Summary
Distal radius fracture is a common fracture of the arm, occurring most frequently in individuals 10–30 years of age and in those older than 65. The injury can be caused by low-energy trauma (common in women with osteoporosis) or high-energy trauma (e.g., sports injuries or motor vehicle accidents). Clinical features include wrist pain and tenderness, soft tissue swelling, visible deformity, and decreased range of motion at the wrist joint. Diagnosis is confirmed by x-ray. Nondisplaced stable fractures are typically managed with closed reduction and immobilization. Fractures that are open, unstable, comminuted, and/or accompanied by neurovascular injury are usually managed surgically.
Epidemiology
- Total incidence: 2.5% of all emergency department (ED) visits [1]
-
Bimodal peak incidence [1]
- 10–30 years of age; most commonly due to high-energy trauma in male individuals
- > 65 years of age; most commonly due to low-energy trauma in women with osteoporosis
Distal radius fractures are the second most common type of fracture in older adults presenting to the ED. [2]
Epidemiological data refers to the US, unless otherwise specified.
Etiology
-
Mechanism of injury [2][3]
-
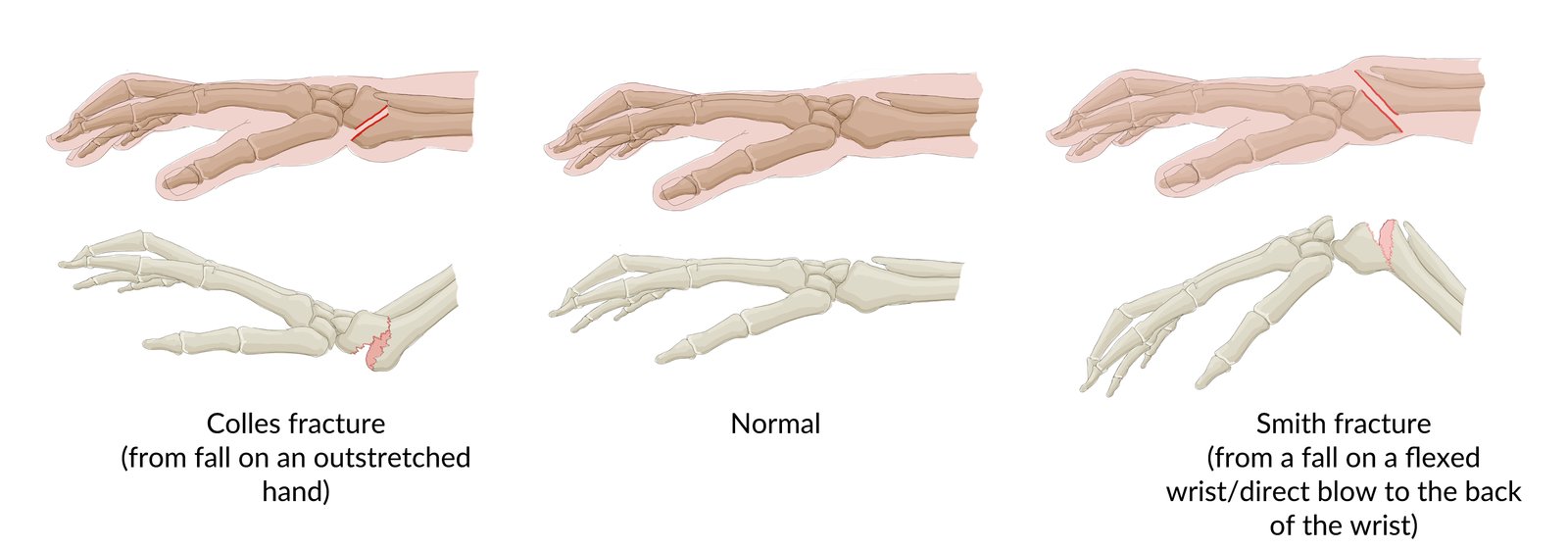
Fall onto an outstretched hand (most common)
- Dorsiflexed wrist (a typical protective action used to break one's fall) → extension fracture (Colles fracture)
- Palmar-flexed wrist → flexion fracture (Smith fracture)
- High-energy trauma, e.g., MVC, contact sports
-
Fall onto an outstretched hand (most common)
-
Risk factors
- Osteoporosis
- See “Etiology of fractures.”

© AMBOSS
Classification
This section lists common types of distal radial fractures and their mechanisms of injury. See “Fracture classification” for general principles of fracture description. [4]
-
Colles fracture
- Result of a fall on an extended wrist
- The distal fragment is usually radially angulated and dorsally displaced.
- Intraarticular extension is possible.
-
Smith fracture
- Result of a fall onto a flexed wrist or direct injury to the back of the wrist
- The distal fragment is volarly angulated and volarly displaced.
- Intraarticular extension, neurovascular compromise, and/or instability are more likely than in Colles fractures.
-
Barton fracture
- Result of a fall on an extended wrist.
- Intraarticular fracture and dislocation
- The radiocarpal segment is avulsed and dorsally displaced.
-
Reverse Barton fracture
- Result of a fall on a flexed wrist
- An intraarticular fracture and dislocation
- The radiocarpal segment is avulsed and volarly displaced.
-
Hutchinson fracture (Chauffeur fracture)
- Result of a direct blow to the radial portion of the wrist
- The radial styloid is intraarticularly avulsed.
-
Die-punch fracture [5]
- Result of an axial or transverse load through the lunate into the radius
- Intraarticular depression fracture of the lunate fossa of the distal radius
")



")

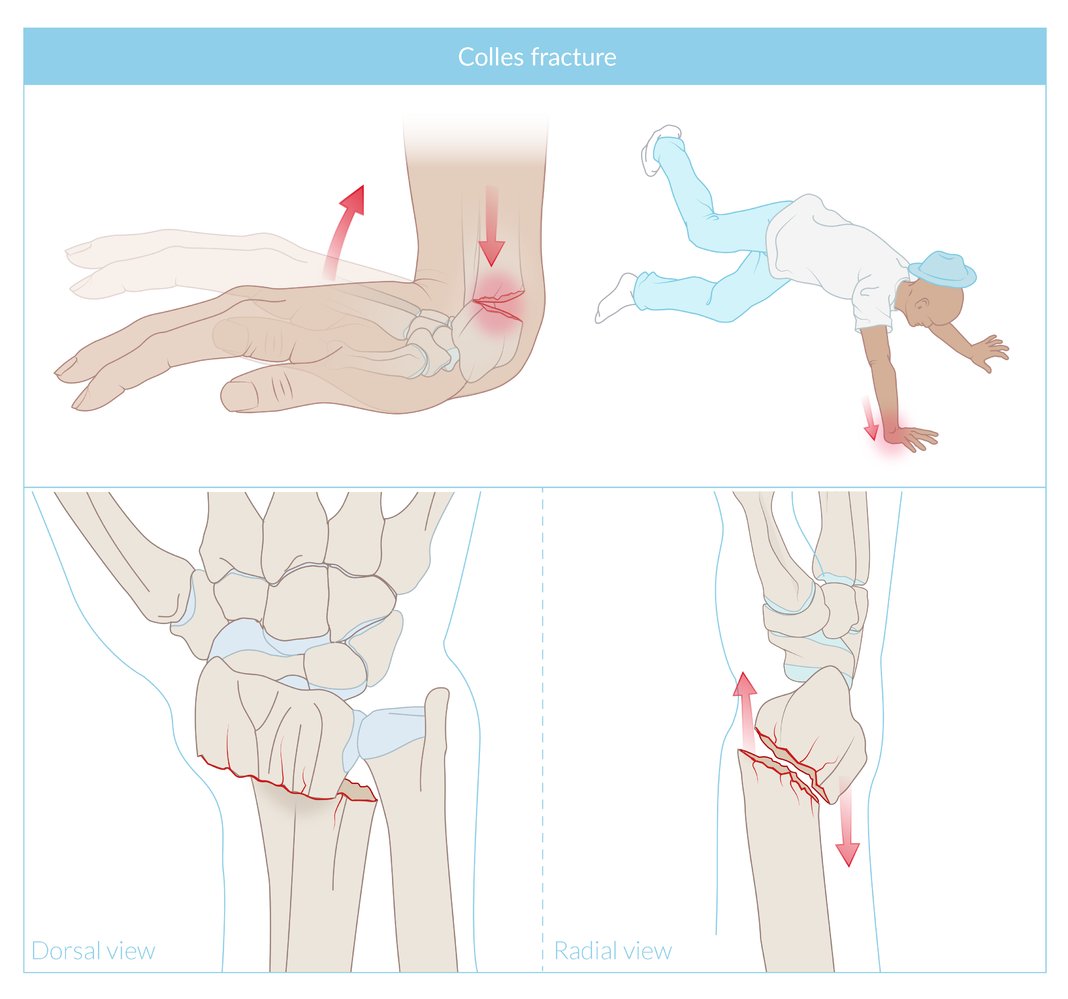
Fracture of the distal radius with radial and dorsal displacement. Commonly a result of falling onto the extended wrist.
© AMBOSS
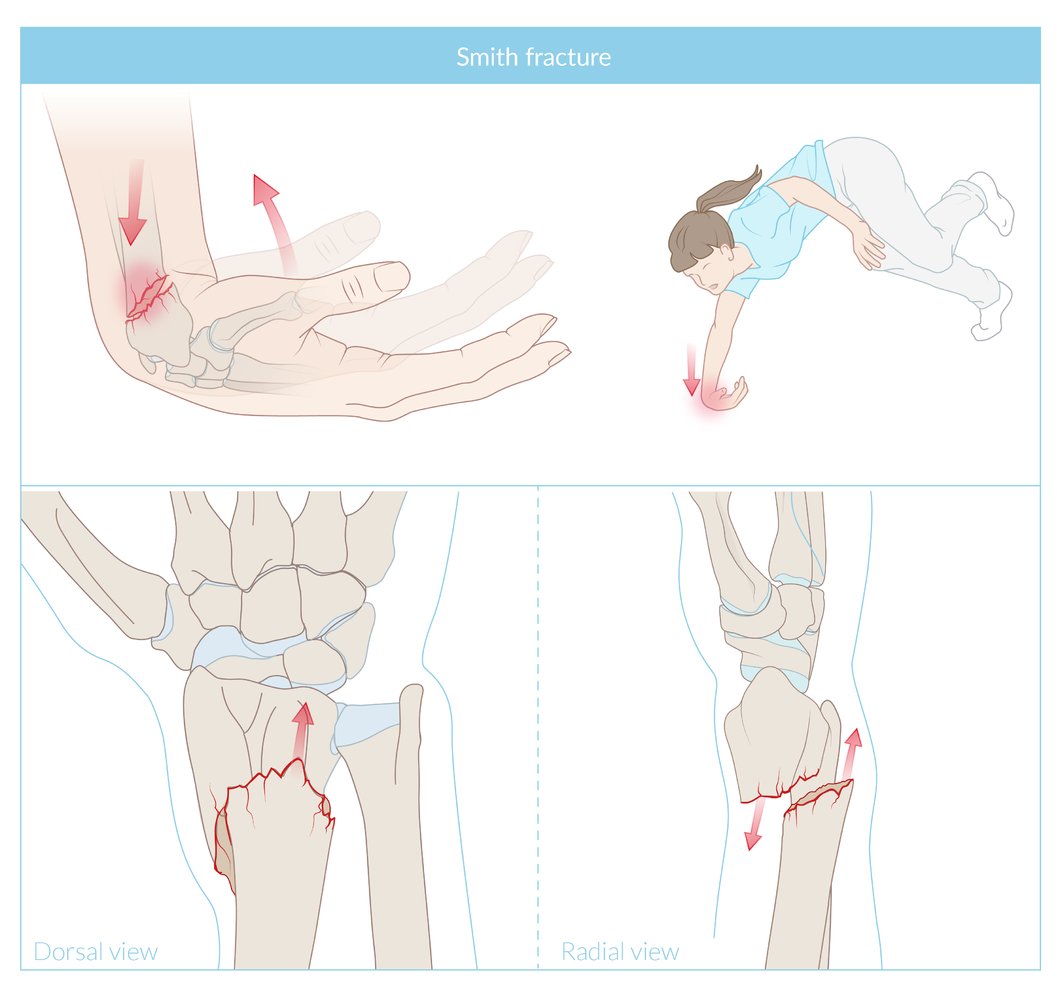
Fracture of the distal radius with volar displacement of the distal radial fragment and dorsal angulation at the fracture site.
© AMBOSS
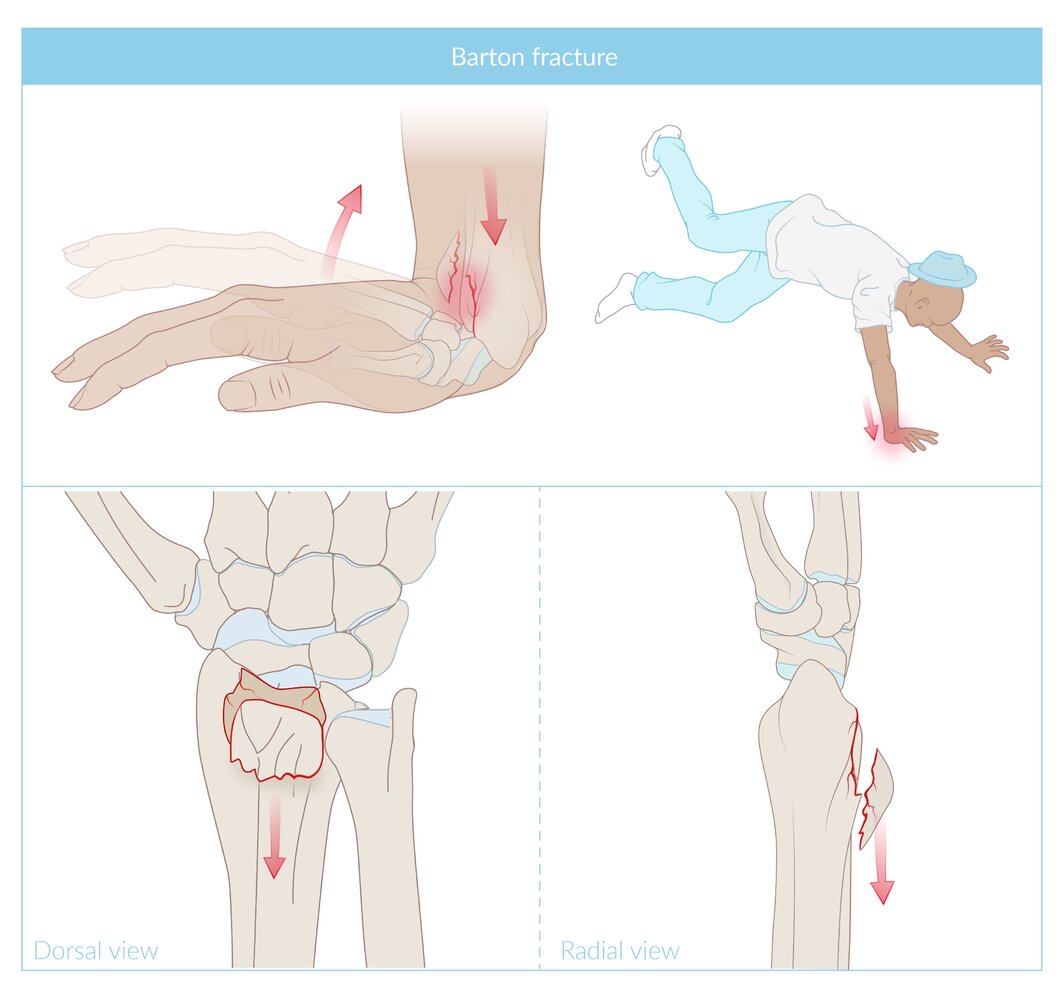
A partial fracture of the distal radius with a dorsal edge fragment. The cause is usually a fall onto the extended hand.
© AMBOSS
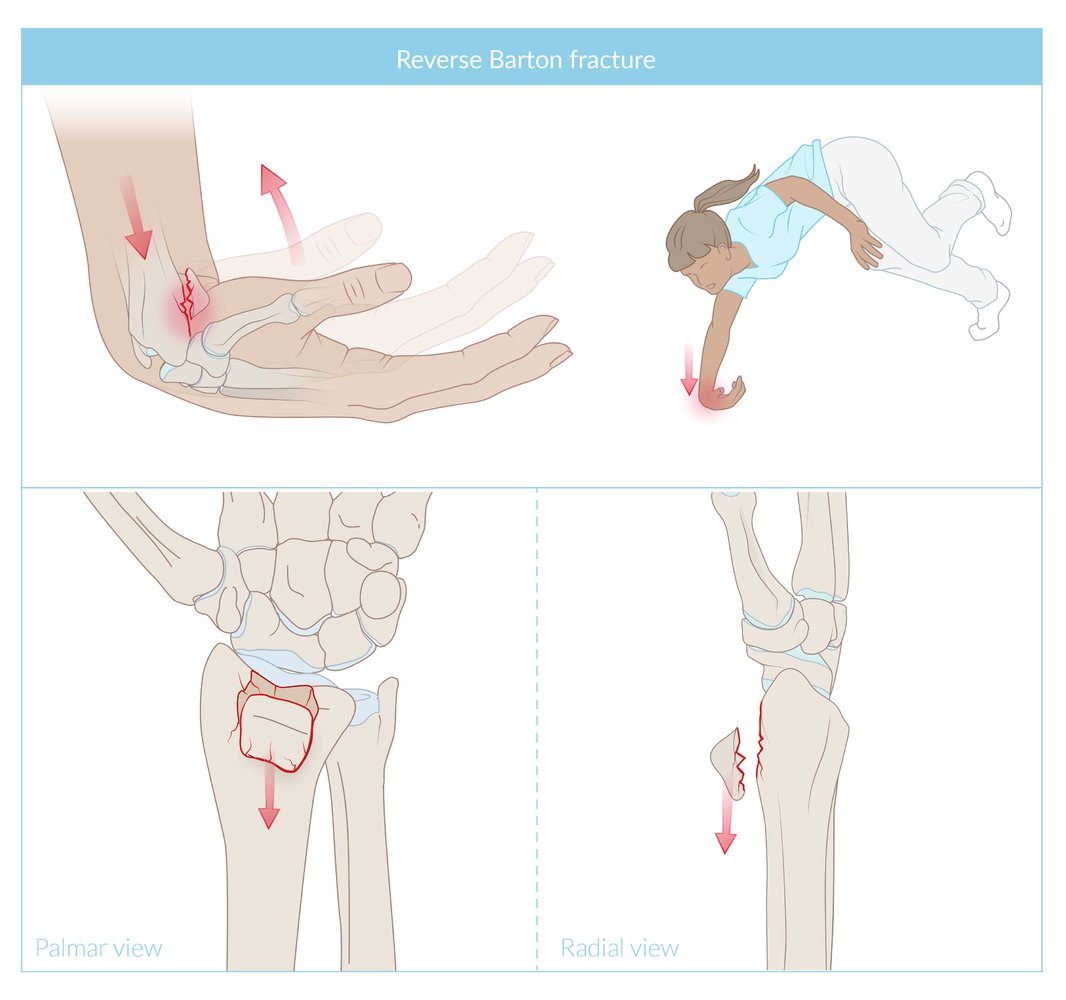
A partial articular radius fracture with a volar edge fragment. The cause is usually a fall onto the flexed hand.
© AMBOSS
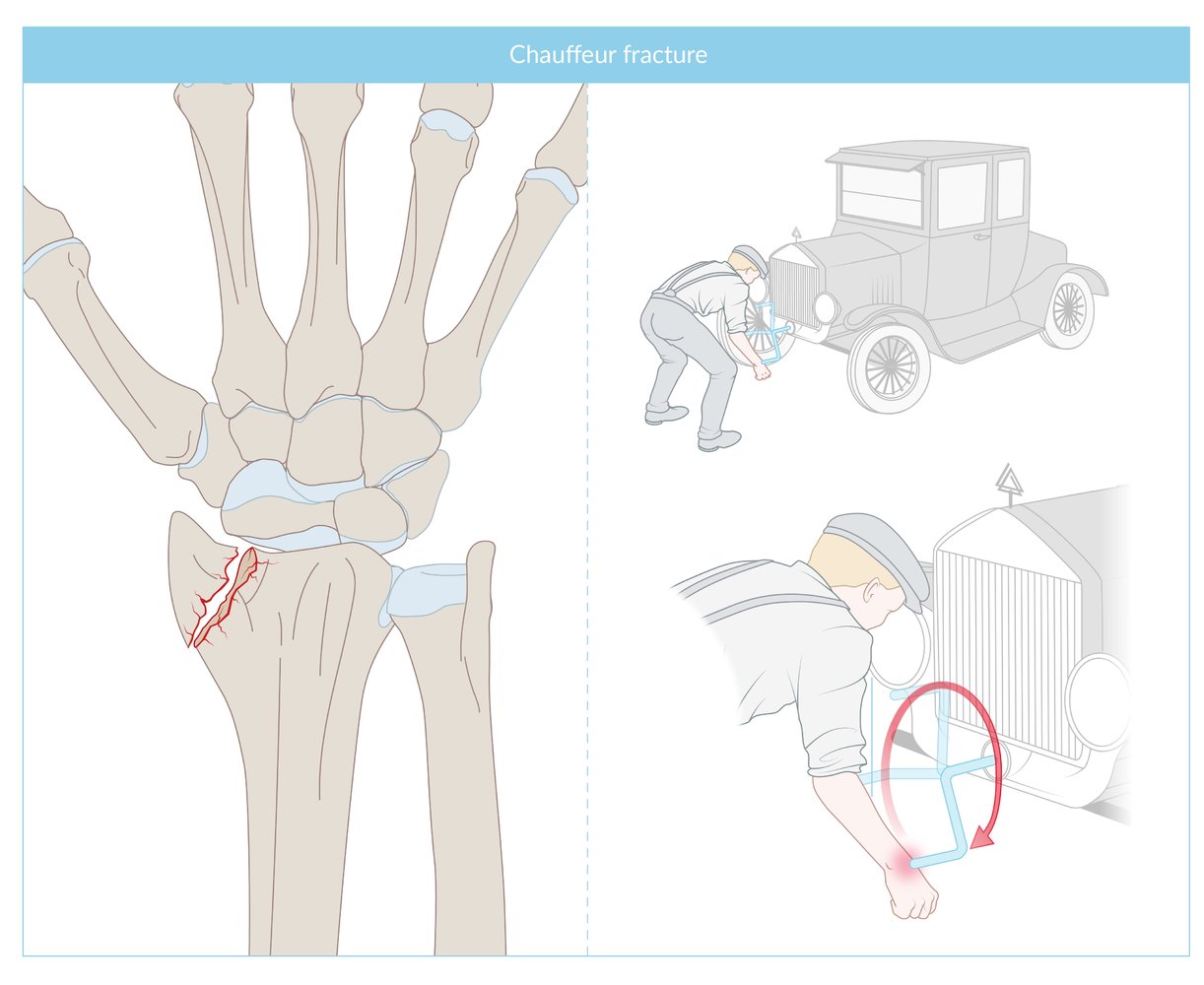
Fracture of the radial styloid, commonly due to direct trauma. The term ''Chauffer fracture' was coined by the British surgeon Jonathan Hutchison in the days when cars were hand-cranked and the crank shooting back could hit and thus fracture the wrist.
© AMBOSS
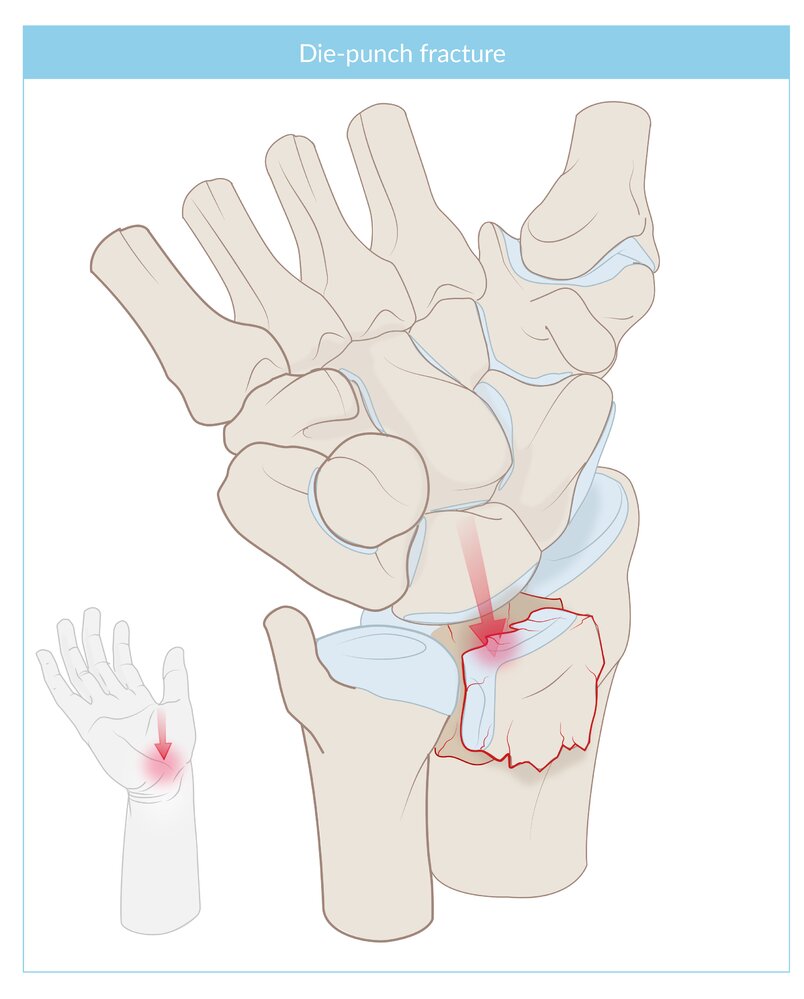
An impacted, intra-articular fracture of the lunate fossa of the distal radius. The cause is most commonly an axial loading force applied against the distal radius.
© AMBOSS
© AMBOSS
Clinical features
- Pain, tenderness, and soft tissue swelling
- Reduced range of motion at the wrist joint
-
Wrist deformities based on the type of fracture
- Colles fracture: dorsally displaced and dorsally angulated fracture (bayonet or dinner fork deformity)
- Smith fracture: garden spade deformity
- See “Fracture signs.”


Left hand of a patient with Colles fracture
The wrist is dorsally displaced and dorsally angulated giving it the appearance of a dinner fork or bayonet.
Source: “File:Poignet Gauche suite a fracture type Pouteau Colles.jpg” by sylvain letuffe, Wikimedia Commos, licensed under CC0 1.0. Modifications: enhanced contrast and brightness. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
{kind=link}
Diagnosis
Clinical evaluation [3]
-
Neurovascular exam
- Assess radial and ulnar artery pulses and capillary refill time.
- Evaluate for median nerve injury , radial nerve injury , and ulnar nerve injury. [3]
- Repeat the exam after reduction and again after immobilization.
- Skin exam: Evaluate for laceration, tearing, and tenting.
Repeat the neurovascular exam after reduction and again after immobilization of the radial fracture. [4]
")


Imaging [3][6][7]
-
X-ray: anterior-posterior, lateral, and oblique views of the wrist (including the carpal bones)
- Assess angulation, rotational deformity, shortening, joint alignment, and comminution.
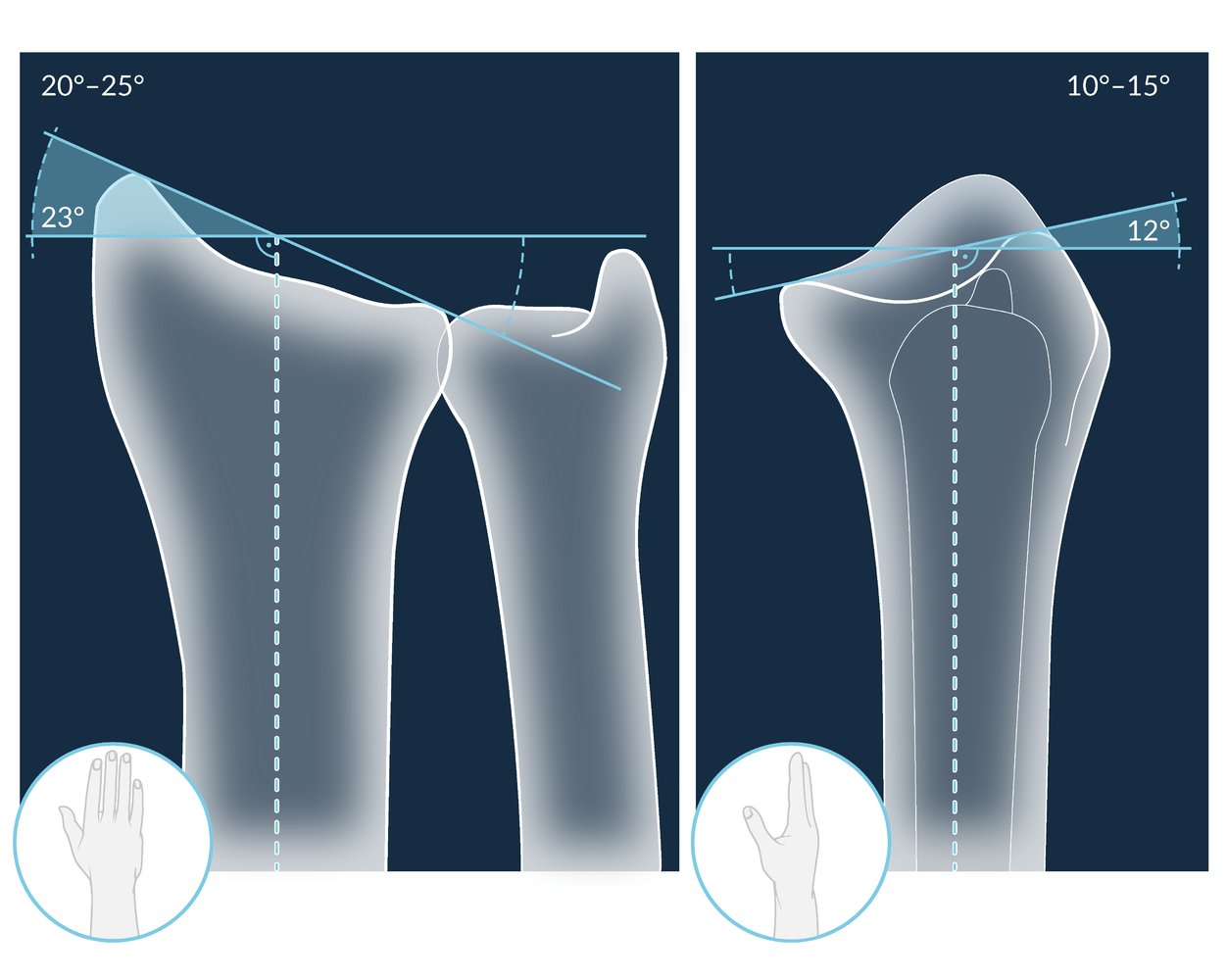
-
Radial inclination: Inclination ≥ 10–15° indicates acceptable fracture reduction. [2][6]
- Normal range: 15–25° [8]
- On posterior-anterior view, measure the angle between:
- A line from the radial styloid to the ulnar border of distal radius
- A line across the articular surface perpendicular to the long axis of the radius
-
Volar inclination: Inclination > 20° indicates a potentially unstable fracture. [6]
- Normal range: 10–25° [8]
- On lateral view, measure the angle between:
- A line along the dorsal to palmar articular surface of radius
- A line across the articular surface perpendicular to the long axis of the radius
- See “Radiographic signs of a fracture.”
- CT wrist: may be required for preoperative planning [2][3]
Obtain a second set of x-rays after reduction and immobilization of the fracture.



")

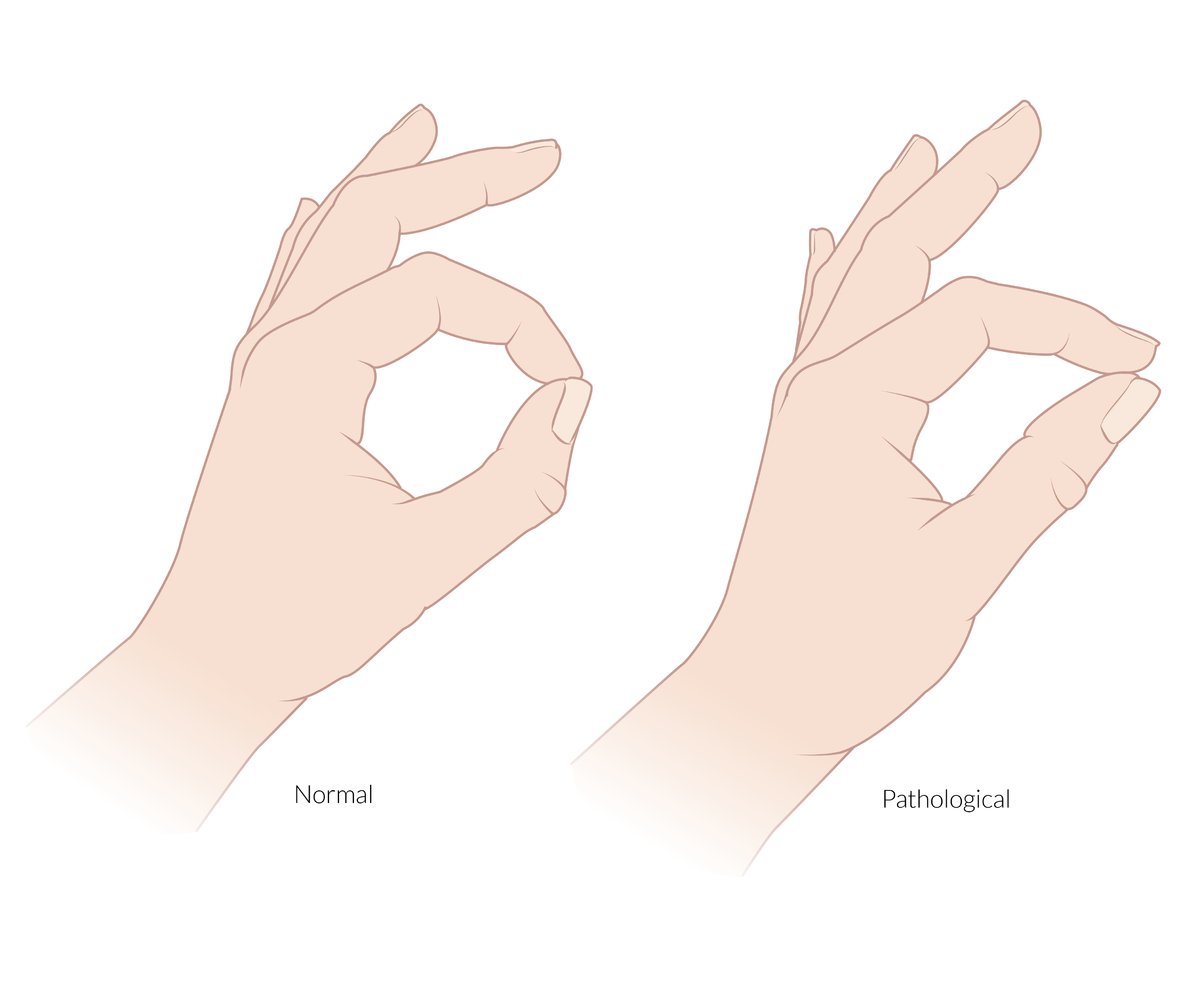
The anterior interosseous nerve is a pure motor branch of the median nerve. It supplies the flexor pollicis longus, the radial half of the flexor digitorum profundus (and the pronator quadratus).
Pinch sign: an inability to flex the DIP of the index finger and IP joint of the thumb when asked to make an “OK” sign that is caused by a lesion or entrapment of the anterior interosseous nerve
© AMBOSS
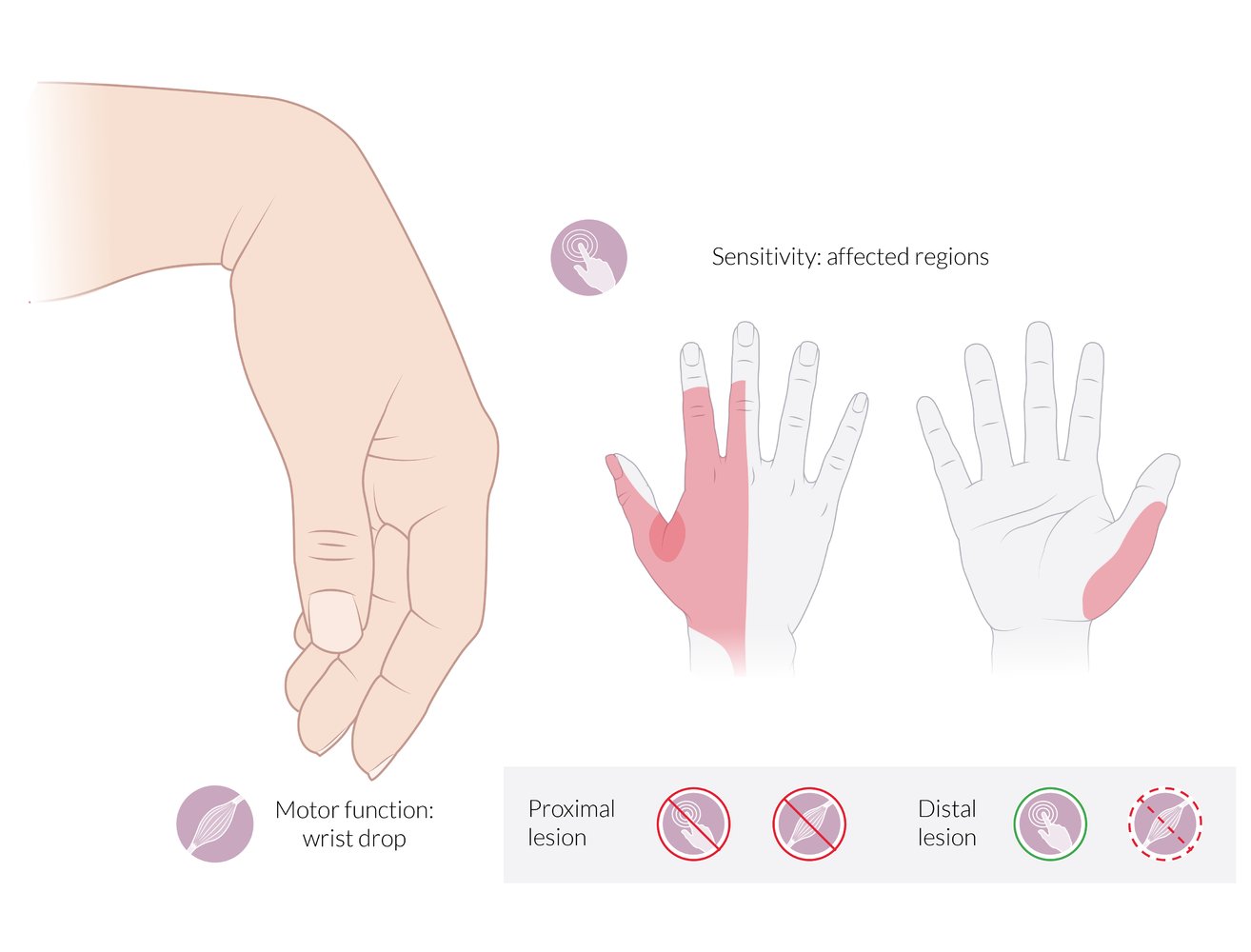
Motor deficits:
- Wrist drop: inability to extend (dorsiflex) the wrist
- Inability to extend the fingers at the MCP joints
Sensory deficits:
- Dorsal aspect: radial 2½ fingers (less commonly, 3½ fingers), excluding the tips of the 2nd and 3rd fingers. The 1st web space is the autonomous sensory zone of the radial nerve and is highlighted in red.
- Palmar aspect: the radial border of the thumb
Proximal lesion: complete loss of motor and sensory function
Distal lesion (radial tunnel syndrome): partial loss of motor function; preservation of sensory function
© AMBOSS
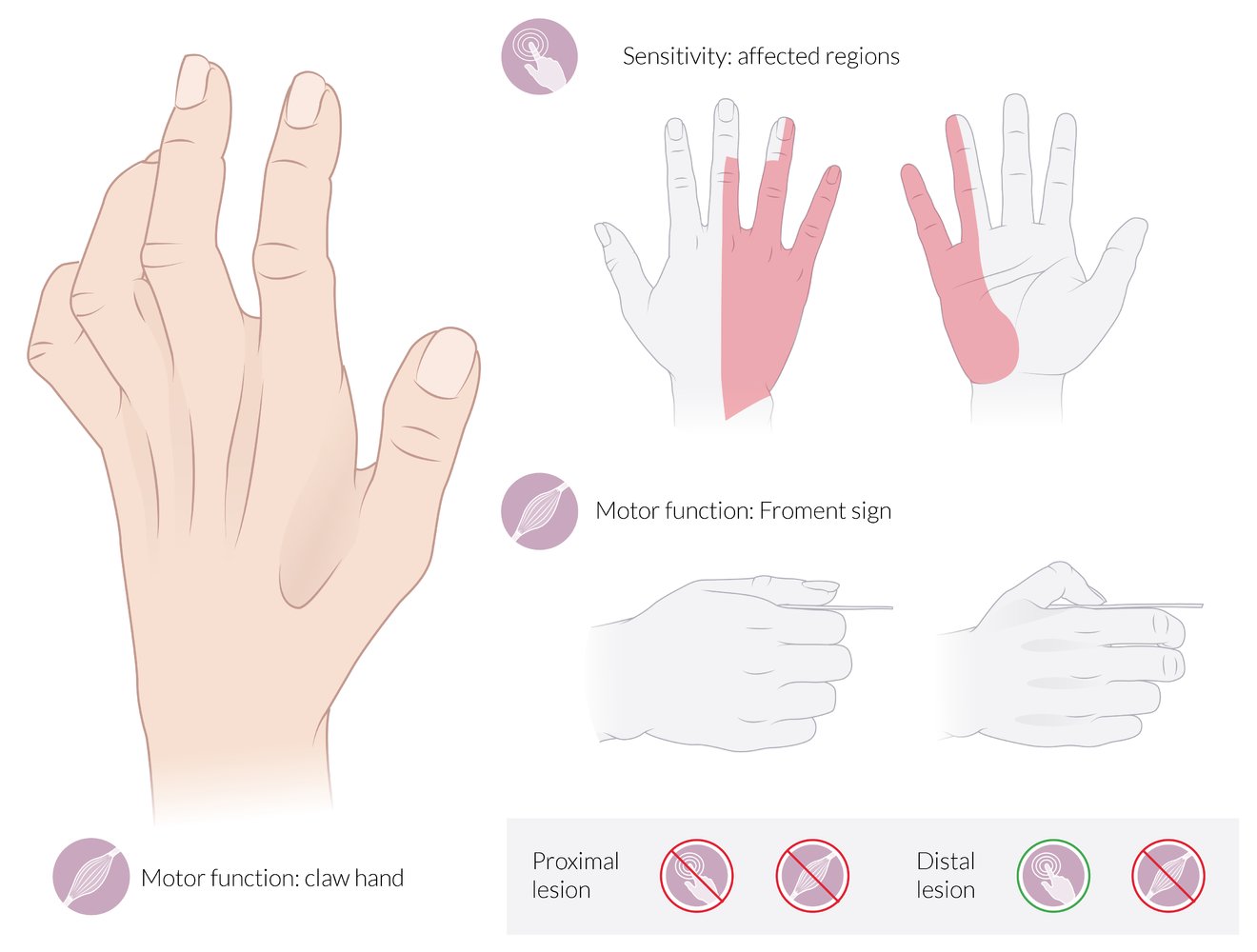
Motor deficits:
- Claw hand: The 4th and 5th joints are hyperextended at the MCP and flexed at the IP joints at rest (neutral position).
- Froment sign: The patient is asked to grasp a piece of paper between the thumb and the index finger. When the examiner tries to pull the paper away, the thumb flexes at the IP joint because the flexor pollicis longus (supplied by the median nerve) compensates for the paralyzed adductor pollicis (supplied by the ulnar nerve).
Also depicted here is hollowing of the intermetacarpal spaces and the 1st web space due to the atrophy of the interossei, which is seen in chronic ulnar nerve palsy.
Sensory deficits:
- Dorsal aspect: ulnar 2½ fingers (less commonly, 1½ fingers), excluding the tips of the 3rd and 4th fingers
- Palmar aspect: ulnar 1½ fingers
Proximal lesion: complete loss of motor and sensory functions
Distal lesion: complete loss of motor function; preservation of sensory function
© AMBOSS

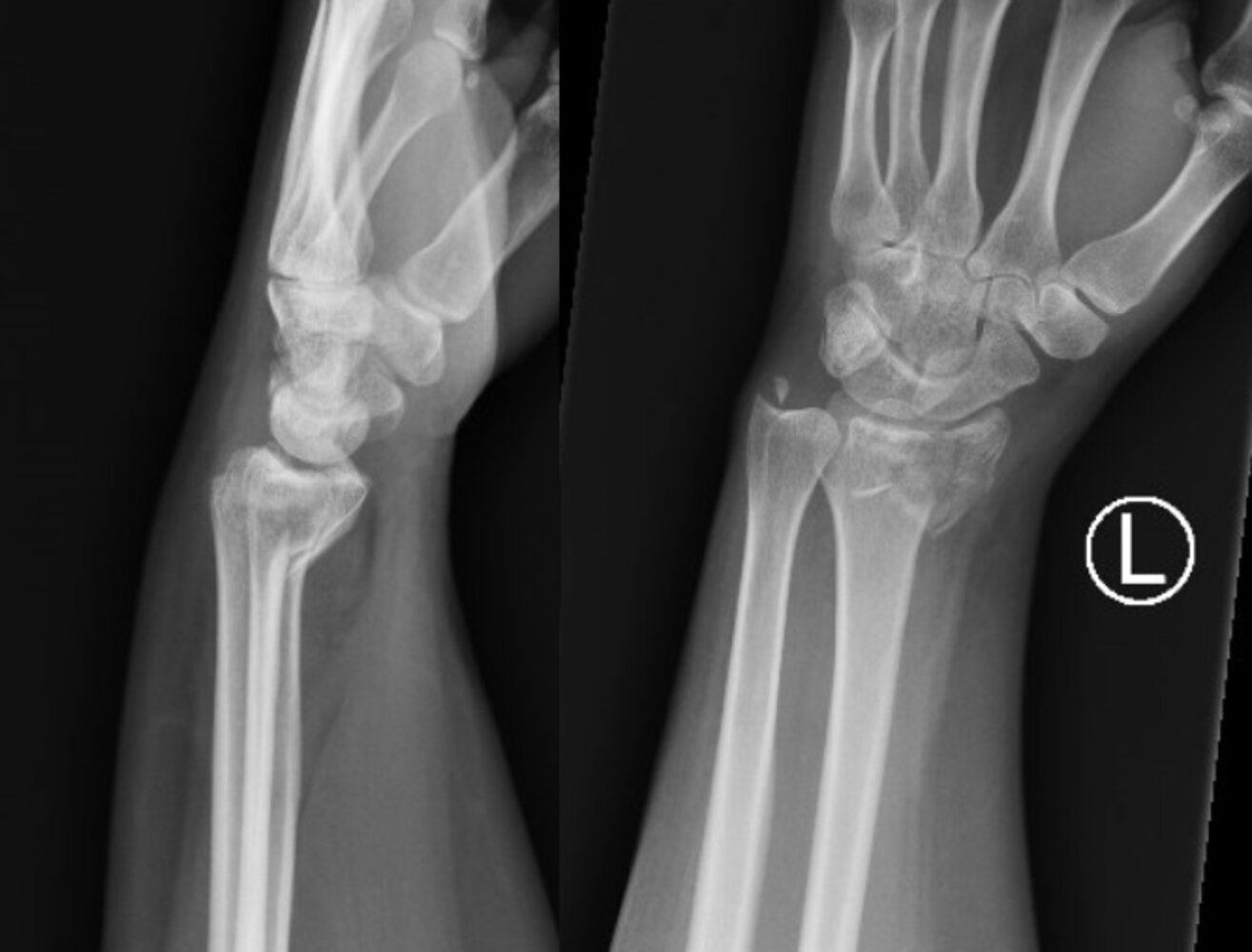
X-ray wrist (left: PA view; right: lateral view) after a fall onto an outstretched hand
A metaphyseal fracture of the distal radius (green line) shows dorsal angulation of the distal fragment and impaction. (The vertical white line represents the axis of the radius. The horizontal white line represents the right angle that the radial articular surface physiologically stands at. The dotted white line illustrates the dorsal angulation of the distal fragment.) This type of fracture has been termed a Colles fracture. The pronator quadratus fat pad is displaced and seen as a convex lucency (red curved line). A fracture of the ulnar styloid is also present (white arrow).
Source: “Collesfracture” by Lucien Monfils, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}

X-ray distal forearm (PA view)
A comminuted fracture (red lines) of the distal radius shows intraarticular extension and radial displacement (indicated by green lines and arrows) of the main distal fragment (F). The ulnar styloid process (USP; normal position indicated by yellow dashed outline) is also fractured and displaced medially (indicated by yellow overlay and arrow).
Source: © IMPP

X-ray distal forearm (lateral view)
A comminuted fracture (red lines) of the distal radius shows intraarticular extension. Dorsal angulation of the main distal fragment has altered the bony alignment (indicated by green lines and arrows).
Source: © IMPP
X-ray wrist (left: lateral view; right: PA view)
A comminuted intraarticular fracture of the distal radius (red overlay) is accompanied by radial displacement (red arrow) and volar angulation (red line and angle) with respect to a line perpendicular (green dashed line) to a line through the shaft (green line). An ulnar styloid fracture (green overlay) is also seen.
Source: “Smith2019Frac” by James Heilman, MD, Wikimedia Commons, licensed under CC BY-SA 4.0. Modifications: Cropped.. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 4.0.
{kind=link}
In the posteroanterior view of a normal wrist joint, a line drawn tangential to the radial styloid and connecting the ends of the distal radius forms an angle of 30° with a line drawn perpendicular to the long axis of the radius.
© AMBOSS
Differential diagnoses
See also “Types of distal radius fractures.”
- Ligamentous injury
- Triangular fibrocartilage complex sprain
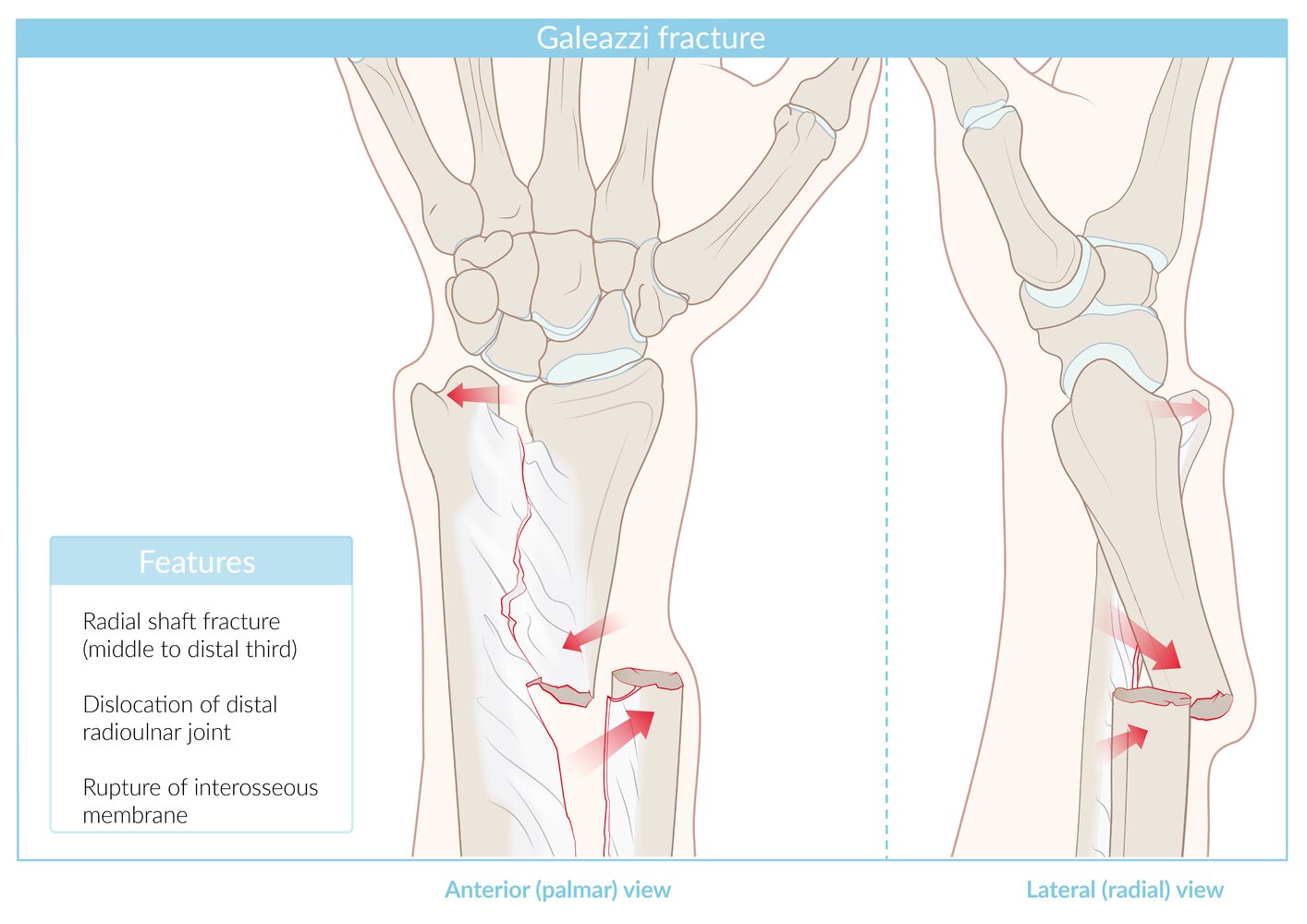
- Galeazzi fracture: associated with DRUJ instability
- Ulnar styloid fracture
- Carpal bone fractures, e.g., scaphoid fracture ,lunate fracture
- Carpal bone subluxation and/or dislocation
- Lunate dislocation
- Perilunate dislocation
- Dorsal intercalated segment instability (DISI)
- Volar intercalated segment instability (VISI)
- See also “Overview of radius and ulna fractures.”


The differential diagnoses listed here are not exhaustive.
Right distal forearm
© AMBOSS

X-ray hand (PA view)
A nondisplaced fracture (red line) is visible through the waist of the scaphoid bone of the wrist.
© AMBOSS
Treatment
Overview [2][9][10]
| Initial management of distal radius fractures by fracture type [4] | ||
|---|---|---|
| Nonoperative management | Indications for an emergent orthopedic consult | |
| Colles fracture |
|
|
| Smith fracture | ||
| Barton fracture |
|
|
| Reverse Barton fracture | ||
| Hutchinson fracture |
|
|
| Die-punch fracture |
|
|
Nonoperative management [2][3][4]
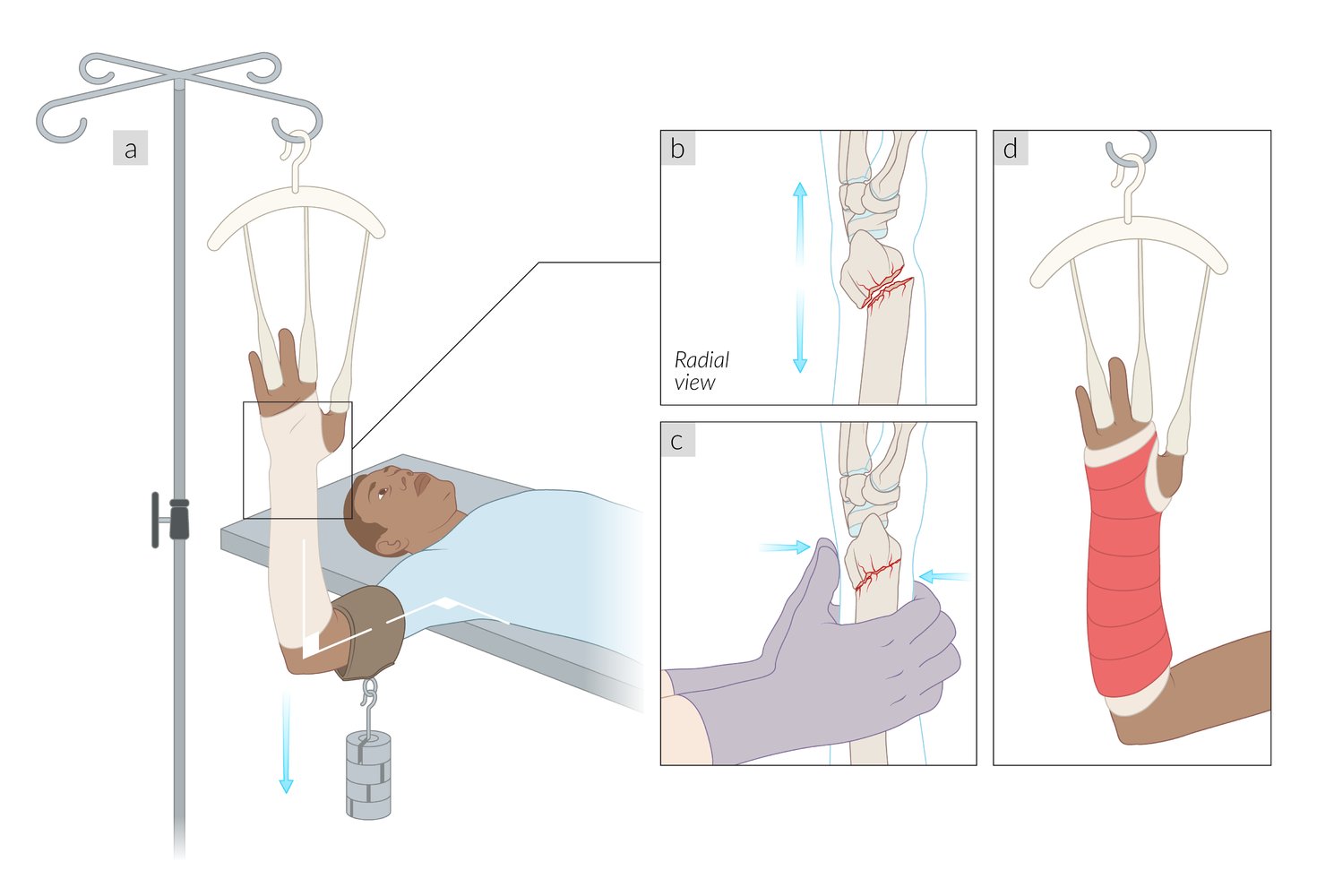
Nondisplaced and stable fractures are typically managed with closed reduction and immobilization. [2]
- Closed reduction while applying longitudinal traction through the fingers either manually or using a finger trap
- Initial immobilization in sugar tong splint
- Short arm cast when edema resolves
- Postreduction x-rays and serial exams to evaluate for subsequent displacement
- Cast removal after 6 weeks
- See also “Conservative management of fractures.”
The radius should be realigned to its normal position after fracture reduction.

Operative management [2][3]
Indications [4][9]
Operative fixation in patients ≥ 65 years of age does not improve long-term functional outcomes. [9][10]
- Open, significantly displaced, intraarticular, and/or unstable fractures
- Neurovascular injury
- Any of the following post-reduction radiographic signs of instability:
- > 3 mm radial shortening
- ≥ 10° dorsal tilt
- Intraarticular step-off > 2 mm
- Concurrent ulnar fracture
- Fracture-dislocation
Common techniques
All procedures require postoperative immobilization of the forearm and wrist.
- Open reduction internal fixation: Fixed-angle volar plates are used for displaced, unstable, and/or involve osteoporotic bone.
- K-wire fixation: typically limited to patients with minimal fracture comminution and healthy bone
- External fixation: typically used in patients with severe soft tissue injury and/or polytrauma
 fixation of distal radius fracture")




© AMBOSS

X-ray right wrist (A: lateral view; B: PA view)
Comminuted fractures (indicated by arrows and red lines) of the distal radius and ulna are accompanied by dorsal angulation and displacement (indicated by dashed and solid lines and curved arrow). Intraarticular extension of the radial fracture (green line) is best seen on the PA view.
D: dorsal; P: pisiform bone; V: volar
Source: “Fig 2, In: Simultaneous Fractures of Distal and Proximal Ends of Radius and Ulna: Four Fractures in One Forearm” by Hashem M, AlMohaini RA, Cureus, licensed under CC BY 4.0. Modifications: placed lateral view (A) to face the opposite way, with volar facing to our left. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).

X-ray distal forearm (left: lateral view; right: PA view)
A comminuted distal radius fracture with intraarticular extension was treated by open reduction and internal fixation with a volar locking plate. A fracture at the base of the ulnar styloid process is also seen (indicated by arrow). The bones appear osteopenic as a result of disuse osteoporosis.
Source: “Fig 1, In: Early Results of a Variable-Angle Volar Locking Plate for Distal Radius Fractures: A Bi-centre Study” by Elerian S, Singh T, A Jagodzinsk N et al., Cureus, licensed under CC BY 4.0. Modifications: image cropped, letter "L" removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
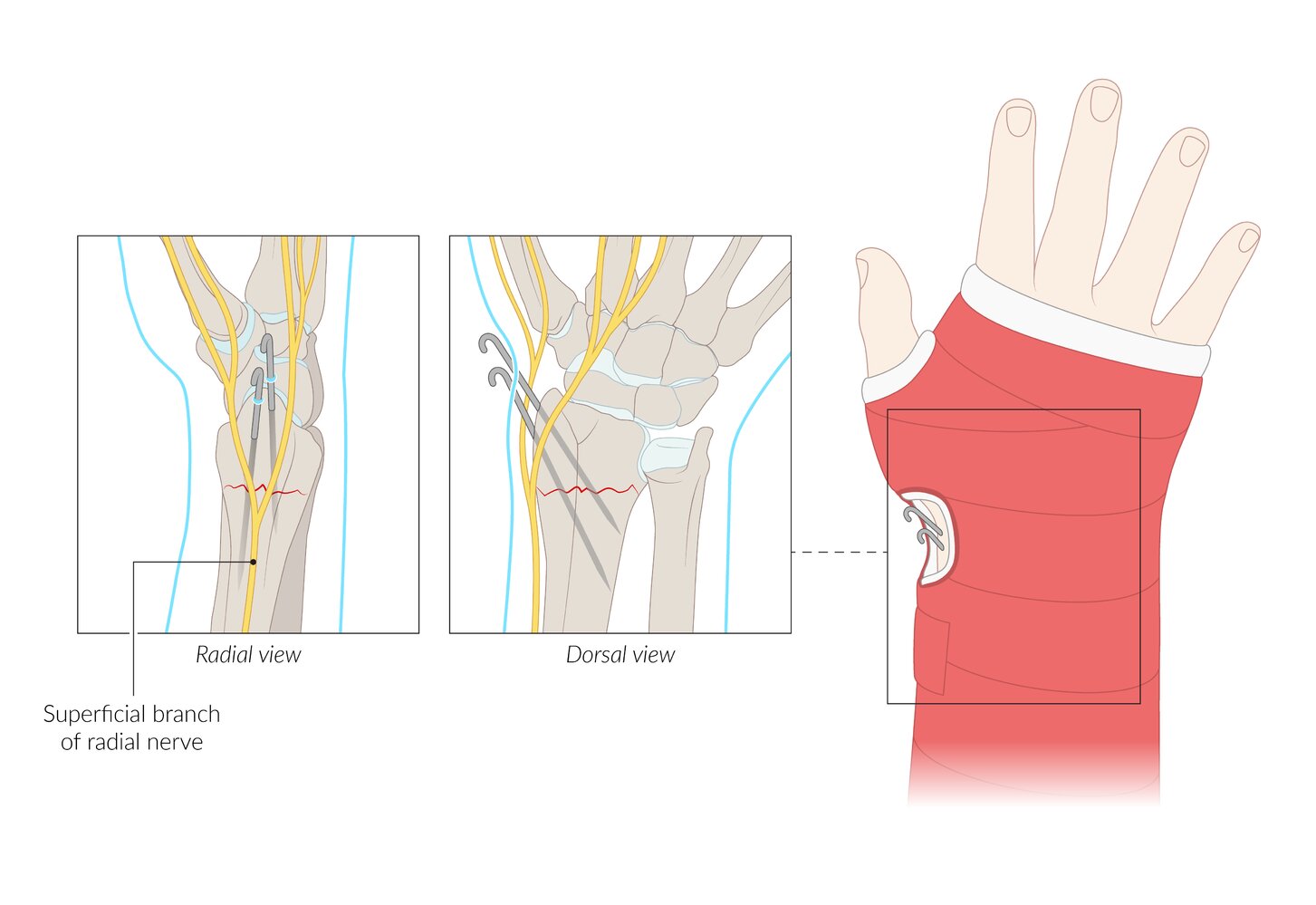
Circular short arm cast with K-wire fixation following distal radius fracture. When inserting the wires, the superficial branch of the radial nerve must be spared. This surgical procedure is mainly used in children.
© AMBOSS
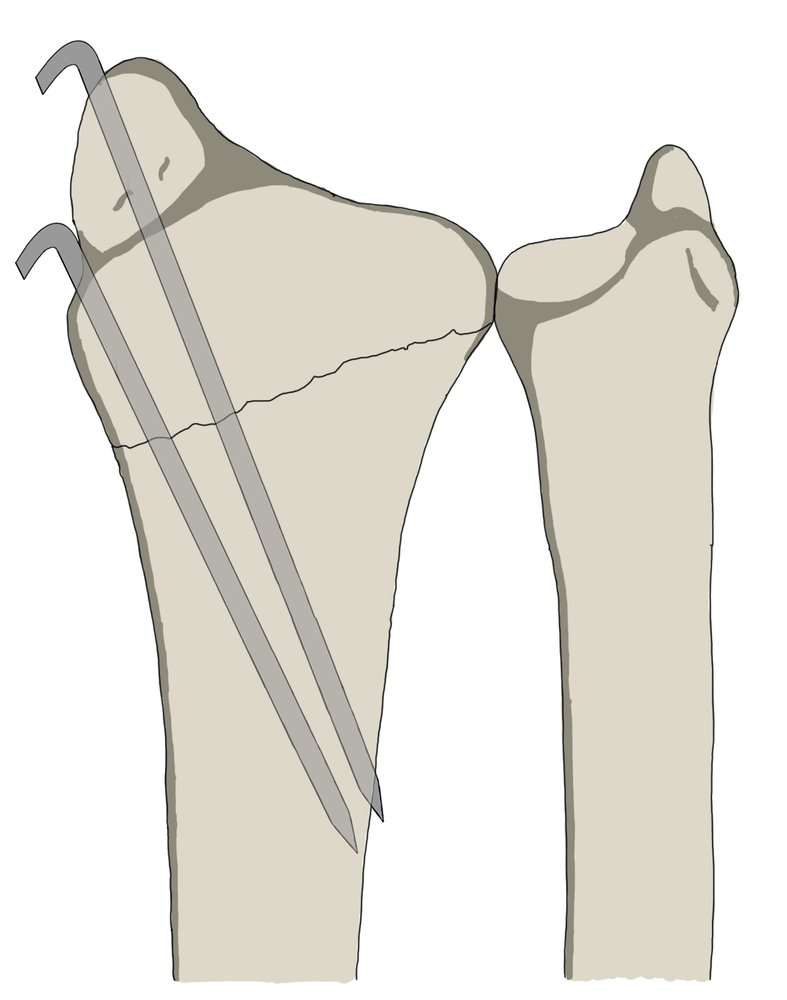
K-wires are stainless steel wires/pins used in orthopedic surgery to fixate bone fragments without compressing them. The free ends are usually bent and left protruding through the skin.
© AMBOSS

X-ray (AP and lateral view) of the wrist and distal forearm.
Image A and B show an oblique and mildly translated fracture of the lateral aspect of the distal radius.
Image C and D show post-operative AP and lateral x-rays following reduction and stabilisation using two Kirschner wires to provide protection against rotational damage.
These images represent adequate reduction and fixation of a distal radius fracture using Kirschner wires.
Source: “Abb. 2a–d. in: Distale Radiusfraktur” by R. Lippisch, B. Lucas, J. P. Schüttrumpf, S. Piatek & F. Walcher, Trauma und Berufskrankheit, Springer Nature, licensed under CC BY 4.0.

X-ray (lateral and AP view) of the right wrist and distal forearm.
Image A and B show a compacted distal radius fracture with dorsal angulation and considerable osteoporosis of the radial head.
Image C and D show post-operative radiographs following closed reduction and external fixation. The image shows the percutaneous placement of three Kirschner wires into the distal radius and a external fixation device mounted to the radial shaft and first metacarpal bone.
This image represents adequate reduction and stabilisation of a distal radius fracture using closed reduction and external fixation.
Source: “Abb. 6a–d. in: Distale Radiusfraktur” by R. Lippisch, B. Lucas, J. P. Schüttrumpf, S. Piatek & F. Walcher, Trauma und Berufskrankheit, Springer Nature, licensed under CC BY 4.0.
Complications
- General complications of fractures
- Traumatic acute carpal tunnel syndrome [2][3]
- Tendinopathy (e.g., extensor pollicis longus) [13]
We list the most important complications. The selection is not exhaustive.
External Resources
References
- Nellans KW, Kowalski E, Chung KC. "The Epidemiology of Distal Radius Fractures". Hand Clin. 28(2). :113-125. (2012)
- Mauck BM, Swigler CW. "Evidence-Based Review of Distal Radius Fractures". Orthop Clin North Am. 49(2). :211-222. (2018)
- Levin LS, Rozell JC, Pulos N. "Distal Radius Fractures in the Elderly". J Am Acad Orthop Surg. 25(3). :179-187. (2017)
- Walls R, Hockberger R, Gausche-Hill M, Erickson TB, Wilcox SR. "Rosen's Emergency Medicine 10th edition- Concepts and Clinical Practice E-Book". Elsevier Health Sciences. (2022). ISBN: 9780323757904
- Zhang J, Ji X ran, Peng Y, et al. "New classification of lunate fossa fractures of the distal radius". J Orthop Surg. 11(1). (2016)
- Ilyas AM, Jupiter JB. "Distal Radius Fractures—Classification of Treatment and Indications for Surgery". Orthop Clin North Am. 38(2). :167-173. (2007)
- Perugia D, Guzzini M, Civitenga C, et al. "Is it really necessary to restore radial anatomic parameters after distal radius fractures?". Injury. 45. :S21-S26. (2014)
- Hosseinzadeh P, Olson D, Eads R, et al. "Radiologic Evaluation of the Distal Radius Indices in Early And Late Childhood". Iowa Orthop J. 38. :137-140. (2018)
- "Management of Distal Radius Fractures Evidence-Based Clinical Practice Guideline". http://www.aaos.org/drfcpg. [2020-12-05]
- Ochen Y, Peek J, van der Velde D, et al. "Operative vs Nonoperative Treatment of Distal Radius Fractures in Adults". JAMA Netw Open. 3(4). :e203497. (2020)
- Zhang B, Hu P, Cheng X, et al. "Volar, Splitting, and Collapsed Type of Die‐Punch Fracture Treated by Volar Locking Plate ( <scp>VLP</scp> ): <scp>A Retrospective</scp> Study". Orthop Surgery. 12(3). :869-877. (2020)
- Zhang X, Hu C, Yu K, et al. "Volar locking plate (VLP) versus non-locking plate (NLP) in the treatment of die-punch fractures of the distal radius, an observational study". Int J Surgery. 34. :142-147. (2016)
- White BD, Nydick JA, Karsky D, et al. "Incidence and Clinical Outcomes of Tendon Rupture Following Distal Radius Fracture". J Hand Surg [Am]. 37(10). :2035-2040. (2012)