Summary
Fever of unknown origin (FUO) is defined as a temperature of > 38.3°C (> 100.9°F) lasting for > 3 weeks with no clear etiology despite appropriate diagnostics. Infections, malignancy, and inflammatory or rheumatic conditions are the most frequent etiologies of FUO. The initial diagnostic approach to FUO should focus on a comprehensive history and physical examination with minimal initial diagnostics to identify diagnostic clues that can guide targeted diagnostics. If the diagnosis remains unknown, additional laboratory studies (e.g., serology, electrophoresis) and advanced diagnostics (e.g., PET-CT, tissue biopsy) should be considered. In a significant number of patients, the underlying etiology remains undiagnosed. Antipyretics and empiric therapy (e.g., antibiotics, glucocorticoids) should be avoided, if feasible, to prevent masking clinical findings and delaying the diagnosis even further. However, if a life-threatening or serious underlying condition (e.g., neutropenic fever, miliary tuberculosis, giant cell arteritis) is suspected, empiric therapy should be considered. The prognosis of FUO depends on the underlying cause and spontaneous remission can occur in up to 40% of patients.
“Fever” and “Neutropenic fever” are covered in detail separately.
Definitions
Definitions of FUO vary in literature. Some authors exclude immunocompromised patients from the FUO definition because the approach to diagnosis and treatment is markedly different from that for immunocompetent patients.
- Classic FUO: temperature of : > 38.3°C (> 100.9°F) recorded on multiple occasions that lasts for > 3 weeks with no clear etiology despite investigations on 3 outpatient visits, 3 days in the hospital, or 1 week of invasive ambulatory investigation
-
Nonclassic FUO is characterized by temperature > 38.3°C recorded on multiple occasions with no clear etiology after at least 2 days of culture incubation in addition the following specific features:
- Neutropenic FUO (immunodeficient FUO): neutrophil count of < 500/mm3 or an anticipated fall in neutrophil count to < 500/mm3 within 1–2 days
- HIV-associated FUO: fever that lasts for > 4 weeks (or > 3 days if hospitalized) in a patient with HIV
- Nosocomial FUO: fever that lasts for > 3 days in a hospitalized patient who was afebrile on admission
References: [1][2]
Etiology
Although there are hundreds of possible etiologies of FUO, an atypical presentation of a common condition is often accountable.
Classic FUO [1][3]
-
Most etiologies of classic FUO can be grouped into four major categories:
- Infection
- Inflammatory (e.g., rheumatic conditions, autoimmune conditions)
- Malignancy
- Miscellaneous
- In 7–51% of cases, the underlying etiology remains undiagnosed.
In recent years, the frequency of infectious and miscellaneous causes of FUO has decreased in high-income countries, whereas the frequency of inflammatory diseases has increased. [1][4]
| Categories of classic FUO [1][3][4][5] | ||
|---|---|---|
|
Category [1] |
Common causes | Less common causes |
| Infection (11–55%) |
|
|
|
Inflammatory or rheumatic conditions (12–34%) |
|
|
|
Malignancy (7–35%)[1][6] |
|
|
|
Miscellaneous (2–20%) |
|
|
Healthcare-associated FUO [1]
In addition to the common causes of fever, consider the following in this group of patients:
- Drug fever
- Intravascular catheter-related infection
- Venous thromboembolism (DVT, pulmonary embolism)
- Clostridioides difficile colitis
- Inflammatory response to major surgery
- Occult abscess
- Transfusion reactions
- Sinusitis
- Candidemia (if critically ill)
Immunodeficiency-associated FUO [1]
In addition to the common causes of fever, consider the following in this group of patients:
- Opportunistic infections (e.g., candidiasis, aspergillosis, CMV infection)
- Drug fever (more common in neutropenic patients) [1]
- Malignancy
- In people living with HIV, also consider HIV-associated conditions (e.g., Pneumocystis pneumonia, MAC infection, Kaposi sarcoma) and immune reconstitution inflammatory syndrome.
Diagnosis
Approach [1][4][7][8][9]
The evaluation of a patient with FUO should proceed in a stepwise fashion, guided by diagnostic clues obtained from the history and physical examination.
-
Perform a comprehensive clinical evaluation.
- Document contact with animals, travel history, diet history, immunosuppression, family history, social and sexual history, occupational history, drugs and medications, implants, catheters, and grafts (see “Focused history” in “Fever”).
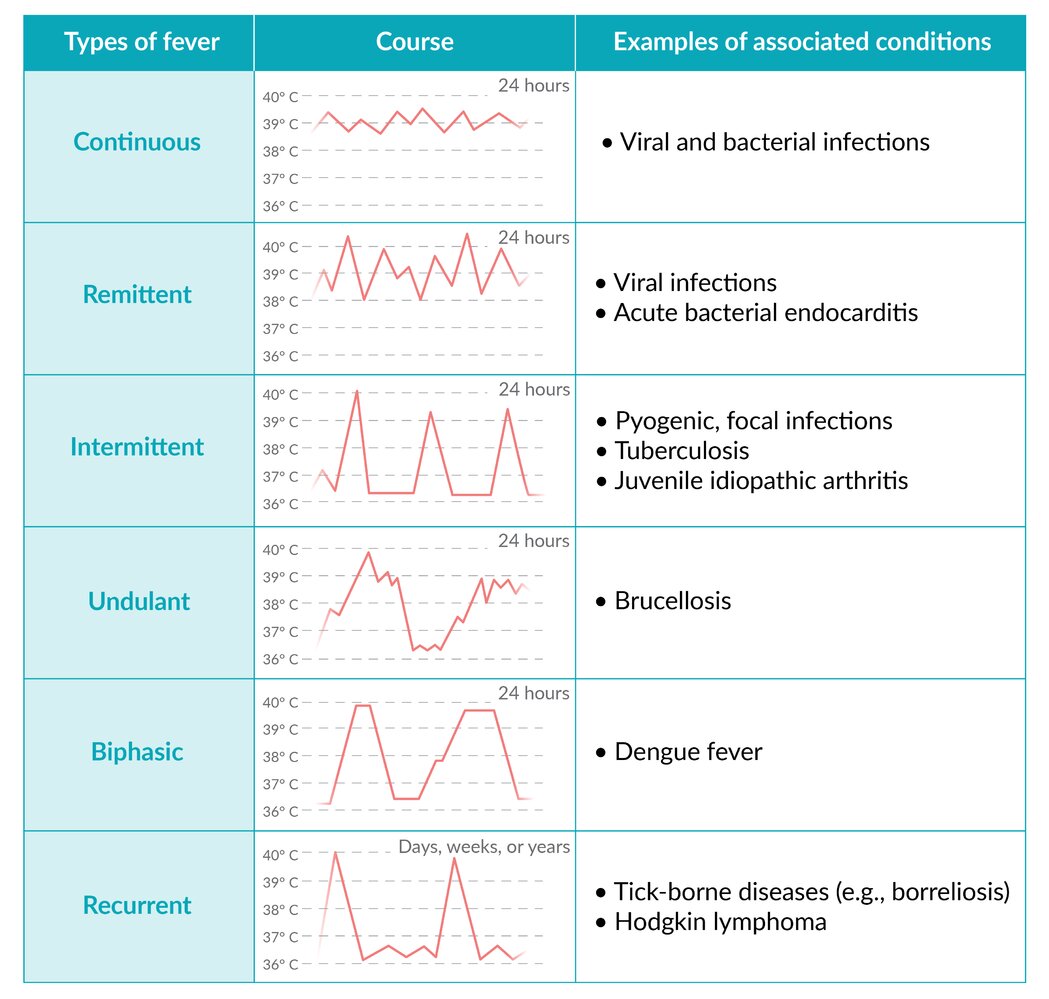
- Conduct serial physical examinations (see “Focused examination” in “Fever” and “Differential diagnosis of fever by course”).
- Consider discontinuing nonessential drugs to exclude drug fever.
- Order minimal initial diagnostics.
- Identify hallmarks or diagnostic clues.
- See “Differential diagnoses of fever by risk factors.”
- See “Differential diagnoses of fever by associated finding.”
- Consult ophthalmology for fundoscopic evaluation. [3]
- Diagnosis evident: Order appropriate diagnostic tests (see “Targeted testing based on diagnostic clues” below).
- Etiology remains undiagnosed (FUO confirmed)
- Consider the naproxen test to differentiate between an infectious etiology and an underlying malignancy.
- Administer naproxen for 3 days.
- Resolution of the fever with naproxen indicates that a malignant etiology is likely. [3]
- Consider measuring procalcitonin levels to distinguish between a bacterial infection and a noninfectious inflammatory condition. [10]
- Consider the naproxen test to differentiate between an infectious etiology and an underlying malignancy.
-
Diagnosis remains unknown
- Perform serial physical examinations and chart review
- Order advanced tests (e.g., PET CT, biopsies) until a diagnostic endpoint is reached or the fever resolves. [11]
The majority of patients with FUO present with atypical symptoms of a common disease rather than common symptoms of a rare disease. [4]
Consider the possibility of factitious fever, especially in medical personnel. [3]
Initial diagnostics [1][2][3][7][12]
Minimum diagnostic workup
-
Laboratory studies
- CBC with differential (see “Differential diagnoses of fever by associated finding” and “Overview of WBC parameters”)
- Acute phase reactants : erythrocyte sedimentation rate; (ESR) and C-reactive protein (CRP)
- Liver chemistries
- Serum electrolytes
- LDH
- Creatine kinase
- Urinalysis and urine culture
- Blood culture (three sets) if bacteremia is suspected [3][8]
-
Imaging
- X-ray or CT chest
- Ultrasound or CT abdomen and pelvis
Additional diagnostics
The identification of diagnostic clues and/or hallmark features on initial clinical and diagnostic evaluation should guide a selective approach to diagnostic studies.
| Targeted testing based on diagnostic clues [1][2][3][9] | |||
|---|---|---|---|
| Category | Diagnostic clues | Suggested testing | |
| Infection |
|
|
|
| Inflammatory disease |
|
|
|
| Malignancy |
|
|
|
| Miscellaneous | Subacute thyroiditis |
|
|
| Thromboembolic disease |
|
|
|
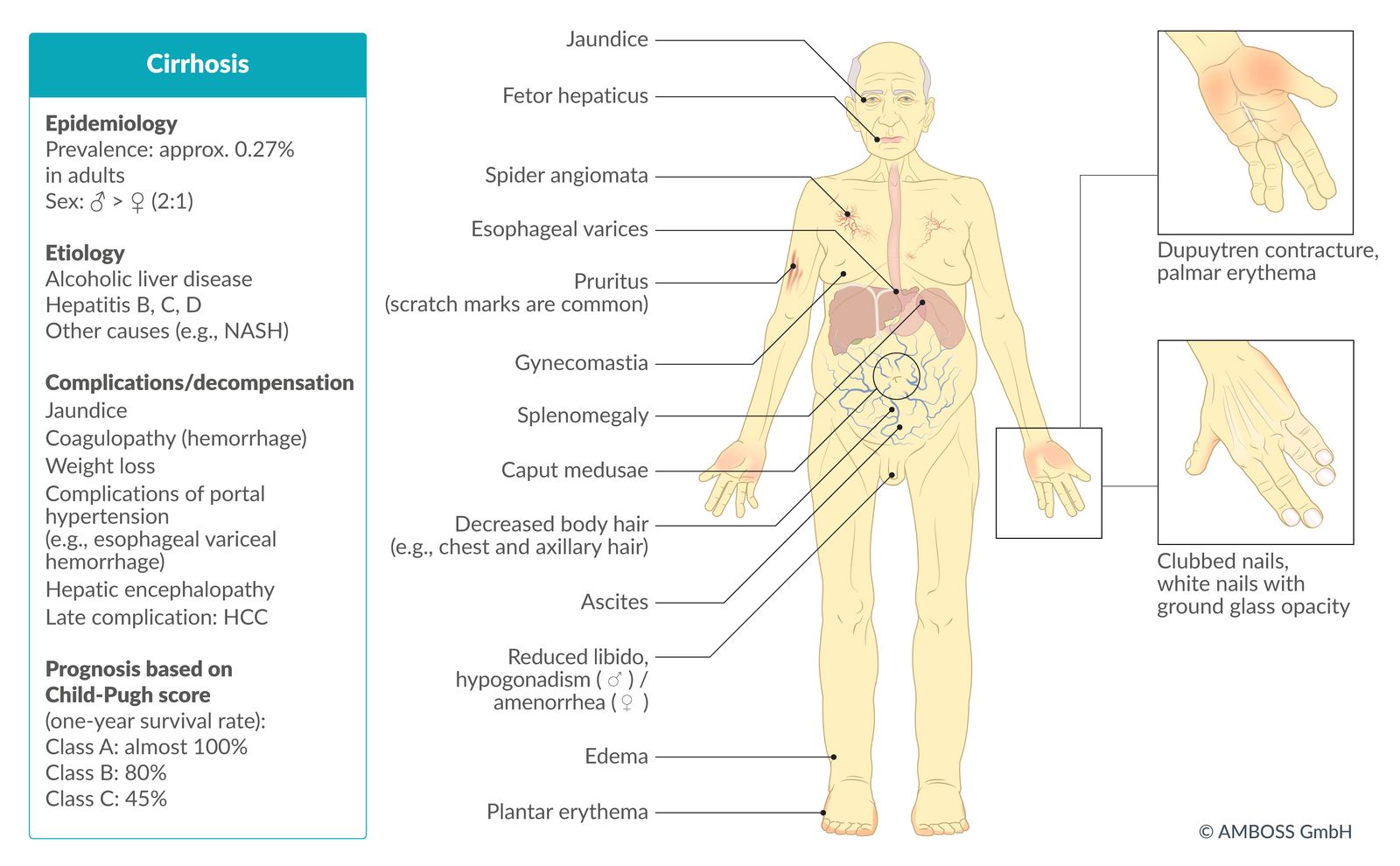
| Cirrhosis |
|
|
|
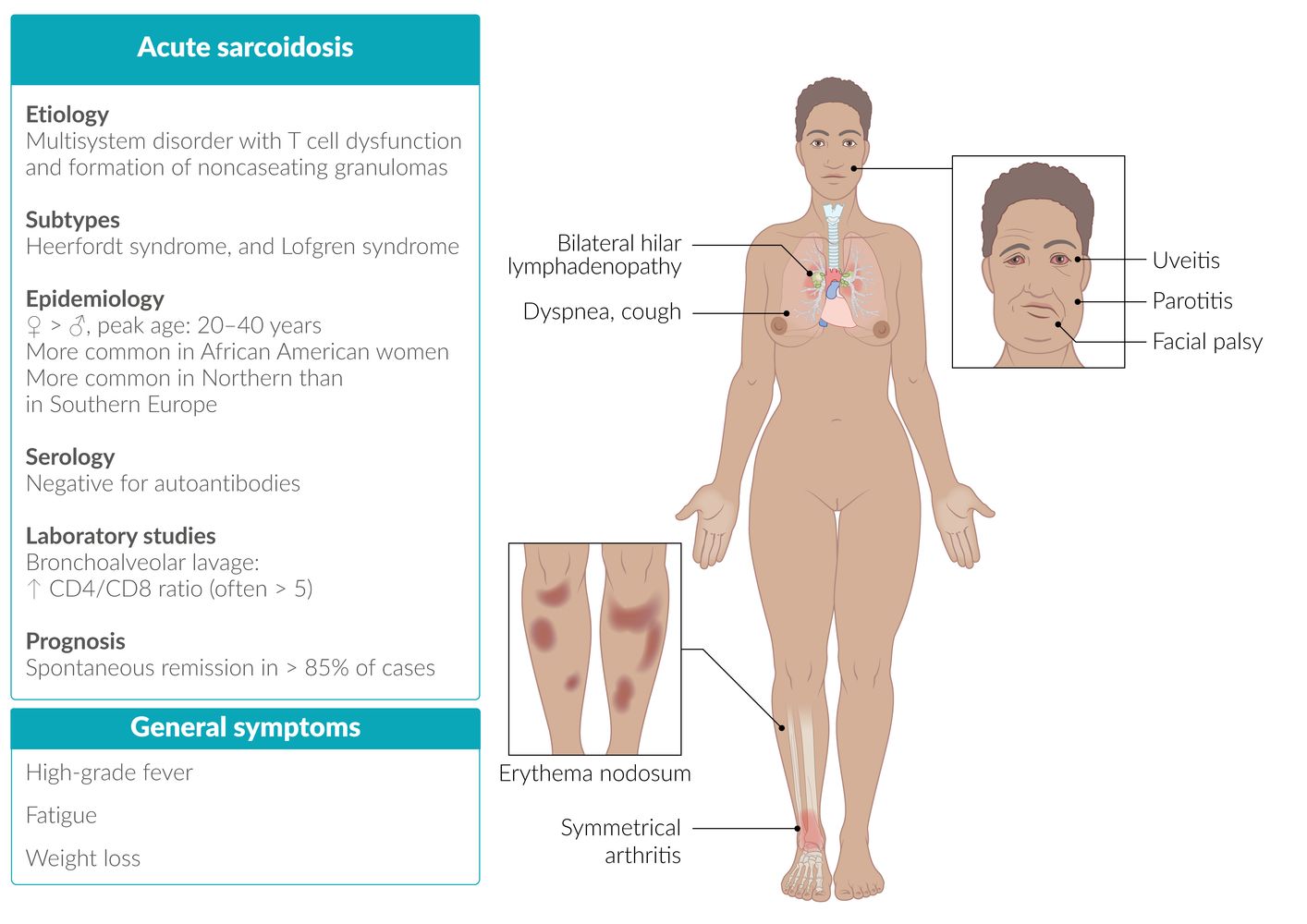
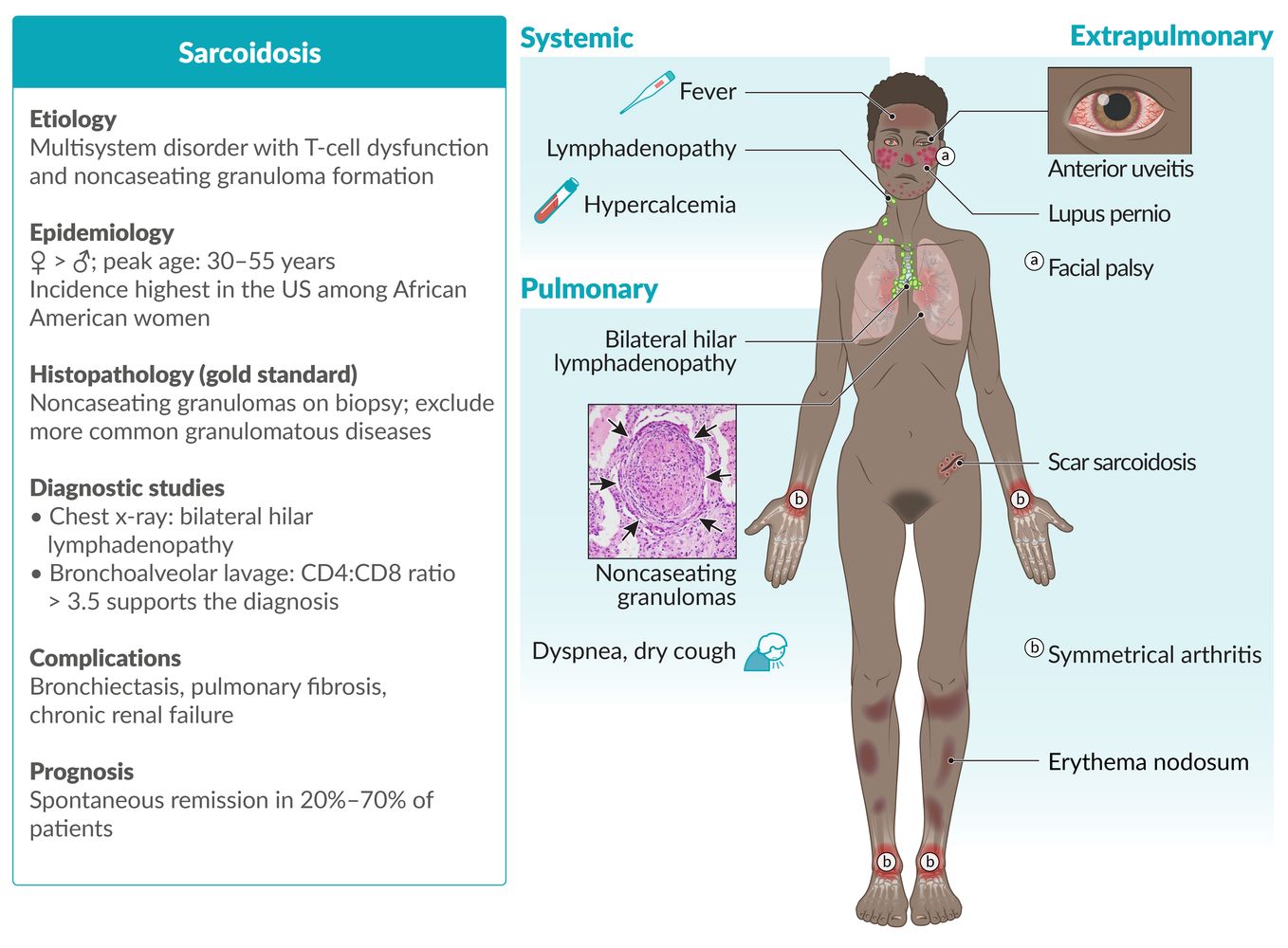
| Sarcoidosis |
|
|
|
| Drug fever |
|
|
|
| Familial Mediterranean fever [16] |
|
|
|
Advanced diagnostics
If the underlying etiology remains undiagnosed despite initial diagnostics, advanced diagnostics to evaluate for less common causes of FUO should be performed.
-
Additional nonspecific laboratory studies
- Serum ferritin: Highly elevated levels are suggestive of a noninfectious etiology. [7][17]
- Cryoglobulins: may be positive in patients with neoplastic disease, inflammatory disease, or viral infection
- Cold agglutinins: elevated in certain infections (e.g., mycoplasma pneumonia, EBV, viral hepatitis), malignancy (e.g., lymphoma), or inflammatory disease
- Uric acid: elevated levels are suggestive of malignancy
- Further serologic testing, e.g., for EBV infection, CMV infection, brucellosis, bartonellosis
-
Serum protein electrophoresis [3]
- Monoclonal gammopathy: e.g., multiple myeloma, Waldenstrom macroglobulinemia
- Polyclonal gammopathy: e.g., HIV, malaria, SLE
-
Advanced imaging studies
-
FDG-PET scan [18][19]
- Consider for all patients without a diagnosis after initial diagnostics, especially those with elevated CRP and/or ESR. [7]
- FDG uptake identifies tissues with high metabolic activity, indicating areas that warrant further investigation.
- CT or MRI chest and abdomen: Consider if not already obtained, FDG-PET is unavailable, or FDG-PET indicates an intrathoracic or intraabdominal abnormality. [3][20]
- Transesophageal echocardiogram (TEE): Consider for suspected bacterial endocarditis. [21][22]
-
FDG-PET scan [18][19]
-
Invasive tests [2][23]
-
Lymph node biopsy [3]
- Consider for patients with lymphadenopathy.
- Posterior cervical, supra/infraclavicular, and epitrochlear nodes have the highest diagnostic yield.
- Avoid anterior cervical, axillary, and inguinal node biopsies, as histological results are usually nondiagnostic.
- Temporal artery biopsy: Consider in patients ≥ 55 years of age. [7][8]
- Liver biopsy: Consider in patients with suspected hepatic involvement (e.g., those with altered liver enzymes or liver abnormalities on imaging studies). [7]
-
Bone marrow studies
- Consider bone marrow biopsy if diagnostic clues for myeloproliferative or myelodysplastic disease are present (e.g., pancytopenia, atypical cells on peripheral blood smear). [7]
- Consider bone marrow culture for suspected culture-negative bacterial endocarditis, miliary tuberculosis, or typhoid fever if it would alter the management. [3][12]
- Diagnostic laparoscopy or laparotomy: rarely indicated unless a biopsy cannot be obtained using another modality [1][3]
-
Lymph node biopsy [3]




© AMBOSS
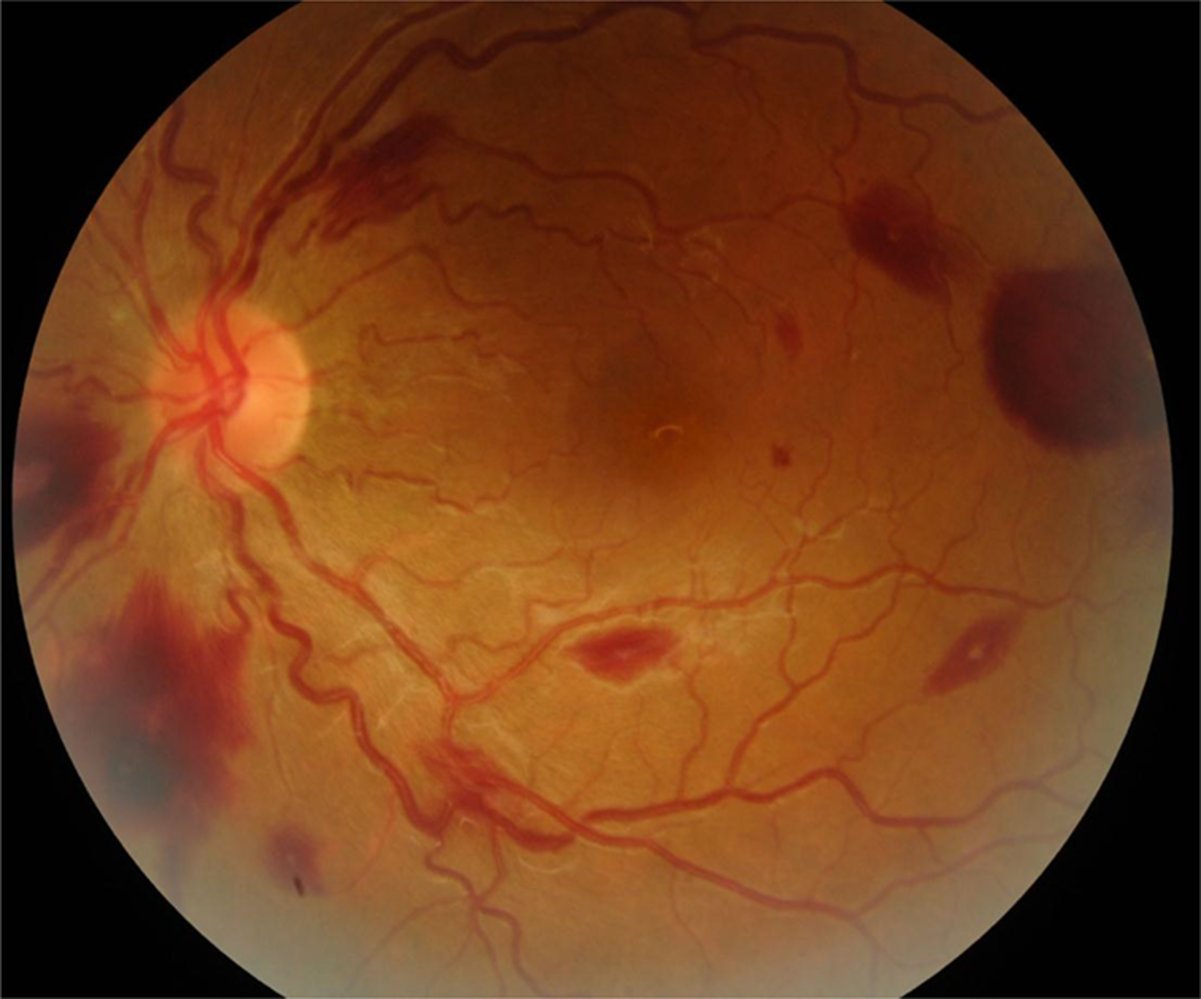
Fundus photography of a left eye
There are multiple red, white-centered lesions, which reflect small retinal hemorrhages with central accumulation of leukocytes or fibrin thrombocyte emboli (examples indicated by arrowheads).
Although these findings were formerly considered to be associated almost exclusively with infective endocarditis, they may actually occur in a variety of conditions, including hypertensive, diabetic, and HIV-related retinopathy; leukemia; and intracranial hemorrhage.
Circle: optic disc; M= macula
Source: “Figure 1. in: Ocular Manifestations of Endocarditis” by M.D. Cheima Wathek, InTechOpen, licensed under CC BY 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
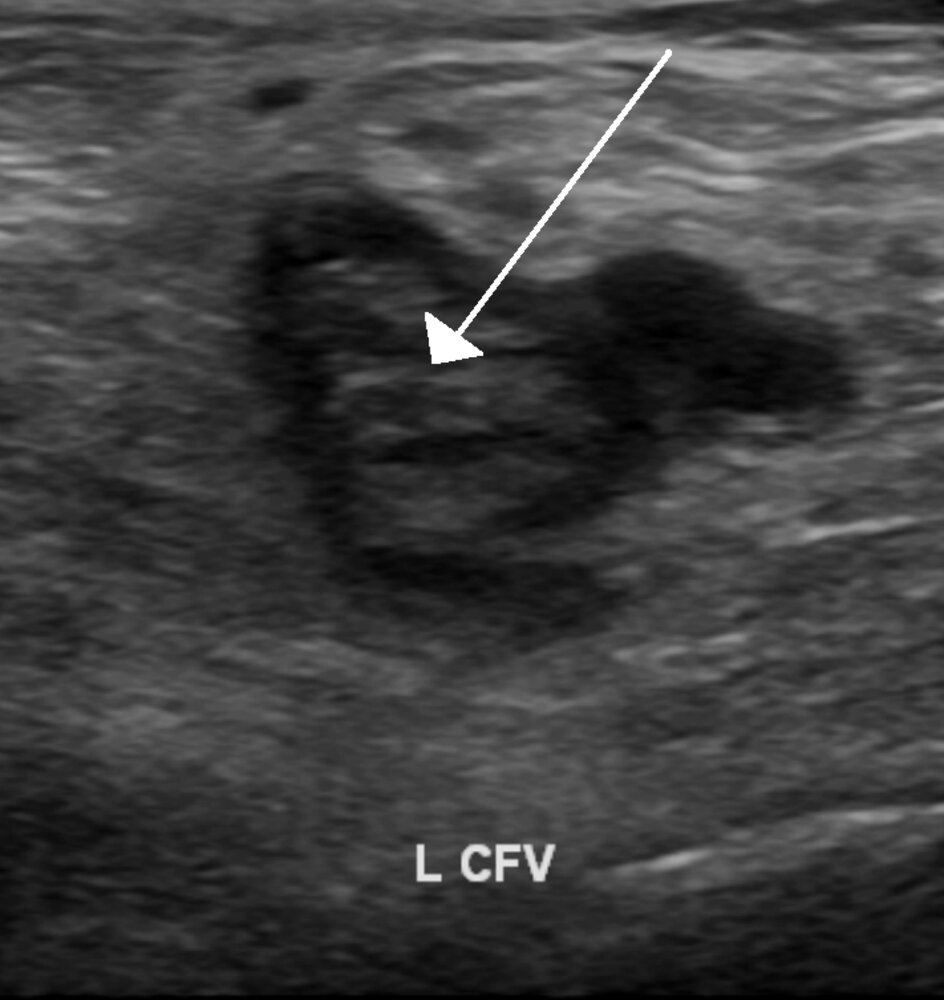
Ultrasound (left common femoral vein; B-mode image; transverse plane)
A hyperechoic thrombus is seen in the lumen of the vein (arrow). The vein could not be compressed with the transducer.
The ultrasound findings are consistent with venous thrombosis. Of note, the presence of blood flow can be assessed by duplex and color Doppler ultrasonography (not shown).
Source: “DVTUS” by James Heilman, MD, Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}
© AMBOSS
© AMBOSS
© AMBOSS. Image source: Fig. 3, in "Physiological Manifestation in Pulmonary Sarcoidosis" by Watanabe K; IntechOpen; 2013; licensed under CC BY 3.0; https://www.intechopen.com/chapters/43575; image cropped, arrows added
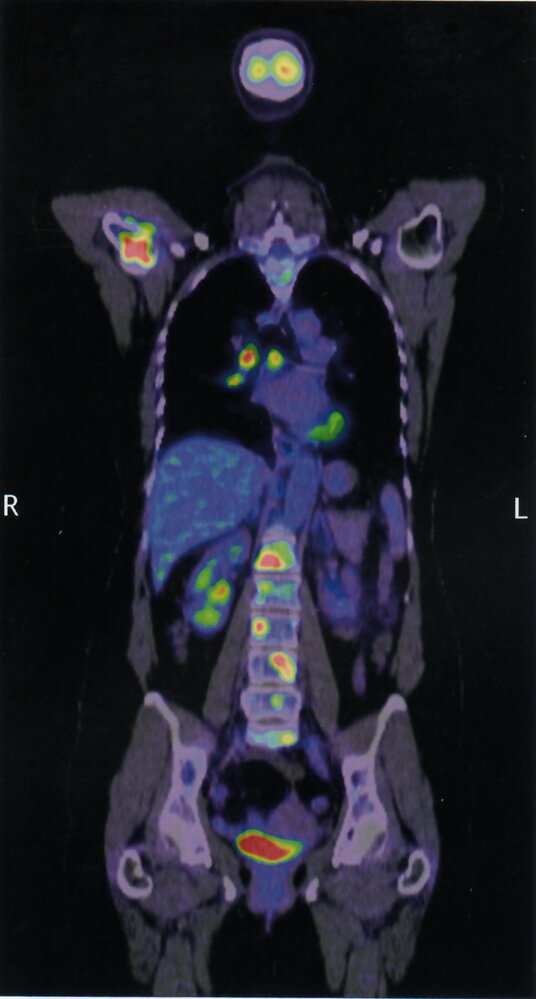
PET-CT (coronal plane)
Intense tracer uptake indicating metastatic disease is present in lumbar vertebrae (green overlay), the right humeral head (blue overlay), and the mediastinal and right hilar lymph nodes (red overlay). The tracer accumulation in the bladder is normal (hatched green overlay).
Source: © IMPP
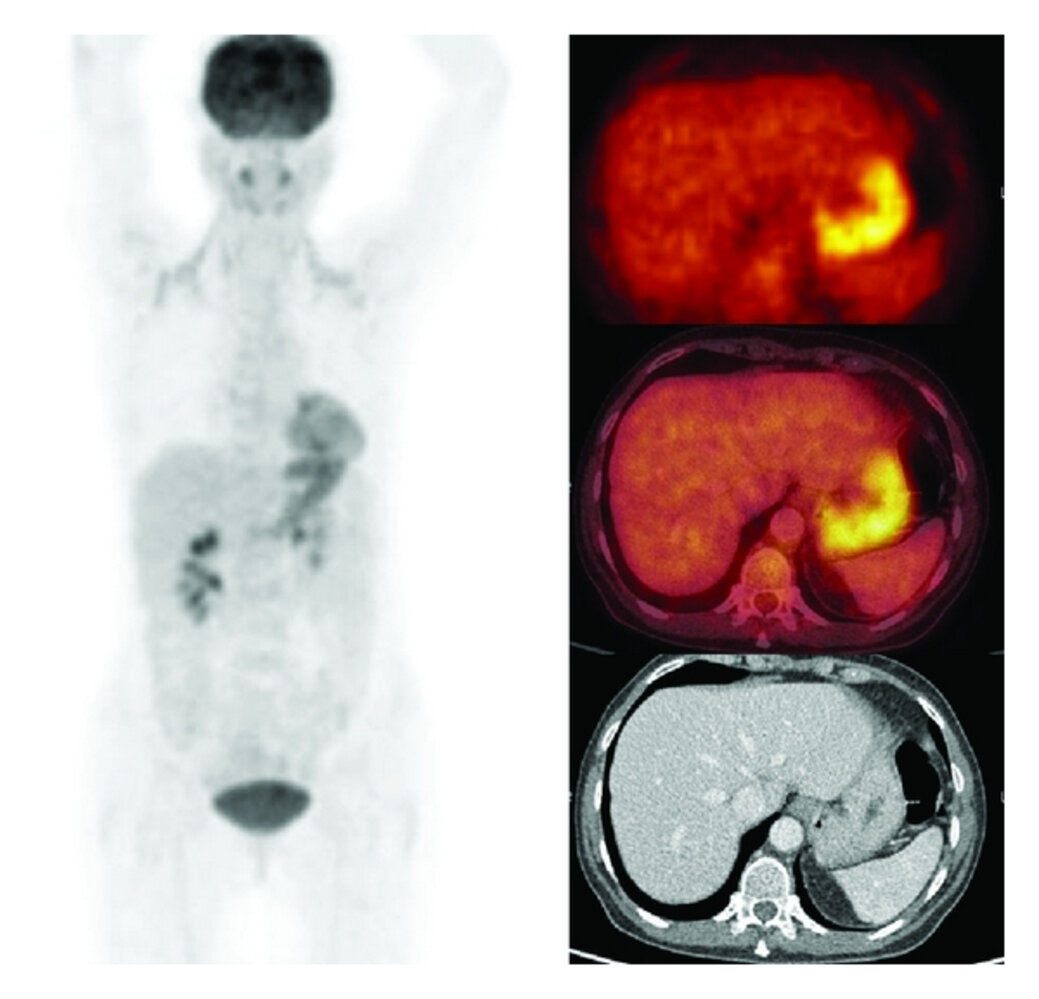
F18-FDG-PET/CT (left: coronal plane; right: axial planes) of a patient with inflammation of unknown origin (IUO)
High uptake is seen in the gastric wall (arrowheads in upper and middle right images). Gastrostomy revealed gastritis with superficial ulcerations. CT thorax and abdomen performed prior to PET/CT were normal.
K: kidneys; B: bladder; H: heart; L: liver; St: stomach; Sp: spleen
Source: “Figure 1: A Rationale for the Use of F18-FDG PET/CT in Fever and Inflammation of Unknown Origin, in: International Journal of Molecular Imaging” by H. Balink, H. J. Verberne, R. J. Bennink, B. L. F. van Eck-Smit, International Journal of Molecular Imaging, licensed under CC BY 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
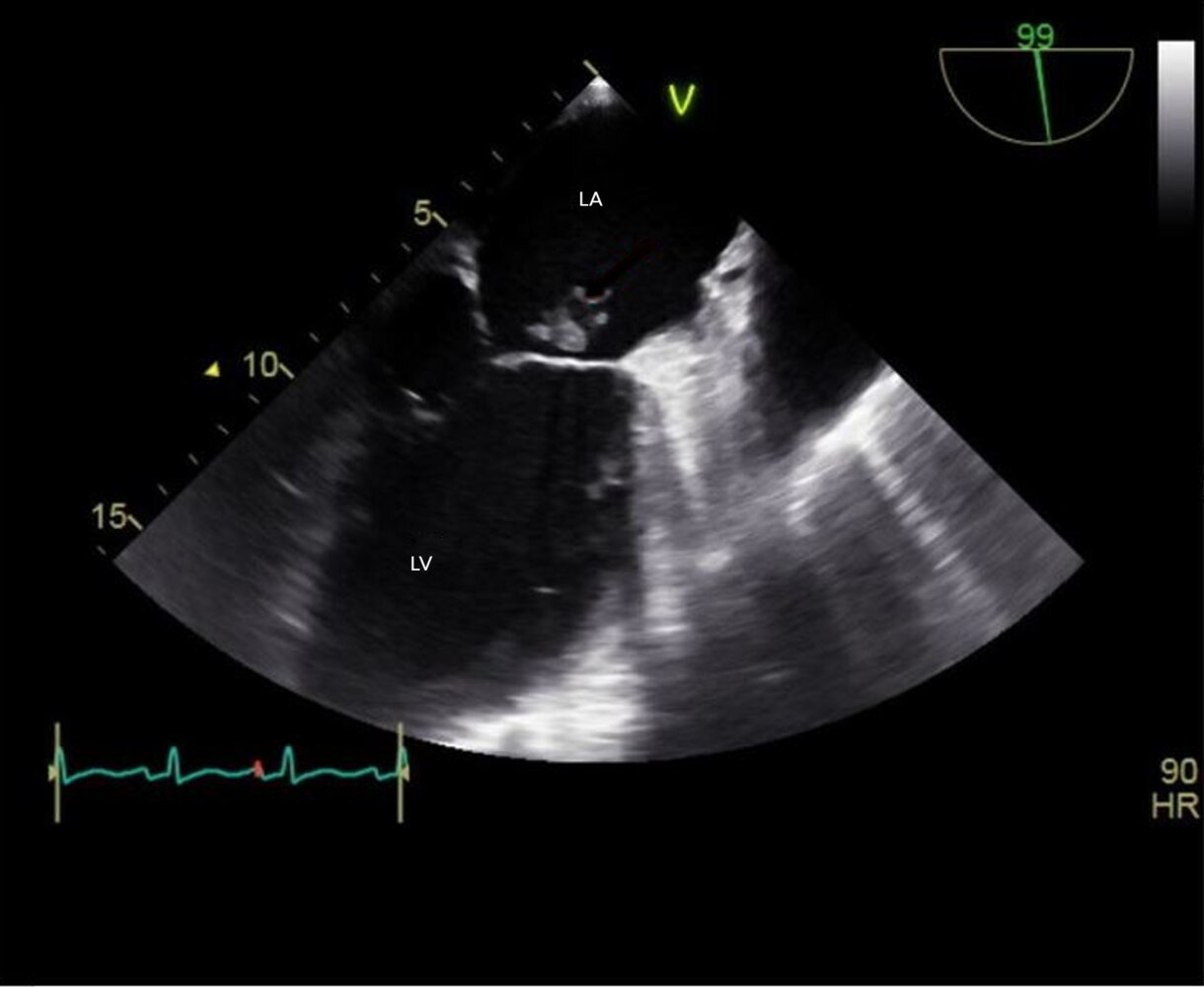
Echocardiography (transesophageal; mid esophageal two-chamber view)
An irregularly shaped vegetation (red overlay) is seen on the mitral valve (green overlay).
LA: left atrium; LV: left ventricle
Source: “Figure 1, in: Infective Endocarditis Manifesting as Severe Elevation in Serum Aminotransferases in the Absence of Severe Tricuspid Regurgitation, Heart Failure, or Shock: A Diagnostic Challenge” by Amaratunga E A, Hoggard J A, Kamau J, Ernst E B, Chalunkal M, Snyder R, Cureus, licensed under CC BY 4.0. Modifications: -Image was cropped, letter "A" in the top left corner was removed -FXV: Red arrow removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
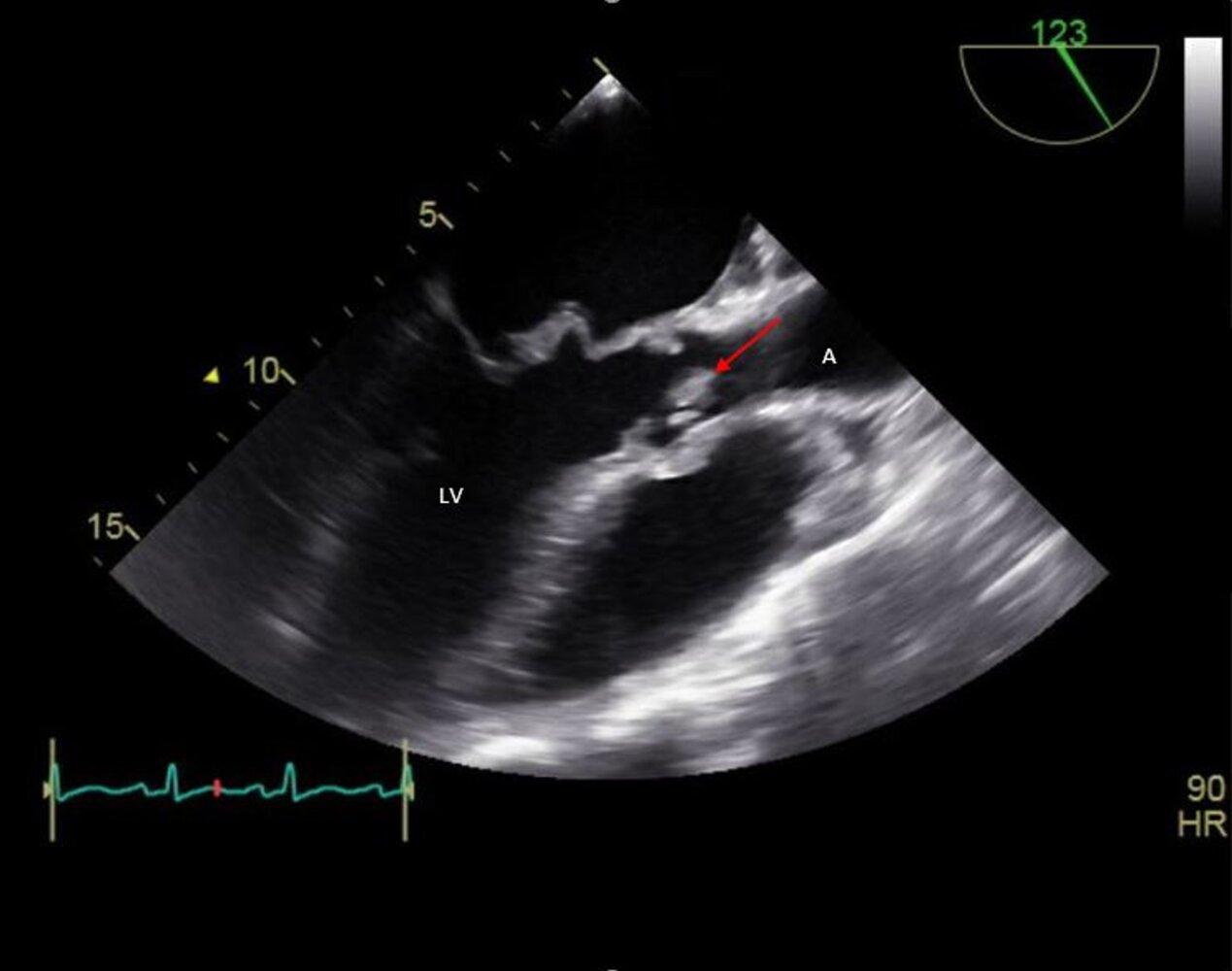
Echocardiography (transesophageal; mid esophageal long axis view)
A vegetation (red arrow) is seen as an echogenic structure on the right coronary cusp (green overlay) of the aortic valve.
A: aorta; LA: left atrium; LV: left ventricle; RV: right ventricle
Source: “Figure 1, in: Infective Endocarditis Manifesting as Severe Elevation in Serum Aminotransferases in the Absence of Severe Tricuspid Regurgitation, Heart Failure, or Shock: A Diagnostic Challenge” by Amaratunga E A, Hoggard J A, Kamau J, Ernst E B, Chalunkal M, Snyder R, Cureus, licensed under CC BY 4.0. Modifications: Image was cropped, letter "B" in the top left corner and letter "V" were removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
Treatment
General principles [1][4][24]
- Avoid antipyretics if feasible.
- Avoid empiric therapy (e.g., antibiotics, glucocorticoids) unless there is rapid clinical deterioration or if a life-threatening etiology is suspected.
- If the underlying etiology remains undiagnosed and FUO persists despite advanced diagnostics:
- Specialist consultation (e.g., infectious diseases, rheumatology, oncology, and/or hematology) is advised.
- Consider a trial of anakinra in patients with a suspected autoinflammatory condition and rapid clinical deterioration. [4][25]
- Once a likely cause has been identified, manage accordingly (see dedicated articles for details).
An infectious etiology is less likely in FUO of prolonged duration.
Role of antipyretics and glucocorticoids [2][3]
-
Antipyretics and glucocorticoids can alter or mask specific features of certain conditions and should be largely avoided unless:
- An infectious etiology and lymphoma have been ruled out
- A potentially debilitating inflammatory etiology (e.g., giant cell arteritis) is suspected
- The patient has significant cardiovascular comorbidities
- If antipyretics are needed, acetaminophen is preferred (see “Antipyretics” for dosages). [2]
- Empiric glucocorticoids should be initiated immediately if temporal arteritis is suspected.
Role of empiric antibiotic therapy [1][3][24]
- Avoid empiric antibiotic therapy in clinically stable and immunocompetent patients.
- Consider empiric antibiotics in the following special populations to prevent rapid deterioration:
- Suspected miliary tuberculosis (e.g., FUO in immunosuppressed individuals): See “Treatment of tuberculosis.”
- Suspected culture-negative infective endocarditis (e.g., prosthetic valve endocarditis): See “Empiric antibiotic therapy for infective endocarditis.”
- Neutropenic FUO: See “Empiric antibiotic therapy for neutropenic fever.”
- Nosocomial FUO: See “Postoperative fever” and “Nosocomial infections.”
- HIV-associated FUO: See “HIV-associated conditions” and “HIV.”
Empiric therapy should only be considered in patients with rapid clinical deterioration, neutropenic fever, giant cell arteritis, or suspected life-threatening underlying etiology (e.g., miliary tuberculosis). [24]
Neutropenic fever is a medical emergency because of the impaired neutrophil-mediated inflammatory response to bacterial infections. Initiate empiric antibiotic therapy immediately after drawing blood and urine cultures.
Prognosis
Prognosis depends on the underlying cause.
- Spontaneous remission of fever occurs in ∼ 40% of patients. [11]
- Mortality rate is ∼ 7% at 5 years (mostly due to malignancy, primarily non-Hodgkin lymphoma) [11][26]
External Resources
References
- Wright WF, Auwaerter PG. "Fever and Fever of Unknown Origin: Review, Recent Advances, and Lingering Dogma". Open Forum Infect Dis. 7(5). (2020)
- Hersch EC, Oh RC. "Prolonged febrile illness and fever of unknown origin in adults". Am Fam Physician. 90(2). :91-6. (2014)
- Bleeker-Rovers CP, Vos FJ, de Kleijn EMHA, et al. "A Prospective Multicenter Study on Fever of Unknown Origin". Medicine. 86(1). :26-38. (2007)
- Mulders-Manders C, Simon A, Bleeker-Rovers C. "Fever of unknown origin". Clin Med. 15(3). :280-4. (2015)
- Roth AR, Basello GM. "Approach to the Adult Patient with Fever of Unknown Origin". Am Fam Physician. 68(11). :2223-2229. (2003)
- Cunha BA, Lortholary O, Cunha CB. "Fever of Unknown Origin: A Clinical Approach". Am J Med. 128(10). :1138.e1-1138.e15. (2015)
- Schüttrumpf S, Binder L, Hagemann T, et al. "Procalcitonin: a useful discriminator between febrile conditions of different origin in hemato-oncological patients?". Ann Hematol. 82(2). :98-103. (2003)
- Mulders-Manders CM, Engwerda C, Simon A, van der Meer JWM, Bleeker-Rovers CP. "Long-term prognosis, treatment, and outcome of patients with fever of unknown origin in whom no diagnosis was made despite extensive investigation". Medicine. 97(25). :e11241. (2018)
- Jameson JL, Fauci AS, Kasper DL, et al. "Harrison's Principles of Internal Medicine, Twentieth Edition (Vol.1 & Vol.2)". McGraw-Hill Education / Medical. (2018). ISBN: 9781259644030
- Mourad O, Palda V, Detsky AS. "A Comprehensive Evidence-Based Approach to Fever of Unknown Origin". Arch Intern Med. 163(5). :545. (2003)
- Ziaj S, Mitchell C, Roufosse C, Dubrey S. "Occult microscopic polyangiitis presenting as pyrexia of unknown origin". Br J Hosp Med. 75(3). :172-173. (2014)
- Yosipovitch G. "Chronic pruritus: a paraneoplastic sign". Dermatol Ther. 23(6). :590-596. (2010)
- Schwartz RA, Nervi SJ. "Erythema nodosum: A sign of systemic disease". Am Fam Physician. 75(5). :695-700. (2007)
- Zadeh N, Getzug T, Grody WW. "Diagnosis and management of familial Mediterranean fever: Integrating medical genetics in a dedicated interdisciplinary clinic". Genetics in Medicine. 13(3). :263-269. (2011)
- Kim SE, Kim UJ, Jang MO, et al. "Diagnostic Use of Serum Ferritin Levels to Differentiate Infectious and Noninfectious Diseases in Patients with Fever of Unknown Origin". Dis Markers. 34(3). :211-218. (2013)
- Takeuchi M, Dahabreh IJ, Nihashi T, et al. "Nuclear Imaging for Classic Fever of Unknown Origin: Meta-Analysis". J Nucl Med. 57(12). :1913-1919. (2016)
- Kotsiri I, Panotopoulos C, Magiorkinis E. "The Role of PET/CT in the Investigation of Fever of Unknown Origin". J Adv Med Med Res. :71-82. (2020)
- Kaya A, Ergul N, Kaya SY et al. "The management and the diagnosis of fever of unknown origin". Expert Rev Anti Infect Ther. 11(8). :805-815. (2014)
- Sekar P, Johnson JR, Thurn JR, et al. "Comparative Sensitivity of Transthoracic and Transesophageal Echocardiography in Diagnosis of Infective Endocarditis Among Veterans With Staphylococcus aureus Bacteremia". Open Forum Infect Dis. 4(2). (2017)
- Reynolds HR, Jagen MA, Tunick PA, Kronzon I. "Sensitivity of transthoracic versus transesophageal echocardiography for the detection of native valve vegetations in the modern era". Journal of the American Society of Echocardiography. 16(1). :67-70. (2003)
- De Kleijn EMHA, van Lier HJJ, van der Meer JWM. "Fever of unknown origin (FUO): II. Diagnostic procedures in a prospective multicenter study of 167 patients". Medicine. 76(6). :401-414. (1997)
- Sipahi OR, Senol S, Arsu G, et al. "Pooled analysis of 857 published adult fever of unknown origin cases in Turkey between 1990-2006". Med Sci Monit. 13(7). :CR318-22. (2007)
- Foggo V, Cavenagh J. "Malignant causes of fever of unknown origin". Clin Med. 15(3). :292-4. (2015)
- Bryan CS, Ahuja D. "Fever of Unknown Origin: Is There a Role for Empiric Therapy?". Infect Dis Clin North Am. 21(4). :1213-1220. (2007)
- Harrison SR, McGonagle D, Nizam S, et al. "Anakinra as a diagnostic challenge and treatment option for systemic autoinflammatory disorders of undefined etiology". JCI insight. 1(6). :e86336. (2016)
- Vanderschueren S, Eyckmans T, De Munter P, Knockaert D. "Mortality in patients presenting with fever of unknown origin". Acta Clin Belg. 69(1). :12-16. (2014)