Summary
Eye pain and redness are symptoms that often manifest together, but not always. They present a diagnostic challenge due to the wide range of possible causes requiring quick risk stratification and appropriate action. Causes are generally diagnosed clinically and include traumatic injury, inflammatory and/or infectious conditions, and other (e.g., neurological) conditions. Vision-threatening causes must be urgently ruled out. Assessment begins with a focused history, including both ophthalmologic and relevant nonophthalmologic symptoms, medical history (e.g., contact lens use, autoimmune conditions), and past surgeries. A focused ophthalmologic examination is then performed, which includes many aspects of the comprehensive eye examination (e.g., visual acuity, examination of the extraocular muscles, and slit-lamp examination). The diagnosis is narrowed based on clinical findings, and condition-specific diagnostics and treatment are initiated. Vision-threatening causes of eye pain require urgent ophthalmology consultation, while most non-vision-threatening causes may be followed up with outpatient ophthalmology.
Etiology
Etiologies of eye pain (with or without redness) can be categorized by immediate threats to vision and underlying mechanism.
Vision-threatening causes [1]
Traumatic
Vision-threatening traumatic injuries are frequently associated with eye redness.
- Open globe injury
- Corneal foreign body
- Blunt trauma
- Orbital fracture
- Ocular burns
- Retrobulbar hematoma
- Corneal laceration
Inflammatory and/or infectious
Inflammatory and/or infectious vision-threatening causes of eye pain generally manifest with a red eye.
-
Keratitis
- Bacterial keratitis
- Viral keratitis
- Fungal keratitis
- Acanthamoeba keratitis
- Scleritis
- Anterior uveitis
- Corneal ulcer
- Orbital cellulitis
- Herpes zoster ophthalmicus
- Endophthalmitis
Other
-
Red eye
- Acute angle-closure glaucoma
- Orbital compartment syndrome
- Stevens-Johnson syndrome or toxic epidermal necrolysis
-
Non-red eye
- Optic neuritis
- Giant cell arteritis
- Cavernous sinus thrombosis
Non-vision-threatening causes [1]
Traumatic
-
Red eye
- Hyphema
- Corneal abrasion
- Corneal erosion
-
Non-red eye
- Eyelid laceration
- Lacrimal duct laceration
Inflammatory and/or infectious
-
Red eye
- Photokeratitis
- Keratoconjunctivitis
- Inflamed pinguecula
-
Non-red eye
- Preseptal cellulitis
- Dacryocystitis
- Dacryoadenitis
- Hordeolum
Conjunctivitis, blepharitis, episcleritis, and allergic contact dermatitis are typically painless but can manifest with discomfort if inflammation is severe.
Other
- Red eye: Keratoconjunctivitis sicca (dry eye disease)
-
Non-red eye
- Orbital tumor
- Intracranial tumor
Cluster headaches and certain types of migraines can manifest with pain localized to the eye (see “Mimics”).
Initial management
Approach
- Perform a focused clinical evaluation to narrow the diagnosis and localize the lesion (see “Clinical evaluation”).
- Begin critical interventions immediately as indicated, e.g.:
- Acute management of traumatic eye injuries (including open globe injuries)
- Treatment of acute angle-closure glaucoma
- Lateral canthotomy and cantholysis in orbital compartment syndrome
- Immediate large-volume irrigation of ocular chemical burns
- Corneal foreign body removal
- Consult ophthalmology urgently for vision-threatening causes of eye pain or red flags for painful red eye.
- Administer analgesia as indicated, e.g., analgesia for corneal pain
- Obtain additional diagnostics as indicated and initiate condition-specific treatment.
Red flags for painful red eye [3]
- Moderate to severe eye pain
- Visual impairment
- Red flags for serious eye injury (e.g., ocular chemical burn, penetrating eye injury)
- Opacification or visible defect of the cornea
- Irregular pupil
- Impaired pupillary reflex
- Ciliary flush
Clinical evaluation
Focused history [1][2]
Ophthalmologic
- Symptom onset
- Character of pain (e.g., burning, dull, sharp, foreign body sensation)
- Presence or absence of eye redness
- Visual disturbances
- Changes in visual acuity or vision loss
- Visual field defects
- Diplopia
- Changes in color vision
- Photophobia
- Discharge or crusting
- Eyelid swelling
- Mechanism of injury, if applicable
- Recent ocular surgery
- New ocular medications
-
Contact lens hygiene
- Wear schedule (e.g., sleeping in contact lenses, overnight wear)
- Factors increasing contamination risk
- Wearing lenses past the expiration date
- Rinsing lenses in tap water and/or improper storage
- Swimming or hot tub use while wearing lenses
Nonophthalmologic
- Fever
- Headache
- Concurrent neurological symptoms
- Jaw claudication
- Skin lesions (e.g., periorbital erythema, vesicular rash)
- History of:
- Systemic diseases (e.g., multiple sclerosis, Sjogren syndrome)
- Immunocompromise
- Allergies
Focused physical examination [1][2]
See also “Examination of the eye.”
- Visual acuity (e.g., using Snellen chart)
- Visual field testing
- External eye examination
- Eversion of the upper eyelid (if indicated)
- Examination of extraocular muscles
- Pupillary examination
- Tonometry
- Slit-lamp examination (if indicated)
- Fluorescein staining (if indicated)



1. Ask the patient to look downwards for the duration of the examination.
2. Pull the upper eyelid down with one hand.
3. Apply pressure to the upper eyelid (∼ 3 mm above the lid margin) with a cotton swab with the other hand. Pull the eyelid forward and upwards and evert it over the cotton swab.
4. Hold the upper eyelid in the everted position and remove the cotton swab.
5. Inspect the conjunctiva and remove any foreign bodies.
6. Release the upper eyelid and ask the patient to look upwards or close the eye (the upper eyelid should return to its natural position).
Source: “Ectropionising, 2012, 08. 22., 01; Ectropionising, 2012, 08. 22., 02” by Marc Gabriel Schmid, Wikimedia Commons, licensed under CC BY-SA 3.0. Modifications: Two images merged, added censor bar.
{kind=link}
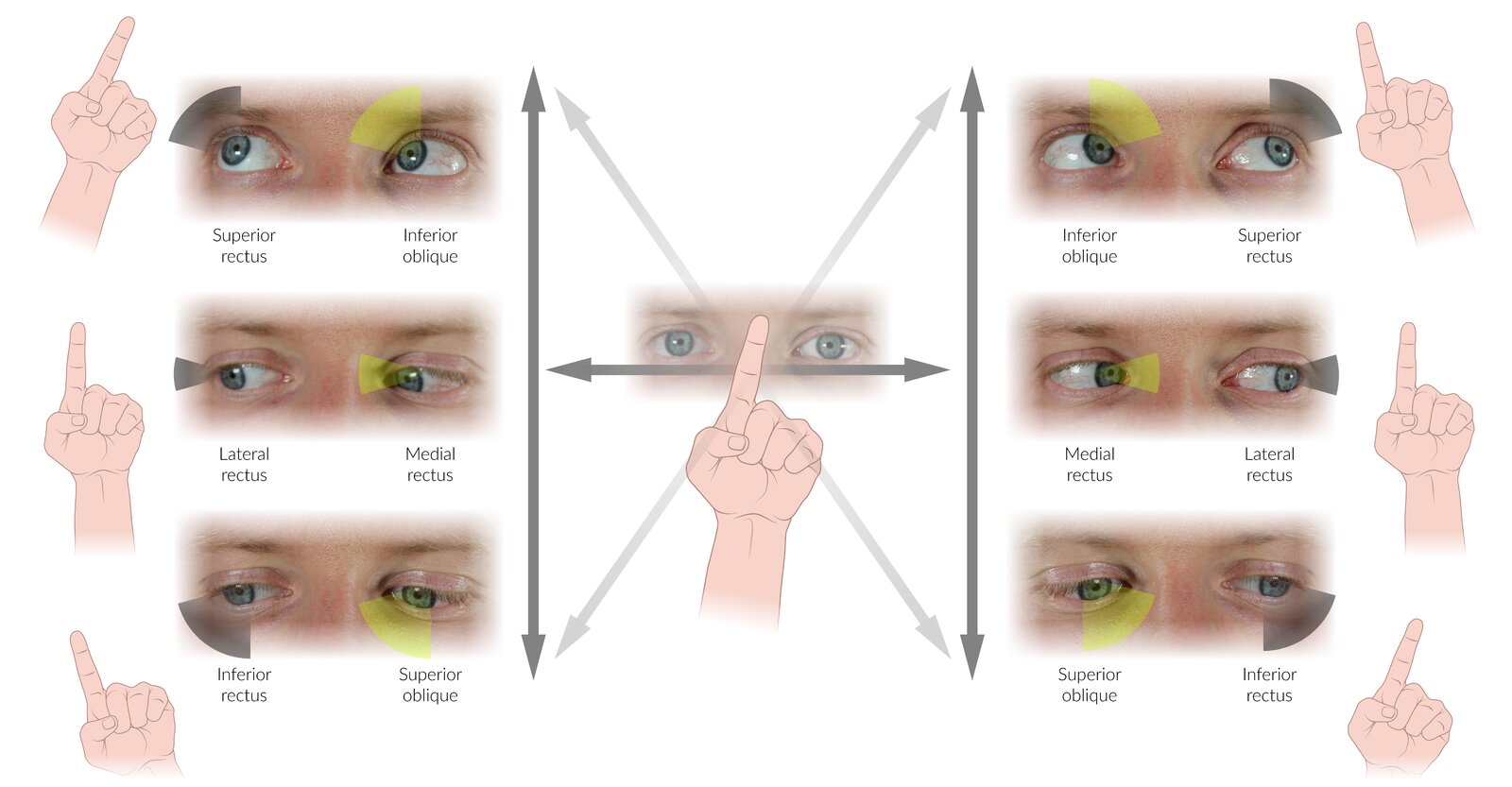
A quick clinical examination of extraocular muscle function can be performed by asking the patient to follow the examiner's finger with the eyes while keeping the head immobile. Tracing the letter “H” in the air (dark grey arrows) will prompt the patient to move through the 6 cardinal positions of gaze. In these positions, a single muscle is the primary mover for each eye.
Some examiners find it beneficial to return to the center between each cardinal position, drawing a star shape (dark grey horizontal arrow plus light grey arrows), while others combine the complete “H” and diagonal movements.
Note that for all muscles except the lateral- and medial recti, the directions in which these muscles are tested clinically (shown here) differ from the direction they would move the eyeball if acting in isolation. The difference arises because eye movements are the result of complex interactions between several extraocular muscles. Therefore, the movement used to test a particular muscle clinically is the movement that most effectively excludes the participation of other muscles. For example, while the superior oblique (SO) depresses and abducts the eye when acting in isolation, depression is also produced by the inferior rectus (IR), and abduction is also produced by the lateral rectus (LR). However, due to their different points of insertion, the IR is the more efficient depressor of the eye in abduction, while the SO is the more efficient depressor in adduction. Looking down and inwards, therefore, allows the isolated clinical examination of the SO (as shown here). Similar principles apply to the movements used for clinical testing of the IR, SR, and IO.
© AMBOSS
Diagnosis
Most conditions causing eye pain and redness are diagnosed clinically; laboratory testing and imaging are indicated in select cases.
Laboratory testing [1]
- Diagnostics for giant cell arteritis: e.g., ESR, CRP
- Urgent diagnostics for trauma patients
- Additional diagnostics as requested by ophthalmology
Imaging [1][2]
-
CT head and/or orbits
- Penetrating trauma and/or foreign body
- Orbital cellulitis (for confirmation and/or to assess for complications such as abscess)
-
MRI
- Suspected neurological cause: e.g., optic neuritis, intracranial tumor
- Contraindicated if a metallic foreign body is suspected
-
Ocular POCUS
- May be useful for assessing suspected penetrating eye injury or intraocular foreign body
- Contraindicated if open globe injury is suspected
Common vision-threatening causes
| Common vision-threatening causes of eye pain [1] | |||
|---|---|---|---|
| Characteristic clinical features | Diagnostic findings | Management | |
| Traumatic eye injuries [4][5][6] |
|
|
|
| Orbital compartment syndrome [7][8] |
|
|
|
| Orbital cellulitis [9][10] |
|
|
|
| Endophthalmitis [11][12] |
|
|
|
| Acute angle-closure glaucoma [13][14] |
|
|
|
| Optic neuritis [15][16] |
|
|
|
| Cranial giant cell arteritis (GCA) [17][18] |
|
|
|
| Herpes zoster ophthalmicus [19] |
|
|
|
| Bacterial keratitis [20] |
|
|
|
| Herpes simplex keratitis [21] |
|
|
|
| Corneal ulcer [22] |
|
|
|
| Corneal foreign body [23] |
|
|
|
| Anterior uveitis [24][25] |
|
|
|

















The left upper and lower eyelids are red and severely swollen, resulting in the patient not being able to open the eye. Orbital cellulitis is an emergency requiring immediate treatment.
Image source of original image: www.paediatrie-in-bildern.de. Created by: Dr. Thomas Rautenstrauch.
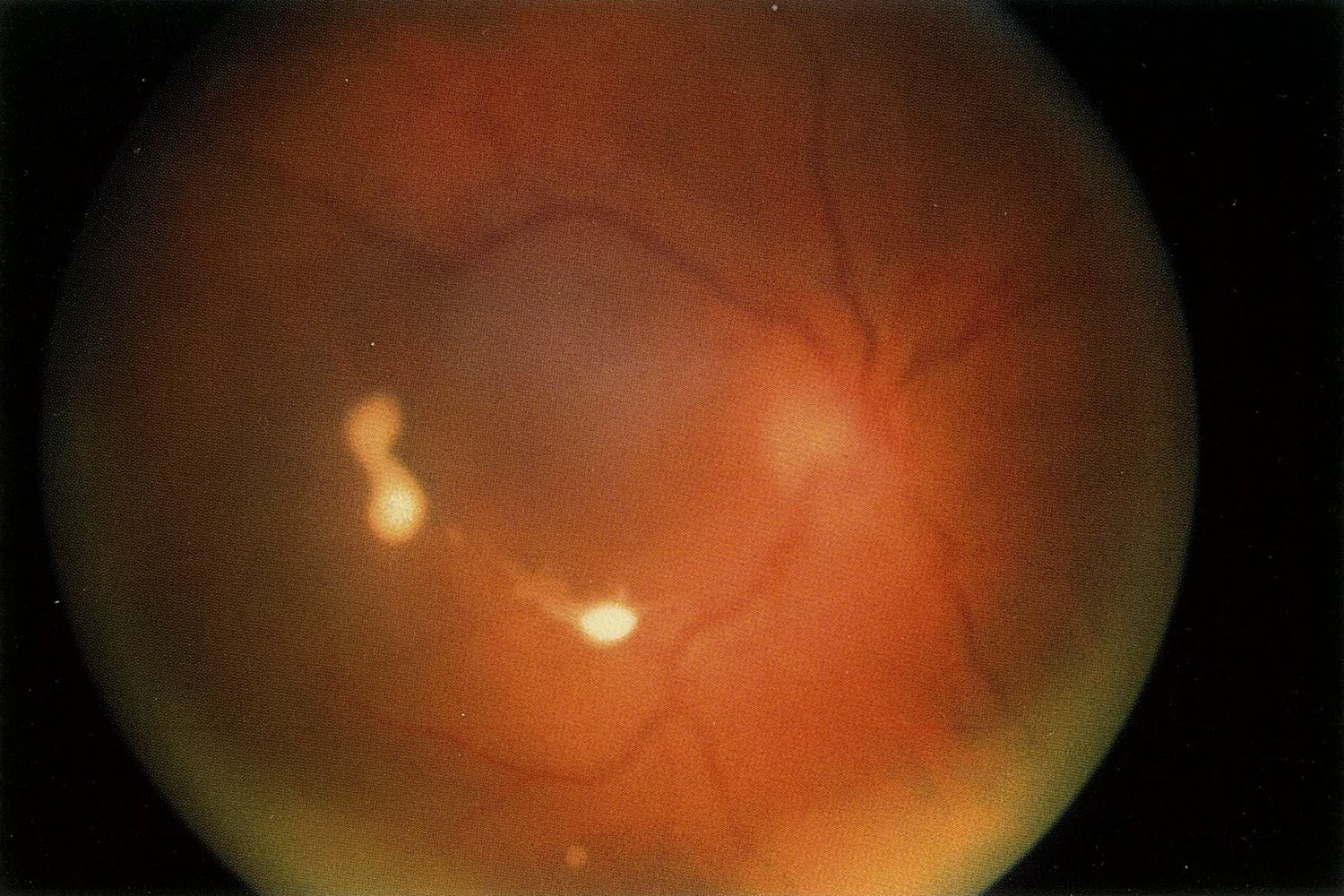
Fundus photography of a right eye
White and fluffy vitreous or retinal infiltrates are visible. Retinal details are blurred through the vitreous cellular infiltrate.
Candida is a common cause of fungal endophthalmitis. In patients with a systemic candida infection, endogenous endophthalmitis is a possible complication, as in the case here.
Source: © IMPP

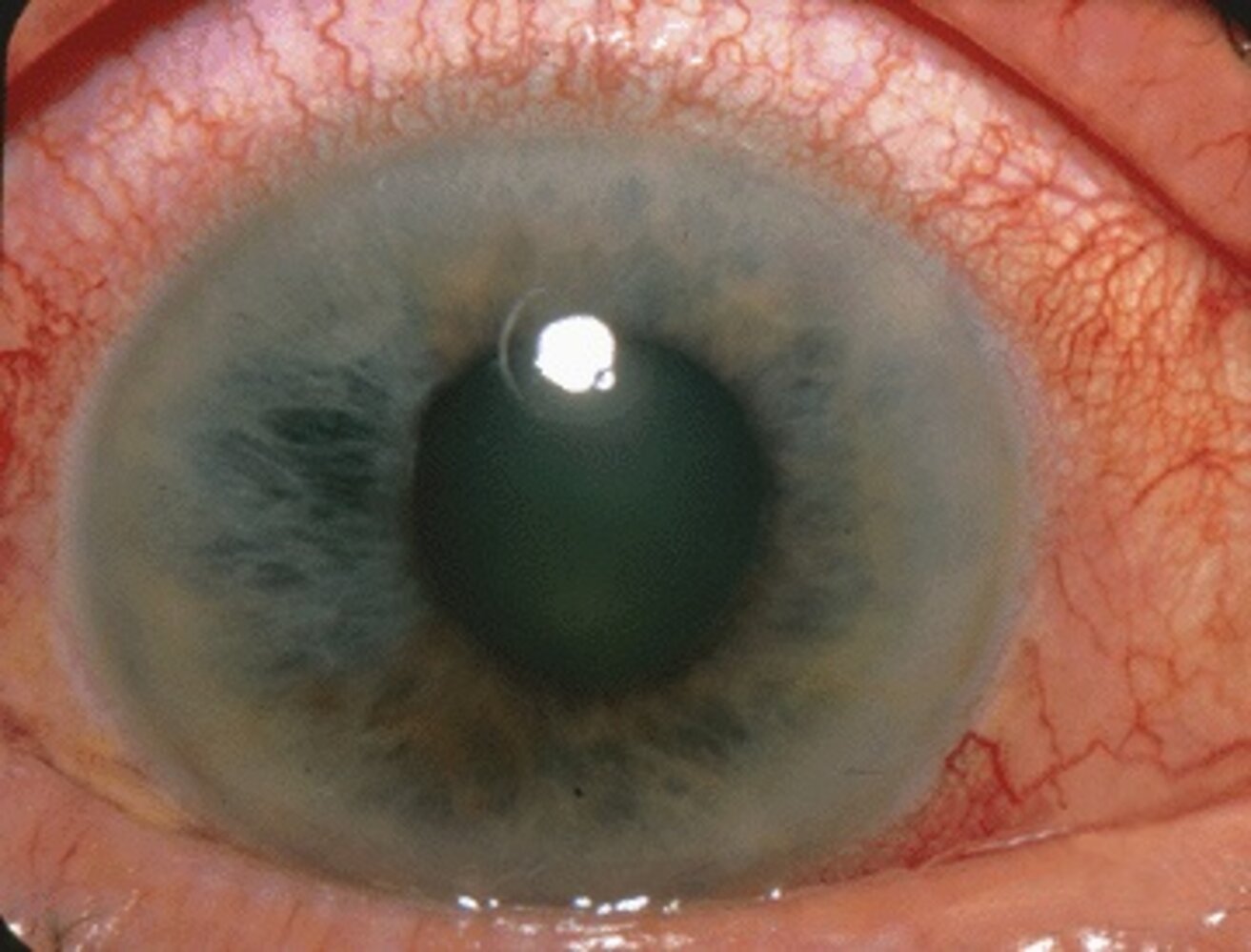
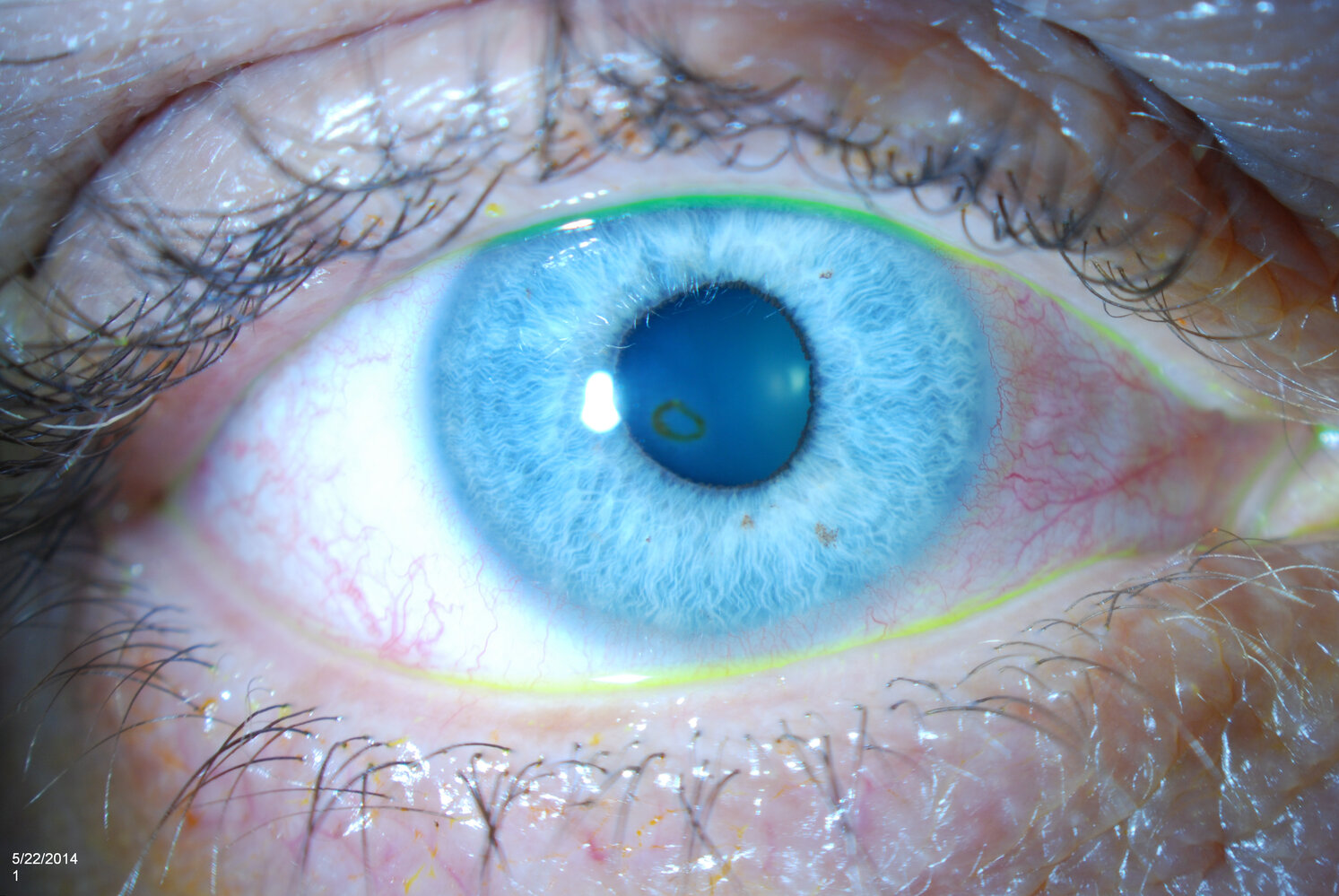
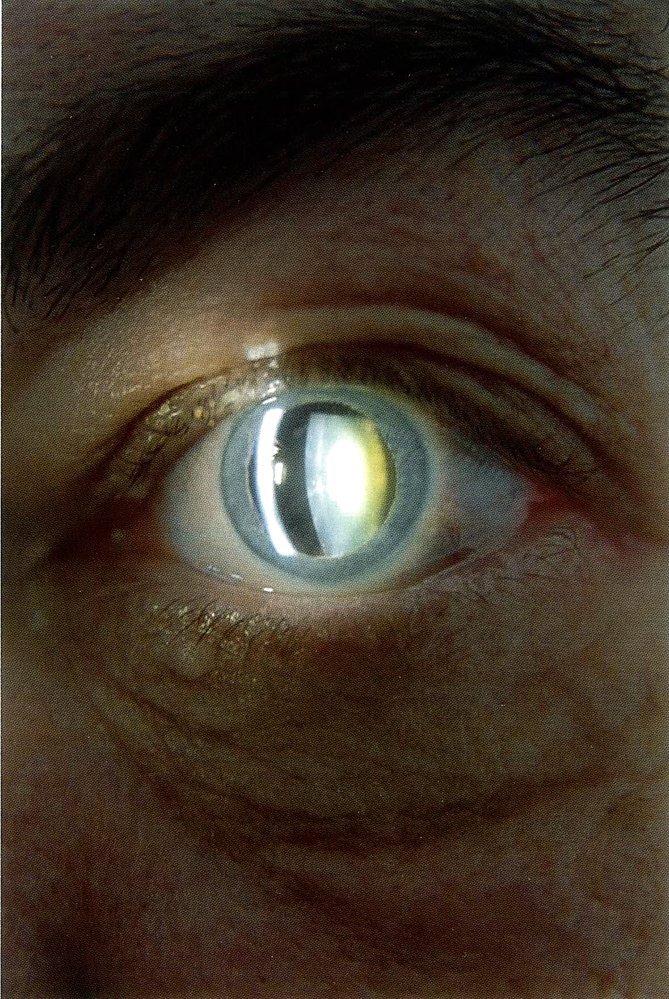
Photograph of the eyes of an adult woman with an intraocular pressure of 42 mm Hg in the right eye
The left eye appears normal. Mixed injection is seen in the right eye and the right pupil is mid-dilated and nonreactive to light.
This is the typical appearance of acute, markedly elevated intraocular pressure, often due to acute angle-closure glaucoma.
Source: “Acute angle closure glaucoma” by James Heilman, MD, Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}
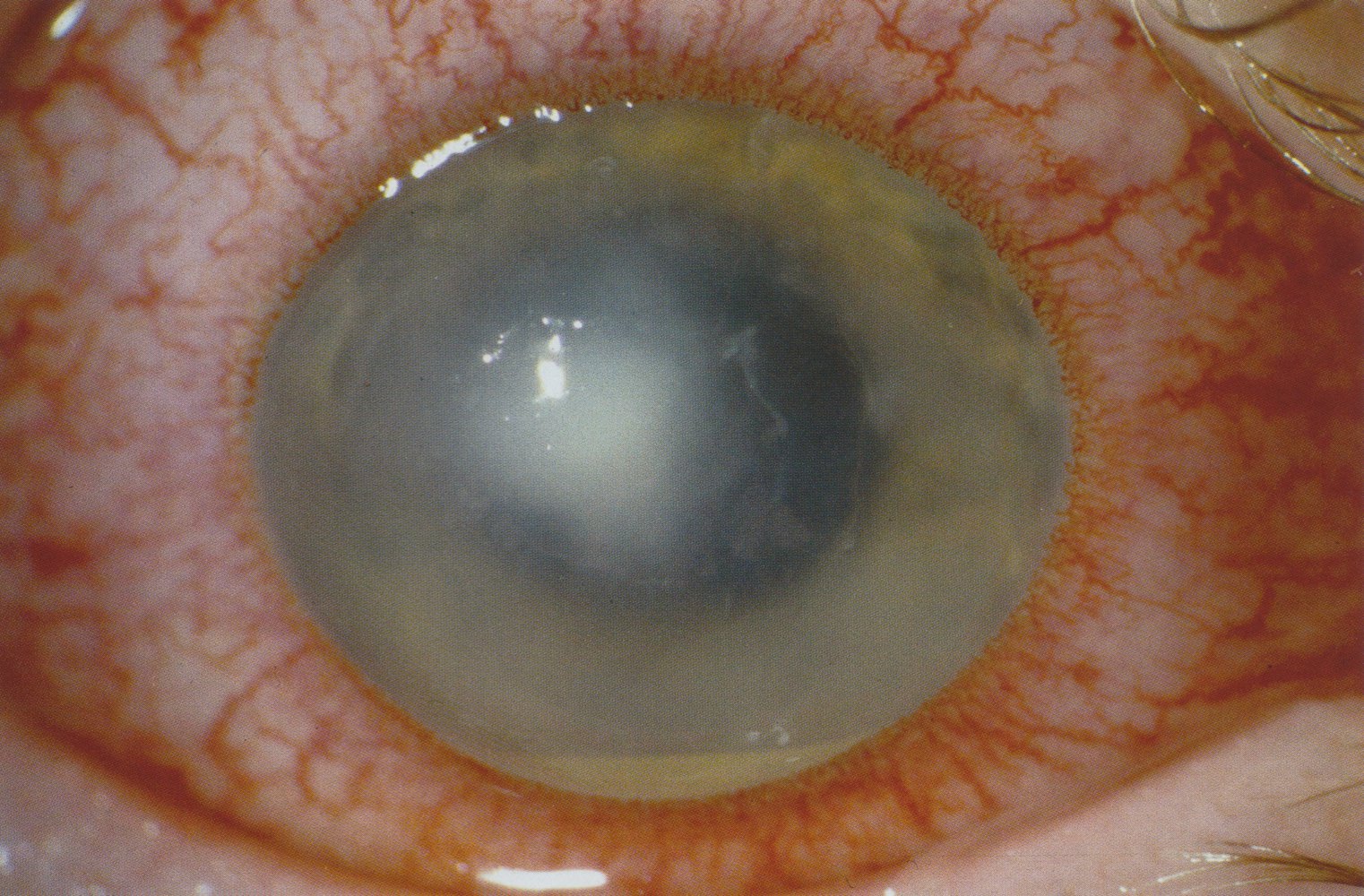
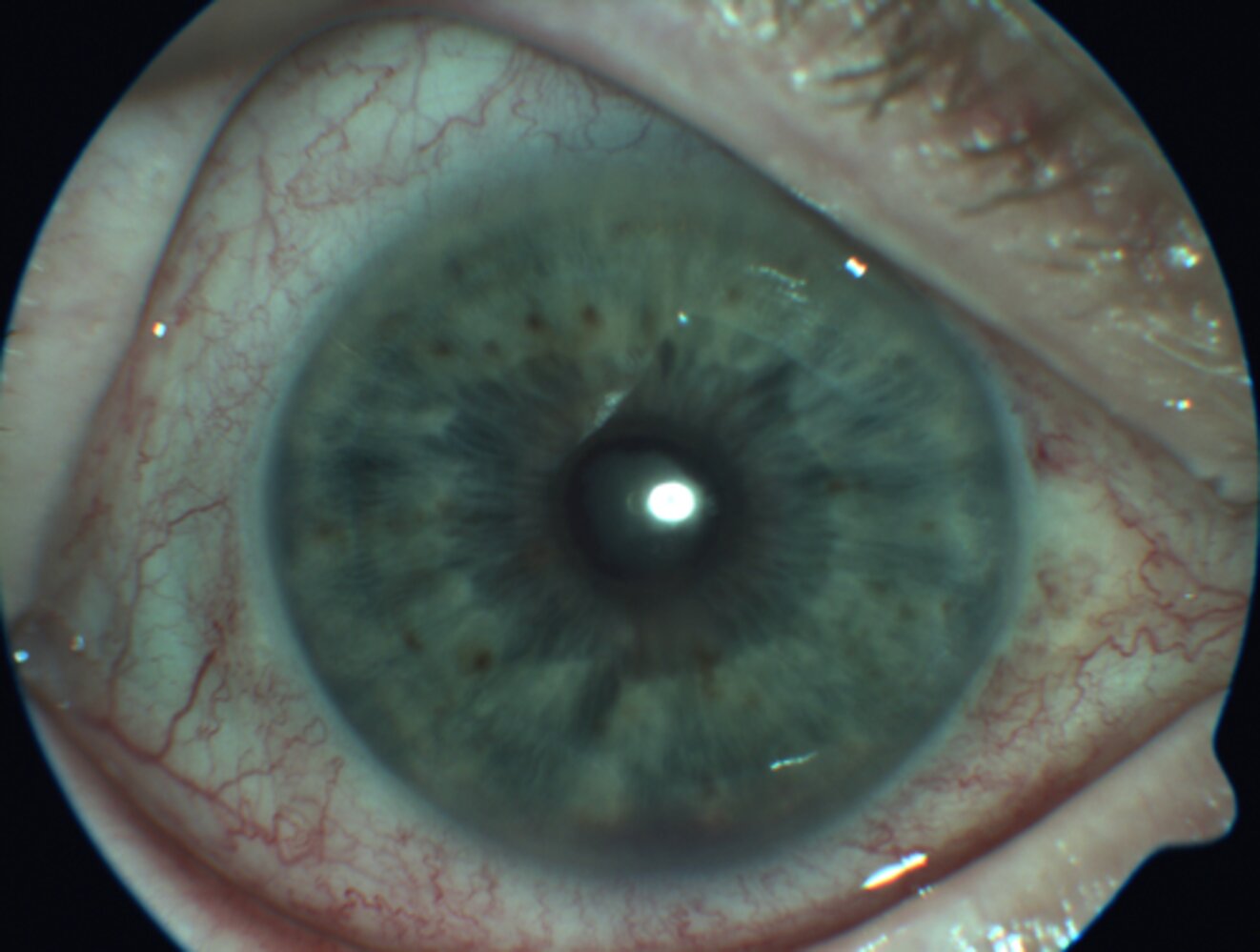
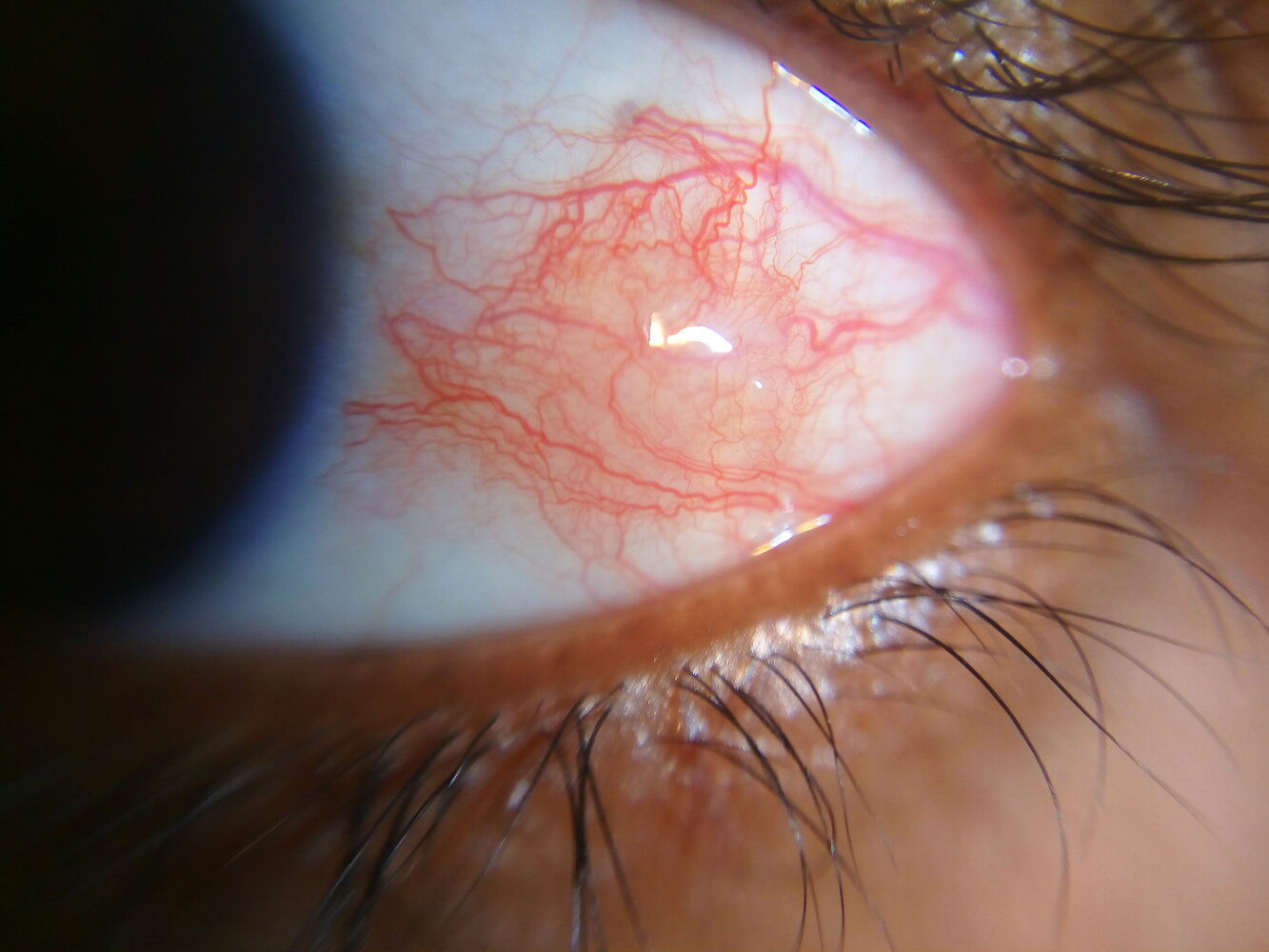
Slit-lamp photograph of anterior eye segment
Prominent blood vessels are visible on the sclera and conjunctiva (mixed injection). The pupil is medium wide and its shape is slightly irregular. Iris details appear blurred due to corneal endothelial decompensation, leading to corneal edema.
Source: “Acute Angle Closure-glaucoma” by Jonathan Trobe, Wikimedia Commons, licensed under CC BY 3.0.
{kind=link}
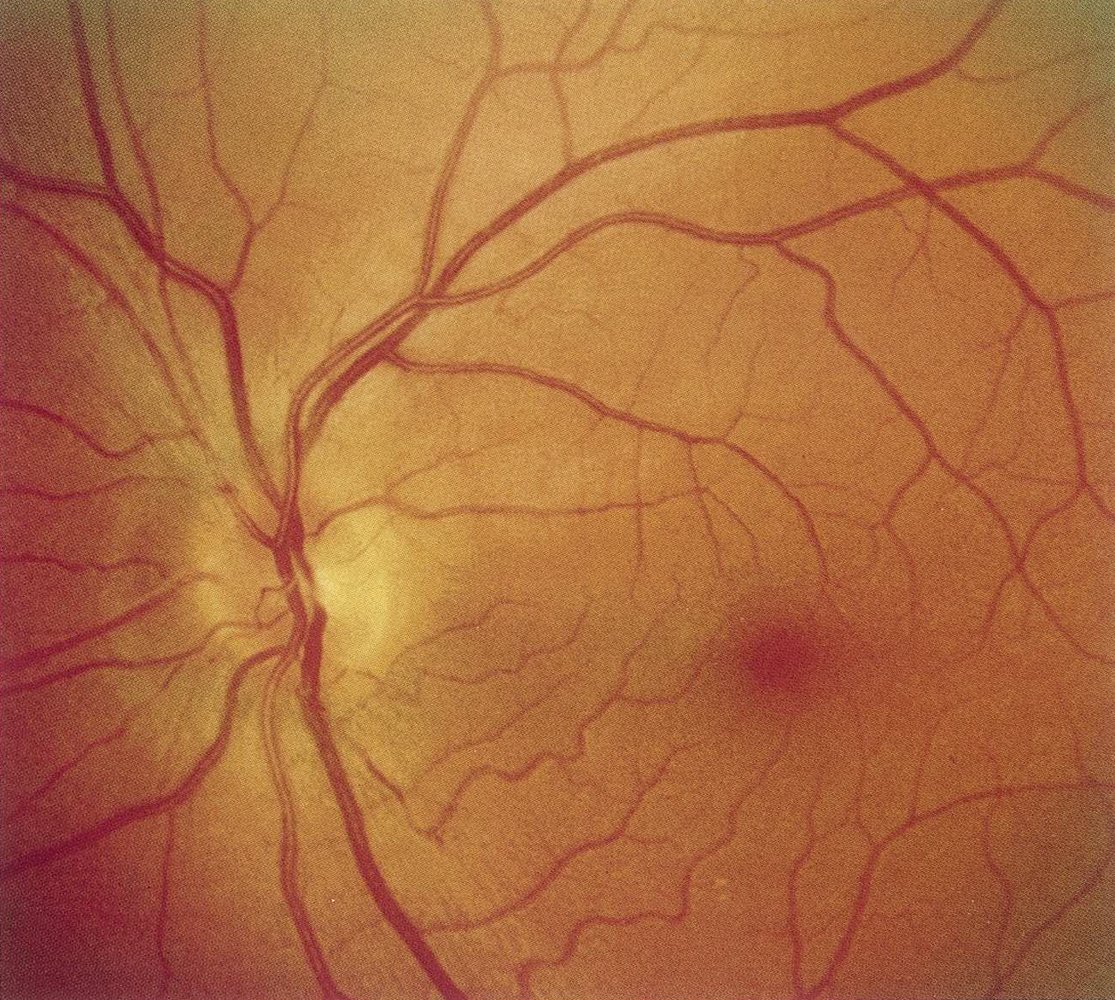
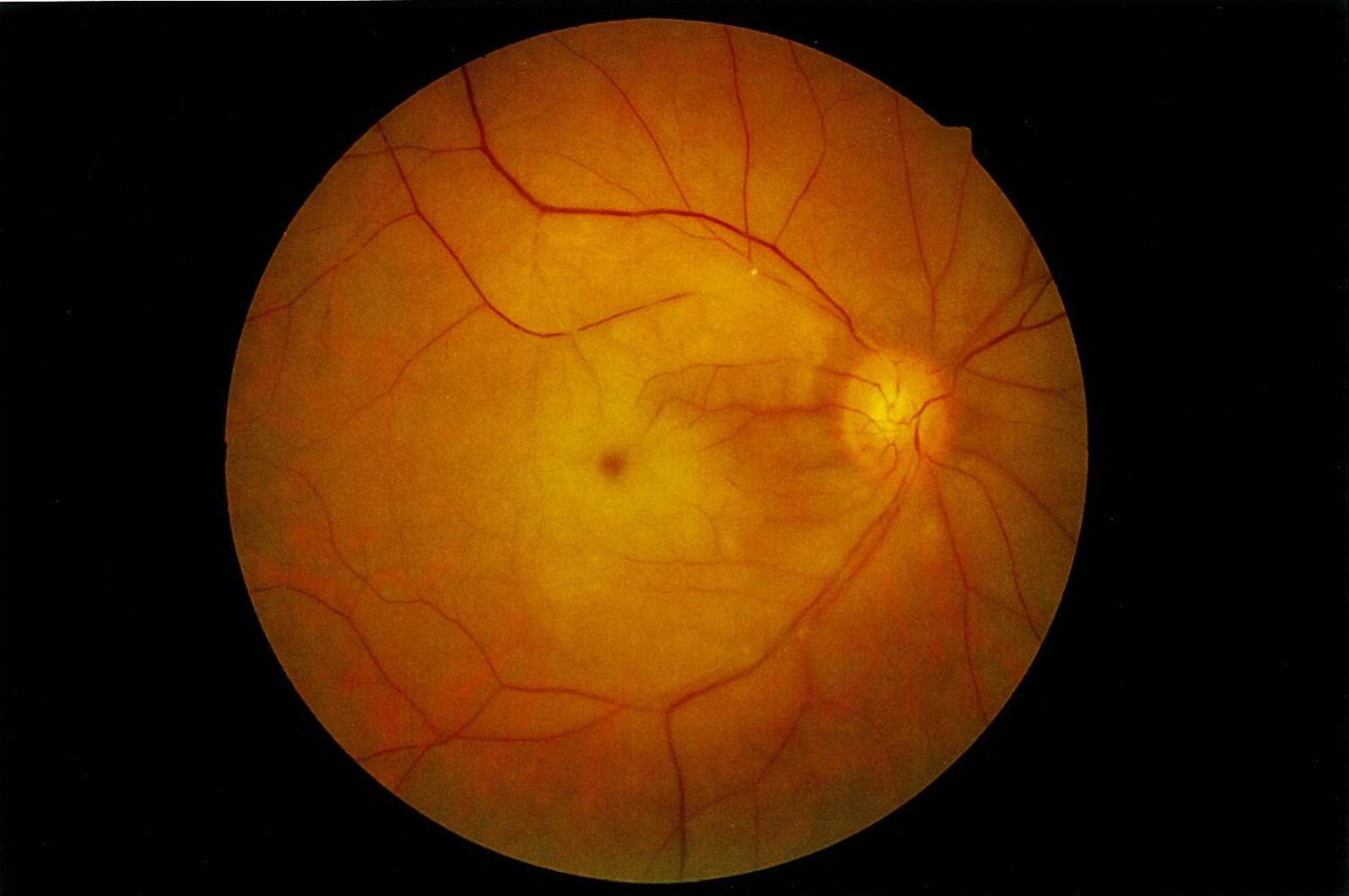
Fundus photography of the left eye of a patient with acute vision loss and painful eye movements
Discrete optic disc edema is visible: Discrete blurring of the nasal superior, superior, and temporal superior disc margin can be seen (green overlay). Otherwise, the fundus is normal.
This finding, in addition to the patient's symptoms, suggests papillitis in optic neuritis.
M: macula; circle: optic disc
Source: © IMPP

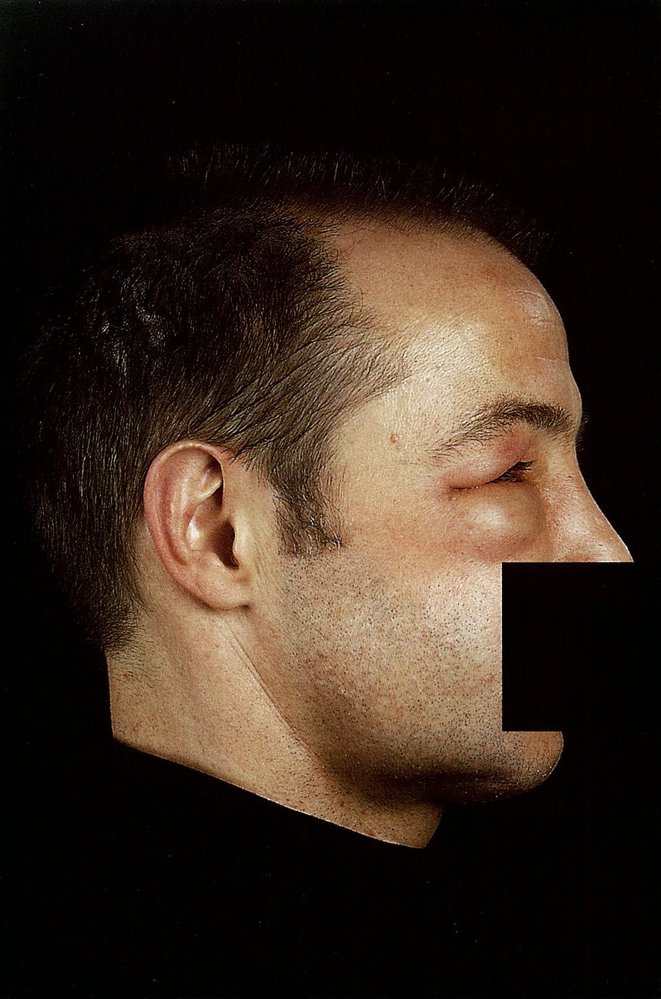
The superficial temporal artery is prominent, which is suggestive of giant cell arteritis.
Source: © IMPP

Three erythematous, maculopapular lesions with crusting can be seen on the left side of the face, at the hairline and supraorbitally. Left periorbital swelling and erythema are also visible.
The distribution and appearance of these lesions suggest herpes zoster ophthalmicus affecting the ophthalmic division of the trigeminal nerve.
This image is an adaptation. Source of original image: Wikimedia Commons. Original title: “Herpes Zoster im Augenbereich”. Created by: StromBer. Licensed under Public Domain. Modifications to original image: Added censor bar.
{kind=link}

Photograph showing reactivation of Herpes zoster infection
On the left side of the face, multiple partially confluent vesicles are visible on the tip and side of the nose (Hutchinson sign) and on the upper lip and cheek.
A positive Hutchinson sign of the nose indicates herpes zoster involvement of the nasociliary nerve (a branch of the ophthalmic division of the trigeminal nerve) and is associated with herpes zoster ophthalmicus.
Source: “Figure 2, in: Hutchinson’s Sign” by Lau L, Mirzakhani H, Governatori N, JETem, licensed under CC BY 4.0.
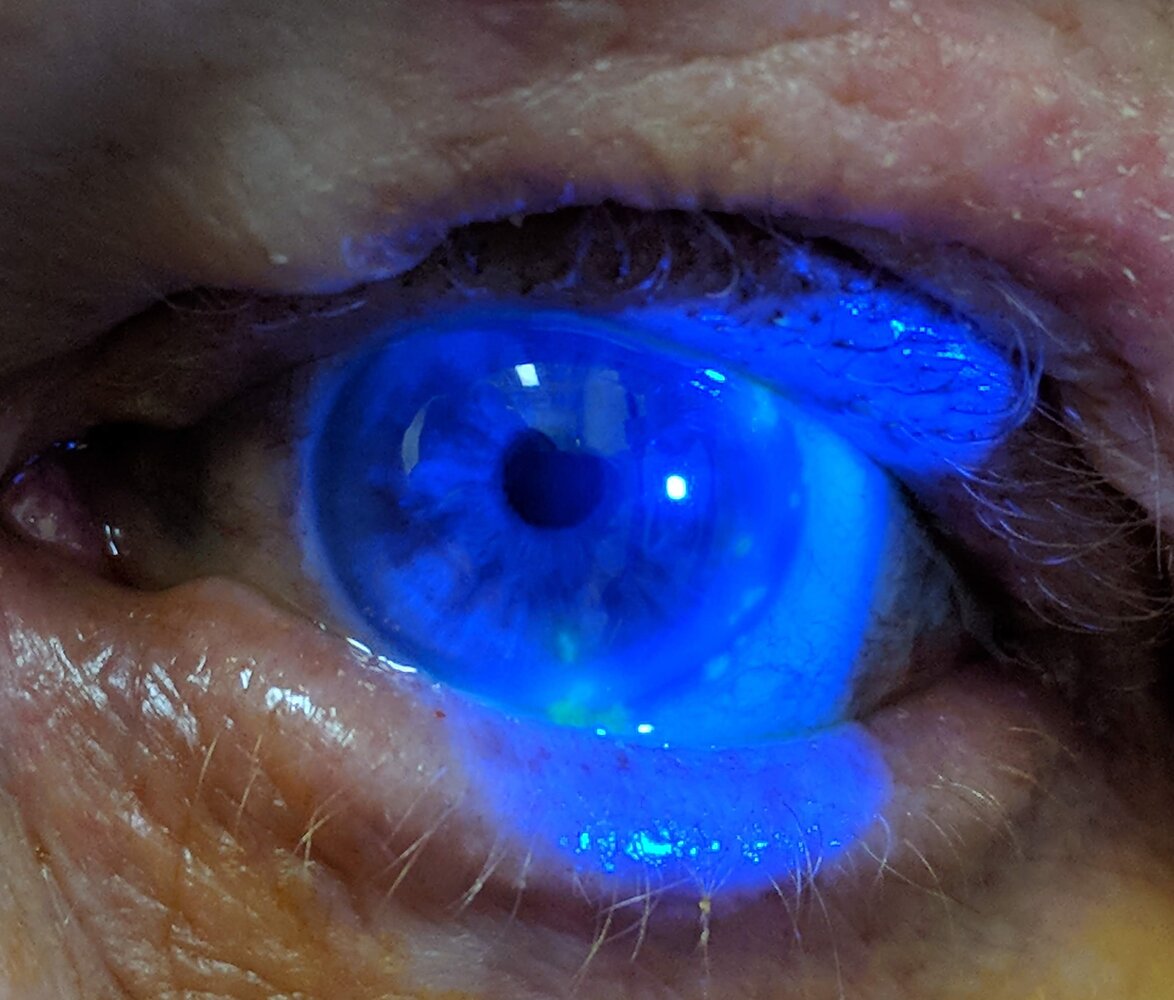
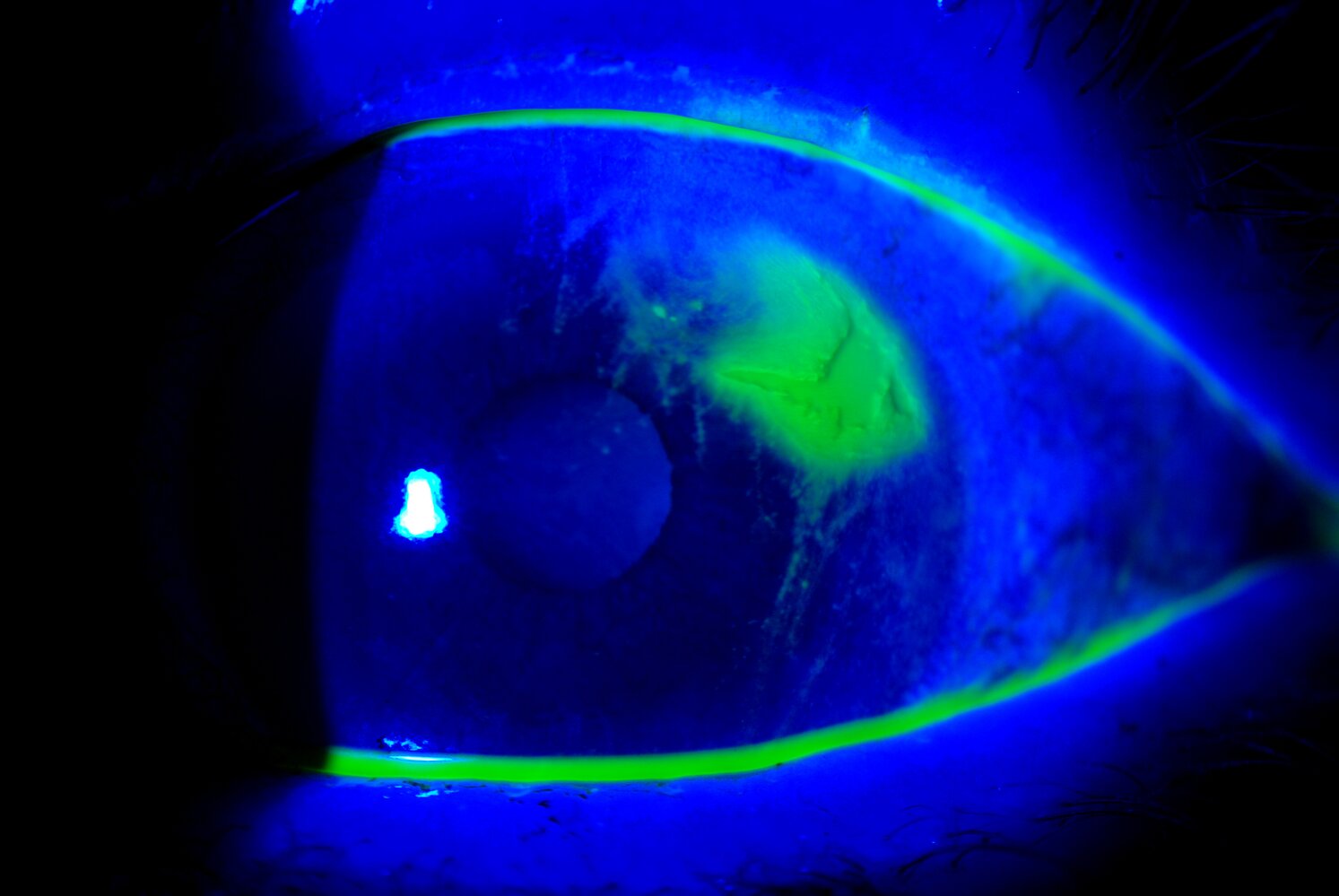
Slit-lamp photography, blue-light filter with fluorescein staining of a left eye
Superficial patchy erosions, marked by the fluorescein staining, are visible in a geographic pattern on the surface of the cornea (examples indicated by red overlay).
In combination with the cutaneous red lesions in the supraorbital region, the findings are typical for keratitis caused by herpes zoster ophthalmicus.
Source: “HerpesZosterOpth” by James Heilman, MD, Wikimedia Commons, licensed under CC BY-SA 4.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 4.0.
{kind=link}
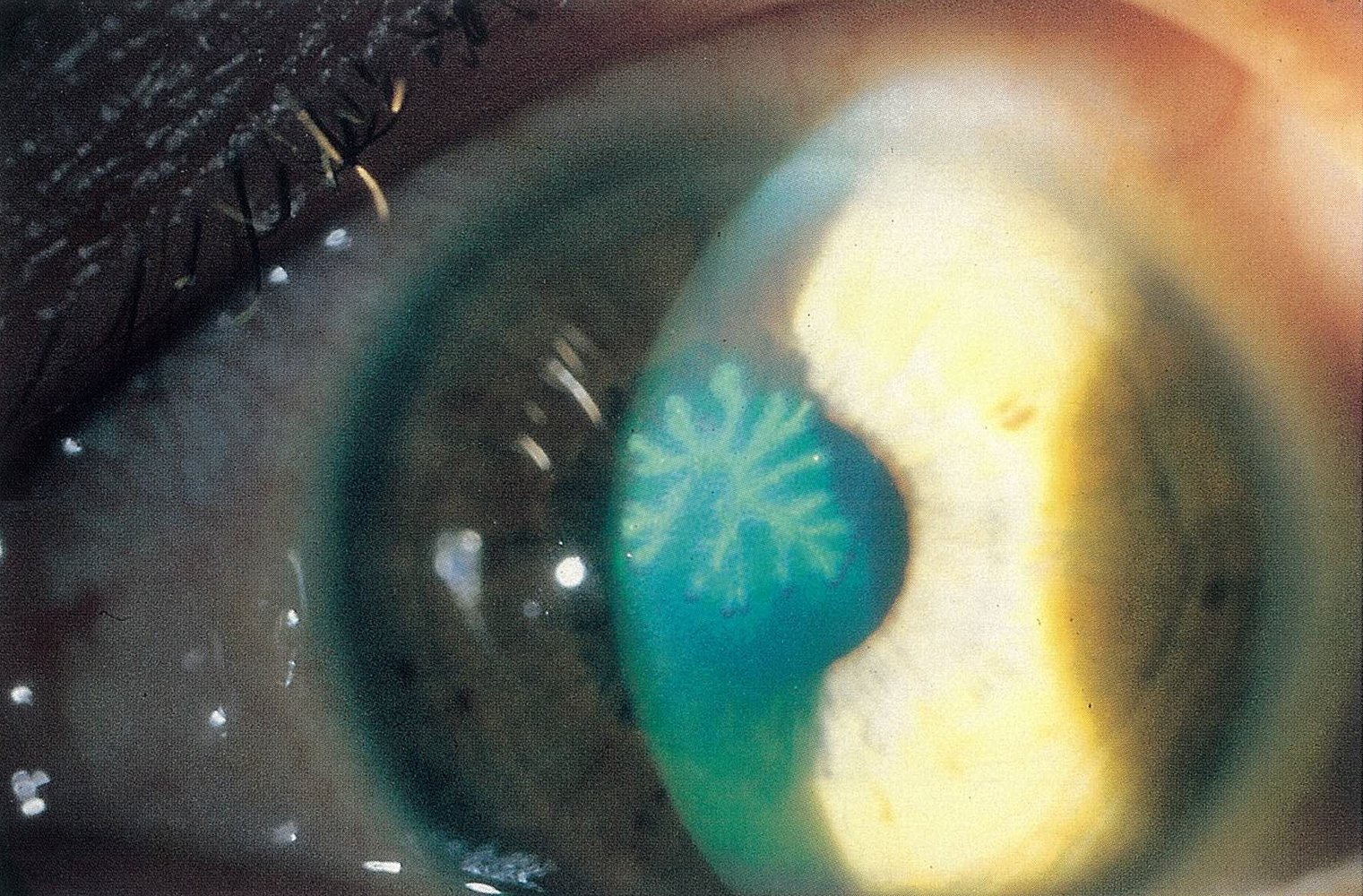
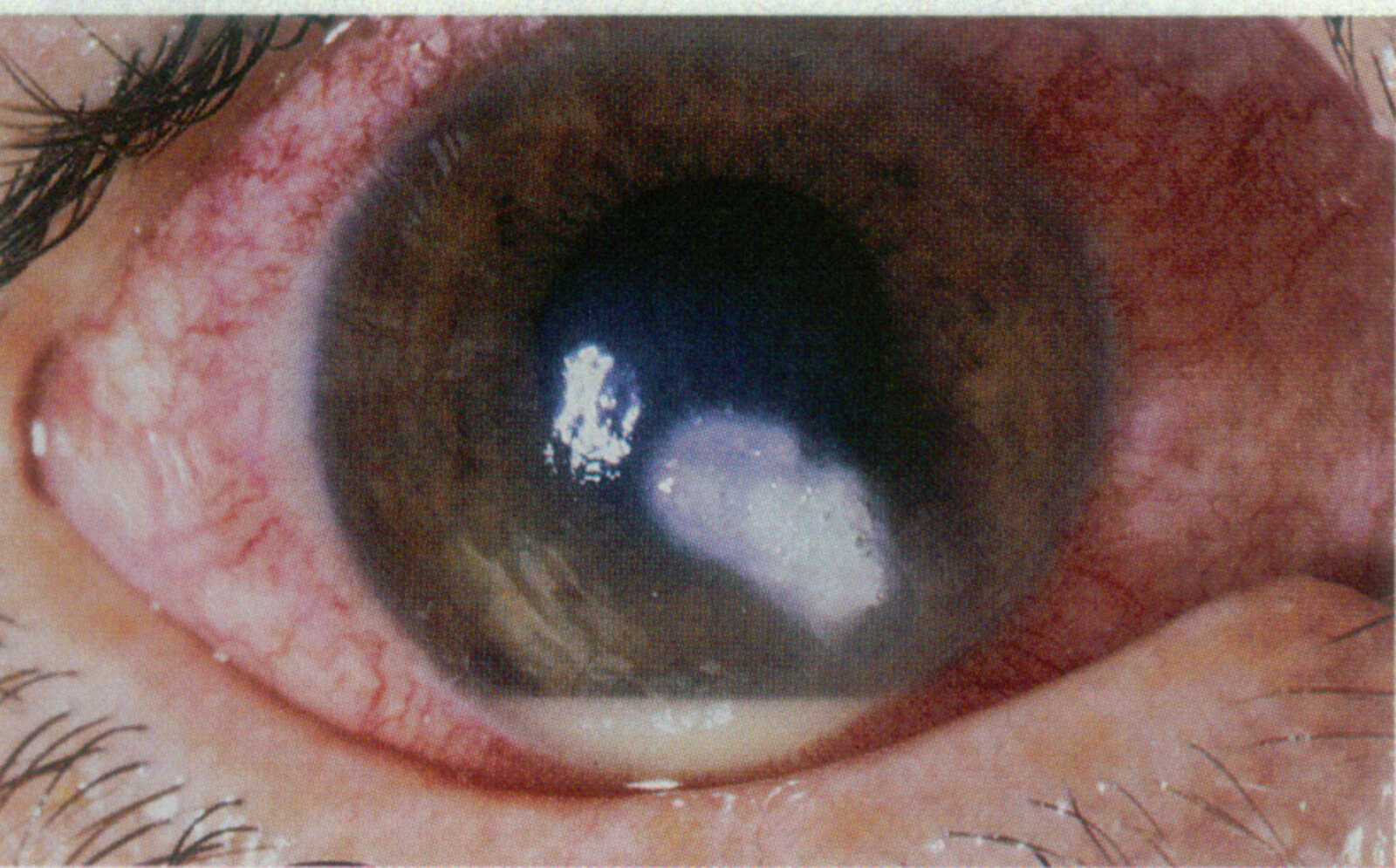
Prominent blood vessels are visible on the sclera and conjunctiva (mixed injection; examples indicated by arrowheads). A dense corneal infiltration (white opacification; green overlay) is visible at the center of the cornea. The peripheral cornea shows slight opacification indicating corneal decompensation (blurred details of the iris). An accumulation of white-yellow exudate (hypopyon; blue overlay) consisting of inflammatory cells and/or bacteria/fungi within the anterior chamber can be seen completely covering the inferior aspect of the iris.
These findings are consistent with infective keratitis, associated here with contact lens use.
Source: © IMPP
Slit-lamp photography of the cornea (fluorescein stain)
Dendritic lesions (red overlay) are visible on the cornea.
This finding is characteristic of herpes simplex keratitis.
Source: © IMPP
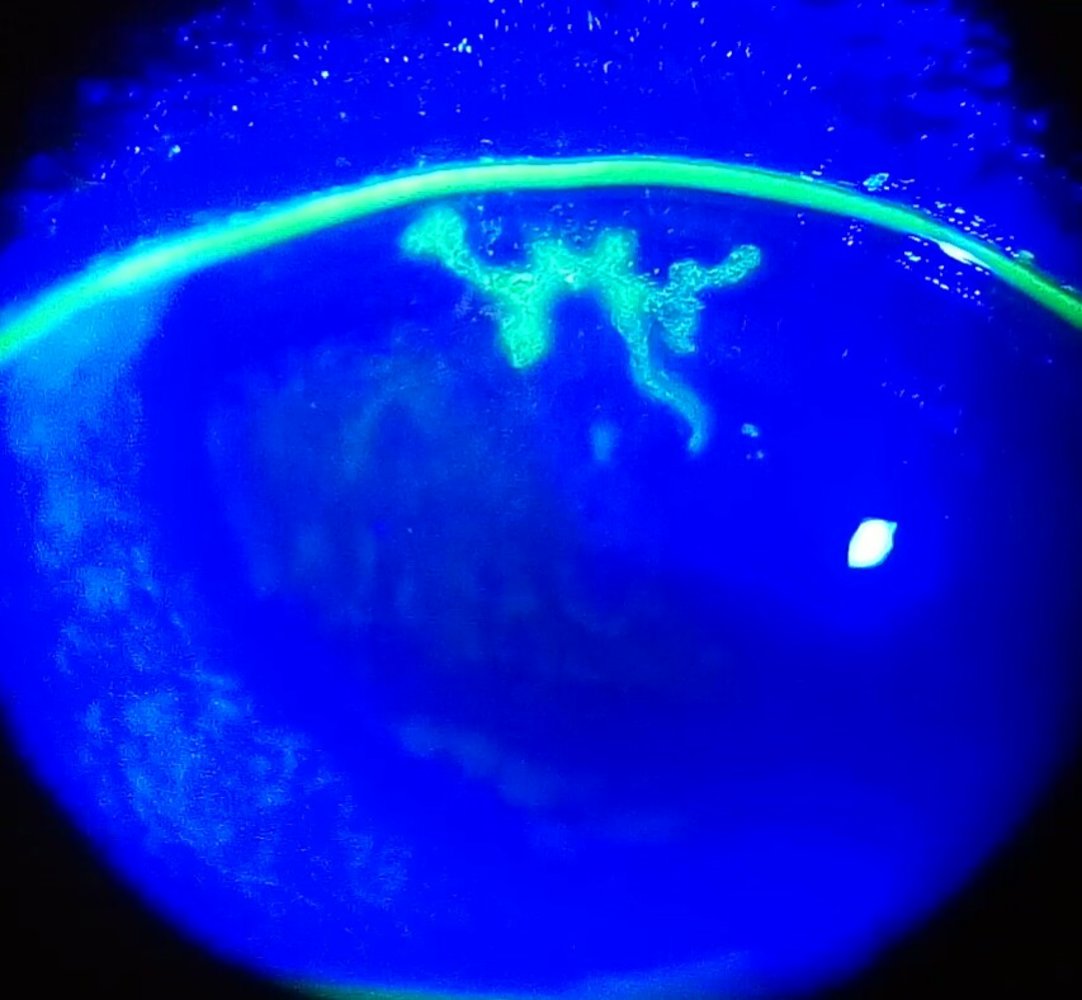
Slit-lamp photography with fluorescein stain and cobalt blue light filter
Dendritic lesions of the cornea appear green under cobalt blue illumination after fluorescein stain.
These lesions are characteristic of keratitis caused by herpes simplex virus (HSV).
Source: “Dendritic corneal ulcer” by Imrankabirhossain, Wikimedia Commons, licensed under CC BY-SA 4.0.
{kind=link}
Slit-lamp photography of the right eye of a patient with a history of contact lens overuse
Paracentral clouding (yellow overlay) is visible on the cornea, suggesting corneal infiltration. There is also a hypopyon (blue overlay) at the base of the anterior chamber, and marked mixed injection (a combination of ciliary and conjunctival injection) is visible.
These findings are typical of a corneal ulcer, which can be caused by contact lens overuse.
© Massachusetts Medical Society. All rights reserved. AMBOSS SE, exclusive licensee.

Right eye
A small brown foreign body (arrowhead) and a slight rust ring can be seen on the temporal corneal margin. Significant conjunctival injections are also visible.
Source: “Foreign body in eye” by E van Herk, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
Slit-lamp photography of the right eye (fluorescein stain) of an individual with tearing and redness after working with a grinding wheel
The paracentral cornea shows a brown rust ring (green overlay). The small brownish flecks are iris nevi (example indicated by arrowhead).
Rust rings develop from metallic foreign bodies of the cornea that are not removed promptly.
Source: "51434_001.JPG", Mayo Clinic Jacksonville, Florida, Retina Gallery licensed under Public Domain
Photograph of the right eye
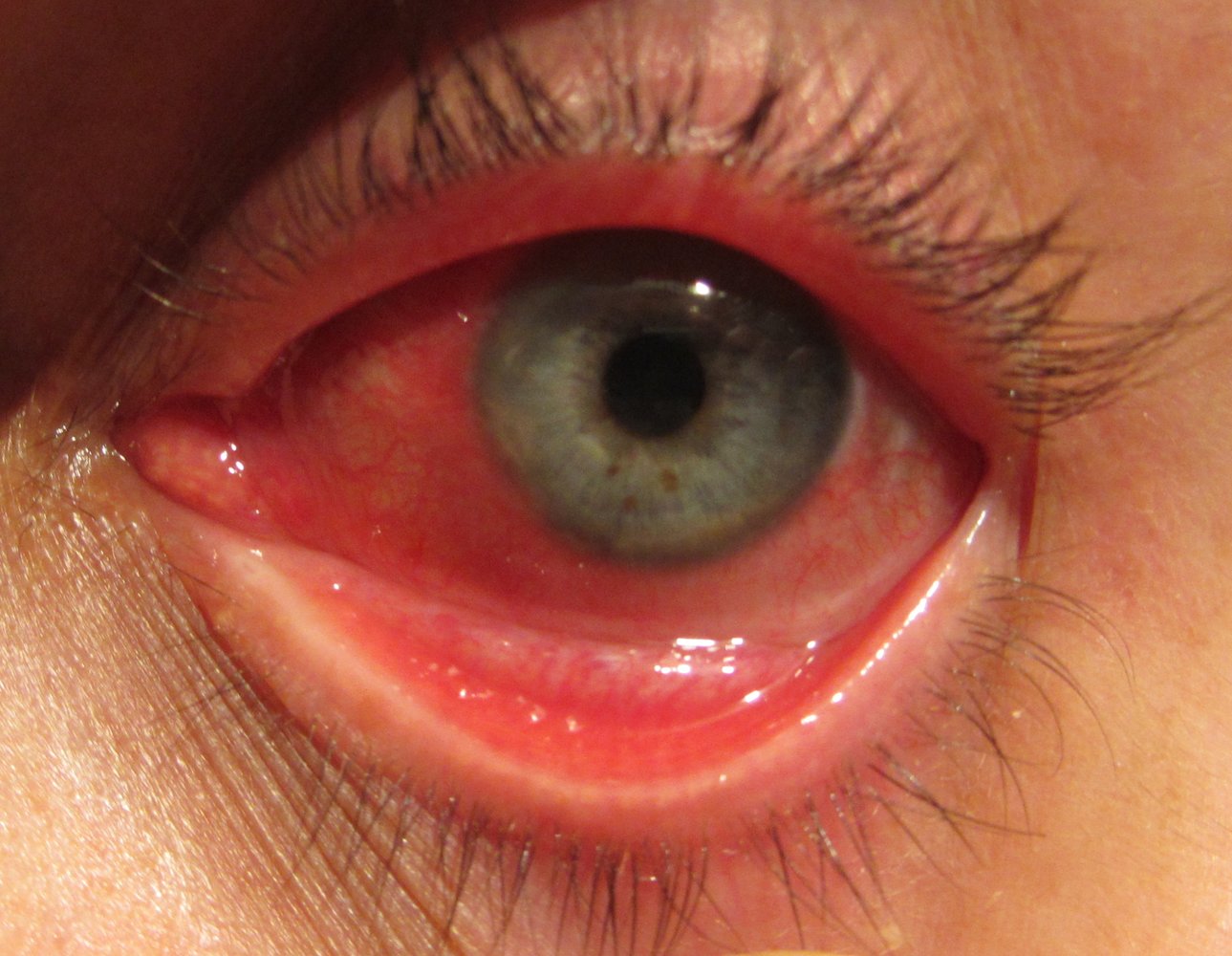
The bulbar conjunctiva and limbus are hyperemic as a result of mixed conjunctival and ciliary injection. There is posterior synechia (adhesion between the iris and the lens), in this case affecting 360° of the pupil.
These features are characteristic of anterior uveitis.
Source: "Anterior Uveitis Vemurafenib - Zelboraf", S. M. Cohen, Retina Gallery licensed under Public Domain
Common non-vision-threatening causes
| Common non-vision-threatening causes of eye pain [1] | |||
|---|---|---|---|
| Characteristic clinical features | Diagnostic findings | Management | |
| Corneal abrasion [23] |
|
|
|
| Preseptal cellulitis [26][27] |
|
|
|
| Dacryoadenitis and dacryocystitis |
|
|
|
| Blepharitis [28] |
|
|
|
| Hordeolum |
|
|
|
| Keratoconjunctivitis sicca [29] |
|
|
|
| Conjunctivitis [30][31] |
|
|
|








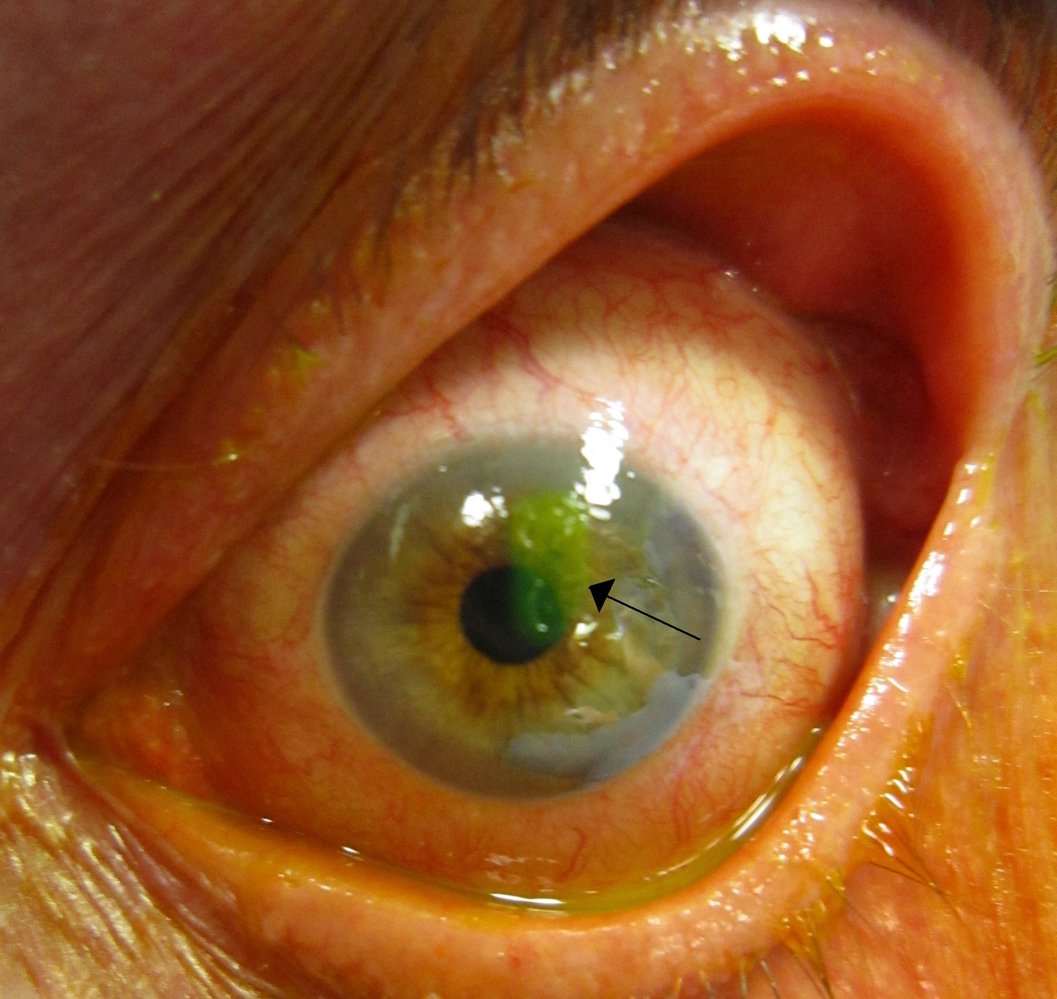
Slit-lamp photography of the left eye with fluorescein staining
A small area of green staining (black arrow) confirms a corneal abrasion. Significant conjunctival injection is also visible.
Source: “Human cornea with abrasion highlighted by fluorescein staining” by James Heilman, MD, Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}
Slit-lamp photography of the left eye with fluorescein staining and blue light
An irregularly shaped corneal abrasion, clearly highlighted by the yellow-green fluorescein stain, is visible. Faintly stained scratch marks (indicated by white overlay and line) can be seen around the abrasion (marked by dotted line).
The irregular shape of the defect and the scratch marks indicate an upper subtarsal foreign body as the underlying cause. Upper eyelid ectropionization is required to confirm the diagnosis and for immediate treatment.
This image is an adaptation. Source of original image: Retina Gallery. Original title: “49487_009”. Created by: Mayo Clinic Jacksonville, Florida. Licensed under Public Domain. Modifications to original image: removal of the date in the lower left corner.

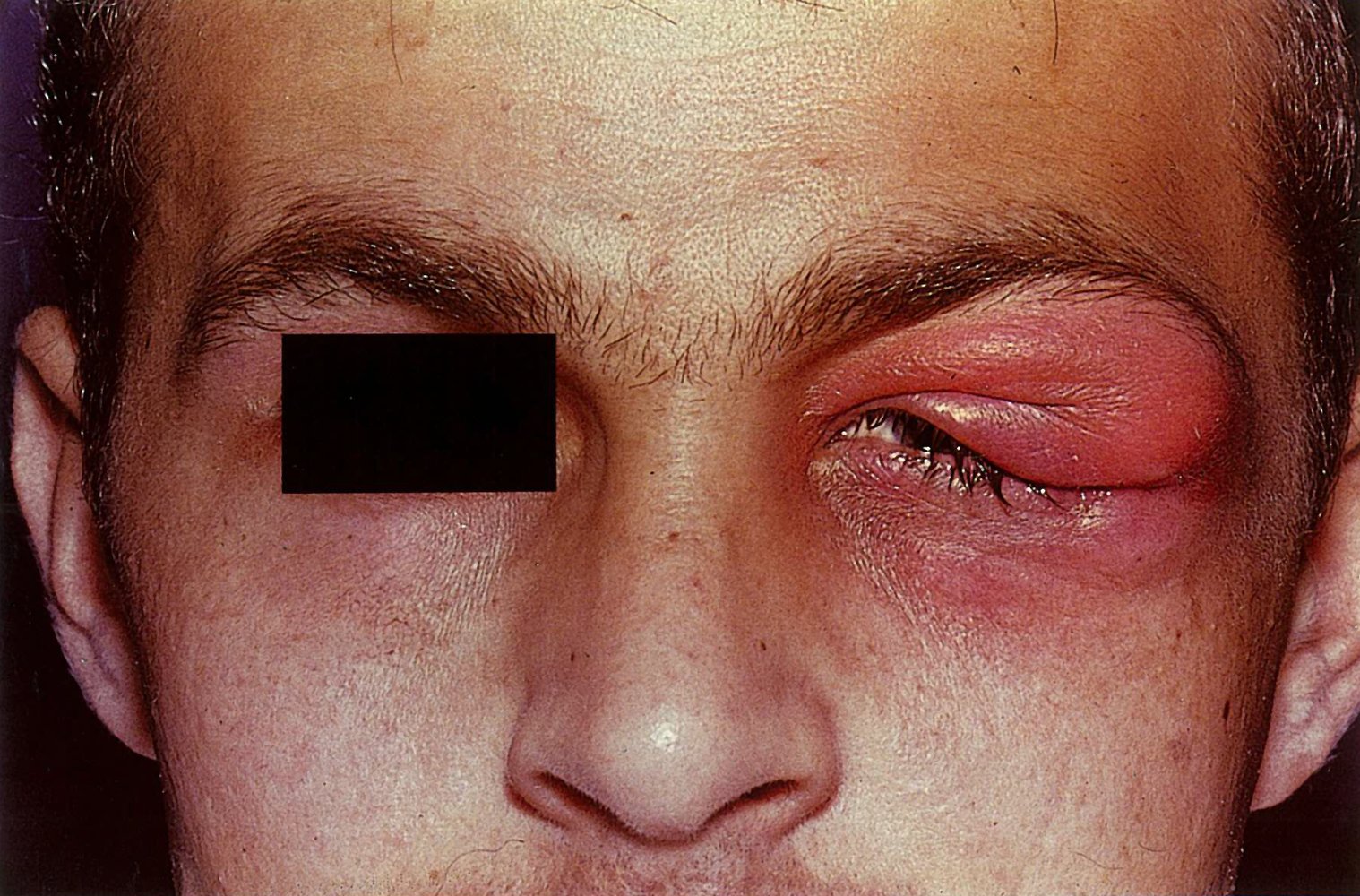
The left eyelid appears swollen and erythematous.
These clinical features are suggestive of preseptal cellulitis, an inflammation of tissue anterior to the orbital septum.
Source: “Preseptal Cellulitis” by Tripp, flickr, licensed under CC BY 2.0.
Swelling and hyperemia of the left lateral upper eyelid can be seen, resulting in the characteristic S-shaped ptosis (green line).
This is the typical appearance of acute dacryoadenitis.
Source: © IMPP
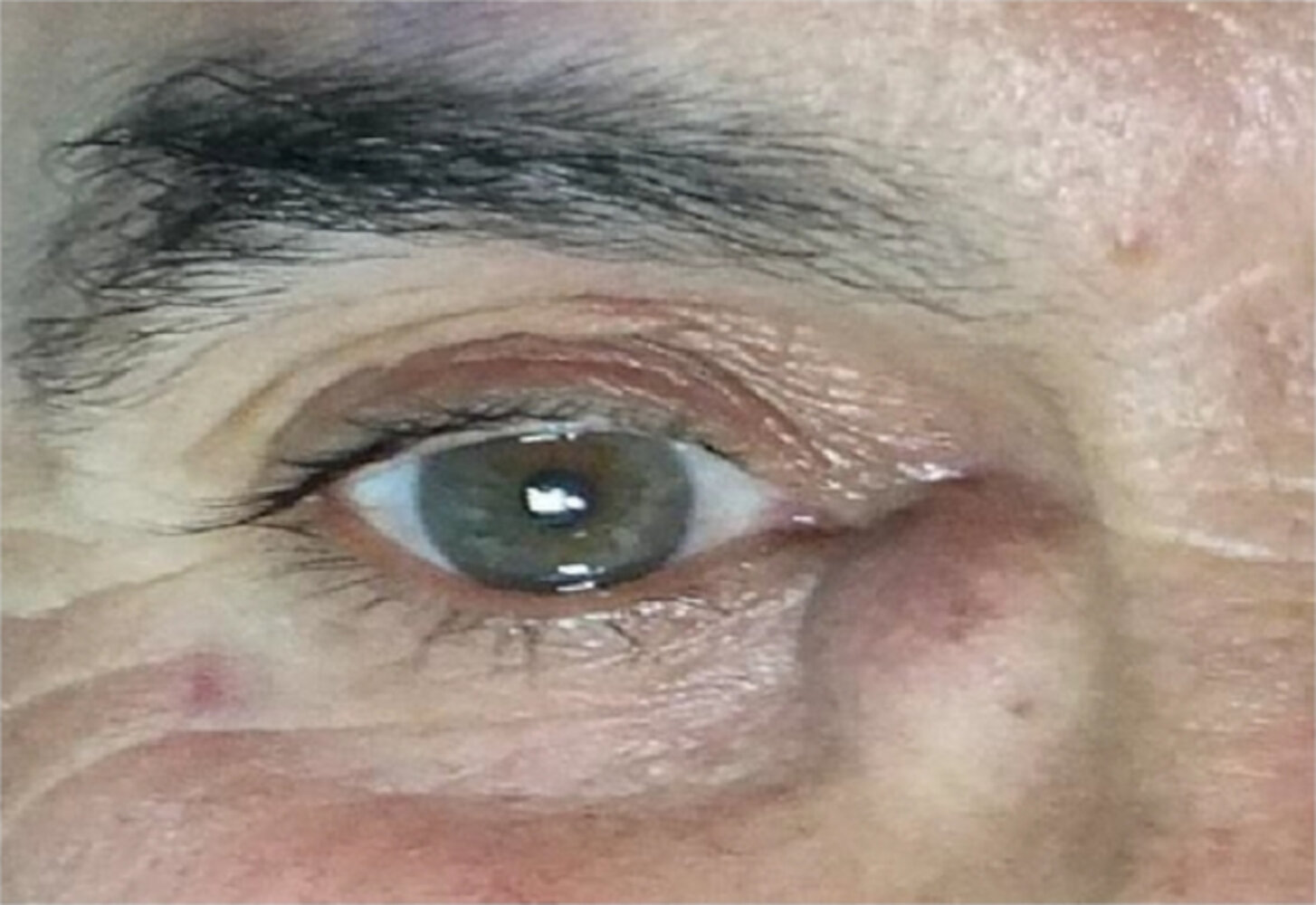
Right eye of a 54-year-old male patient
A solid and immobile mass can be seen in the right fossa lacrimalis. There is no discharge of pus or other secretions.
These findings are typical of dacryocystitis, which can result from chronic inflammation of the lacrimal sac and/or chronic stenosis of the tear duct.
Source: “Figure 1, in: Clinical, Radiological, Microbiological, and Histopathological Aspects of Acquired Dacryocystoceles” by Selam Yekta Sendul, Sonmez Cinar, Halil Hüseyin Çağatay, Mehmet Demir, Burcu Dirim, Dilek Guven, Hindawi, licensed under CC BY 3.0.
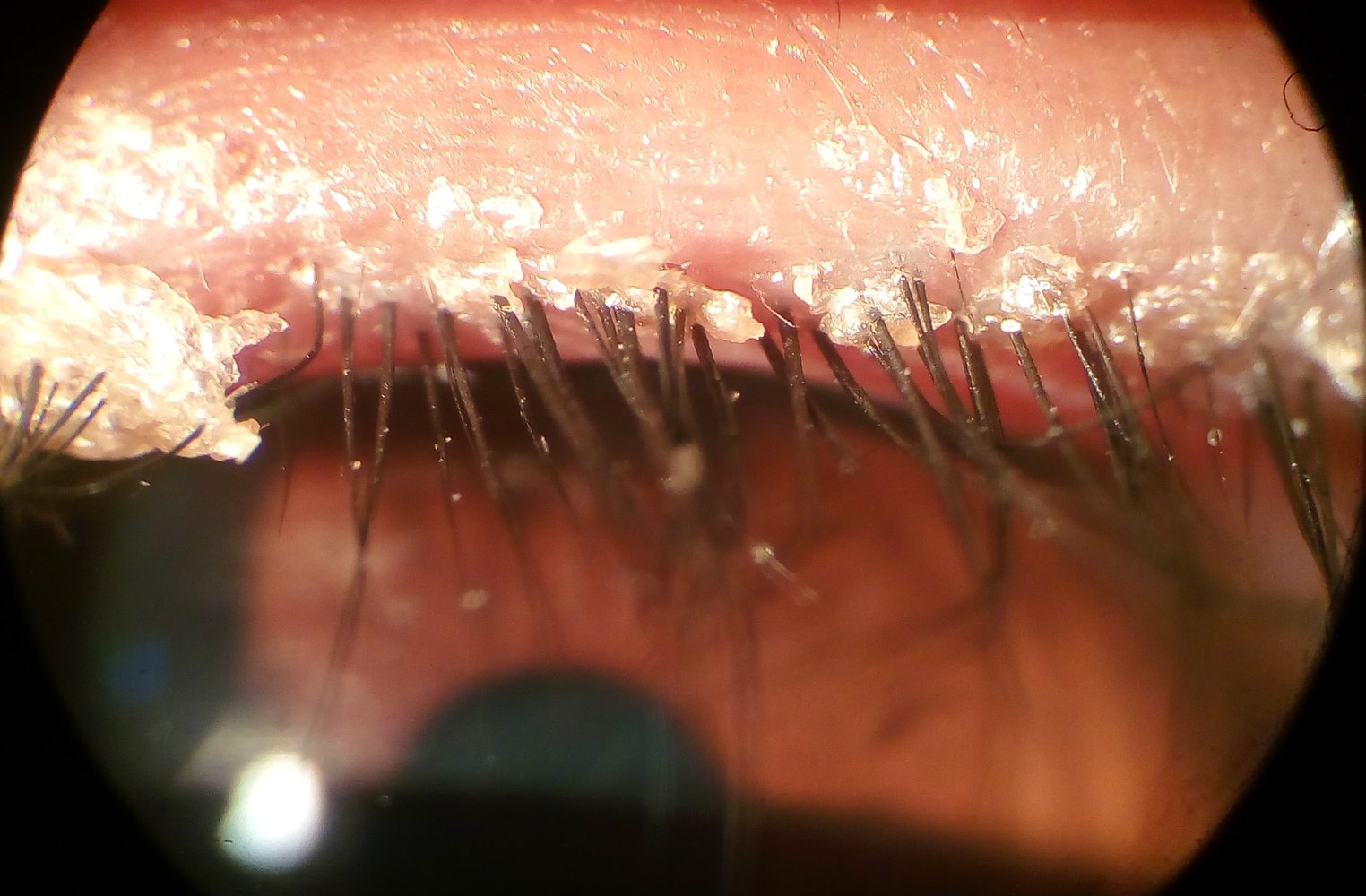
Slit-lamp photography
There is crusting at the base of the eyelashes and the lid margin appears injected.
This is the typical appearance of blepharitis.
Source: “Anterior Blepharitis” by Imrankabirhossain, Wikimedia Commons, licensed under CC BY-SA 4.0.
{kind=link}

Right eye (temporal view)
There is erythema and swelling of the upper eyelid. A yellow pus point is visible at the lid margin near the base of the eyelash follicle.
This is the typical appearance of an external hordeolum.
Source: "File:Stye02.jpg", Jacek Halicki, Wikimedia Commons licensed under Public Domain
{kind=link}
Left eye
Significant conjunctival injection is visible. There is increased tearing visible in the inferior fornix.
These findings are typical for conjunctivitis. The absence of purulent secretion suggests a viral infection, although conjunctival injection can also be caused by various other conditions.
Source: “Conjunctivitis” by Raimundo Pastor, Wikimedia Commons, licensed under CC BY 4.0.
.png){kind=link}
Acute management checklist
- Perform a focused clinical evaluation, including:
- Eye examination
- Slit-lamp examination
- Narrow the diagnosis based on the suspected location of the lesion and characteristic clinical features.
- Begin critical interventions immediately as indicated, e.g.:
- Management of traumatic eye injuries
- Treatment of acute angle-closure glaucoma
- Lateral canthotomy and cantholysis in orbital compartment syndrome
- Immediate large-volume irrigation of ocular chemical burns
- Corneal foreign body removal
- Consult ophthalmology urgently for the following:
- Red flags for painful red eye
- Vision-threatening causes of eye pain
- Obtain additional diagnostics as indicated and initiate condition-specific treatment.
Mimics
Headache and facial pain
- Trigeminal neuralgia (involving V1 of trigeminal nerve)
- Cluster headache
- Migraine
- Tension headache
- Frontal or ethmoid sinusitis
- Postherpetic neuralgia
-
Referred pain from:
- Otitis media
- TMJ dysfunction
- Dental infection
- Nasal masses
Painless causes of red eye [30]
The following conditions are typically painless but can cause eye discomfort when severe.
- Viral conjunctivitis
- Bacterial conjunctivitis
- Allergic conjunctivitis
- Conjunctivitis due to irritants (e.g., contact lenses, chlorinated water, dust)
- Drug-induced conjunctival hyperemia (e.g., cannabis, prostaglandin analogs) [32]
- Blepharitis
- Subconjunctival hemorrhage
- Episcleritis
- Conjunctival melanoma
- Irritation of pinguecula or pterygium
Painless causes of red eye are typically non-vision-threatening.







Painless eyelid or orbital swelling
- Chalazion
- Angioedema
- Lymphedema
- Graves ophthalmopathy
- Allergic contact dermatitis



Painless visual disturbances
-
Sudden
- Monocular
- Central retinal artery occlusion
- Central retinal vein occlusion
- Retinal detachment
- Vitreous hemorrhage
- Nonarteritic anterior ischemic optic neuropathy
- Macular hole
- Retinal migraine aura
- Scotoma
- Binocular
- Occipital stroke (cortical blindness)
- Posterior reversible encephalopathy syndrome
- Toxic or metabolic causes (e.g., methanol poisoning)
- Monocular
-
Gradual
- Cataracts
- Open-angle glaucoma
- Age-related macular degeneration
- Diabetic retinopathy
- Refractive errors (e.g., myopia, hyperopia, astigmatism)
- Retinitis pigmentosa
- Hereditary optic neuropathies (e.g., Leber hereditary optic neuropathy)
- Fuchs endothelial corneal dystrophy
Sudden painless visual loss (especially monocular) is a medical emergency that requires urgent evaluation and in many cases ophthalmology consultation.
Functional vision disorders can manifest suddenly or gradually with monocular or binocular symptoms.




")





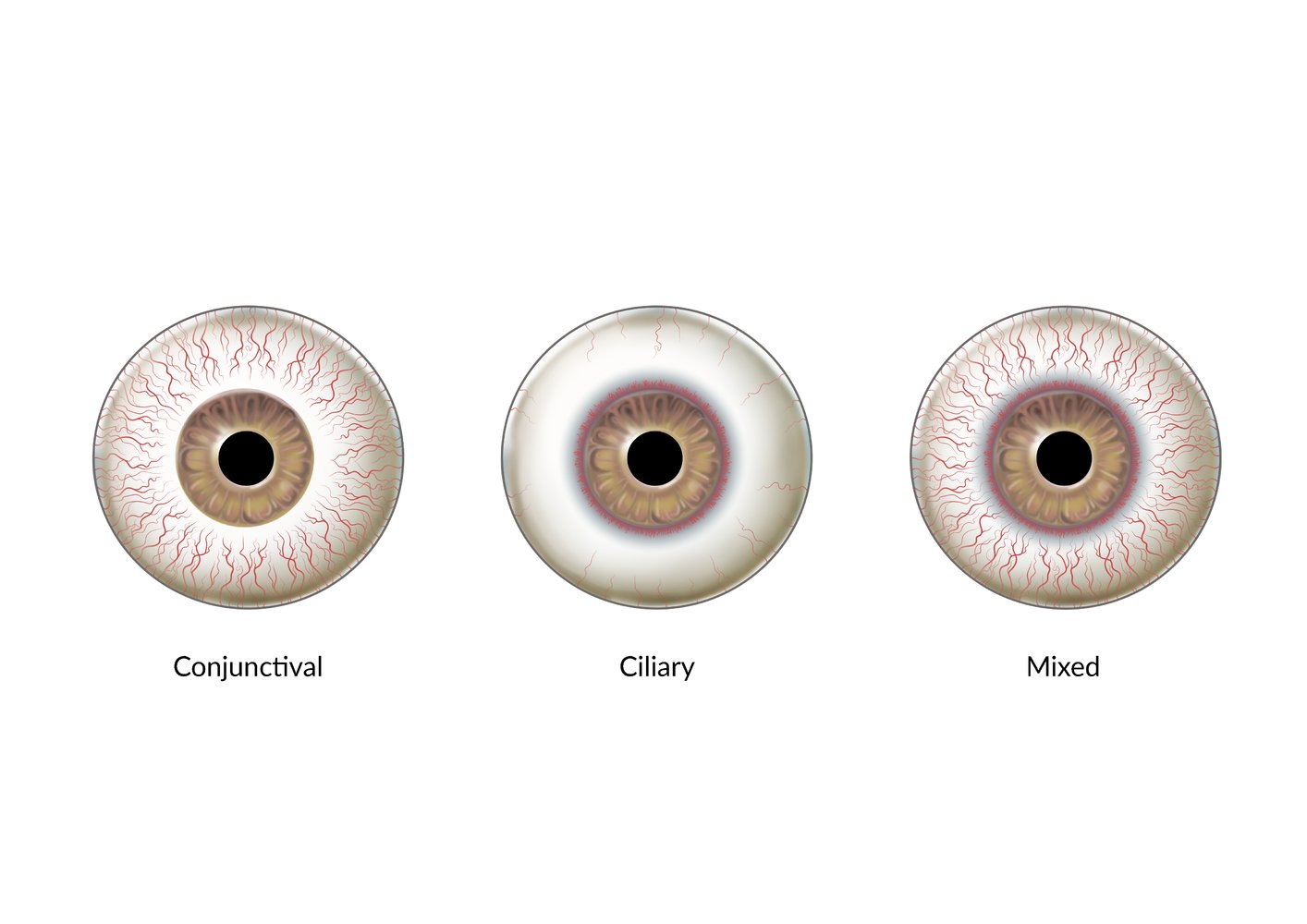
Three main patterns of ocular hyperemia help to identify the underlying cause.
– Conjunctival hyperemia: diffuse redness of the eye that is most marked in the periphery (i.e., near the conjunctival fornices), can reach far anteriorly, but spares the circumlimbal region. It is caused by dilation of the conjunctival vessels, which can be moved over the sclera with the conjunctiva. This pattern is typically seen in conjunctivitis.
– Ciliary flush: focal ocular redness in the circumlimbal region (i.e., a perilimbal halo). It is caused by dilation of the deep vessels, which cannot be moved over the sclera with the conjunctiva. This pattern is typically seen in anterior uveitis, keratitis, and acute angle-closure glaucoma, and it is sometimes more easily detected without the slit-lamp as a diffuse blue-red coloration of the circumlimbal region.
– Mixed: a combination of peripheral and perilimbal hyperemia. This pattern is frequently seen in various conditions.
© AMBOSS

Left eye
The conjunctival blood vessels are dilated (injection). There is no purulent discharge.
This finding is consistent with viral conjunctivitis.
Source: “An eye infected with viral conjunctivitis” by Joyhill09, Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}

Left eye
There is massive conjunctival injection (hyperemia) and purulent discharge, especially visible in the medial corner of the eye and the margin of the lower lid.
This is the characteristic appearance of bacterial conjunctivitis.
Source: “Swollen eye with conjunctivitis” by Tanalai, Wikimedia Commons, licensed under CC BY 3.0.
{kind=link}
Right eye of an older adult
Conjunctival injection, massive chemosis, and tearing are visible. The eyelids appear edematous.
This is the classical appearance of allergic conjunctivitis.
Source: “Allergic conjunctivitis” by James Heilman, MD, Wikimedia Commons, licensed under CC BY-SA 4.0.
{kind=link}

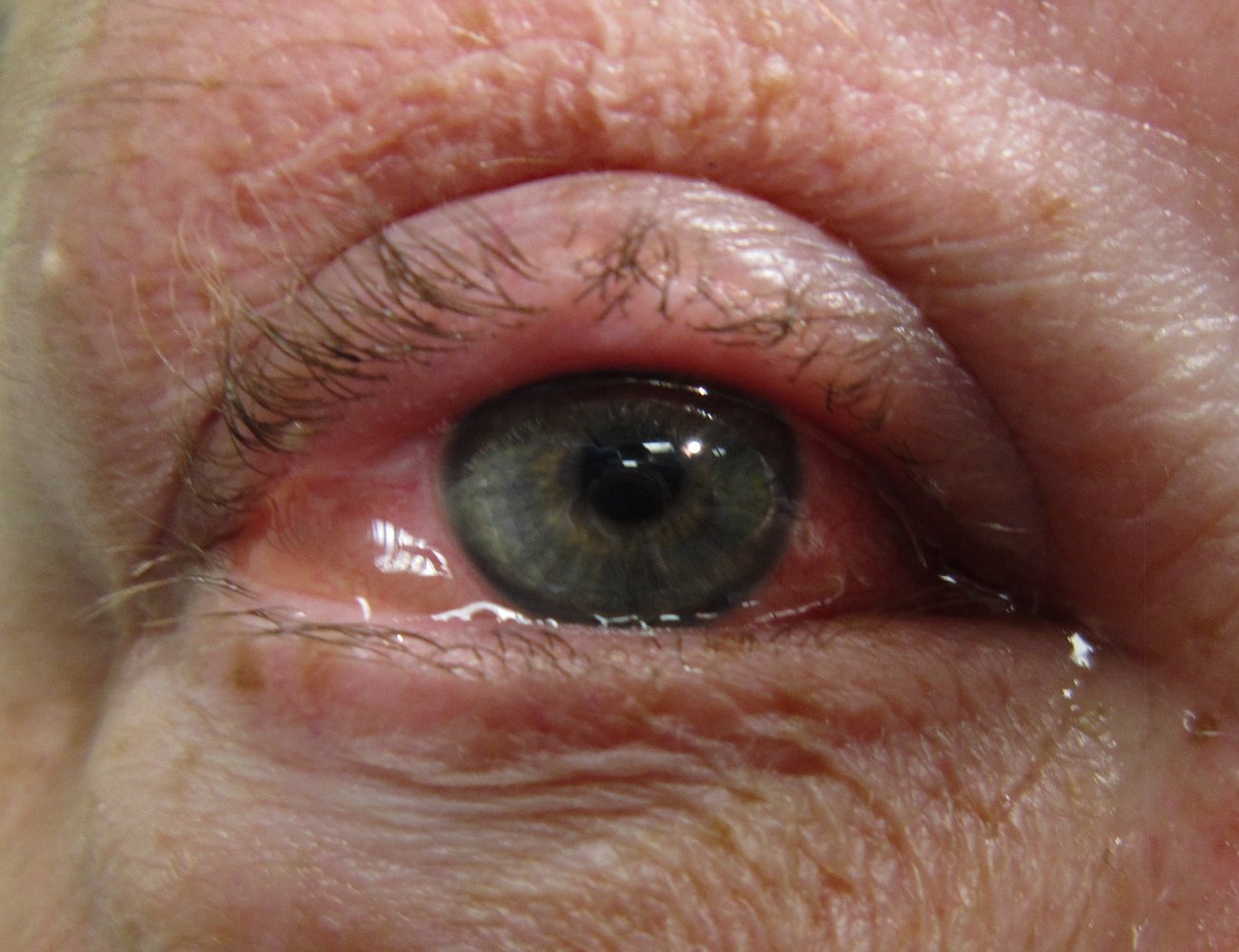
Photograph of the right eye
Swelling and redness of the right upper eye lid are apparent.
This finding is consistent with blepharitis, an inflammation of the eyelid. Other symptoms include dryness, itching, accompanying conjunctivitis, and scaling of the eyelid.
Source: "Blepharitis", clubtable, Wikimedia Commons licensed under Public Domain
{kind=link}
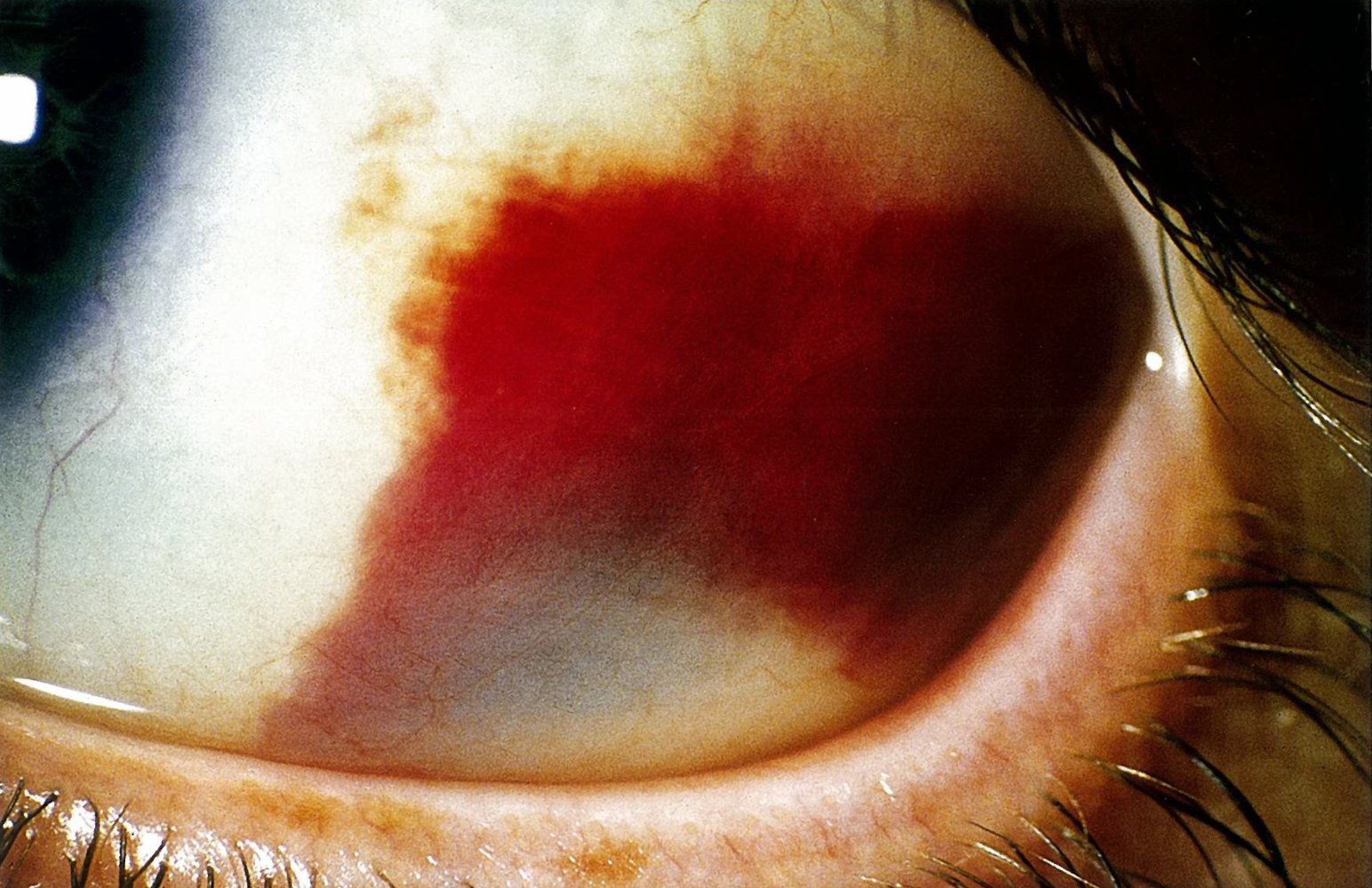
Slit-lamp photography of the left eye
The temporal conjunctiva shows a subconjunctival hemorrhage.
Source: © IMPP
Left eye
The temporal episclera shows vascular injection and a nodule shaped swelling.
This is the typical appearance of a nodular episcleritis.
Source: “Episcleritis.jpg” by Imrankabirhossain, Wikimedia commons, licensed under CC BY 4.0.
{kind=link}

Slit-lamp photography of the left eye
The temporal conjunctiva shows a darkly pigmented and irregurlarly demarcated lesion. Prominent afferent blood vessels and infiltrative growth in the cornea are further signs for a malignancy process.
Source: © IMPP

Left eye with ectropionized lower eyelid
A localized, nodular swelling is visible on the medial portion of the ectropionized lower eyelid. Both bulbar and tarsal conjunctiva are hyperemic.
This is the typical appearance of a chalazion.
Source: “Hordoleum” by Michal Klajban, Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}
Facial edema, primarily affecting the eyelids, is visible on the patient's face.
Source: © IMPP
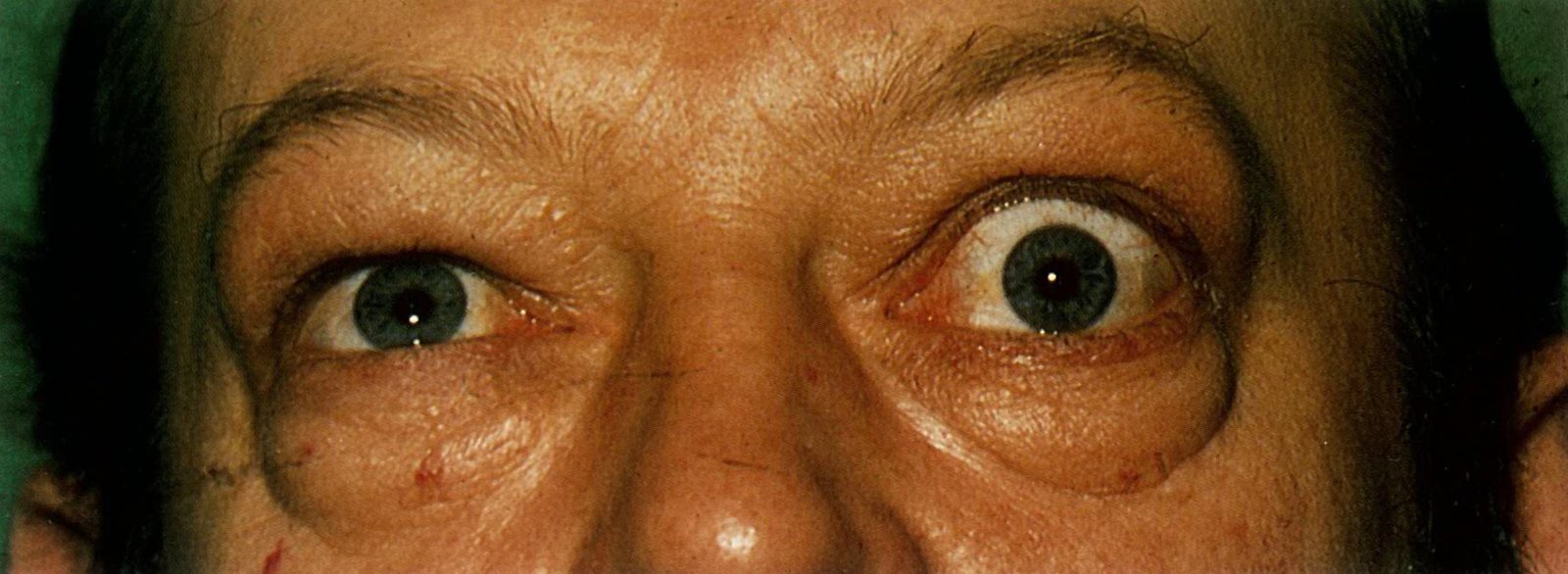
The left eye shows retraction of the upper eye lid, resulting in the visibility of the superior sclera (Dalrymple sign). The globe protrudes from the orbital cavity (exophthalmos). Conjunctival injection is evident and there is swelling of the eyelids. Comparison of light reflexes in the corneas shows the light reflex at the inferior margin of the pupil in the right eye and in the middle of the pupil in the left eye. The patient is trying to look upwards but the elevation of the left eye is impaired. Furthermore, reduced elevation of the left eye (ocular misalignment) becomes apparent as the patient tries to look upward, resulting in binocular diplopia, a further classic symptom of Graves ophthalmopathy.
Source: © IMPP
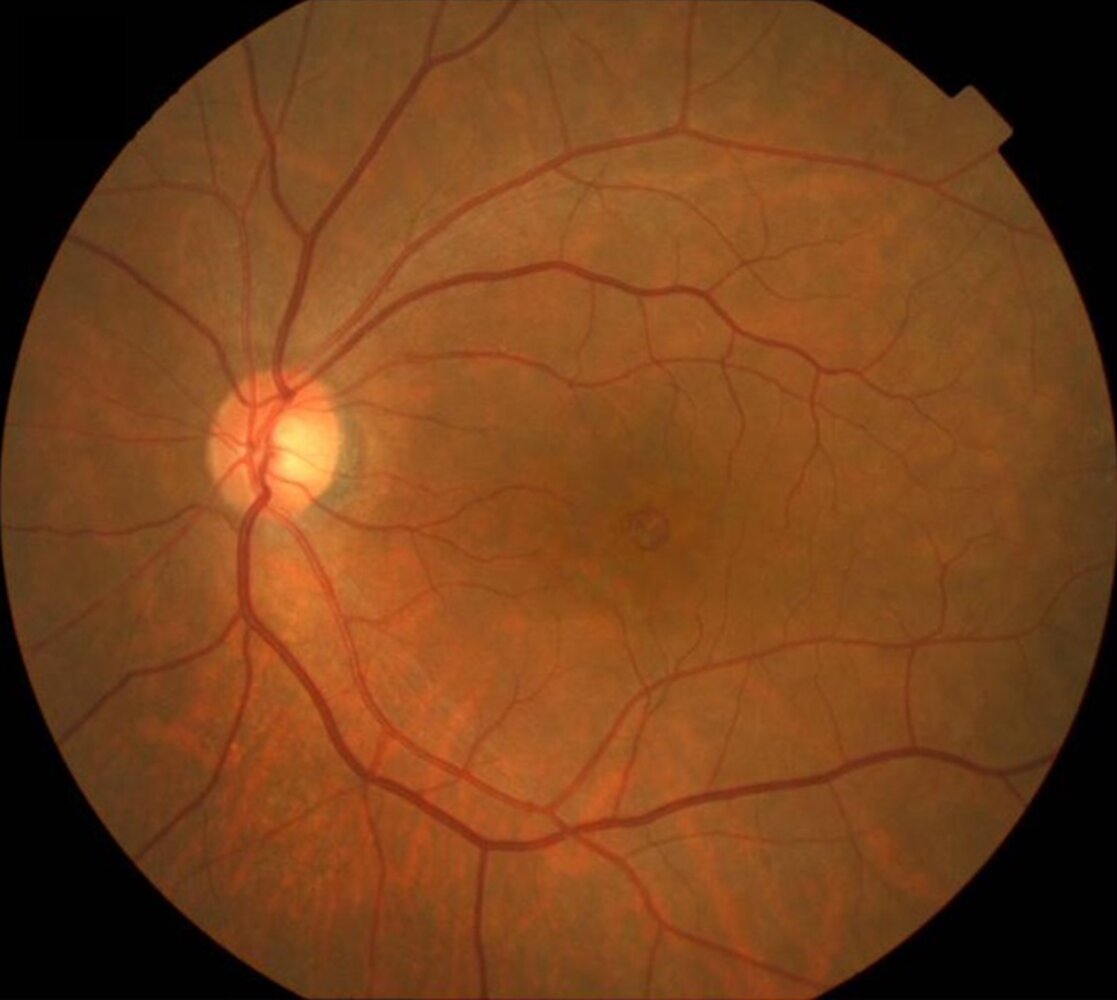
Fundus photography of a right eye
Narrow retinal arteries with box-carring of the retinal vessels (black dashed outline) and a pale retina indicating nerve fiber layer edema are visible. The fovea centralis appears red (cherry-red spot; purple overlay) due to the transparency of this part of the retina lacking nerve fibres, causing the well-vascularized choroid to shine through. Additionally, at the temporal superior arcade an embolus is present (arrow-head).
This is the classical finding of acute central retinal artery occlusion.
Purple circle: Optic disc
Source: © IMPP
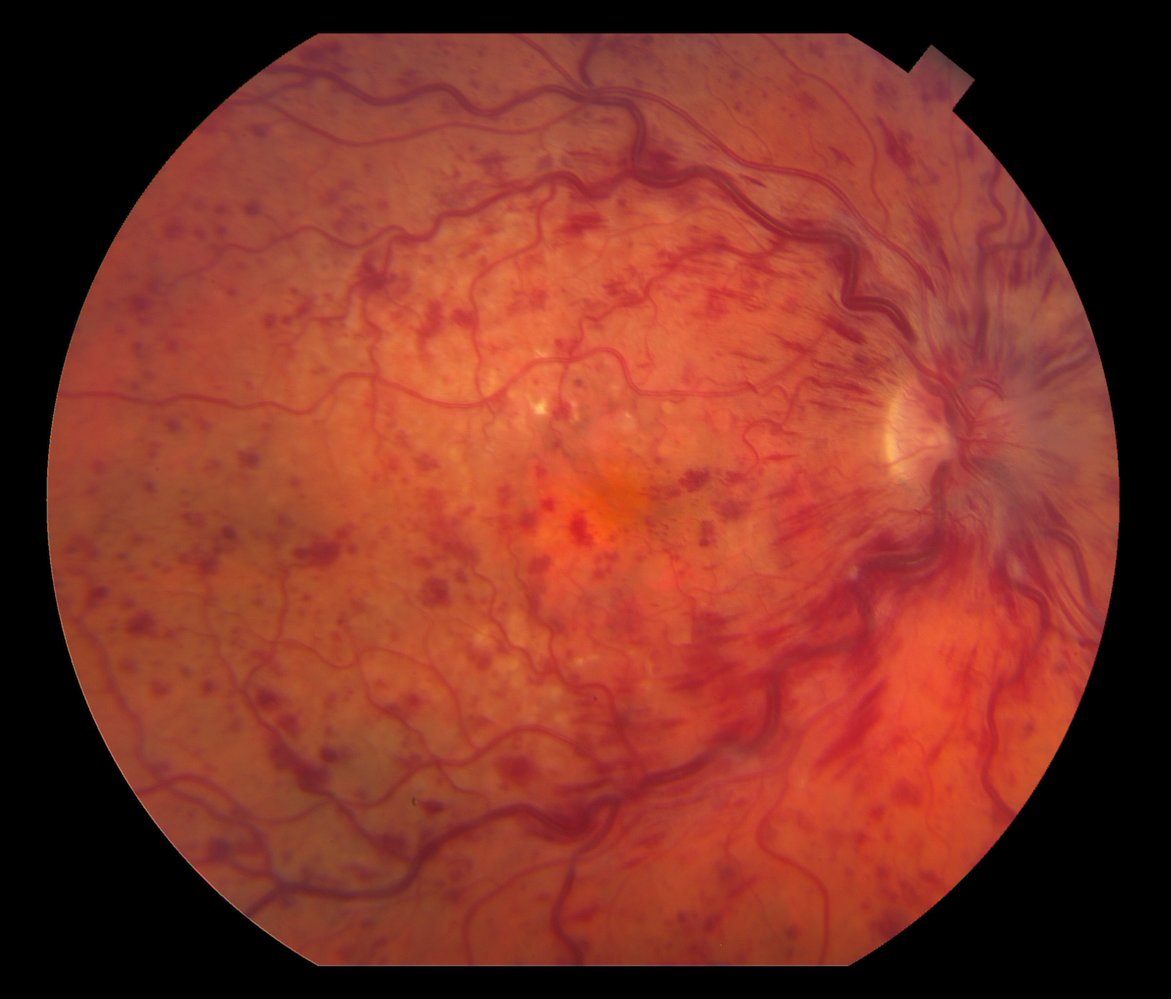
Fundus photography of a right eye
Multiple punctual hemorrhages in every quadrant of the retina and flame-shaped hemorrhages in the peripapillary and perivascular region are present (examples marked by blue overlay), as are markedly dilated tortuous veins (example framed by white lines) and mild disk edema (blurry margin of the disc marked by dashed blue line, sharply demarcated margin marked by blue line).
This is the classic appearance of central retinal vein occlusion.
M: Macula
Source: “Figure 1, in: Intravitreal Bevacizumab in the treatment of neovascular glaucoma secondary to central retinal vein occlusion: a case report” by Tarek Alasil, Michael E Rauser, Cases Journal, licensed under CC BY 2.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
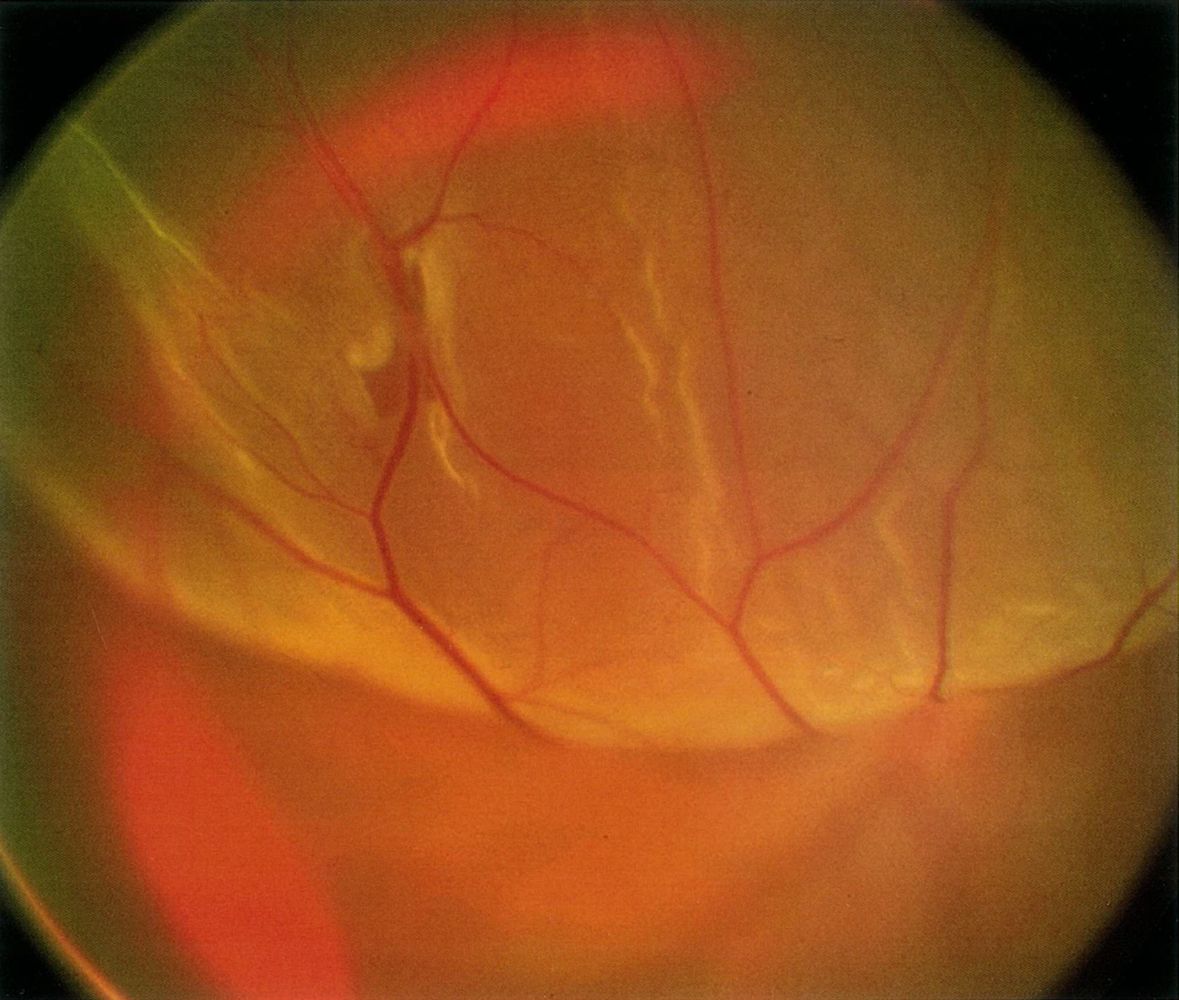
Fundus photography of the eye
The detached part of the retina is visible as a yellow-gray, bullous elevation (blue overlay) in the upper part of the image. The detachment is due to a retinal tear (dashed outline).
Source: © IMPP

Fundus photography of the left eye
Fundus details appear blurred. Dark red flowing patches of blood (green overlay) are visible at the temporal edge and in the central fundus, completely covering the aspect of the retina.
This is the typical appearance of a vitreous hemorrhage.
White circle: optic disc
Image source of original image: retinagallery.com. Original title: “Diabetic Vitreous Hemorrhage Left Eye”. Created by: Dr. Steve Cohen.
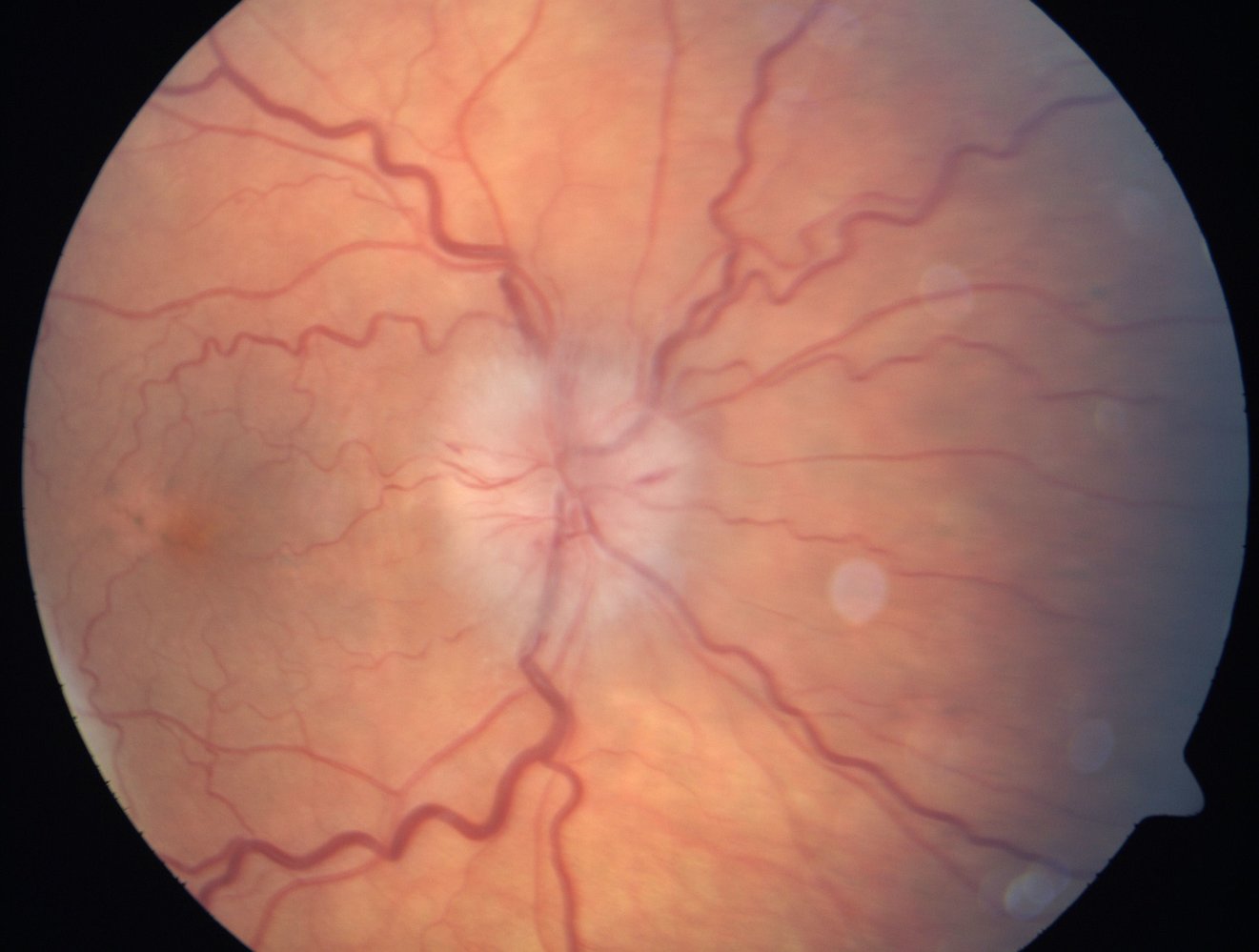
Fundus photography of a right eye
The optic disc (dashed circle) shows blurred margins and radial bleedings (arrowheads). The retinal veins are dilated and tortuous (examples indicated by white lines). In addition, the macula (M) shows pigment alterations (blue overlay).
This is the typical appearance of papilledema, in this case caused by NAION. Papilledema can also be caused by arteritic anterior ischemic optic neuropathy (AAION), inflammatory processes, or elevated intracranial pressure.
Hatched overlay: artifacts
Image source of original image: Retina Gallery. Original title: “Acute Non-arteritic Anterior Ischemic Optic Neuropathy Right Eye”. Created by: Dr. Steve Cohen.
Fundus photography of the left eye
A round defect is visible in the macula (blue overlay).
This is the typical appearance of a macular hole.
Circle: optic disc
Source: “Figure 1 B, in: Wider Retinal Artery Trajectories in Eyes with Macular Hole Than in Fellow Eyes of Patients with Unilateral Idiopathic Macular Hole” by Yoshihara N, Sakamoto T, Yamashita T, Yamashita T, Yamakiri K, Sonoda S, et al., PLoS ONE, licensed under CC BY 4.0. Modifications: image has been cropped and a letter was removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
Slit-lamp photograph of a left eye
The pupil is dilated. The lens (solid green overlay) appears cloudy and yellow.
This is the typical appearance of cataracts.
Dashed lines: optical path from the slit-lamp to the eye
Hatched green overlay: optical cross-section of the cornea, produced by the light of the slit-lamp
Source: © IMPP
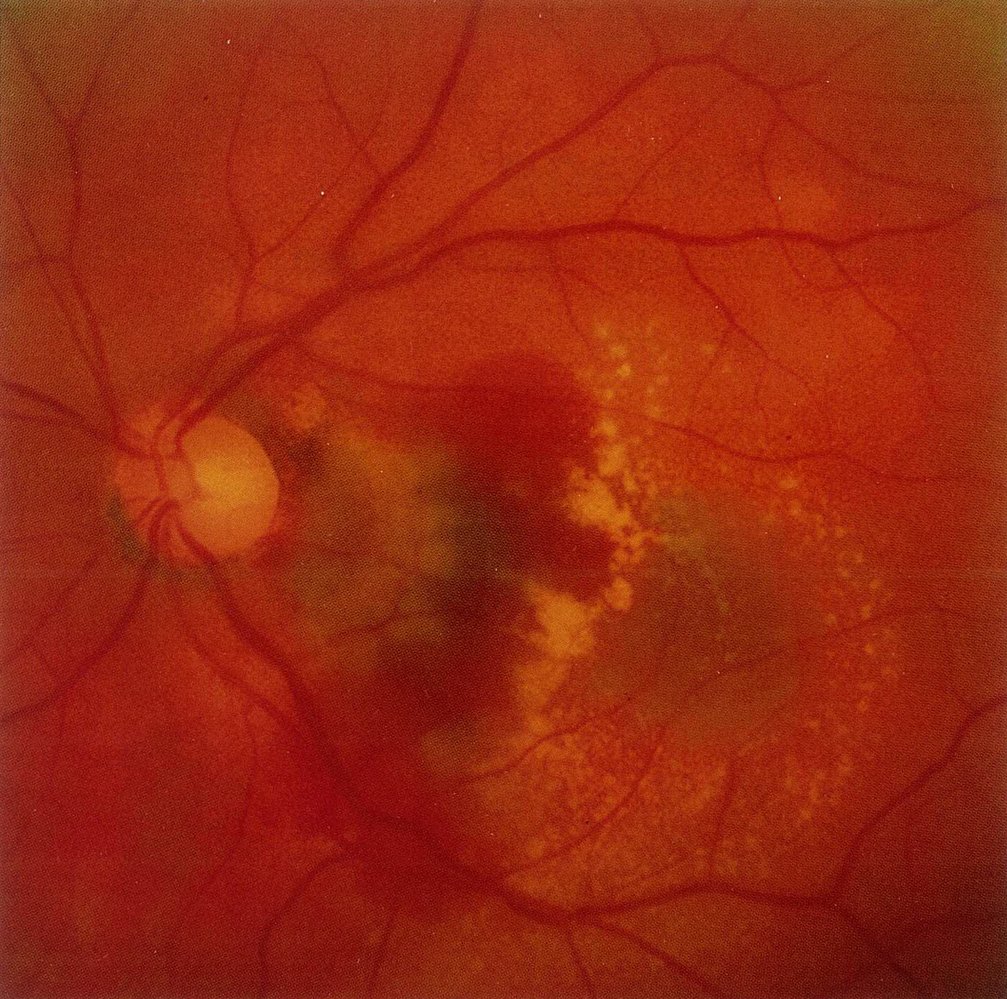
Fundus photography of the left eye
Subretinal and intraretinal hemorrhage (blue overlay) is visible in the region between the optic disc (blue circle) and macula (the macula is not visible, its approximate position is marked with an “M”). The light-yellow spots in the region of the macula indicate exudates and drusen (hatched overlay).
Subretinal and intraretinal hemorrhages can result from pathological neovascularization of the choroid (CNV). The presence of CNV is required for the diagnosis of exudative/wet/neovascular macular degeneration.
Source: © IMPP
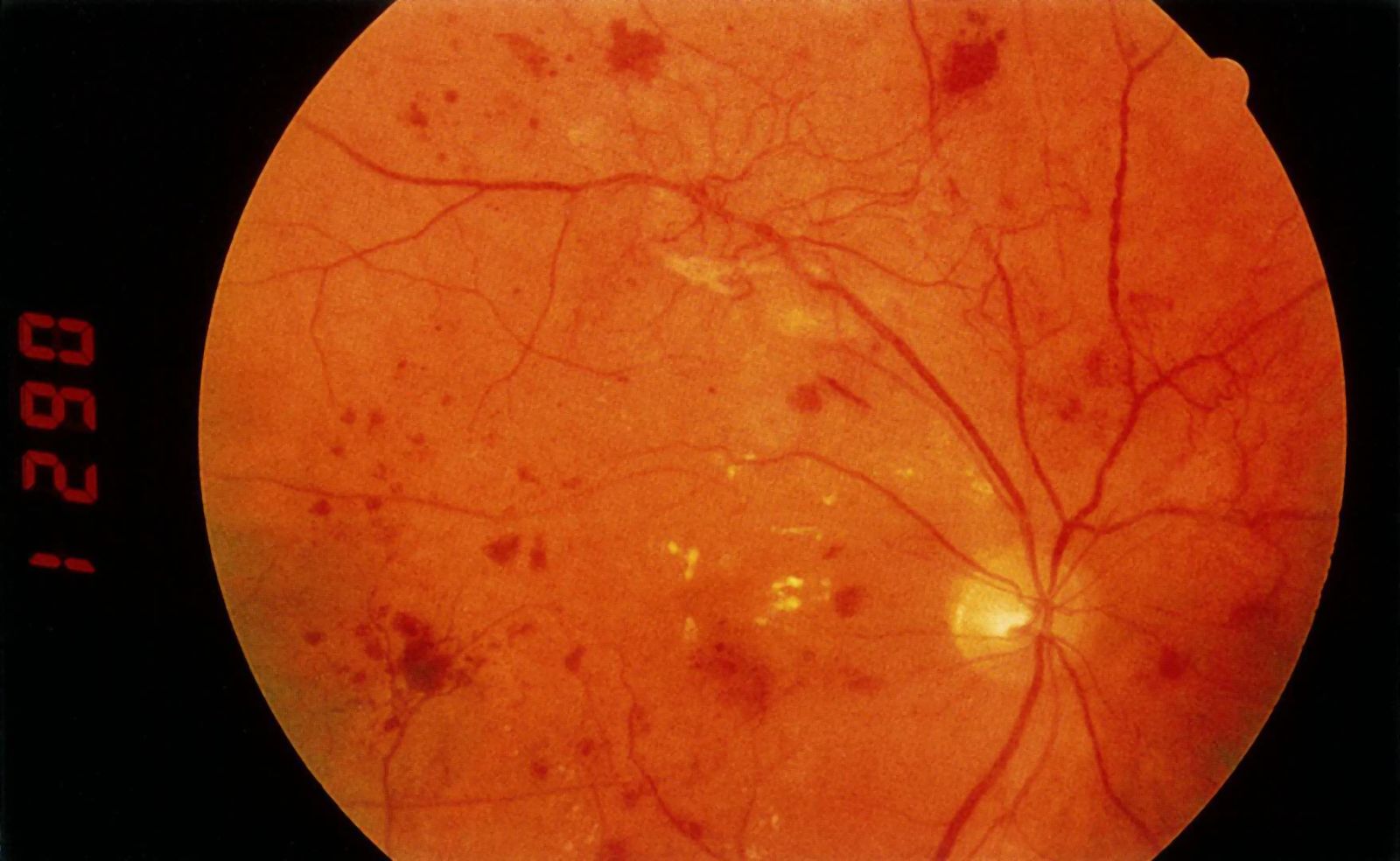
Fundus photography of a right eye
Neovascularization (example indicated by arrowhead) is evident at the temporal superior arcade as tortuous vessels originate from the normal retinal vasculature. Microaneurysms and retinal hemorrhages appear as small red dots and larger red blotches (examples indicated by blue overlay). Hard exudates appear as yellow lesions (examples indicated by green overlay). The retinal veins show periodic dilatations (venous beading; example indicated by yellow overlay).
The diagnosis of proliferative disease requires the presence of neovascularization.
Source: © IMPP
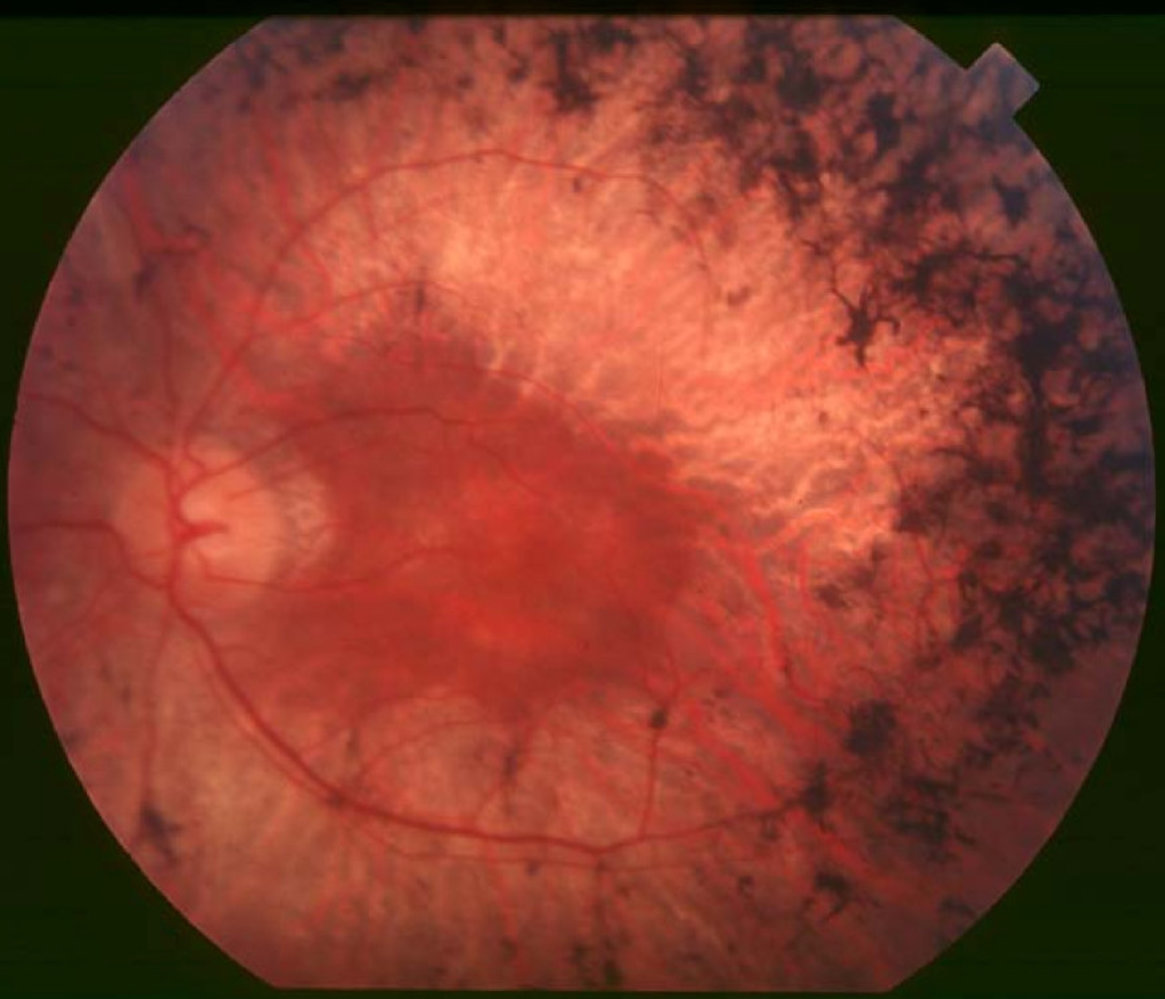
Fundus photography of a left eye
The retina shows pigmentary deposits (blue overlay) resembling bone spicules in the mid periphery of the fundus along with retinal atrophy (yellow overlay), enhancing the visibility of the choroid vessels (examples indicated by arrowheads). The macula (M) shows a circular depigmentation (green overlay). The retinal blood vessels are attenuated.
This is the typical fundoscopic appearance of retinitis pigmentosa.
Circle: optic disc
Source: “Figure 1. in: Retinitis pigmentosa” by Christian Hamel, Orphanet Journal of Rare Diseases, licensed under CC BY-SA 2.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 2.0.
References
- Walls R, Hockberger R, Gausche-Hill M, Erickson TB, Wilcox SR. "Rosen's Emergency Medicine 10th edition- Concepts and Clinical Practice E-Book". Elsevier Health Sciences. (2022). ISBN: 9780323757904
- Rho JY, Dryden SC, Jerkins BM, Fowler BT. "Management of Eye Trauma for the Primary Care Physician". J Am Board Fam Med. 34(5). :1018-1029. (2021)
- Bord SP, Linden J. "Trauma to the Globe and Orbit". Emerg Med Clin North Am. 26(1). :97-123. (2008)
- Heath Jeffery RC, Dobes J, Chen FK. "Eye injuries: Understanding ocular trauma". Aust J Gen Pract. 51(7). :476-482. (2022)
- Murali S, Davis C, McCrea MJ, Plewa MC. "Orbital compartment syndrome: Pearls and pitfalls for the emergency physician.". J Am Coll Emerg Physicians Open. 2(2). :e12372. (2021)
- McCallum E, Keren S, Lapira M, Norris JH. "Orbital Compartment Syndrome: An Update With Review Of The Literature.". Clin Ophthalmol. 13. :2189-2194. (2019)
- Sundar G, Hegde R. "Orbital cellulitis- A review". J Ophthalmic Sci Research. 55(3). :211. (2017)
- Pelletier J, Koyfman A, Long B. "High risk and low prevalence diseases: Orbital cellulitis". Am J Emerg Med. 68. :1-9. (2023)
- Wang X, Zhang P, Suo J, Li Q, Zhang Y. "The diagnosis and treatment progress of infectious endophthalmitis". Eye. 39(3). :492-504. (2024)
- Kernt M, Kampik A. "Endophthalmitis: Pathogenesis, clinical presentation, management, and perspectives". Clin Ophthalmol. 4. :121-135. (2010)
- Prum BE, Herndon LW, Moroi SE, et al. "Primary Angle Closure Preferred Practice Pattern® Guidelines". Ophthalmology. 123(1). :P1-P40. (2016)
- Sihota, Tandon R. "Parsons' Diseases of the Eye". Elsevier India. (2019). ISBN: 9788131254165
- Bennett JL. "Optic Neuritis". Continuum (Minneap Minn). 25(5). :1236-1264. (2019)
- Bennett JL, Costello F, Chen JJ, et al. "Optic neuritis and autoimmune optic neuropathies: advances in diagnosis and treatment". Lancet Neurol. 22(1). :89-100. (2023)
- van der Geest KSM, Sandovici M, Brouwer E, Mackie SL. "Diagnostic Accuracy of Symptoms, Physical Signs, and Laboratory Tests for Giant Cell Arteritis". JAMA Intern Med. 180(10). :1295. (2020)
- Ponte C, Grayson PC, Robson JC, et al. "2022 American College of Rheumatology/EULAR Classification Criteria for Giant Cell Arteritis.". Arthritis Rheumatol. 74(12). :1881-1889. (2022)
- Liesegang T. "Herpes Zoster OphthalmicusNatural History, Risk Factors, Clinical Presentation, and Morbidity". Ophthalmology. 115(2). :S3-S12. (2008)
- Rhee MK, Ahmad S, Amescua G, et al. "Bacterial Keratitis Preferred Practice Pattern®". Ophthalmology. 131(4). :P87-P133. (2024)
- Azher T, Yin XT, Tajfirouz D, Huang A, Stuart P. "Herpes simplex keratitis: challenges in diagnosis and clinical management". Clin Ophthalmol. Volume 11. :185-191. (2017)
- Gilani CJ, Yang A, Yonkers M, Boysen-Osborn M. "Differentiating Urgent and Emergent Causes of Acute Red Eye for the Emergency Physician". Western Journal of Emergency Medicine. 18(3). :509-517. (2017)
- Wipperman JL, Dorsch JN. "Evaluation and management of corneal abrasions". Am Fam Physician. 87(2). :114-20. (2013)
- John Salmon. "Kanski's Clinical ophthalmology E-Book A systemic approach". Elsevier health sciences. (2019). ISBN: 9780702077135
- Harman LE, Margo CE, Roetzheim RG. "Uveitis: the collaborative diagnostic evaluation". Am Fam Physician. 90(10). :711-6. (2014)
- Pflipsen M, Massaquoi M, Wolf S. "Evaluation of the Painful Eye". Am Fam Physician. 93(12). :991-8. (2016)
- C. Ramanayake RPJ, K. Basnayake BMT. "Evaluation of red flags minimizes missing serious diseases in primary care". J Family Med Prim Care. 7(2). :315. (2018)
- Hauser A, Fogarasi S. "Periorbital and Orbital Cellulitis". Pediatric Rev. 31(6). :242-249. (2010)
- Gordon AA, Phelps PO. "Management of preseptal and orbital cellulitis for the primary care physician". Dis Mon. 66(10). :101044. (2020)
- Lin A, Ahmad S, Amescua G, et al. "Blepharitis Preferred Practice Pattern®". Ophthalmology. 131(4). :P50-P86. (2024)
- Akpek EK, et al. "Dry Eye Syndrome Preferred Practice Pattern®". Ophthalmology. 126(1). :P286-P334. (2019)
- Varu DM, Rhee MK, Akpek EK, et al. "Conjunctivitis Preferred Practice Pattern®". Ophthalmology. 126(1). :P94-P169. (2019)
- Azari AA, Barney NP. "Conjunctivitis". JAMA. 310(16). :1721. (2013)
- Singh RB, Liu L, Anchouche S, et al. "Ocular redness – I: Etiology, pathogenesis, and assessment of conjunctival hyperemia". Ocul Surf. 21. :134-144. (2021)