Summary
This article covers important clinical findings of urological and renal conditions, including changes in micturition (e.g., dysuria, anuria) and changes in urine (e.g., hematuria, proteinuria) as well as the routine diagnostics for the initial evaluation of patients with urological and renal symptoms, including urinalysis and renal function testing. Urinalysis helps to evaluate urinary abnormalities and involves gross assessment of urine, dipstick, and microscopy of urine sediment. Dipstick is a diagnostic tool consisting of a urine test strip that allows for quick assessment of potentially pathological changes of various parameters (e.g., pH, glucose, protein). Urine sediment allows for microscopic detection of cells, urinary casts, urinary crystals, bacteria, and yeast in a urine sample. Renal function testing involves a panel of parameters to assess for renal dysfunction. Inulin clearance and creatinine clearance provide the most accurate calculation of the GFR while serum creatinine can be used together with demographic data to provide an estimated GFR. The BUN/creatinine ratio and fractional excretion of sodium can be used to evaluate the cause of acute kidney injury. The findings of these tests may be diagnostic or provide guidance for further diagnostic evaluation (e.g., renal biopsy, imaging)
For more on imaging and urodynamic tests, see “Diagnostic investigations in urology.” For more on urine culture, see “Laboratory tests” under diagnostics in “Urinary tract infections.” Current NBME laboratory reference values can be found under “Tips and Links” below.”
History and physical examination
Clinical examination
- Changes in urine and micturition: evaluate amount, frequency, appearance, and discomfort (see table below for details)
-
Flank pain
- Colicky pain radiating to the groin or genitals is most commonly seen in urolithiasis
- Persistent pain: indicative of inflammatory diseases (e.g., pyelonephritis)
- Costovertebral angle tenderness: : characteristic of pyelonephritis
- Nausea/vomiting: can be a sign of end-stage renal disease: or urolithiasis
- Hypertension: can be an extrarenal manifestation of kidney injury
- Peripheral edema: See “Proteinuria.”
- Pericardial friction rub: See “Uremic pericarditis.”
- Pulmonary edema: can indicate volume overload due to renal injury with low urine output
-
Skin changes: can be indicative of an underlying systemic disease
- Allergic rash (e.g., tubulointerstitial nephritis, systemic lupus erythematosus)
- Petechiae, purpura (e.g., IgA vasculitis, thrombotic thrombocytopenic purpura)

Acute appendicitis should be differentiated from right-sided renal colic. Findings that suggest appendicitis include nausea, fever, and pain at McBurney point (see appendicitis signs).
Changes in micturition
| Overview of micturition changes | |||
|---|---|---|---|
| Definition | Common diagnoses | ||
| Quality of micturition | |||
| Dysuria |
|
|
|
| Pollakiuria |
|
|
|
| Nocturia |
|
|
|
| Quantity of urine excretion | |||
| Polyuria |
|
|
|
| Oliguria |
|
|
|
| Anuria |
|
|
|
Changes in urine
| Overview of urine changes | |||
|---|---|---|---|
| Definition | Common diagnoses | ||
| Isosthenuria |
|
|
|
| Glycosuria |
|
|
|
| Ketonuria |
|
|
|
| Proteinuria |
|
|
|
| Bacteriuria |
|
|
|
| Pyuria |
|
|
|
| Hematuria |
|
|
|
| Hemoglobinuria |
|
|
|
| Myoglobinuria |
|
|
|

© AMBOSS
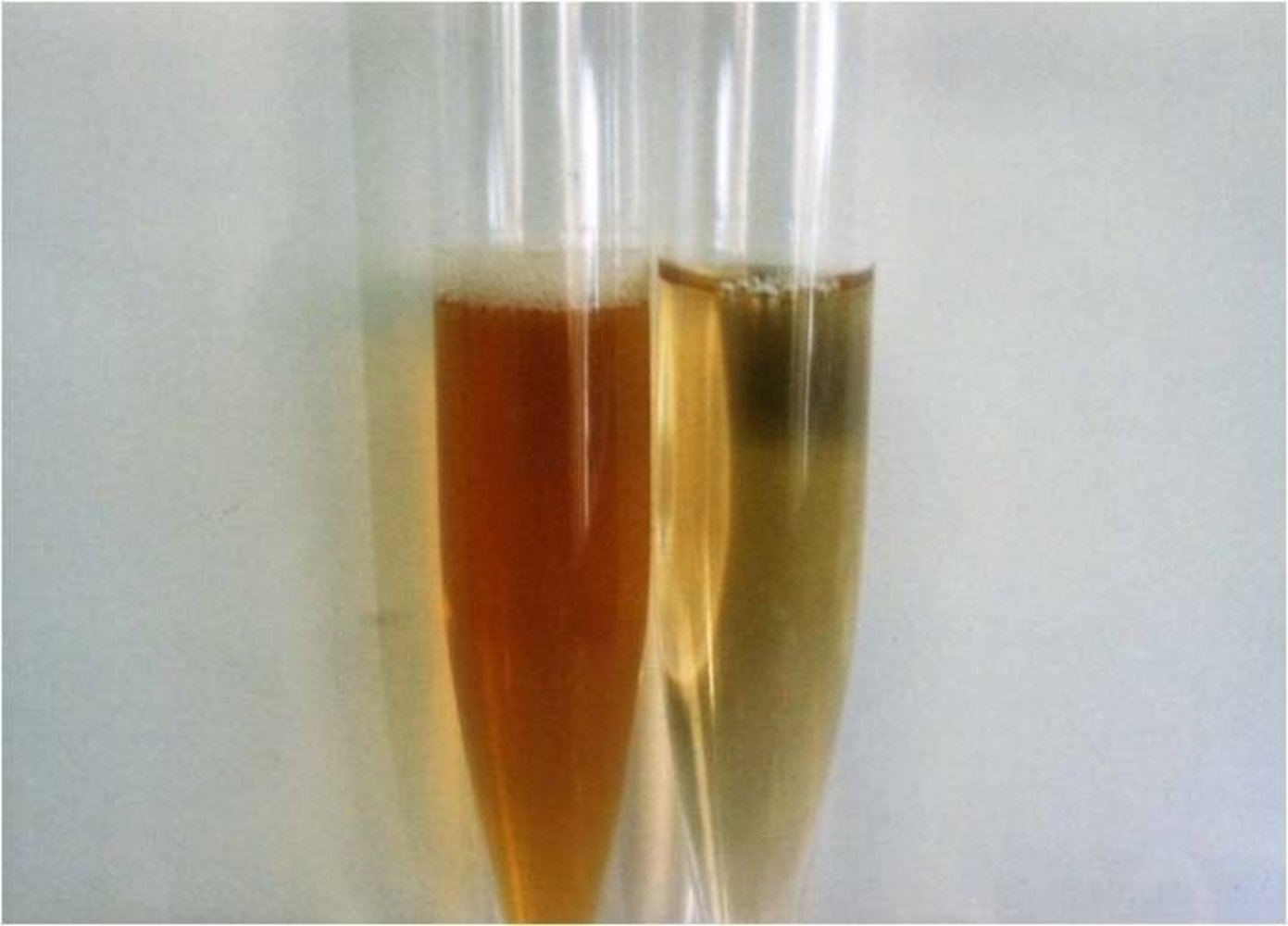
Urine sample of a patient with paroxysmal nocturnal hemoglobinuria (left) next to control urine (right)
The patient's urine appears significantly darker and redder than the control urine.
Source: “Figure 1. in: Paroxysmal nocturnal hemoglobinuria in systemic lupus erythematosus: a case report” by Norio Nakamura et al., Journal of Medical Case Reports, BioMed Central, licensed under CC BY 2.0.
Urinalysis
Urinalysis involves the gross examination of urine, chemical evaluation using urine dipstick, and microscopic assessment of urine sediment. Further tests include urine culture and urinary electrolyte levels. Indications for urinalysis include renal, urinary, and metabolic conditions.
Gross urine assessment
-
Urine color
- Normal: pale yellow to dark amber
- Red urine: See “Hematuria.”
- Black urine: alkaptonuria
- Turbidity (cloudiness of the urine): cloudy urine suggests infection or chyluria
Certain drugs (e.g., rifampin, phenazopyridine), foods (e.g., beetroot), and types of porphyria cause red discoloration of urine.
Urine dipstick
A diagnostic tool consisting of a urine test strip that allows for quick assessment of potentially pathological changes of various parameters.
- pH (urine pH usually ranges from 4.5–8)
-
Urine specific gravity: Measures the ratio of urine density over pure water density (normally 1.005–1.030)
- High urine specific gravity: volume loss, heart failure, presence of large molecules (e.g., glucose, radiocontrast media)
- Low urine specific gravity: renal failure, diabetes insipidus
- Heme: > 90% sensitivity for hematuria (low specificity)
- Leukocyte esterase: enzyme produced by WBC that indicates a urinary tract infection
- Protein (albumin): See “Proteinuria.”
- Glucose: glycosuria is a key finding of diabetes mellitus
- Ketones: ketonuria can help diagnose diabetic ketoacidosis, a complication of type 1 diabetes mellitus
- Urobilinogen: See “Prehepatic jaundice” and “Intrahepatic jaundice.”
- Nitrite: indicative of urinary tract infection caused by gram-negative bacteria (e.g., Enterobacteriaceae)
 test strip")
A urine dipstick cannot differentiate between hematuria, hemoglobinuria, or myoglobinuria. Therefore, every positive test result for heme must be confirmed with the presence of RBCs on microscopy.
Urine sediment
- Indications: can help identify acute and chronic kidney diseases, classify renal calculi, and diagnose UTIs
- Method: Urine is centrifuged and the pellets are examined under the microscope (supernatant is discarded).
-
Assessment: provides valuable information about the underlying cause of kidney damage
- Cells
- Erythrocytes
- Leukocytes
- Acanthocytes
-
Urinary casts: Tubular structures formed in the distal convoluted tubule and collecting duct of the kidneys that are indicative of a disease affecting the renal tubules and/or glomeruli
- See table below for details.
- Crystals: See overview of urinary calculi.
- Bacteria
- Yeast
- Cells
| Urinary casts [2] | |||
|---|---|---|---|
| Structure | Microscopy | Interpretation | |
| Hyaline casts |
|
|
|
| Granular casts |
|
|
|
| Muddy brown casts |
|
|
|
| Hemoglobin casts |
|
|
|
| Fatty casts |
|
|
|
| Renal tubular epithelial cell casts |
|
|
|
| White blood cell casts |
|
|
|
| Red blood cell casts |
|
|
|
| Waxy casts |
|
|
|
| Broad casts |
|
|
|




 casts in urine sediment")


Further laboratory tests
-
Urine osmolality
- Can be used to evaluate urine concentration
- More accurate than the dipstick measurement for specific gravity
- Urine osmolar gap (UOG): The difference between measured urine osmolality and calculated urine osmolality, used to estimate urine NH4+ concentration in metabolic acidosis.
-
Urine electrolytes
- Urine sodium (Na+): e.g., low urine sodium indicates that the kidneys are trying to retain free water by reabsorbing Na+ (e.g., due to dehydration)
- Fractional excretion of sodium: can help determine the cause of acute kidney injury
- Urine creatinine: used to calculate creatinine clearance
- Urine culture: See diagnosis section in “Urinary tract infections.”
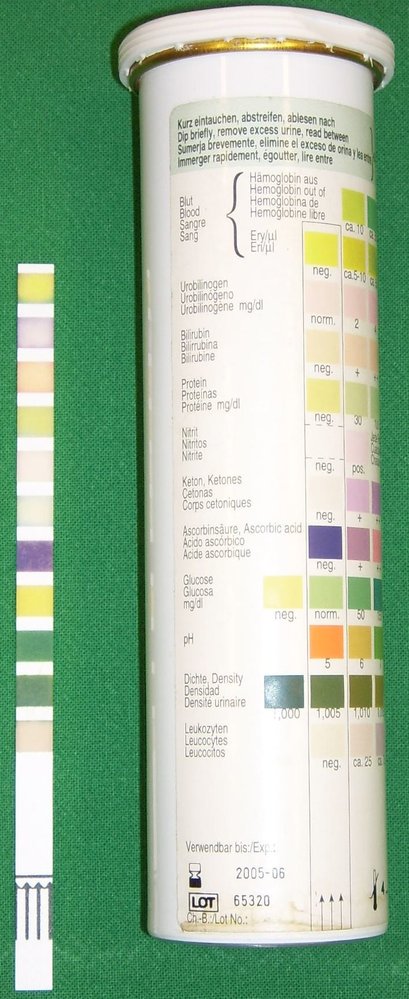
Left: test strip following immersion in urine
Right: test strip packaging with instructions on how to interpret findings
Source: “Urine Quicktest” by Uwe Gille, Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}

Urine sediment microscopy (left: unstained; right: Sternheimer stain, 400x magnification)
Left: A translucent, cylindrical, acellular structure is seen.
Right: The stain has enhanced the protein matrix, which appears light blue.
These features are typical of hyaline casts, which are composed of a mucoprotein matrix of Tamm-Horsfall protein and contain neither cells nor debris.
Hyaline casts are a nonspecific finding on urinalysis as they are also seen in healthy individuals.
Source: “Figure 3/1-U&1-S. in: Enhancing the Detection of Dysmorphic Red Blood Cells and Renal Tubular Epithelial Cells with a Modified Urinalysis Protocol” by Yu Chu-Su, Kenichi Shukuya, Takashi Yokoyama, Wei-Chou Lin, Chih-Kang Chiang & Chii-Wann Lin, Scientific Reports Journal, Nature, licensed under CC BY 4.0.

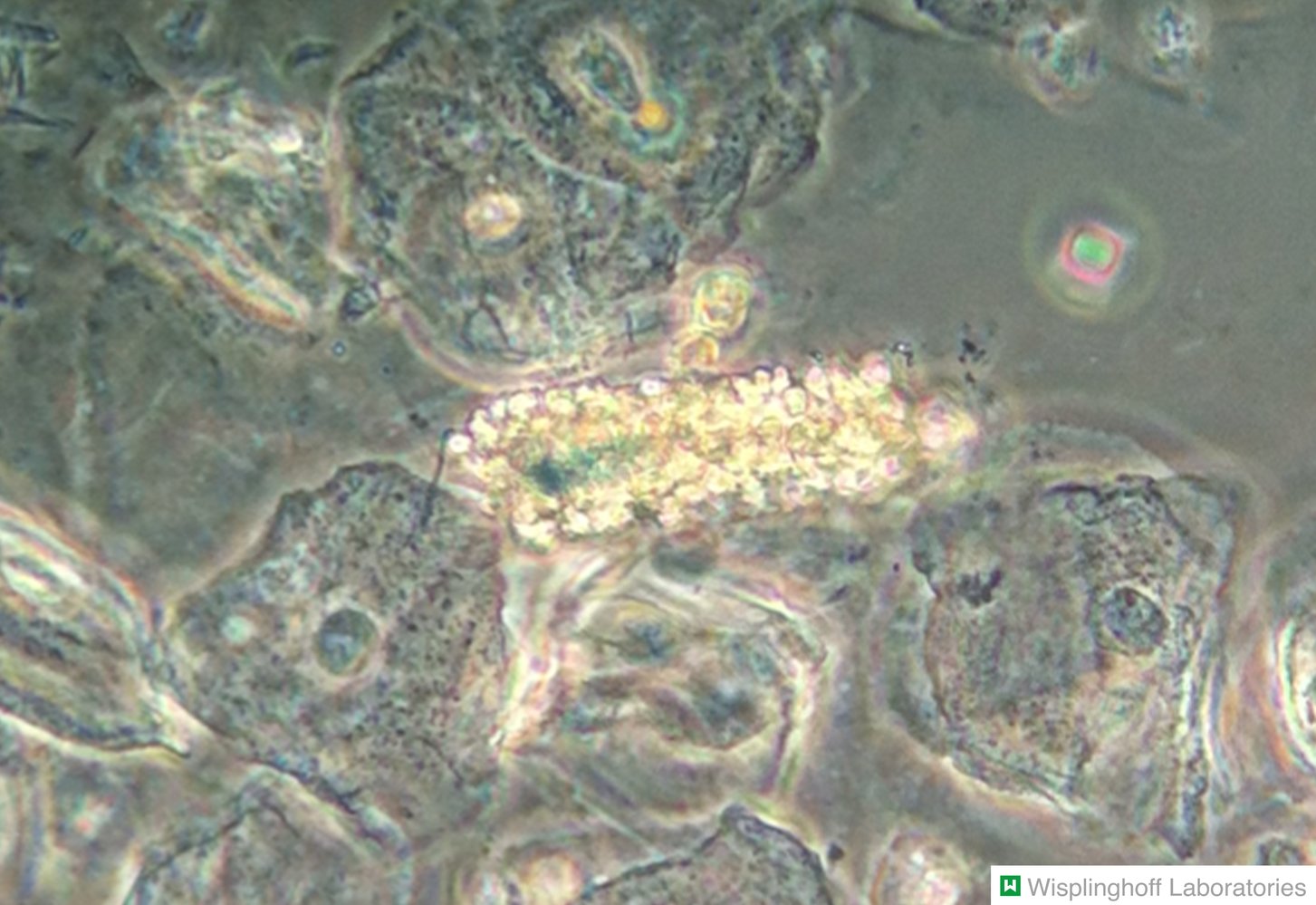
Photomicrograph of urine sediment (phase-contrast microscopy; high magnification)
The granular cast in the center of the image is comprised of a hyaline matrix (green overlay) with large droplets of plasma proteins embedded within.
Granular casts can be an indication of proteinuria (e.g., in glomerulonephritis or pyelonephritis). However, they may also be present in healthy individuals (e.g., after severe physical stress).
Our great thanks to Dr. Wisplinghoff (Dr. Wisplinghoff's laboratory) for kindly providing this image.
Polarized light micrograph of lyotropic liquid crystals
These Lα liquid crystals have a characteristic Maltese cross appearance (examples indicated by green overlay) under polarized light. Fatty casts from urinary sediment have the same appearance under polarized light.
Source: “Figure 4 (a), in: Development and Characterization of Nanostructured Pharmacosomal Mesophases: An Innovative Delivery System for Bioactive Peptides” by Maryam Rezvani, Javad Hesari, Seyed Hadi Peighambardoust, Maria Manconi, Hamed Hamishehkar, Advanced Pharmaceutical Bulletin, licensed under CC BY 4.0. Modifications: image cropped. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
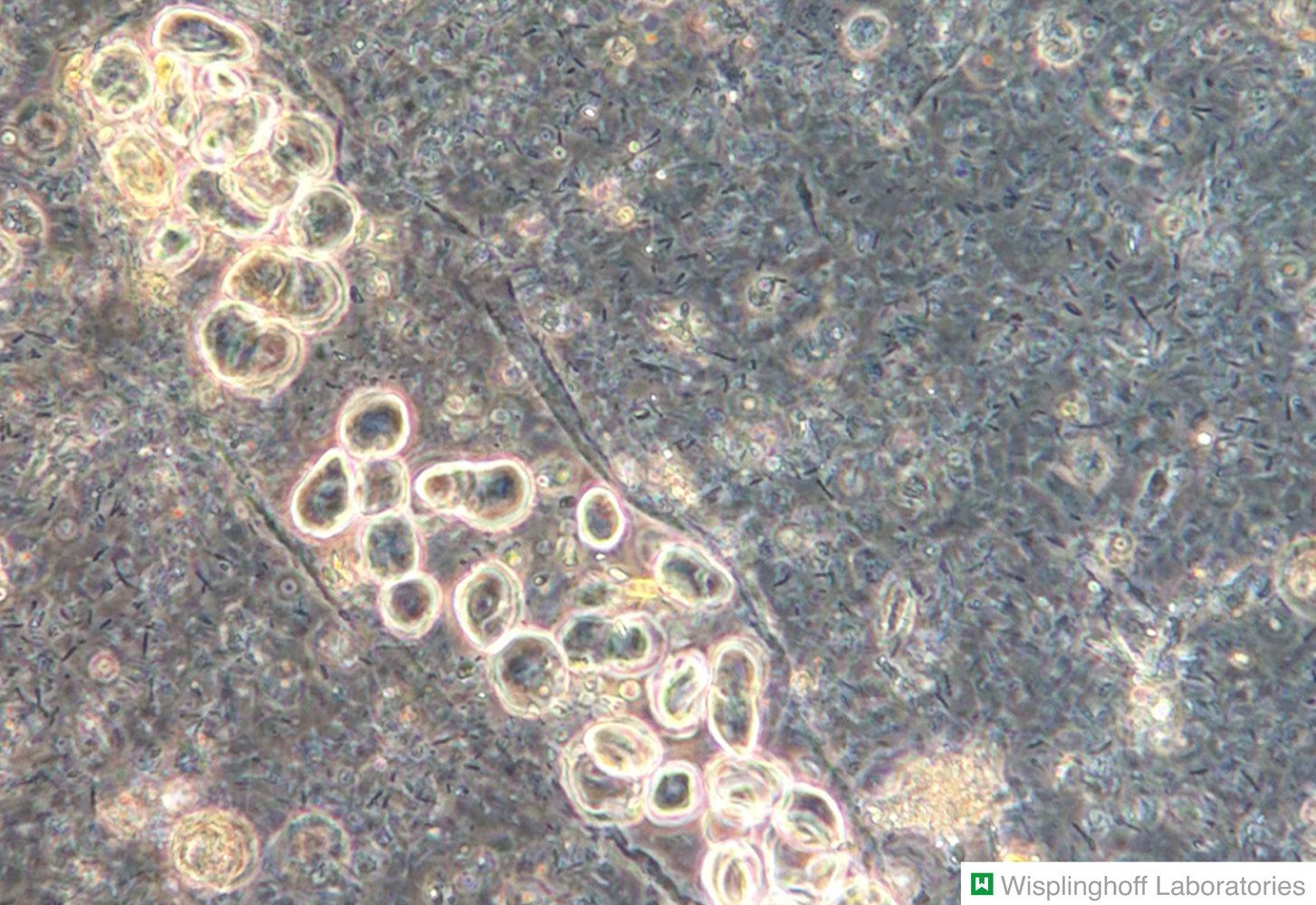
Photomicrograph of urine sediment (phase-contrast microscopy; high magnification)
White blood cell (WBC) casts (blue overlay) contain leukocytes (examples outlined in yellow) that are compressed in a matrix. Sharp margins are characteristic of WBC casts, differentiating them from randomly assembled leukocyte conglomerates.
Our great thanks to Dr. Wisplinghoff (Dr. Wisplinghoff's laboratory) for kindly providing this image.

Photomicrograph of urine sediment (high magnification)
A cast consisting of multiple red blood cells is visible.
RBC casts are typically seen in patients with glomerular damage (e.g., glomerulonephritis).
Source: © IMPP
Photomicrograph of urine sediment (phase-contrast microscopy)
A tubular cast (blue overlay) is visible in the center of the image. The cast is composed of numerous RBCs, identifiable by their characteristic biconvex shape (examples outlined in yellow), in a matrix of fibrin and plasma proteins. Several epithelial cells surrounding the RBC cast are also visible.
RBC casts in urinary sediment are typically seen in glomerulonephritis.
Our great thanks to Dr. Wisplinghoff (Dr. Wisplinghoff's laboratory) for kindly providing this image.

Photomicrograph of urine sediment (high magnification)
Degenerating granular casts are described as waxy casts, which typically have a homogeneous, smooth, yellowish appearance and show clearly defined, dark borders with blunt and broken-off ends. They are more brittle and fragile in comparison with other casts. The lower figure shows a segmented example, where sharp indentations are easily recognizable.
Waxy casts are found in the urine sediment of patients with chronic kidney failure.
Original title: “Waxy casts”. Created by: kdi. Modifications to original image: Image cropped. Further notes: Used with kind permission of José A. T. Poloni
Renal function test
Overview
- Parameters of renal function allow for the evaluation of changes in renal function.
- Inulin clearance and creatinine clearance (with 24-hour urine collection): allow for the most accurate calculation of the glomerular filtration rate
- Serum creatinine and serum cystatin C allow for indirect measurement of the glomerular filtration rate (see estimated GFR).
- Urea (BUN) and uric acid are largely dependent on renal excretion; however, they only provide an inaccurate assessment of renal function.
- Fractional excretion of urine is used to establish the cause of acute kidney injury.
- Current NBME laboratory reference values can be found under “Tips and Links” below.”
Glomerular filtration rate (GFR) [3][4]
- Defined as the volume of primary urine that is filtrated by the kidneys over a certain amount of time per standardized body surface area (1.73 m2)
- Normal GFR: ≥ 90 mL/min/1.73m2
- GFR is ∼ 120 mL/min/1.73m2 in young adults, decreases with age, and varies considerably between males and females
- After the age of 29, a physiological decrease in the GFR of about 10 mL/min/1.73m2 occurs every 10 years.
- GFR can be calculated or estimated using various methods (e.g., estimated GFR).
Serum creatinine
-
Indirect indicator of renal function
- Creatinine is a metabolite of creatine in the muscle (creatine + ATP ⇄ phosphocreatine + ADP).
- Creatinine is entirely removed by glomerular filtration.
- Because creatinine is produced at a relatively constant rate and freely filtered by the glomeruli, it can be used to estimate GFR.
-
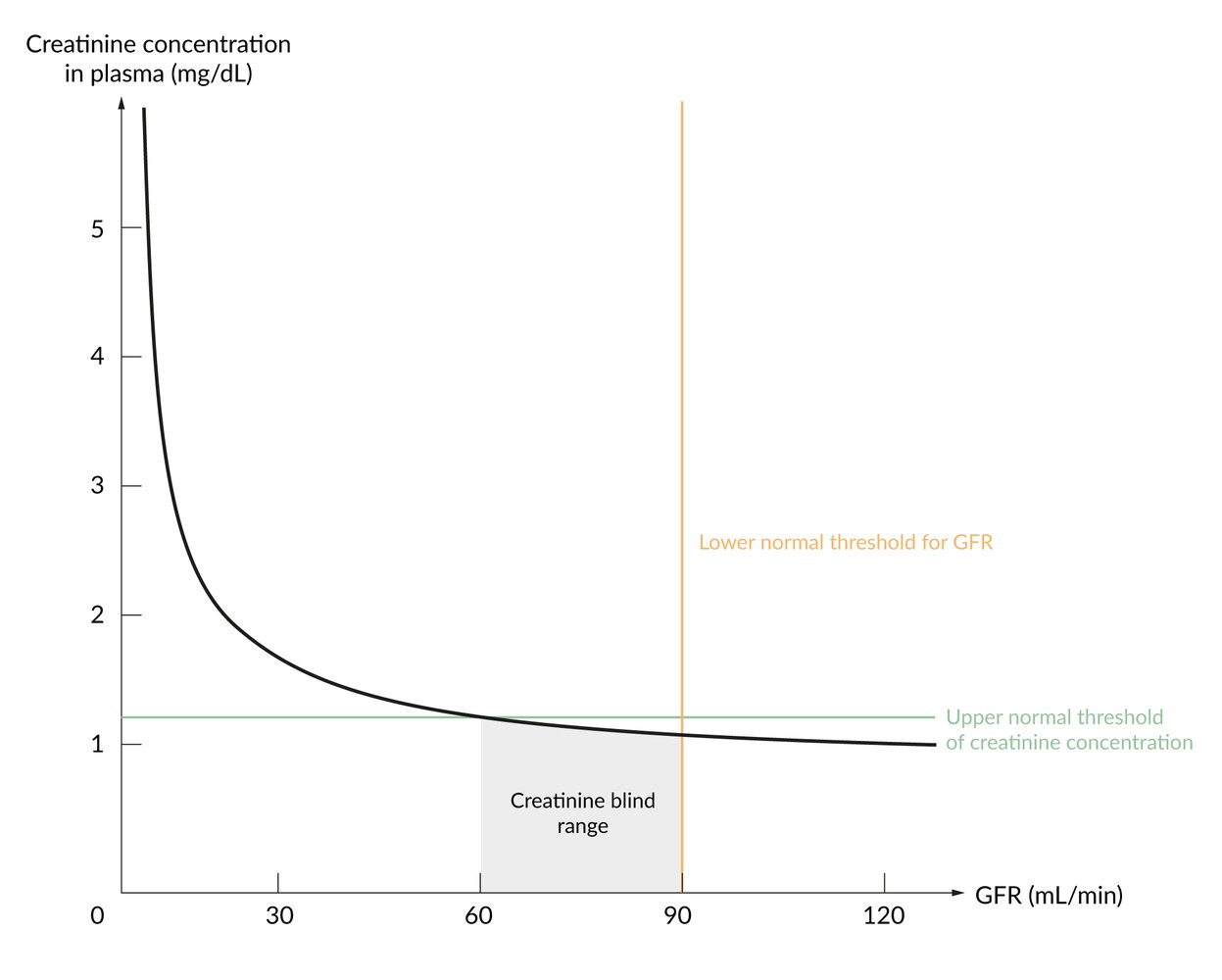
Creatinine-blind range
- Serum creatinine levels do not start rising until the GFR is reduced by approx. 50%.
- If the GFR is > 60 mL/min, serum creatinine cannot be used to assess kidney function.
- Additional interfering factors:
- Increased creatinine levels
- High-protein diet
- High muscle mass
- Rigorous exercise
- Decreased creatinine levels: low muscle mass
- Increased creatinine levels

Serum creatinine levels do not start rising until the GFR is reduced by approx. 50%.
Creatinine clearance
- Used in clinical settings to approximate the glomerular filtration rate (GFR)
- Slightly overestimates GFR because of minimal creatinine secretion in the proximal tubules [5]
- A precise evaluation of creatinine clearance requires measuring creatinine in the urine over a 24-hour period.
-
Creatinine clearance = (CreaUrine x V) / CreaPlasma ≈ GFR
- CreaUrine = creatinine concentration in urine
- V = rate of urine flow in mL/min (volume/time)
- CreaPlasma = creatinine concentration in plasma
Creatinine clearance can be used to approximate the GFR.
Estimated GFR (eGFR)
- Calculated using serum creatinine concentration and demographic data
- Several prediction equations can be used in clinical practice.
- Cockcroft-Gault equation: creatinine clearance = [(140 – age) x weight (kg) x constant] / serum creatinine (mmol/L)
- Modification of Diet in Renal Disease (MDRD) study equation
- Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation
Serum cystatin C
- A more precise indicator of the GFR than serum creatinine
- Cystatin C is a small protein that inhibits cysteine proteinases and is produced by all nucleated cells.
- Analysis is more complex and expensive; therefore, not routinely ordered.
- Lower “blind range” than serum creatinine: used particularly when urine sampling is not feasible (e.g., in infants)
Blood urea nitrogen (BUN)
- A waste product produced by the liver in the urea cycle after protein degradation
- Filtered and excreted by the kidneys
- Elevated with
- Reduced GFR
- High protein diet
- Protein catabolism
BUN/creatinine ratio
- Can help diagnose the underlying cause in acute kidney injury
- 10:1–20:1 can be normal or may indicate a postrenal cause.
- ≥ 20:1 indicates prerenal cause: Urea reabsorption is increased, which is typical in patients with dehydration or hypoperfusion.
- ≤ 15:1 indicates intrarenal cause: Renal damage causes decreased urea reabsorption.
Fractional excretion of sodium (FeNa)
- Definition: percentage of the glomerular filtered sodium (NaFiltered) that is eventually excreted in the urine (NaExcreted)
-
Usage
- Can help establish the cause of acute kidney injury
- Can help distinguish between renal and extrarenal etiology in hypotonic hyponatremia (see “Diagnostic approach to hyponatremia”)
-
Calculation
- Filtered Na = NaPlasma x GFR
- Excretion rate of Na = NaUrine x V
- FeNa = NaExcreted / NaFiltered
- FeNa = (NaUrine x V) / (NaPlasma x GFR)
- FeNa = (NaUrine x V) / (NaPlasmax [CreaUrine x V / CreaPlasma])
- FeNa = (NaUrine x CreaPlasma) / (NaPlasmax CreaUrine)
-
Interpretation
-
In acute kidney injury
- Low FeNa (< 1%): indicates a prerenal cause (renal hypoperfusion)
- High FeNa (> 2%): indicates an intrarenal etiology (e.g., acute tubular necrosis)
- Inconclusive FeNa (1–2%): can be seen with either disorder
- In hypotonic hyponatremia
- Low FeNa (< 1%): extrarenal cause
- High FeNa (> 1%): renal cause
-
In acute kidney injury
Additional blood tests
- Autoantibodies: : particularly antinuclear antibodies (ANCA) as an indication of glomerulonephritis
-
Uric acid: a metabolite of purine bases
- Uric acid crystals can form in the joints, where they can trigger inflammatory reactions and pain (i.e., gout attack).
- Hyperuricosuria can lead to uric acid nephropathy.
-
Other
- Other parameters that should be evaluated in renal disease (particularly in chronic renal failure) are serum electrolytes (Na+, K+, Ca2+, phosphate), vitamin D, and parathyroid hormone (PTH).
- See “Diagnostics” in “Chronic kidney disease” for details.

Renal parameter changes
| Overview of renal parameters | ||
|---|---|---|
| Laboratory parameter | Causes of increased values | Causes of decreased values |
| Creatinine |
|
|
| Cystatin C |
|
|
| Blood urea nitrogen (BUN) |
|
|
| Uric acid |
|
|
© AMBOSS

© AMBOSS
Renal biopsy
Overview
- Usually performed percutaneously under local anesthesia and with ultrasound guidance.
- Examination of the tissue sample includes light, immunofluorescence, and electron microscopy.
- The most common complication is bleeding.
Indications
- Nephritic and/or nephrotic syndrome with no apparent underlying disease: allows diagnosing type of glomerulonephritis
- Suspected lupus nephritis
- Rapidly progressive glomerulonephritis
- Renal transplant rejection or dysfunction
- Unexplained acute kidney injury
Contraindications
- Solitary kidney (relative contraindication)
- Infection of the kidneys
- Coagulation disorders (e.g., thrombocytopenia, disorders of the platelet function, bleeding diathesis)
- Uncontrolled hypertension
- Anatomic abnormalities
- Abnormal position of the kidneys
- Atrophic kidneys
- Vascular malformations in the kidney region
- Hydronephrosis
- Multiple, bilateral renal cysts
Related One-Minute Telegram
- One-Minute Telegram 14-2020-3/3: GFR formulas are just estimates, but can we estimate better?
Interested in the newest medical research, distilled down to just one minute? Sign up for the One-Minute Telegram in “Tips and links” below.
External Resources
References
- Klahr S, Miller SB. "Acute Oliguria". N Engl J Med. 338(10). :671-675. (1998)
- "Urinalysis". https://library.med.utah.edu/WebPath/TUTORIAL/URINE/URINE.html. [2017-01-01]
- Redal-Baigorri B, Rasmussen K, Heaf JG. "Indexing glomerular filtration rate to body Surface area: clinical consequences". J Clin Lab Anal. 28(2). :83-90. (2013)
- "GFR". https://www.kidney.org/kidneydisease/siemens_hcp_gfr
- Lin Y, Bansal N, Vittinghoff E, Go AS, Hsu C. "Determinants of the creatinine clearance to glomerular filtration rate ratio in patients with chronic kidney disease: a cross-sectional study". BMC Nephrol. 14(1). (2013)
- Fischbach FT, Dunning MB. "A Manual of Laboratory and Diagnostic Tests". Lippincott Williams & Wilkins. (2009). ISBN: 9780781771948