Quick guide
Diagnostic approach
- Inflammatory diarrhea or noninflammatory diarrhea that is not self-limited: stool GI pathogen panel (PCR) or culture
- Severe illness with fever: CBC, CMP, ESR, CRP, blood cultures
- Risk factors for C. difficile infection: C. difficile PCR or EIA
Diagnostic testing is not indicated for most cases of acute diarrhea.
Management checklist
- Mild to moderate dehydration: oral rehydration therapy
- Severe dehydration: IV fluid resuscitation
- Antidiarrheal agents (as needed): bismuth (safe for all patients), loperamide (for patients with noninflammatory diarrhea)
- Supportive therapy for gastroenteritis
- Empiric antibiotics for bacterial gastroenteritis as indicated
- Suspected C. difficile infection: antibiotic therapy for CDI
- Traveler's diarrhea: ciprofloxacin (off label) (most destinations) OR azithromycin (off label) (travelers to South or Southeast Asia)
Red flag features
- Fever
- Hypotension
- Severe dehydration
- Bloody stools
- Severe abdominal pain
- Chronic illness
- Immunocompromise
- Age > 65 years
- Recent antibiotic use
- > 48 hours duration without improvement
Life-threatening causes
- Hemolytic uremic syndrome
- Gas gangrene
- Shigellosis
- Cholera
- Ischemic colitis
Summary
Diarrhea, defined as three or more loose stools per day or more frequent stool passage than is normal for the individual, is a common disease with a monthly prevalence of around 5% in the United States. Acute diarrhea lasts 14 days or less and is almost always caused by an infectious agent, typically a virus. Testing is seldom required, as the disease tends to be self-limited and care is primarily supportive. Persistent diarrhea, lasting 15–30 days, is also typically caused by an infectious agent, but stool testing for pathogens is generally warranted to confirm the diagnosis. Chronic diarrhea, defined as diarrhea lasting longer than 30 days, has an extensive differential diagnosis. A thorough history followed by systematic stool and blood testing is required to identify the specific etiology. The presence of any red flags for severe or rapidly progressing diarrheal disease (e.g., sepsis, extreme dehydration, blood in the stool) mandates escalation of testing and, in some cases, empiric antibiotics for bacterial gastroenteritis. Ensuring adequate oral hydration, correcting dehydration, and providing symptomatic relief are fundamental components in the care of all patients with diarrhea. Curative treatment is directed toward the underlying cause.
Definitions
The WHO defines diarrhea as ≥ 3 loose or watery stools per day or more frequent passage than is normal for the individual. [1][2]
Etiology
For etiologies of acute, persistent, or chronic diarrhea, see specific subsections below.
Overview of pathogens causing watery and bloody diarrhea
| Overview | ||||
|---|---|---|---|---|
| Type of diarrhea | Pathogen | Pathogen characteristics | Associated disorders | |
| Watery diarrhea |
|
|
|
|
|
|
|
||
|
|
|
||
|
|
|
||
|
|
|
|
|
|
|
|||
|
|
|||
|
|
|
|
|
|
|
|
||
|
|
|
||
| Bloody diarrhea |
|
|
|
|
|
|
|
||
|
|
|
||
|
|
|
||
|
|
|
||
|
|
|
||
|
|
|
||












")
Infectious causes [4][5]
| Conditions | ||
|---|---|---|
| Viral |
|
|
| Bacterial |
|
|
| Parasitic | Protozoan |
|
| Helminth infections |
|
|
Noninfectious [7][8][9]
| Conditions | |
|---|---|
| Foodborne toxins |
|
| Food poisoning |
|
| Gastrointestinal |
|
| |
| |
|
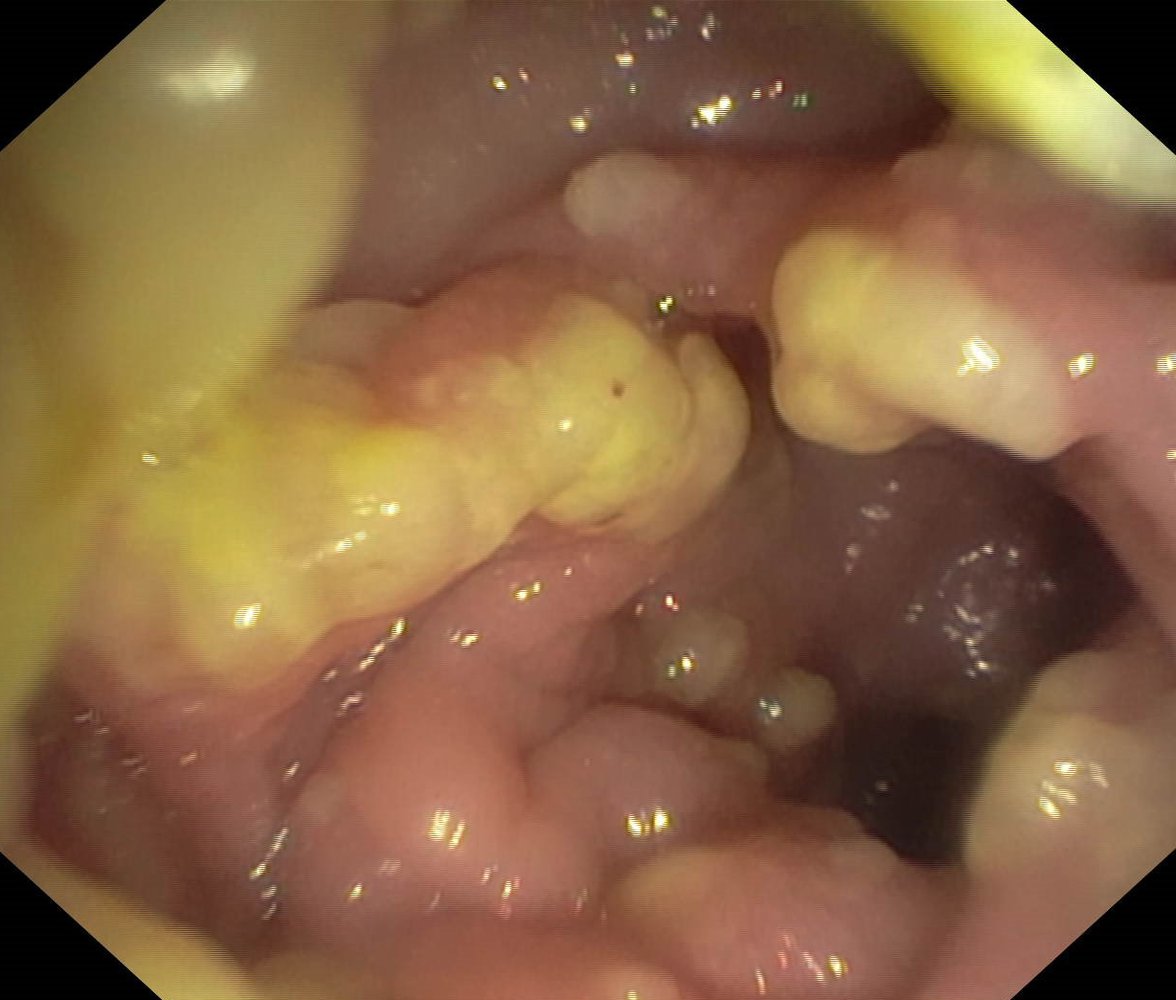
Endoscopic view of the colon
The colonic mucosa is erythematous and edematous. Fibrin exudate has formed partially confluent, yellow plaques over the mucosa (referred to as “pseudomembranes”).
These findings are diagnostic of pseudomembranous colitis.
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.
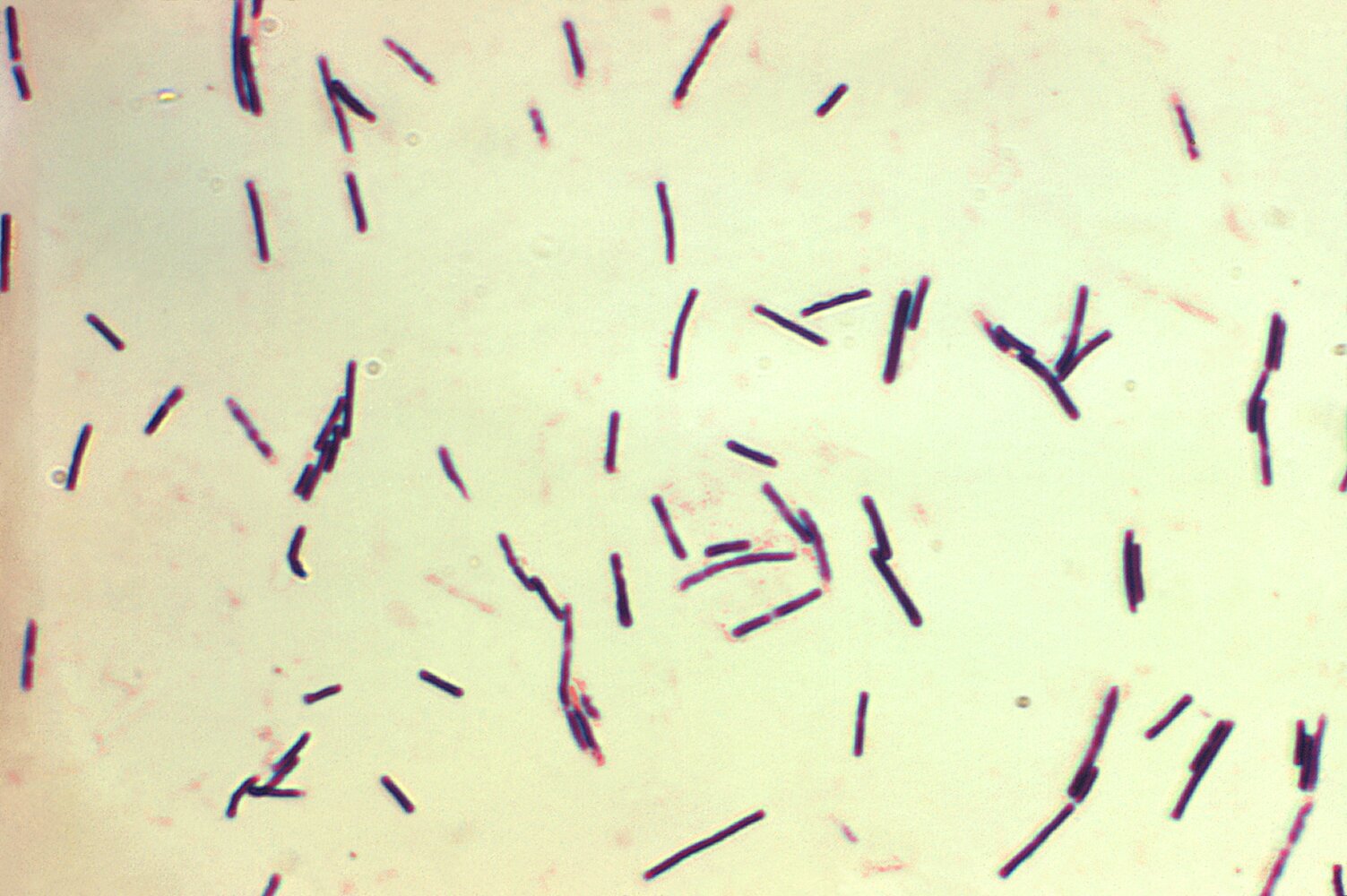
Photomicrograph of a bacterial culture (Gram stain; very high magnification; cultivated in Schaedler broth)
Multiple gram-positive, rod-shaped Clostridium perfringens bacteria are seen.
Source: Centers for Disease Control and Prevention (CDC) licensed under Public Domain

X-ray of the right hip and thigh of a 39-year-old male patient
A feathering pattern of multiple foci of radiolucent gas (green overlay) is visible within the muscles of the right thigh.
This appearance is pathognomonic of gas gangrene.
Source: “Plain x-ray films in soft tissue infections” by Diogo Carrola Gomes, Luísa Quaresma, The Pan African Medical Journal, licensed under CC BY 2.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
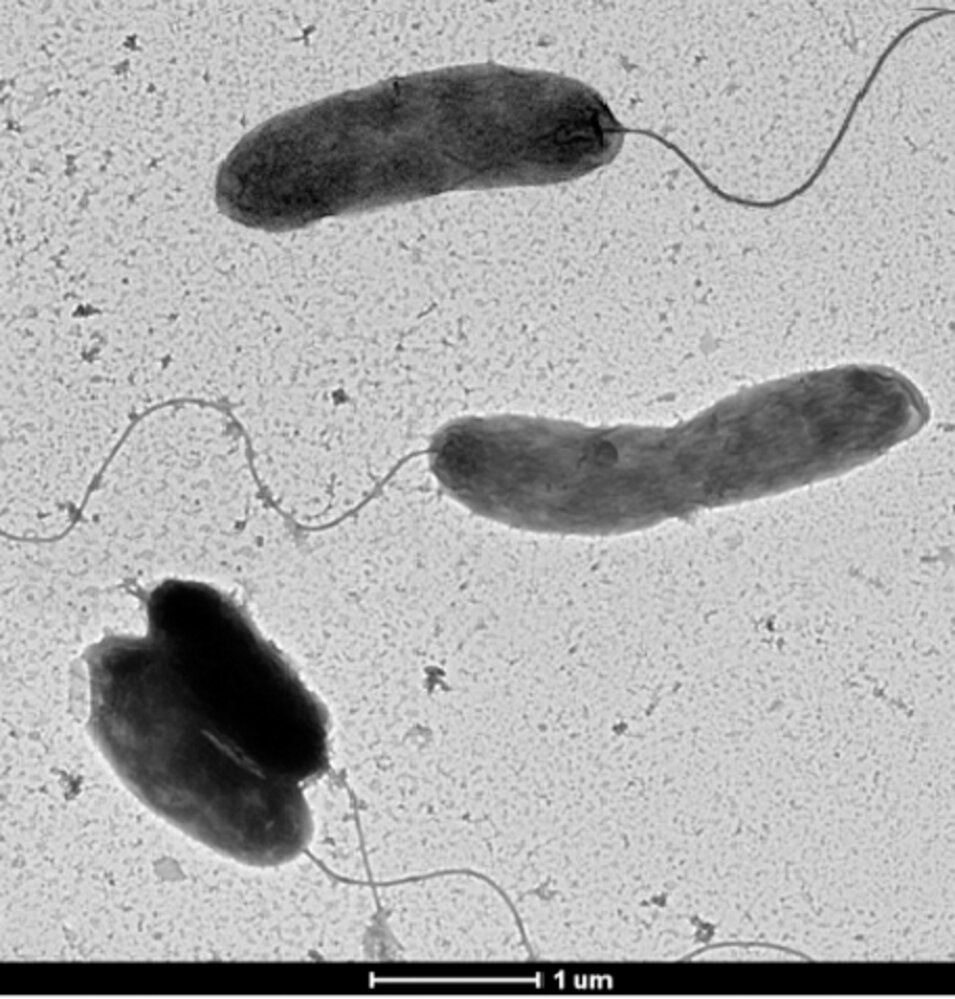
Electron micrograph
Comma-shaped bacteria with flagellae used for motility are visible.
Source: “Figure 6, in: Isolation and Characterization of the New Mosaic Filamentous Phage VFJ Φ of Vibrio cholerae” by Wang Q, Kan B, Wang R, Plos one, licensed under CC BY 4.0. Modifications: Image cropped.
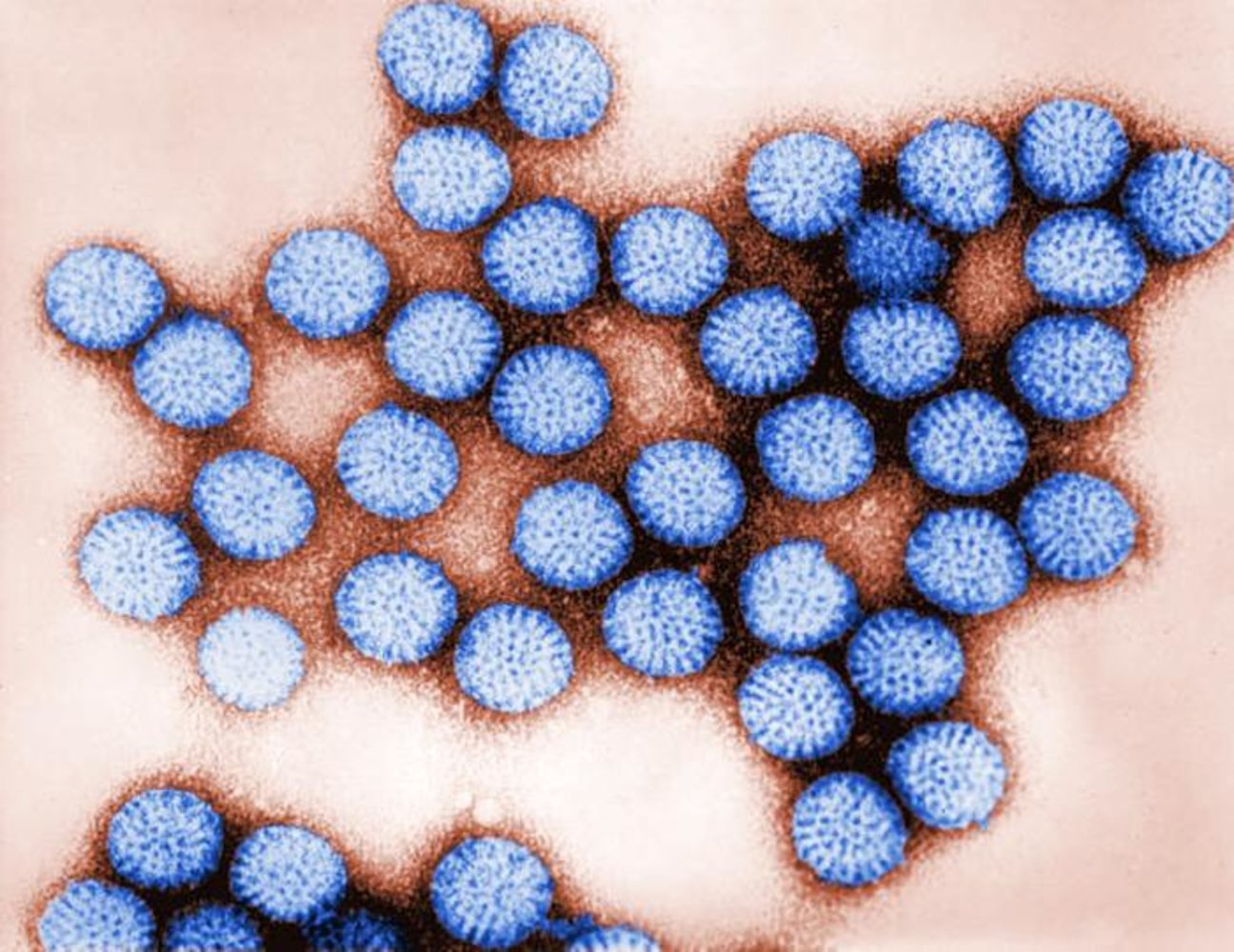
Transmission electron microscopy (TEM)
Spherical particles (Rota virions) with globular structures (capsomere proteins) on their surfaces can be seen.
Source: "ID#: 178", CDC/ Dr. Erskine Palmer, Bryon Skinner, Centers for Disease Control and Prevention licensed under Public Domain Further notes: Public Health Image Library (PHIL); ID:178
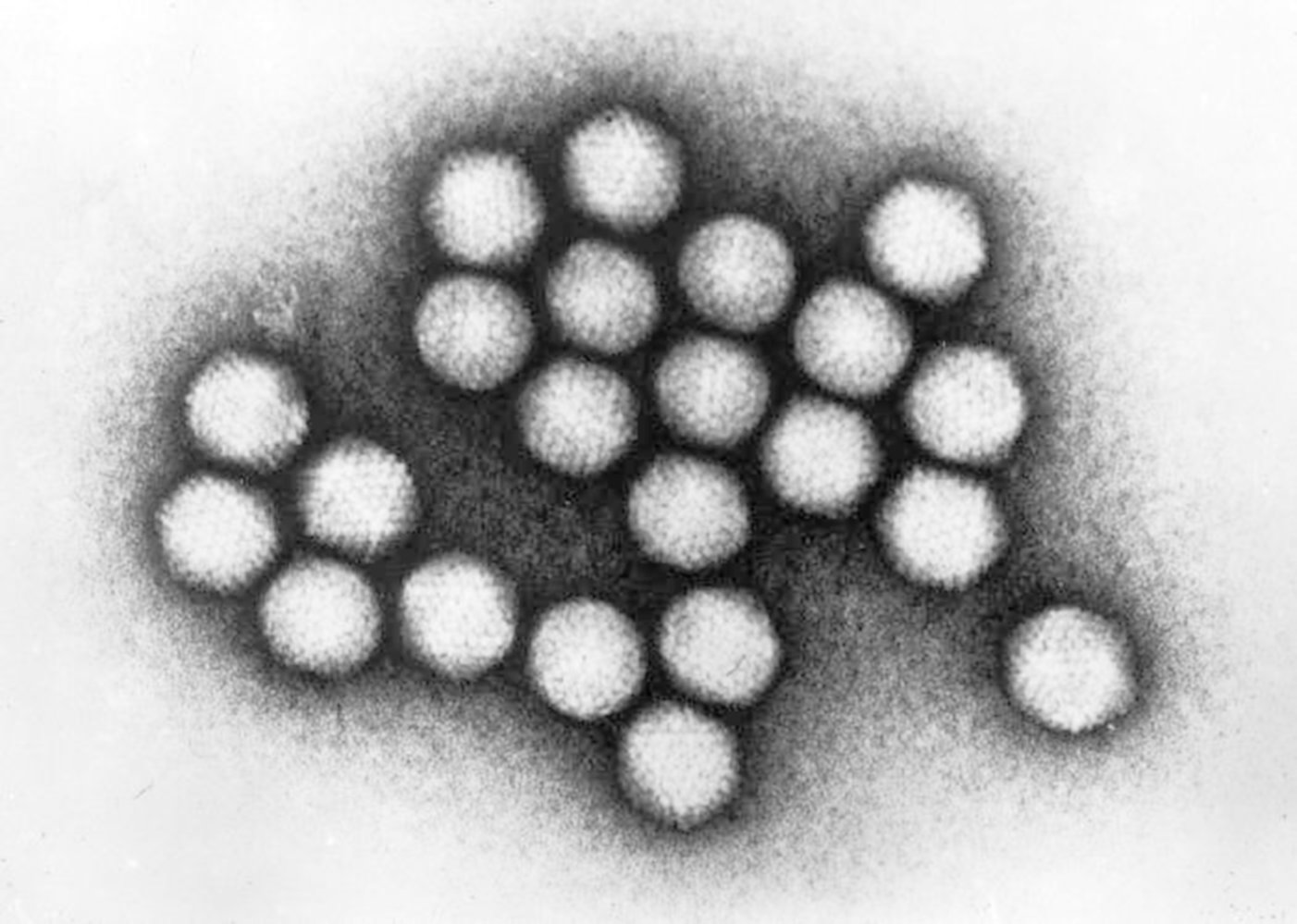
Electron micrograph of adenoviruses
The clustered virus particles appear to have a symmetrical, circular to icosahedral shape.
The appearance of the adenovirus is dictated by the icosahedral shape of its nucleocapsid, as the virus does not have a lipid envelope. The absence of a lipid envelope results in relatively high tenacity.
Source: "ID#: 237", CDC/ Dr. G. William Gary, Jr., Centers for Disease Control and Prevention (CDC) licensed under Public Domain
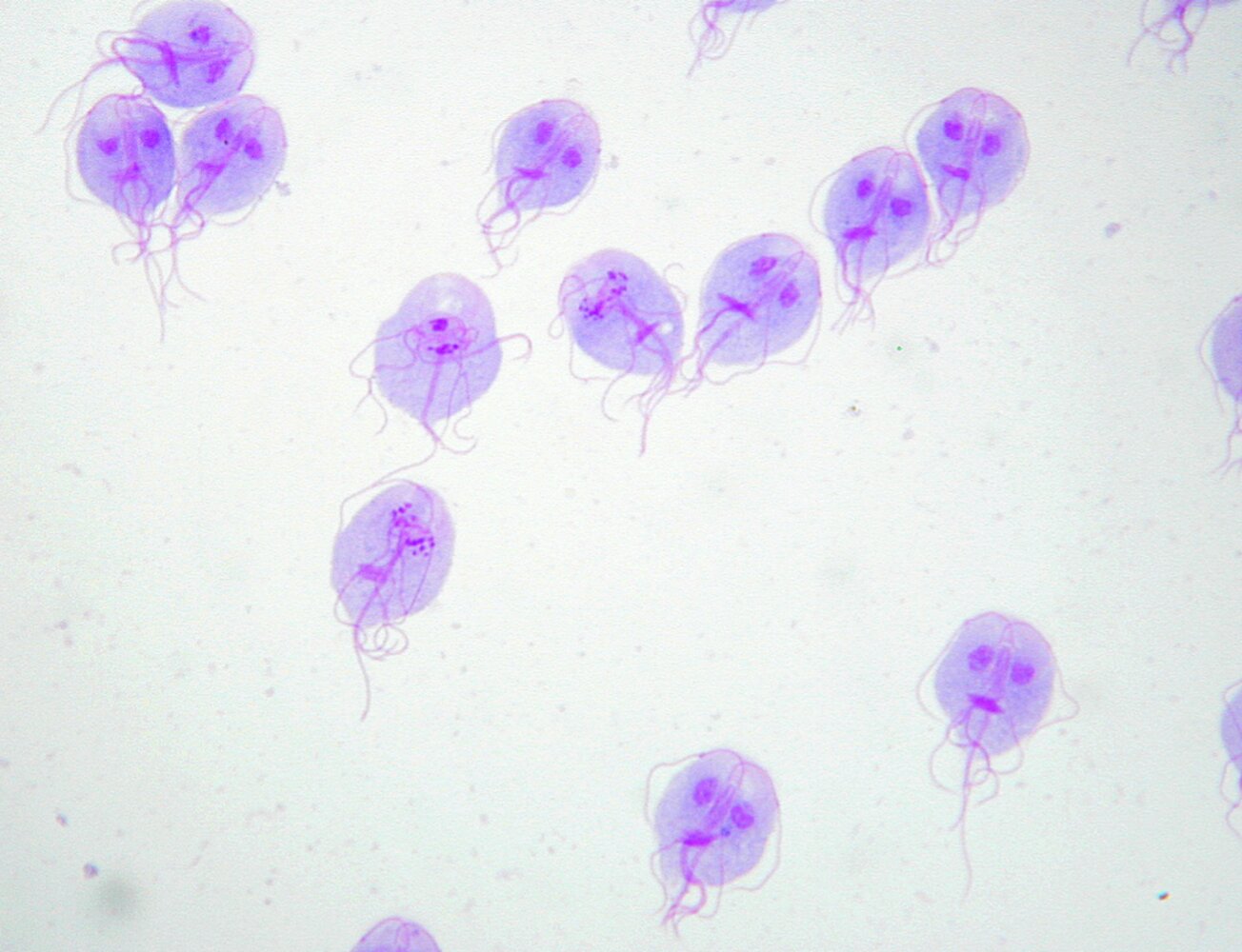
Photomicrograph of a laboratory culture (Giemsa stain; 100x magnification)
Eleven pear-shaped trophozoites, each with four pairs of flagella (black arrows), two nuclei of equal size (green overlay), and one or two median bodies (hatched green overlay), are visible.
These features are characteristic of Giardia lamblia trophozoites.
Source: “Figure 2, in: Giardia and Vilém Dušan Lambl” by Marie Lipoldova, Plos Neglected Tropical Diseases, licensed under CC BY 4.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
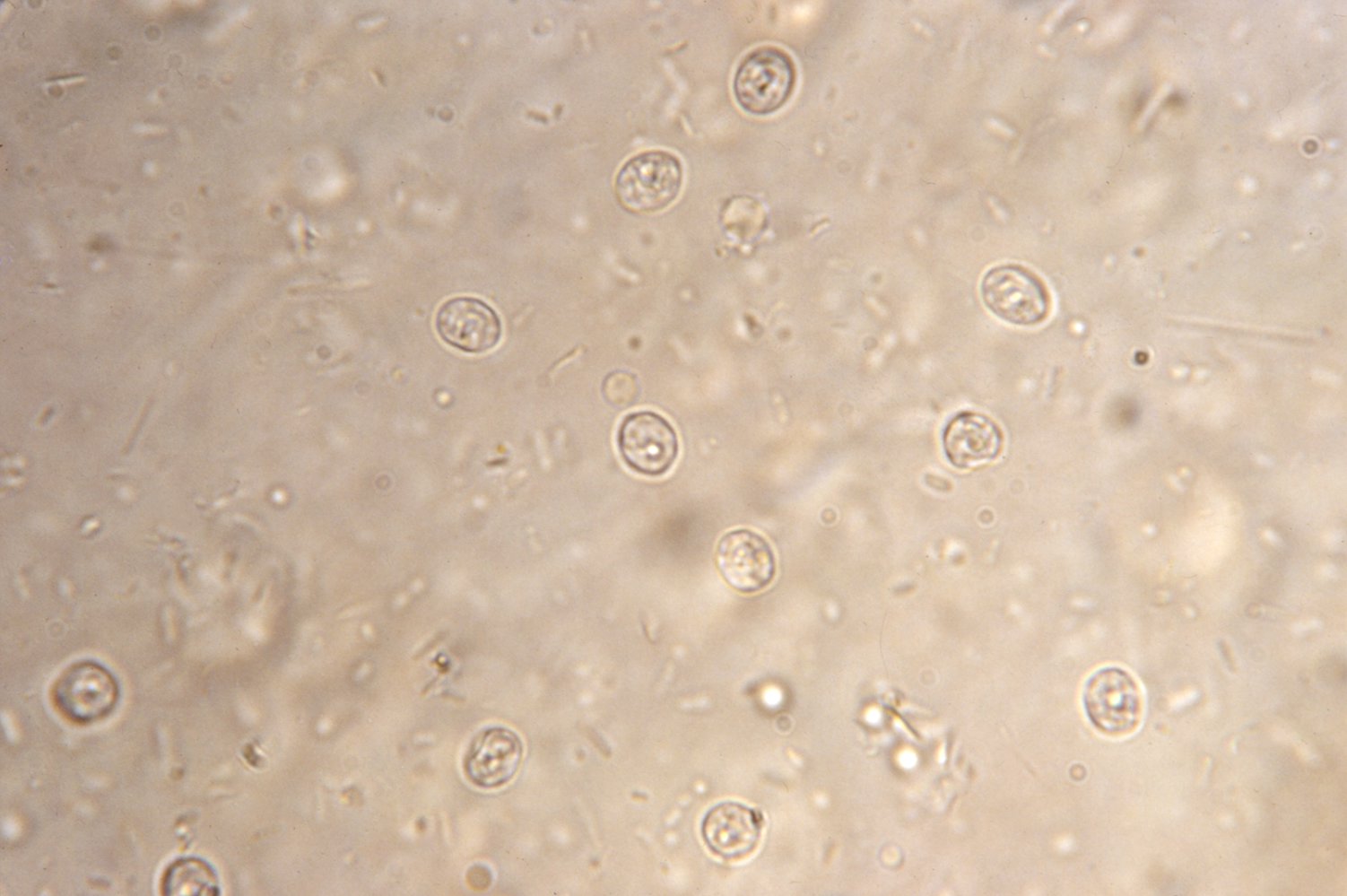
Fecal sample of a patient with cryptosporidiosis
Several round oocysts (red) that contain a large number of sporozoites. Oocysts are highly resistant to environmental factors and disinfectants (also to chlorine, e.g., in drinking water). They are the infective form of the parasite Cryptosporidium parvum.
Source: "ID#: 4384", CDC/ Dr. Peter Drotman, Centers for Disease Control and Prevention (CDC) licensed under Public Domain
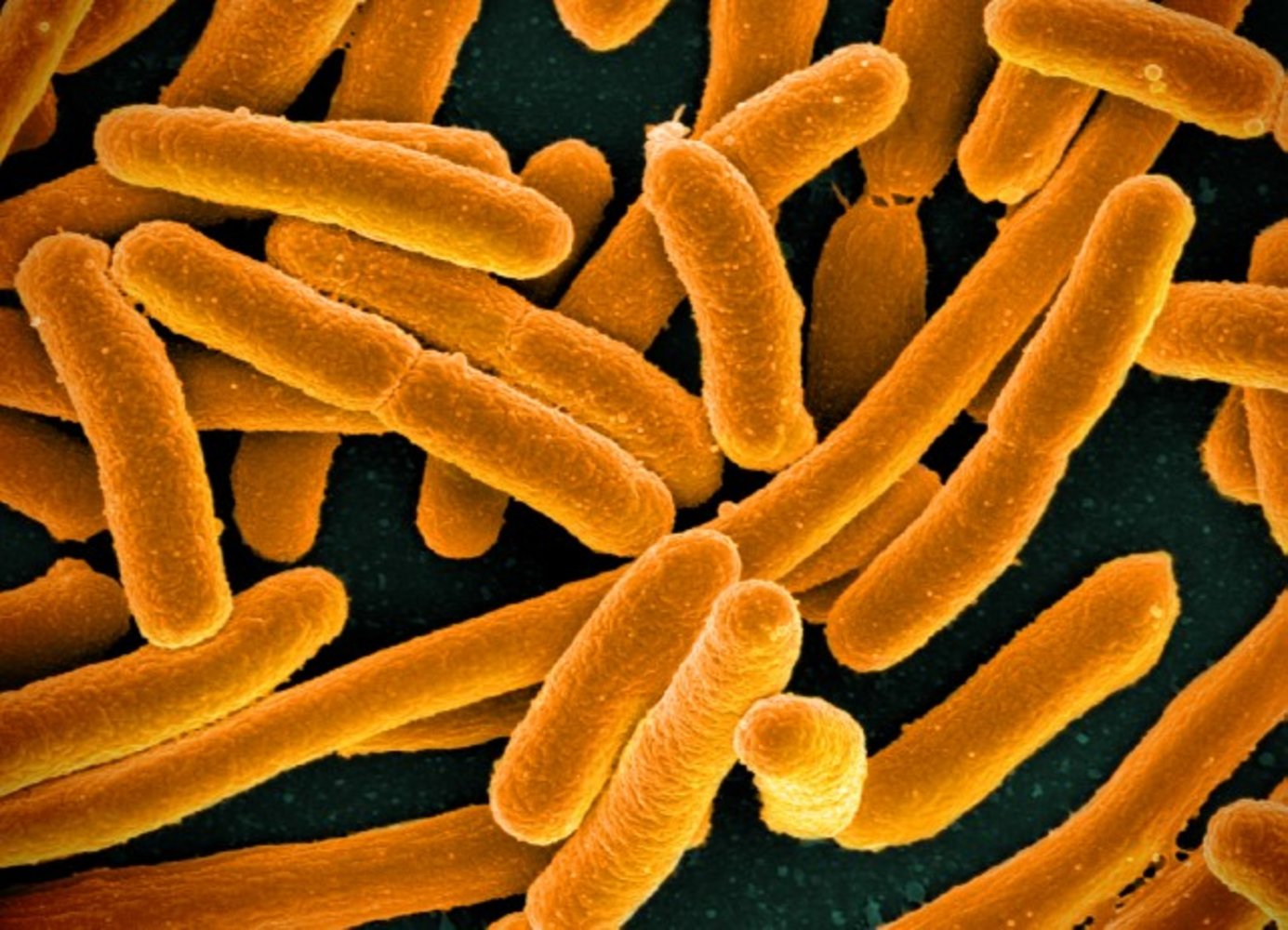
Colorized scanning electron micrograph
There are rod-shaped bacteria with hemispherical caps.
Source: “E. coli Bacteria” by NIAID, Flickr, licensed under CC BY 2.0.
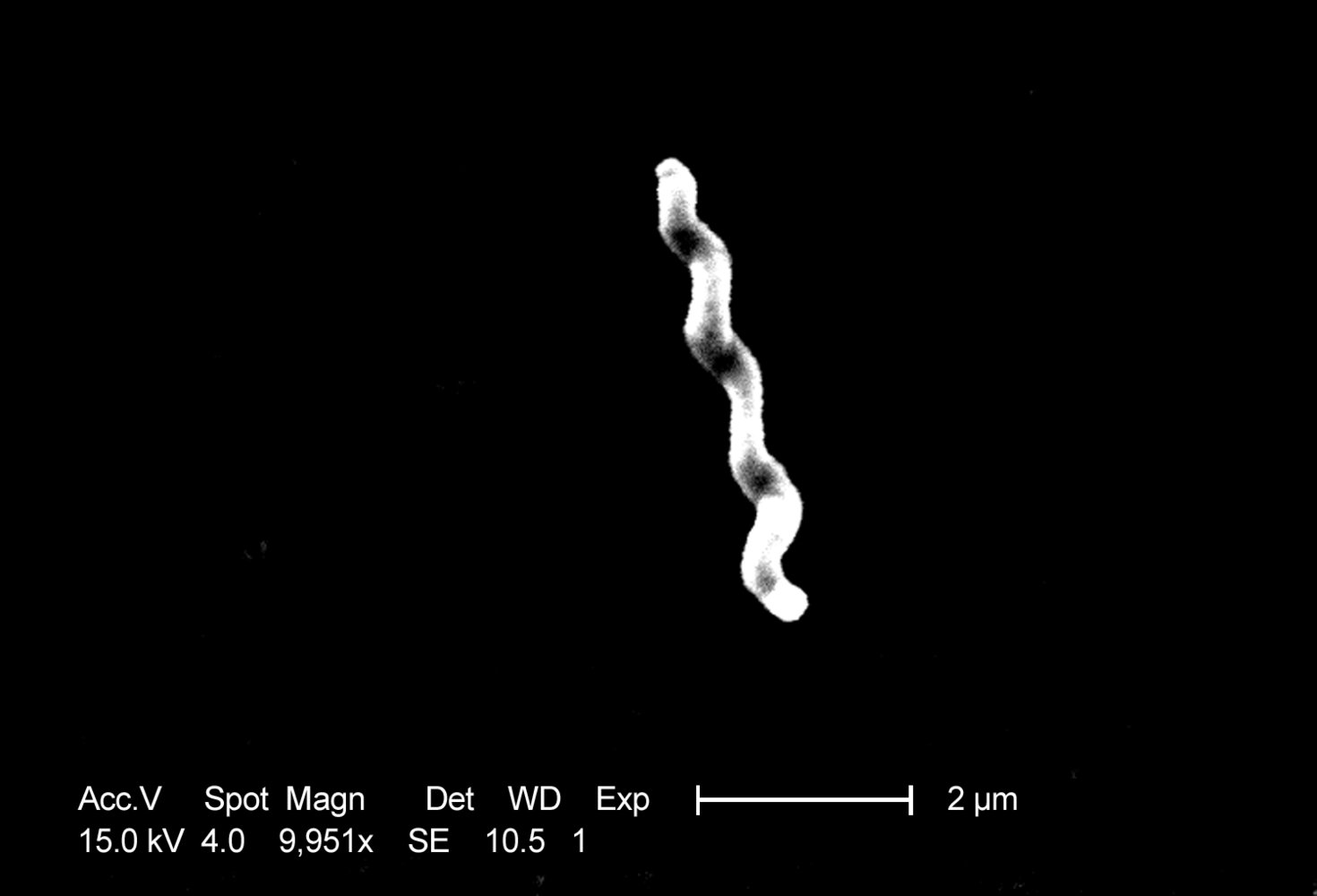
Scanning electron micrograph
C. jejuni is a spirillum bacteria. Contamination with even very small quantities of C. jejuni causes inflammatory gastroenteritis.
Source: "ID#: 5781", CDC/ Dr. Patricia Fields, Dr. Collette Fitzgerald, Janice Carr, Centers for Disease Control and Prevention (CDC) licensed under Public Domain

Colorized scanning electron micrograph
The flagellated, Gram negative rod Salmonella (red) is infecting an immune cell (yellow).
Source: “Salmonella Bacteria” by NIAID, Flickr, licensed under CC BY 2.0.
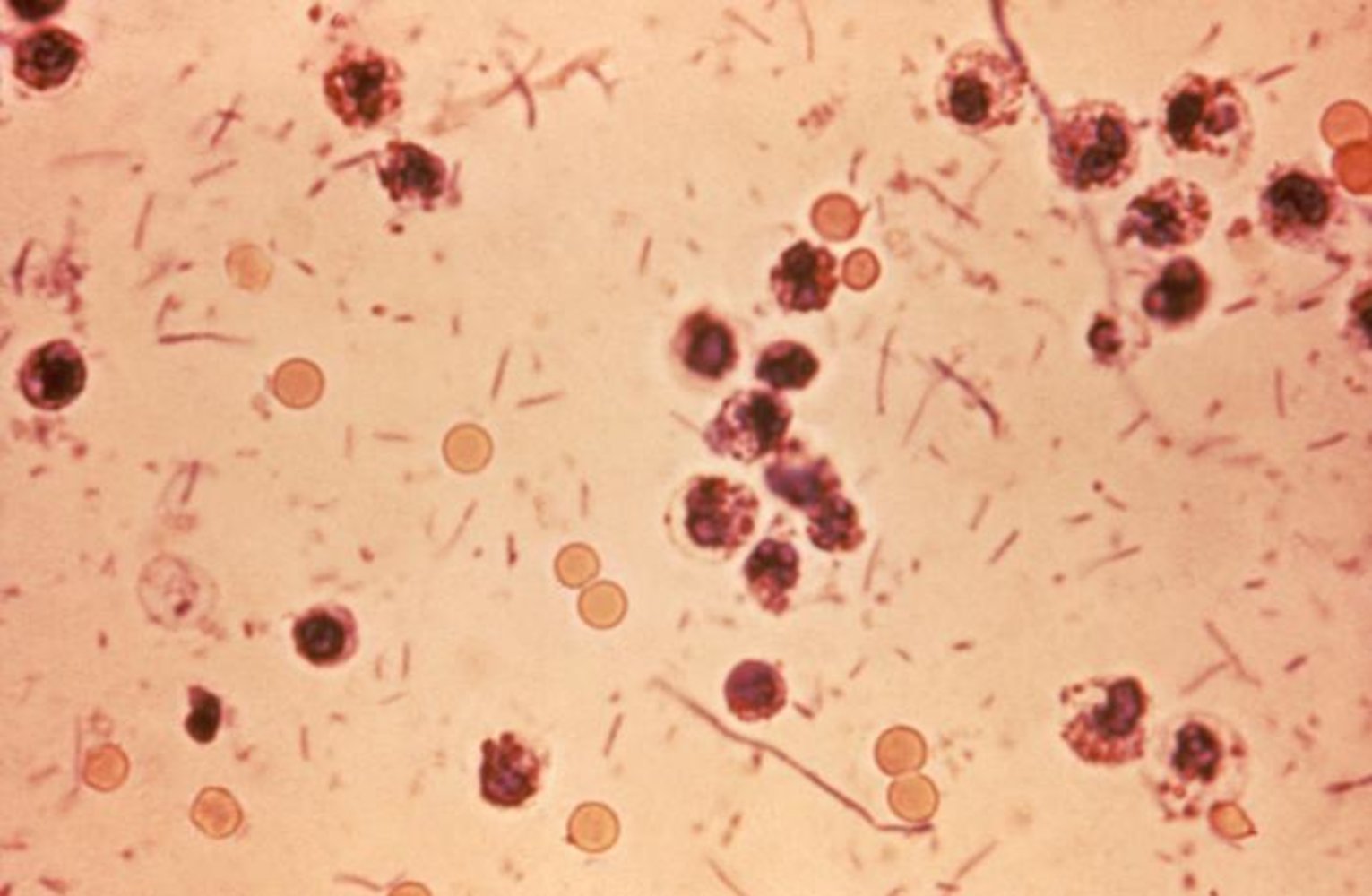
Photomicrograph of a stool sample
Rod-shaped bacteria (examples in blue overlay) that also occasionally form short chains are visible. Erythrocytes (arrowheads indicate examples) and an inflammatory leukocytic exudate (examples in green overlay) can also be seen.
These findings are consistent with Shigella dysentery.
Source: "ID#6659", CDC, Public Health Image Library licensed under Public Domain
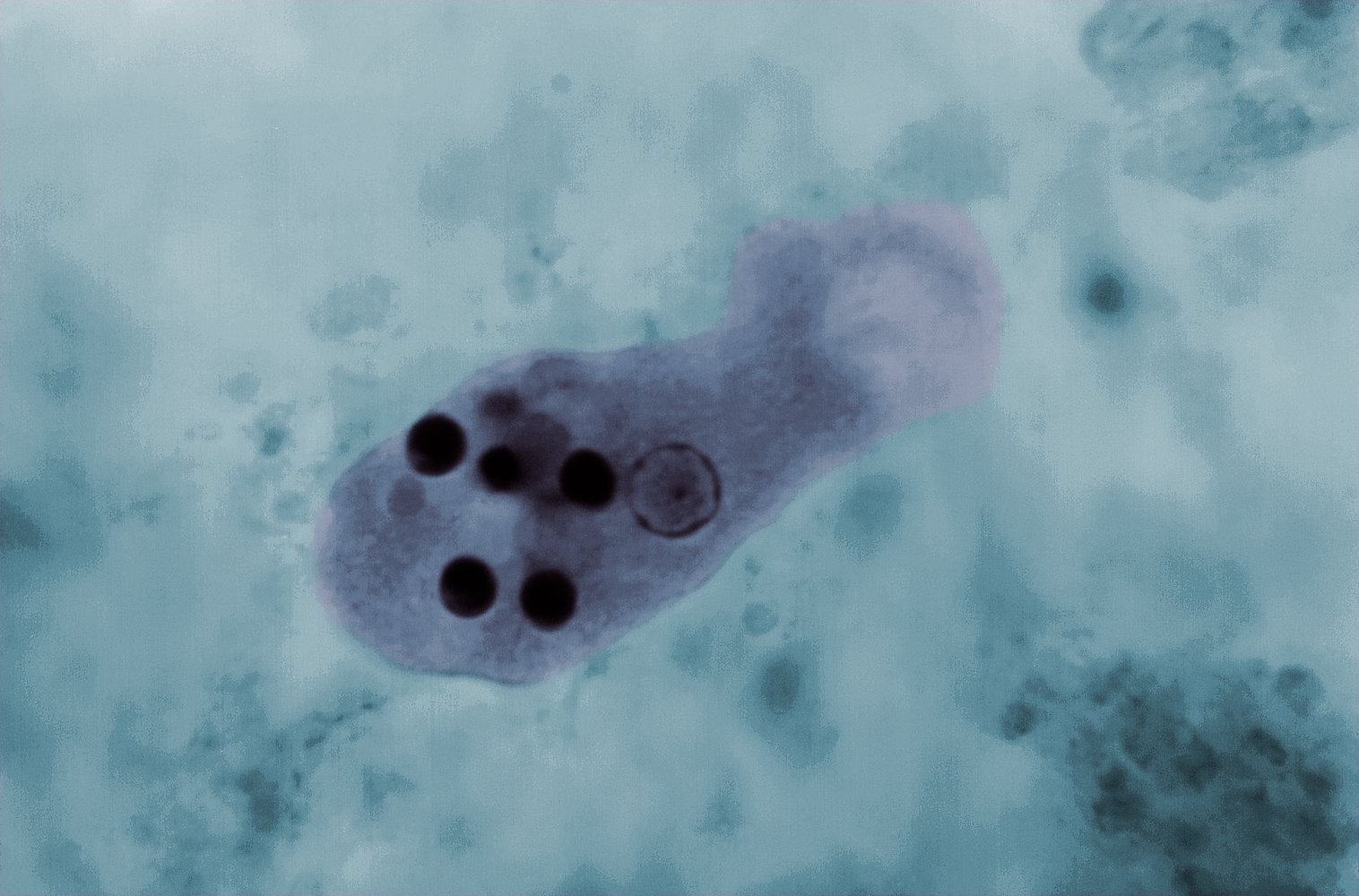
Photomicrograph of a fresh stool mount (trichrome stain; very high magnification)
An Entamoeba histolytica trophozoite with several engulfed erythrocytes (red circles) is visible. The nucleus of E. histolytica has a central karyosome (white overlay), and the chromatin (green circle) is evenly distributed in the periphery.
This appearance is characteristic of E. histolytica infection, indicating active intestinal amebiasis.
Source: "ID#: 14544", CDC/ Dr. Mae Melvin; Dr. Greene, Centers for Disease Control and Prevention (CDC) licensed under Public Domain
Classification
Diarrhea is often classified as watery, fatty, and/or inflammatory to facilitate diagnosis and management. This classification scheme is most relevant for the approach to chronic diarrhea.
| Classification of diarrhea by functional pathology [10][11][12] | |||
|---|---|---|---|
| Pathophysiology | Associated disorders | ||
| Inflammatory diarrhea |
|
|
|
| Fatty diarrhea | Malabsorption |
|
|
| Maldigestion |
|
|
|
| Watery diarrhea | Secretory diarrhea |
|
|
| Osmotic diarrhea |
|
|
|
| Functional diarrheal disorders [10] |
|
|
|
Management
Approach to diarrhea [11]
-
Detailed history and physical examination
- Exclude fecal incontinence and fecal impaction; see “Differential diagnoses of diarrhea.”
- Rule out medication-induced diarrhea and consider factitious diarrhea.
- Classify diarrhea:
- By duration of diarrheal illness: acute, persistent, or chronic
- By clinical presentation: watery, fatty, inflammatory
- Identify any red flags in diarrhea and risk factors for specific causes.
- Review medical and surgical history.
- Supportive care: Start oral hydration (or IV fluids) and offer symptom relief.
- Diagnostics: Obtain only when appropriate.
- Directed therapy: Consider empiric or targeted therapy (e.g., antibiotics) based on clinical presentation and study results.
Though most patients with diarrhea have mild symptoms and can be managed as outpatients, some patients may present with severe and even life-threatening symptoms that require hospitalization.
In older adults, rule out fecal impaction, which can manifest atypically with paradoxical diarrhea (due to decreased rectal sensation) and nonspecific symptoms (e.g., functional decline, delirium). [14]
Antibiotics should only be utilized for specific indications.
Clinical assessment of diarrhea [10][12]
Key features of the disease presentation that facilitate efficient testing and prompt diagnosis include:
-
Duration of diarrheal illness
- Acute diarrhea: duration ≤ 14 days
- Persistent diarrhea: duration 15–30 days
- Chronic diarrhea: duration > 30 days
- Stool characteristics: watery, fatty, or bloody stools
-
Associated symptoms
- Fever
- Abdominal pain and cramping
- Nausea and vomiting in cases of gastroenteritis
- Signs of dehydration
- Chronic cases: malnutrition and, in children, failure to thrive
- Weight loss
- Defecation urgency, tenesmus, and/or nocturnal symptoms
| Characteristic clinical features in diarrhea according to functional pathology | |||
|---|---|---|---|
| Inflammatory diarrhea |
|
||
| Fatty diarrhea |
|
||
| Watery diarrhea | Secretory diarrhea | Loose, watery stools |
|
| Functional diarrheal disorders |
|
||
| Osmotic diarrhea |
|
||
Risk factors for diarrhea
Assess for the presence of risk factors for specific etiologies, including:
- Recent travel : associated with traveler's diarrhea
-
Occupational or recreational exposure
- May be associated with an infectious disease outbreak
- Potential routes of exposure include:
- Ingestion of contaminated food or beverages at a high-risk event (e.g., picnic, restaurant, buffet)
- Daycare (e.g., in a daycare attendee, family member of attendee, or daycare staff member)
- Direct contact with contaminated surfaces or objects
- Direct contact with an infected individual (e.g., shaking hands, sharing food)
- Animal contact
- Recent hospitalization: associated with health care-associated infections (e.g., C. difficile infection)
-
Medication use
- May cause medication-induced diarrhea
- Medications commonly associated with diarrhea include: [15]
- Broad-spectrum antibiotics (especially cephalosporins)
- Antacids and PPIs
- NSAIDs
- Metformin
- Colchicine
- Cholesterol-lowering agents
- Antineoplastic drugs
-
Surgery [16]
- Cholecystectomy [17]
- Bowel resection: may cause short bowel syndrome [18]
- Vagotomy: induces rapid gastric emptying, which may disrupt the protective effect of stomach acid [18]
- Gastric and/or esophageal surgery, e.g., bariatric surgery: may result in fat malabsorption, SIBO, or dumping syndrome
- Radiation therapy: may cause secondary enterocolitis [16]
More than 700 medications can cause diarrhea and, therefore, the introduction of a new medication within 6–8 weeks of the onset of diarrhea should be considered as a potential cause. [15]
Chronic diarrhea is common after bariatric surgery. [19][20]
Red flags in diarrhea [21][22][23][24]
-
Acute or persistent diarrhea
- Symptoms of inflammatory diarrhea (dysentery)
- Systemic symptoms, e.g., fever, hypotension
- Severe dehydration
- Bloody stools
- Severe abdominal pain
- Patient characteristics that suggest an increased risk of severe disease
- Chronic illness or immunocompromise
- Age > 65 years
- Recent antibiotic use
- > 48 hours duration without improvement
- Symptoms of inflammatory diarrhea (dysentery)
-
Chronic diarrhea
- Hypoalbuminemia
- Bloody stools
- Symptoms wake the patient from sleep
- Unintended weight loss
- Family history of GI cancer
- Symptom onset after 50 years of age
Diagnostics
General principles [10][12][22][25]
-
Acute diarrhea
- Testing is not required in the majority of cases.
- Indications for testing include the presence of red flags in diarrhea and risk factors for specific etiologies.
- Persistent diarrhea: Testing is usually limited to stool studies for infectious gastroenteritis.
-
Chronic diarrhea
- Testing is initially broad with advanced follow-up testing as indicated. [21][25]
- Repeat stool testing for infectious gastroenteritis.
Diagnostic testing is seldom indicated in acute diarrhea in the absence of red flag symptoms.
Testing for diarrhea
For specific indications for testing, see the respective subsections below on acute, persistent, and chronic diarrhea.
-
Blood tests
- CBC: To evaluate for anemia, leukocytosis, and/or leukopenia
- CMP: Assessment of laboratory findings in dehydration (e.g., electrolyte abnormalities, AKI) and/or liver disease
- CRP, ESR: Markers of inflammation
- Blood cultures: Identification of bacteremia
- Blood gases: Assessment of acid-base status
- Celiac disease serology: Initial testing for celiac disease
-
Breath tests [26]
- Hydrogen breath test (e.g., glucose hydrogen breath test, lactose hydrogen breath test): Diagnosis of SIBO and carbohydrate intolerance
- C-D-xylose breath test: Diagnosis of intestinal malabsorption and SIBO
- CT abdomen or MRI abdomen: Identification of inflammation, structural disease, and/or ischemia [12]
-
Endoscopic studies [12][18]
- Upper endoscopy or enteroscopy with biopsy (± aspiration): Diagnosis of mucosal disease (e.g., celiac disease), infection, or malignancy in the small intestine
- Colonoscopy with biopsies: Diagnosis of inflammatory disease, infection, or malignancy
Endoscopic studies have limited diagnostic value in acute diarrhea but are commonly needed for the workup of chronic diarrhea to evaluate for the presence of inflammatory or neoplastic diseases. Their utility in persistent diarrhea is uncertain.
Stool diagnostic studies
- Stool culture: can be indicated if red flags in diarrhea are present (e.g., suspected invasive bacterial enteritis)
- Stool tests for CDI: if C. difficile infection is suspected
| Stool diagnostic studies in diarrhea | ||
|---|---|---|
| Suspected etiology | Test | Purpose |
| Infectious diseases | Stool culture | Identification of infectious agents (e.g., in bacterial gastroenteritis) |
| Stool microscopy | Visualization of ova or parasites in the stool | |
| Culture-independent methods, e.g., multiplex molecular diagnostic panel for diarrhea (PCR) | Identification of infectious agents in bacterial, viral, and protozoal gastroenteritis [25] | |
| Quantitative culture of small intestinal aspirate | Used to diagnose SIBO (gold standard test for bacterial overgrowth) | |
| Stool tests for C. difficile infection (e.g., toxin test) | Identification of C. difficile infection | |
| Inflammation | Stool microscopy | Visualization of fecal leukocytes |
| Fecal occult blood test (FOBT) | To screen for malignancy and mucosal inflammation | |
| FIT DNA test | To screen for colonic cancer and adenomatous polyps | |
| Fecal calprotectin and lactoferrin | Markers of inflammatory bowel disease (IBD) | |
| Malabsorption | Sudan stain | Qualitative test for steatorrhea |
| 72-hour quantitative fecal fat estimation | Quantitative test for steatorrhea | |
| Fecal elastase-1 | Confirmation of steatorrhea due to exocrine pancreatic insufficiency | |
| Stool electrolytes (e.g., Na+, K+) | Used to calculate stool osmotic gap | |
| Stool pH | Identification of carbohydrate malabsorption | |
-
Stool osmotic gap [11][16][18]
- An equation used in patients with watery diarrhea to differentiate between osmotic, secretory, and functional diarrhea
- Calculation: 290 - [2 × (stool sodium + stool potassium)]
- Normal stool osmotic gap: 50–100 mOsm/kg
| Low stool osmotic gap | High stool osmotic gap | |
|---|---|---|
| Osmotic gap |
|
|
| Interpretation |
|
|
| Example causes |
|
|
The loss of bicarbonate-rich fluid in severe diarrhea may cause nonanion gap metabolic acidosis.
Supportive care
Dehydration and hypovolemia [21]
Therapy is guided by clinical features of dehydration and hypovolemia and laboratory findings in dehydration and hypovolemia.
- Mild to moderate dehydration: Start oral rehydration therapy, e.g., use oral rehydration solution. [21]
-
Severe cases
- Start IV fluid resuscitation (e.g., with normal saline) and monitor hemodynamic parameters.
- Consider hospitalization.
Acute diarrhea is usually a self-limited viral infection and management primarily supportive.
Early rehydration is especially important in children.
Antidiarrheal agents [16][25]
-
Bismuth subsalicylate [25]
- Converts to bismuth and salicylic acid in the GI tract
- Has antisecretory, antimicrobial, and antiinflammatory effects
- Can be used in bacterial diarrhea
-
Loperamide ; [25][27][28]
- Opioid receptor agonist that increases intestinal transit time
- Best initial treatment for chemotherapy-induced diarrhea
- Cautions
- Should not be used for > 48 hours without reevaluation of the patient
- Should be avoided if the patient is febrile or has bloody stools (dysenteric diarrhea)
-
Racecadotril (not available in the US) [16][29]
- Enkephalinase inhibitor that reduces the hypersecretion of electrolytes and water into the intestinal lumen
- Appears to be well-tolerated and effective in bacterial diarrhea
Loperamide should be avoided in patients with suspected invasive diarrhea with inflammatory features, as it reduces intestinal motility, which consequently increases the risk of bacterial colonization and invasion. [30]
Acute or persistent diarrhea (≤ 30 days)
Approach to acute diarrhea (≤ 14 days) [21][22][25][28]
The management of acute diarrhea is primarily supportive, as the disease is usually a self-limited viral infection. Further management focuses on determining whether diagnostic testing and directed therapy are needed (e.g., antibiotic therapy for bacterial gastroenteritis). [22]
- Start hydration and offer symptom relief; see “Supportive care.”
- Determine whether the diarrhea is inflammatory (dysentery) or noninflammatory.
- Reserve stool diagnostic testing for pathogen identification (stool cultures with or without culture-independent methods) for specific scenarios [25]
- The presence of red flags in diarrhea (e.g., inflammatory diarrhea, sepsis)
- The presence of risk factors for specific infectious diseases (e.g., risk factors for C. difficile infection)
- High risk of infecting others (e.g., daycare workers, food handlers, current known or suspected disease outbreaks)
- If the results would alter management
- Consider empiric antibiotics for bacterial gastroenteritis after stool samples have been obtained. [28]
- Start targeted treatment based on the results; see also “Infectious gastroenteritis.”
If symptoms of an acute abdomen are present, consider an urgent CT abdomen to identify ischemic, hemorrhagic, obstructive, and/or inflammatory diseases. [28]
When indicated, stool studies in patients with acute diarrhea should include tests that can detect the presence of Salmonella, Shigella, Campylobacter, Yersinia, C. difficile infection, and Shiga toxin-producing E. coli. [31]
Noninflammatory diarrhea (watery diarrhea) [21][25][31]
-
Mild symptoms (e.g., daily activities of life are not affected)
- < 7 days: Diagnostic testing is not recommended.
- ≥ 7 days: Consider stool studies for pathogen identification if the results may alter management, e.g., initiation of targeted therapy.
-
Moderate to severe symptoms (e.g., daily activities of life are affected)
- For traveler's diarrhea, start empiric antibiotics. [31]
- < 72 hours: symptom control (e.g., loperamide); no diagnostic testing recommended
- ≥ 72 hours: Obtain stool studies for pathogen identification and targeted therapy.
- Severe symptoms, fever, or patients at risk for severe disease: Obtain stool studies for pathogen identification and targeted therapy.
Inflammatory diarrhea (dysentery) [28]
- No or low-grade fever: stool cultures or multiplex molecular diagnostic panel for diarrhea (PCR)
-
Severe illness with fever
- Obtain blood tests (e.g., CBC, CMP, inflammatory markers, and blood cultures) and stool studies for pathogen identification and targeted therapy.
- Consider empiric antibiotics for bacterial gastroenteritis. [31]
Approach to persistent diarrhea (15–30 days) [28][32]
- Review associated symptoms, history, and stool appearance.
- Obtain stool studies for pathogen identification (including parasites) in all patients.
- Avoid routine blood tests, imaging, and endoscopy in patients with a negative stool workup and no red flag symptoms.
- Offer empiric antibiotics to patients with suspected traveler's diarrhea.
- Start targeted treatment based on diagnostic results; see also “Infectious gastroenteritis.”
In patients with prominent abdominal pain and/or bloody diarrhea, evaluate for ischemic colitis, ulcerative colitis, and Crohn disease if stool testing does not indicate an infectious etiology.
Persistent diarrhea has a broader differential diagnosis than acute diarrhea. Parasitic infection (e.g., giardiasis), recurrent bacterial infection (e.g., C. difficile infection), and noninfectious causes (e.g., IBS-D) must be considered. [32]
Etiology of acute and persistent diarrhea [10][11][15][22]
| Etiology of acute and persistent diarrhea | |
|---|---|
| Viral [21] |
|
| Bacterial |
|
| Parasitic |
|
| Food poisoning |
|
| Medications |
|
| Other |
|
Chronic diarrhea (> 30 days)
Approach to chronic diarrhea
The differential diagnosis of chronic diarrhea is extensive. A systematic approach with efficient use of testing is needed to arrive at a diagnosis quickly. [10][12][33]
- Provide general supportive care.
- Assess for a possible health care-related etiology: e.g., medication-induced diarrhea
- Consider factitious diarrhea. [11]
- Order initial diagnostics for chronic diarrhea.
- Consider a preliminary diagnosis of IBS-D if all of the following criteria are met: [18]
- Initial tests are normal.
- No red flags are present.
- Rome IV criteria for IBS are met.
- Consider further investigations: e.g., additional advanced tests, therapeutic trials
- Start directed therapy once a likely etiology of chronic diarrhea has been identified.
Chronic diarrhea can be classified as inflammatory, fatty, or watery. Grouping patients into broad categories based on clinical features and basic laboratory findings narrows the differential diagnosis and facilitates efficient advanced testing. [18]
IBS-D is an intermediate diagnosis; it does not eliminate the possibility of another disease. Evaluation should continue if symptoms persist despite treatment for IBS-D. [12]
Etiology of chronic diarrhea [12]
Chronic diarrhea is commonly classified as watery, fatty, or inflammatory.
| Etiology of chronic diarrhea [12] | ||
|---|---|---|
| Inflammatory |
|
|
| Fatty | Malabsorption |
|
| Maldigestion |
|
|
| Watery | Secretory |
|
| Functional |
|
|
| Osmotic |
|
|
Initial diagnostics for chronic diarrhea [10][12][24][33]
Order initial studies. See also “Testing for diarrhea” in “Diagnostics.”
-
Stool studies
- Repeat stool testing for infectious gastroenteritis.
- Perform fecal leukocyte, calprotectin, and lactoferrin studies and a FOBT.
- Consider further studies to help classify diarrhea: e.g., fecal fat estimation, stool osmotic gap, stool pH [12][16]
- Blood tests: Obtain CRP levels , CBC, CMP, and diagnostic studies for anemia. [12]
-
Imaging studies [12]
- Use imaging studies to evaluate red flags in diarrhea and consider initially to rule out structural disease.
- Preferred modality: CT abdomen or MRI abdomen with enterography
Always test for Giardia infection in chronic diarrhea. [24]
Subsequent evaluation [10][11]
Perform guided diagnostics based on characteristic clinical features in diarrhea and the results of initial diagnostic testing.
| Diagnostic workup of patients with chronic diarrhea | |||
|---|---|---|---|
| Classification | Initial results | Further diagnostics | |
| Inflammatory diarrhea |
|
|
|
| Fatty diarrhea [10][12][16] |
|
|
|
| Watery diarrhea [11] | Secretory diarrhea or functional diarrheal disorders |
|
|
| Osmotic diarrhea |
|
|
|
In watery diarrhea, the stool osmotic gap differentiates osmotic from secretory diarrhea. In osmotic watery diarrhea, a stool pH < 6 suggests carbohydrate malabsorption.
Endoscopic studies with mucosal biopsies are required to diagnose inflammatory diarrhea in patients with chronic diarrhea.
Therapeutic trials [10][11][18][24]
-
Indications
- Consider if a diagnosis has not been established after a thorough evaluation.
- Consider if diagnostic tests for specific etiologies are not available.
-
Examples of empiric therapies for specific causes [18]
- Elimination diets: e.g., lactose-free diet for lactose intolerance
- Empiric antibiotics: e.g., rifaximin for suspected SIBO [34]
- Cholestyramine for suspected bile acid malabsorption [35]
- Oral steroids for microscopic colitis
- Pancreatic enzyme replacement therapy for exocrine pancreatic insufficiency
Differential diagnoses
-
Fecal incontinence
- Involuntary release of stool, usually without a sensation of urgency
- May indicate abnormal neuromuscular function or anorectal structure
- Diagnosis is made based on history and a digital rectal examination.
-
Impaction with fecal overflow (paradoxical diarrhea)
- Rectal distention relaxes the internal anal sphincter, allowing leakage of stool.
- Diagnosis is made based on a digital rectal examination.
-
Pseudodiarrhea
- Frequent passage of small amounts of stool
- Usually accompanied by fecal urgency or the feeling of incomplete emptying of the rectum
- Often accompanies IBS and proctitis
References:[11][22][23]
The differential diagnoses listed here are not exhaustive.
Subtypes and variants
Traveler's diarrhea [36][37]
- Definition: ≥ 3 unformed stools with at least one additional enteric symptom occurring after recent travel
-
Epidemiology
- The highest rates occur after travel to Africa and South, Central, and West Asia.
- Approximately 25% of all travelers develop traveler's diarrhea.
-
Etiology
- Enterotoxigenic E. coli (ETEC) is the most common cause of traveler's diarrhea globally.
- Campylobacter jejuni is the most common cause in Southeast Asia.
- Other pathogens
- Bacterial: Shigella spp., Salmonella spp., other E. coli strains (e.g., EAEC)
- Viral: norovirus, rotavirus, astrovirus
- Protozoal: Giardia duodenalis, E. histolytica
- Clinical features: exudative-inflammatory or secretory diarrhea, abdominal cramping, abdominal pain
-
Antibiotics for traveler's diarrhea: Reserve for moderate to severe illness. [25][32][36]
- For most destinations: ciprofloxacin (off label) OR rifaximin [36]
- For travelers to South or Southeast Asia: azithromycin (off label) [36]
-
Supportive care [25]
- Treatment for dehydration (e.g., oral rehydration solution)
- Bismuth subsalicylate for patients with mild to moderate illness
- Loperamide for patients receiving antibiotic therapy (can reduce the duration of illness)
- See “Antidiarrheal agents” for dosages.
-
Postinfectious sequelae
- Postinfectious IBS: may occur in 3–20% of patients
- Reactive arthritis: may last months to years
- Guillain-Barre syndrome: may develop 1–4 weeks after infection (most commonly after Campylobacter infection)
Antibiotic treatment is not recommended in patients with mild traveler's diarrhea.
Bismuth subsalicylate is an antidiarrheal agent used to treat traveler's diarrhea (caused by enterotoxigenic Escherichia coli).
Pharmacological prophylaxis for traveler's diarrhea [25][36]
Consider for travelers to high-risk areas (under specialist guidance); options include:
-
Bismuth subsalicylate (off label) [25][36][38]
- Consider for travelers with no contraindications for use.
- Should be taken with meals and at bedtime
-
Antibiotic prophylaxis (generally discouraged) :
- Consider short-term administration in travelers who are at high-risk for developing serious complications.
- Agents include fluoroquinolones, azithromycin, and rifaximin.
- Probiotics, prebiotics, and synbiotics are not recommended.
Factitious diarrhea [11]
- Definition: self-induced diarrhea, usually due to laxative abuse (often occurs in individuals with factitious disorders), or dilution of stools with solutions
-
Epidemiology
- Most prevalent in women
- Patients are usually health care professionals.
- History of multiple hospital admissions
- Clinical features: chronic diarrhea without an identifiable cause
-
Diagnostics
- Laboratory tests: metabolic acidosis , metabolic alkalosis , hypokalemia, hypermagnesemia
- Stool osmolarity
- < 290 mOsm/L: indicates dilution of the stool with a hypotonic solution
- > 600 mOsm/L: indicates dilution of the stool with a hypertonic solution
- Laxative screen [18]
- Colonoscopy: may show melanosis coli in cases of anthraquinone abuse
-
Treatment
- Correction of electrolyte disturbances and dehydration
- Referral for psychotherapy
Laxative abuse
-
Types of laxative
- Bulking agent: e.g., flaxseed
- Osmotic laxatives: e.g., lactulose, macrogols (polyethylene glycol), magnesium sulfate, sodium sulfate
- Diphenolic laxatives: bisacodyl, sodium picosulfate
- Anthraquinones: e.g., senna, aloe vera, rhubarb
-
Clinical features
- Osmotic diarrhea, meteorism
- Dehydration
- Hypokalemia
-
Melanosis coli: benign hyperpigmentation of the colonic mucosa caused by anthraquinone abuse [39]
- Colonoscopy: patches of dark brown pigmentation interspersed with pale mucosa
- Biopsy: lipofuscin-laden macrophages demonstrated on periodic acid-Schiff staining


Bile acid diarrhea
- Definition: secretory diarrhea with or without steatorrhea due to increased colonic secretion and motility secondary to an increased concentration of bile acids within the colon
- Epidemiology: approx. 1% global prevalence [40]
-
Etiology
- Ileal dysfunction or decreased bile acid reabsorption in the ileum (e.g., due to ileal resection, Crohn disease)
- Postcholecystectomy
- Hepatic overproduction of bile acids
- Biliary-enteric fistula
-
Clinical features
- Bowel frequency and urgency
- Fecal incontinence
- Abdominal cramping, abdominal pain
- Nocturnal fecal urgency
- Bloating, flatulence
-
Management [41]
- First-line: bile-acid sequestrants (e.g., cholestyramine, colestipol)
- Dietary intervention: low-fat diet
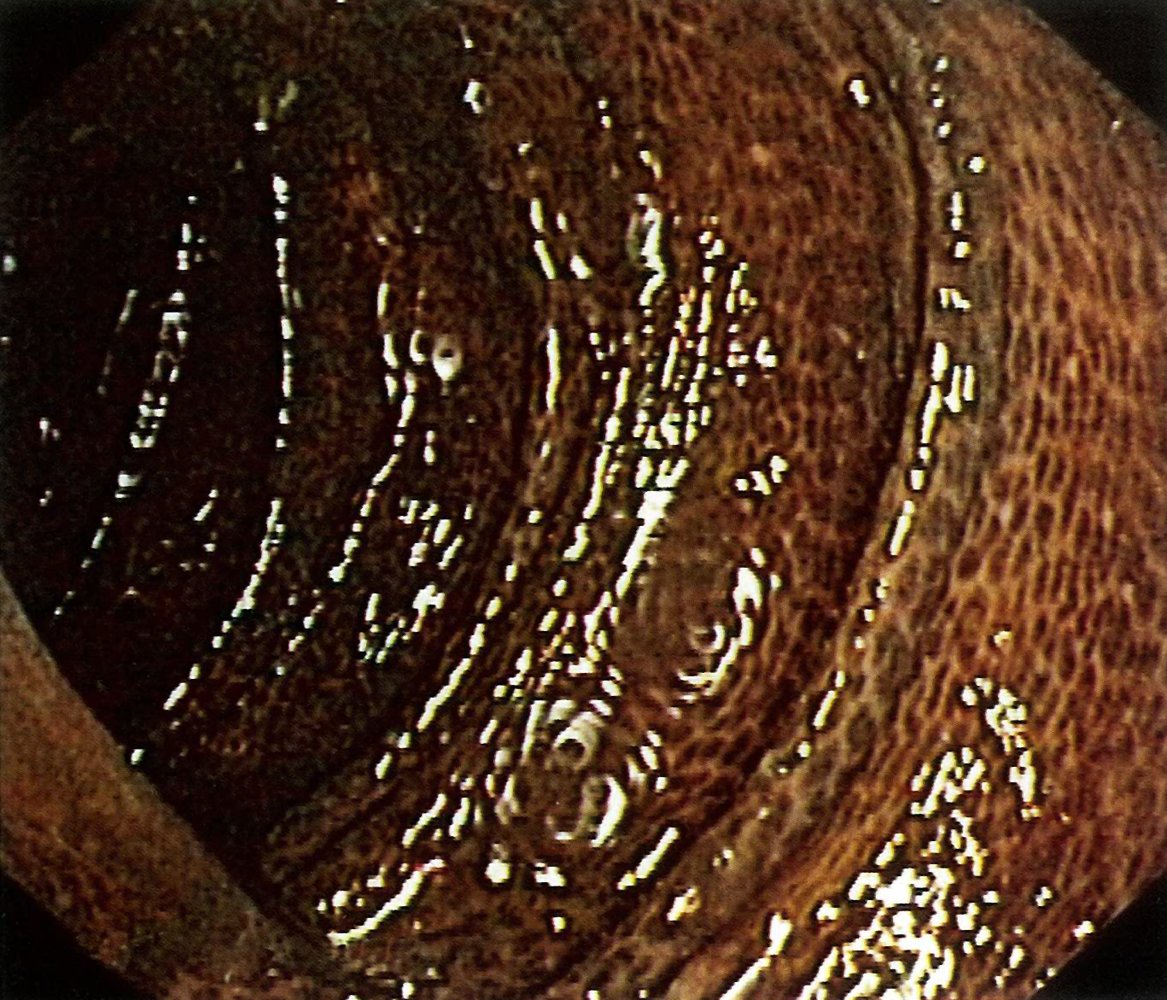
Endoscopic view of the colon in a patient with a history of laxative abuse
The colonic mucosa is lined with a pattern of sharply demarcated, dark brown hyperpigmentations, caused by the deposition of anthraquinone pigments from a plant-based laxative (e.g., senna gylcosides or aloe emodin) in the mucosa. The mucosa's surface texture and the colon's haustral folds are unchanged.
Source: © IMPP
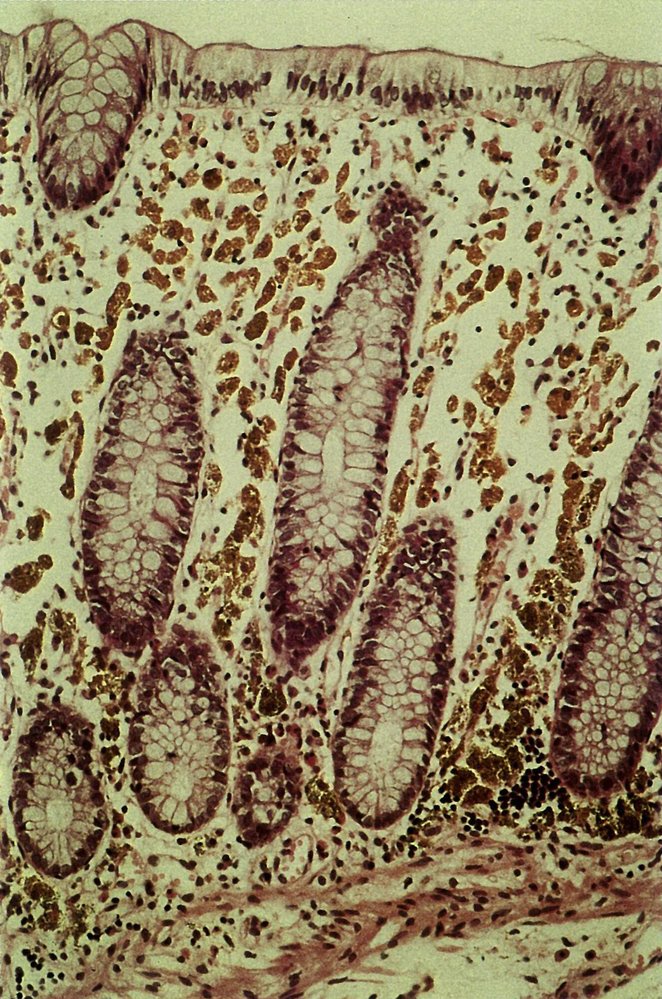
Photomicrograph of a tissue sample from the colonic mucosa (H&E stain)
The mucosa is not inflamed. Brown discoloration of the tissue results from brown deposits of anthraquinone pigments in the lamina propria.
These findings are consistent with chronic laxative abuse.
Source: © IMPP
External Resources
References
- Sweetser S. "Evaluating the Patient With Diarrhea: A Case-Based Approach". Mayo Clinic Proceedings. 87(6). :596-602. (2012)
- Jamshed N, Lee Z-E, Olden KW. "Diagnostic Approach to Chronic Constipation in Adults". Am Fam Physician. 84(3). :299-306. (2011)
- Burgers K, Lindberg B, Bevis ZJ. "Chronic Diarrhea in Adults: Evaluation and Differential Diagnosis.". Am Fam Physician. 101(8). :472-480. (2020)
- Schiller LR. "Evaluation of chronic diarrhea and irritable bowel syndrome with diarrhea in adults in the era of precision medicine". Am J Gastroenterol. 113(5). :660-669. (2018)
- Abraham B, Sellin JH. "Drug-induced diarrhea". Curr Gastroenterol Rep. 9(5). :365-372. (2007)
- Semrad CE. "Approach to the Patient with Diarrhea and Malabsorption". Elsevier. :895-913. (2012). ISBN: 9780323640336
- Farahmandfar MR, Chabok M, Alade M, Bouhelal A, Patel B. "Post Cholecystectomy Diarrhoea—A Systematic Review". Surgical Science. 03(06). :332-338. (2012)
- Schiller LR, Pardi DS, Sellin JH. "Chronic Diarrhea: Diagnosis and Management". Clinical Gastroenterology and Hepatology. 15(2). :182-193.e3. (2017)
- Borbély YM, Osterwalder A, Kröll D, Nett PC, Inglin RA. "Diarrhea after bariatric procedures: Diagnosis and therapy". World Journal of Gastroenterology. 23(26). :4689. (2017)
- Ma IT, Madura JA 2nd. "Gastrointestinal Complications After Bariatric Surgery". Gastroenterol Hepatol. 11(8). :526-35. (2015)
- Barr W, Smith A. "Acute diarrhea in adults". Am Fam Physician. 89(3). :180-189. (2014)
- Jameson JL, Fauci AS, Kasper DL, et al. "Harrison's Principles of Internal Medicine, Twentieth Edition (Vol.1 & Vol.2)". McGraw-Hill Education / Medical. (2018). ISBN: 9781259644030
- Hammer HF. "Management of Chronic Diarrhea in Primary Care: The Gastroenterologists Advice". Digestive Diseases. (2021)
- Smalley W, Falck-Ytter C, Carrasco-Labra A, et al. "AGA Clinical Practice Guidelines on the Laboratory Evaluation of Functional Diarrhea and Diarrhea-Predominant Irritable Bowel Syndrome in Adults (IBS-D)". Gastroenterology. 157(3). :851-854. (2019)
- Camilleri M, Sellin JH, Barrett KE. "Pathophysiology, Evaluation, and Management of Chronic Watery Diarrhea". Gastroenterology. 152(3). :515-532.e2. (2017)
- Pimentel M, Saad RJ, Long MD, Rao SSC. "ACG Clinical Guideline: Small Intestinal Bacterial Overgrowth". Am J Gastroenterol. 115(2). :165-178. (2020)
- Vijayvargiya P, Camilleri M, Shin A, Saenger A. "Methods for Diagnosis of Bile Acid Malabsorption in Clinical Practice". Clinical Gastroenterology and Hepatology. 11(10). :1232-1239. (2013)
- Riddle MS, DuPont HL, Connor BA. "ACG Clinical Guideline: Diagnosis, Treatment, and Prevention of Acute Diarrheal Infections in Adults". Am J Gastroenterol. 111(5). :602-622. (2016)
- DuPont HL. "Acute Infectious Diarrhea in Immunocompetent Adults". N Engl J Med. 370(16). :1532-1540. (2014)
- Shane AL, Mody RK, Crump JA, et al. "2017 Infectious Diseases Society of America Clinical Practice Guidelines for the Diagnosis and Management of Infectious Diarrhea". Clin Infect Dis. 65(12). :e45-e80. (2017)
- DuPont HL. "Persistent Diarrhea". JAMA. 315(24). :2712. (2016)
- Qiu FZ, Shen XX, Li GX, et al. "Adenovirus associated with acute diarrhea: a case-control study.". BMC Infect Dis. 18(1). :450. (2018)
- "Histamine Toxicity". https://www.aaaai.org/conditions-and-treatments/related-conditions/histamine-toxicity. [2017-03-01]
- "Overview of Food Poisoning". http://www.msdmanuals.com/home/injuries-and-poisoning/poisoning/overview-of-food-poisoning. [2017-03-01]
- Juckett G, Trivedi R. "Evaluation of Chronic Diarrhea". Am Fam Physician. 84(10). :1119-1126. (2011)
- DuPont HL. "Adverse Effect of Lomotil Therapy in Shigellosis". JAMA. 226(13). :1525. (1973)
- Singh N, Narayan S. "Racecadotril : A Novel Antidiarrheal". Med J Armed Forces India. 64(4). :361-2. (2008)
- Benjamin I. "Andreoli and Carpenter's Cecil Essentials of Medicine". Elsevier Health Sciences. (2016). ISBN: 9781437718997
- "Diarrhoeal disease". http://www.who.int/mediacentre/factsheets/fs330/en/. [2013-04-01]
- Schiller LR, Pardi DS, Spiller R, et al. "Gastro 2013 APDW/WCOG Shanghai Working Party Report: Chronic diarrhea: Definition, classification, diagnosis". J Gastroenterol Hepatol. 29(1). :6-25. (2013)
- Dellon ES, Ringel Y. "Treatment of functional diarrhea". Curr Treat Options Gastroenterol. 9(4). :331-342. (2006)
- "Travelers' Diarrhea". https://web.archive.org/web/20240929175416/https://wwwnc.cdc.gov/travel/yellowbook/2024/preparing/travelers-diarrhea. [2019-11-22]
- Giddings SL, Stevens AM, Leung DT. "Traveler’s Diarrhea". Med Clin North Am. 100(2). :317-330. (2016)
- Herbert L. DuPont, Charles D. Ericsson, P. C. Johnson, F. Javier de la Cabada. "Use of Bismuth Subsalicylate for the Prevention of Travelers' Diarrhea". Clinical Infectious Diseases. 12(Supplement_1). :S64-S67. (1990)
- Freeman HJ. "“Melanosis” in the small and large intestine". World J Gastroenterol. 14(27). :4296. (2008)
- Walters JR, Pattni SS. "Managing bile acid diarrhoea.". Therap Adv Gastroenterol.. 3(6). :349-57. (2010)
- Farrugia A, Arasaradnam R. "Bile acid diarrhoea: pathophysiology, diagnosis and management". Frontline Gastroenterology. 12(6). :500-507. (2020)
- "Guidelines for the Prevention and Treatment of Opportunistic Infections in Adults and Adolescents with HIV". https://web.archive.org/web/20260126024001/https://clinicalinfo.hiv.gov/sites/default/files/guidelines/documents/adult-adolescent-oi/guidelines-adult-adolescent-oi.pdf. [2025-07-14]
- Kasper DL, Fauci AS, Hauser SL, et al. "Harrison's Principles of Internal Medicine". McGraw-Hill Education. (2015). ISBN: 9780071802161
- Walker HK, Hall WD, Hurst WJ, Silverman ME, Morrison G. "Clinical Methods: The History, Physical, and Laboratory Examinations". Butterworths. (1990). ISBN: 040990077x
- Saad RJ, Chey WD. "Breath Testing for Small Intestinal Bacterial Overgrowth: Maximizing Test Accuracy". Clin Gastroenterol Hepatol. 12(12). :1964-1972. (2014)