Summary
A femoral hernia is an uncommon type of inguinal hernia, in which intra-abdominal contents (e.g., intraperitoneal fat, mesentery, bowels) herniate into the femoral canal through the femoral ring. Risk factors for femoral hernias include old age, female sex, obesity, and previous hernia repair. Patients present with a globular swelling inferior to the inguinal ligament and medial to the femoral vein that worsens with coughing or straining. The diagnosis is primarily clinical with ultrasonography being indicated if the diagnosis is inconclusive. Although femoral hernias are uncommon, they are associated with a high risk of incarceration and strangulation and should, therefore, be surgically treated as early as possible. The preferred treatment for non-complicated femoral hernias is mesh hernioplasty, while repair without a mesh is used for complicated femoral hernias.
Epidemiology
- Uncommon hernia (∼ 5% of all hernias)
- Sex: ♀ > ♂ (3:1)
- Peak incidence: 40–70 years [1]
Epidemiological data refers to the US, unless otherwise specified.
Etiology
- Advancing age and female sex (see “Epidemiology” above)
-
Increased intra-abdominal pressure
- Obesity
- Chronic constipation
- Chronic cough (e.g., due to COPD)
- Straining during micturition (e.g., due to prostatic hypertrophy)
- Multiparity
- Previous abdominal surgeries (especially those involving the inguinal region)
In contrast to indirect inguinal hernias, which may occur congenitally, femoral hernias are almost always acquired.
References:[2]
Pathophysiology
-
Boundaries of the femoral canal
- Anterior: inguinal ligament (Poupart's ligament)
- Posterior: pubic ramus and pectineal ligament
- Medial: lacunar ligament (Gimbernat ligament)
- Lateral: femoral vein
- Typical femoral hernia (common): protrusion of intraperitoneal contents along with the transverse abdominal fascia through the femoral ring into the femoral canal
To remember the femoral triangle contents, think LaMe NAVEL: (from lateral to medial) femoral Nerve, Artery, Vein, Empty space (femoral canal → femoral hernia), Lymphatics
References:[1][3]
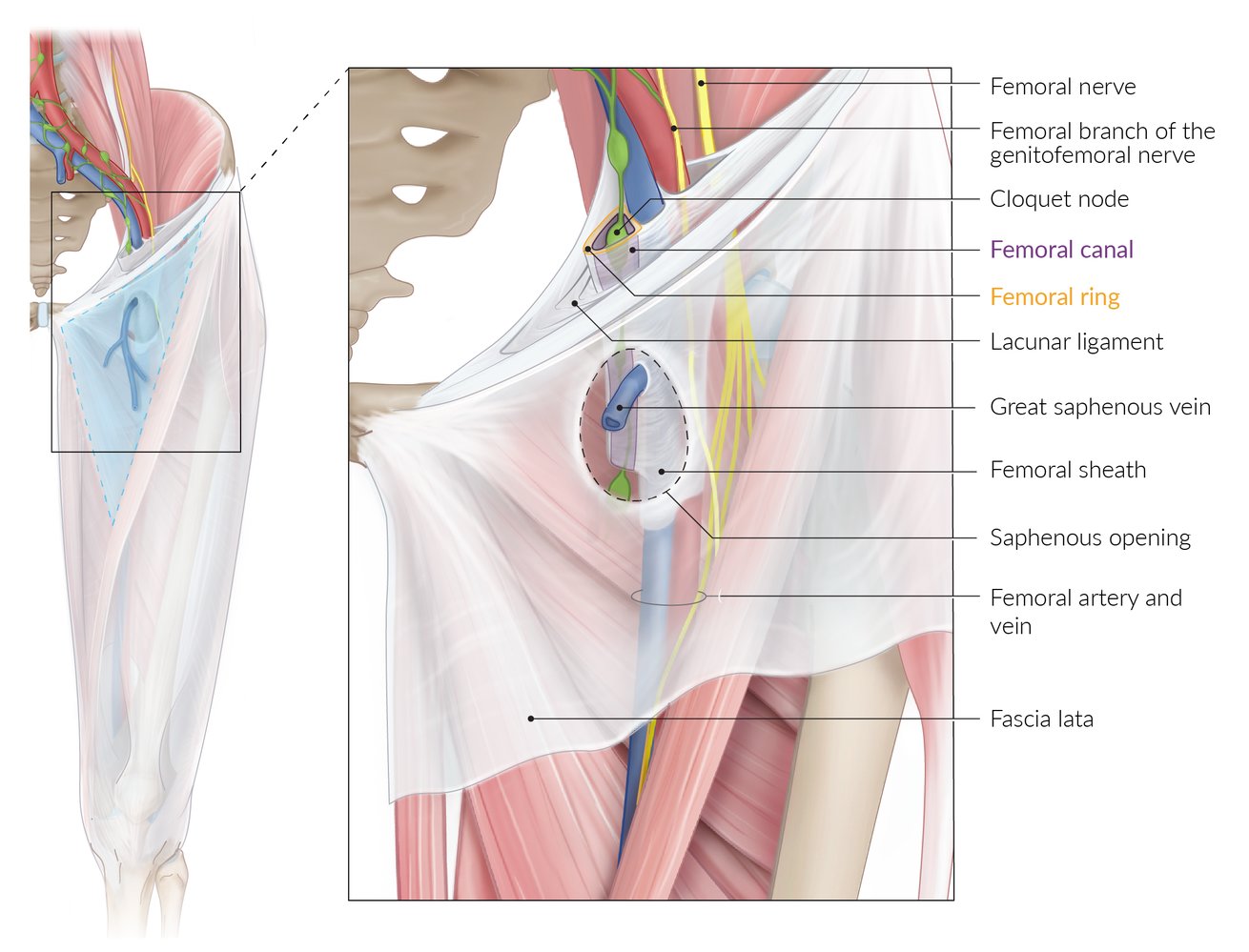
Topographic anatomy of the femoral canal region and surrounding regions. The femoral ring (yellow outline) forms the base of the femoral canal and is bounded by the inguinal ligament (anteriorly), lacunar ligament (medially), pectineal ligament (posteriorly), and fibrous septum of the femoral vein (laterally). The canal is wider in women. The cribriform fascia is not depicted in order to better visualize the saphenous opening.
© AMBOSS
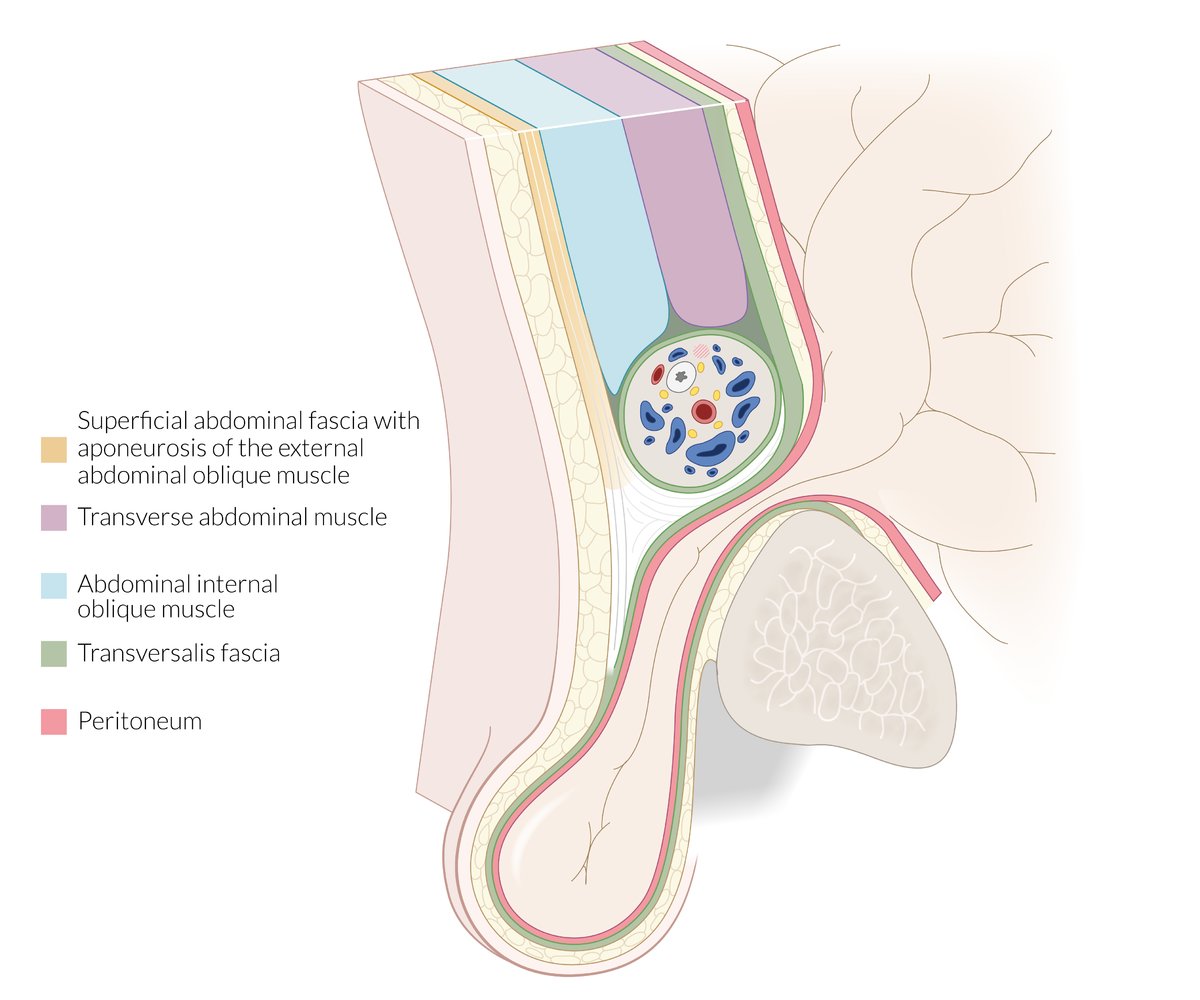
Sagittal view of the male inguinal region at the level of the superior pubic ramus, medial to the epigastric vessels
There is a protruding hernial sac (comprised of the transversalis fascia and parietal peritoneum) below the inguinal ligament but above the pubic bone, which, in the example shown, contains intestine.
© AMBOSS
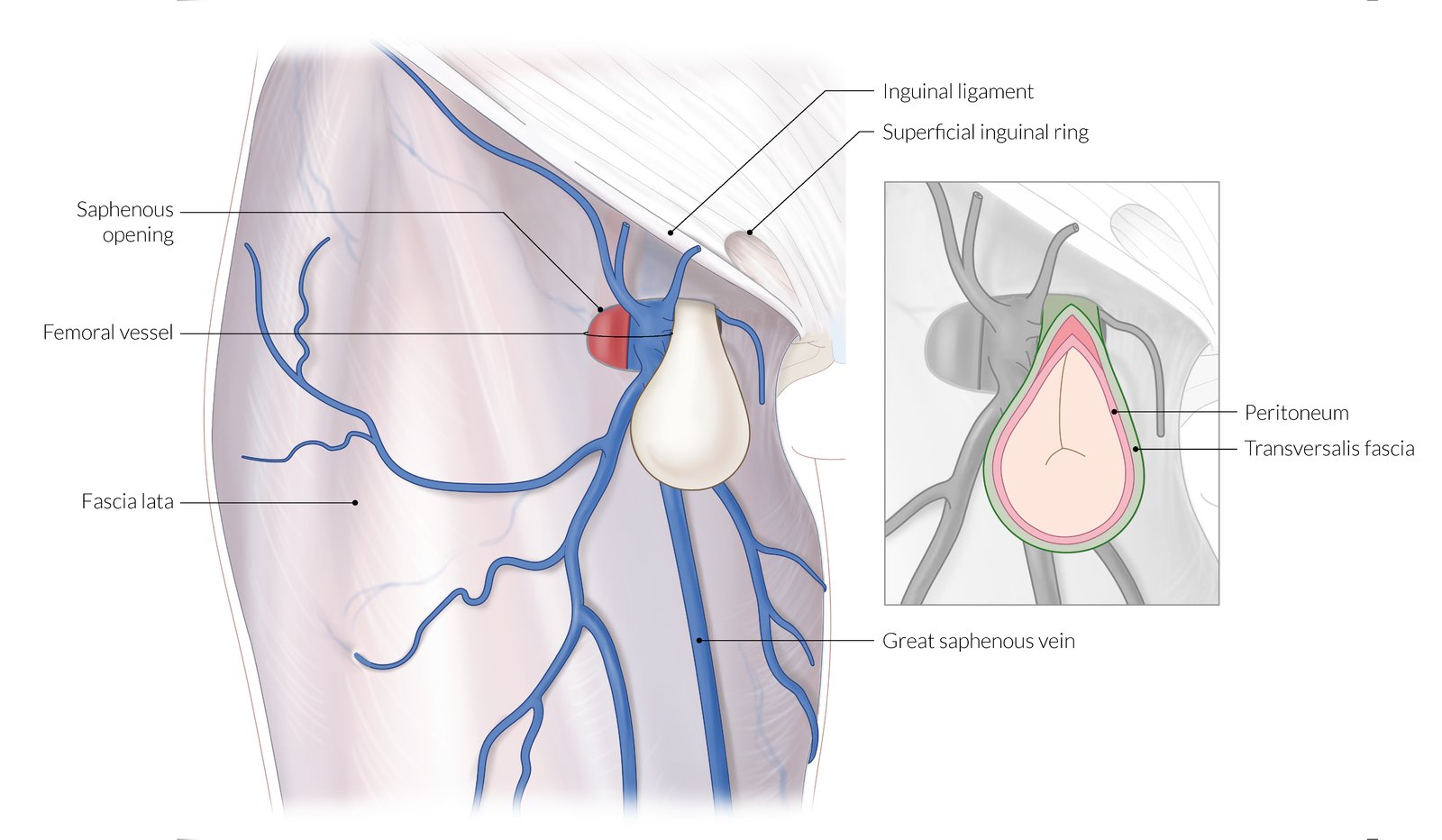
Femoral hernia passes through the vascular lacuna (internal hernial orifice), below the inguinal ligament and usually medial to the femoral vein and runs through the femoral canal until it reaches the saphenous opening (external hernial orifice; approx. 2cm caudal).
The saphenous opening typically contains loose connective and fatty tissue as well as inguinal lymph nodes.
Due to the increased width of the female pelvis, and therefore larger vascular lacuna, femoral hernia occurs predominantly in women.
© AMBOSS
Clinical features
-
Non-complicated femoral hernia
- A globular, subcutaneous swelling in the groin
- Localization: inferior to the inguinal ligament, lateral to the pubic tubercle, and medial to the femoral vein
- Swelling enlarges with coughing (palpable cough impulse) or a Valsalva maneuver
- Possibly, non-specific, dragging pain
- A globular, subcutaneous swelling in the groin
- Complicated femoral hernia: see “Complications” below
References:[1][4]
Diagnosis
- A femoral hernia is primarily a clinical diagnosis.
- Groin ultrasound is used when the diagnosis is inconclusive (see “Differential diagnosis” below).
Femoral hernias can be difficult to palpate in obese patients. Ultrasound is indicated if a femoral hernia is suspected in this patient group!
References:[5]
Differential diagnoses
- Direct or indirect inguinal hernias (see “Overview of hernias”)
- Femoral pseudohernia
- Lipoma
- Lymph node enlargement
- Femoral artery aneurysm
- Saphenous varix: a dilated, saccular swelling of the great saphenous vein that lies just distal to the junction of the femoral vein and the great saphenous vein
- Psoas abscess
References:[1]
The differential diagnoses listed here are not exhaustive.
Treatment
- Non-complicated femoral hernia: early elective surgical repair with mesh hernioplasty (tension-free repair)
- Complicated femoral hernia: (see “Complications” below): herniorrhaphy (non-mesh repair)
All femoral hernias should be surgically repaired because of the high risk of complications.
References:[6][7][8][9]
Complications
-
Incarceration: irreducible femoral hernia due to trapped hernia contents in hernia sac
- Richter hernia: herniation of only a part of the circumference of the bowel wall.
-
Strangulation: ischemic necrosis of contents within the hernia sac as blood flow is compromised due to incarceration
- Warm, tender, and erythematous/discolored swelling
- Features of mechanical bowel obstruction
- Possibly fever, leukocytosis, and hemodynamic instability
- Features of paralytic ileus supervene once bowel perforation and/or peritonitis develop
Reduction of a strangulated hernia should not be attempted because generalized peritonitis would occur following reduction of strangulated bowel loops!
Although femoral hernias account for only about 5% of all hernias, they account for about 40% of all complicated hernias!
A femoral hernia should be considered among 40–70-year-old women presenting with signs of mechanical bowel obstruction!

References:[5][8][10][11]
We list the most important complications. The selection is not exhaustive.
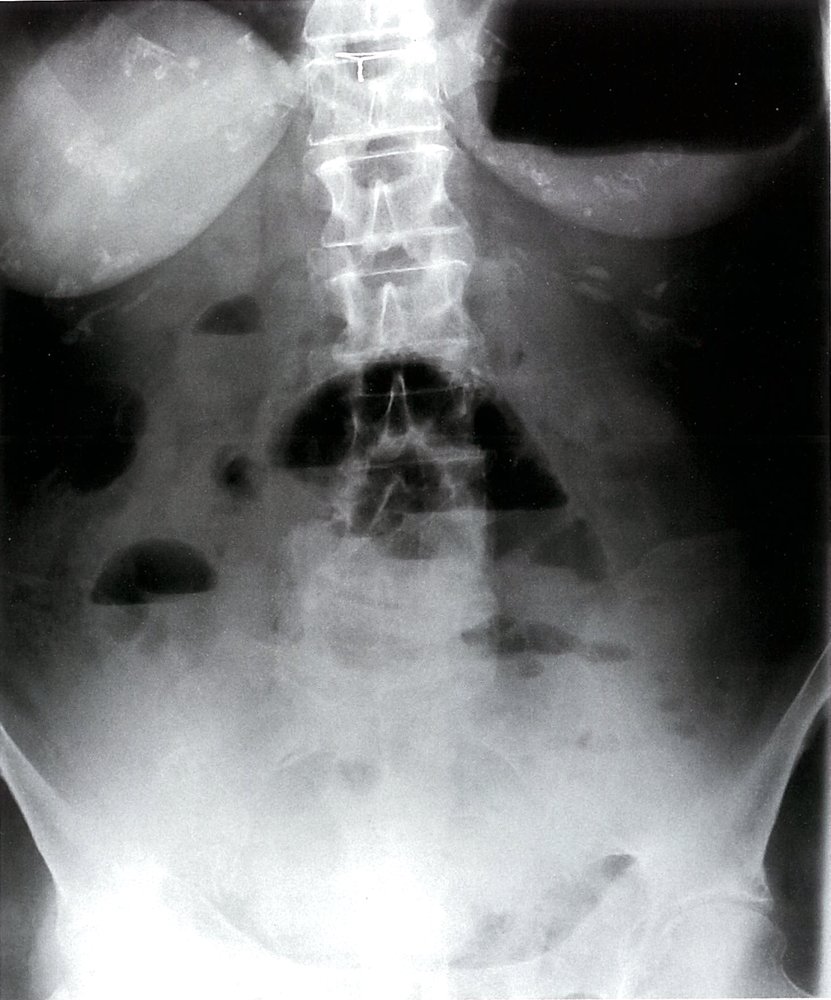
X-ray abdomen (AP view; erect position)
Multiple air-fluid levels (green overlay) are visible in the mid-abdomen. The opaque appearance of the pelvis (red overlay) is due to fluid-filled loops of small bowel. There is a paucity of gas in the colon, and an air-fluid level is present in the dilated stomach (S).
Erect and decubitus radiographs can reveal air-fluid levels that are not identifiable on supine radiographs. Air-fluid levels can indicate ileus or mechanical obstruction. A lack of distal gas and air-fluid levels at different heights in the same bowel loop (differential air-fluid levels) suggest obstruction.
Source: © IMPP
References
- Nigam VK, Nigam S. "Essentials Of Abdominal Wall Hernias ". I.K. International Publishing House. (2008). ISBN: 9788189866938
- Kingsnorth AN, LeBlanc KA. "Management of Abdominal Hernias". Springer. (2013). ISBN: 9781848828766
- Schumpelick V, Fitzgibbons RJ, Conze J, et al. "Recurrent Hernia: Prevention and Treatment". Springer. (2007). ISBN: 9783540375456
- Lawrence P, Bell RM, Dayton MT, Ahmed MI, Hebert JC. "Essentials of General Surgery". Lippincott Williams & Wilkins. (2006). ISBN: 9780781750035
- Brooks DC, Hawn M. "Classification, clinical features and diagnosis of inguinal and femoral hernias in adults". UpToDate. UpToDate. https://www.uptodate.com/contents/classification-clinical-features-and-diagnosis-of-inguinal-and-femoral-hernias-in-adults. [2016-02-04]
- Brooks DC. "Overview of treatment for inguinal and femoral hernia in adults". UpToDate. UpToDate. https://www.uptodate.com/contents/overview-of-treatment-for-inguinal-and-femoral-hernia-in-adults. [2016-09-01]
- Griffen FD. "Open surgical repair of inguinal and femoral hernia in adults". UpToDate. UpToDate. https://www.uptodate.com/contents/open-surgical-repair-of-inguinal-and-femoral-hernia-in-adults. [2016-08-03]
- Brunicardi F, Andersen D, Billiar T, et al. "Schwartz's Principles of Surgery". McGraw-Hill Education. (2014). ISBN: 9780071800921
- Sarosi GA, Kfir B-D. "Laparoscopic inguinal and femoral hernia repair in adults". UpToDate. UpToDate. https://www.uptodate.com/contents/laparoscopic-inguinal-and-femoral-hernia-repair-in-adults?source=search_result&search=Laparoscopic%20repair%20of%20femoral%20hernia&selectedTitle=1~39. [2016-01-27]
- Klingensmith ME, Chen LE, Glasgow SC, Goers TA, Melby SJ. "The Washington Manual of Surgery". Washington University. (2008). ISBN: 9780781774475
- Bendavid R, Abrahamson J, Arregui ME, et al. "Abdominal Wall Hernias: Principles and Management". Springer. (2001). ISBN: 9781461264408