Summary
Diphtheria is an infectious disease caused by Corynebacterium diphtheriae, which is usually transmitted via respiratory droplets. The clinical features of diphtheria are caused by a toxin produced by C. diphtheriae after it colonizes the upper respiratory tract. Patients initially present with fever, malaise, and sore throat. Within a few days, a grayish-white pseudomembrane develops over the tonsils, posterior pharyngeal wall, and/or larynx. Other manifestations include cervical lymphadenopathy, soft tissue swelling of the neck, stridor, and/or difficulty breathing as a result of partial airway obstruction. Systemic absorption of the toxin can result in myocarditis, acute tubular necrosis, and/or polyneuropathy. Even before culture reports come back positive, patients should be promptly treated with penicillin and antitoxins, as untreated diphtheria is associated with a high mortality rate. In tropical countries, there is also a cutaneous form of diphtheria without systemic manifestations. Cutaneous diphtheria manifests as a scaly erythematous rash and/or a deep punched-out ulcer following direct entry of C. diphtheriae into the skin. Since the introduction of routine immunization against diphtheria in the 1920s, the incidence of the disease has decreased dramatically in the US.
Epidemiology
- Incidence: 0–2 cases/year [1]
- Most cases occur in patients 20 years of age or older.
Epidemiological data refers to the US, unless otherwise specified.
Etiology
-
Pathogen: Corynebacterium diphtheriae
- A gram-positive, nonsporulating, club-shaped bacillus
- Contains metachromatic granules; (volutin granules; stain red with a blue dye)
-
Route of infection
- Droplet transmission
- Less commonly through direct or indirect contact with open lesions
- Infectious period: variable

References:[2]
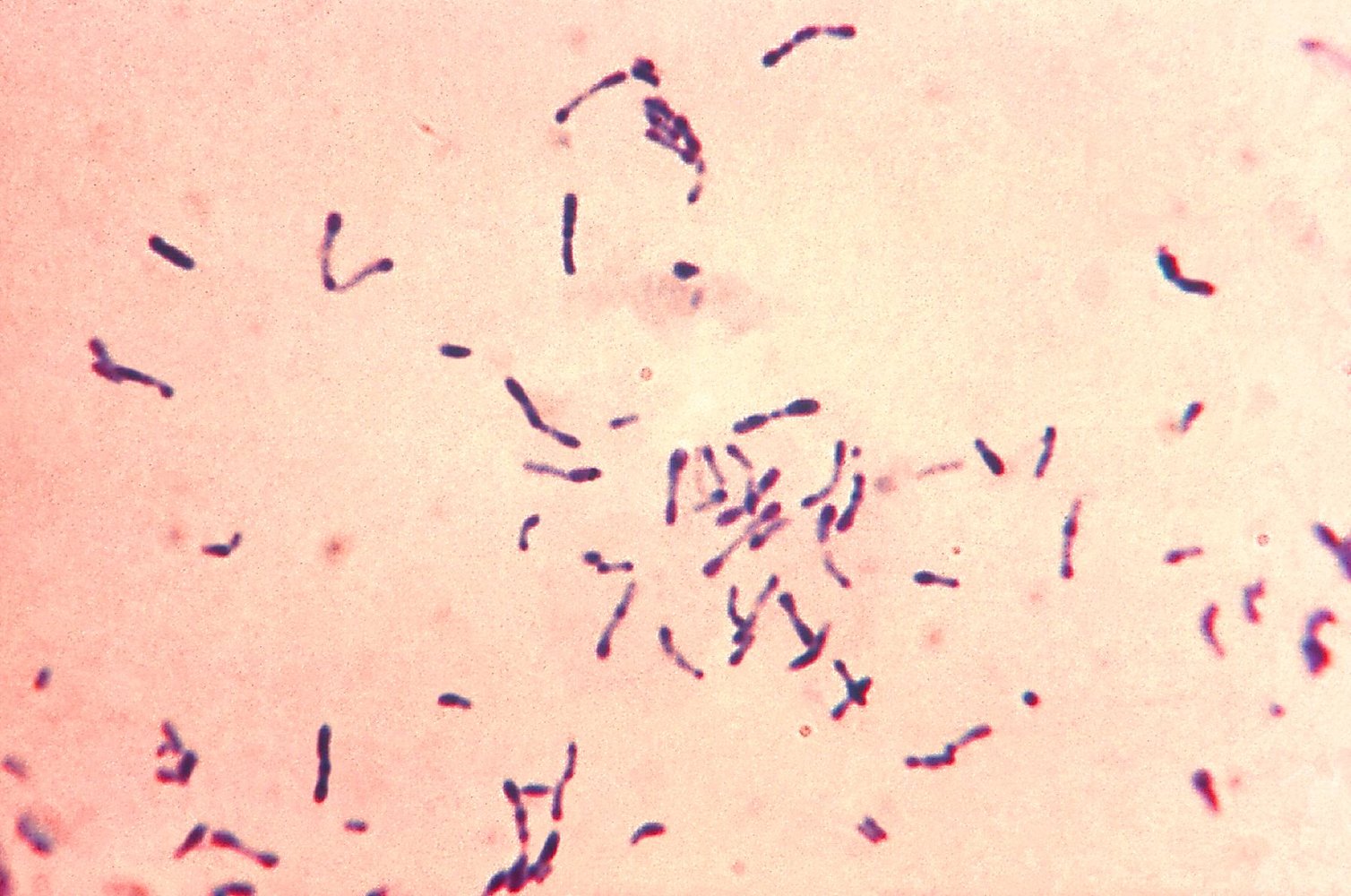
Photomicrograph (methylene blue stain)
Numerous gram-positive, rod-shaped bacteria can be seen (examples marked by blue overlay). The pathogens exhibit pleomorphism and do not show a particular arrangement.
The bacterial poles appear nodular (exampled indicated by arrow-heads). The nodules usually contain granules, which can be made visible with special metachromatic stains (not shown here).
Source: "ID#: 7323", Centers for Disease Control and Prevention, Centers for Disease Control and Prevention licensed under Public Domain
Pathophysiology
- C. diphtheriae colonizes the mucous membrane of the respiratory tract (respiratory diphtheria) and, less commonly, preexisting skin lesions (cutaneous diphtheria) .
-
C. diphtheriae has both toxigenic and nontoxigenic strains; toxigenic strains contain a beta-prophage gene (tox), which encodes for the exotoxin diphtheria toxin
- General characteristics: a heat-labile protein with a molecular weight of 62,000 kDa made of A and B fragments
- Mechanism of action: : the A fragment enters cells and catalyzes the transfer of ADP-ribosylation of the elongation factor-2 (EF-2) → inhibition of EF-2 → arrested protein translation and synthesis → cell death and necrosis
-
Local effects of the toxin: destruction of the respiratory epithelium with a subsequent inflammatory response
- Deposition of necrotic epithelium embedded within fibrinosuppurative inflammatory exudate (pseudomembrane) over the pharynx, tonsils, and/or larynx
- Enlargement of the cervical lymph nodes and edema of the soft tissue of the neck → bull neck appearance, airway obstruction
-
Systemic effects of the toxin
- Fatty changes and focal necrosis of the myocardium and, less commonly, the liver, kidney, and adrenal glands
- Nerve demyelination

ABCDEFG of C. diphtheria: ADP-ribosylation, Beta-prophage, Club-shaped, Diphtheria, Elongation Factor 2, metachromatic Granules.
References:[2][3][4]
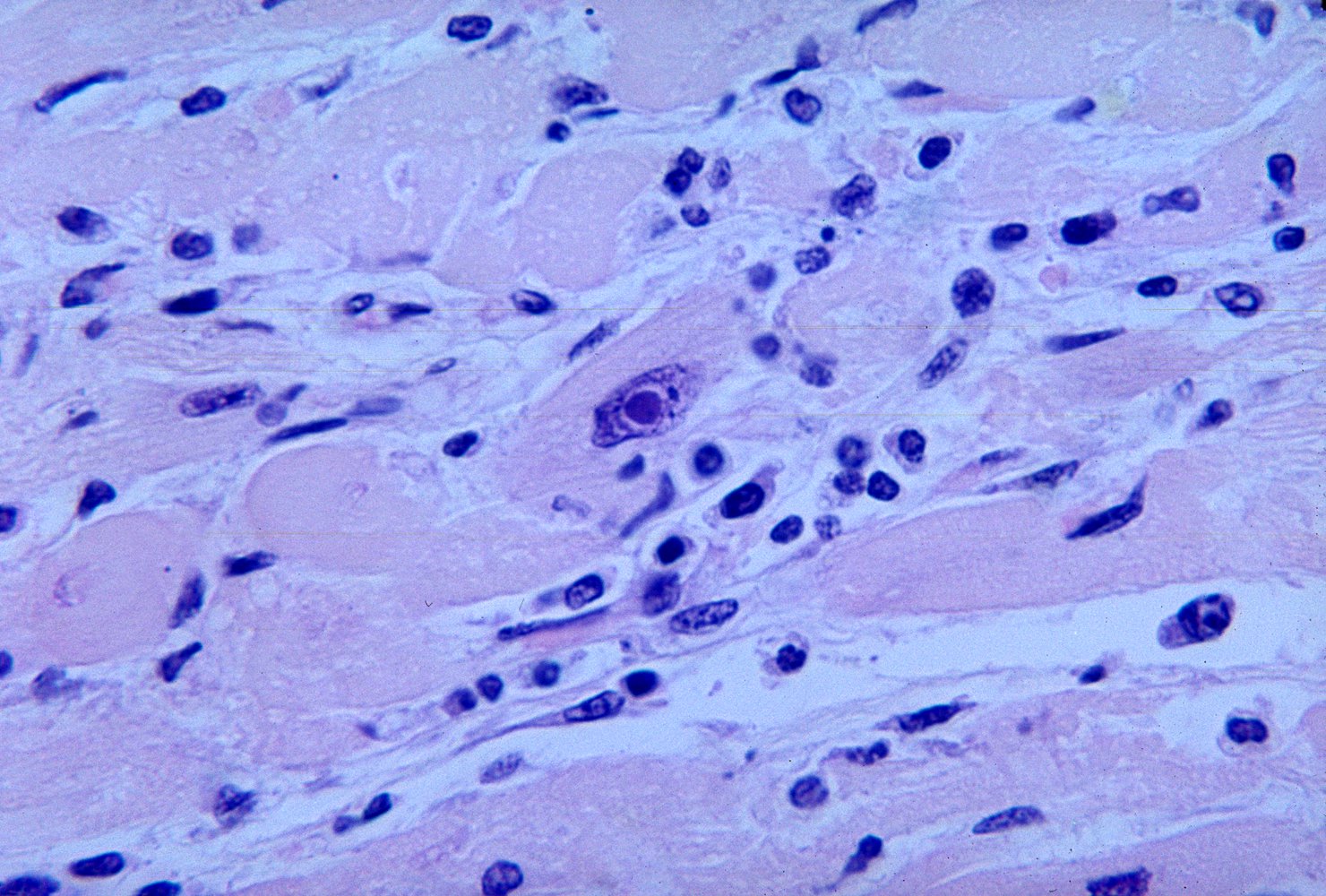
Photomicrograph of myocardium (H&E stain; very high magnification)
A lymphocytic infiltrate can be seen in the myocardium. Additionally, an intranuclear inclusion body is visible within a central cardiomyocyte.
These findings suggest infectious myocarditis. Immunofluorescence staining of the diphtheria toxin confirmed the diagnosis of diphtheritic myocarditis.
Source: "ID#: 23056", CDC/ Dr. Martin Hicklin, Centers for Disease Control and Prevention (CDC) licensed under Public Domain
Clinical features
Respiratory diphtheria
Patients initially present with prodromal symptoms: fever, malaise, and sore throat. Four to five days after the onset of prodromal symptoms, symptoms due to the local and systemic effects of the toxin occur.
- Incubation period: 2–5 days
-
Local features
- Anterior nasal diphtheria: bloody rhinorrhea
-
Tonsillar and pharyngeal diphtheria
- Grayish-white pseudomembrane over the posterior pharyngeal wall, and/or tonsils
- Any attempt to scrape off the pseudomembrane exposes the underlying capillaries and results in heavy bleeding.
- Bull neck due to cervical lymphadenopathy and swelling of the soft tissue of the neck → airway obstruction
- Foul mouth odor
- Laryngeal diphtheria: difficulty breathing, inspiratory stridor
-
Systemic features (due to dissemination of toxin)
-
Cardiac
- Myocarditis
- Arrhythmias
- Rarely, endocarditis
- Reversible polyneuropathy
- Acute tubular necrosis
- Adrenal insufficiency
- Septic arthritis
-
Cardiac


Cutaneous diphtheria
- Cutaneous diphtheria is the result of direct inoculation of C. diphtheriae into the skin (e.g., skin abrasions) or preexisting skin lesions.
- Usually seen in tropical regions, where it is more common than respiratory diphtheria
- Patients present with scaly erythematous rash, impetigo, or deep, punched-out ulcers
- Cutaneous diphtheria does not result in systemic effects.

References:[3]

A gray-white pseudomembrane extends from the left palatine tonsil over the uvula to the hard palate. The pseudomembrane consists of fibrinous exudate as well as immune and epithelial cells and is characteristic of tonsillar and pharyngeal diphtheria.
Source: “Dirty white pseudomembrane classically seen in diphtheria” by Dileepunnikri, Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}

Source: "ID#: 5325", CDC, Centers for Disease Control and Prevention (CDC) licensed under Public Domain

Patients with cutaneous diphtheria present with deep, non-healing and extremely painful ulcers.
Source: "ID#: 1941", CDC, Centers for Disease Control and Prevention (CDC) licensed under Public Domain
Diagnosis
-
Cultures: Obtain from all suspected patients (before initiating antibiotic therapy) to confirm the diagnosis.
- Respiratory diphtheria: Obtain nasal and pharyngeal cultures.
- Cutaneous diphtheria: Obtain cultures from skin lesions
- Microscopic examination: multiple Gram-positive club-shaped bacilli clustered in angular arrangements
-
Culture media of choice
- Cystine-tellurite agar: C. diphtheriae appears as black colonies.
- Loffler medium: shows metachromatic granules
-
Tests to identify toxigenic strains (if the culture reveals C. diphtheriae)
-
Elek test
- An immunoprecipitation test in which C. diphtheriae are grown in an agar culture that is embedded with an antitoxin-impregnated filter paper
- Positive if the strain is toxicogenic
- Polymerase chain reaction: to identify the tox gene
-
Elek test
Therapy (including antitoxin administration) should be started immediately upon clinical suspicion, even before diagnostic confirmation of diphtheria. [5]
Differential diagnoses
- Acute tonsillitis
- Croup
- Oropharyngeal candidiasis
The differential diagnoses listed here are not exhaustive.
Treatment
-
The patient should be isolated as soon as diphtheria is suspected. [2][5]
- Respiratory diphtheria: Initiate droplet precautions.
- Cutaneous diphtheria: Initiate contact precautions.
- Continue isolation until: [6]
- Cultures are negative for toxigenic C. diphtheria
- OR, if a toxigenic strain is isolated, two consecutive cultures taken ≥ 24 hours apart and ≥ 24 hours after completing antibiotic therapy are negative
- Antibiotic therapy; : penicillin G (IM injection) OR erythromycin (oral/IV) for 14 days [5]
-
Immediate administration of diphtheria antitoxin: The antitoxin can only neutralize the unbound toxin and should therefore be administered early in the course of the disease. [7]
- Contact the Center for Disease Control (CDC) urgently to request diphtheria antitoxin.
- Monitor closely during administration: Ensure anaphylaxis management is immediately available. [7]
- Laryngeal/pharyngeal diphtheria lasting < 48 hours: 20,000–40,000 units IV over 60 minutes
- Nasopharyngeal diphtheria: 40,000–60,000 units IV over 60 minutes
- Bull neck or diphtheria lasting > 3 days: 80,000–120,000 units IV over 60 minutes
- Airway support
- Monitor for myocarditis; : Conduct multiple ECGs; and serial measurement of cardiac markers.
Diphtheria is a nationally notifiable disease: Report all cases of respiratory diphtheria and toxigenic cutaneous diphtheria to the appropriate health departments. [5]
Administration of the antitoxin is a critical part of treatment, as the clinical features of diphtheria are not caused by the pathogen itself but rather by the exotoxin that C. diphtheriae produces.
Prevention
Immunization [8][9][10]
- The diphtheria vaccine is a toxoid vaccine.
- Four diphtheria vaccines are available in the US:
- Diphtheria, tetanus, acellular pertussis vaccine (DTaP)
- Tetanus diphtheria acellular pertussis vaccine (Tdap)
- Diphtheria and tetanus vaccine (DT)
- Tetanus and diphtheria vaccine (Td)
- See “ACIP immunization schedule” for details.
Exposure control [6][11][12]
Close contacts [5][6][12]
- Those with frequent direct contact with the patient
- Anybody exposed to secretions from the infected source .
- For healthcare workers, exposure includes:
- Unprotected face-to-face contact with an individual with respiratory diphtheria )
- Unprotected exposure to skin lesions in a patient with cutaneous diphtheria
Management of exposed contacts
In addition to isolating and treating infected patients, the following measures should be performed in exposed close contacts regardless of their diphtheria immunity status. [5][6][12]
-
All exposed contacts
- Obtain cultures for C. diphtheria.
- Provide postexposure prophylaxis for diphtheria.
- Quarantine while awaiting culture results.
- Monitor for clinical features of diphtheria for 7–10 days.
- If cultures are negative: Discontinue quarantine and complete chemoprophylaxis. [12]
- If cultures are positive: [12]
- Asymptomatic individuals (carriers): Isolate until completion of chemoprophylaxis and two cultures are negative.
- Symptomatic patients: See “Treatment.”
Postexposure prophylaxis for diphtheria [5][12]
All exposed close contacts should receive prophylactic antibiotics and be assessed for immunization.
- Antibiotic chemoprophylaxis: erythromycin OR a single IM dose of benzathine penicillin G [5][13]
-
Active immunization with a diptheria vaccine [6][12]
- Unknown or incomplete diphtheria vaccine status (see “ACIP immunization schedule”): Administer an immediate dose of a diphtheria vaccine.
- Up-to-date diphtheria vaccine status (see “ACIP immunization schedule”):
- Last dose ≥ 5 years prior: Immediately administer a booster dose of a diphtheria vaccine.
- Last dose < 5 years prior: No dose is required at this time.
External Resources
References
- "Diphteria"
- Kasper DL, Fauci AS, Hauser SL, et al. "Harrison's Principles of Internal Medicine". McGraw-Hill Education. (2015). ISBN: 9780071802161
- AAP Committee on Infectious Diseases. "Red Book: 2021–2024 Report of the Committee on Infectious Diseases". American Academy of Pediatrics. (2021). ISBN: 9781610025218
- "Information to collect on close contacts of diphtheria cases: Appendix 2". https://web.archive.org/save/https://www.cdc.gov/diphtheria/downloads/appendix-2-close-contact-form.pdf. [2022-11-02]
- "WHO Guideline on the clinical management of diphtheria". https://web.archive.org/web/20251006133127/https://iris.who.int/server/api/core/bitstreams/6f1840f0-056e-4823-991c-19fdae2d09d3/content. [2024-02-02]
- "Child and Adolescent Immunization Schedule. Recommendations for Ages 18 Years or Younger, United States, 2023". https://web.archive.org/web/20230324163634/https://www.cdc.gov/vaccines/schedules/hcp/imz/child-adolescent.html. [2023-02-10]
- "Catch-up Immunization Schedule for Children and Adolescents Who Start Late or Who Are More than 1 Month Behind Recommendations for Ages 18 Years or Younger, United States, 2023". https://web.archive.org/web/20230324164753/https://www.cdc.gov/vaccines/schedules/hcp/imz/catchup.html. [2023-02-10]
- "Adult Immunization Schedule by Age Recommendations for Ages 19 Years or Older, United States, 2023". https://web.archive.org/web/20230324184103/https://www.cdc.gov/vaccines/schedules/hcp/imz/adult.html. [2023-02-10]
- "Infection Control in Healthcare Personnel: Epidemiology and Control of Selected Infections Transmitted Among Healthcare Personnel and Patients". https://www.cdc.gov/infectioncontrol/guidelines/healthcare-personnel/selected-infections/diphtheria.html. [2022-11-02]
- "Infection Control in Healthcare Personnel: Epidemiology and Control of Selected Infections Transmitted Among Healthcare Personnel and Patients". https://web.archive.org/web/20230510152507/https://www.cdc.gov/infectioncontrol/guidelines/healthcare-personnel/selected-infections/diphtheria.html#:~:text=Occupational%20Exposures,-Transmission%20of%20diphtheria&text=Exposure%20to%20cutaneous%20diphtheria%20lesions,i.e.%2C%20gown%20and%20gloves).. [2022-11-01]
- Bader MS, McKinsey DS. "Postexposure prophylaxis for common infectious diseases.". Am Fam Physician. 88(1). :25-32. (2013)
- Kumar V, Abbas AK, Aster JC. "Robbins & Cotran Pathologic Basis of Disease". Elsevier Saunders. (2014). ISBN: 9781455726134
- "Vaccine-preventable diseases: monitoring system. 2020 global summary". https://apps.who.int/immunization_monitoring/globalsummary/incidences?c=USA. [2020-07-15]
- Herold G. "Internal Medicine". Herold G. (2014). ISBN: 9781291727333
- Furger P, Suter TM. "SURF-med Guidelines Medizin der Schweiz". Editions D&F, Neuhausen am Rheinfall (CH) (2008). (2010). ISBN: 3905699109
- Sitzmann FC. "Duale Reihe Pädiatrie". Thieme Verlag (2006). ISBN: 9783131253323
- Hoffmann B. "Crashkurs Pädiatrie". Urban&Fischer bei Elsevier (2003). ISBN: 9783437432002
- von Schweinitz D, Heinrich M, Schäfer K. "Kinderchirurgie Basiswissen und Praxis". Zuckschwerdt Verlag (2008). ISBN: 9783886039425