Summary
Elbow dislocation is an atypical separation of the radial, ulnar, and humeral joint surfaces. A posterior dislocation of the elbow is common and is typically caused by a fall on an outstretched hand. Clinical features include pain, swelling, visible deformity, and reduced active range of motion of the joint. An elbow dislocation is classified as complex if there is an associated fracture. Diagnosis is confirmed with radiography. Elbow dislocations without an associated fracture are managed conservatively with closed reduction and immobilization. Complex elbow dislocations require surgery with open reduction and internal fixation. Complications of elbow dislocation include nerve injury, brachial artery injury, joint instability, and posttraumatic stiffness.
See “Radial head subluxation” for information on partial dislocation of the head of the radius at the radio-humeral joint.
Epidemiology
- The second most frequently dislocated joint (after the shoulder joint) [1]
- Sex: ♂ > ♀ [2]
- Peak incidence: 10–20 years of age [3]
Epidemiological data refers to the US, unless otherwise specified.
Etiology
Elbow dislocations are most commonly caused by sports-related trauma (e.g., falls while cycling, skating, or performing gymnastics). [3]
- A fall on an outstretched hand (most common) causes posterior elbow dislocation.
- Posterior, direct trauma to a flexed elbow causes anterior elbow dislocation.
- Medial or lateral trauma to the elbow causes medial or lateral elbow dislocation.
- High-impact trauma to the elbow causes divergent elbow dislocation.
Classification
Elbow dislocations are classified by anatomical position and complexity.
Anatomical position [3]
The type of dislocation is defined by the position of the ulna relative to the olecranon.
- Posterior dislocation (most common)
- Anterior dislocation
- Medial dislocation
- Lateral dislocation
- Divergent dislocations (rare)
Complexity [4]
- Simple dislocation: no concomitant fracture
-
Complex dislocation: one or more associated fractures
- Radial head
- Ulnar coronoid process
- Terrible triad of the elbow: fractures of both the radial head and coronoid process and disruption of the medial collateral ligament

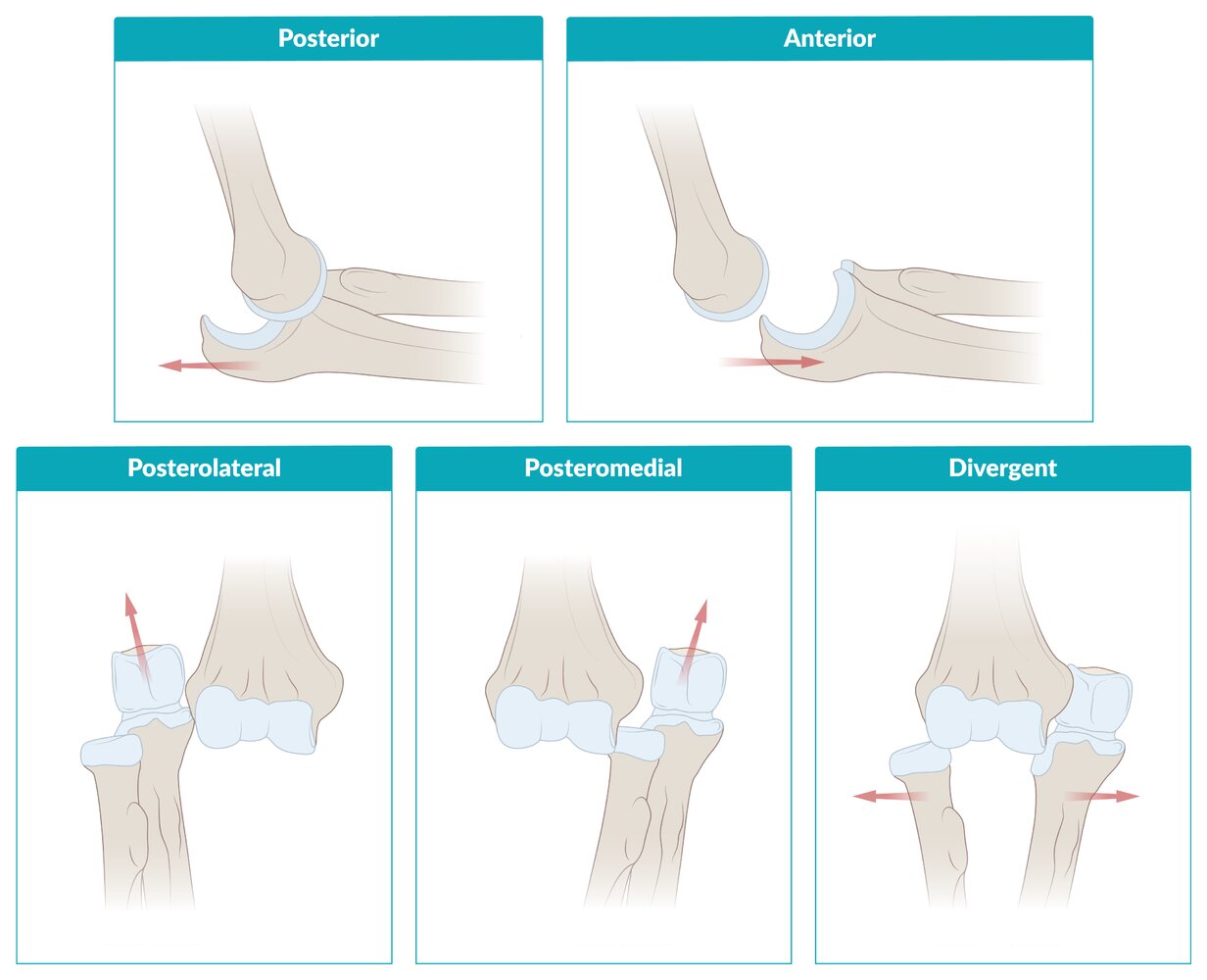
The type of dislocation is defined by the position of the ulna relative to the olecranon.
© AMBOSS
Clinical features
- Pain and/or swelling of the elbow
- Reduced active range of motion [3]
- Posterior dislocation: Patient typically holds elbow at 45° of flexion.
- Anterior dislocation: Patient typically holds elbow in extension.
- Visible deformity [3]
- Prominent olecranon
- Posterior dislocation: shortened forearm
- Anterior dislocation: lengthened forearm
- Anesthesia, paresthesias, and/or weakness [3]
- Ulnar nerve palsy and/or median nerve palsy (most common)
- Radial nerve palsy and/or posterior interosseous neuropathy (uncommon)
- Signs of vascular injury and/or signs of acute limb ischemia (rare)
If the elbow has spontaneously reduced before examination, patients may present with only swelling, pain, and/or tenderness. [1]
Diagnosis
Clinical evaluation [1]
-
Visual inspection
- Assess for gross deformities (e.g., olecranon prominence, forearm shortening).
- Evaluate skin for laceration, tearing, bruising, and/or tenting.
-
Neurovascular examination
- Assess pulses in the brachial artery, radial artery, and ulnar artery.
- Test capillary refill time.
- Evaluate for median nerve injury , radial nerve injury , and ulnar nerve injury.
Intact distal pulses do not exclude brachial artery injury. Obtain arteriography and consult vascular surgery if arterial injury is suspected. [1]
")



Imaging [1][5]
X-ray of the elbow
-
Views [3]
- Anteroposterior and lateral: all patients
- Oblique: patients with suspected medial epicondyle fracture (most common in pediatric patients) [3]
-
Findings
- Type of dislocation (i.e., position of ulna relative to olecranon)
- Associated fractures: typically radial head, ulnar coronoid, and/or distal humerus
- Posterior fat pad sign: suggests a fracture of the humerus and/or radial head [6]
-
Radiocapitellar line: a line drawn along the axis of the radial neck on a lateral elbow x-ray
- Normally passes through the center of the capitellum
- Misalignment suggests elbow dislocation and/or radial head subluxation.






Advanced testing
- CT elbow: may be used in situations where additional diagnostic detail is required
- Detection of subtle fractures despite negative or inconclusive x-ray
- Evaluation of complexity (e.g., intra-articular involvement, comminution) or injury extent of known fractures
- For surgical planning
- Arteriography: to evaluate for suspected brachial artery injury (e.g., thrombosis, laceration)
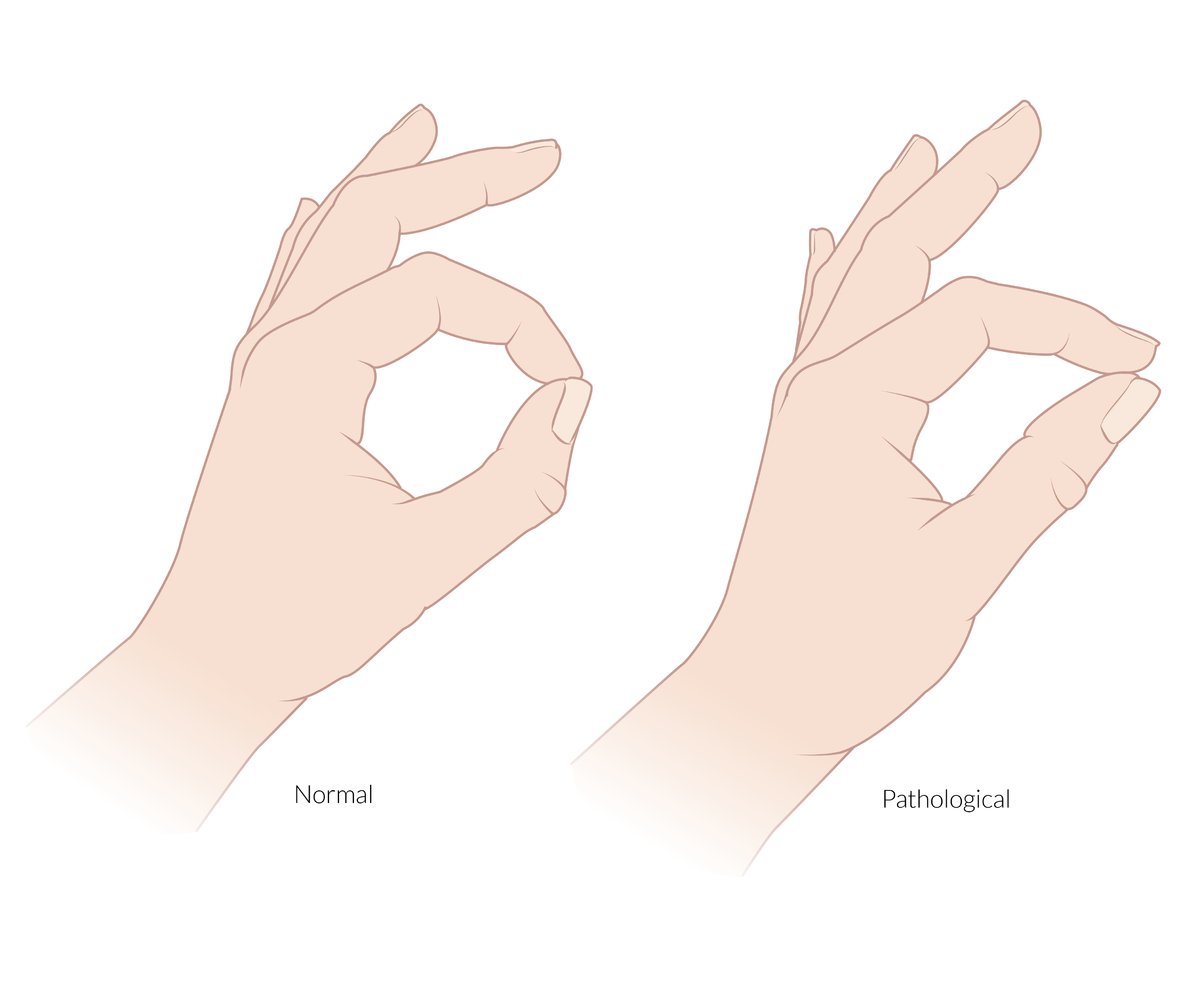
The anterior interosseous nerve is a pure motor branch of the median nerve. It supplies the flexor pollicis longus, the radial half of the flexor digitorum profundus (and the pronator quadratus).
Pinch sign: an inability to flex the DIP of the index finger and IP joint of the thumb when asked to make an “OK” sign that is caused by a lesion or entrapment of the anterior interosseous nerve
© AMBOSS

An inability to flex the index and middle fingers at the MCP and IP joints and an inability to oppose the thumb.
The hand of benediction is an active sign and is only seen when the patient is asked to make a fist. It indicates a paralysis of the thenar muscles (except the adductor pollicis), the flexor digitorum superficialis, and the radial half of the flexor digitorum profundus caused by a proximal lesion of the median nerve (above the elbow).
Also depicted is atrophy of the thenar muscles, which is seen in chronic median nerve palsy.
© AMBOSS
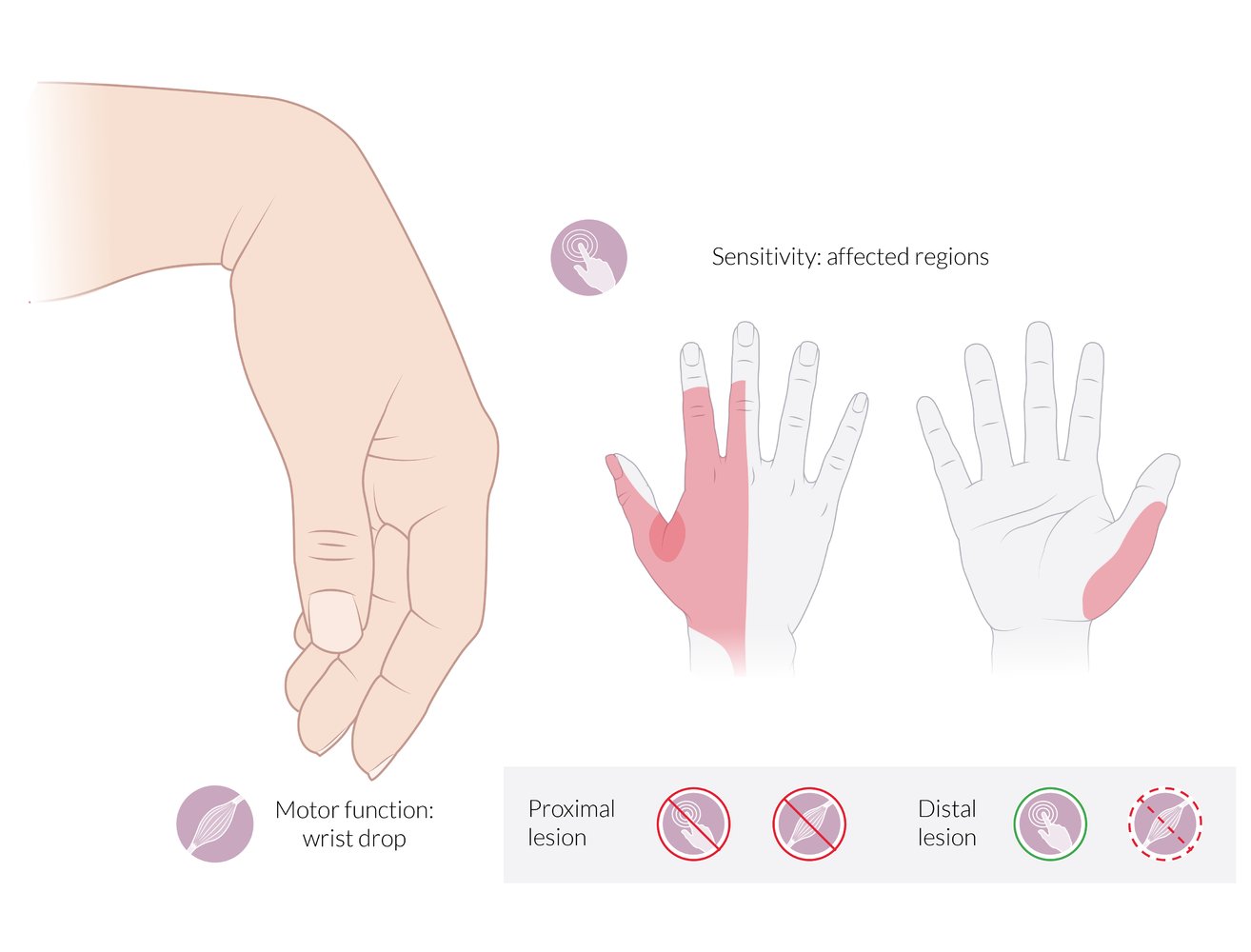
Motor deficits:
- Wrist drop: inability to extend (dorsiflex) the wrist
- Inability to extend the fingers at the MCP joints
Sensory deficits:
- Dorsal aspect: radial 2½ fingers (less commonly, 3½ fingers), excluding the tips of the 2nd and 3rd fingers. The 1st web space is the autonomous sensory zone of the radial nerve and is highlighted in red.
- Palmar aspect: the radial border of the thumb
Proximal lesion: complete loss of motor and sensory function
Distal lesion (radial tunnel syndrome): partial loss of motor function; preservation of sensory function
© AMBOSS
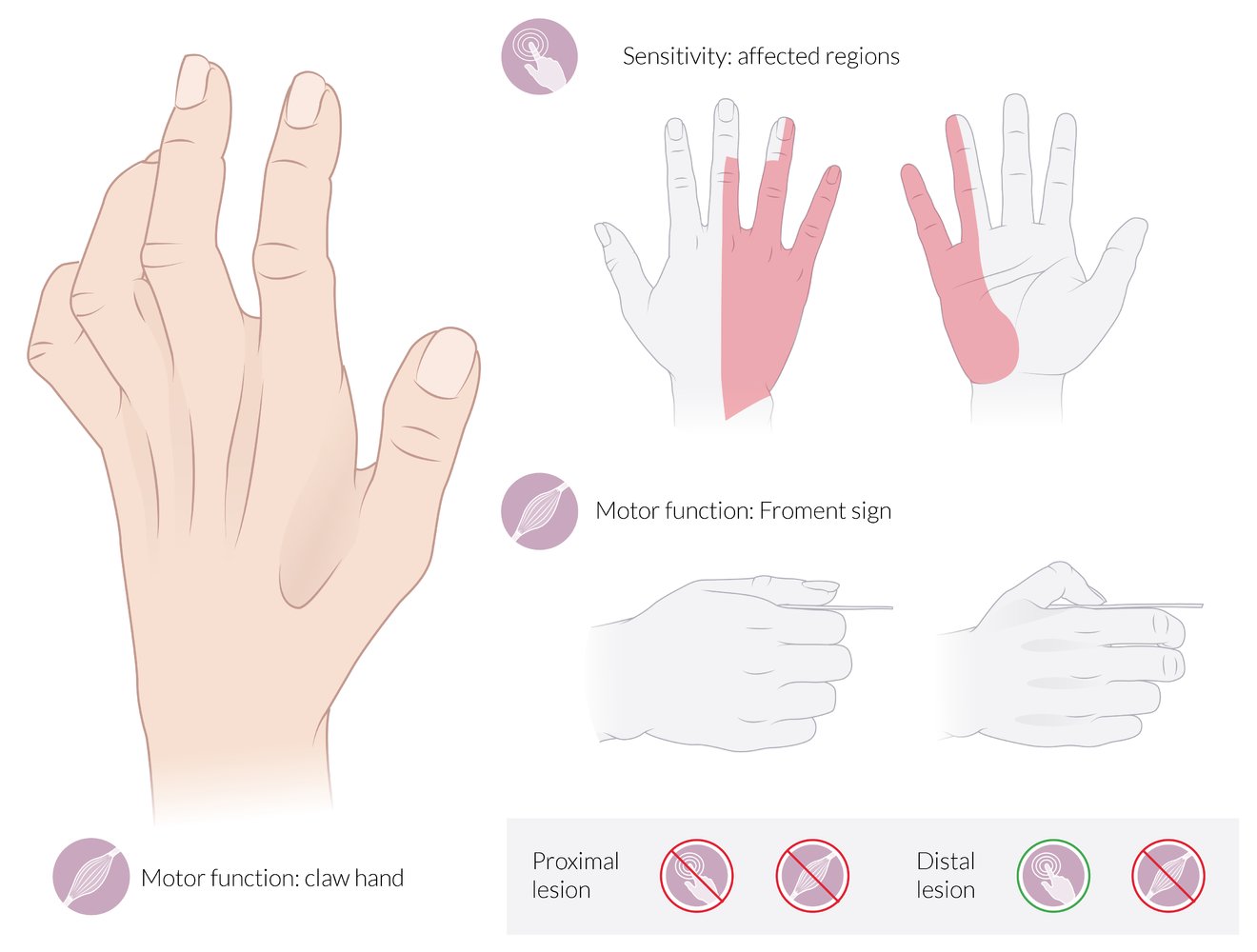
Motor deficits:
- Claw hand: The 4th and 5th joints are hyperextended at the MCP and flexed at the IP joints at rest (neutral position).
- Froment sign: The patient is asked to grasp a piece of paper between the thumb and the index finger. When the examiner tries to pull the paper away, the thumb flexes at the IP joint because the flexor pollicis longus (supplied by the median nerve) compensates for the paralyzed adductor pollicis (supplied by the ulnar nerve).
Also depicted here is hollowing of the intermetacarpal spaces and the 1st web space due to the atrophy of the interossei, which is seen in chronic ulnar nerve palsy.
Sensory deficits:
- Dorsal aspect: ulnar 2½ fingers (less commonly, 1½ fingers), excluding the tips of the 3rd and 4th fingers
- Palmar aspect: ulnar 1½ fingers
Proximal lesion: complete loss of motor and sensory functions
Distal lesion: complete loss of motor function; preservation of sensory function
© AMBOSS
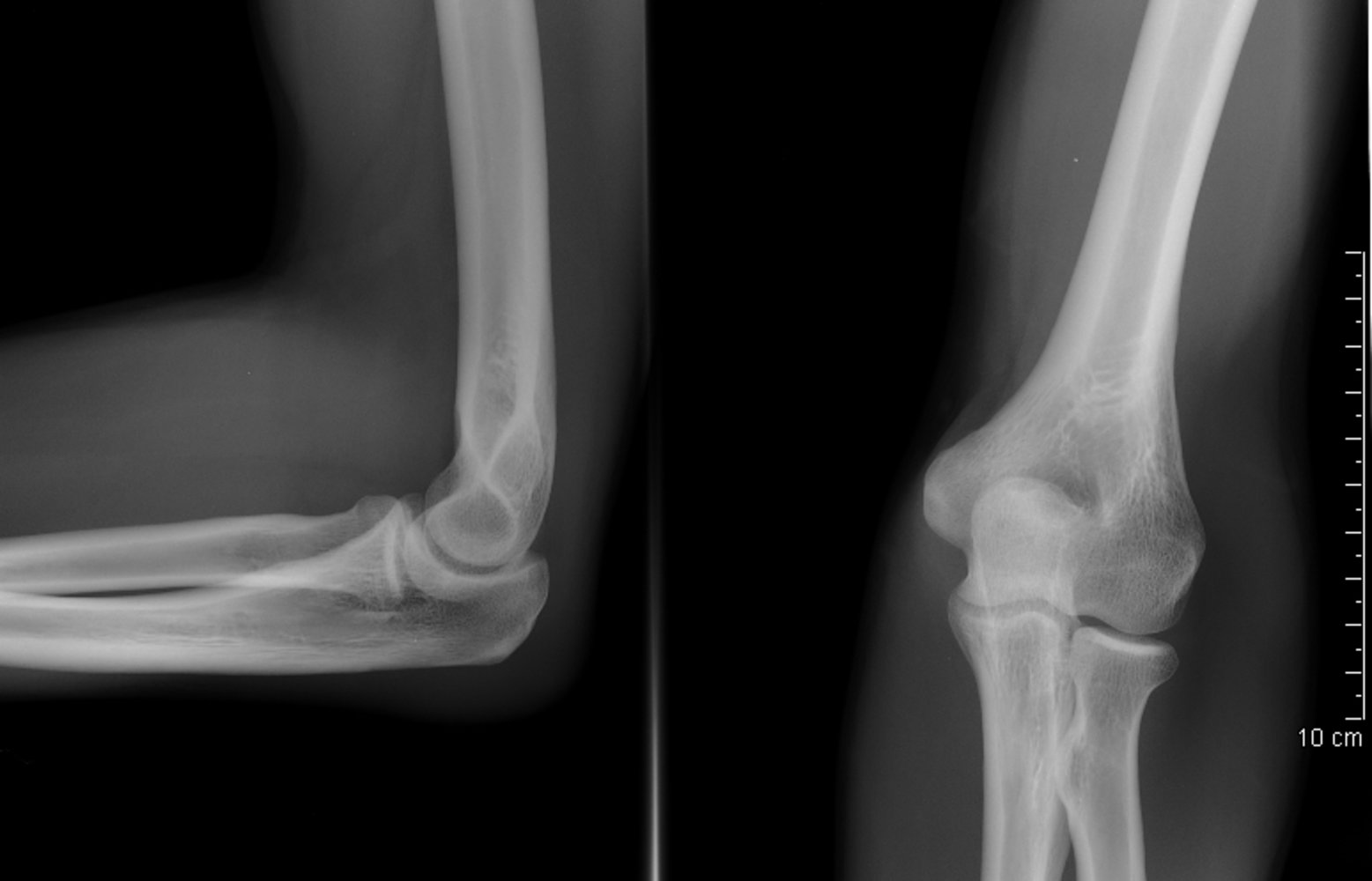
X-ray elbow (left: lateral view; right: AP view)
There is no evidence for fracture or dislocation. The anterior fat pad (white overlay on left image) is not abnormally elevated. No posterior fat pad is visible.
C: capitulum (also highlighted by green dotted line); CP: coronoid process; H: humerus; LE: lateral epicondyle; ME: medial epicondyle; OP: olecranon process (also highlighted by white line); RH: radial head; R: radius; T: trochlea (also highlighted by red-dotted line); U: ulna
Source: “Coude fp.PNG” by MB, Wikimedia Commons, licensed under CC BY 2.5. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
{kind=link}

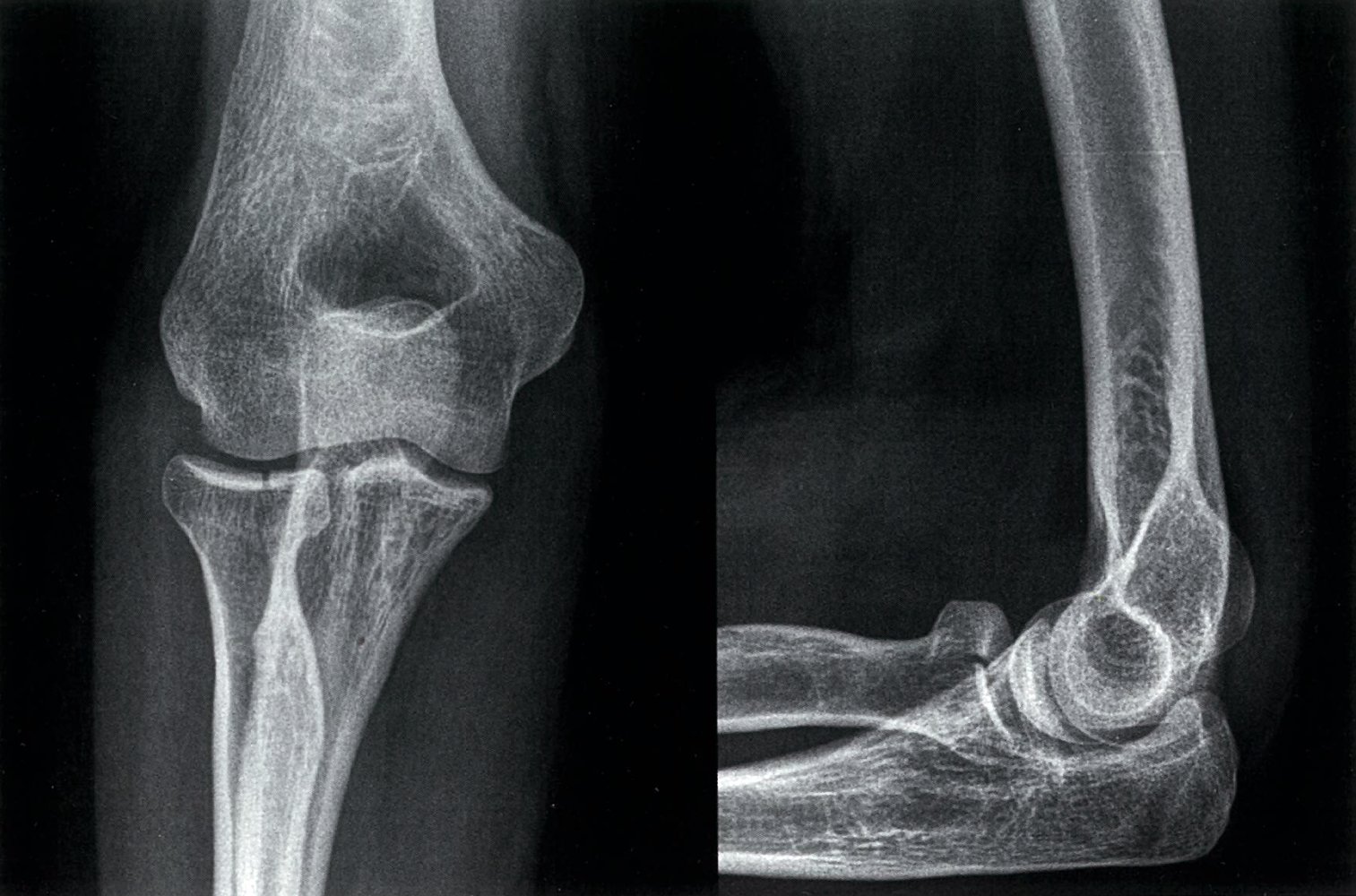
X-ray elbow (left: AP view; right: lateral view)
A posterolateral dislocation is seen (white arrows), with elevation of the posterior fat pad (red overlay) caused by a joint effusion. The dislocation is considered simple since there is no associated fracture.
Elbow dislocations may be posterolateral, posteromedial, posterior, anterior, medial, or lateral. The majority of dislocations are posterolateral or posterior. In anatomical position, the radius is located lateral to the ulna.
Green overlay: trochlear notch
Source: “Elbow2010D” by James Heilman, MD, Wikimedia Commons, licensed under CC BY-SA 3.0. Modifications: images merged (above info relates to AP image); lateral: Elbow1, https://commons.wikimedia.org/wiki/File:Elbow1.jpg, same copyright and author as AP. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
X-ray left elbow (left: AP view; right: lateral view)
The radial head fracture shows intraarticular extension and slight distraction (widening) at the fracture line (red overlay).
Source: © IMPP

X-ray right elbow (lateral view) of an adolescent
A fracture through the physis (growth plate) is accompanied by physeal widening (white dashed outline) and displacement of the olecranon process (green overlay).
Source: “Olecranon Fracture.jpg” by Benoudina samir, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
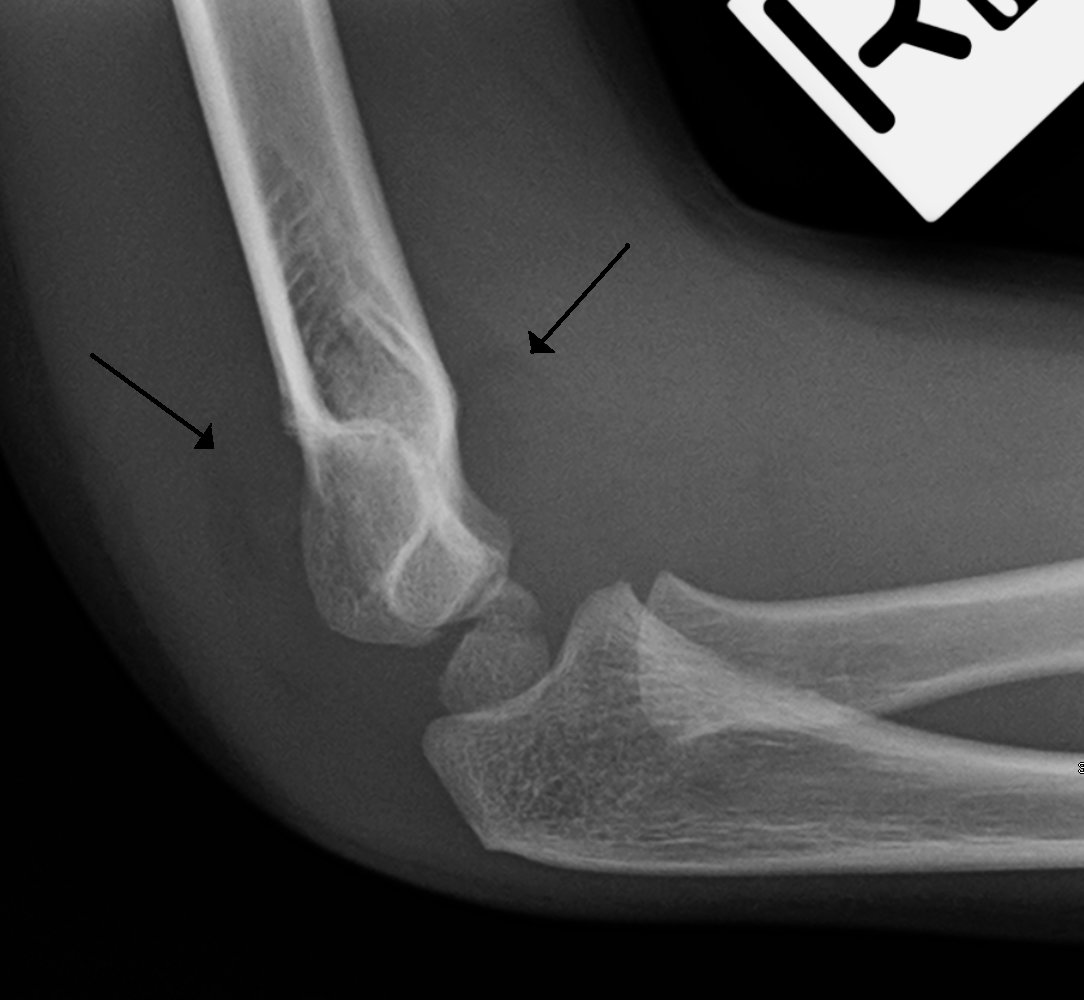
X-ray (lateral view) of a child's elbow
Posterior displacement of the capitulum. Both anterior and posterior fat pad signs can be seen as areas of decreased radiodensity (arrows). The anterior fat pad sign is also called "sail sign" because of its distinctive shape.
Source: “Sailsign” by James Heilman, MD, Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}
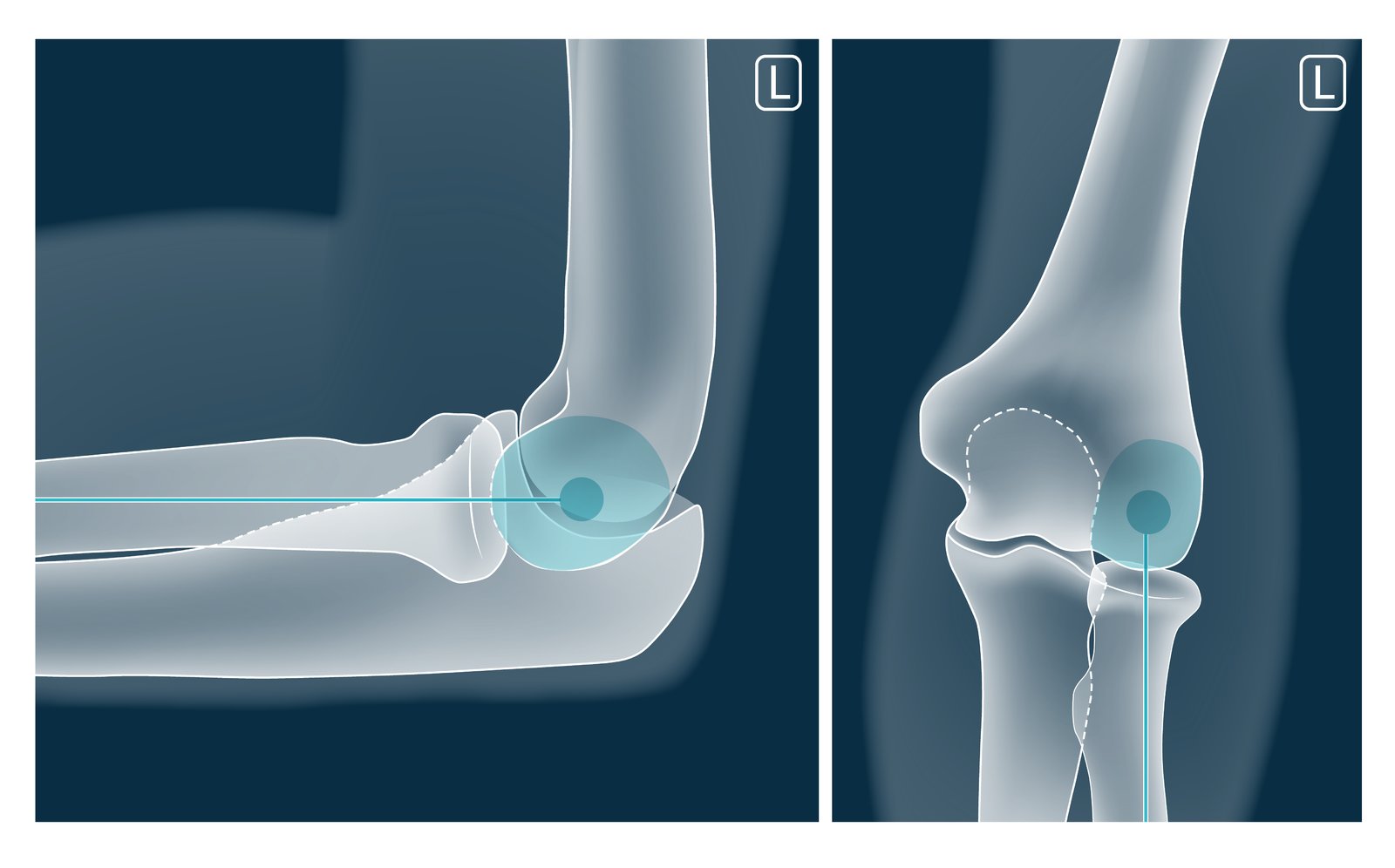
A straight line drawn down the neck of the radius should intersect the capitellum. If it does not, there is a dislocation of the radial head.
© AMBOSS
Treatment
Initial management
- Follow the ABCDE approach for patients with polytrauma.
- Manage acute pain while initiating steps for immediate closed reduction (e.g., preparation for procedural sedation).
- Consult orthopedics urgently if surgery is required.
Closed reduction of a posterior elbow dislocation [3][5]
Procedure
- Indication: uncomplicated simple posterior elbow dislocation
-
Preparation
- Obtain informed consent.
- Administer procedural sedation and analgesia.
- Position the patient for the procedure (typically prone or sitting).
-
Technique
- Flex the elbow to 90° and pronate (preferred) or supinate the forearm.
- Apply slow axial traction to the forearm while applying counter traction to the middle or distal humerus.
- Simultaneously apply direct pressure on the posterior aspect of the olecranon.
- Monitor for signs of successful reduction.
- Palpable clunk
- Normal triangular orientation of the three bony prominences of the elbow
- Reduced pain
- Verify the stability of relocation by moving the arm through a range of motion.
- Obtain repeat x-rays to verify correct positioning.
- Repeat neurovascular examination.
Postreduction
-
Elbow immobilization
- Use a posterior long arm splint or brace.
- Place the elbow at 90° flexion with the forearm in slight pronation.
- Reassess vascular status after the splint is applied.
- Maintain immobilization for 5–10 days. [1][5]
- POLICE principle
- Range of motion exercises (after a period of immobilization)
- Orthopedic follow-up (within 1 week) [3]



Surgery [7]
-
Indications
- Complex elbow dislocation
- Failed closed reduction
- Joint instability postreduction
- Vascular injury
- Compartment syndrome
-
Techniques
- Open reduction and internal fixation of the fracture
- Tenodesis and/or ligament repair
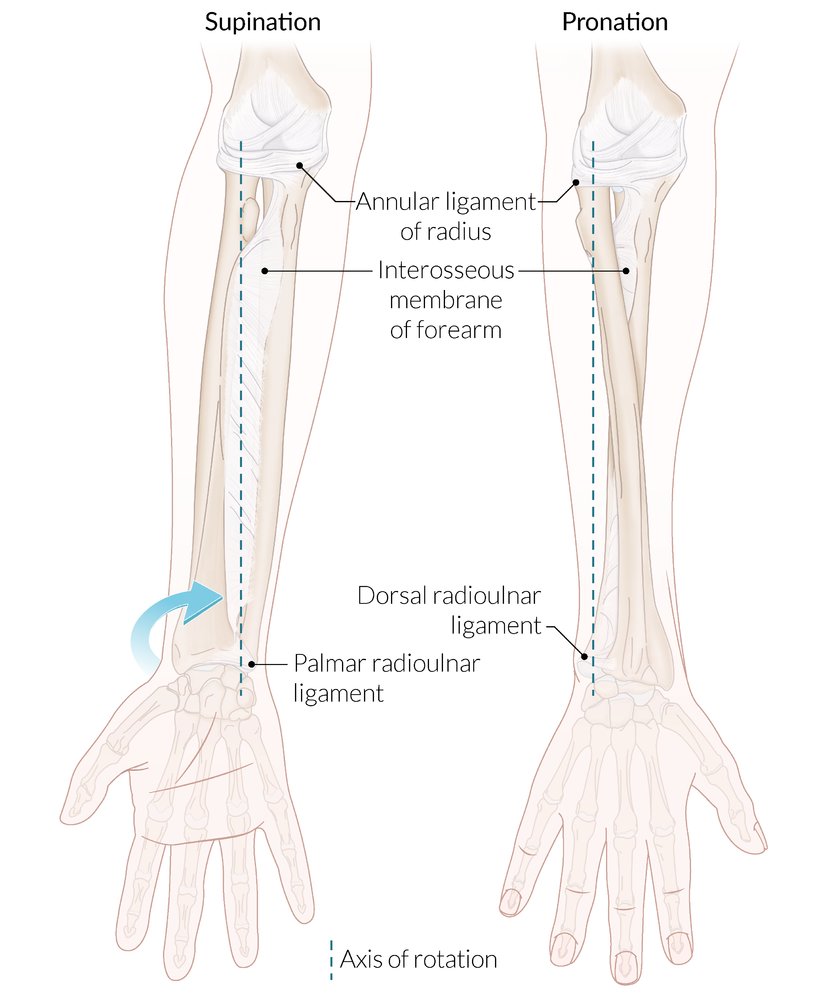
Right forearm; ventral view
Supination is an external rotational movement of the forearm that occurs at the proximal and distal radioulnar joints. When the forearm is in the supine position, the radius and ulna lie parallel to each other and the palm faces up. The supinator and biceps brachii (not shown here) are the supinators of the forearm.
Pronation is an internal rotational movement of the forearm that occurs at the proximal and distal radioulnar joints. When the forearm is in the prone position, the radius and ulna form an X shape and the palm faces down. The pronator quadratus and pronator teres (not shown here) are the pronators of the forearm.
The interosseous membrane stabilizes the proximal and distal radioulnar joints during pronation and supination.
© AMBOSS
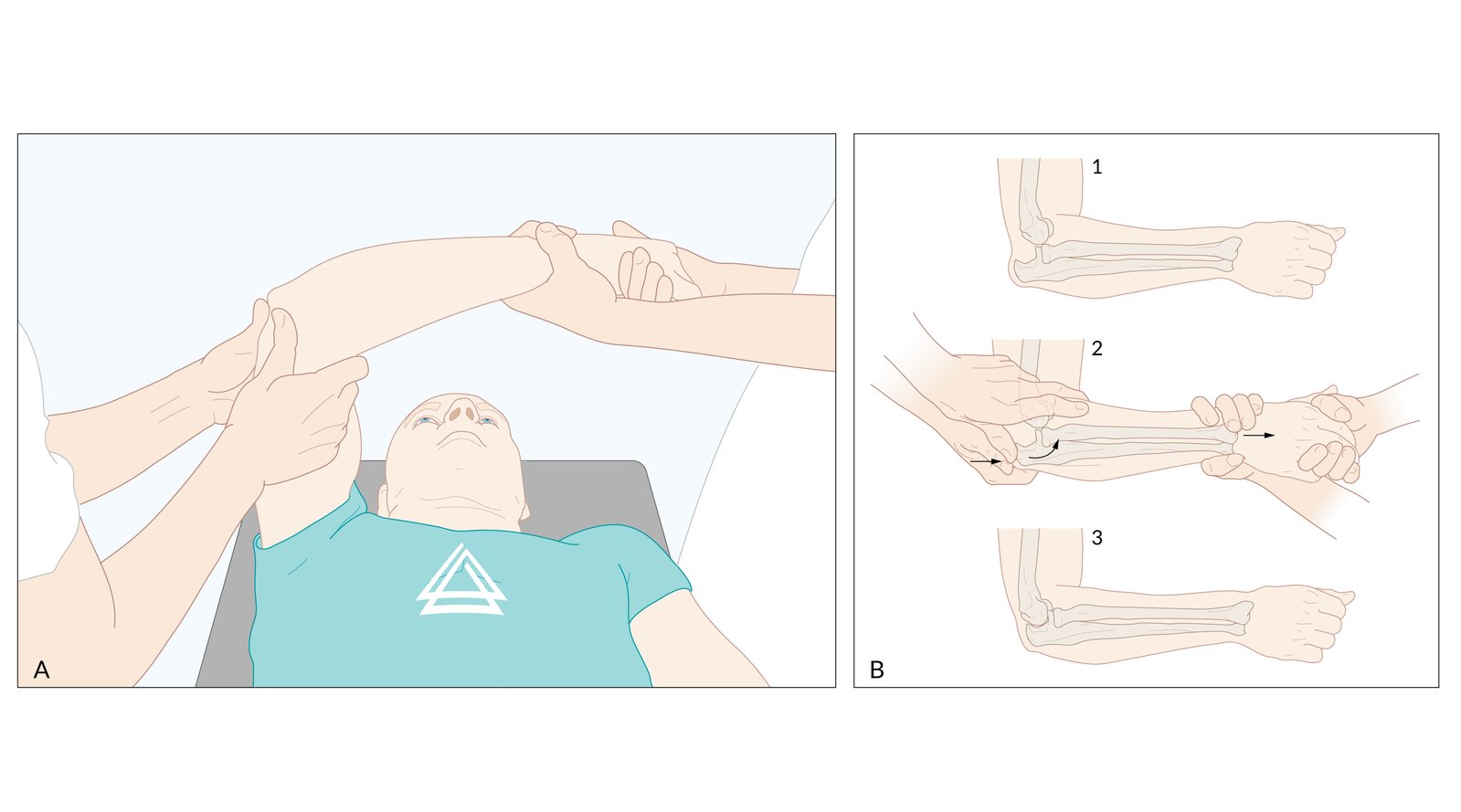
There are various techniques that can be used in a number of combinations. Administration of analgesics prior to the procedure is advisable.
This illustration shows a common approach in which the patient lies down on a stretcher in a supine position with one physician on each side (A).
One of the physicians raises the affect arm, clasping the elbow from both sides with both thumbs placed on the olecranon. The elbow is flexed to 90 degrees. The second physician then gently applies axial traction in the distal direction. At the same time, the first physician carefully applies pressure on the olecranon (to guide it back into position) and simultaneously applies gentle counter-traction to stabilize the position of the humerus (B).
Depending on the injury, the patient's condition, and possible concomitant injuries, this procedure can also be conducted with the forearm supinated rather than a pronated.
If neurovascular damage and/or fractures are present or suspected, additional diagnostic steps and different therapeutic measures are necessary.
© AMBOSS

The angle between the brace's upper and lower parts is adjustable at the elbow joint.
Source: “Terminator-esque arm brace” by Juhan Sonin, flickr, licensed under CC BY 2.0.
Complications
- Recurrent dislocation and instability
- Posttraumatic stiffness (especially after prolonged immobilization)
- Posttraumatic arthritis and/or soft tissue ossification
- Brachial artery injury and/or vascular compromise
- Peripheral nerve injury
- Acute compartment syndrome
- See also “Complications of fractures.”
We list the most important complications. The selection is not exhaustive.
References
- Walls R, Hockberger R, Gausche-Hill M, Erickson TB, Wilcox SR. "Rosen's Emergency Medicine 10th edition- Concepts and Clinical Practice E-Book". Elsevier Health Sciences. (2022). ISBN: 9780323757904
- Reichert ILH, Ganeshamoorthy S, Aggarwal S, Arya A, Sinha J. "Dislocations of the elbow – An instructional review". J Clin Orthop Trauma. 21. :101484. (2021)
- Gottlieb M. "Managing Elbow Dislocations". Ann Emerg Med. 80(5). :460-464. (2022)
- Mühlenfeld N, Frank J, Lustenberger T, Marzi I, Sander AL. "Epidemiology and treatment of acute elbow dislocations: current concept based on primary surgical ligament repair of unstable simple elbow dislocations". Eur J Trauma Emerg Surg. 48(1). :629-636. (2020)
- Roberts JR. "Roberts and Hedges' Clinical Procedures in Emergency Medicine and Acute Care". Elsevier. (2018). ISBN: 9780323354783
- Pandian NG, Kim JK, Arias-Godinez JA, et al. "Recommendations for the Use of Echocardiography in the Evaluation of Rheumatic Heart Disease: A Report from the American Society of Echocardiography". J Am Soc Echocardiogr. 36(1). :3-28. (2023)
- Breulmann FL, Lappen S, Ehmann Y, et al. "Treatment strategies for simple elbow dislocation - a systematic review". BMC Musculoskelet Disord. 25(1). (2024)