Summary
Food poisoning is a specific subset of foodborne illnesses and is caused by the ingestion of any substance that is contaminated with a preformed toxin. Symptoms usually occur within hours of ingesting contaminated food and resolve over the course of 1–2 days. Common clinical features include nausea, vomiting, diarrhea, and abdominal cramping. Diagnostic testing is usually not required unless the symptoms are severe, prolonged, or systemic, e.g., high fever or severe dehydration. Most cases of food poisoning are self-limited and require only supportive care (e.g., oral and/or parenteral rehydration and antiemetics) to ensure adequate hydration. Young children, immunocompromised individuals, and older adults are at greater risk for developing complications related to food poisoning and may require close monitoring. Seafood poisoning may involve more dangerous toxins and additional treatment from antihistamines to cardiopulmonary resuscitation may be required.
For a general overview of all foodborne illnesses, see “Overview of foodborne illnesses,” for an overview of all infectious gastroenteritis types, see “Infectious gastroenteritis.”
Definitions
-
Food poisoning: a type of foodborne illness caused by the ingestion of toxins produced by bacteria in food prior to consumption [1][2][3]
- Toxin-producing bacteria: e.g., Staphylococcus aureus, Clostridium perfringens, Bacillus cereus
- Marine toxins: scombroid fish poisoning, ciguatera fish poisoning, puffer fish poisoning [4]
Clostridium botulinum is a rare and potentially fatal cause of food poisoning. See botulism for details.
Overview of foodborne diseases
Foodborne illness refers to any disease following ingestion of contaminated food. Contaminants include infectious (e.g., bacteria, viruses) and noninfectious agents (e.g., pesticides, food additives, allergens, mushroom poisoning, metal toxicity). An overview of infectious foodborne illnesses classified according to the predominating symptoms is provided here. For details on bacterial pathogens, see the article on bacterial gastroenteritis. [1][2][3][5]
Predominantly vomiting
Pathophysiology: Vomiting is commonly due to delayed gastric emptying caused by changes to gastric motility.
| Overview of pathogens predominantly causing vomiting | |||
|---|---|---|---|
| Pathogen | Foods/transmission | Incubation period | Treatment |
| Staphylococcus aureus |
|
|
|
| Bacillus cereus |
|
|
|
| Noroviruses (e.g., Norwalk virus) [6] |
|
|
|
Symptom onset and resolution are quick in S. aureus and B. cereus poisoning: S. aureus and B. cereus are fast and fureus.
Predominantly diarrhea
Watery diarrhea [7]
- Pathophysiology: enterotoxin or bacterial invasion shifts water and electrolyte excretion/absorption in proximal small intestine → watery diarrhea
-
Clinical features
- Mild–moderate: abdominal pain, diarrhea
- Severe
- Tachycardia, hypotension
- Fever
- Bloody or profuse watery diarrhea
- Metabolic acidosis
-
Diagnostics: stool tests
- WBC negative
- No blood
| Overview of pathogens predominantly causing watery diarrhea | |||
|---|---|---|---|
| Pathogen | Foods/transmission | Incubation period | Treatment |
| Staphylococcus aureus |
|
|
|
| Clostridium perfringens [8][9] (Heat-labile enterotoxins cause the symptoms.) |
|
|
|
| Enterotoxic Escherichia coli (ETEC) [10] (Heat-labile toxin induces diarrhea; most common cause of traveler's diarrhea) |
|
|
|
| Listeria monocytogenes |
|
|
|
| Vibrio cholerae |
|
|
|
| Enteric viruses (adenovirus, norovirus, rotavirus) |
|
|
|
| Cryptosporidium [11] |
|
|
|
| Cyclospora (Cryptosporidium cyclospora cayetanensis) [12][13] |
|
|
|
| Intestinal tapeworms |
|
|
|



Invasive diarrhea [14][15][16]
- Pathophysiology: penetration of mucosa and subsequent invasion of reticuloendothelial system in the distal small intestine → enteric fever
-
Diagnostics: stool tests
- WBC positive (fecal mononuclear leukocytes)
- Blood may be present.
| Overview of pathogens predominantly causing invasive diarrhea | |||
|---|---|---|---|
| Pathogen | Foods/transmission | Incubation period | Treatment |
| Salmonella typhi or paratyphi |
|
|
|
| Yersinia |
|
|
|
Inflammatory diarrhea [14][15][17]
- Pathophysiology: damage to the colonic mucosa → blood in stool, fever
-
Diagnostics: stool tests
- WBC positive (fecal polymorphonuclear leukocytes)
- Blood present
| Overview of pathogens predominantly causing inflammatory diarrhea | ||||
|---|---|---|---|---|
| Pathogen | Association | Foods/transmission | Incubation period | Treatment |
| Salmonella (hundreds of strains, including S. enteritidis and S. typhimurium) |
|
|
|
|
| Campylobacter jejuni |
|
|
|
|
| Shigella dysenteriae |
|
|
|
|
| Yersinia enterocolitica |
|
|
|
|
| Vibrio (usually parahaemolyticus) [18][19] |
|
|
|
|
| Enterohemorrhagic Escherichia coli (EHEC) [10] |
|
|
|
|
Additional nongastrointestinal symptoms
| Pathogens | Predominating symptoms | Foods/Transmission | Incubation period | Treatment |
|---|---|---|---|---|
| Clostridium botulinum |
|
|
|
|
| Histamine fish poisoning |
|
|
|
|
| Brucellosis (Brucella spp.) [20] |
|
|
|
|
| Hepatitis A (Hepatitis A virus) [23] |
|
|
|
|
| Vibrio vulnificus [24][25] |
|
|
|
|
| Salmonella typhi and paratyphi |
|
|
|
|
| Ciguatoxin |
|
|
|
|
Common sources of fecal-oral transmission in intestinal diseases are the 5 F's: fingers, feces, food, fluids, flies.
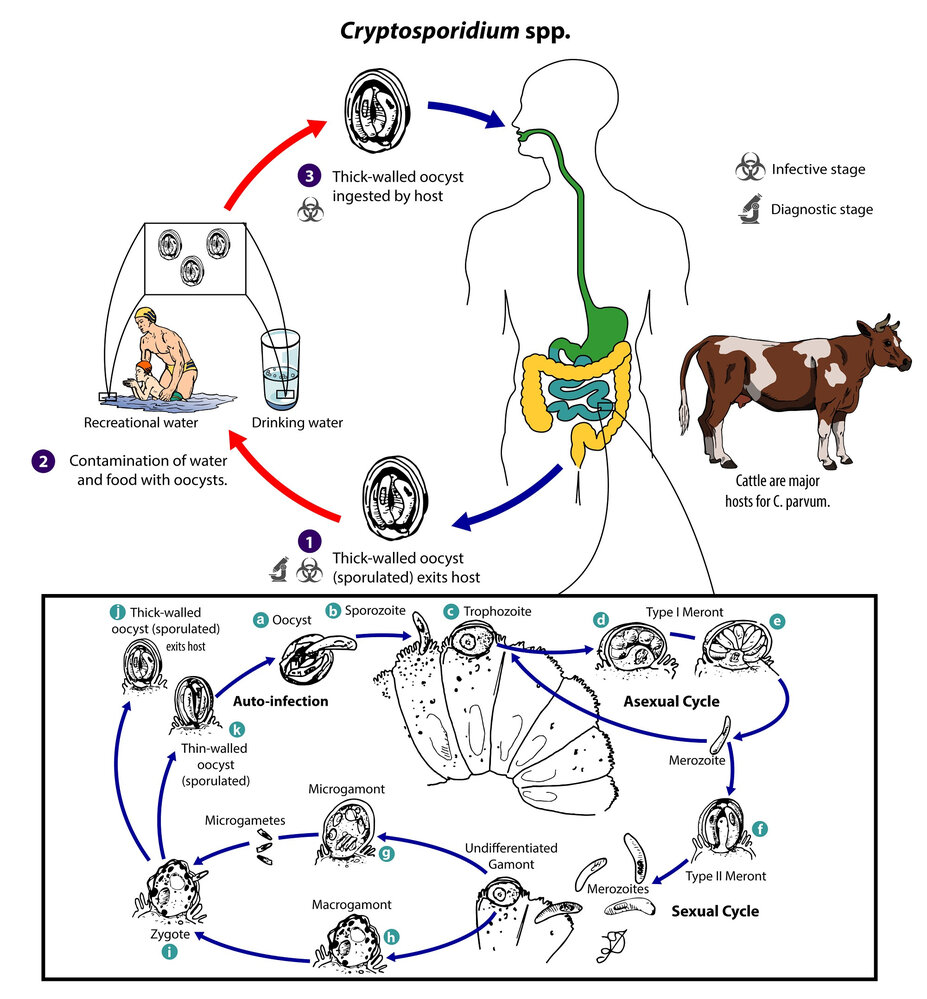
1. Diagnostic/infective stage: An infected host (e.g., cattle, humans) sheds thick-walled oocysts containing 4 sporozoites each via the feces and possibly other routes (e.g., respiratory secretions).
2. Oocysts contaminate food and water.
3. Infective stage: Infection occurs via ingestion or, possibly, inhalation of contaminated material following direct contact with infected hosts or exposure to contaminated (recreational or drinking) water or foods (e.g., raw milk).
Reproductive cycle (box): Following infection, the sporozoites excyst from the oocyte (a) and colonize epithelial cells of the gastrointestinal and, possibly, respiratory tract, where they develop into trophozoites (c). Here, the trophozoites undergo asexual multiplication through fission (merogony; d), resulting in 8 merozoites within a type I meront (e) or 4 merozoites within a type II meront (f). The meronts rupture and release the merozoites into the intestinal lumen, where they undergo further cycles of merogony, resulting in additional merozoites, or sexual multiplication (gametogony) and form undifferentiated gamonts that develop into microgamonts (g; male) containing 16 non-flagellated microgametes or macrogamonts (h; female). Upon release from the microgamonts, the microgametes fertilize the macrogamonts, leading to the development of zygotes (i) within a thick- or thin-walled oocyte and subsequent sporulation of the zygote. Thick-walled oocysts are excreted by the host with the feces (j), while thin-walled oocysts remain within the host and enter into an autoinfective cycle (k).
This image is an adaptation. Source of original image: CDC/ DPDx. Original title: “Cryptosporidium spp.”. Created by: CDC/ DPDx. Licensed under Public Domain. Modifications to original image: CDC/DPDx logo removed by request.
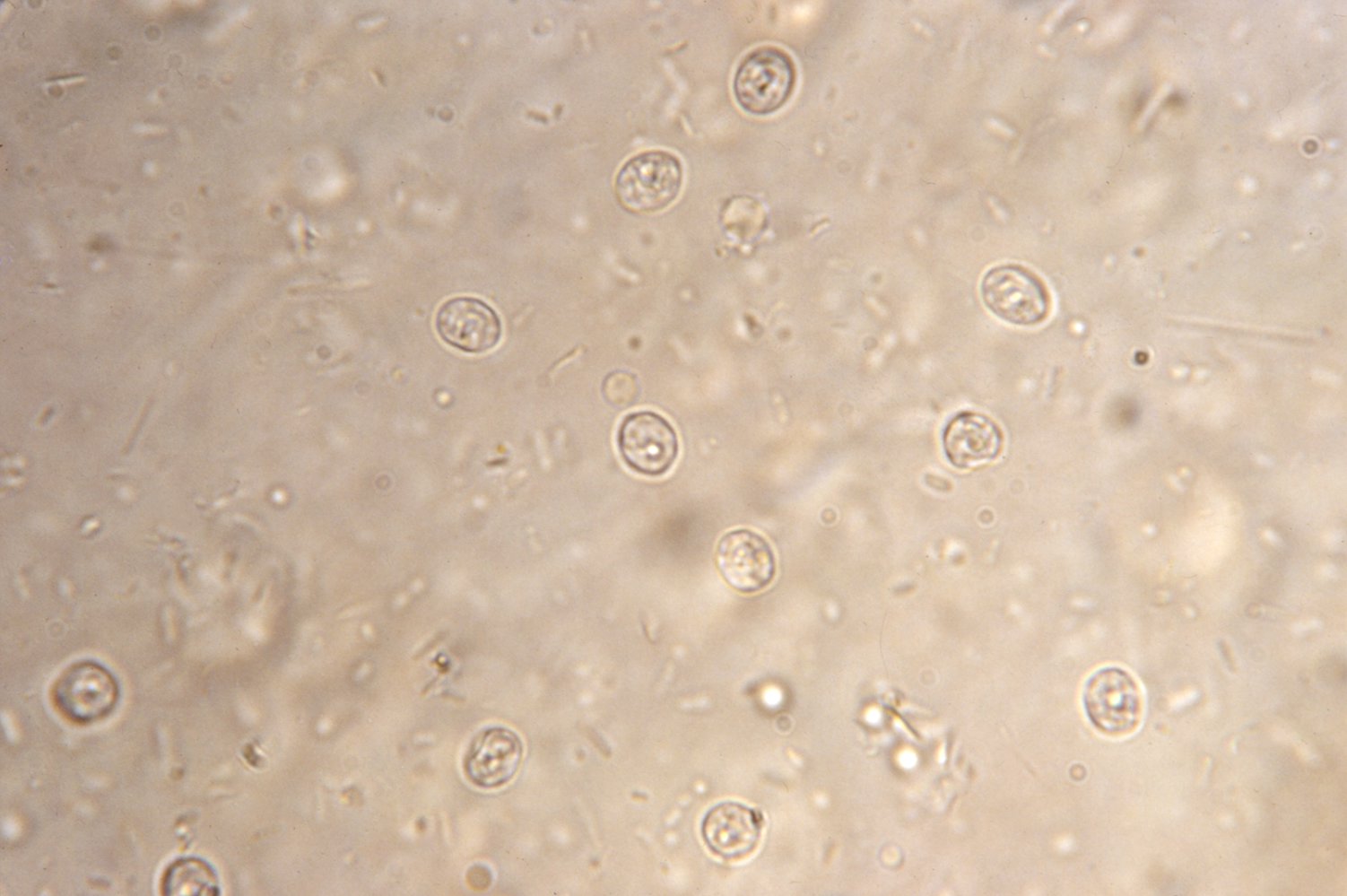
Fecal sample of a patient with cryptosporidiosis
Several round oocysts (red) that contain a large number of sporozoites. Oocysts are highly resistant to environmental factors and disinfectants (also to chlorine, e.g., in drinking water). They are the infective form of the parasite Cryptosporidium parvum.
Source: "ID#: 4384", CDC/ Dr. Peter Drotman, Centers for Disease Control and Prevention (CDC) licensed under Public Domain
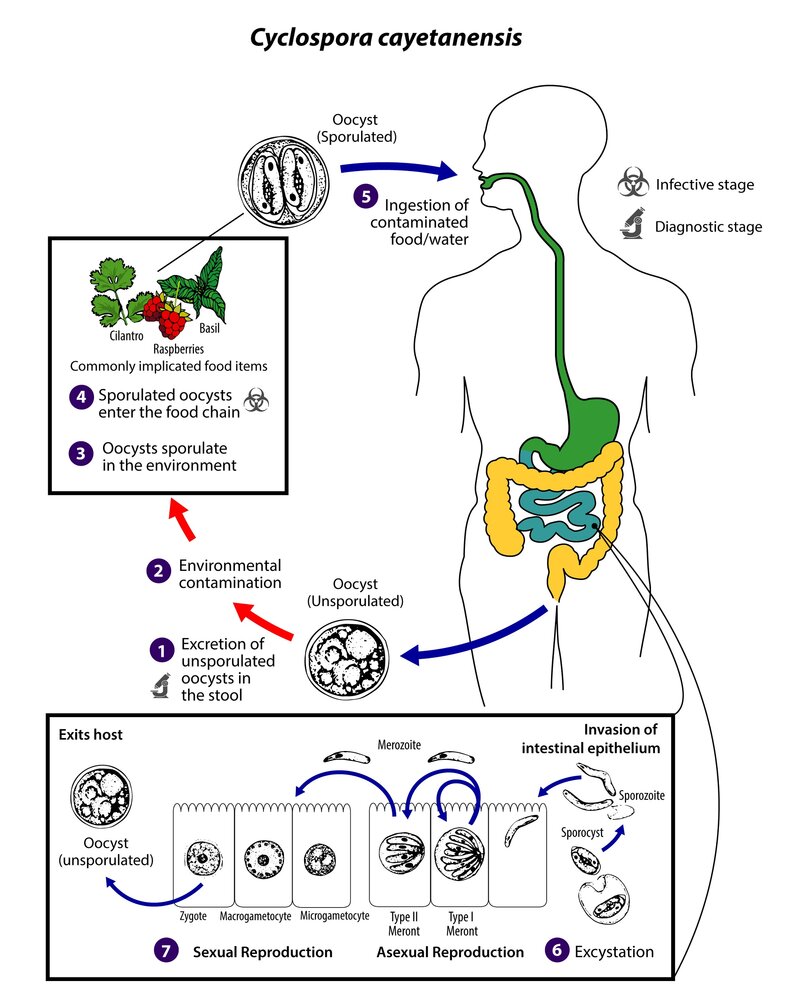
1. Diagnostic stage: Unsporulated oocysts are excreted with the stool of an infected human host (definitive host). Oocytes are not infective, which is why direct fecal-oral transmission is not possible.
2. Contaminated stools contaminate the environment.
3. Oocysts sporulate and the sporont divides into two sporocysts, with each containing two sporozoites. The oocysts are now infective.
4. Infective stage: Sporulated oocytes enter the food chain.
5. Ingestion of sporulated oocytes with contaminated food or water.
6. Sporulated oocysts enter the gastrointestinal tract, where they excyst, releasing the sporozoites, which invade the epithelium of the small intestine.
7. Here, they reproduce asexually into type I and type II meronts. Type I meronts produce merozoites that remain in the asexual cycle. Type II meronts produce merozoites that invade other host cells, in which they undergo sexual development into macrogametocytes and microgametocytes. After fertilization, the zygote develops into an oocyst that is released from the host cell into the intestine and subsequently passed with the stool.
This image is an adaptation. Source of original image: CDC/ DPDx. Original title: “Cyclospora cayetanensis”. Created by: CDC/ DPDx. Licensed under Public Domain. Modifications to original image: CDC/DPDx logo removed by request.
Management of food poisoning
-
Diagnostics
- Testing for presence of toxins is not routinely done. [5][15]
- Patients with severe symptoms (e.g., severe gastroenteritis, red flags of diarrhea): Follow “Diagnostics for infectious gastroenteritis.”
-
Treatment: mostly supportive as disease course is short-lived (∼ 24 hours) [5][15]
- Oral rehydration therapy for mild to moderate dehydration
- IV fluid resuscitation for moderate to severe dehydration
- Antiemetics, e.g., ondansetron
- See “Supportive therapy for gastroenteritis” for details.
-
Disposition
- Consider hospital admission for patients who are severely dehydrated, unable to tolerate oral liquids, and/or have severe symptoms. [15]
- Report cases of food poisoning to public health authorities per local protocol.
Staphylococcal food poisoning
Staphylococcal food poisoning is one of the most common confirmed source of foodborne illness. [26][27]
-
Pathogen: Staphylococcus aureus
- Gram-positive bacterium
- Some strains produce heat-stable staphylococcal enterotoxins that cause food poisoning and, in severe cases, toxic shock syndrome. [1]
-
Transmission
- Ingestion of preformed toxins in contaminated food
- Bacteria proliferate in inadequately refrigerated food (meat, mayonnaise, potato salad, custards).
- While Staphylococcus aureus is destroyed by cooking, the heat-stable enterotoxins are not.
- Onset after ingestion: typically has a short latency period of 1–6 hours [27]
- Duration: 24–48 hours [7]
-
Clinical features
- Severe vomiting (often with sudden onset)
- Abdominal cramping
- Diarrhea
-
Treatment [7][15][27]
- Supportive: Follow management of food poisoning.
- Antibiotics are not indicated in uncomplicated illness.
Clostridium perfringens food poisoning
Clostridium perfringens is the second most common cause of foodborne illness in the United States. [1][28]
- Pathogen: Clostridium perfringens serotype A
- Transmission: ingestion of bacteria that produce enterotoxin in the GI tract [1]
- Onset after ingestion: 7–30 hours
- Duration: 24–48 hours
-
Clinical features
- Abdominal cramping and pain
- Diarrhea
- Vomiting (uncommon)
-
Treatment [5][15][29]
- Follow management of food poisoning.
- Supportive only; antibiotics are not indicated in uncomplicated illness.
Bacillus cereus infection
Bacillus cereus can produce two different enterotoxins which cause two distinct food poisoning syndromes. [1][7]
- Pathogen: Bacillus cereus, a heat-stable, spore-forming gram-positive rod
- Transmission: ingestion of bacteria growing in heated food that is improperly refrigerated
-
Emetic form [30]
- A heat-stable toxin (cereulide) is produced by bacteria in food and survives cooking.
- Commonly associated with reheated rice: Spores survive the cooking process, germinate in warm rice, and produce more enterotoxin.
- Onset after ingestion: 1–3 hours
- Duration: 6–24 hours
- Clinical features: Nausea and vomiting predominate.
-
Diarrheal form
- A thermolabile toxin is produced by organisms during the growth phase in the intestine.
- Associated with a broad range of food, e.g., meat, vegetables, milk products
- Onset after ingestion: 8–16 hours
- Duration: 12–24 hours
- Clinical features: abdominal pain, diarrhea, nausea
-
Treatment: both forms [5][15]
- Supportive: Follow management of food poisoning.
- Antibiotics are not effective against toxins.
Poisoning from reheated rice can be serious (B. cereus).
Seafood poisoning
Histamine fish poisoning (scombroid poisoning) [2][15][31]
- Transmission: ingestion of contaminated, inadequately refrigerated dark-meat fish, e.g., mackerel, bonito, mahi-mahi, and tuna
- Mechanism of action: Histidine (found in high concentrations in these fish) is converted into histamine by histidine decarboxylase in the bacteria that normally colonize the fish.
- Onset after ingestion: 20–30 minutes
- Duration: 6–8 hours (malaise may last longer)
-
Clinical features: usually mild and self-limited
- Erythema, facial flushing, itching, urticaria
- Burning sensation in the mouth
- Diarrhea, abdominal cramping, vomiting
- Severe headache
- Palpitations
-
Severe reactions (similar to anaphylaxis) are rare but can include:
- Angioedema
- Hypotension
- Bronchospasm and/or respiratory distress
- Diagnosis: usually a clinical diagnosis
-
Treatment [2][15][31]
- All patients: Follow management of food poisoning for supportive treatment.
- Mild symptoms: antihistamines, e.g., diphenhydramine (off-label) [15][31]
- Severe symptoms: epinephrine, bronchodilators, IV fluid resuscitation [2][31]
Scombroid poisoning is often confused with fish allergy; offer patient education on histamine fish poisoning and/or skin testing after symptoms have resolved. [31]
Individuals taking isoniazid or monoamine oxidase inhibitors are at increased risk for histamine fish poisoning because these drugs impair histamine metabolism. [31]
Reef fish poisoning (ciguatera fish poisoning) [2][15][32]
-
Transmission: ingestion of reef fish containing ciguatoxins produced by Gambierdiscus toxicus ; [33]
- Most common in large predatory fish: barracuda, moray eel, snapper, sea bass, amberjack
- Over 400 species of fish can carry ciguatoxin.
- Mechanism of action: ingestion of ciguatoxin → opening of Na+ channels → depolarization
- Onset after ingestion: 4–6 hours (delay of up to 24 hours not uncommon)
-
Duration
- Gastrointestinal symptoms: 2–5 days
- Neurologic symptoms: 1–2 weeks (residual symptoms may persist for months)
-
Clinical features [34][35]
- Gastrointestinal: diarrhea, nausea, vomiting, abdominal cramping (initial symptoms)
- Cardiovascular: hypotension, heart block, bradycardia (early onset)
- Neurologic (delayed for 1–2 days)
- Cold allodynia: contact with cold objects causes dysesthesia; pathognomonic for reef fish poisoning
- Dysesthesia and paresthesia of mouth, lips, throat
- Paresthesias resembling peripheral neuropathy
- Ataxia, vertigo, hallucinations, coma
- Diagnosis: clinical diagnosis
-
Treatment [2][15][32]
- Supportive treatment: Follow management of food poisoning.
- Patients with severe symptoms: Consider calling the local Poison Control Center for specialist treatments (e.g., IV mannitol).
- Bradycardia and/or hypotension: Follow the “Adult unstable bradycardia algorithm.” [15][32]
- Dysesthesias and/or pruritus: Consider antihistamine, e.g., diphenhydramine (off-label), or amitriptyline (off-label). [15][32]
Recommend avoidance of alcohol and nuts for 3–6 months after poisoning as they may exacerbate residual symptoms. [2]
Puffer fish poisoning [2][36]
- Transmission: ingestion of puffer fish containing tetrodotoxin produced by bacteria inhabiting the animal's gut [37]
- Mechanism of action: Tetrodotoxin is a neurotoxin that blocks voltage-gated sodium channels, which inhibits action potential propagation.
- Onset: 5–45 minutes
- Duration: days
-
Clinical features: dose-dependent
- Neurological
- Paresthesias (usually the first reported symptom)
- Muscle weakness, paralysis, loss of reflexes
- CNS depression, coma
- Gastrointestinal: nausea, diarrhea
- Cardiopulmonary
- Respiratory failure, cyanosis
- Hypotension, bradycardia, heart failure
- Neurological
- Diagnosis: clinical diagnosis
-
Treatment [2][36][38]
-
Initiate supportive care as soon as possible: Death may occur within minutes.
- Respiratory distress: early intubation and mechanical ventilation
- Hemodynamic instability: IV fluid resuscitation and inoconstrictors
- Consider calling the local Poison Control Center for specialist treatments (e.g., gastrointestinal decontamination, hemodialysis).
-
Initiate supportive care as soon as possible: Death may occur within minutes.
No antidote exists for tetrodotoxin, but recovery is likely if the patient survives the first 24 hours. [38]
Prevention
Food and water precautions are the best means for preventing food poisoning. [39][40]
-
Food hygiene
- Wash hands and disinfect surfaces frequently.
- Wash fruits and vegetables with safe drinking water.
- Avoid cross-contamination by keeping raw meat products, eggs, and seafood separated from other kinds of food.
- Use a food thermometer while cooking.
- Maintain a refrigerator temperature < 4°C (< 39°F).
- When traveling (especially in resource-limited countries): Only consume fully cooked or dry (e.g., bread, crackers) foods, pasteurized dairy products, and fruits and vegetables you can peel or have properly washed yourself.
-
Water hygiene
- Do not consume untreated water or ice.
- Options if water treatment is unknown:
- Consume sealed bottled beverages.
- Boil water for at least one minute before consuming.
- Use an appropriate filter.
There is a simple rule to avoid foodborne illness while traveling: Boil it, cook it, peel it, or forget it. [39]
External Resources
References
- Feng C, Teuber S, Gershwin ME. "Histamine (Scombroid) Fish Poisoning: a Comprehensive Review". Clin Rev Allergy Immunol. 50(1). :64-69. (2015)
- Lawrence DT, Dobmeier SG, Bechtel LK, Holstege CP. "Food Poisoning". Emerg Med Clin North Am. 25(2). :357-373. (2007)
- Walls R, Hockberger R, Gausche-Hill M, Erickson TB, Wilcox SR. "Rosen's Emergency Medicine 10th edition- Concepts and Clinical Practice E-Book". Elsevier Health Sciences. (2022). ISBN: 9780323757904
- Friedman M, Fleming L, Fernandez M, et al. "Ciguatera Fish Poisoning: Treatment, Prevention and Management". Mar Drugs. 6(3). :456-479. (2008)
- Chan T. "Regional Variations in the Risk and Severity of Ciguatera Caused by Eating Moray Eels". Toxins. 9(7). :201. (2017)
- "Fever Without Fear: Information for Parents". https://web.archive.org/web/20230814193750/https://www.healthychildren.org/English/health-issues/conditions/fever/Pages/Fever-Without-Fear.aspx. [2022-12-13]
- Raman R, Coppes S, Hellingman T, Laclé C. "Junctional bradycardia caused by ciguatera intoxication". BMJ Case Rep. 12(5). :e229354. (2019)
- Katikou P, Gokbulut C, Kosker AR, Campàs M, Ozogul F. "An Updated Review of Tetrodotoxin and Its Peculiarities". Mar Drugs. 20(1). :47. (2022)
- Bane V, Lehane M, Dikshit M, et al. "Tetrodotoxin: Chemistry, Toxicity, Source, Distribution and Detection". Toxins. 6(2). :693-755. (2014)
- How CK, Chern CH, Huang YC, et al. "Tetrodotoxin poisoning". Am J Emerg Med. 21(1). :51-54. (2003)
- Bintsis T. "Foodborne pathogens". AIMS Microbiology. 3(3). :529-563. (2017)
- Law RKY, Kisselburgh H, Roblin D, et al. "Noninfectious Foodborne Exposures Reported to 2 National Reporting Systems, United States, 2000-2010". Public Health Rep. 134(5). :552-558. (2019)
- Switaj TL, Winter KJ, Christensen SR. "Diagnosis and Management of Foodborne Illness.". Am Fam Physician. 92(5). :358-65. (2015)
- "Norovirus (Norwalk Virus)". https://web.archive.org/web/20250202083753/https://www.foodsafety.gov/food-poisoning/bacteria-and-viruses#norovirus. [2017-04-10]
- Acheson DWK. "Food and Waterborne Illnesses". Encyclopedia of Microbiology. :365-381. (2009)
- "Clostridium perfringens". https://www.foodsafety.gov/poisoning/causes/bacteriaviruses/cperfringens/. [2017-04-10]
- "Food Safety: Clostridium perfringens". https://web.archive.org/web/20170502095138/https://www.cdc.gov/foodsafety/diseases/clostridium-perfringens.html. [2017-01-10]
- "E.coli (Escherichia coli)". https://web.archive.org/web/20170419192907/https://www.cdc.gov/ecoli/general/. [2015-11-06]
- Fayer R, Xiao L. "Cryptosporidium and Cryptosporidiosis". Taylor & Francis Group. (2007). ISBN: 9781420052268
- "Treatment for Cyclosporiasis". https://web.archive.org/web/20170527083752/https://www.cdc.gov/parasites/cyclosporiasis/health_professionals/tx.html. [2013-01-10]
- "Cryptosporidium: Treatment". https://web.archive.org/web/20170520092703/https://www.cdc.gov/parasites/crypto/treatment.html. [2015-02-20]
- Xie L, Ming L, Ding M, et al. "Paratyphoid Fever A: Infection and Prevention". Front Microbiol. 13. (2022)
- Shane AL, Mody RK, Crump JA, et al. "2017 Infectious Diseases Society of America Clinical Practice Guidelines for the Diagnosis and Management of Infectious Diarrhea". Clin Infect Dis. 65(12). :e45-e80. (2017)
- Talan DA, Moran GJ, Newdow M, et al. "Etiology of Bloody Diarrhea among Patients Presenting to United States Emergency Departments: Prevalence of Escherichia coli O157:H7 and Other Enteropathogens". Clin Infect Dis. 32(4). :573-580. (2001)
- "Vibrio Infections". https://www.foodsafety.gov/poisoning/causes/bacteriaviruses/vibrio_infections/. [2017-04-10]
- "Vibrio Species Causing Vibriosis". https://web.archive.org/web/20170502131407/https://www.cdc.gov/vibrio/index.html. [2016-10-24]
- "Brucellosis: Transmission". https://web.archive.org/web/20170526063120/https://www.cdc.gov/brucellosis/transmission/index.html. [2012-11-12]
- "CDC Yellow Book 2024: Brucellosis". https://web.archive.org/web/20240118153834/https://wwwnc.cdc.gov/travel/yellowbook/2024/infections-diseases/brucellosis. [2023-05-01]
- "Brucellosis". https://web.archive.org/web/20240225100803/https://www.who.int/news-room/fact-sheets/detail/brucellosis. [2020-07-29]
- Fiore AE. "Hepatitis A transmitted by food". Clin Infect Dis. 38(5). :705-715. (2004)
- Bross MH, Soch K, Morales R, Mitchell RB. "Vibrio vulnificus Infection: Diagnosis and Treatment". Am Fam Physician. 76(4). :539-544. (2007)
- Daniels NA. "Vibrio vulnificus oysters: pearls and perils". Clin Infect Dis. 52(6). :788-792. (2011)
- Dewey-Mattia D, Manikonda K, Hall AJ, Wise ME, Crowe SJ. "Surveillance for Foodborne Disease Outbreaks — United States, 2009–2015". MMWR Surveill Sum. 67(10). :1-11. (2018)
- Kadariya J, Smith TC, Thapaliya D. "Staphylococcus aureus and Staphylococcal Food-Borne Disease: An Ongoing Challenge in Public Health". Biomed Res Int. 2014. :1-9. (2014)
- Todd ECD. "Foodborne Diseases: Overview of Biological Hazards and Foodborne Diseases". Encyclopedia of Food Safety. :221-242. (2014)
- Julian E. Grass, L. Hannah Gould, Barbara E. Mahon. "Epidemiology of Foodborne Disease Outbreaks Caused by Clostridium perfringens, United States, 1998–2010". Foodborne Pathog Dis. 10(2). :131-136. (2013)
- Shrestha A, Uzal FA, McClane BA. "Enterotoxic Clostridia: Clostridium perfringens Enteric Diseases". Microbiol Spectr. 6(5). (2018)
- Sobel J, Painter J. "Illnesses Caused by Marine Toxins". Clin Infect Dis. 41(9). :1290-1296. (2005)
- Schwartz KL, Keystone JS. "Protection of Travelers". Principles and Practice of Pediatric Infectious Diseases. :79-85.e2. (2018)
- Canadian Pediatric Society. "How to avoid food poisoning". Paediatr Child Health. 6(4). :218-218. (2001)