Summary
A femoral shaft fracture is a fracture anywhere along the diaphysis of the femur. These injuries typically result from high-impact trauma (e.g., motor vehicle collisions) and are more common in younger individuals. Low-impact shaft fractures most commonly occur in older adults with pre-existing osteopenia. Affected patients often present with pain and swelling along the thigh and additional findings consistent with fracture (e.g., limb shortening). Signs of fracture on x-ray confirm the diagnosis; advanced imaging studies may be required for surgical planning or if results are inconclusive. In adults, a traction splint may be considered as a temporizing measure; definitive treatment involves internal fixation with an intramedullary nail. In children, treatment varies with age. Complications include vascular compromise and fat embolism.
For fractures of the femoral head, neck, and trochanter, see “Hip fractures.”
Epidemiology
-
Age: bimodal distribution, based on exposure to causative force
- High-energy trauma associated: common in younger population (< 25 years)
- Low-energy trauma associated: common in older population (> 65 years)
- Sex: ♂ > ♀
Epidemiological data refers to the US, unless otherwise specified.
Etiology
A fracture in the diaphysis (shaft) of the femur caused by:
- High-impact trauma: motor vehicle collision, pedestrian-versus-vehicle accidents, falls, gunshot wounds
- Low-impact injuries associated with pathological fractures : fall from standing (height > 1 m)
- Stress fractures (rare): seen in long-distance runners
Classification
Femoral shaft fractures are divided by the Winquist-Hansen classification, based on the degree of comminution. This includes the following categories:
- Type 0: no comminution, simple transverse or oblique
-
Type I
- Small butterfly fragment
- Minimal to no comminution
- Type II: butterfly fragment with at least 50% of the circumference of the cortices of the two major fragments intact
- Type III: butterfly fragment with 50–100% of the circumference of the two major fragments comminuted
-
Type IV
- Segmental comminution
- All cortical contact is lost
Clinical features
- Painful, swollen, tense thigh
- Restricted range of motion
- Limb shortening
- Signs of fracture (e.g., deformity, crepitus)
- Features of open fractures (e.g., lacerations)
- Signs of neurovascular injury (rare in closed injuries) [1]
- Commonly associated injuries include knee and hip fractures and knee ligament injuries. [1]
Diagnosis
Clinical evaluation [1]
Urgent orthopedic consultation is indicated for patients with any features of neurovascular injury or open fracture.
-
Neurovascular examination
- Assess capillary refill time and distal pulses.
- Evaluate for sciatic nerve injuries.
- Skin examination: Evaluate for lacerations, tearing, and tenting.
X-ray
Views [2]
- Femur: anteroposterior (AP) and lateral views
- Hip: AP and lateral views
- Knee: AP and lateral views
- Pelvis: AP view
Findings [1]
- Radiographic signs of a fracture
- Fracture fragments, displacement, angulation, and/or dislocation

Advanced imaging
-
CT
- Indicated if x-ray findings are inconclusive and for preoperative planning in complicated fractures and assessment of associated injuries
- See “CT imaging in trauma.”
- CT angiography: indicated for signs of vascular injury
- MRI: : may be indicated to assess for associated tendon and ligament injuries and pathological fractures [3]
")
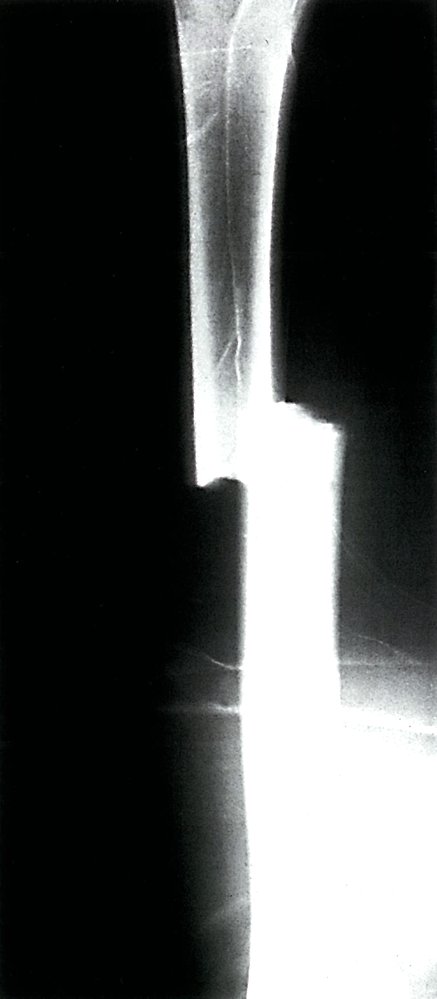
X-ray of femoral shaft; anteroposterior view
Femoral shaft fracture (red overlay) with translation (green arrow) and longitudinal displacement (white arrow)
Source: © IMPP

3D CT reconstruction: multifragmentary, displaced right femoral shaft fracture. Comminuted fracture of the right head of the fibula and tibia. Impacted fracture of the left tibial plateau.
Source: © IMPP
Management
Often managed surgically in adults. See “Femoral shaft fractures in children” for the management of pediatric patients.
Initial management [1][4]
For unstable patients and those with polytrauma, follow the ATLS algorithm.
- Initiate general fracture care, including analgesia.
- Consider a traction splint for temporary immobilization. [4]
- Urgently consult orthopedic surgery.
- Admit to the hospital for surgery.
Femoral shaft fractures can cause significant blood loss into the thigh compartment, potentially leading to hemorrhagic shock.
Surgical management [1][5]
- First-line: internal fixation with an intramedullary nail
-
Alternatives
- Temporary external fixation (e.g., in patients with polytrauma or open fractures) [6]
- Plate fixation [7]

Intramedullary nailing is a method of immobilizing a fracture in a long bone by inserting a metal rod (usually steel or titanium) into the medullary cavity.
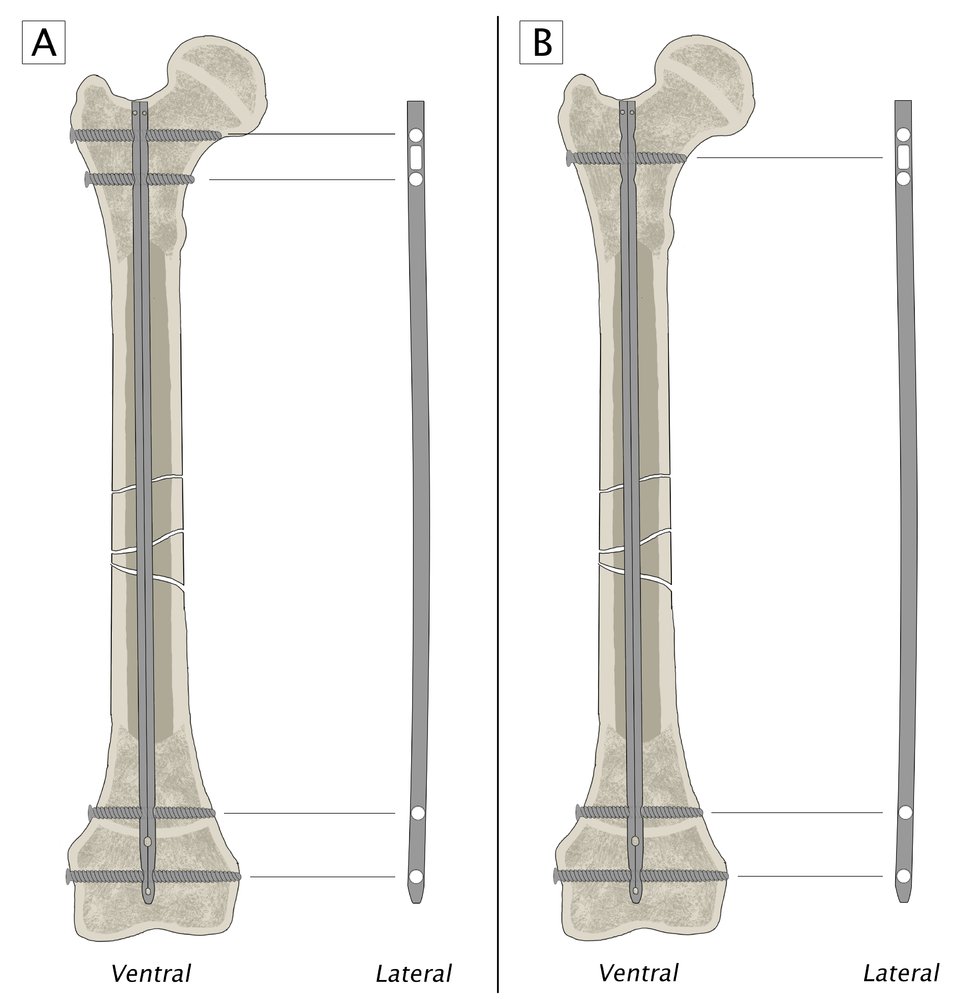
Proximal and/or distal locking screws can be used to improve fixation.
A: Use of the round screw holes on both sides of the fracture provides length-stable locking
B: Use of the elongated screw hole on one side of the fracture permits limited movement along the long axis of the bone (allowing a little fracture impaction) while still maintaining rotational stability
© AMBOSS
Complications
- See “Complications of fractures” (especially vascular injury and fat embolism).
- Posttraumatic deformity
- Rotational error
- Osteoarthritis of the knee
- Myositis ossificans
Look out for symptoms of fat embolism: altered mental status, respiratory distress, petechiae, and fever. [8]
We list the most important complications. The selection is not exhaustive.
Special patient groups
Femoral shaft fractures in children [9]
-
Etiology
- Blunt trauma (e.g., due to falls, motor vehicle collision, sports injuries)
- Nonaccidental trauma
- Clinical features: See “Clinical features of femoral shaft fractures.”
-
Diagnosis
- See “Diagnosis of femoral shaft fractures.”
- Children < 36 months should be evaluated for nonaccidental trauma (e.g., with a skeletal survey).
-
Treatment
- < 6 months of age: Pavlik harness or hip spica cast
- 6 months–5 years of age: hip spica cast
- ≥ 5 years of age: surgery (e.g., internal fixation with an intramedullary nail)



X-ray femur (AP view) of an 11-year-old child
The leg is rotated such that the femur is seen as a lateral projection while the pelvis is seen as a frontal projection. A minimally comminuted transverse fracture of the mid femoral diaphysis is present, and there is overriding of the fracture fragments. No callus formation is seen.
Source: “Figure 1, in: Leg Length Discrepancy Due to Loss of Femoral Antecurvatum After Elastic Stable Intramedullary Nailing of Diaphyseal Fractures of the Femur in Children” by Samelis P V, Papagrigorakis E, Troupis T, Koulouvaris P, Cureus, licensed under CC BY 3.0.
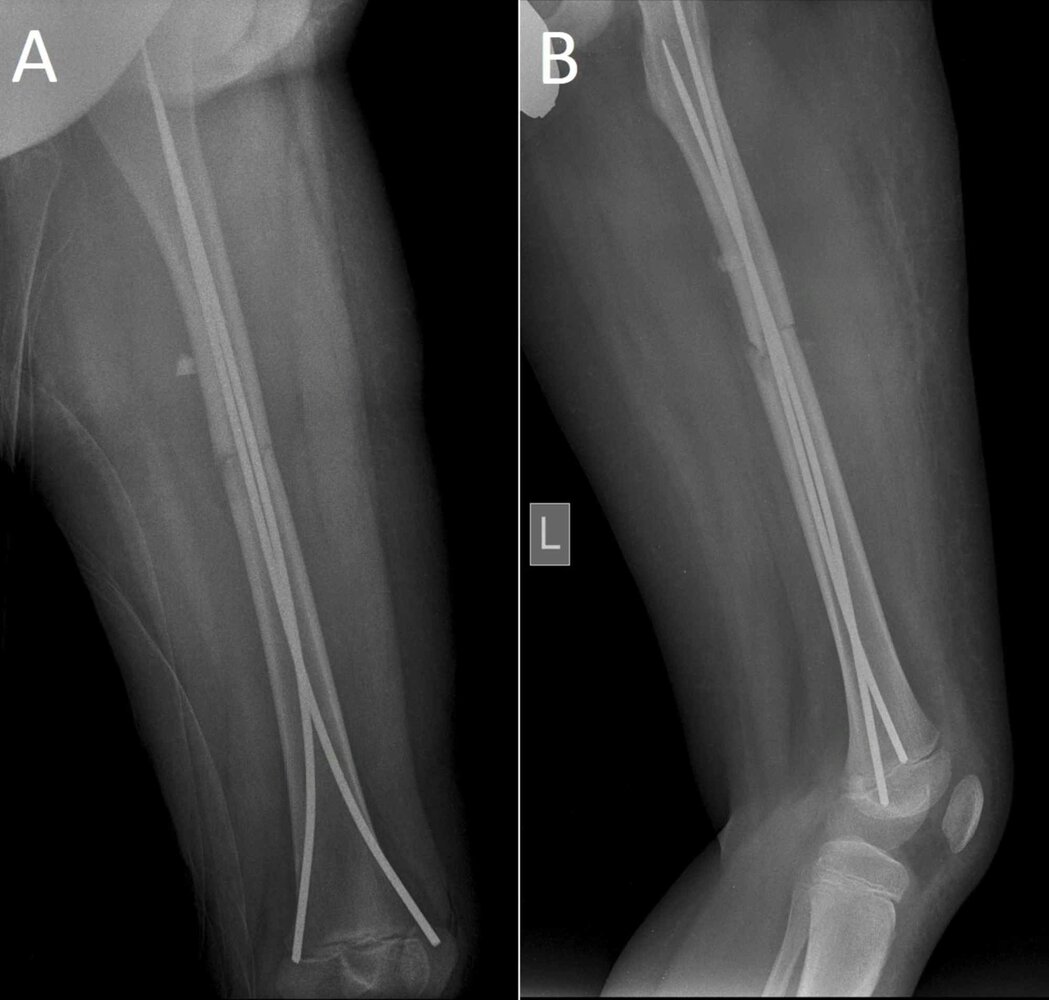
X-ray femur (A: AP view; B: lateral view) of an 11-year-old child
Postreduction radiographs show a minimally comminuted transverse fracture of the mid femoral diaphysis (red lines in zoom-box) with two titanium intramedullary nails in place. There is slight diastasis of the fracture fragments (indicated by double-arrows).
Blue overlay: bone fragments
Source: “Figure 2: "Postoperative X-ray ...", in: Leg Length Discrepancy Due to Loss of Femoral Antecurvatum After Elastic Stable Intramedullary Nailing of Diaphyseal Fractures of the Femur in Children” by Samelis P V, Papagrigorakis E, Troupis T, Koulouvaris P, Cureus, licensed under CC BY 3.0. Modifications: - arrows removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
External Resources
References
- Walls R, Hockberger R, Gausche-Hill M, Erickson TB, Wilcox SR. "Rosen's Emergency Medicine 10th edition- Concepts and Clinical Practice E-Book". Elsevier Health Sciences. (2022). ISBN: 9780323757904
- Makhni MC, Makhni EC, Swart EF, Day CS. "Orthopedic Emergencies". Springer. (2017). ISBN: 9783319315249
- Miao KH, Miao JH. "Radiological Diagnosis and Imaging of Femoral Shaft Fractures". Anatomia. 2(3). :282-299. (2023)
- American College of Surgeons and the Committee on Trauma. "ATLS Advanced Trauma Life Support". American College of Surgeons. (2018). ISBN: 9780996826235
- Gandhi RR, Overton TL, Haut ER, et al. "Optimal timing of femur fracture stabilization in polytrauma patients". J Trauma Acute Care Surg. 77(5). :787-795. (2014)
- Testa G, Aloj D, Ghirri A, et al. "Treatment of femoral shaft fractures with monoaxial external fixation in polytrauma patients". F1000Res. 6. :1333. (2017)
- Zlowodzki M, Vogt D, Cole PA, Kregor PJ. "Plating of Femoral Shaft Fractures: Open Reduction and Internal Fixation Versus Submuscular Fixation". J Trauma. 63(5). :1061-1065. (2007)
- Rothberg DL, Makarewich CA. "Fat Embolism and Fat Embolism Syndrome". J Am Acad Orthop Surg. 27(8). :e346-e355. (2019)
- "Treatment of Pediatric Diaphyseal Femur Fractures Evidence-Based Clinical Practice Guideline". https://web.archive.org/web/20250401081019/https://www.aaos.org/globalassets/quality-and-practice-resources/pdff/pdffcpg.pdf. [2020-12-05]