Summary
Fetal growth restriction (FGR), also known as intrauterine growth restriction, is defined as estimated fetal weight or abdominal circumference below the 10th percentile for a given gestational age. FGR is a pathological condition caused by an underlying maternal (e.g., substance use), placental (e.g., placental insufficiency), or fetal factor (e.g., aneuploidy) that impedes the fetus from reaching its expected growth potential, unlike a constitutionally small fetus. All pregnant individuals should be screened for FGR with fundal height measurements from 24 weeks' gestation. Obstetric ultrasound is indicated if fundal height is more than 3 cm below the expected size for gestational age. Further studies may be required to identify the underlying cause of FGR. Management involves treatment of the underlying cause and referral to maternal-fetal medicine for antepartum surveillance and delivery planning.
Definitions
- Fetal growth restriction: fetal estimated weight or abdominal circumference < 10th percentile for current gestation caused by a pathological factor that impedes fetal growth (e.g., placental insufficiency, maternal comorbidities, genetic abnormalities)
- Constitutionally small fetus: estimated fetal weight < 10th percentile, thought to be due to physiological rather than pathological factors [2]
- Small for gestational age: birth weight < 10th percentile for gestational age
Epidemiology
- Second leading cause of perinatal morbidity and mortality following preterm birth worldwide [3]
- Occurs in ∼ 10% of pregnancies [4]
Epidemiological data refers to the US, unless otherwise specified.
Etiology
Maternal causes
- Substance use (e.g., alcohol, cigarettes, cocaine, heroin)
- Teratogenic drugs: ACE inhibitors, carbamazepine, phenytoin, warfarin
- Maternal phenylketonuria
- Systemic diseases resulting in placental insufficiency
Uteroplacental causes
-
Placental insufficiency (most common cause in the US) [1]
- Definition: A disorder of the fetomaternal circulation that causes inadequate blood flow to the placenta and impaired substance exchange (e.g., oxygen) between the mother and fetus, leading to metabolic compromise of the fetus.
- Causes and risk factors
- Maternal conditions (smoking during pregnancy, diabetes mellitus with vasculopathy, chronic hypertension, severe anemia, anorexia nervosa, antiphospholipid syndrome, SLE, sickle cell disease)
- Pregnancy-related conditions (preeclampsia, Rh incompatibility)
- Clinical features: depend on the underlying cause
- Complications: fetal growth restriction, placental abruption, preterm labor, stillbirth, Potter sequence, oligohydramnios
- Placenta previa
- Multiple gestation
- Placental abruption
- Umbilical artery thrombosis/extensive infarction [5]
- Uterine malformations (e.g., fibroids)
Fetal factors
- Genetic abnormalities in the fetus (e.g., aneuploidy)
- Cyanotic congenital heart defects
- Early intrauterine infections (TORCH)
Asymmetrical fetal growth restriction is the most common manifestation of fetal growth restriction (∼ 70%), has a late onset, and is usually due to maternal systemic disease (e.g., hypertension) that results in placental insufficiency. Symmetrical fetal growth restriction is less common (∼ 30%) and is usually due to a genetic disorder (e.g., aneuploidy), congenital heart disease, or early intrauterine TORCH infection that affects the fetus early in gestation.
Pathophysiology
Recent studies show that the symmetry of growth restriction alone cannot reliably indicate an intrinsic or extrinsic cause; therefore, the terms “symmetrical” and “asymmetrical” FGR should be avoided. Symmetrical and asymmetrical FGR are covered in this article for exam purposes. [7]
Asymmetrical fetal growth restriction
- The head is normally proportioned while the body and limbs are thin and small.
- Caused by extrinsic factors, which affect the fetus in the later stages of gestation (i.e., third trimester).
-
Impaired function of the uteroplacental unit (see placental function) → insufficient transplacental delivery of oxygen and nutrients to the fetus and impaired return of carbon dioxide and fetal metabolic waste products from the fetus to the mother's circulation
- Effect on fetal development
- Fetal hypoxia and hypoglycemia → shunting of blood flow to vital fetal organs (brain, heart, and adrenal glands) bypassing other organs (e.g., liver, muscle, fat tissue)
- Fetal switch to anaerobic glycolysis → metabolic acidosis → lactic acid accumulates → progressive damage to vital fetal organs (e.g., brain, myocardium) → permanent damage, possibly fetal death
- Effect on maternal factors
- Decreased placental growth (↓ placental surface area) → further impairs placental function
- ↑ Risk of preeclampsia, preterm labor, vaginal bleeding [8]
- Effect on fetal development
Symmetrical fetal growth restriction
- Global growth restriction, affecting all parts of the body
- Caused by intrinsic factors (e.g., genetic abnormalities, infections), which affect the fetus in the early stages of gestation.
Clinical features
Fetal signs
- Decreased or absent fetal movements [9]
- At birth: small for gestational age (birth weight below 10th percentile)
Maternal signs
- Mostly asymptomatic
-
Decreased symphysis-fundal height
- Measured between 24 and 36 weeks of gestation [10]
- Fundal height at least 3 cm less than gestational age in weeks is a sign of FGR.
- Small uterus (e.g., a smaller abdomen than in previous pregnancies)
- Symptoms of underlying etiology of FGR (e.g., vaginal bleeding secondary to placental abruption)

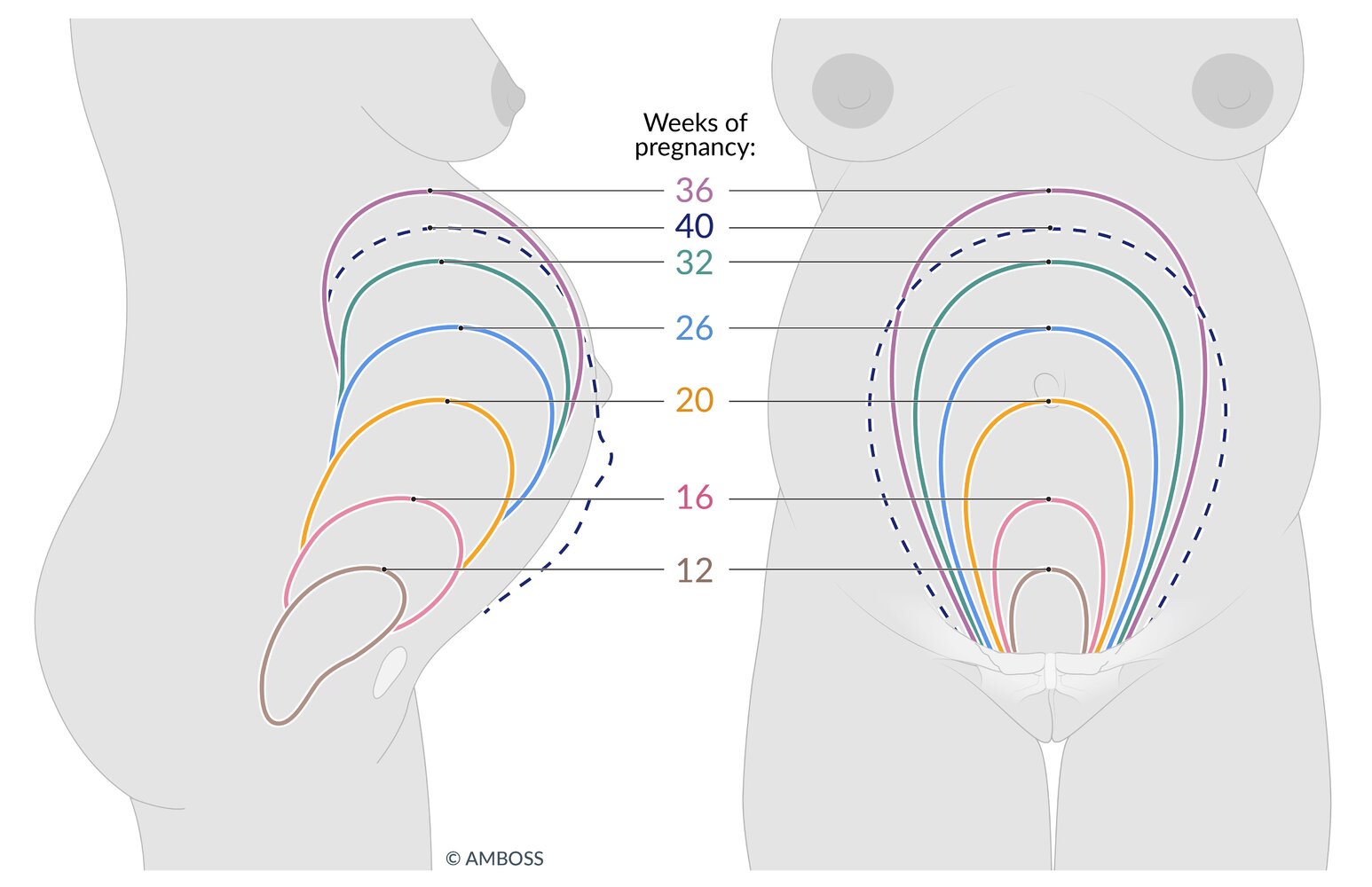
Illustration of expected fundal height throughout pregnancy
At 12 weeks' gestation, the fundus is usually just emerging from the pelvic brim. By 20 weeks, it is palpable at the height of the umbilicus. The fundus is highest at 36 weeks' gestation at the costal arch; at 40 weeks' gestation, it usually drops to two finger widths below the costal arch.
© AMBOSS
Diagnosis
FGR is usually discovered as part of routine prenatal care (e.g., if fundal height is smaller than expected for gestation).
Approach [11][12]
- Obtain an obstetric ultrasound if:
- Fundal height is more than 3 cm below expected size for gestational age after 24 weeks' gestation
- A risk factor for FGR has been identified [12]
- Assess for underlying etiologies (e.g., screening for hypertensive pregnancy disorders).
- Determine if FGR is early or late.
- Early-onset FGR: < 32 weeks' gestation
- Late-onset FGR: ≥ 32 weeks' gestation
- Refer to maternal-fetal medicine for advanced diagnostic studies.
Preeclampsia and genetic disorders are common underlying causes of early-onset FGR; a more comprehensive workup is recommended in early-onset FGR than late-onset FGR. [11][12]
Initial ultrasound
- Finding: estimated fetal weight or abdominal circumference < 10th percentile for gestational age [12][13]
- Growth restriction may be: [14]
- Disproportionate: head is normal size but body and limbs are thin and small
- Proportionate: the entire body is proportionally small
- Manifestations of underlying causes (e.g., fetal anomalies secondary to aneuploidy, signs of placental insufficiency) may be visible.
Advanced diagnostic studies [11]
- All patients: detailed obstetric ultrasound
- Perform invasive prenatal genetic testing (and CMV PCR if amniocentesis is performed) for patients with:
- Early-onset FGR
- Polyhydramnios
- Fetal anomalies detected on ultrasound
Differential diagnoses
Constitutionally small fetus
- Definition: estimated fetal weight < 10th percentile without an identified underlying condition
-
Predisposing factors [15]
- Low maternal height
- Low maternal weight before/in early pregnancy
- Asian descent [16]
- Parity
- Fetal female sex
-
Diagnosis
- Assessment of fetal growth using customized growth charts [17]
- Doppler velocimetry of the umbilical artery: normal systolic/diastolic ratio [18]
- Prognosis: constitutionally small fetuses are not at increased risk for adverse perinatal outcomes
The differential diagnoses listed here are not exhaustive.
Management
Start treating underlying causes of FGR (e.g., hypertensive pregnancy disorders, diabetes in pregnancy) and refer patients to maternal-fetal medicine for further management. [1][12]
Fetal monitoring [11][19][20]
- Initiate antepartum fetal surveillance once the fetus is viable.
- The modality and frequency varies based on maternal and fetal factors, but usually includes: [11][12][19][21]
- Ultrasound for fetal growth (fetal biometric parameters) [19]
-
Doppler velocimetry of the umbilical artery to evaluate for placental insufficiency
- Assesses for reduced, absent, or reversed end-diastolic flow
- Results determine the frequency of repeat monitoring, cardiotocography, and delivery.
- Biophysical profile (BPP) or modified BPP (often including a nonstress test)
- Cardiotocography
Delivery planning [11][19]
- Immediate delivery if there are signs of fetal distress (e.g., BPP score ≤ 4, repetitive late decelerations)
-
Consideration of early scheduled delivery
- Timing of delivery is based on results of Doppler velocimetry of the umbilical artery. [11]
- Give antenatal corticosteroid therapy for fetal maturation if delivery is scheduled for < 34 weeks' gestation. [11][12]
 showing late decelerations")
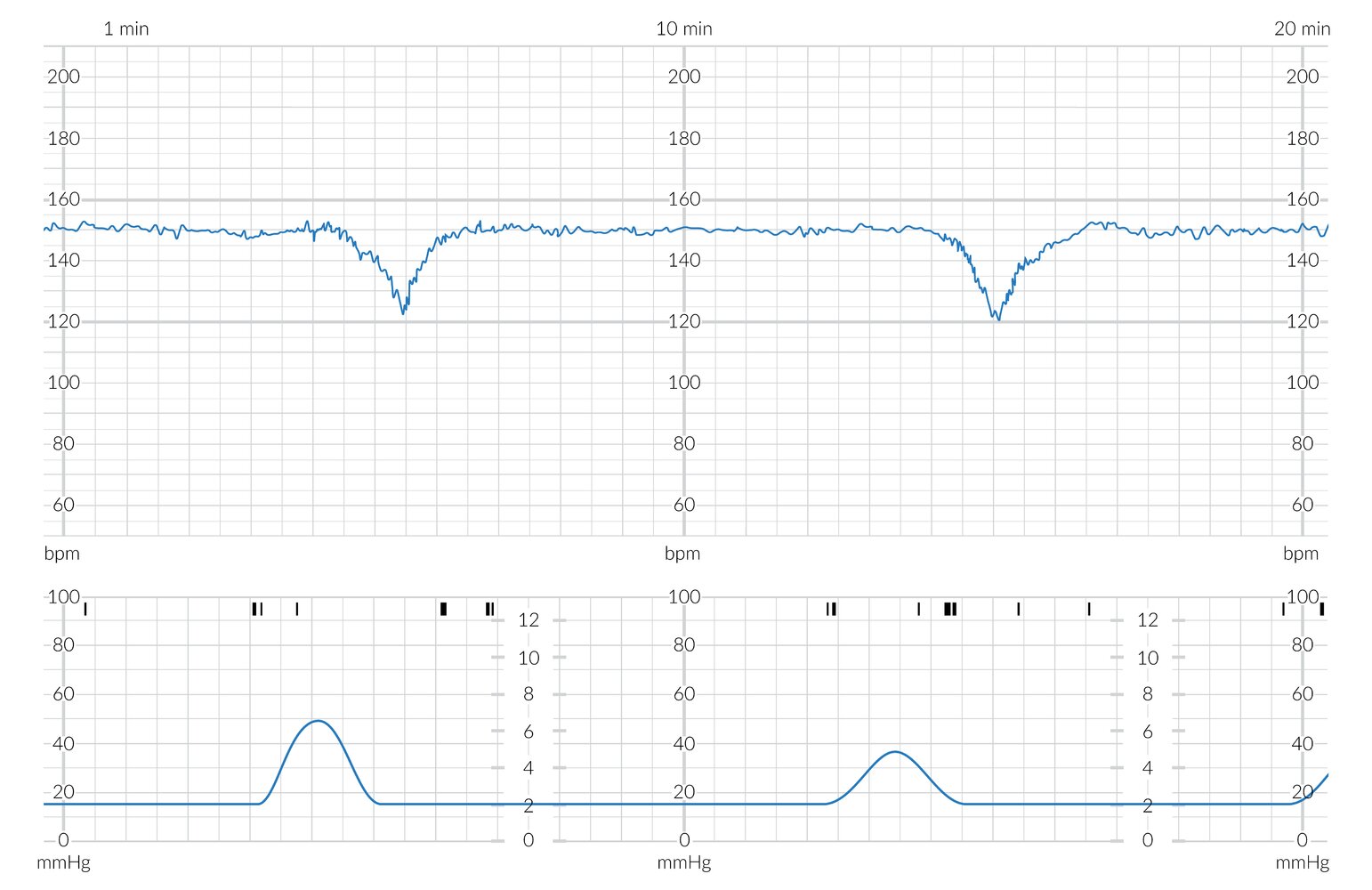
The upper blue tracing shows the fetal heart rate (FHR) in beats per minute (bpm) with a baseline of approx. 150 bpm (green dashed line overlay). The FHR lies within the normal range (green shading overlay) and shows minimal variability (< 6 bpm; normal range 6–25 bpm).
The lower blue tracing shows the maternal uterine contractions (in mm Hg). The black markings above this tracing show fetal movements (blue shading overlay).
The decelerations begin after the peaks of the uterine contractions (red dashed line overlay). These are gradual, with ≥ 30 s from onset to nadir (red arrow overlay). These findings are characteristic of late decelerations.
© AMBOSS
Complications
- Stillbirth
- Preterm labor
- Low birth weight; (< 2500 g) with ↑ risk of sudden infant death syndrome
- Perinatal asphyxia
- Hypoglycemia, hypocalcemia
- Hypothermia
- Possibly motor and neurological disabilities
The risk of morbidity and mortality increases in pregnancies affected by early-onset FGR. [12]
We list the most important complications. The selection is not exhaustive.
Prevention
- No specific interventions have been shown to be effective at preventing FGR. [1]
- Early identification and treatment of underlying causes (e.g., hypertensive pregnancy disorders) is recommended.
There is insufficient evidence to recommend bed rest, aspirin or heparin, sildenafil, or specific nutrition to prevent FGR. [1][11]
References
- Martins JG, Biggio JR, Abuhamad A. "Society for Maternal-Fetal Medicine Consult Series #52: Diagnosis and management of fetal growth restriction". Am J Obstet Gynecol. 223(4). :B2-B17. (2020)
- Westby A, Miller L. "Fetal Growth Restriction Before and After Birth". Am Fam Physician. 104(5). :486-492. (2021)
- AIUM, ACR, ACOG, et al. "AIUM-ACR-ACOG-SMFM-SRU Practice Parameter for the Performance of Standard Diagnostic Obstetric Ultrasound Examinations". J Ultrasound Med. 37(11). :E13-E24. (2018)
- Lees C, Visser GHA, Hecher K. "Placental-Fetal Growth Restriction". Cambridge University Press. (2018). ISBN: 9781108548182
- Suhag A, Berghella V. "Intrauterine Growth Restriction (IUGR): Etiology and Diagnosis". Curr Obstet Gynecol Rep. 2(2). :102-111. (2013)
- Colella M, Frérot A, Novais ARB, Baud O. "Neonatal and Long-Term Consequences of Fetal Growth Restriction". Curr Pediatr Rev. 14(4). :212-218. (2018)
- ACOG. "Fetal Growth Restriction Practice Bulletin 227". Obstet Gynecol. 137(2). :e16-e28. (2021)
- Leveno K, Bloom S, Casey B, et al. "Williams Obstetrics". McGraw-Hill Education Ltd. 25th. (2018). ISBN: 9781259644320
- Moh W, Graham JM Jr, Wadhawan I, Sanchez-Lara PA. "Extrinsic factors influencing fetal deformations and intrauterine growth restriction". J Pregnancy. 2012. :750485. (2012)
- Salomon LJ, Alfirevic Z, Da Silva Costa F, et al. "ISUOG Practice Guidelines: ultrasound assessment of fetal biometry and growth". Ultrasound in Obstetrics & Gynecology. 53(6). :715-723. (2019)
- Beckmann CRB. "Obstetrics and Gynecology". Lippincott Williams & Wilkins. (2010). ISBN: 0781788072
- Baschat DAA. "Fetal responses to placental insufficiency: an update". BJOG. 111(10). :1031-1041. (2004)
- Belizán JM, Villar J, Nardin JC, Malamud J, De Vicurna LS. "Diagnosis of intrauterine growth retardation by a simple clinical method: measurement of uterine height". Am J Obstet Gynecol. 131(6). :643-6. (1978)
- Gardosi J. "New Definition of Small for Gestational Age Based on Fetal Growth Potential". Hormone Research in Paediatrics. 65(Suppl. 3). :15-18. (2006)
- Lee AC, Katz J, Blencowe H, et al. "National and regional estimates of term and preterm babies born small for gestational age in 138 low-income and middle-income countries in 2010". The Lancet Global Health. 1(1). :e26-e36. (2013)
- Gardosi J, Francis A, Turner S, Williams M. "Customized growth charts: rationale, validation and clinical benefits". Am J Obstet Gynecol. 218(2). :S609-S618. (2018)
- Harkness UF, Mari G. "Diagnosis and management of intrauterine growth restriction". Clin Perinatol. 31(4). :743-764. (2004)
- ACOG. "ACOG Practice bulletin 229-Antepartum Fetal Surveillance (reaffirmed 2024)". Obstet Gynecol. 137(6). :e116-e127. (2021)
- ACOG. "Indications for Outpatient Antenatal Fetal Surveillance (reaffirmed 2024)". Obstetrics & Gynecology. 137(6). :e177-e197. (2021)
- Shipp TD, Zelop CM, Maturen KE, et al. "ACR Appropriateness Criteria® Growth Disturbances-Risk of Fetal Growth Restriction". J Am Coll Radiol. 16(5). :S116-S125. (2019)
- Figueras F, Caradeux J, Crispi F, et al. "Diagnosis and surveillance of late-onset fetal growth restriction". Am J Obstet Gynecol. 218(2). :S790-S802.e1. (2018)