or CT venography [77]
- May be preferred for evaluation of central or abdominal veins
- Second-line modality if ultrasound findings are negative or equivocal despite high clinical suspicion
- Venography: rarely performed
- Duplex compression ultrasound
-
Evaluation for an underlying cause
- Thrombophilia testing: indicated if there is no apparent cause for DVT [75]
- Further workup (e.g., for congenital anomalies): consider if thrombophilia testing is negative [76]
D-dimer has limited specificity in children with VTE and should not be used as a standalone diagnostic test. [76][77][79]
Management [75]
Manage pediatric DVT in consultation with pediatric hematology. [75]
- All patients: Evaluate for clinical features of pulmonary embolism. [80]
-
Symptomatic DVT
- Start anticoagulation for pediatric VTE in all patients without contraindications to anticoagulation.
- Advanced therapy for DVT may be considered in select patients. [75][78]
- Catheter-related DVT: Remove catheter if nonfunctional or no longer needed. [75][76]
- Clinically unsuspected (asymptomatic) DVT: Expectant management or anticoagulation for pediatric VTE may be appropriate. [75]
Anticoagulation for pediatric VTE [75]
Initial parenteral anticoagulation
- Indications: all patients without contraindications to anticoagulation
- Agents: LMWH, UFH, or fondaparinux
-
Duration: varies depending on long-term anticoagulation plan
- ≥ 5 days prior to initiation of DOACs [75]
- Until therapeutic INR is reached in patients starting VKAs (i.e., bridging anticoagulation)
- May be continued as long-term anticoagulation
Long-term anticoagulation
-
Agents
- Preferred: DOACs (e.g., rivaroxaban, dabigatran) [75]
- Alternatives: VKAs, LMWH, fondaparinux, UFH
-
Duration
-
Provoked VTE: 3 months
- Longer duration if there are ongoing risk factors for VTE [75]
- Shorter duration (6 weeks) may be considered in select patients.
- Unprovoked VTE: 6–12 months [75]
-
Provoked VTE: 3 months
Related One-Minute Telegram
- One-Minute Telegram 140-2026-3/3: Revisiting D-dimers in old-timers
- One-Minute Telegram 83-2023-1/3: Hormonal contraception and NSAIDs: a risky tango
- One-Minute Telegram 77-2023-2/3: DOACs safe and effective in cancer-associated VTE
- One-Minute Telegram 68-2023-1/3: After orthopedic trauma, two aspirin a day keep fatal blood clots away
Interested in the newest medical research, distilled down to just one minute? Sign up for the One-Minute Telegram in “Tips and links” below.
External Resources
- Sign up for the One-Minute Telegram
- 2024 ASH/International Society on Thrombosis and Haemostasis Guidelines for Treatment of Venous Thromboembolism in Pediatric Patients
- 2023 ASCO Guideline for VTE Prophylaxis and Treatment in Patients With Cancer
- 2020 ASH Guidelines for Management of Venous Thromboembolism: Treatment of Deep Vein Thrombosis and Pulmonary Embolism
- 2019 ASH Guidelines for Management of Venous Thromboembolism: Prevention of Venous Thromboembolism in Surgical Hospitalized Patients
- 2018 ASH Guidelines for Management of Venous Thromboembolism: Prophylaxis for Hospitalized and Nonhospitalized Medical Patients
- 2018 ASH Guidelines for Management of Venous Thromboembolism: Diagnosis of Venous Thromboembolism
- 2018 ACOG Practice Bulletin No. 196: Thromboembolism in Pregnancy
- 2016 CHEST Guideline for Antithrombotic Therapy for VTE Disease
- 2012 CHEST Guideline for Antithrombotic Therapy for VTE Disease
References
- Piazza G, Goldhaber SZ. "Acute pulmonary embolism: part I: epidemiology and diagnosis.". Circulation. 114(2). :e28-32. (2006)
- Ortel TL, Neumann I, Ageno W, et al. "American Society of Hematology 2020 guidelines for management of venous thromboembolism: treatment of deep vein thrombosis and pulmonary embolism". Blood Advances. 4(19). :4693-4738. (2020)
- Jaffray J, Bauman M, Massicotte P. "The Impact of Central Venous Catheters on Pediatric Venous Thromboembolism". Frontiers in Pediatrics. 5. (2017)
- Prandoni P, Lensing AW, Cogo A, et al. "The long-term clinical course of acute deep venous thrombosis.". Ann Intern Med. 125(1). :1-7. (1996)
- Al-Azzawi HF, Obi OC, Safi J, Song M. "Nephrotic syndrome-induced thromboembolism in adults.". International journal of critical illness and injury science. 6(2). :85-8
- ENGBERS MJ, VAN HYLCKAMA VLIEG A, ROSENDAAL FR. "Venous thrombosis in the elderly: incidence, risk factors and risk groups". J Thromb Haemost. 8(10). :2105-2112. (2010)
- "Iliofemoral Deep Vein Thrombosis". http://www.acc.org/latest-in-cardiology/articles/2015/11/23/13/39/iliofemoral-deep-vein-thrombosis. [2015-10-24]
- Branchford BR, Carpenter SL. "The Role of Inflammation in Venous Thromboembolism". Frontiers in Pediatrics. 6. (2018)
- Khan O, Marmaro A, Cohen DA. "A review of upper extremity deep vein thrombosis". Postgrad Med. 133(sup1). :3-10. (2021)
- Lim W et al. "American Society of Hematology 2018 guidelines for management of venous thromboembolism: diagnosis of venous thromboembolism". Blood Adv. 2(22). :3226-3256. (2018)
- Engelberger RP, Kucher N. "Management of Deep Vein Thrombosis of the Upper Extremity". Circulation. 126(6). :768-773. (2012)
- Kearon C, Akl EA, Comerota AJ, et al. "Antithrombotic therapy for VTE disease: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines.". Chest. 141(2 Suppl). :e419S-e496S. (2012)
- Mazzolai L, Aboyans V, Ageno W, et al. "Diagnosis and management of acute deep vein thrombosis: a joint consensus document from the European Society of Cardiology working groups of aorta and peripheral vascular diseases and pulmonary circulation and right ventricular function". Eur Heart J. 39(47). :4208-4218. (2017)
- Bates SM, Jaeschke R, Stevens SM, et al. "Diagnosis of DVT". Chest. 141(2). :e351S-e418S. (2012)
- Needleman L, Cronan JJ, Lilly MP, et al. "Ultrasound for Lower Extremity Deep Venous Thrombosis". Circulation. 137(14). :1505-1515. (2018)
- Kearon C, Akl EA, Ornelas J, et al. "Antithrombotic Therapy for VTE Disease". Chest. 149(2). :315-352. (2016)
- Cho HJ, Dunn AS. "The Value of Using Ultrasound to Rule Out Deep Vein Thrombosis in Cases of Cellulitis". Journal of Hospital Medicine. 12(4). :259-261. (2017)
- Patel H, Sun H, Hussain AN, Vakde T. "Advances in the Diagnosis of Venous Thromboembolism: A Literature Review". Diagnostics. 10(6). :365. (2020)
- Schouten HJ, Koek HL, Oudega R, et al. "Validation of two age dependent D-dimer cut-off values for exclusion of deep vein thrombosis in suspected elderly patients in primary care: retrospective, cross sectional, diagnostic analysis". BMJ. 344(jun06 1). :e2985-e2985. (2012)
- Schouten HJ, Geersing GJ, Koek HL, et al. "Diagnostic accuracy of conventional or age adjusted D-dimer cut-off values in older patients with suspected venous thromboembolism: systematic review and meta-analysis". BMJ. 346. :f2492-f2492. (2013)
- Ho VB et al. "ACR Appropriateness Criteria® on Suspected Lower Extremity Deep Vein Thrombosis". J Am Coll Radiol. 8(6). :383-387. (2011)
- Desjardins B, Hanley M, Steigner ML, et al. "ACR Appropriateness Criteria® Suspected Upper Extremity Deep Vein Thrombosis". Journal of the American College of Radiology. 17(5). :S315-S322. (2020)
- Canty D, Mufti K, Bridgford L, Denault A. "Point‐of‐care ultrasound for deep venous thrombosis of the lower limb". Australasian Journal of Ultrasound in Medicine. 23(2). :111-120. (2019)
- American College of Emergency Physicians. "Emergency ultrasound imaging criteria compendium". Ann Emerg Med. 48(4). :487-510. (2006)
- Parakh RS, Sabath DE. "Venous Thromboembolism: Role of the Clinical Laboratory in Diagnosis and Management.". The journal of applied laboratory medicine. 3(5). :870-882. (2019)
- Van Es N, Le Gal G, Otten H-M, et al. "Screening for Occult Cancer in Patients With Unprovoked Venous Thromboembolism". Ann Intern Med. 167(6). :410. (2017)
- Carrier M, Lazo-Langner A, Shivakumar S, et al. "Screening for Occult Cancer in Unprovoked Venous Thromboembolism". N Engl J Med. 373(8). :697-704. (2015)
- Sharifi M, Berger J, Beeston P, et al. "Pulseless electrical activity in pulmonary embolism treated with thrombolysis (from the “PEAPETT” study)". Am J Emerg Med. 34(10). :1963-1967. (2016)
- Wilbur J, Shian B. "Deep Venous Thrombosis and Pulmonary Embolism: Current Therapy.". Am Fam Physician. 95(5). :295-302. (2017)
- Konstantinides SV, Barco S, Lankeit M, Meyer G. "Management of Pulmonary Embolism". J Am Coll Cardiol. 67(8). :976-990. (2016)
- Key NS, Khorana AA, Kuderer NM, et al. "Venous Thromboembolism Prophylaxis and Treatment in Patients With Cancer: ASCO Guideline Update". J Clin Oncol. 41(16). :3063-3071. (2023)
- Smythe MA, Priziola J, Dobesh PP, et al. "Guidance for the practical management of the heparin anticoagulants in the treatment of venous thromboembolism.". J Thromb Thrombolysis. 41(1). :165-86. (2016)
- van Es N, Coppens M, Schulman S, Middeldorp S, Büller HR. "Direct oral anticoagulants compared with vitamin K antagonists for acute venous thromboembolism: evidence from phase 3 trials.". Blood. 124(12). :1968-75. (2014)
- Gómez-Outes A, Terleira-Fernández AI, Lecumberri R, Suárez-Gea ML, Vargas-Castrillón E. "Direct oral anticoagulants in the treatment of acute venous thromboembolism: A systematic review and meta-analysis". Thromb Res. 134(4). :774-782. (2014)
- Wigle P, Hein B, Bloomfield HE, Tubb M, Doherty M. "Updated guidelines on outpatient anticoagulation.". Am Fam Physician. 87(8). :556-66. (2013)
- Casey ET et al. "Treatment of acute iliofemoral deep vein thrombosis". J Vasc Surg. 55(5). :1463-1473. (2012)
- Bikdeli B et al. "Inferior Vena Cava Filters to Prevent Pulmonary Embolism". J Am Coll Cardiol. 70(13). :1587-1597. (2017)
- White RH, Brunson A, Romano PS, Li Z, Wun T. "Outcomes After Vena Cava Filter Use in Noncancer Patients With Acute Venous Thromboembolism: A Population-Based Study.". Circulation. 133(21). :2018-29. (2016)
- Liu Z et al. "Bed Rest versus Early Ambulation with Standard Anticoagulation in The Management of Deep Vein Thrombosis: A Meta-Analysis". PLoS ONE. 10(4). :e0121388. (2015)
- Meune C, Aissaoui N, et al. "Is bed rest recommendation in the management of patients with pulmonary embolism and/or deep vein thrombosis evidence-based medicine: A meta-analysis". Circulation. (2018)
- Aissaoui N, Martins E, Mouly S, Weber S, Meune C. "A meta-analysis of bed rest versus early ambulation in the management of pulmonary embolism, deep vein thrombosis, or both.". Int J Cardiol. 137(1). :37-41. (2009)
- Risser A, Donovan D, Heintzman J, Page T. "NSAID prescribing precautions.". Am Fam Physician. 80(12). :1371-8. (2009)
- Barrett TW, Wrenn KD, Slovis CM, et al. "An Outpatient Management Protocol for Emergency Department Patients With a Newly Diagnosed Lower Extremity Deep Venous Thrombosis". Critical Pathways in Cardiology: A Journal of Evidence-Based Medicine. 15(3). :75-76. (2016)
- Musani MH, Musani MA, Verardi MA. "Venous Gangrene a Rare but Dreadful Complication of Deep Venous Thrombosis". Clinical and Applied Thrombosis/Hemostasis. 17(6). :E1-E3. (2010)
- Schünemann HJ, Cushman M, Burnett AE, et al. "American Society of Hematology 2018 guidelines for management of venous thromboembolism: prophylaxis for hospitalized and nonhospitalized medical patients". Blood Advances. 2(22). :3198-3225. (2018)
- Anderson DR et al. "American Society of Hematology 2019 guidelines for management of venous thromboembolism: prevention of venous thromboembolism in surgical hospitalized patients". Blood Adv. 3(23). :3898-3944. (2019)
- Kahn SR, Lim W, Dunn AS, et al. "Prevention of VTE in Nonsurgical Patients". Chest. 141(2). :e195S-e226S. (2012)
- Laryea J, Champagne B. "Venous thromboembolism prophylaxis.". Clinics in colon and rectal surgery. 26(3). :153-9. (2013)
- Chen A, Stecker E, A. Warden B. "Direct Oral Anticoagulant Use: A Practical Guide to Common Clinical Challenges". Journal of the American Heart Association. 9(13). (2020)
- Cesarone MR, Belcaro G, Nicolaides AN, et al. "Venous thrombosis from air travel: the LONFLIT3 study--prevention with aspirin vs low-molecular-weight heparin (LMWH) in high-risk subjects: a randomized trial.". Angiology. 53(1). :1-6
- William H. Geerts, Graham F. Pineo, John A. Heit, et al. "Prevention of Venous Thromboembolism". Chest. 126(3). :338S-400S. (2004)
- Powers WJ, Rabinstein AA, Ackerson T, et al. "Guidelines for the Early Management of Patients With Acute Ischemic Stroke: 2019 Update to the 2018 Guidelines for the Early Management of Acute Ischemic Stroke: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association". Stroke. 50(12). (2019)
- Mandernach MW, Beyth RJ, Rajasekhar A. "Apixaban for the prophylaxis and treatment of deep vein thrombosis and pulmonary embolism: an evidence-based review.". Therapeutics and clinical risk management. 11. :1273-82. (2015)
- Carrier M, Abou-Nassar K, Mallick R, et al. "Apixaban to Prevent Venous Thromboembolism in Patients with Cancer". N Engl J Med. 380(8). :711-719. (2019)
- Khorana AA, Soff GA, Kakkar AK, et al. "Rivaroxaban for Thromboprophylaxis in High-Risk Ambulatory Patients with Cancer". N Engl J Med. 380(8). :720-728. (2019)
- Kirkilesis G, Kakkos SK, Bicknell C, Salim S, Kakavia K. "Treatment of distal deep vein thrombosis". Cochrane Database of Systematic Reviews. (2020)
- Galioto NJ, Danley DL, Van Maanen RJ. "Recurrent venous thromboembolism.". Am Fam Physician. 83(3). :293-300. (2011)
- Ageno W, Squizzato A, Wells PS, Büller HR, Johnson G. "The diagnosis of symptomatic recurrent pulmonary embolism and deep vein thrombosis: guidance from the SSC of the ISTH". Journal of Thrombosis and Haemostasis. 11(8). :1597-1602. (2013)
- Monagle P, Azzam M, Bercovitz R, et al. "American Society of Hematology/International Society on Thrombosis and Haemostasis 2024 updated guidelines for treatment of venous thromboembolism in pediatric patients". Blood Adv. 9(10). :2587-2636. (2025)
- Audu CO, Wakefield TW, Coleman DM. "Pediatric deep venous thrombosis". J Vasc Surg Venous Lymphat Disord. 7(3). :452-462. (2019)
- Jaffray J, Young G. "Deep vein thrombosis in pediatric patients". Pediatr Blood Cancer. 65(3). (2017)
- Bittles M, Colombani P, Goldenberg N, Betensky M. "How We Manage Pediatric Deep Venous Thrombosis". Semin Intervent Radiol. 34(01). :35-49. (2017)
- Avila L, Amiri N, Pullenayegum E, et al. "Diagnostic value of D‐dimers for limb deep vein thrombosis in children: A prospective study". Am J Hematol. 96(8). :954-960. (2021)
- Ross C, Kumar R, Pelland-Marcotte MC, et al. "Acute Management of High-Risk and Intermediate-Risk Pulmonary Embolism in Children: A Review". Chest. 161(3). :791-802. (2022)
- Wells PS, Hirsh J, Anderson DR, et al. "Accuracy of clinical assessment of deep-vein thrombosis.". Lancet (London, England). 345(8961). :1326-30. (1995)
- Wells PS, Anderson DR, Rodger M, et al. "Evaluation of D-dimer in the diagnosis of suspected deep-vein thrombosis". N Engl J Med. 349(13). :1227-1235. (2003)
- Engelberger RP et al. "Comparison of the diagnostic performance of the original and modified Wells score in inpatients and outpatients with suspected deep vein thrombosis". Thromb Res. 127(6). :535-539. (2011)
- Di Nisio et al. "Treatment for superficial thrombophlebitis of the leg". Cochrane Database Syst Rev. (2004)
- Perttu ET Arkkila. "Thromboangiitis obliterans (Buerger's disease)". Orphanet J Rare Dis. 1(1). (2006)
- Quéré I et al. "Superficial venous thrombosis and compression ultrasound imaging". J Vasc Surg. 56(4). :1032-1038.e1. (2012)
- Konkle BA. "Superficial venous thrombosis: cause for concern". Blood. 122(10). :1691-1692. (2013)
- Sobreira ML, Maffei FH, Yoshida WB, et al. "Prevalence of deep vein thrombosis and pulmonary embolism in superficial thrombophlebitis of the lower limbs: prospective study of 60 cases.". Int Angiol. 28(5). :400-8. (2009)
- Ellis MH, Fajer S. "A current approach to superficial vein thrombosis.". Eur J Haematol. 90(2). :85-8. (2013)
- Scott G, Mahdi AJ, Alikhan R. "Superficial vein thrombosis: a current approach to management". Br J Haematol. 168(5). :639-645. (2014)
- Beyer-Westendorf J, Schellong SM, Gerlach H, et al. "Prevention of thromboembolic complications in patients with superficial-vein thrombosis given rivaroxaban or fondaparinux: the open-label, randomised, non-inferiority SURPRISE phase 3b trial". The Lancet Haematology. 4(3). :e105-e113. (2017)
- Decousus H et al. "Fondaparinux for the Treatment of Superficial-Vein Thrombosis in the Legs". N Engl J Med. 363(13). :1222-1232. (2010)
- ACOG. "ACOG Practice Bulletin No. 196: Thromboembolism in Pregnancy". Obstetrics & Gynecology. 132(1). :e1-e17. (2018)
- Bates SM, Rajasekhar A, Middeldorp S, et al. "American Society of Hematology 2018 guidelines for management of venous thromboembolism: venous thromboembolism in the context of pregnancy". Blood Advances. 2(22). :3317-3359. (2018)
- Scarvelis D, Wells PS. "Diagnosis and treatment of deep-vein thrombosis". Can Med Assoc J. 175(9). :1087-1092. (2006)
- Bates SM, Greer IA, Middeldorp S, et al. "VTE, Thrombophilia, Antithrombotic Therapy, and Pregnancy". Chest. 141(2). :e691S-e736S. (2012)