Summary
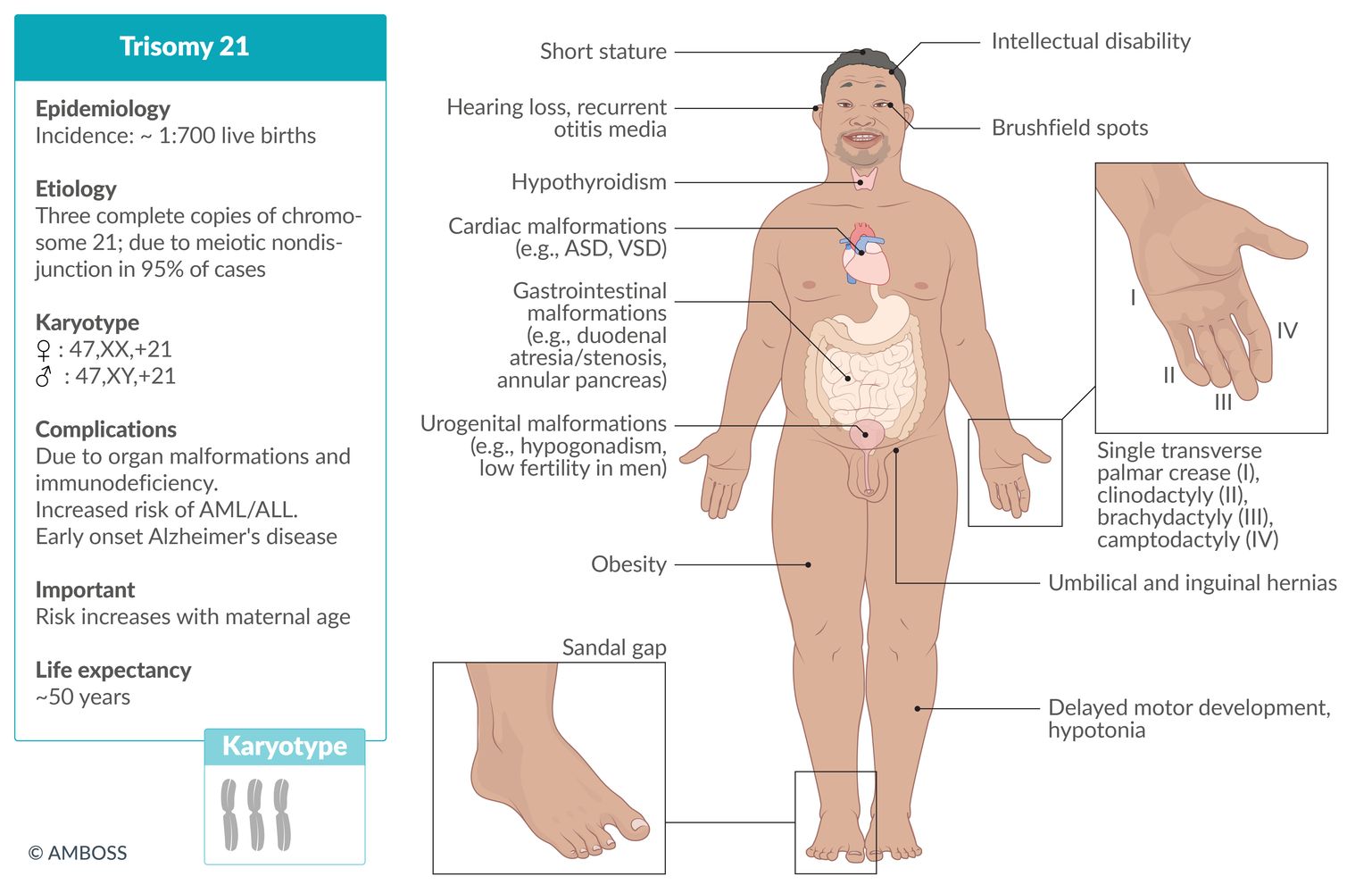
Down syndrome, also called trisomy 21, is the most common autosomal chromosomal irregularity, occurring in approximately 1:700 live births. The risk of a trisomy 21 pregnancy increases with maternal age. Most individuals with Down syndrome have full trisomy 21, which occurs due to meiotic nondisjunction and results in a genotype with three complete copies of chromosome 21 and a total of 47 chromosomes. Other less common forms of Down syndrome are translocation trisomy 21 and mosaic trisomy 21. Clinically, trisomy 21 manifests as a syndrome involving a characteristic appearance (e.g., upward-slanting palpebral fissures, epicanthal folds, protruding tongue, short stature, transverse palmar crease, sandal gap), organ malformations (e.g., heart defects, duodenal atresia, Hirschsprung disease), and endocrine disorders (e.g., obesity, diabetes mellitus, hypothyroidism). Trisomy 21 is associated with an increased risk of malignancy (e.g., high risk of leukemia) and intellectual disability. Down syndrome is primarily detected in prenatal tests, including ultrasound measurement of nuchal translucency and maternal blood tests for certain hormones (e.g., increased inhibin A and β-hCG; decreased estriol, alpha-fetoprotein, and pregnancy-associated protein A). Fetal karyotyping via chorionic villus sampling or amniocentesis confirm the diagnosis, but these procedures are associated with an increased risk of fetal injury or loss. Management of trisomy 21 involves evaluation, monitoring, and treatment of the symptom complex and malformations as necessary.

 fact sheet")

Original title: “Genetics: Section 10.1 - Down Syndrome”. Created by: Physeo™.
© AMBOSS
Epidemiology
- Most common viable autosomal chromosome aberration; (∼ 1:700; live births) and most common genetic cause of cognitive impairment [1][2]
-
The risk of a Down syndrome pregnancy increases with maternal age. [3]
- Incidence at 20 years: ∼ 1:2000
- Incidence at 30 years: ∼ 1:900
- Incidence at 40 years: ∼ 1:100
- Incidence at 45 years: ∼ 1:30
The general risk of trisomy 21 increases with maternal age. This does not, however, apply to translocation trisomies!
Epidemiological data refers to the US, unless otherwise specified.
Etiology
Full trisomy 21 (∼ 95% of cases)
- Definition: three complete copies of chromosome 21 are present in all cells, with a total of 47 chromosomes
- Occurrence: : Full trisomy 21 is not a hereditary disease; ; the chromosomal irregularity occurs spontaneously.
-
Pathogenesis: meiotic nondisjunction; [4]
- Maternal nondisjunction occurs during meiosis I in approx. 70% of cases and during meiosis II in approx. 20% of cases.
- May occur due to paternal nondisjunction during spermatogenesis, more commonly during meiosis II (approx. 5% of cases)
- Karyotype: ♀: 47,XX,+21 or ♂: 47,XY,+21


Translocation trisomy 21 (3–4% of cases)
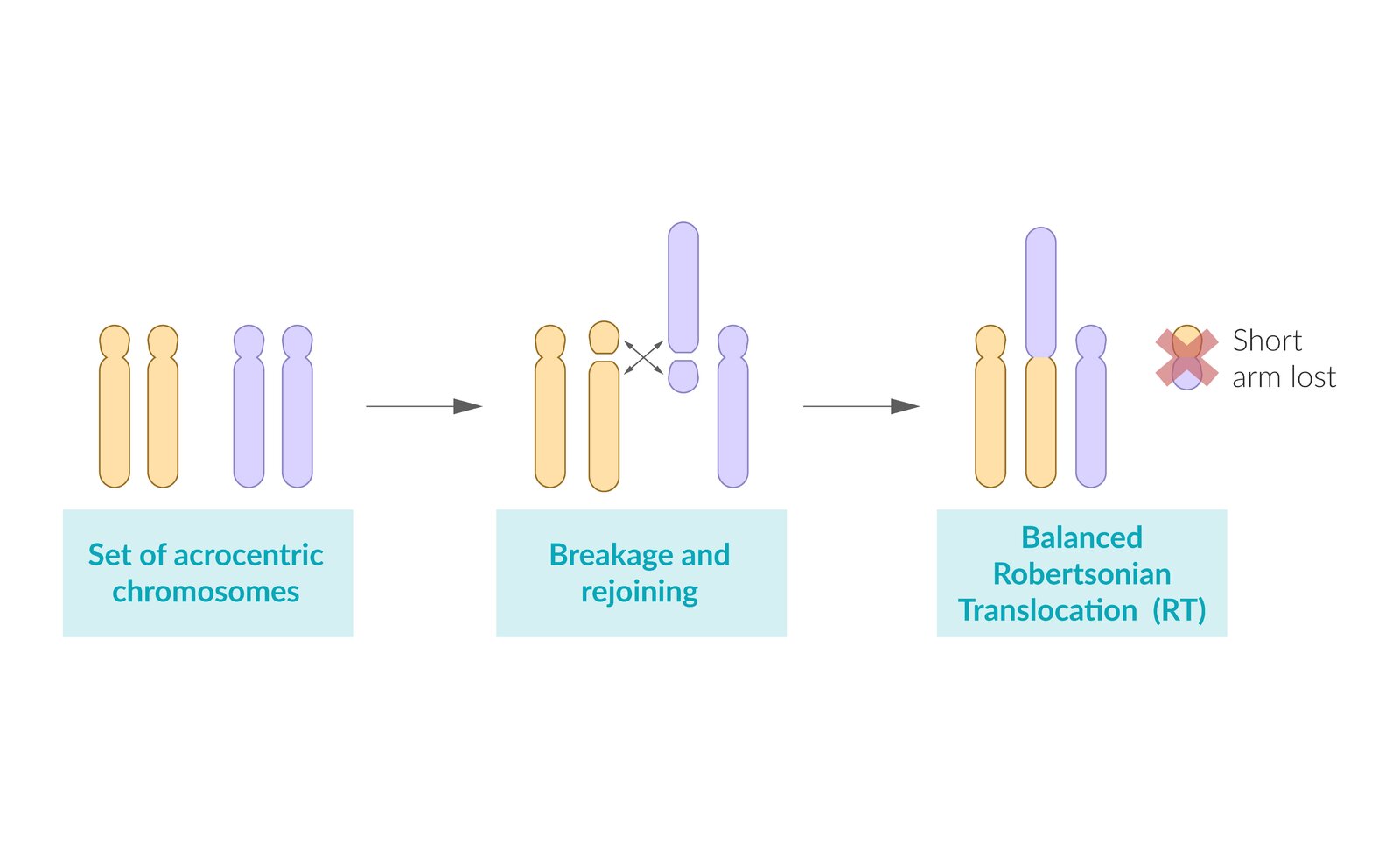
- Definition: : three copies of chromosome 21 are present, one of which is attached to another chromosome, usually chromosome 14 (less likely attached to chromosomes 13, 15, or 22)
- Occurrence: : independent of maternal age; occurs as a spontaneous translocation
-
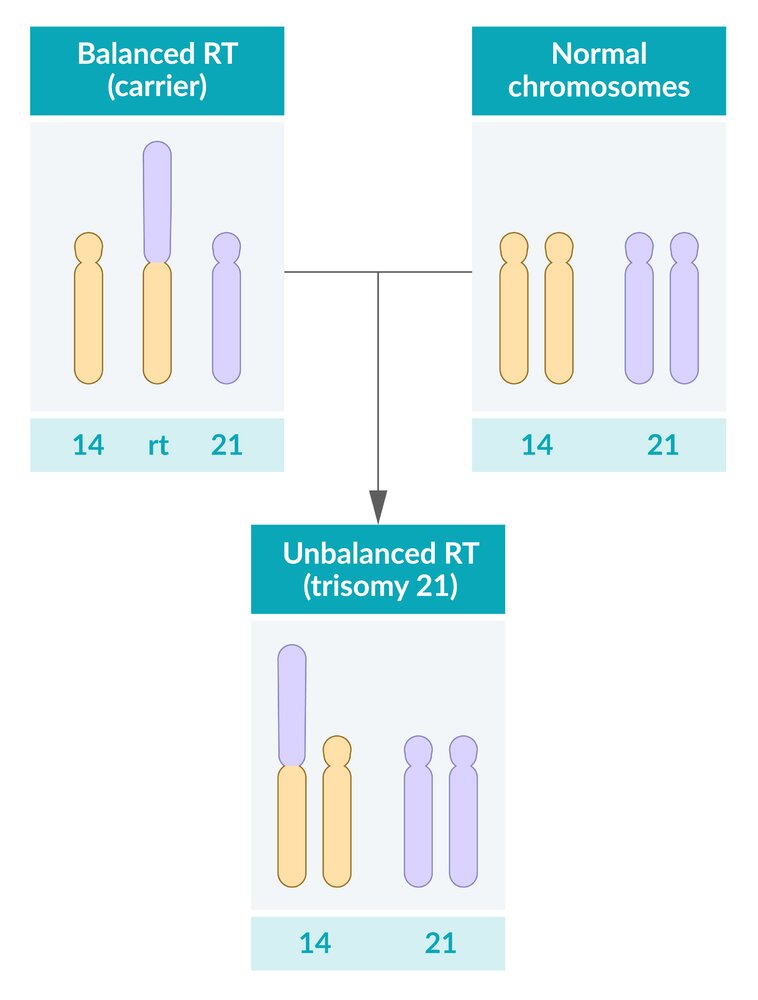
Pathogenesis and karyotype: Carriers of balanced Robertsonian translocation have a normal phenotype. Children of a translocation carrier can inherit a normal karyotype, balanced translocation, or unbalanced translocation (trisomy 21).
-
In approx. 50% of cases, a balanced translocation is inherited from a parent, usually the mother, who does not show phenotypic expression of trisomy 21. [5]
-
Balanced Robertsonian translocation: translocation of the long arm of chromosome 21 to the long arm of chromosome 14
- Karyogram shows a total number of 45 chromosomes and may be expressed as either ♀: 45,XX,t(14;21) or ♂: 45,XY,t(14;21)
- Affected individuals inherit a balanced translocation from their phenotypically normal parent.
-
Unbalanced Robertsonian translocation: clinical features of trisomy 21 caused by inheritance of a translocation chromosome and a normal chromosome
- Although there are only 46 chromosomes present, there are three copies of genetic material from chromosome 21.
- Results in the karyotypes ♀: 46,XX,+21,t(14;21) and ♂: 46,XY,+21,t(14;21)
- Pregnancy can end in miscarriage. [6]
-
Balanced Robertsonian translocation: translocation of the long arm of chromosome 21 to the long arm of chromosome 14
- The other cases of balanced Robertsonian translocation are caused by new translocations during meiosis.
-
In approx. 50% of cases, a balanced translocation is inherited from a parent, usually the mother, who does not show phenotypic expression of trisomy 21. [5]
")


Mosaic trisomy 21 (1–2% of cases)
- Definition: two cell lines are present, the trisomy 21 cell line and the normal cell line
-
Pathogenesis
- Nondisjunction during mitosis that occurs after fertilization
- Depending on the timing of the mitotic error, there is a variable proportion of trisomic and normal cells.
- Phenotypic expression varies according to the ratio of healthy to trisomic cells.
- Karyotype: either ♀: 46,XX/47,XX,+21 or ♂: 46,XY/47,XY,+21
Although symptoms may be less severe in mosaic trisomies, the clinical manifestation generally provides no indication of the underlying genetic mutation.
To remember that Down syndrome is caused by trisomy 21, think of the Drinking age of 21 (in the US).
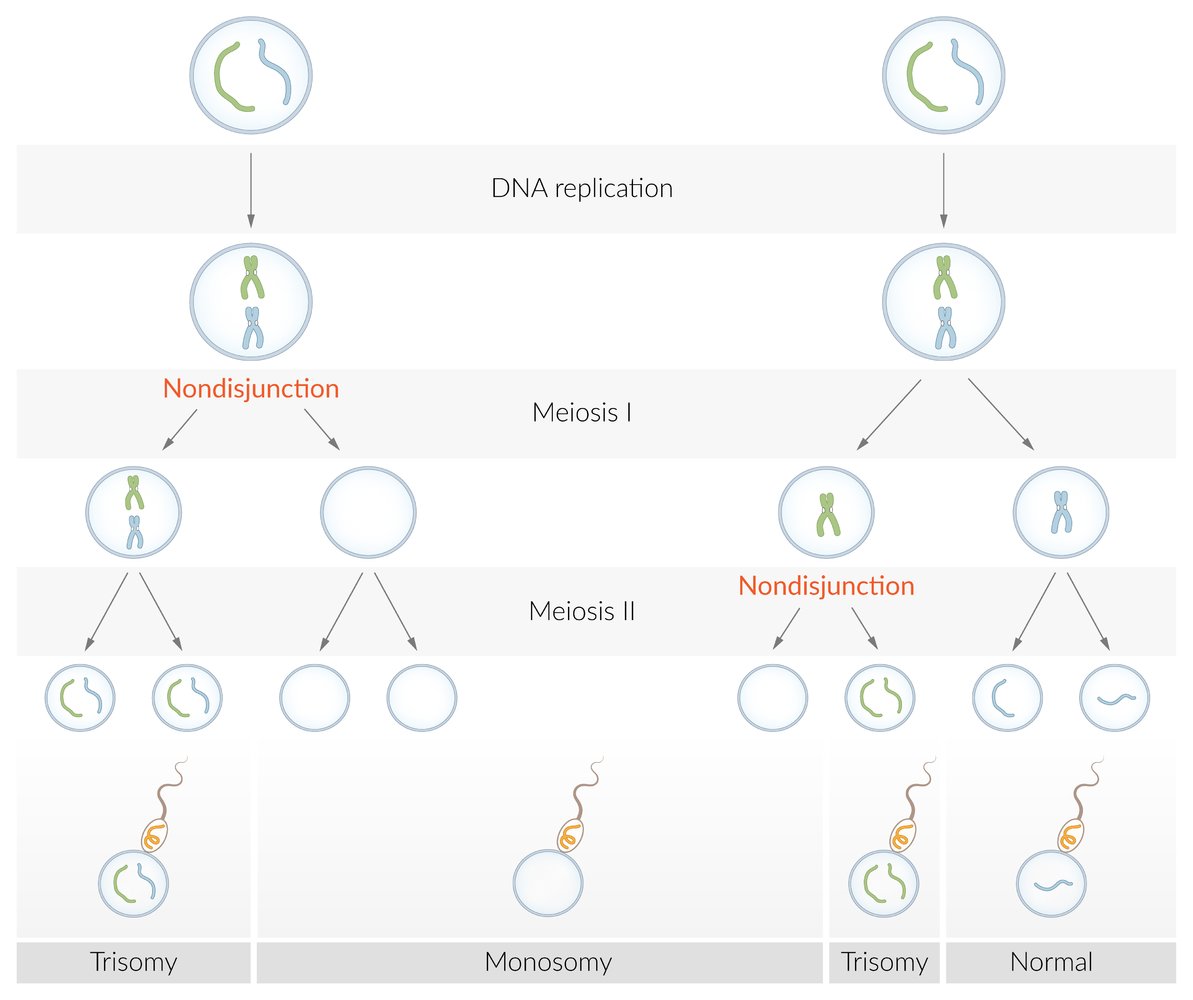
A numeric chromosome aberration, i.e., a differing number of chromosomes, can occur through an incorrect distribution of chromosomes during meiosis. The homologous chromosome pairs usually separate during the reduction division (meiosis I), while the homologous sister chromatids do so during the equational division (meiosis II).
The occurrence of nondisjunction during one of these two steps leads to the development of aneuploid gametes, in which the chromosome is either duplicated (24 chromosomes in total) or missing (only 22 chromosomes in total). This results in trisomy (e.g., trisomy 21) or monosomy (e.g., Turner syndrome).
© AMBOSS
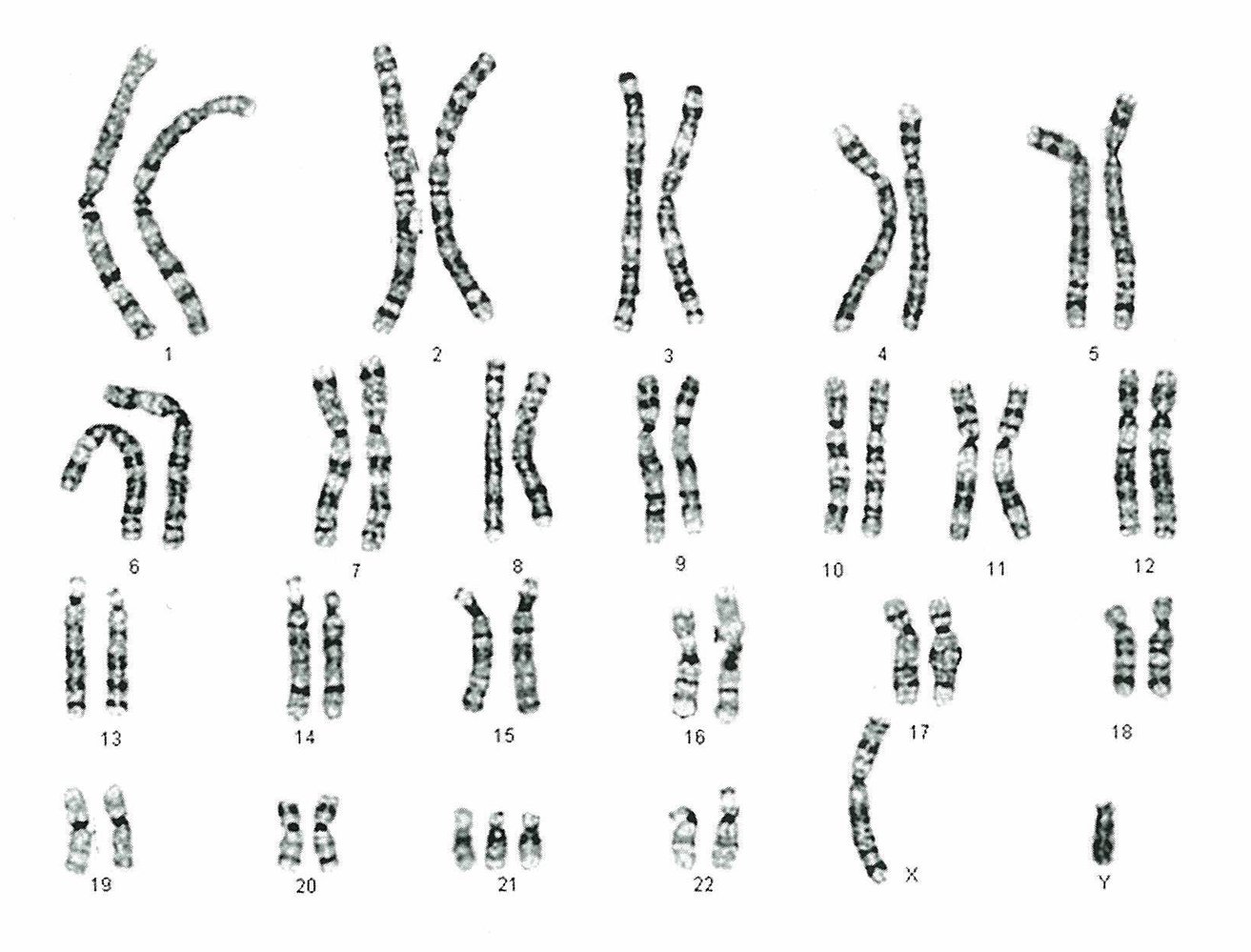
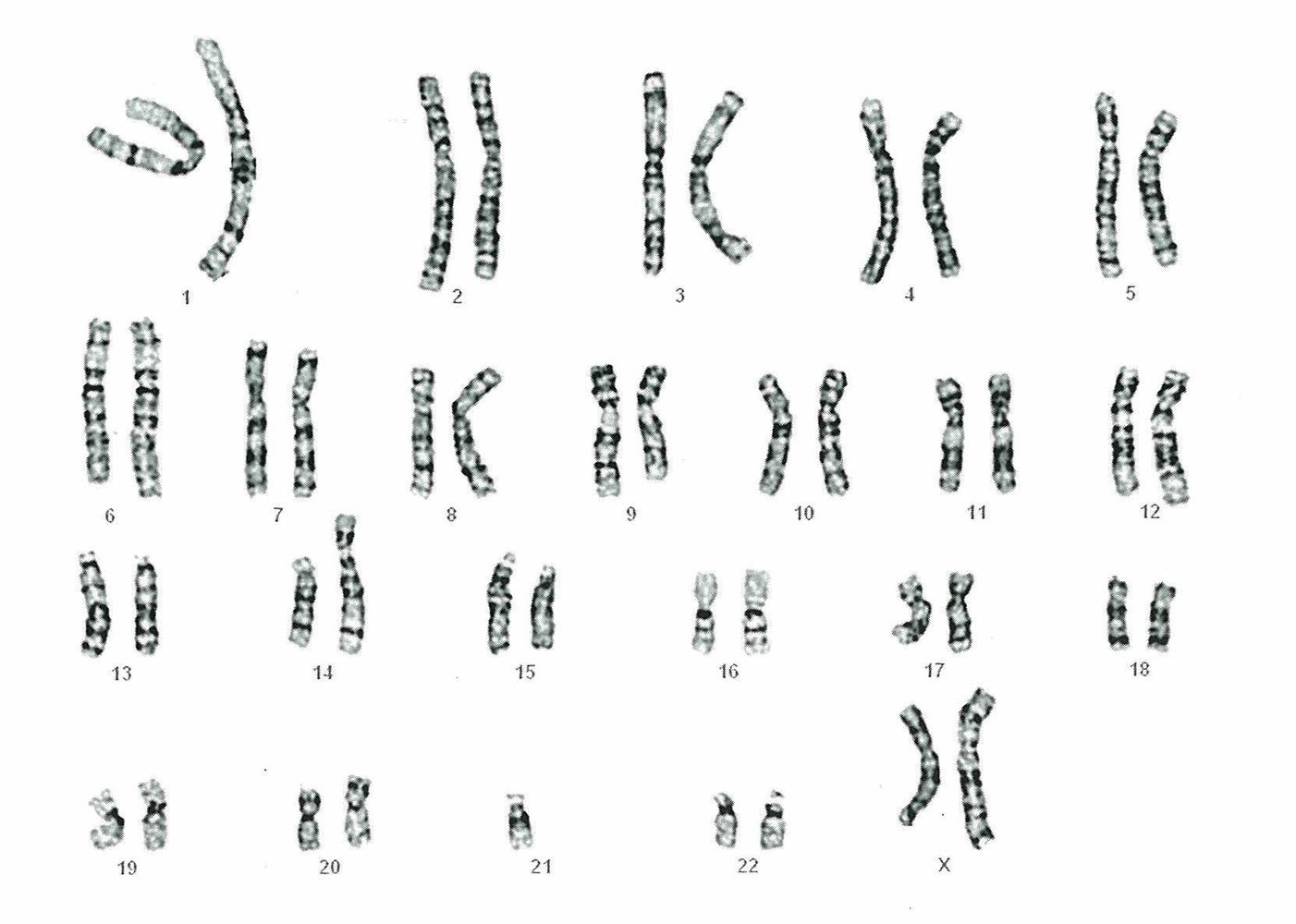
The karyogram for karyotype 47,XY,+21 shows three complete copies of chromosome 21 and a total of 47 chromosomes.
Source: © IMPP
© AMBOSS
The karyogram for karyotype 45,XX,t(14;21) shows the translocation of the long arm of chromosome 21 to the long arm of chromosome 14 with the elimination of the respective short arms and fusion of the chromosomes.
Source: © IMPP
© AMBOSS
Clinical features
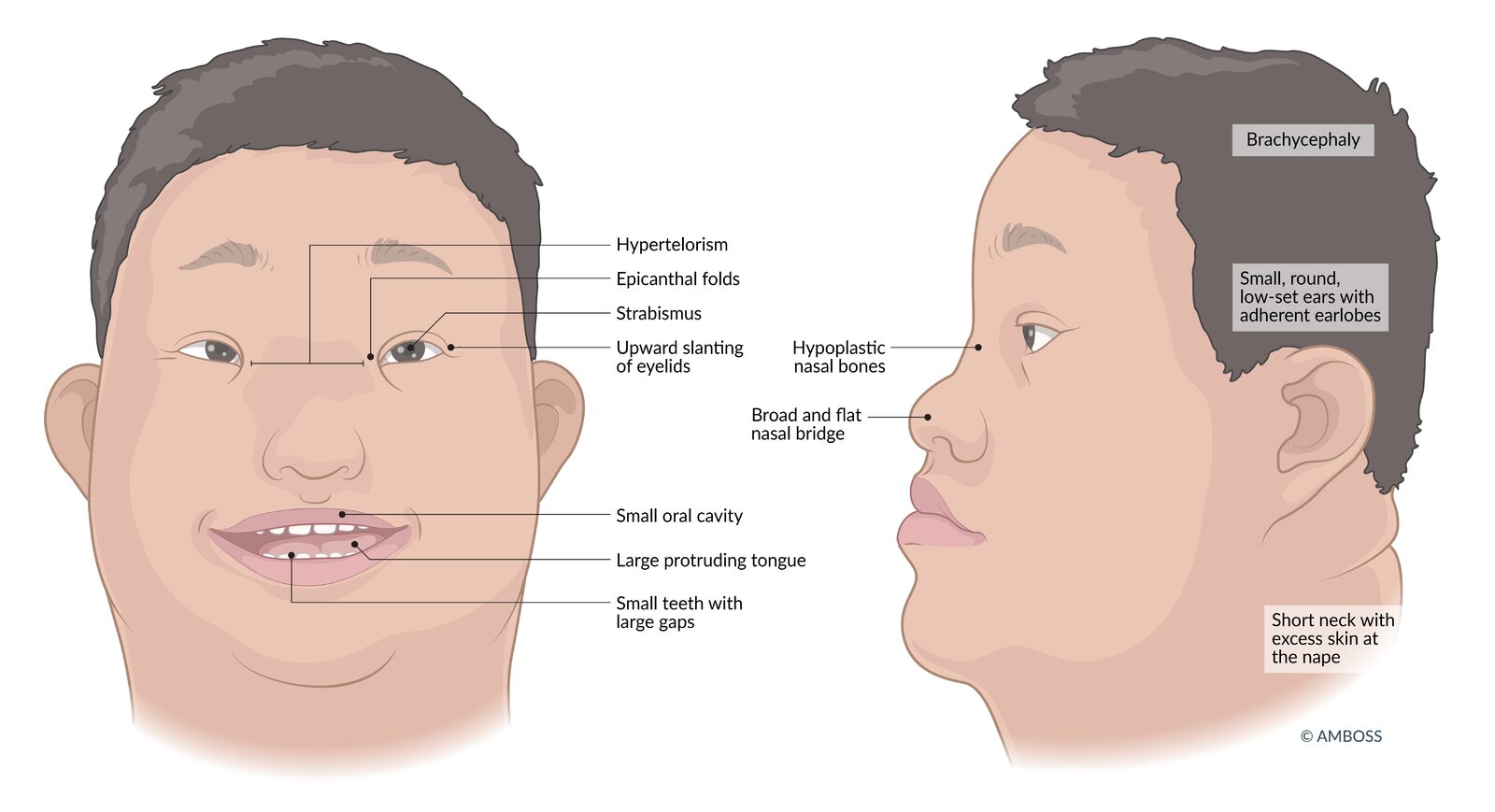
Facial and cranial features (craniofacial dysmorphia)
-
Eyes
- Upward-slanting palpebral fissures
- Epicanthal folds
- Ocular hypertelorism: a distance between the eyes greater than the 95th percentile
- Brushfield spots: an aggregation of connective tissue in the periphery of the iris, visible as white or grayish-brown spots.
- Refractive errors (e.g., myopia, astigmatism)
- Strabismus
- Cataracts (congenital, infantile, or juvenile) [7]
-
Mouth
- A small oral cavity together with a large and furrowed tongue results in the appearance of a protruding tongue.
- High arched and narrow palate [8]
- Teeth: late development, small size with short roots, large gaps between teeth
-
Further features
- Brachycephaly
- Hypoplastic nasal bones, broad and flat nasal bridge
- Ear anomalies (small, round, low-set ears, adherent earlobes)
- Short neck, excess skin at the nape of the neck (may be seen on prenatal ultrasound)


Extremities, soft tissue, and skeletal features
-
Extremities
- Transverse palmar crease: single crease that runs across the palm, along the metacarpophalangeal joints perpendicular to the fingers [9]
- Sandal gap: a medial displacement of the first toe leading to a large space between the first and second toes [10]
- Clinodactyly; : abnormal curvature of a finger (typically refers to inward curvature of the 5th finger)
-
Camptodactyly
- A congenital, fixed digital flexion deformity most often seen in the 5th digit
- Associated with several congenital syndromes, including Down syndrome
- Brachydactyly
-
Soft tissue
- Connective tissue deficiency → ↑ risk of umbilical and inguinal hernias
- Marked hyperextension of joints
- Obesity: prevalence is approx. 50% (higher than in the general population) [11]
-
Skeletal features
- Atlantoaxial instability
-
Short stature
- Reduced growth with shortening of long bones
- Average adult height: 150 cm (4 ft 11 in) [12]


Organ malformations and associated conditions
-
Heart: congenital heart defects in trisomy 21 (∼ 50% of cases) [13]
- Atrioventricular septal defect (endocardial cushion defect) is the most common heart defect in individuals with Down syndrome.
- Ventricular septal defect
- Atrial septal defects
- Tetralogy of Fallot
- Patent ductus arteriosus
-
Gastrointestinal tract
- Duodenal atresia/stenosis
- Annular pancreas
- Anal atresia
- Megacolon
- Rectal prolapse
- Hirschsprung disease
-
Urogenital system
- Hypogonadism
- Cryptorchidism
- Decreased fertility in men
-
Further features
- Hypothyroidism
- Type 1 diabetes
- Celiac disease
- Obstructive sleep apnea
- Hearing loss due to recurrent otitis media
- Increased risk of leukemia (acute lymphoblastic leukemia, acute myeloid leukemia)
- Early-onset Alzheimer disease; (The amyloid precursor protein; , which generates amyloid beta, is located on chromosome 21.)
- Increased risk of developing epilepsy
Development
-
Motor skills
- Delayed motor development
- Muscle hypotonia
-
Intelligence
- Varying levels of intellectual disability (average IQ: 50) [14]
- Apparent within the first 12 months: Developmental milestones (e.g., sitting, walking, talking) are achieved at approximately twice the age of children without Down syndrome. [15]
-
Behavioral and psychiatric disorders
- Behavioral disorders
- ADHD
- Conduct disorder
- Autism spectrum disorder
- Behavioral disorders
Down syndrome is the most common genetic cause of intellectual disability.
To remember the most important features associated with Down syndrome, think of the 5 A's: Advanced maternal age, duodenal Atresia, Atrioventricular septal defect, AML/ALL, early onset of Alzheimer disease.

Upward slanting of the eyelids, prominent epicanthal folds (resulting in almond-shaped eyes), broad and flat nasal bridge, prominent tongue due to macroglossia and muscular hypotonia, low-set ears, and a short neck.
© AMBOSS
© AMBOSS

A single transverse palmar crease is visible running along the metacarpophalangeal joints perpendicular to the fingers.
This finding is consistent with genetic chromosomal abnormalities such as trisomy 21 but may also be seen in individuals without such conditions.
Source: “Single transverse palmar crease adult” by WurdBendur, Wikimedia Commons, licensed under CC BY-SA 4.0.
{kind=link}

There is medial displacement of the first toe leading to a large space between the first and second toes.
This anatomical variant may be a manifestation of Down syndrome but can also be seen in individuals without this condition.
Source: “Feet of a boy with Down Syndrome” by Loranchet, Wikimedia Commons, licensed under CC BY 3.0.
{kind=link}
Diagnosis
Diagnostic approach
- Diagnosis of Down syndrome is primarily prenatal and the diagnostic approach is dependent on the week of gestation.
- Initial screening test
- Standard tests
- First-trimester combined test (11–13 weeks)
- Second-trimester quadruple test (15–18 weeks)
- Additional tests, usually performed optionally in high-risk pregnancies (e.g., maternal age > 35 years, history of prior pregnancy with trisomy, ultrasound features suggesting aneuploidy) [16][17]
- Integrated tests over the first and second trimesters
- Cell-free DNA (10–20 weeks)
- Standard tests
- If any of the above screening tests yield an abnormal result, one of the following confirmatory diagnostic tests is performed:
- Amniocentesis (15–22 weeks)
- Chorionic villus sampling (9–14 weeks)
- Percutaneous umbilical cord sampling (18–22 weeks)
- See “Prenatal diagnostics.”
Prenatal screening
Counseling
- Precedes screening procedures
- Provides information that screening is voluntary
- Explains the option of terminating the pregnancy if trisomy 21 is diagnosed
Screening procedures
- Indication: recommended for all women prior to the 20th week of gestation
-
Combined test (first trimester) (11–13 weeks)
- Has a 90% detection rate [18]
-
Maternal serum
- ↑ Beta human chorionic gonadotropin (β-hCG)
- ↓ Pregnancy-associated plasma protein A (PAPP-A)
-
Ultrasound
- Nuchal translucency; measurement: nuchal translucency increases due to the large amount of fluid collecting behind the neck [19]
- Short neck, thickened nuchal fold
- Absent or hypoplastic nasal bone
- Shortened middle phalanges of the fifth digits with clinodactyly
- Shortened long bones (humerus, femur)
-
Quadruple test (second trimester) (15–18 weeks)
- ↓ Free estriol
- ↓ Alpha-fetoprotein (AFP)
- ↑ Inhibin A
- ↑ β-hCG
-
Additional screening tests: The following tests are optional and performed in addition to the above-mentioned tests, and they are evaluated along with the results of the second-trimester quadruple test.
- Sequential integrated test: combines the results from the first-trimester combined test and second-trimester quadruple test
-
Cell-free fetal DNA (10–20 weeks): fetal DNA is isolated from a maternal blood specimen and evaluated for chromosomal abnormalities [20]
- Noninvasive (for the fetus) but expensive test
- More predictive in women with a high risk
- The test is currently available but not guideline-recommended.
In the quadruple test, hCG and Inhibin A are both HIgh up (↑) and Estriol and α-fEtoprotein are both dEficient (↓).


Fetal karyotyping (confirmatory test)
-
Indications
- Positive screening test
- Previous trisomy 21 pregnancy
- Parent with known chromosomal translocation or aberration
-
Procedures [21]
- Chorionic villus sampling (9–14 weeks)
- Amniocentesis (15–22 weeks)
- Percutaneous umbilical cord sampling (18–22 weeks) [22]
-
Complications
- Bleeding
- Infection
- Fetal injury
- Amniocentesis has a lower risk of fetal loss compared to chorionic villus sampling.
Postnatal diagnostics
- Chromosome analysis
- Screening for associated conditions (see “Clinical features”), e.g., echocardiography to detect heart defects
Typical features and malformations are important indicators but diagnostic confirmation is still required.

Ultrasound of a fetal head and neck during the first trimester (sagittal view)
There is an anechoic region of subcutaneous fluid collection in the posterior portion of the neck (green overlay) measuring 1.57 mm.
This value is used to calculate the statistical risk for fetal chromosome disorders. A nuchal translucency measurement >3 mm is considered abnormal.
© AMBOSS

Ultrasound of a fetal head and neck during the first trimester (sagittal view; nuchal translucency scan)
There is an increased depth of the nuchal translucency (yellow cursors; green overlay). The nasal bone is also absent.
These findings are consistent with Down syndrome.
Source: “Nuchal edema in Down Syndrome Dr. W. Moroder” by Dr. W. Moroder, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
Differential diagnoses
- Isolated hypotonia
- Zellweger syndrome
- Congenital hypothyroidism
- Trisomy 13
- Trisomy 18
- Williams syndrome
- Turner syndrome
The differential diagnoses listed here are not exhaustive.
Treatment
- Evaluation, monitoring, and treatment of the symptom complex and malformations as necessary (e.g., cardiac screening with an echocardiogram and heart surgery for cardiac malformations)
- Early, targeted intervention, educational programs, and support
- Physical therapy
- Behavioral therapy
- Speech therapy
- Occupational therapy
Prognosis
- Decreased life expectancy with an average lifespan of approx. 60 years [23]
- Common causes of death in individuals with Down syndrome (in decreasing order of incidence) [24][25]
- Infections, particularly pneumonia
- Congenital malformations, particularly congenital heart diseases
- Circulatory diseases (e.g., coronary artery disease)
- Dementia
References
- "Birth Defects - Data and Statistics". https://web.archive.org/web/20170512194729/https://www.cdc.gov/ncbddd/birthdefects/data.html. [2014-10-21]
- "Data & Statistics on Birth Defects". https://web.archive.org/web/20200630200725/https://www.cdc.gov/ncbddd/birthdefects/data.html. [2020-01-23]
- "What is Down Syndrome?". https://www.ndss.org/about-down-syndrome/down-syndrome/. [2020-01-01]
- Antonarakis SE, Petersen MB, McInnis MG, et al. "The meiotic stage of nondisjunction in trisomy 21: determination by using DNA polymorphisms.". Am J Hum Genet. 50(3). :544-50. (1992)
- Shaffer LG, Jackson-Cook CK, Stasiowski BA, Spence JE, Brown JA.. "Parental origin determination in thirty de novo Robertsonian translocations.". American Journal of Medical Genetics. (1992)
- Priya PK, Mishra VV, Roy P, Patel H. "A Study on Balanced Chromosomal Translocations in Couples with Recurrent Pregnancy Loss.". Journal of Human Reproductive Sciences. (2018)
- Haargaard B, Fledelius HC. "Down's syndrome and early cataract". Br J Ophthalmol. 90(8). :1024-1027. (2006)
- Klingel D, Hohoff A, Kwiecien R, Wiechmann D, Stamm T. "Growth of the hard palate in infants with Down syndrome compared with healthy infants-A retrospective case control study.". PLoS ONE. 12(8). :e0182728. (2017)
- "Single Palmar Crease - Medline Plus - U.S. National Library of Medicine (NIH)". https://medlineplus.gov/ency/article/003290.htm. [2019-05-17]
- Ryu JK, Cho JY, Choi JS. "Prenatal sonographic diagnosis of focal musculoskeletal anomalies.". Korean journal of radiology. 4(4). :243-51
- Bertapelli F, Pitetti K, Agiovlasitis S, Guerra-Junior G. "Overweight and obesity in children and adolescents with Down syndrome—prevalence, determinants, consequences, and interventions: A literature review". Res Dev Disabil. 57. :181-192. (2016)
- Edgren G, Hjalgrim H, Rostgaard K, et al. "Risk of gastric cancer and peptic ulcers in relation to ABO blood type: a cohort study". Am J Epidemiol. 172(11). :1280-1285. (2010)
- Stoll C, Alembik Y, Dott B, Roth MP. "Study of Down syndrome in 238,942 consecutive births.". Ann Genet. 41(1). :44-51. (1998)
- Boleracki M, Farkas F, Meszely A, Szikszai Z, Sik Lányi C. "Developing an Animal Counting Game in Second Life for a Young Adult with Down Syndrome.". Stud Health Technol Inform. 217. :71-7. (2015)
- Winders P, Wolter-Warmerdam K, Hickey F. "A schedule of gross motor development for children with Down syndrome". Journal of Intellectual Disability Research. 63(4). :346-356. (2018)
- Bianchi DW, Parker RL, Wentworth J, et al. "DNA Sequencing versus Standard Prenatal Aneuploidy Screening". N Engl J Med. 370(9). :799-808. (2014)
- N.J. Wald, H.C. Watt, A.K. Hackshaw. "Integrated Screening for Down's Syndrome Based on Tests Performed during the First and Second Trimesters". N Engl J Med. 341(7). :461-467. (1999)
- Santorum M, Wright D, Syngelaki A, Karagioti N, Nicolaides KH. "Accuracy of first-trimester combined test in screening for trisomies 21, 18 and 13". Ultrasound in Obstetrics & Gynecology. 49(6). :714-720. (2017)
- "Nuchal translucency". https://radiopaedia.org/articles/nuchal-translucency-1
- Grace MR, Hardisty E, Dotters-Katz SK, Vora NL, Kuller JA. "Cell-Free DNA Screening: Complexities and Challenges of Clinical Implementation.". Obstet Gynecol Surv. 71(8). :477-87. (2016)
- "Down Syndrome Tests". https://medlineplus.gov/lab-tests/down-syndrome-tests/. [2019-06-01]
- Ghi T, Sotiriadis A, Calda P, et al. "ISUOG Practice Guidelines: invasive procedures for prenatal diagnosis". Ultrasound in Obstetrics & Gynecology. 48(2). :256-268. (2016)
- "Down syndrome". https://www.mayoclinic.org/diseases-conditions/down-syndrome/symptoms-causes/syc-20355977#:~:text=Life%20expectancy&text=Today%2C%20someone%20with%20Down%20syndrome,the%20severity%20of%20health%20problems.
- Colvin KL, Yeager ME. "What people with Down Syndrome can teach us about cardiopulmonary disease". European Respiratory Review. 26(143). :160098. (2017)
- Alan H. Bittles, Carol Bower, Rafat Hussain, Emma J. Glasson. "The four ages of Down syndrome". European Journal of Public Health. (2006)
- "Epocrates - Down Syndrome". https://online.epocrates.com/diseases/70035/Down-syndrome/Differential-Diagnosis. [2019-07-09]
- Tabor A, Vestergaard CH, Lidegaard Ø. "Fetal loss rate after chorionic villus sampling and amniocentesis: an 11-year national registry study.". Ultrasound Obstet Gynecol. 34(1). :19-24. (2009)
- "Growth Charts for Children with Down Syndrome". https://web.archive.org/web/20201016230730/https://www.cdc.gov/ncbddd/birthdefects/downsyndrome/growth-charts.html. [2019-12-05]