Summary
Folate deficiency is most commonly caused by malnutrition, e.g., in individuals with insufficient dietary intake or alcohol use disorder. Patients typically present with signs of anemia (e.g., fatigue). Initial laboratory studies show macrocytic anemia, circulating megaloblasts, and, in some cases, pancytopenia. Low fasting serum folate levels confirm the diagnosis, but sensitivity is limited; if levels are normal, RBC folate or plasma homocysteine testing should be performed. Treatment of folate deficiency consists of oral folate replacement and increasing dietary intake of folate-rich foods (e.g., leafy green vegetables, fruits, and fortified foods).
Physiology
-
Folate: coenzyme in single-carbon transfers and methylation reactions → DNA synthesis and amino acid metabolism [1]
- Active form: tetrahydrofolate (THF), obtained after reduction of folate by dihydrofolate reductase
- Sources: folate-rich foods
- Absorption: in the jejunum
- Storage: liver (stores folate for up to three months, after which time signs and symptoms of deficiency begin to appear)
Etiology
-
Malnutrition
- Insufficient intake (e.g., “tea and toast” diet)
- Alcohol use disorder
-
Malabsorption
- Small bowel disease (e.g., tropical sprue, celiac disease, inflammatory bowel disease)
- Surgical procedures (e.g., resection of the small intestine, gastric bypass)
-
Increased requirement
- Pregnancy or lactation
- Severe hemolytic anemia
- Exfoliative skin disease (e.g., eczema) [2][3]
-
Medication-related [4]
- Methotrexate
- Antiepileptic drugs (e.g., phenytoin)
- Sulfonamides
- Trimethoprim
Pathophysiology
Decreased folate levels lead to decreased levels of tetrahydrofolate. This, in turn, leads to the following effects:
- ↓ DNA synthesis → megaloblastic erythropoiesis → megaloblastic anemia (and ↓ in other cell lines)
- ↓ Methionine and ↑ homocysteine → endothelial damage → ↑ risk of cardiovascular disease and thromboembolic events
- During fetal development: nucleotide synthesis impairment → neural tube defects
- Aberrant DNA methylation → ↑ risk of cancer [5][6]

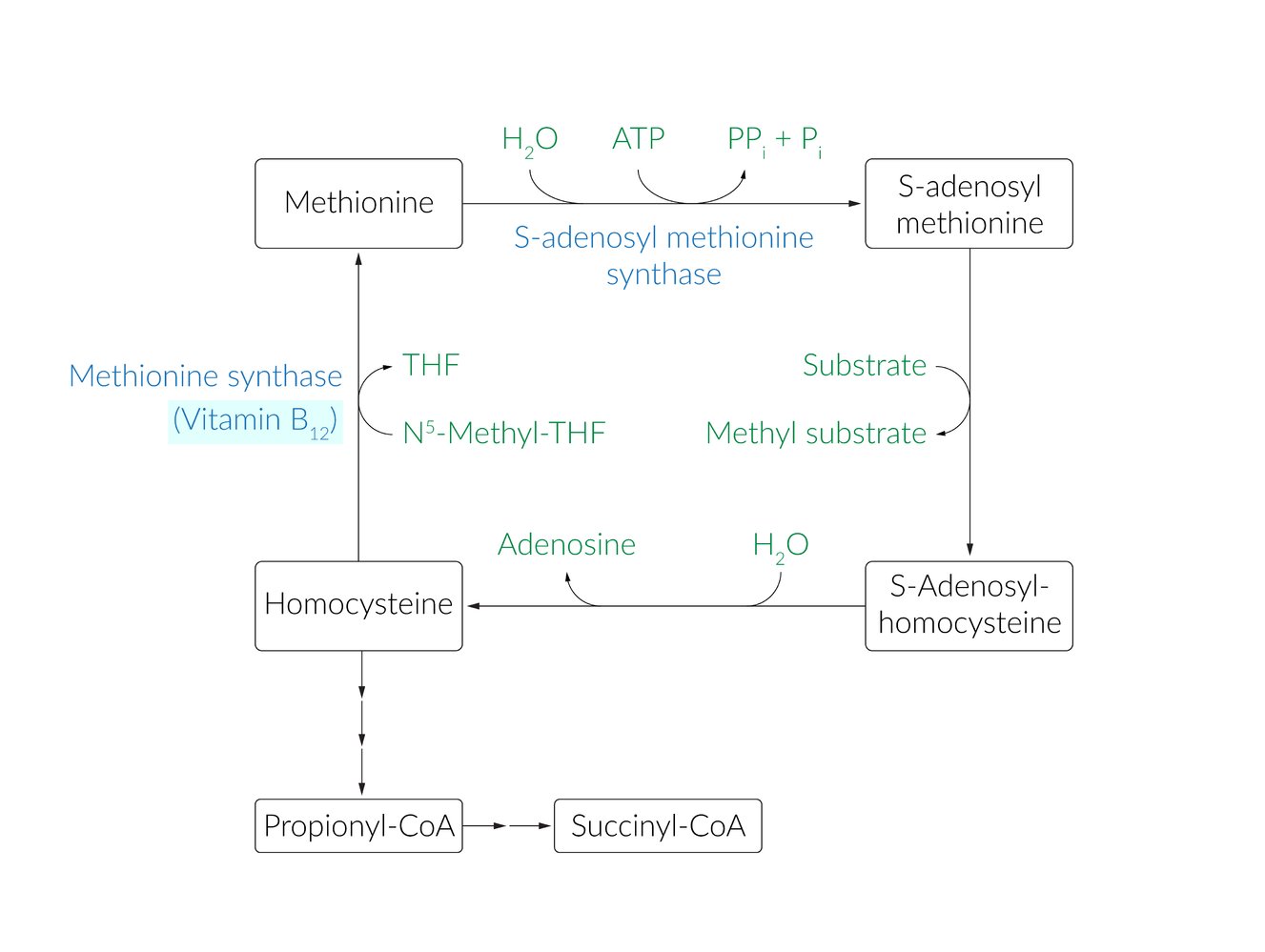
Methionine is an essential amino acid that generates sulfur-containing amino acids (i.e., cysteine, homocysteine, and taurine) as well as S-adenosyl methionine (SAM), a coenzyme of several methylation reactions, through the methionine cycle.
ATP donates adenosine to methionine, converting it to SAM. SAM then loses its methyl group to form S-adenosylhomocysteine, which loses its adenosine molecule to form homocysteine. Homocysteine can then enter three pathways: It can be converted to succinyl CoA (which enters the citric acid cycle), cysteine (from which taurine is generated; not shown here), or back to methionine. Methionine synthase catalyzes the regeneration of methionine from homocysteine in the presence of vitamin B12 and N5-methyltetrahydrofolate (N5-methyl-THF).
© AMBOSS
Clinical features
- Signs of anemia (e.g., fatigue, pallor)
- Glossitis
- Maternal deficiency: fetal spina bifida or anencephaly
Unlike vitamin B12 deficiency, folate deficiency does not typically cause neurological symptoms; rarely, neuropsychiatric conditions (e.g., cognitive impairment, depression) or peripheral neuropathy can occur. [7][8]
Diagnosis
Initial studies [3]
- Evaluate CBC and morphology.
- CBC: macrocytic anemia (MCV > 100 μm3)
- Peripheral blood smear: oval macrocytes, circulating megaloblasts; , and hypersegmented neutrophils
-
Rule out vitamin B12 deficiency.
- Vitamin B12 level
- Methylmalonic acid (MMA): normal in folate deficiency [9]
In folate deficiency, MMA is normal; in vitamin B12 deficiency, MMA is elevated.
Diagnostic confirmation [2][3]
- Fasting serum folate level (first line): < 3 ng/mL (limited sensitivity) [2][3][10]
- If folate level is normal, obtain either:
- Plasma homocysteine: ↑ (sensitive, but not specific)
- RBC folate: ↓
Additional evaluation
Consider further assessment based on the suspected underlying cause.
- Assessment of nutritional status
- Diagnostics for malabsorption
- Diagnostics for celiac disease
- Diagnostics for alcohol use disorder
Treatment
-
Initiate folate replacement in patients with confirmed folate deficiency. [2][3]
- Folic acid
- Duration of treatment depends on the underlying cause.
- Encourage consumption of folate-rich foods, e.g., leafy green vegetables, fruits, and fortified foods.
- Manage the underlying condition.
- See also “Folic acid supplementation in pregnancy.”
In combined vitamin B12 and folate deficiency, folate replacement without vitamin B12 may exacerbate neurological symptoms. Rule out vitamin B12 deficiency before starting folate replacement. [11]
Folic acid supplementation is recommended for all individuals planning or capable of pregnancy because of the risk of neural tube defects due to maternal folate deficiency. [12]
Prevention
-
Prevention of folate deficiency includes:
- Adequate dietary intake of folate-rich foods in all individuals
- Folic acid supplementation in all individuals capable of pregnancy (see “Folic acid supplementation in pregnancy”) [14]
-
Folate-rich foods include:
- Leafy green vegetables
- Fortified foods (e.g., breads, pastas, cereals)
- Legumes
- Fruits (e.g., citrus fruits) [3]
- Other: nuts, eggs, meat [3]
| Recommended dietary intake of folate [13] | |
|---|---|
| Age | Intake |
| 0–6 months | 65 mcg |
| 7–12 months | 80 mcg |
| 1–3 years | 150 mcg |
| 4–8 years | 200 mcg |
| 9–13 years | 300 mcg |
| ≥ 14 years | 400 mcg |
Special patient groups
Folate deficiency in children [3][15][16]
-
Etiology
- Similar to etiology of folate deficiency in adults
- Exclusive consumption of goat's milk or boiled milk during infancy can also cause deficiency.
- Clinical features: similar to the clinical features of folate deficiency in adults
- Diagnosis: similar to the diagnosis of folate deficiency in adults
-
Treatment
- Similar to the treatment of folate deficiency in adults
- Refer to pediatric hematology for further evaluation if there is insufficient response to treatment. [16]
- Prevention: See “Prevention of folate deficiency.”
External Resources
References
- Stanger O. "Physiology of folic acid in health and disease". Curr Drug Metab. 3(2). :211-23. (2002)
- Devalia V, Hamilton MS, Molloy AM. "Guidelines for the diagnosis and treatment of cobalamin and folate disorders". Br J Haematol. 166(4). :496-513. (2014)
- Socha DS, DeSouza SI, Flagg A, Sekeres M, Rogers HJ. "Severe megaloblastic anemia: Vitamin deficiency and other causes". Cleve Clin J Med. 87(3). :153-164. (2020)
- Bebel Stargrove M, Treasure J, McKee DL. "Herb, Nutrient, and Drug Interactions, Clinical Implications and Therapeutic Strategies". Elsevier. (2008). ISBN: 9780323029643
- "Folate and Cancer Risk - Position Statement". https://www.cancercouncil.com.au/35607/cancer-prevention/diet-exercise/nutrition-diet/other-foods-nutrients/folate-and-cancer-risk-position-statement/
- Vollset SE, Clarke R, Lewington S, et al. "Effects of folic acid supplementation on overall and site-specific cancer incidence during the randomised trials: meta-analyses of data on 50 000 individuals". The Lancet. 381(9871). :1029-1036. (2013)
- Reynolds EH. "The neurology of folic acid deficiency". Elsevier. :927-943. (2014). ISBN: 9789356963696
- Ansari R, Mahta A, Mallack E, Luo JJ. "Hyperhomocysteinemia and Neurologic Disorders: a Review". J Clin Neurol. 10(4). :281-288. (2014)
- Green R. "Vitamin B12 deficiency from the perspective of a practicing hematologist". Blood. 129(19). :2603-2611. (2017)
- Snow CF. "Laboratory Diagnosis of Vitamin B12 and Folate Deficiency". Arch Intern Med. 159(12). :1289. (1999)
- Green R, Allen LH, Bjørke-Monsen AL, et al. "Vitamin B12 deficiency". Nat Rev Dis Primers. 3(1). (2017)
- Bibbins-Domingo et al. "Folic Acid Supplementation for the Prevention of Neural Tube Defects". JAMA. 317(2). :183-189. (2017)
- Gallagher PG. "Anemia in the pediatric patient". Blood. 140(6). :571-593. (2022)
- Raleigh MF, Yano AS, Shaffer NE. "Anemia in Infants and Children: Evaluation and Treatment". Am Fam Physician. 110(6). :612-620. (2024)
- Institute of Medicine, Food and Nutrition Board. "Dietary Reference Intakes for Thiamin, Riboflavin, Niacin, Vitamin B6, Folate, Vitamin B12, Pantothenic Acid, Biotin, and Choline". National Academies Press. (1998). ISBN: 0309064112
- Barry MJ, Nicholson WK, et al. "Folic Acid Supplementation to Prevent Neural Tube Defects". JAMA. 330(5). :454. (2023)