Summary
Esophageal cancer (EC) is the eighth most common type of cancer worldwide and affects men more than women (3:1 ratio). The two main forms are esophageal adenocarcinoma and squamous cell carcinoma. Esophageal adenocarcinomas are among the neoplasms with the fastest increasing incidence in northern and western Europe and North America, while squamous cell carcinoma is the most common form worldwide. Adenocarcinoma, which usually affects the lower third of the esophagus, may be preceded by gastroesophageal reflux disease and Barrett esophagus. Other risk factors include smoking and obesity. Risk factors for squamous cell carcinoma include carcinogen exposure (e.g., in the form of alcohol and tobacco) and a diet high in nitrosamines but low in fruits and vegetables. Locally advanced disease is common at the time of diagnosis because EC is typically asymptomatic early in the disease course. Symptomatic patients may experience weight loss, dyspepsia, progressive dysphagia, cervical adenopathy, hoarseness or persistent cough, and signs of upper gastrointestinal bleeding, such as hematemesis, melena, or anemia. Esophagogastroduodenoscopy (EGD) is used to directly visualize the lesion and obtain a biopsy sample for histopathological confirmation. Staging of the tumor involves CT scan of the chest and abdomen, a PET scan, and often transesophageal endoscopic ultrasound (EUS). Curative surgical resection may be considered for locally invasive cancers, but EC is unresectable in approximately 60% of patients at the time of diagnosis. For patients with unresectable disease, treatment options include chemotherapy, radiation, and palliative stenting. Prognosis is generally poor because of the aggressive nature of EC and oftentimes late diagnosis.
Epidemiology
- Sex: ♂ > ♀ (3:1) [1]
- Incidence: an estimated 20,640 new cases of esophageal cancer will be diagnosed in 2022 in the United States [1]
- Median age of onset: : between 60 and 70 years of age
- Adenocarcinoma: : most common type of esophageal cancer in the US [2]
- Squamous cell carcinoma (SCC): most common type of esophageal cancer worldwide [3]
Adenocarcinoma is more common in the US of America.
Epidemiological data refers to the US, unless otherwise specified.
Etiology
Adenocarcinoma [4]
-
Exogenous risk factors
- Smoking (twofold risk)
- Obesity
-
Endogenous risk factors
- Male sex
- Older age (50–60 years)
- Gastroesophageal reflux
- Barrett esophagus
- Localization: mostly in the lower third of the esophagus
The most important risk factors for esophageal adenocarcinoma are gastroesophageal reflux and associated Barrett esophagus.
Squamous cell carcinoma (SCC) [4][5]
-
Exogenous risk factors
- Alcohol consumption
- Smoking (ninefold risk)
- Diet low in fruits and vegetables
- Hot beverages
- Nitrosamines exposure (e.g., cured meat, fish, bacon) [6]
- Caustic strictures
- HPV [7]
- Radiotherapy
- Betel or areca nut chewing
- Esophageal candidiasis [8][9]
-
Endogenous risk factors
- Male sex
- Older age (60–70 years)
- African American descent
- Plummer-Vinson syndrome
- Achalasia
- Diverticula (e.g., Zenker diverticulum)
- Tylosis
- Localization: : mostly in the upper two-thirds of the esophagus
The primary risk factors for squamous cell esophageal cancer are alcohol consumption, smoking, and dietary factors (e.g., diet low in fruits and vegetables).
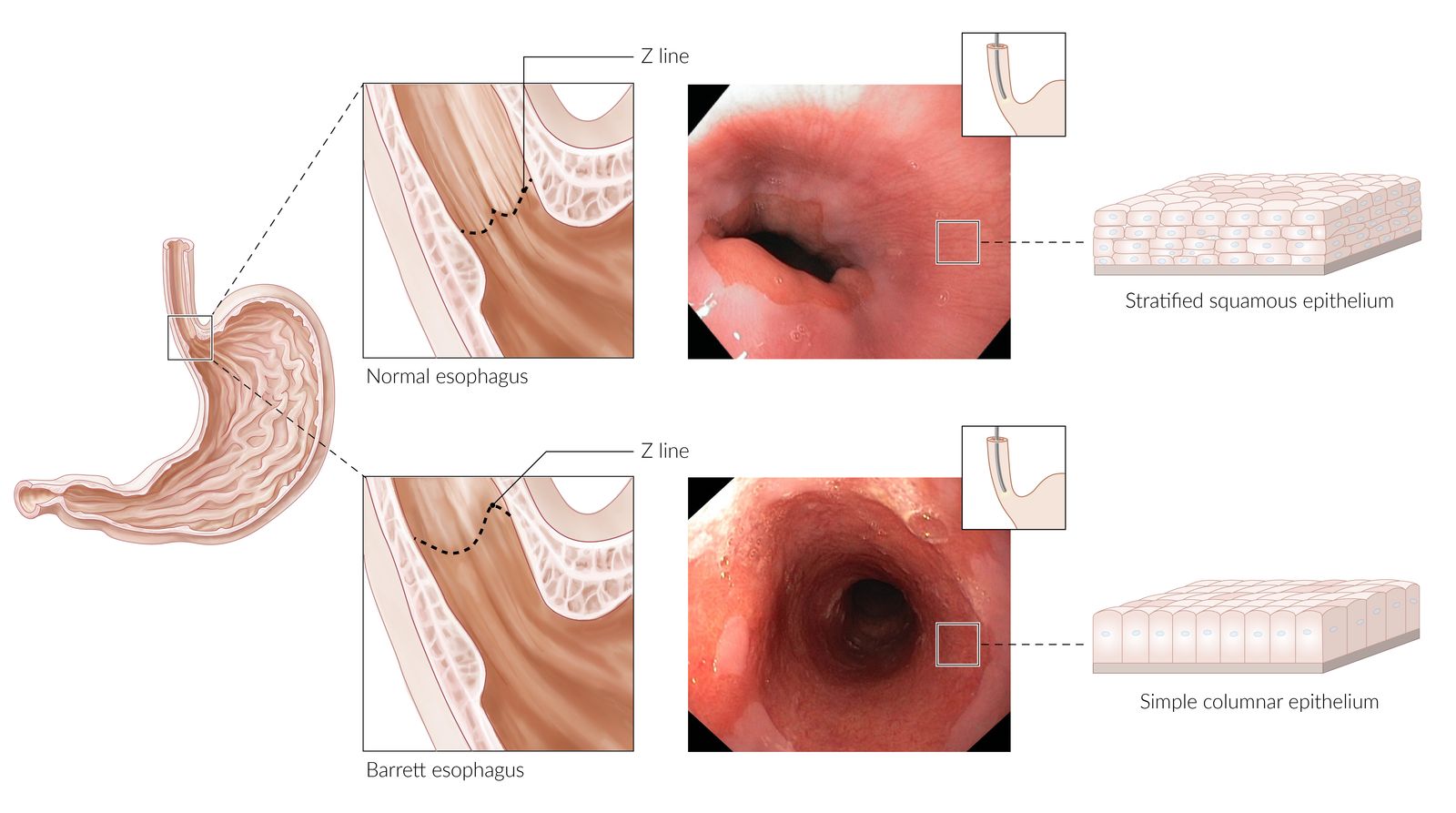
Visible in both photographs is the transformation zone (Z-line), where the stratified squamous epithelium of the esophagus (paler pink color) meets the columnar epithelium of the stomach (darker red color).
Normal esophagus: the Z-line is located at or just proximal to the gastroesophageal junction, which typically corresponds to the level of the diaphragmatic hiatus and the lower esophageal sphincter.
Barrett esophagus: chronic reflux esophagitis damages the stratified squamous mucosa of the distal esophagus (which is not adapted to tolerate gastric acid) → metaplastic replacement of stratified squamous epithelium by columnar epithelium → proximal displacement of the Z line
© AMBOSS. "Normal esophagus" endoscopy image kindly provided by Dr. J. Guntau - Albertinen Krankenhaus, Hamburg, Germany (endoskopiebilder.de). "Barrett esophagus" endoscopy image kindly provided by Dr. med. Merkel, Dr. med. Wiens, Dr. med. Kämmer - St. Hedwig Krankenhaus, Berlin, Germany.
Classification
Siewert classification of adenocarcinoma of the esophagogastric junction [10]
- Based on the location of the tumor in relation to the Z line
- Siewert type I and II tumors are managed as esophageal cancer. [11]
| Overview of Siewert classification [11] | ||
|---|---|---|
| Type | Localization | Surgical approaches |
| Siewert type I |
|
|
| Siewert type II |
|
|
| Siewert type III |
|
|

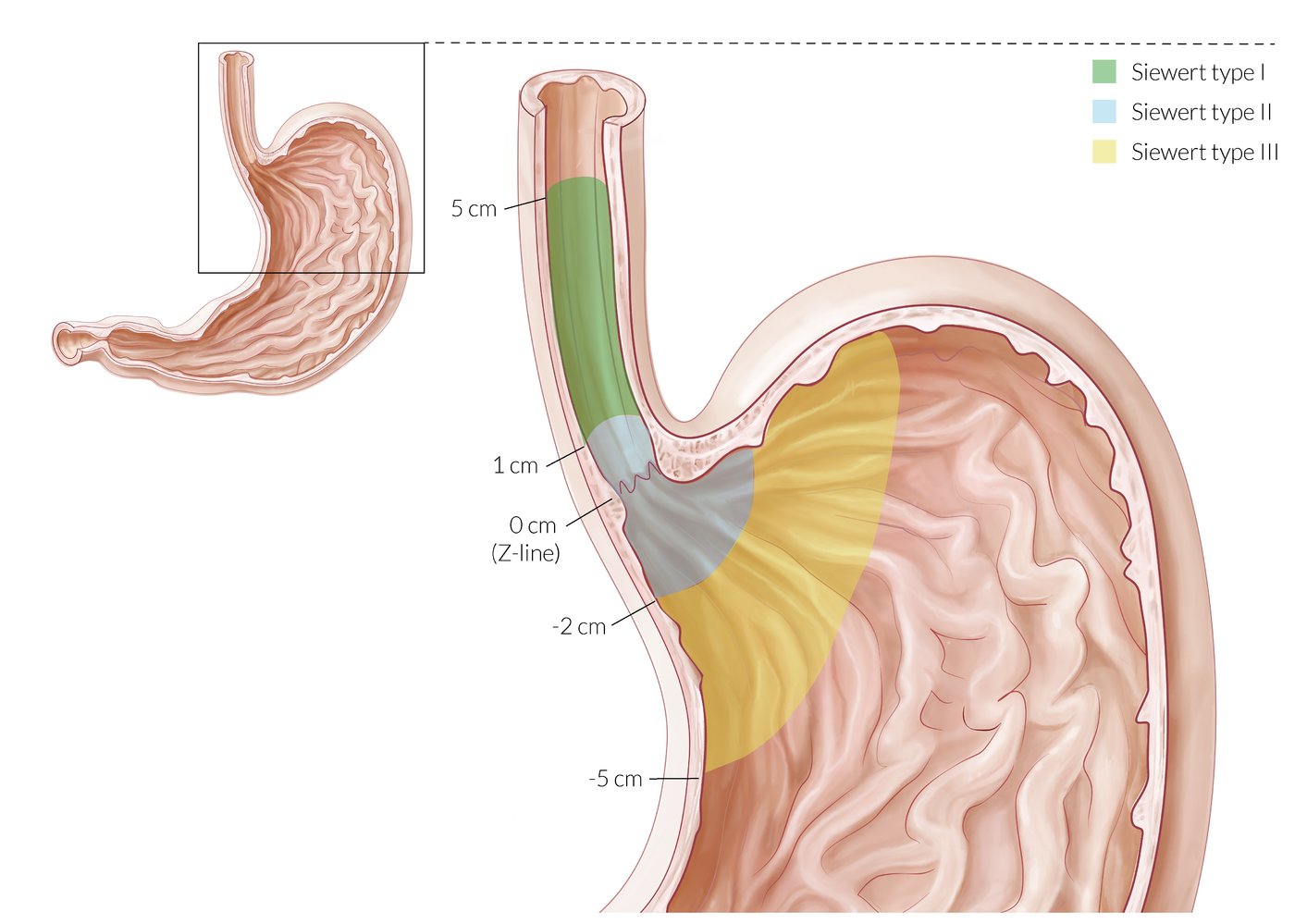
Adenocarcinoma of the esophagogastric junction is classified by tumor location in relation to the Z line, where the esophageal squamous epithelium changes into gastric columnar epithelium.
– Siewert type I: The center of the tumor is located 1–5 cm above the Z line within the esophagus (associated with Barrett mucosa).
– Siewert type II: The center of the tumor is located 1 cm above or 2 cm below the Z line (true carcinoma of the cardia).
– Siewert type III: The center of the tumor is located 2–5 cm below the Z line.
© AMBOSS
Clinical features
Early stages [4]
- Often asymptomatic
- May manifest with dysphagia or retrosternal discomfort
Advanced stages [4]
-
General signs
- Unintentional weight loss
- Dyspepsia
- Signs of anemia
-
Signs of advanced disease
- Progressive structural dysphagia (from solids to liquids) with possible odynophagia
- Retrosternal chest or back pain
- Cervical adenopathy
- Hoarseness and/or persistent cough
- Horner syndrome
-
Signs of upper gastrointestinal bleeding
- Hematemesis
- Melena
Initially, esophageal cancer is often asymptomatic. It typically becomes symptomatic at advanced stages.
Diagnosis
Esophagogastroduodenoscopy (EGD) with biopsy is the best initial and confirmatory test in patients with suspected esophageal cancer. [12][13]
EGD [14]
-
Indications
- Red flags for dysphagia
- Patients with both clinical features and risk factors for EC
-
Uses
- Direct visualization of the tumor
- Biopsy of any suspicious lesions


Barium swallow [12]
-
Indications
- Severe esophageal strictures
- Suspected tracheoesophageal fistula
- Tumors near the Z line: to differentiate between gastroesophageal junction and gastric tumors
-
Findings
- Characteristic stenosis and proximal dilatation (apple core lesion)
- Asymmetrical and irregular esophagal borders


Staging investigations [12]
Consider the following studies in consultation with a multidisciplinary team.
-
Routine studies [15]
- CT chest and abdomen with IV contrast
- FDG-PET/CT skull base to mid-thigh
- Transesophageal EUS with fine-needle aspiration biopsy
-
Additional studies
- Bronchoscopy: for lesions at or above the tracheal carina to rule out airway involvement
- Laparoscopy: to increase staging accuracy in adenocarcinoma of the gastroesophageal junction


Laboratory studies [4]
- CBC: iron deficiency anemia may indicate occult GI bleeding
-
Liver chemistries
- ↑ Transaminases may indicate liver metastases
- ↑ ALP may indicate bone metastases
- Serum creatinine: to determine pretreatment renal function [13]
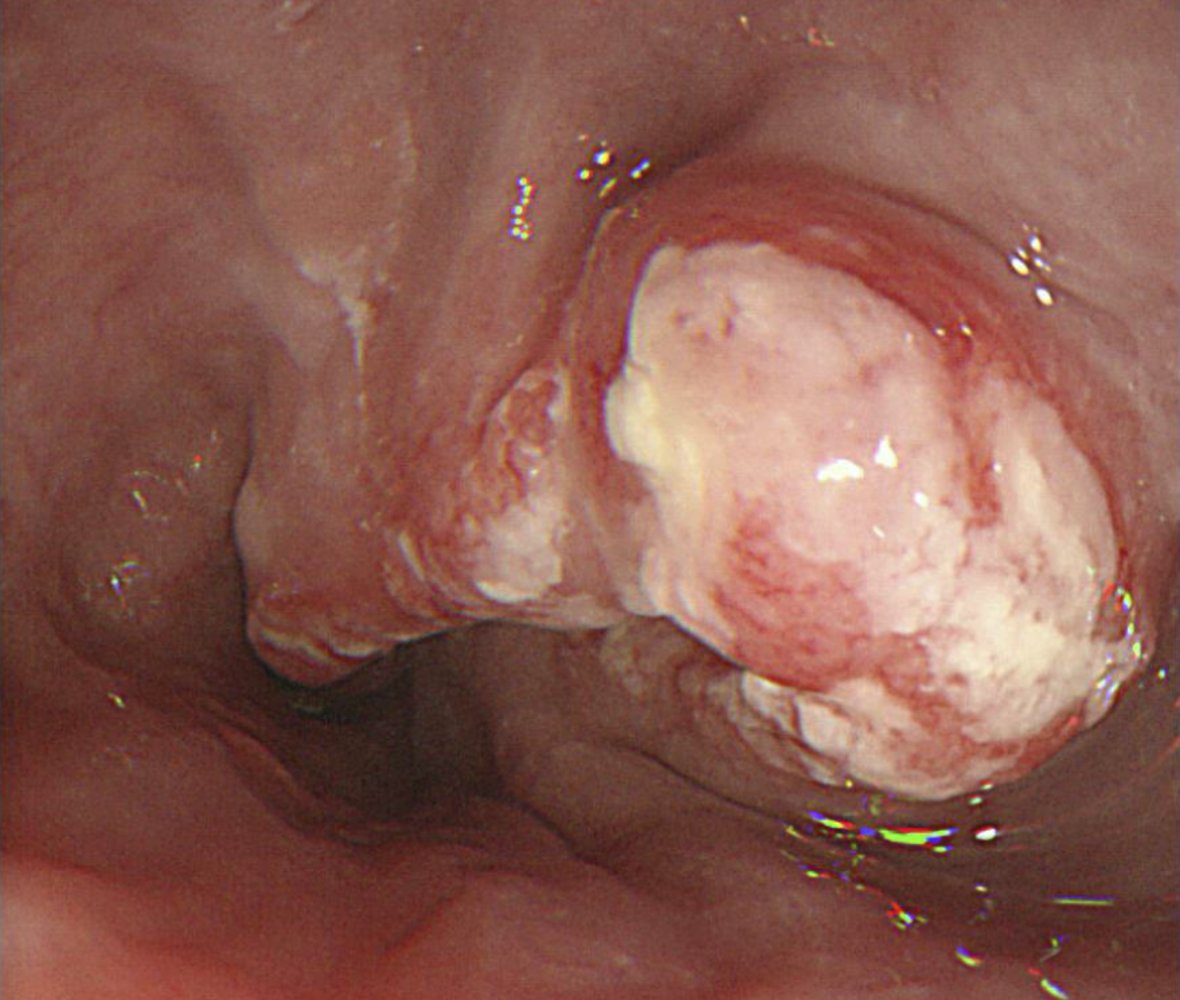
Endoscopic view of the thoracic esophagus
A large exophytic mass with raised edges is partially obstructing the esophageal lumen. The surface is amorphous and covered with white deposits.
The location and gross appearance of the tumor suggest a squamous cell carcinoma.
Source: “Figure 3. in: The Alcohol Flushing Response: An Unrecognized Risk Factor for Esophageal Cancer from Alcohol Consumption” by Philip J Brooks ,Mary-Anne Enoch,David Goldman,Ting-Kai Li,Akira Yokoyama, PLOS Medicine Journal, licensed under CC BY 4.0.
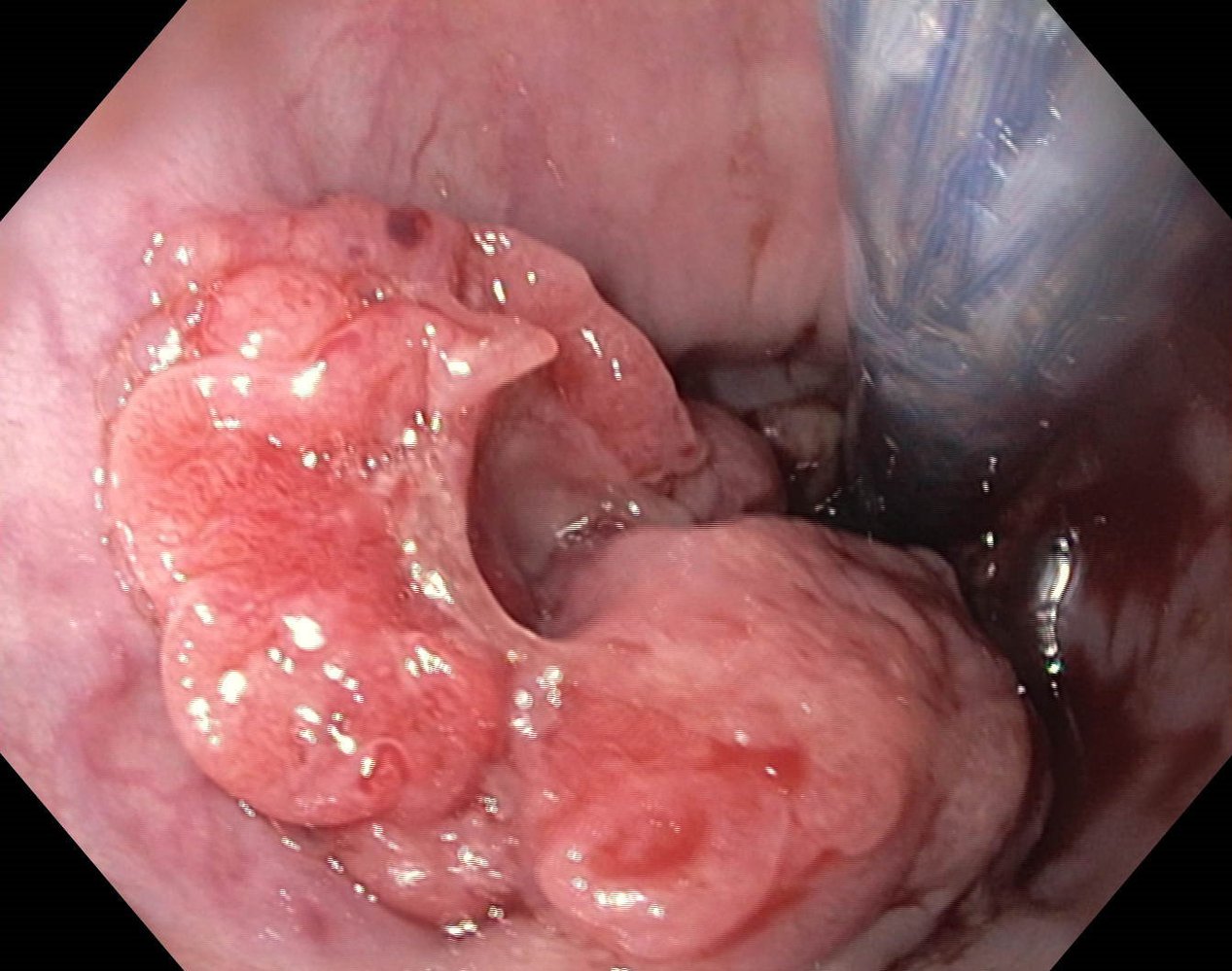
Endoscopic view of the esophagus
An exophytic, irregularly demarcated mass with raised edges (green line) and central ulceration (dashed line) is partially obstructing the esophageal lumen.
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.
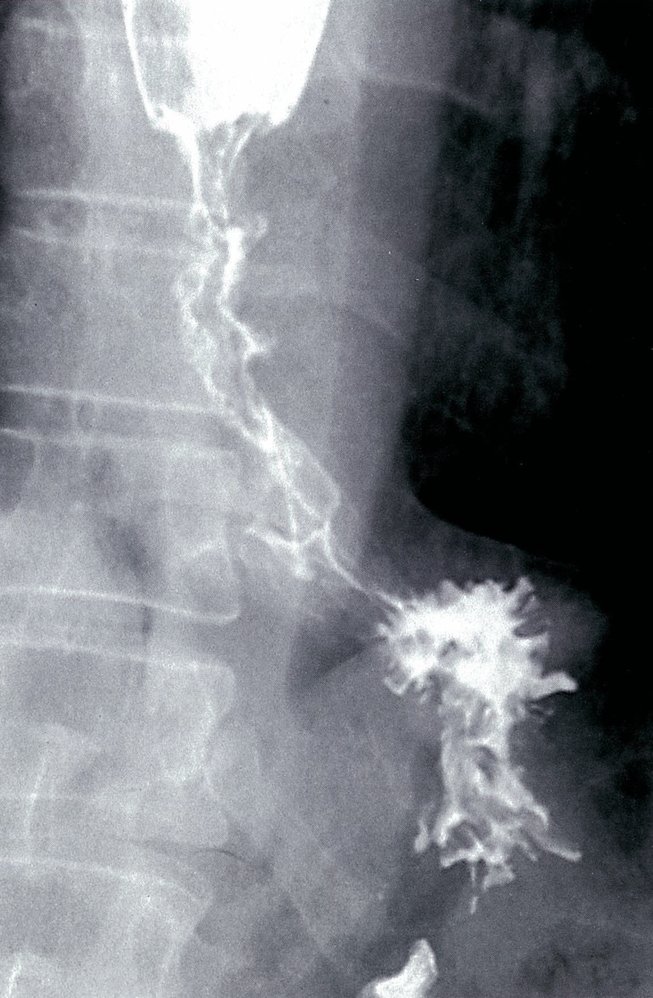
Barium esophagram (frontal view) of a patient with a history of chronic gastroesophageal reflux and Barrett esophagus
Long segment narrowing of the distal esophagus is seen with irregularity of the mucosa and an apple-core configuration (green outline). The esophagus (E) is dilated proximal to the stricture.
This appearance suggests esophageal carcinoma.
S: stomach
Source: © IMPP
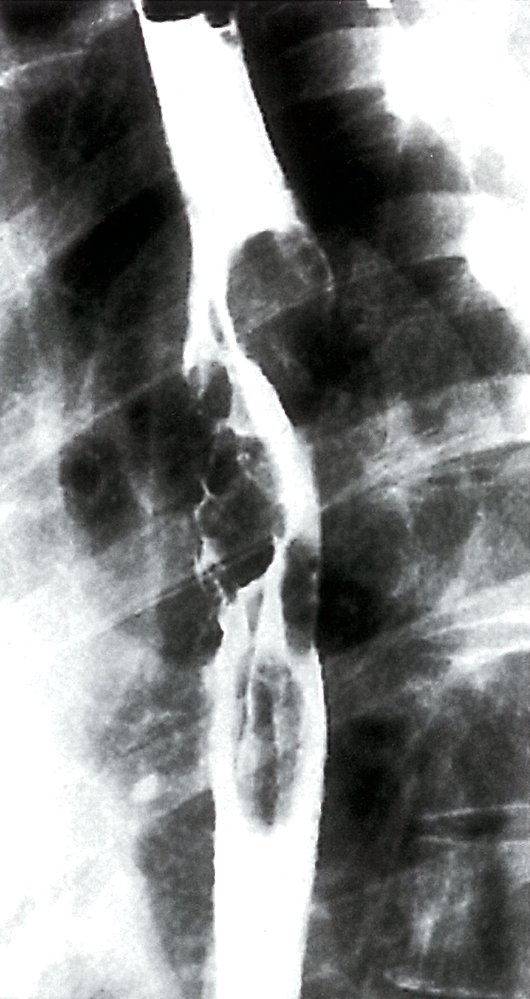
Barium esophagram (lateral view) of a patient with esophageal carcinoma
A long segment irregular stricture is seen in the mid third of the thoracic esophagus (green overlay). The superior aspect of the stricture has an apple-core appearance (indicated by dashed line).
Source: © IMPP
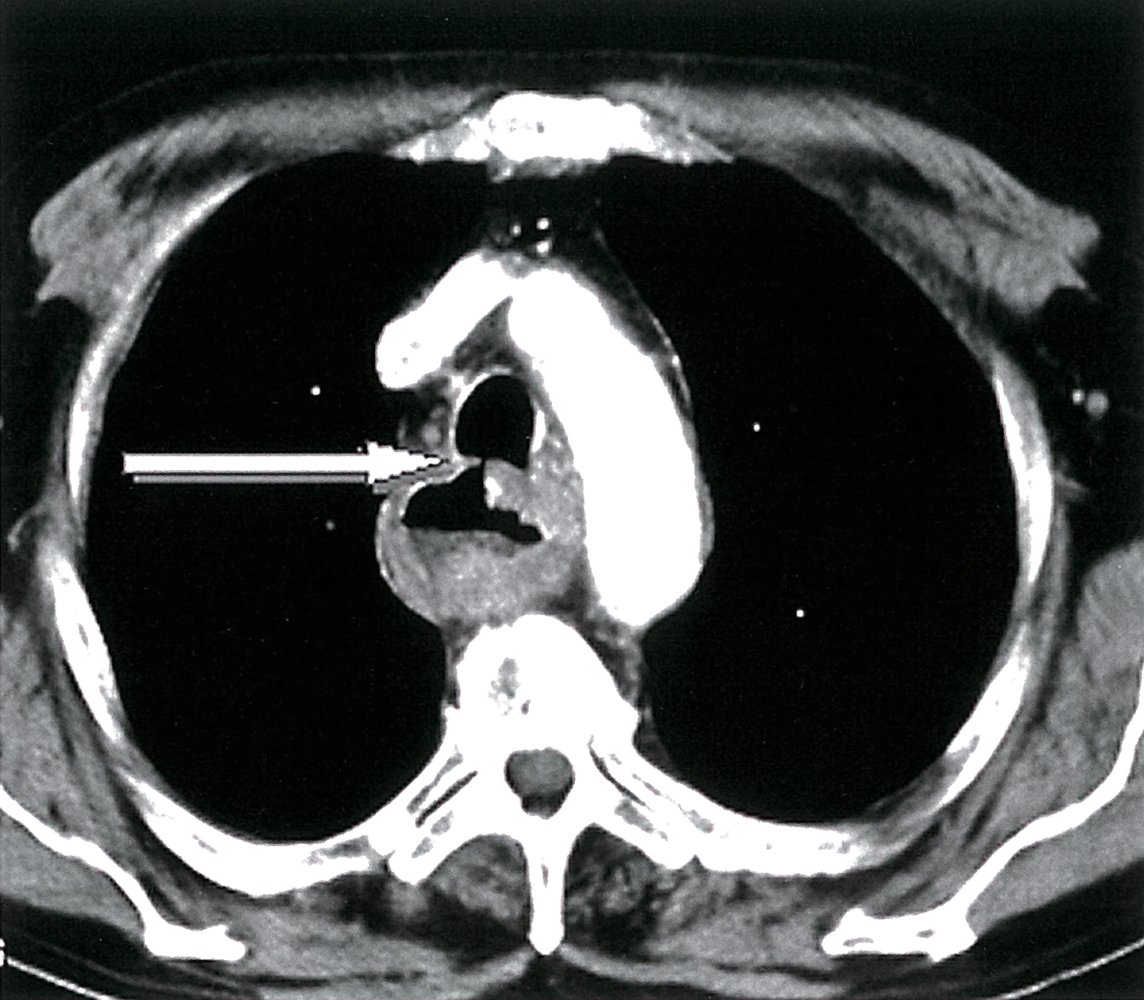
CT chest (with contrast; axial plane; mediastinal window)
The wall of the esophagus is markedly thickened (green overlay). A fistula (arrow) is seen between the esophagus and trachea (T). Dependent material (red overlay) is present in the esophagus.
Source: © IMPP
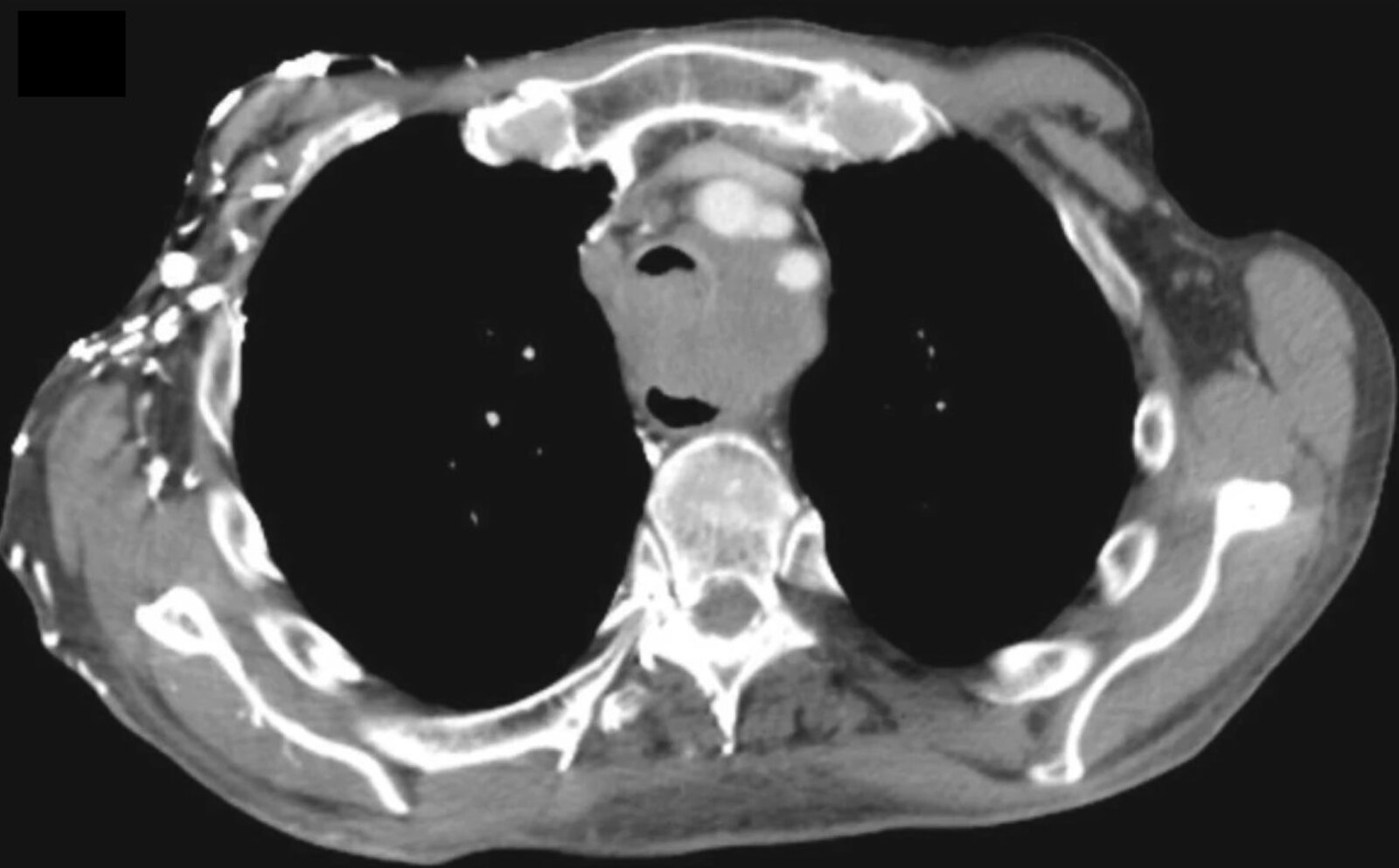
CT chest (with contrast; axial plane; mediastinal window) of a patient with esophageal carcinoma
A soft tissue mass between the trachea and esophagus (arrows) widens the distance between the two lumens. The mass involves the anterior wall of the esophagus (green overlay) and invades the posterior trachea. The tracheal lumen (L) is markedly narrowed.
Multiple contrast-enhanced right chest-wall blood vessels (arrowheads) raise concern for obstruction of the superior vena cava.
Source: “Fig 1.9 C, In: A Systematic Approach to Chest Radiographic Analysis” by Klein JS, Rosado-de-Christenson ML, SpringerLink, licensed under CC BY 4.0. Modifications: image cropped & removal of the letter c in the upper left corner. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
Staging
Once the diagnosis is confirmed, EC should be staged to determine management. The American Joint Committee for Cancer (AJCC) TNM classification is currently the standard staging system used in clinical practice.
AJCC staging (8th Edition, 2017) [16]
- Use a staging calculator based on the type of EC:
- Adenocarcinoma
- Squamous cell carcinoma

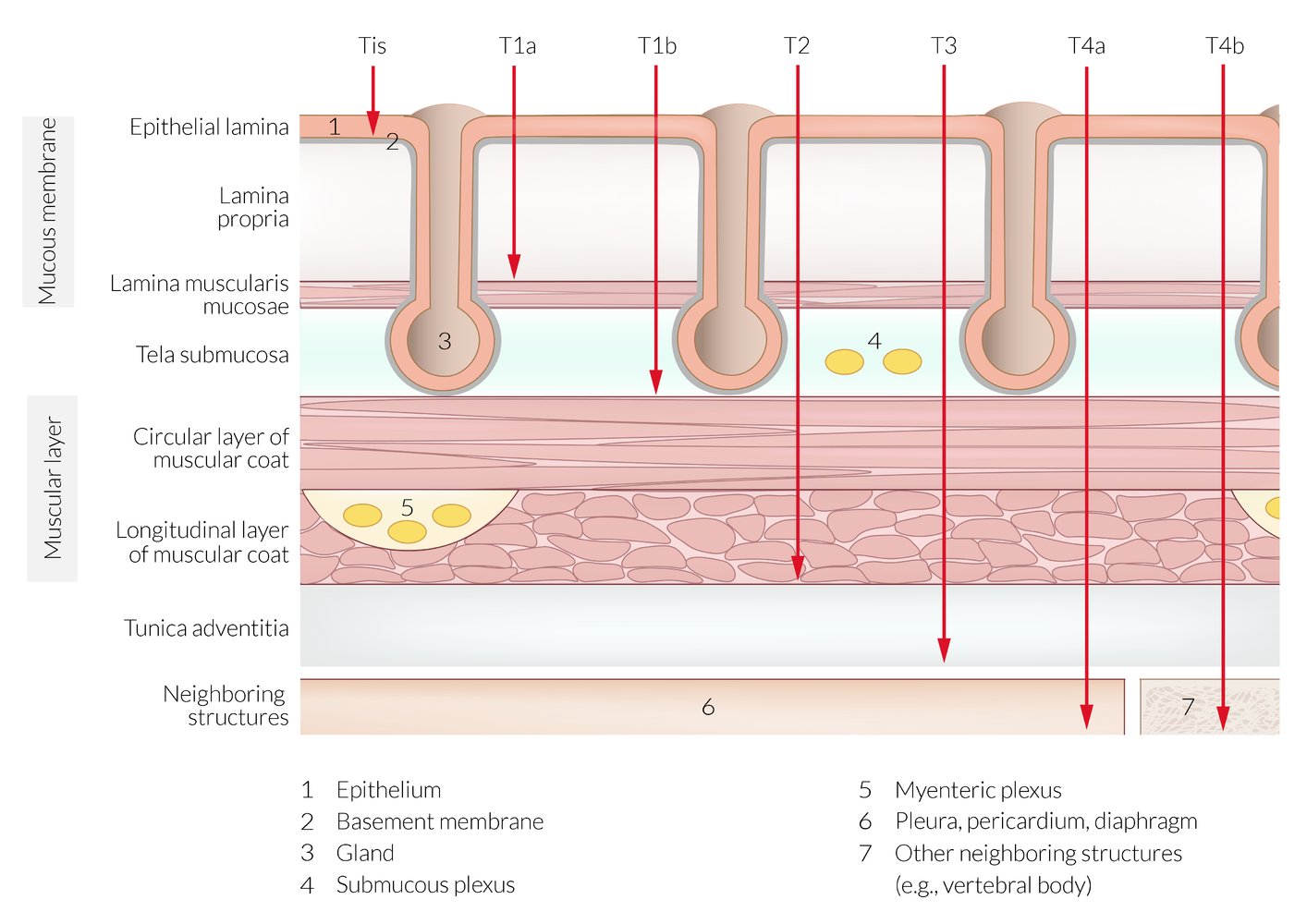
Cross-section of the esophageal wall showing the stages of infiltration by malignant tumors
© AMBOSS
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
Pathology
Adenocarcinoma [17]
- Carcinoma arises in context of Barrett esophagus (columnar epithelium with goblet cells) and high-grade dysplasia
- Gland-forming tumors with different possible growth patterns (tubular, papillary, tubulopapillary)
- Mucinous differentiation possible
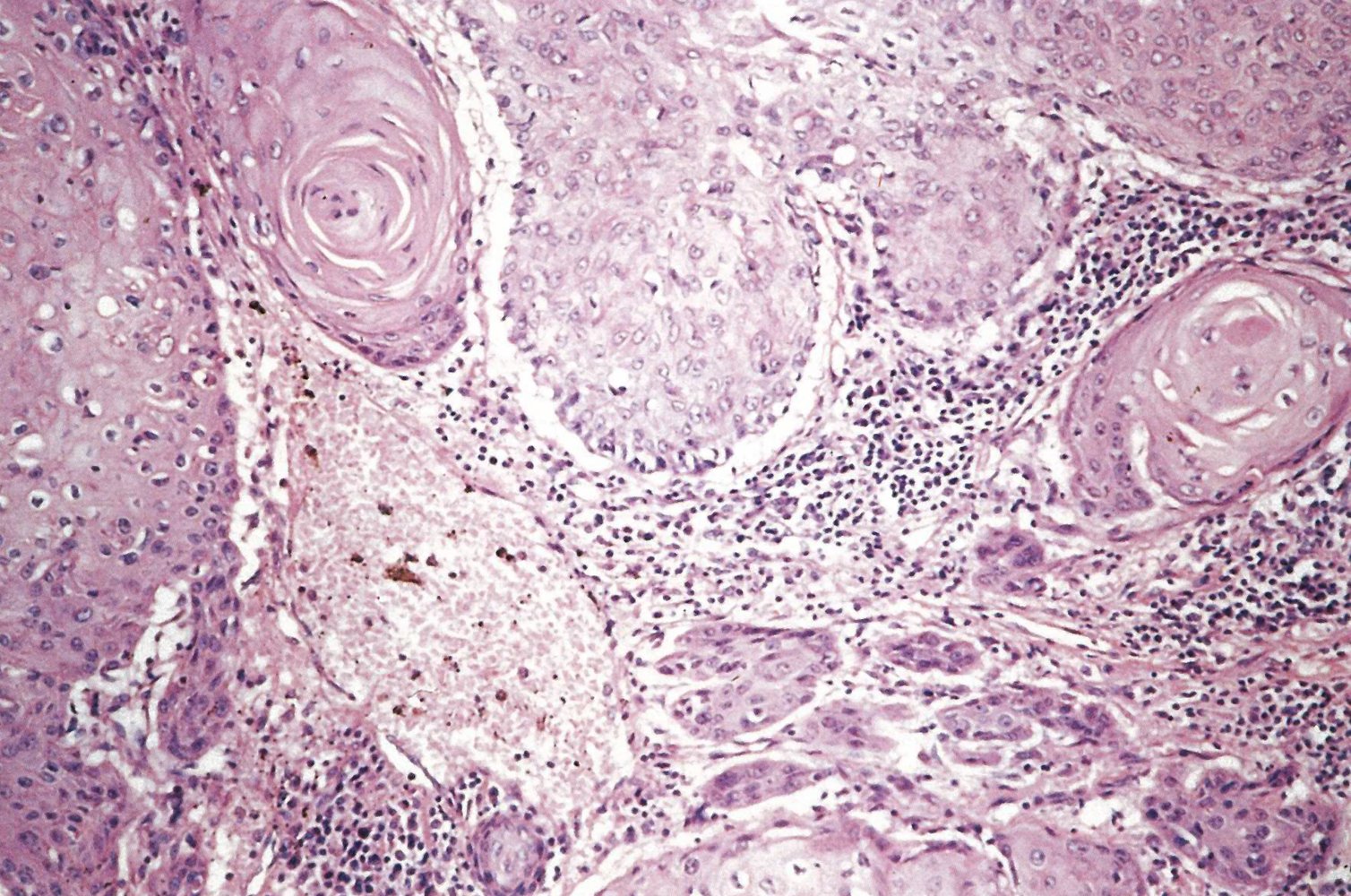
Squamous cell carcinoma [17]
- Breakdown of uniform tissue structure
- Squamous cell carcinoma clusters with circular keratinization
- Lymphocytic infiltration between the carcinoma clusters




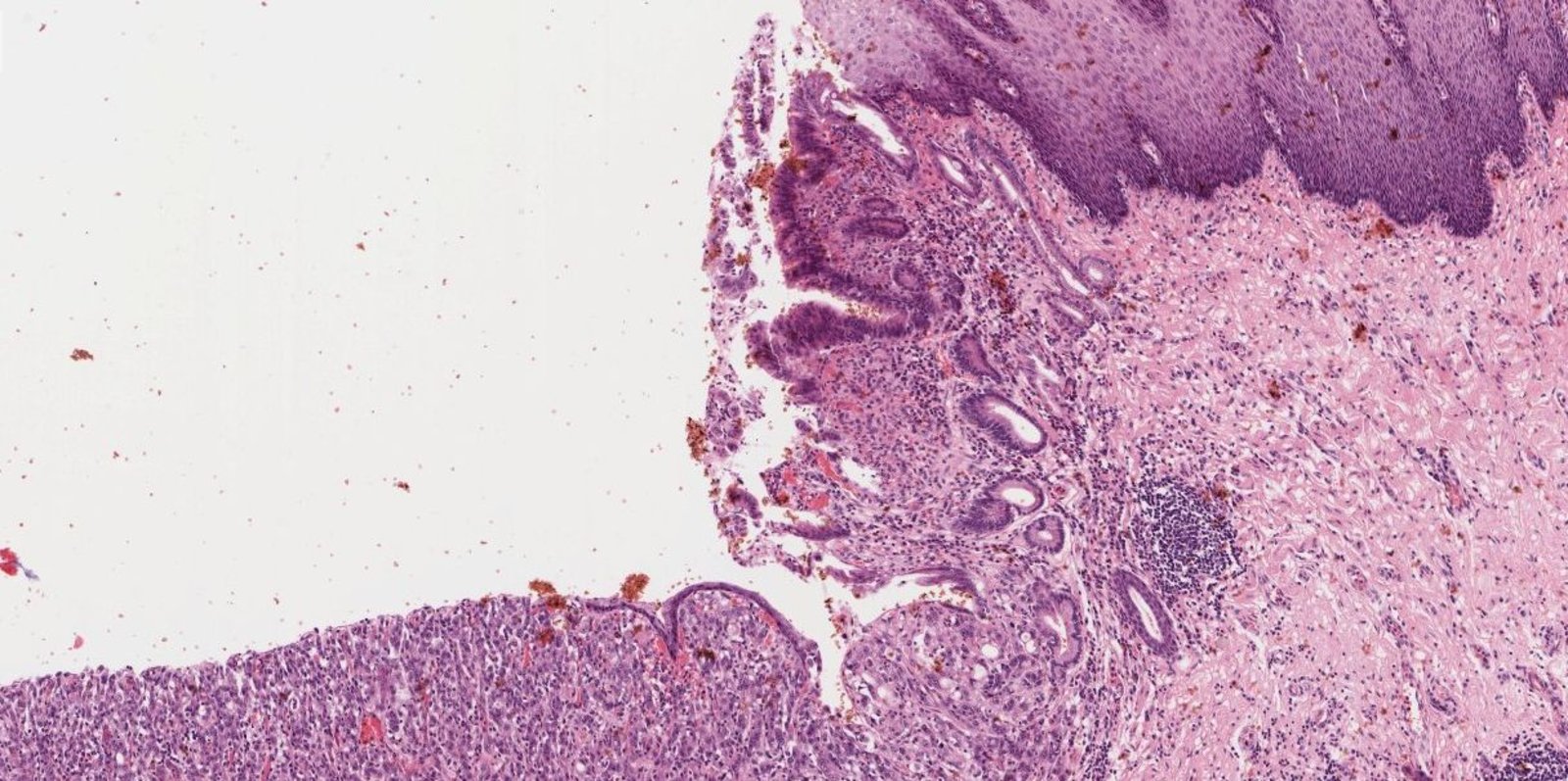
Photomicrograph of an esophageal tissue biopsy specimen (H&E stain; intermediate magnification)
The upper right edge of the image shows physiological multilayered squamous epithelium of the esophageal mucosa (white overlay), which changes into metaplastic prismatic epithelium with goblet cells (Barrett metaplasia; yellow overlay) toward the center of the image. Barrett metaplasia can eventually develop into epithelial dysplasia and, further, to adenocarcinoma of the esophagus (blue overlay). The carcinoma is characterized by loss of tissue architecture (atypical to absent gland formation) and invasive growth.
Click on the Smartzoom button to view the entire specimen through a virtual microscope.
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: PD Dr. med. Alberto Perez Bouza, Facharzt für Pathologie
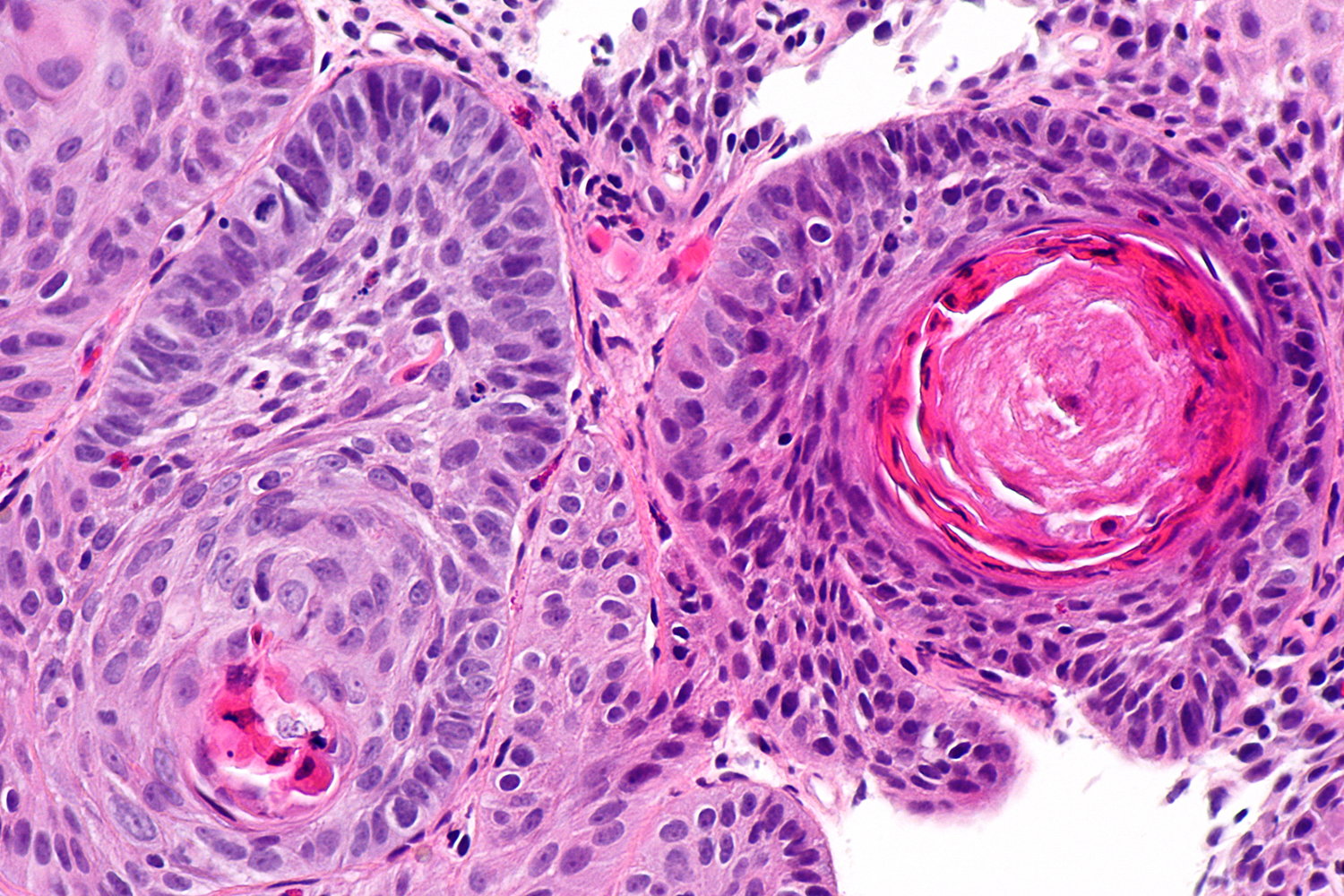
Photomicrograph of esophageal tumor (H&E stain; high magnification)
Normal squamous epithelium (yellow overlay) of the esophagus is visible at the top. Additionally, atypical squamous cell clusters (examples indicated by dashed outlines) with keratinization (examples indicated by arrows) are seen infiltrating the lamina propria below the basement membrane.
This infiltrative growth indicates esophageal squamous cell carcinoma.
Source: © IMPP
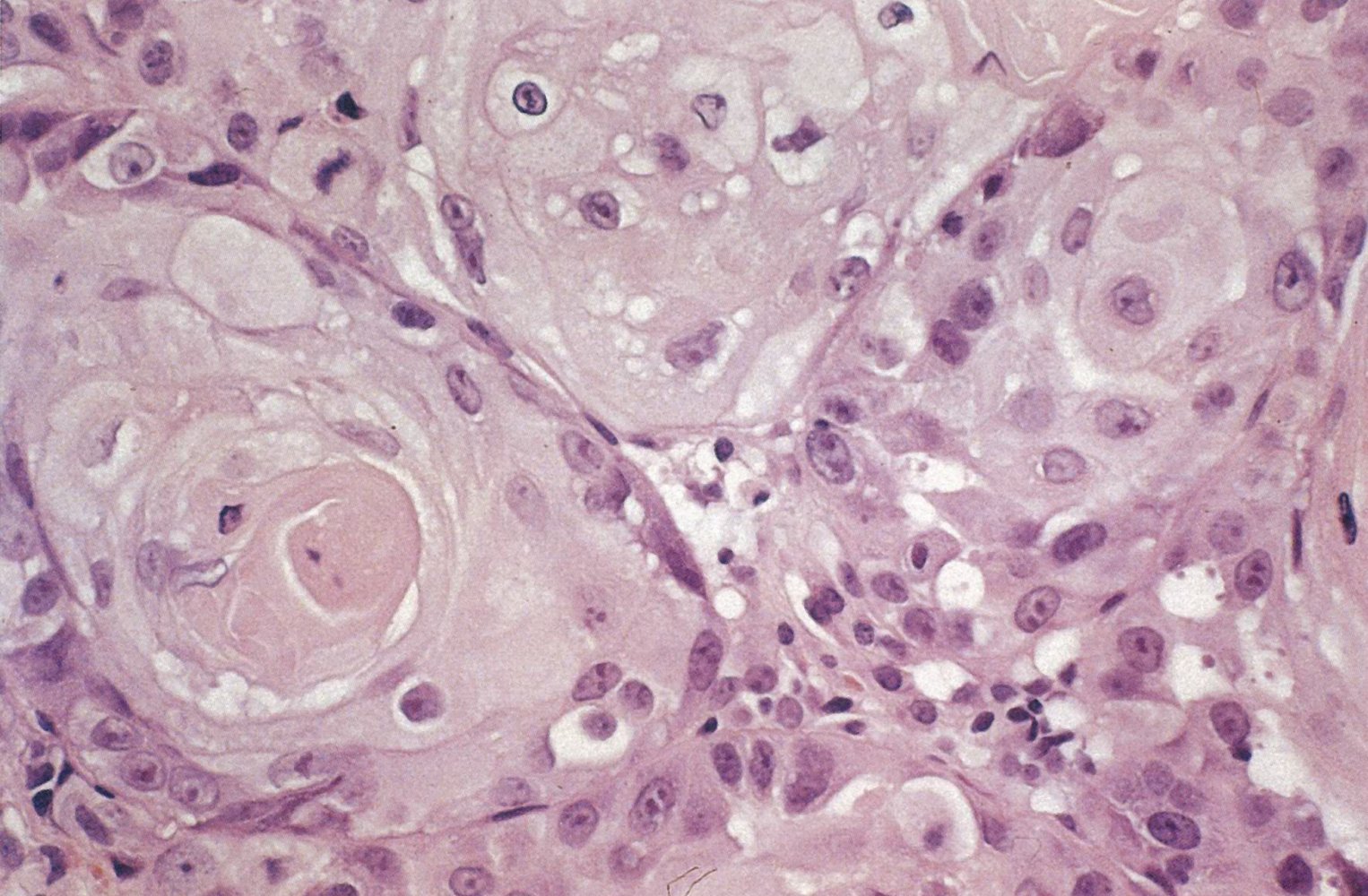
Photomicrograph of esophageal tumor (H&E stain; very high magnification)
Nests of large epithelial cells (examples indicated by blue overlay) with pale eosinophilic cytoplasm and central keratinization (example indicated by yellow overlay) are seen. The cell membranes (examples indicated by arrowheads) are relatively prominent.
These histological findings are characteristic of esophageal keratinizing squamous cell carcinoma.
Source: © IMPP
Photomicrograph of esophageal tissue (H&E stain)
Nests of neoplastic squamous cells with nuclear atypia (yellow overlay) surround prominent keratin pearls (green overlay). Components of nonkeratinizing basal-like tumor cells can be seen as well.
This carcinoma is moderately differentiated and keratinizing.
Source: “Esophageal squamous cell carcinoma - a1 -- high mag” by Nephron, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
Treatment
General principles
- Multidisciplinary cancer care should be utilized if available.
- The treatment approach should be guided by shared decision-making and the patient's performance status.
- Treatment goals [4]
-
Curative for patients with:
- High-grade metaplasia in Barrett esophagus
- Localized lesions that have not infiltrated surrounding structures
- Palliative for patients with unresectable locally advanced or metastatic cancer
-
Curative for patients with:
- See “Principles of cancer care.”
Surgical resection [18]
- Endoscopic submucosal resection for mucosal lesions [19]
-
Subtotal or total esophagectomy
- Indications: localized or resectable locally advanced disease
- Options include: gastric pull-through procedure, colonic interposition
Chemoradiotherapy [18][20]
-
Neoadjuvant chemoradiotherapy
- Indications: locally advanced disease
- Common regimen: fluorouracil, leucovorin, oxaliplatin, and docetaxel (FLOT) [18]
-
Chemoradiotherapy with or without targeted therapies
- Indication: unresectable or metastatic disease
- Common regimens
- Cisplatin and fluorouracil [20]
- Oxaliplatin and capecitabine [20]
- Adenocarcinomas overexpressing ERBB2: trastuzumab [20]
- Tumors overexpressing PD-L1: pembrolizumab or nivolumab [21][22]
- Recurrence after chemoradiotherapy and surgical resection: nivolumab [23]
Other interventional therapy [13]
- Endoscopic placement of self-expanding metal stents for palliation of dysphagia and fistulae
- Gastrojejunostomy (GJ) tube for specialized nutrition support [24]

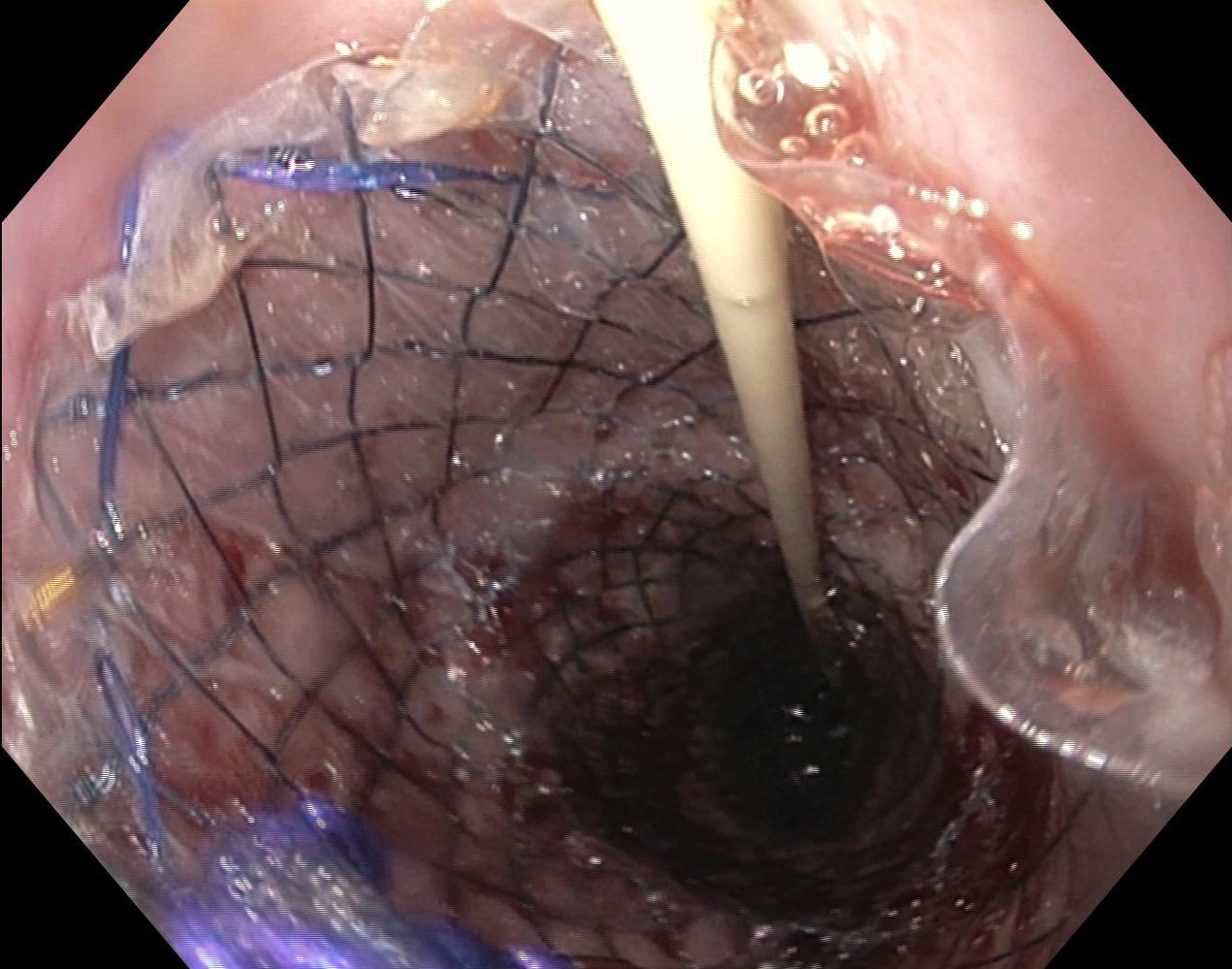
Endoscopic view of the esophagus
A newly placed self-expanding metal (nitinol) stent is visible. The stent holds the esophagus open as part of the palliative treatment for esophageal cancer.
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.
Complications
Cancer-associated complications
- Esophageal stenosis
- Tracheoesophageal fistula → passage of food and fluid into the respiratory tract → ↑ risk of aspiration pneumonia
-
Metastasis, e.g.: [13]
- Squamous cell carcinoma → lungs and thorax
- Adenocarcinoma → liver, peritoneum, bones [13]
Treatment-associated complications
-
Surgical complications
- Anastomotic leak or stricture
- Recurrent laryngeal nerve injury
-
Functional gastrointestinal disorders
- Dysphagia
- Reflux
- Dumping syndrome
We list the most important complications. The selection is not exhaustive.
CT chest (with contrast; axial plane; mediastinal window)
The wall of the esophagus is markedly thickened (green overlay). A fistula (arrow) is seen between the esophagus and trachea (T). Dependent material (red overlay) is present in the esophagus.
Source: © IMPP
Prognosis
- Prognosis is generally poor due to an aggressive course (due to an absent serosa in the esophageal wall) and typically late diagnosis. [12][25]
- The Surveillance, Epidemiology, and End Results (SEER) database tracks survival rates for patients with EC in the United States.
| Estimated survival of patients diagnosed with EC between 2012–2018 [26] | ||
|---|---|---|
| SEER stage | 5-year relative survival rate | |
| Localized |
|
|
| Regional |
|
|
| Distant |
|
|
| Combined (any stage) |
|
|
Related One-Minute Telegram
- One-Minute Telegram 144-2026-1/3: Is meat-free risk-free? A pooled cohort view of diet and cancer
Interested in the newest medical research, distilled down to just one minute? Sign up for the One-Minute Telegram in “Tips and links” below.
External Resources
References
- "Esophagus cancer - Key Statistics for Esophageal Cancer". https://www.cancer.org/cancer/esophagus-cancer/about/key-statistics.html. [2020-03-20]
- Patel N, Benipal B. "Incidence of Esophageal Cancer in the United States from 2001-2015: A United States Cancer Statistics Analysis of 50 States". Cureus. (2018)
- Wang Q-L, Xie S-H, Wahlin K, Lagergren J. "Global time trends in the incidence of esophageal squamous cell carcinoma". Clinical Epidemiology. Volume 10. :717-728. (2018)
- Short MW, Burgers KG, Fry VT. "Esophageal Cancer.". Am Fam Physician. 95(1). :22-28. (2017)
- Ribeiro U, Posner MC, Safatle-ribeiro AV, Reynolds JC. "Risk factors for squamous cell carcinoma of the oesophagus". British Journal of Surgery . 83(9). :1174-85. (1996)
- Straif K, Weiland SK, Bungers M et al. "Exposure to high concentrations of nitrosamines and cancer mortality among a cohort of rubber workers". Occupational and Environmental Medicine. 57(3). :180-187. (2000)
- Liyanage SS, Rahman B, Ridda I, et al. "The Aetiological Role of Human Papillomavirus in Oesophageal Squamous Cell Carcinoma: A Meta-Analysis". PLoS ONE. 8(7). :e69238. (2013)
- Domingues-Ferreira M, Grumach AS, Duarte AJDS, De Moraes-Vasconcelos D. "Esophageal cancer associated with chronic mucocutaneous candidiasis. Could chronic candidiasis lead to esophageal cancer?". Medical Mycology. 47(2). :201-205. (2008)
- Delsing CE, Bleeker-Rovers CP, van de Veerdonk FL, et al. "Association of esophageal candidiasis and squamous cell carcinoma". Medical Mycology Case Reports. 1(1). :5-8. (2012)
- Siewert JR, Stein HJ. "Classification of adenocarcinoma of the oesophagogastric junction". Br J Surg. 85(11). :1457-1459. (1998)
- Lin D, Khan U, Goetze TO, et al. "Gastroesophageal Junction Adenocarcinoma: Is There an Optimal Management?". American Society of Clinical Oncology educational book. American Society of Clinical Oncology. Annual Meeting. 39. :e88-e95. (2019)
- Rice TW, Gress DM, Patil DT, et al. "Cancer of the esophagus and esophagogastric junction-Major changes in the American Joint Committee on Cancer eighth edition cancer staging manual". CA Cancer J Clin. 67(4). :304-317. (2017)
- Varghese TK, Hofstetter WL, Rizk NP et al. "The society of thoracic surgeons guidelines on the diagnosis and staging of patients with esophageal cancer". The Annals of Thoracic Surgery. 96(1). :346-56. (2013)
- Alsop BR, Sharma P. "Esophageal Cancer". Gastroenterol Clin North Am. 45(3). :399-412. (2016)
- Wilkinson JM, Codipilly DC, Wilfahrt RP. "Dysphagia: Evaluation and Collaborative Management". Am Fam Physician. 103(2). :97-106. (2021)
- Raptis CA, Goldstein A, Henry TS, et al. "ACR Appropriateness Criteria® Staging and Follow-Up of Esophageal Cancer". J Am Coll Radiol. 19(11). :S462-S472. (2022)
- Jain S, Dhingra S. "Pathology of esophageal cancer and Barrett’s esophagus". Annals of Cardiothoracic Surgery. 6(2). :99-109. (2017)
- Shah MA, Kennedy EB, Catenacci DV, et al. "Treatment of Locally Advanced Esophageal Carcinoma: ASCO Guideline". J Clin Oncol. 38(23). :2677-2694. (2020)
- Evans JA, Early DS, Chandraskhara V, et al. "The role of endoscopy in the assessment and treatment of esophageal cancer". Gastrointest Endosc. 77(3). :328-334. (2013)
- Shah MA. "Update on Metastatic Gastric and Esophageal Cancers". J Clin Oncol. 33(16). :1760-1769. (2015)
- Sun JM, Shen L, Shah MA, et al. "Pembrolizumab plus chemotherapy versus chemotherapy alone for first-line treatment of advanced oesophageal cancer (KEYNOTE-590): a randomised, placebo-controlled, phase 3 study". Lancet. 398(10302). :759-771. (2021)
- Doki Y, Ajani JA, Kato K, et al. "Nivolumab Combination Therapy in Advanced Esophageal Squamous-Cell Carcinoma". N Engl J Med. 386(5). :449-462. (2022)
- Shah MA, Hofstetter WL, Kennedy EB. "Immunotherapy in Patients With Locally Advanced Esophageal Carcinoma: ASCO Treatment of Locally Advanced Esophageal Carcinoma Guideline Rapid Recommendation Update". J Clin Oncol. 39(28). :3182-3184. (2021)
- Ahmed O, Lee JH, Thompson CC, Faulx A. "AGA Clinical Practice Update on the Optimal Management of the Malignant Alimentary Tract Obstruction: Expert Review". Clin Gastroenterol Hepatol. 19(9). :1780-1788. (2021)
- Berry MF. " Esophageal cancer: staging system and guidelines for staging and treatment". Journal of Thoracic Disease. 6(Suppl 3). :S289-97. (2014)
- "Survival Rates for Esophageal Cancer". https://www.cancer.org/cancer/esophagus-cancer/detection-diagnosis-staging/survival-rates.html. [2022-03-01]