CME information and disclosures
To see contributor disclosures related to this article, hover over this reference: [1]
Physicians may earn CME/MOC credit by reading information in this article to address a clinical question, and then completing a brief evaluation, in which they will identify their question and report the impact of any information learned on their clinical practice.
AMBOSS designates this Internet point-of-care activity for a maximum of 0.5 AMA PRA Category 1 Credit(s)™. Physicians should claim only credit commensurate with the extent of their participation in the activity.
For answers to questions about AMBOSS CME, including how to redeem CME/MOC credit, see "Tips and links" at the bottom of this article.
Summary
Fractures of the radius and/or ulna occur frequently. Important forearm fracture patterns include complete forearm fractures, Galeazzi fractures, and Monteggia fractures. Fractures of the forearm bones at the elbow level include radial head fractures and olecranon fractures, while those at the wrist level include distal radius fractures. The mechanism of injury can be low-energy, such as a fall on an outstretched hand (FOOSH), or high-energy, such as a motor vehicle collision (MVC). Clinical presentation is typically characterized by pain near the fracture site, gross deformity, and swelling. X-ray is the main diagnostic modality. Evaluation includes imaging of the forearm; wrist and elbow imaging are added for moderate to severe injuries. Management varies depending on the age group and fracture characteristics, and includes a thorough neurovascular assessment, acute immobilization, pain management, and referral to orthopedics for definitive open reduction and internal fixation (ORIF) or closed reduction and casting.
For more details on fractures involving the distal radius, see “Distal radius fractures.”
Overview
Relevant anatomy
Important musculoskeletal structures
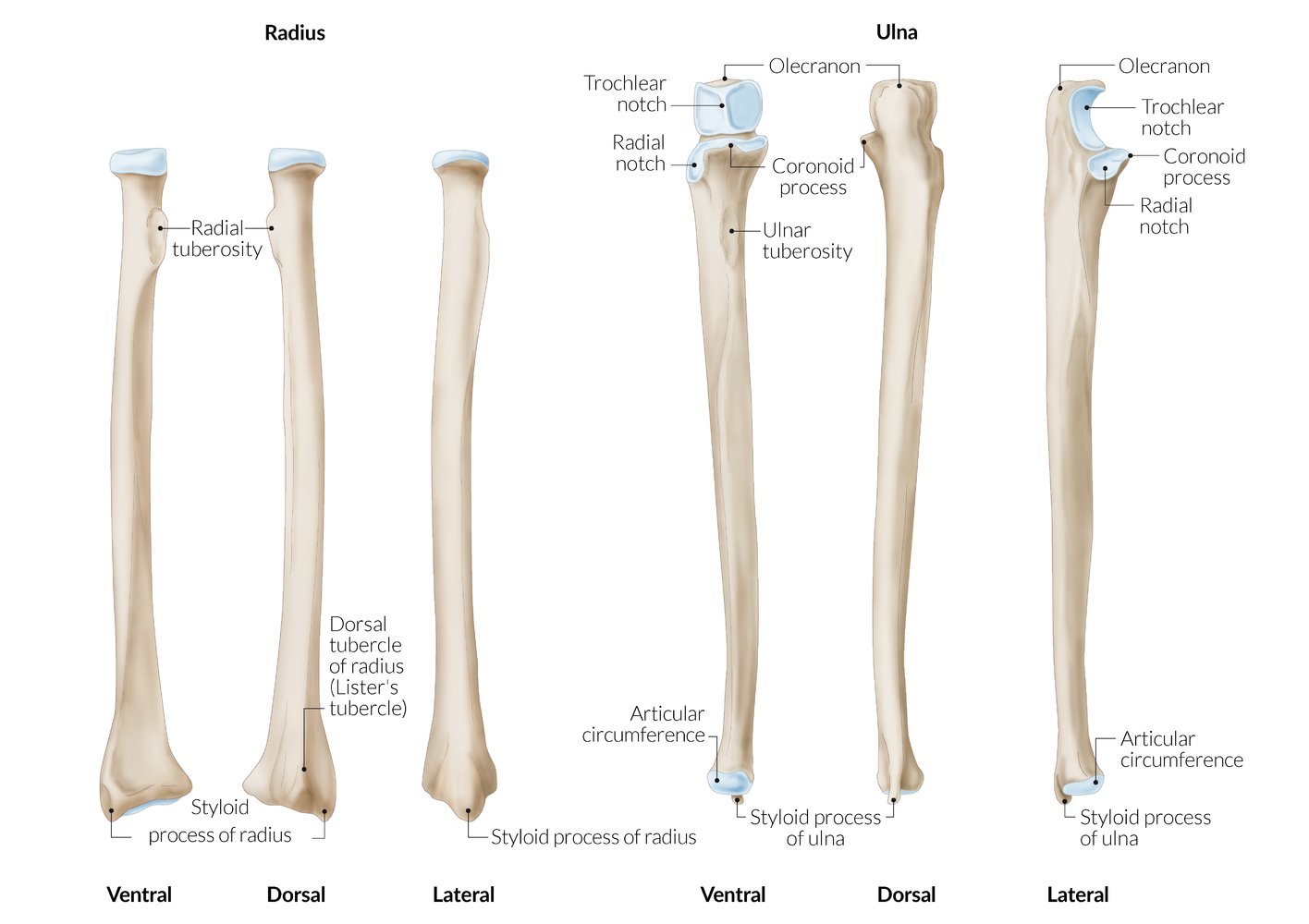
- Radius: composed of the radial head, radial shaft, and distal radius (including radial styloid)
- Ulna: composed of the olecranon process, coronoid process, ulnar shaft, and distal ulna (including ulnar styloid)
- Connective tissue: interosseous membrane of the forearm, annular ligament of the radius
- Joints: elbow joints (i.e., radiohumeral joint and humeroulnar joint), proximal radioulnar joint , wrist joints (i.e., radiocarpal joints), and distal radioulnar joint (DRUJ)
Important neurovascular structures
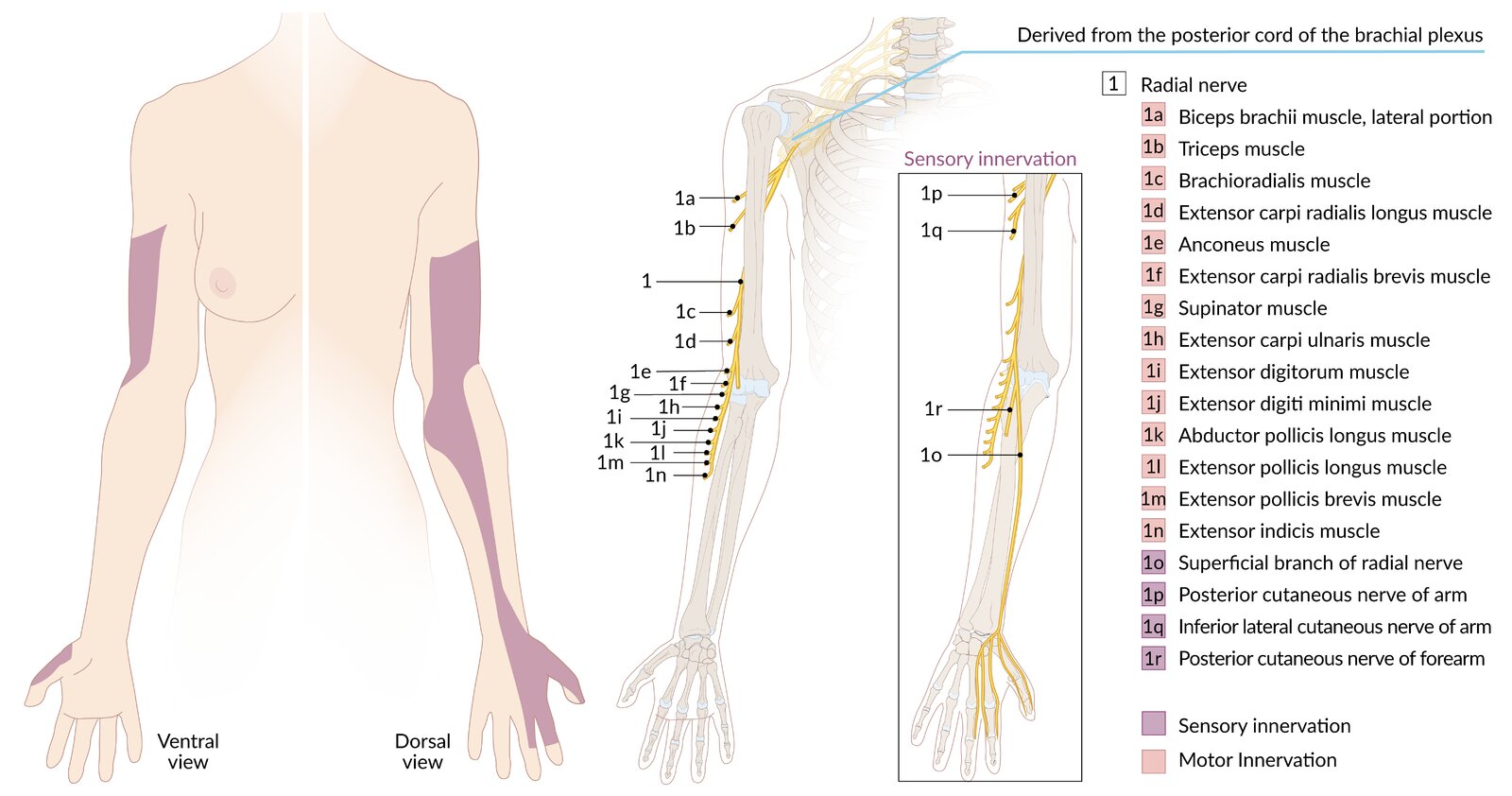
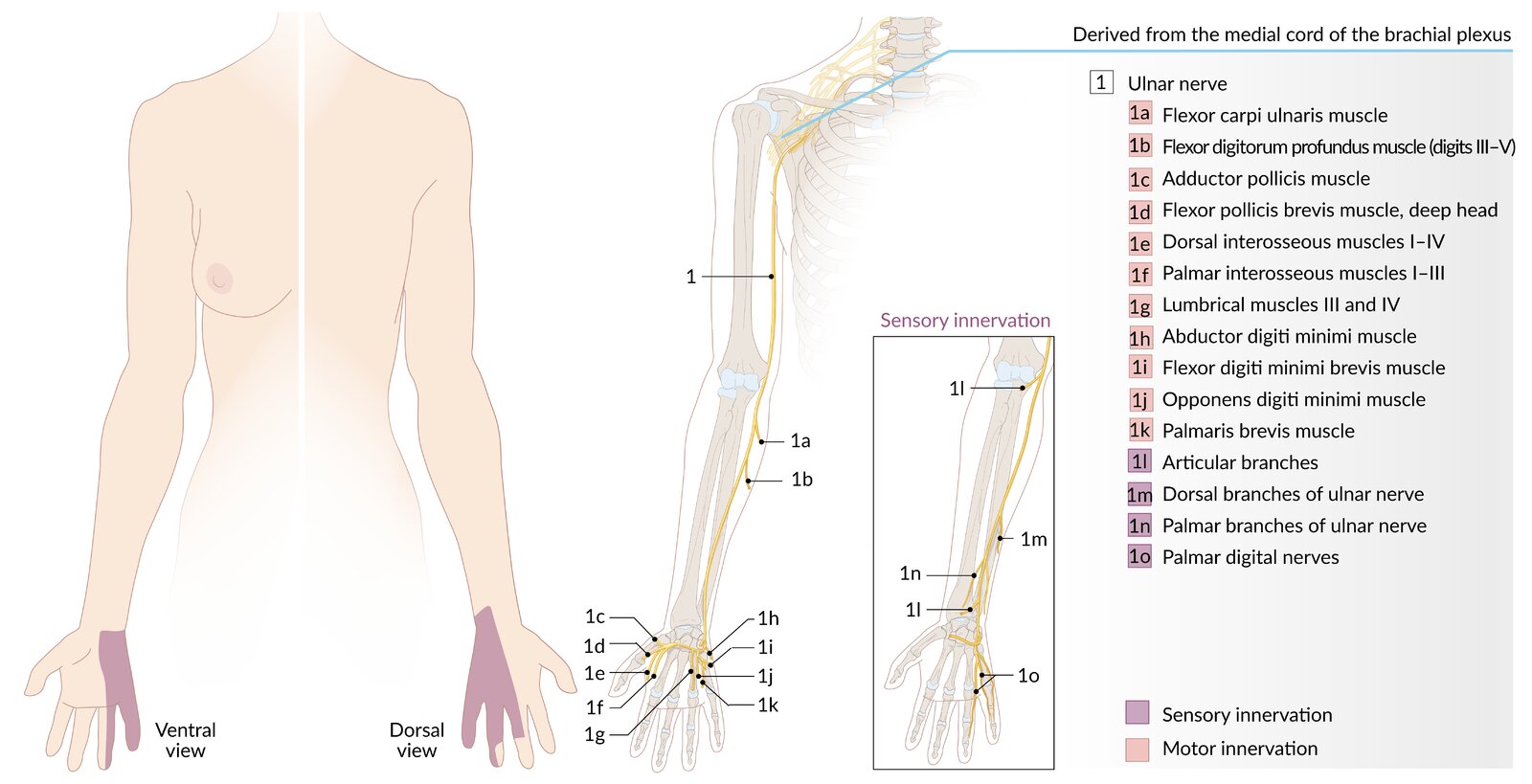
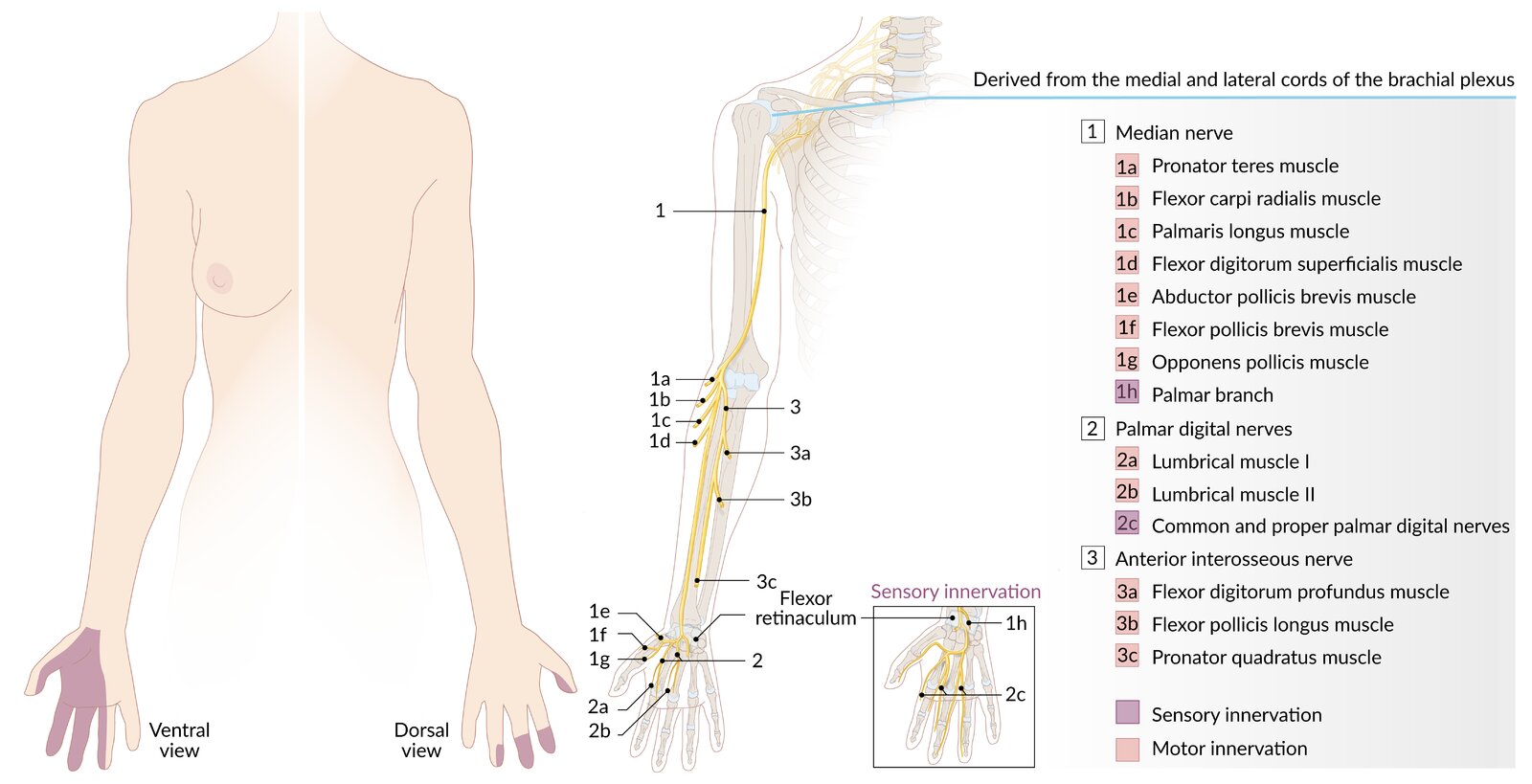
- Nerves: the radial nerve , ulnar nerve , and median nerve (including its branch anterior interosseous nerve)
- Arteries: the brachial artery and its branches, the radial artery and ulnar artery
Overview of forearm fractures
- Although the term forearm fracture most often focuses on midshaft fractures of the radius and/or ulna, the proximal and distal portions of these bones which make up the wrist and elbow joints can also be involved.
- See “Overview of radius and ulna fractures” for the various fracture patterns that can affect these bones.
- For further detail on distal radius fracture patterns, See “Types of distal radius fractures.”
- For other bones that can be fractured in the wrist, see “Causes of wrist fractures.”
- For other bones that can be fractured in the elbow, see “Distal humerus fractures.”
| Overview of radius and ulna fractures | ||||
|---|---|---|---|---|
| Affected structures | Mechanism of injury | Management | ||
| Fractures with elbow involvement | Monteggia fracture |
|
|
|
| Isolated radial head fracture |
|
|
|
|
| Olecranon fracture |
|
|
|
|
| Fractures of the mid-forearm | Complete forearm fracture (Combined radial and ulnar shaft fracture) |
|
|
|
| Isolated radial shaft fracture [2] |
|
|
|
|
| isolated ulnar shaft fracture (Parry fracture; nightstick fracture) [2][3] |
|
|
|
|
| Fractures with wrist involvement | Galeazzi fracture |
|
|
|
| Colles fracture |
|
|
|
|
| Smith fracture |
|
|
||
| Barton fracture |
|
|
||
| Reverse Barton fracture |
|
|
||
| Hutchinson fracture |
|
|
||
| Die-punch fracture |
|
|
||
| Ulnar styloid fracture [4] |
|
|
|
|
| Fractures with elbow and wrist involvement | Essex-Lopresti injury [3] |
|
|
|


")



")


© AMBOSS
Right forearm; ventral view
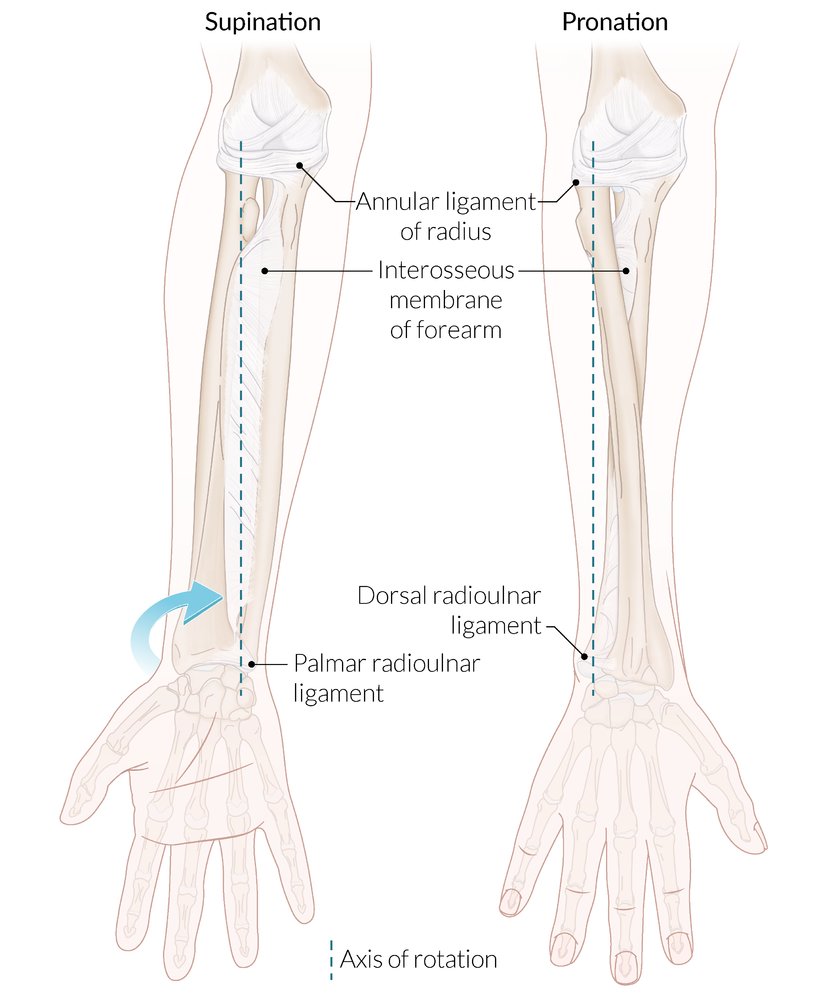
Supination is an external rotational movement of the forearm that occurs at the proximal and distal radioulnar joints. When the forearm is in the supine position, the radius and ulna lie parallel to each other and the palm faces up. The supinator and biceps brachii (not shown here) are the supinators of the forearm.
Pronation is an internal rotational movement of the forearm that occurs at the proximal and distal radioulnar joints. When the forearm is in the prone position, the radius and ulna form an X shape and the palm faces down. The pronator quadratus and pronator teres (not shown here) are the pronators of the forearm.
The interosseous membrane stabilizes the proximal and distal radioulnar joints during pronation and supination.
© AMBOSS
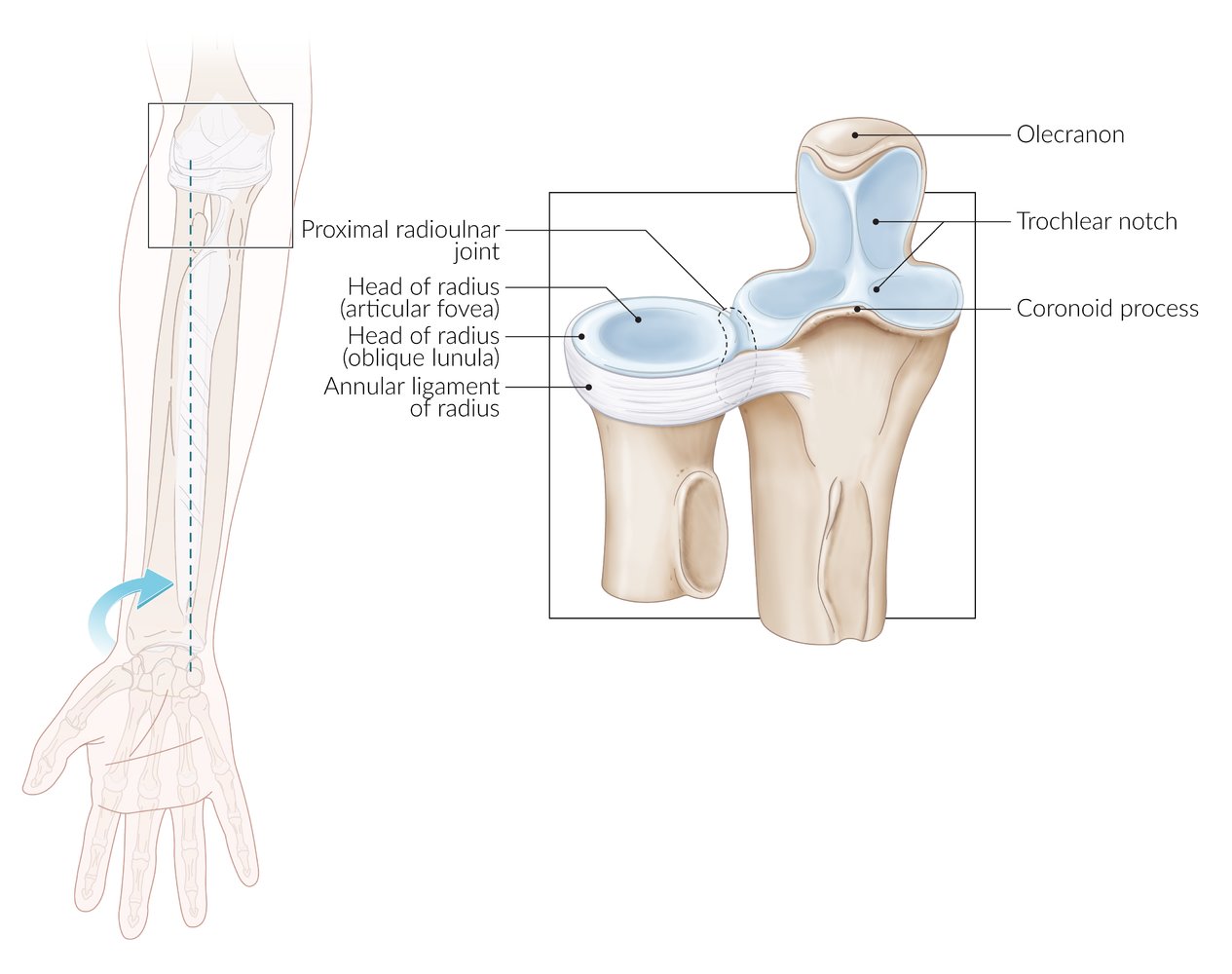
A pivot joint formed by the head of the radius articulating with the radial notch of the ulna
The annular ligament is a thick, ring-shaped ligament that surrounds the head of the radius and is attached to the radial notch of the ulna, thereby stabilizing the proximal radioulnar joint (PRUJ).
Pronation and supination of the forearm occur at the proximal and distal radioulnar joints (the axis of rotation is depicted on the left). The PRUJ, along with the distal end of the humerus, also forms the elbow joint, at which elbow flexion and extension occur.
© AMBOSS
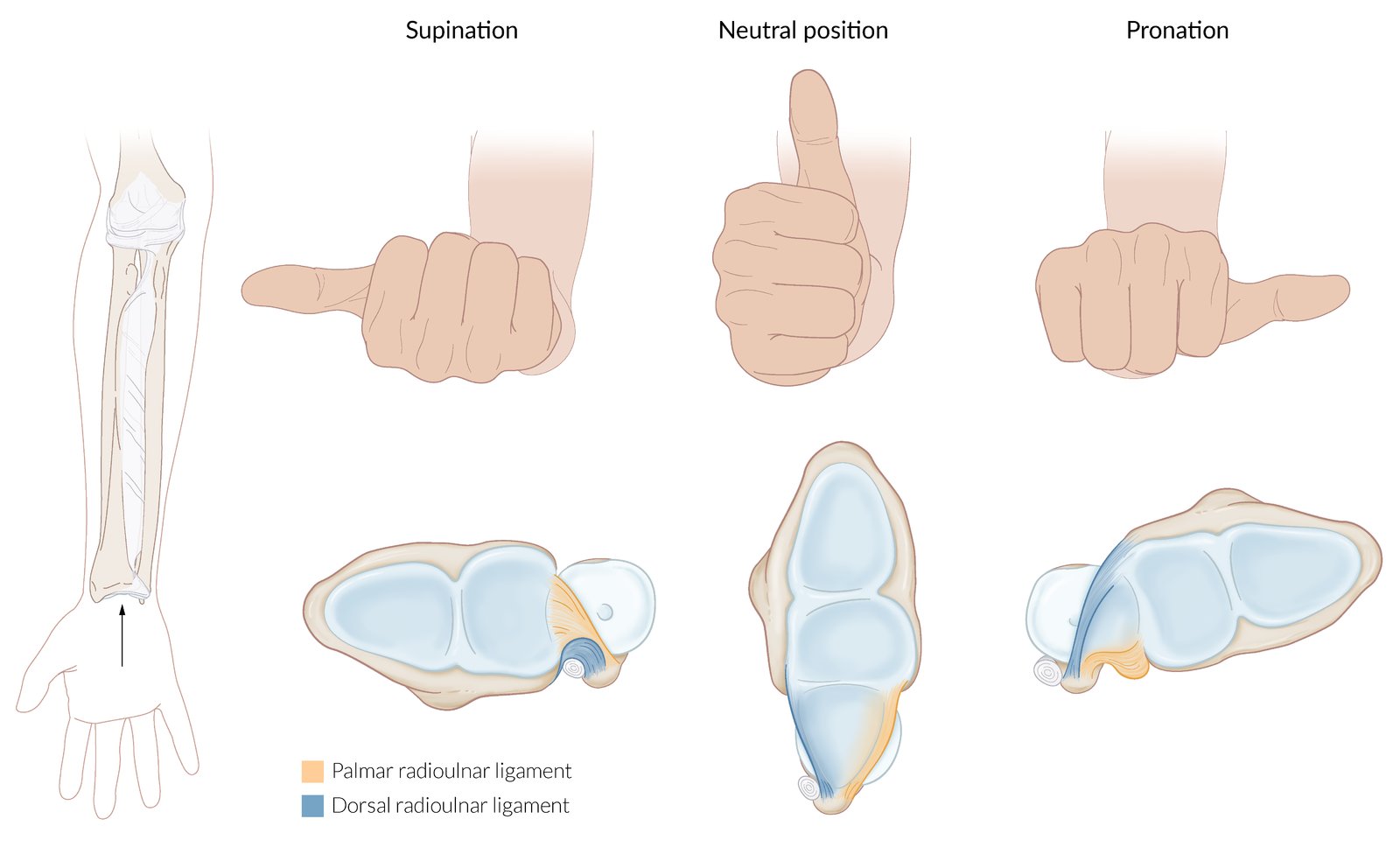
A pivot joint formed by the articulation of the ulnar head with the ulnar notch on the radius. Pronation and supination of the forearm occur at the proximal and distal radioulnar joints. The distal radioulnar joint also articulates with the proximal row of carpal bones, forming a part of the wrist joint.
The palmar and dorsal radioulnar ligaments extend from the medial surface of the distal radius and insert into the ulnar styloid. They stabilize the distal radioulnar joint. During pronation, the dorsal ligament tightens, while the palmar ligament becomes lax. The opposite occurs during supination.
© AMBOSS
© AMBOSS
© AMBOSS
© AMBOSS
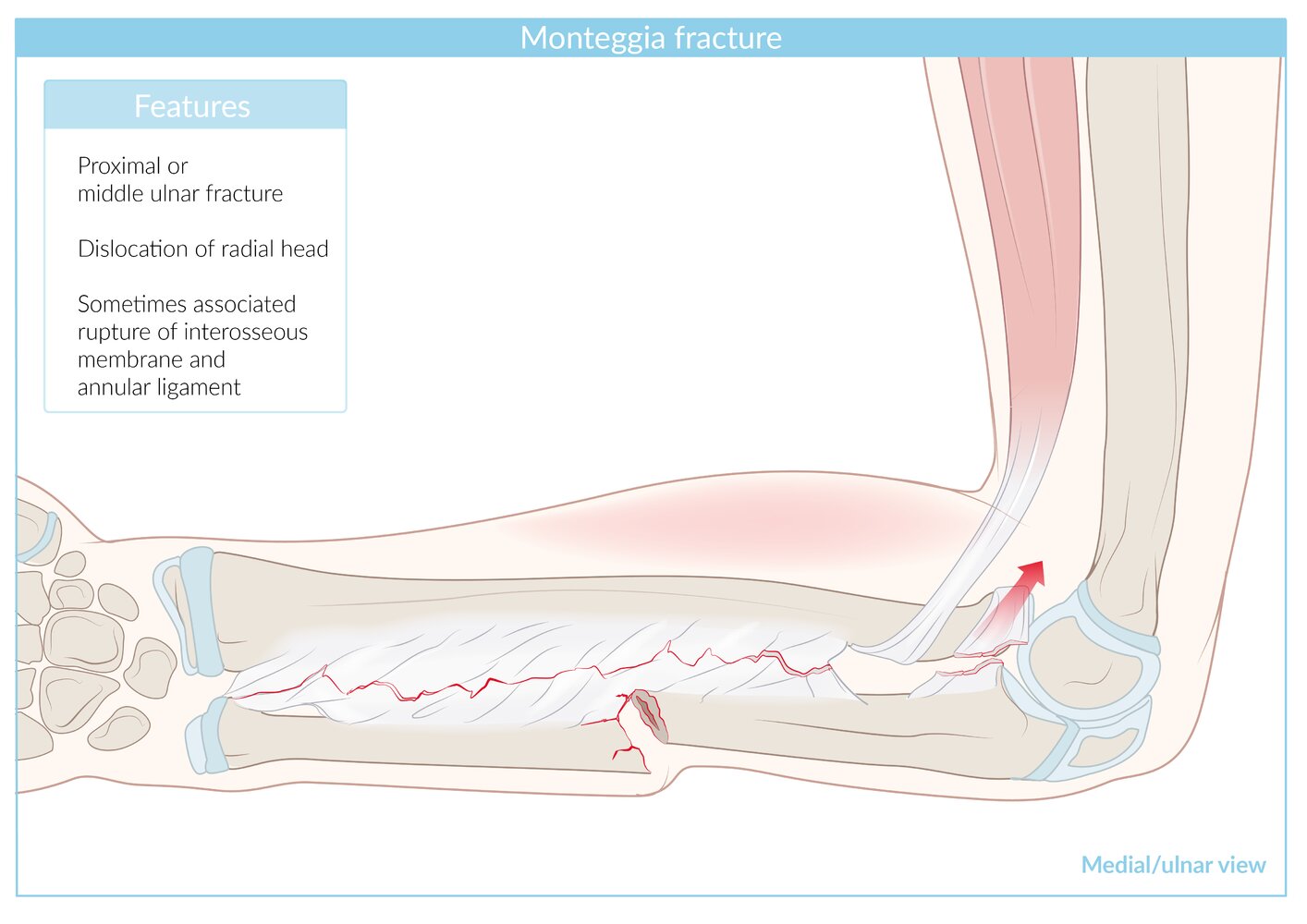
Right forearm; medial/ulnar view.
Monteggia fracture is defined as a fracture of the ulna (most commonly proximal) with concomitant dislocation of the radial head.
This fracture is more common in children, therefore the illustration depicts the distal humerus, radius, and ulna with epiphyseal (growth) plates (dark blue) and incompletely ossified epiphyses (light blue).
© AMBOSS
X-ray left elbow (left: AP view; right: lateral view)
The radial head fracture shows intraarticular extension and slight distraction (widening) at the fracture line (red overlay).
Source: © IMPP
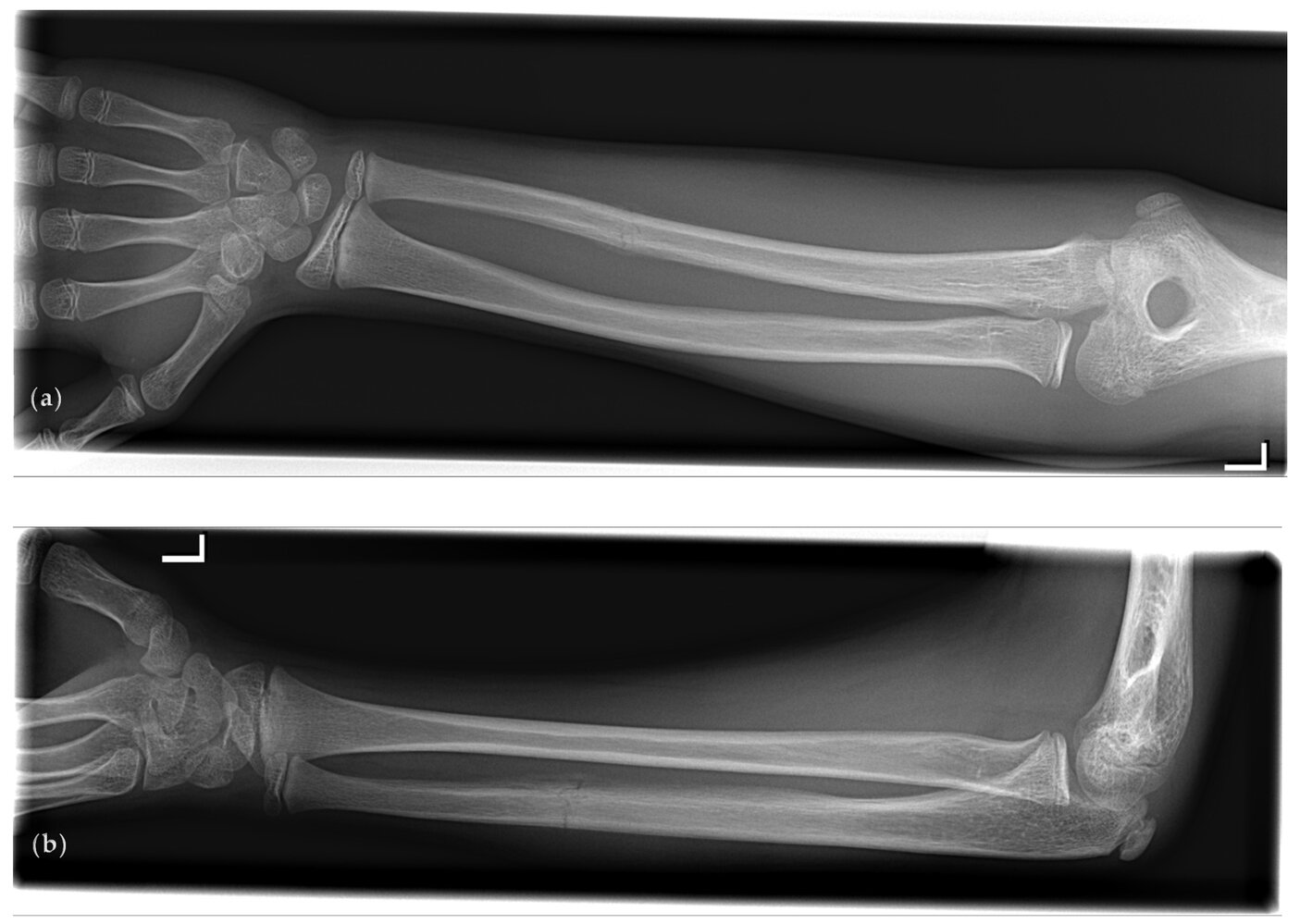
X-ray left forearm (top: AP view; bottom: lateral view) of an adolescent patient
There is an isolated transverse fracture of the distal third of the ulna with minimal displacement (green overlay). A small amount of adjacent periosteal reaction (yellow overlay) is seen.
The findings are consistent with a parry (or nightstick) fracture, which is typically a defensive injury incurred when the forearm is used to block a blow.
Red overlay: growths plates
Source: “Figure 1, in: Is a Parry Fracture—An Isolated Fracture of the Ulnar Shaft—Associated with the Probability of Abuse in Children between 2 and 16 Years Old?” by Hermans K, Fransz D, Walbeehm-Hol L, Hustinx P, Staal H, MDPI, licensed under CC BY 4.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).

X-ray forearm (left: AP view; right: lateral view) of a child
An isolated fracture of the mid ulnar diaphysis is accompanied by displacement of the distal fragment (indicated by arrows). There is no disruption of the distal radioulnar joint.
This type of fracture has been termed a “parry” or “nightstick fracture.” It occurs when the ulna is more exposed than the radius to injury. It may be the result of direct trauma (forearm raised in self-defense) or indirect trauma (fall).
Arrowheads: bracelet; R: radius; U: ulnar
Source: “Fig. 1, in: Locked Intramedullary Nailing versus Compression Plating for Stable Ulna Fractures: A Comparative Study” by Vito Pavone; Marco Ganzi; Giacomo Papotto et al., J. Funct. Morphol. Kinesiol., licensed under CC BY 4.0. Modifications: -cropped -letter removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
Right distal forearm
© AMBOSS
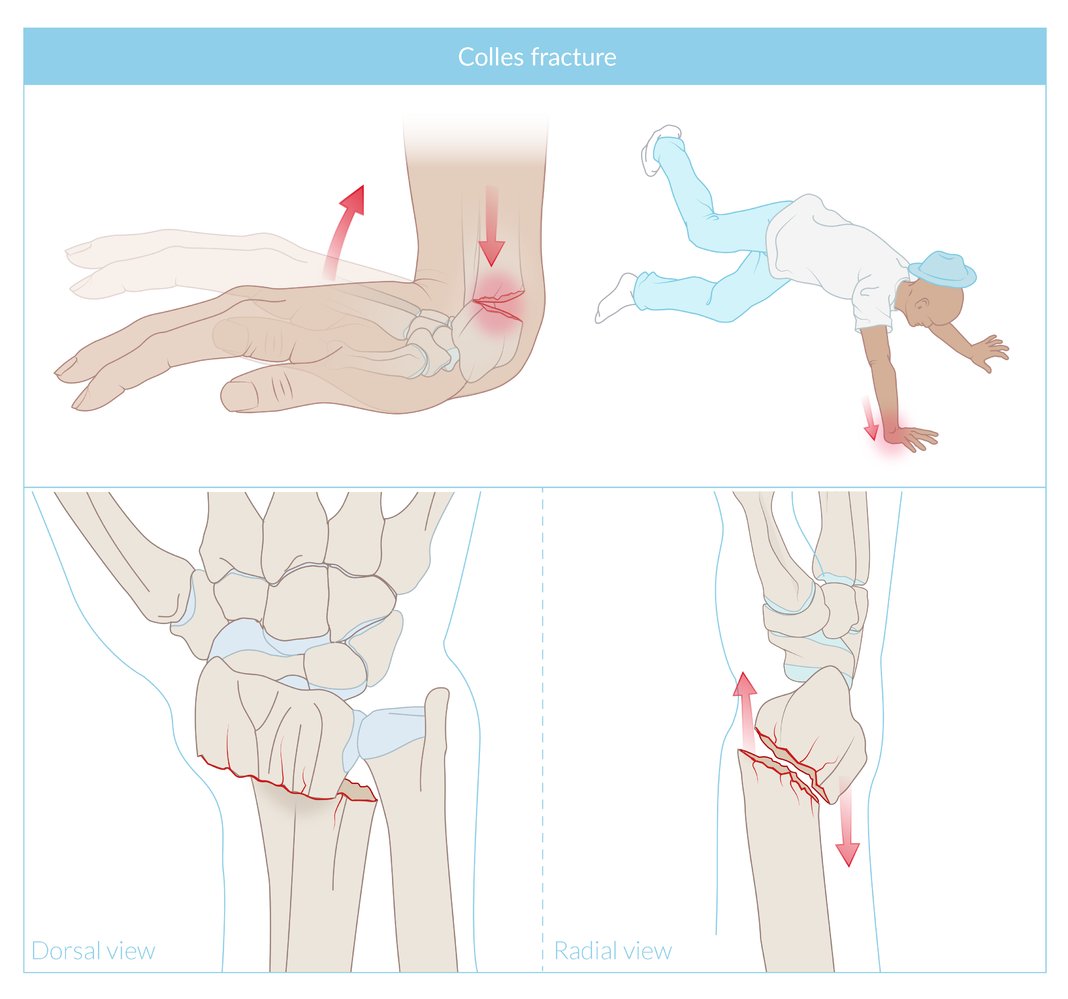
Fracture of the distal radius with radial and dorsal displacement. Commonly a result of falling onto the extended wrist.
© AMBOSS
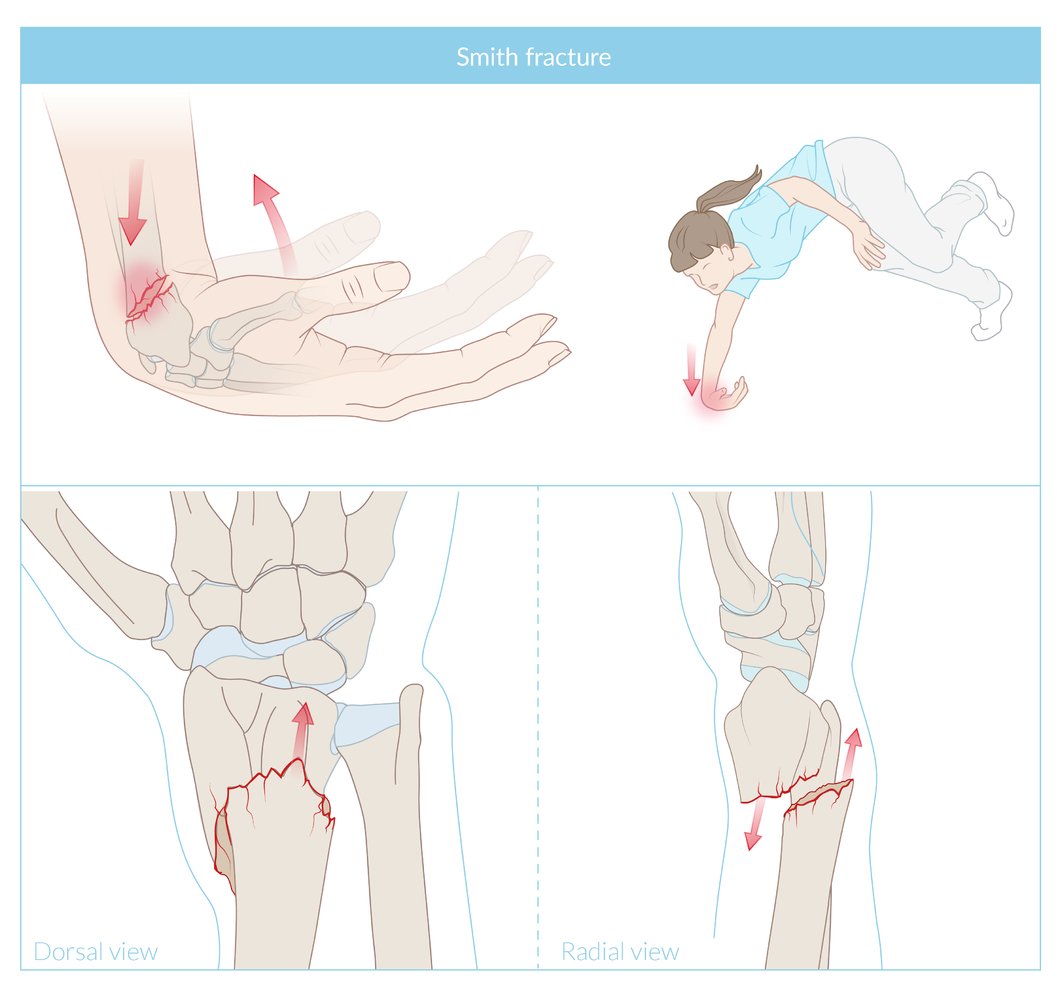
Fracture of the distal radius with volar displacement of the distal radial fragment and dorsal angulation at the fracture site.
© AMBOSS
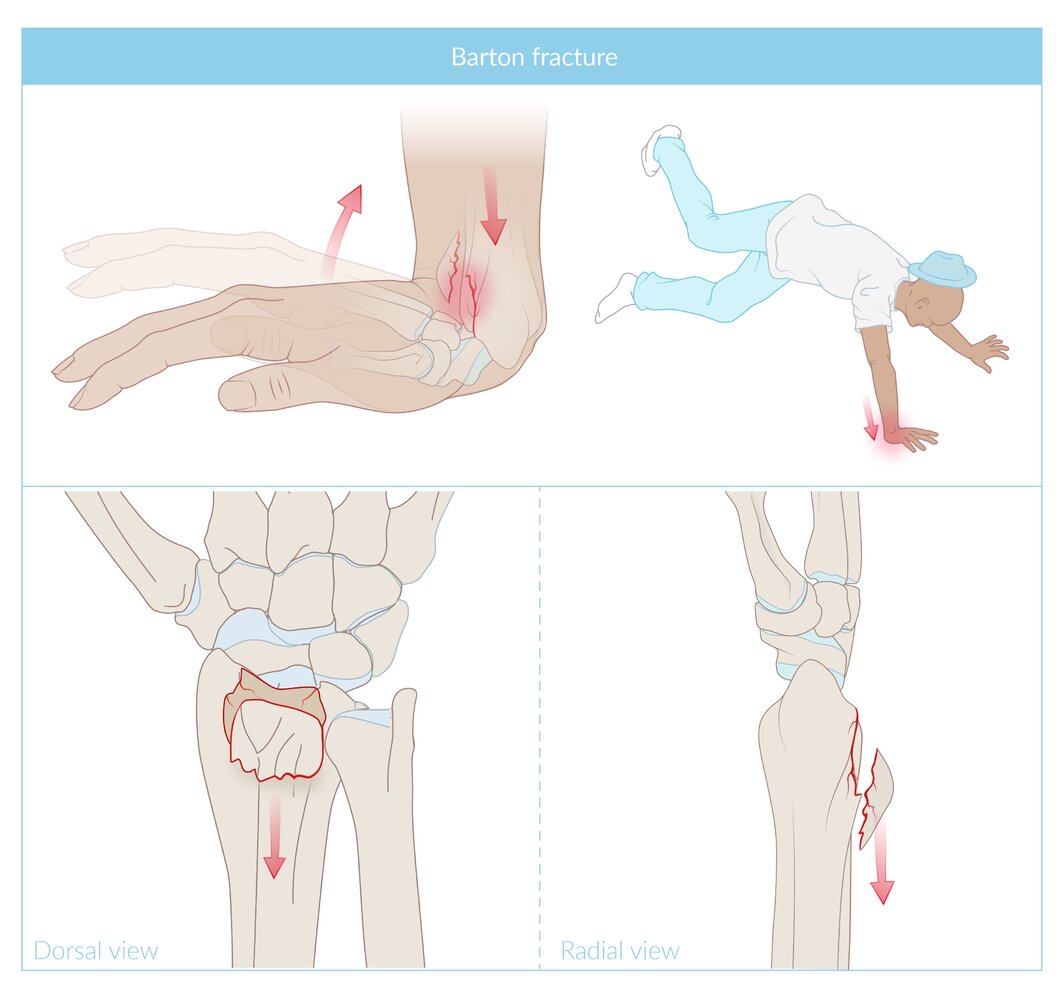
A partial fracture of the distal radius with a dorsal edge fragment. The cause is usually a fall onto the extended hand.
© AMBOSS
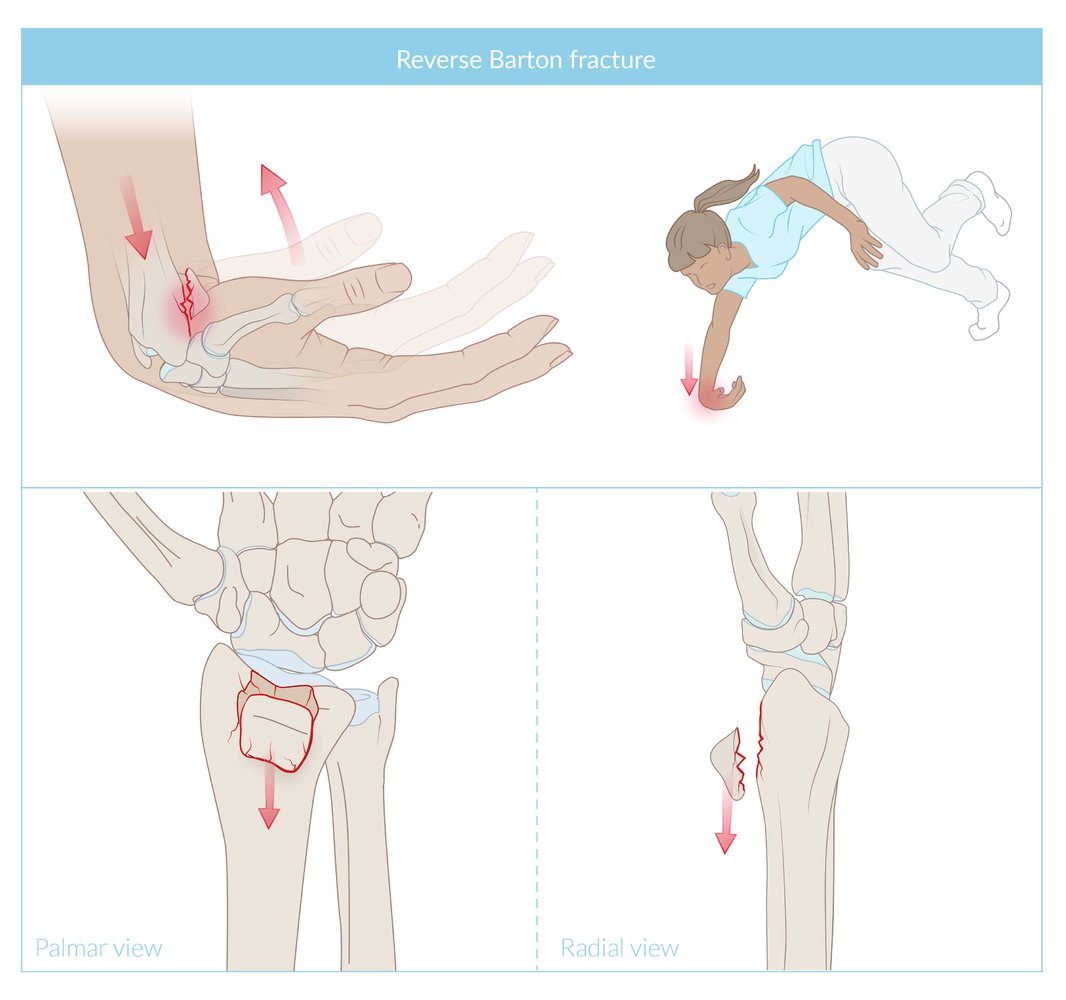
A partial articular radius fracture with a volar edge fragment. The cause is usually a fall onto the flexed hand.
© AMBOSS
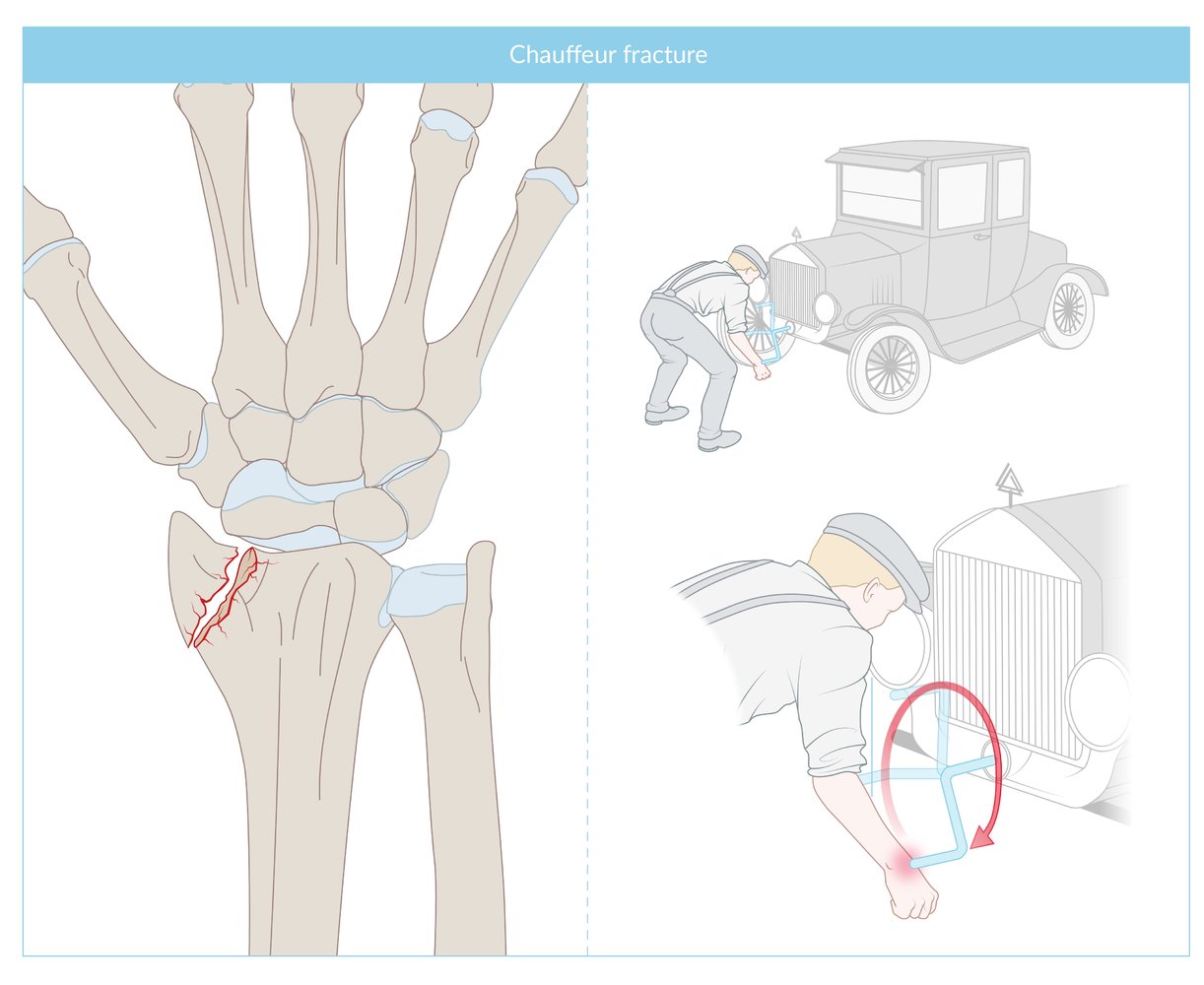
Fracture of the radial styloid, commonly due to direct trauma. The term ''Chauffer fracture' was coined by the British surgeon Jonathan Hutchison in the days when cars were hand-cranked and the crank shooting back could hit and thus fracture the wrist.
© AMBOSS
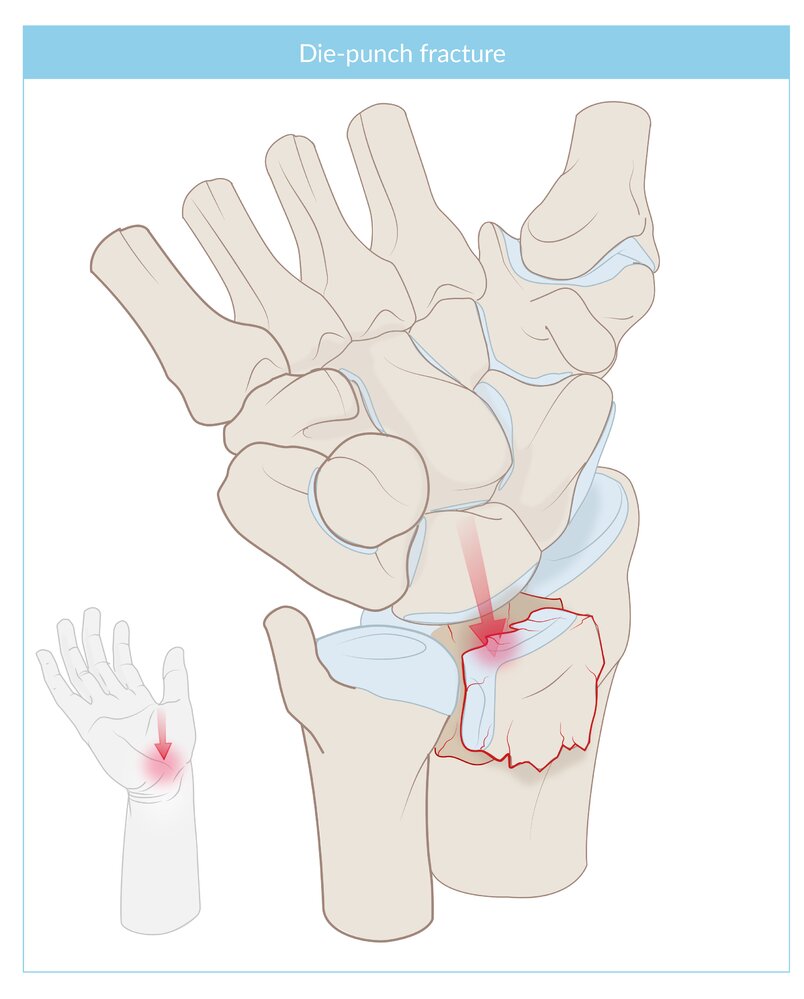
An impacted, intra-articular fracture of the lunate fossa of the distal radius. The cause is most commonly an axial loading force applied against the distal radius.
© AMBOSS

X-ray hand (PA view)
A nondisplaced fracture (red line) is visible through the waist of the scaphoid bone of the wrist.
© AMBOSS
Initial management
The following are indicated irrespective of the fracture type and bones involved: [2][3]
- Perform neurovascular exam.
- Assess radial and ulnar artery pulses and capillary refill time.
- Evaluate for median nerve injury , radial nerve injury , and ulnar nerve injury.
- Consider indications for orthopedic consultation for fractures.
- Obtain imaging of the forearm and consider adding imaging of the elbow and wrist to check for associated injuries.
- Evaluate for signs of compartment syndrome in any patient with high-energy impact trauma.
- Provide analgesia for acute fractures.
- Continue with management specific to the injury identified on imaging, e.g., complete forearm fracture, Monteggia fracture, Galeazzi fracture
")



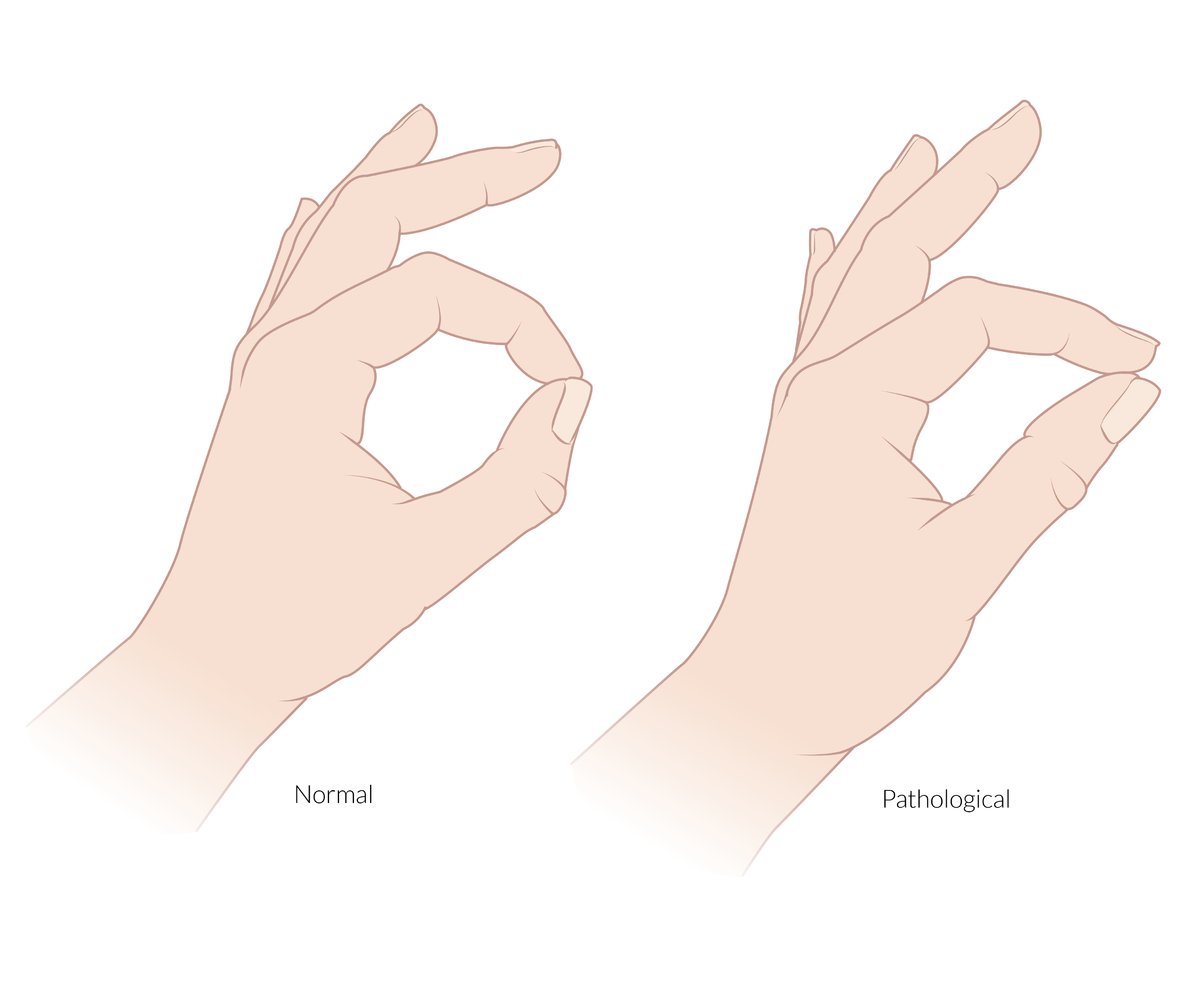
The anterior interosseous nerve is a pure motor branch of the median nerve. It supplies the flexor pollicis longus, the radial half of the flexor digitorum profundus (and the pronator quadratus).
Pinch sign: an inability to flex the DIP of the index finger and IP joint of the thumb when asked to make an “OK” sign that is caused by a lesion or entrapment of the anterior interosseous nerve
© AMBOSS

An inability to flex the index and middle fingers at the MCP and IP joints and an inability to oppose the thumb.
The hand of benediction is an active sign and is only seen when the patient is asked to make a fist. It indicates a paralysis of the thenar muscles (except the adductor pollicis), the flexor digitorum superficialis, and the radial half of the flexor digitorum profundus caused by a proximal lesion of the median nerve (above the elbow).
Also depicted is atrophy of the thenar muscles, which is seen in chronic median nerve palsy.
© AMBOSS
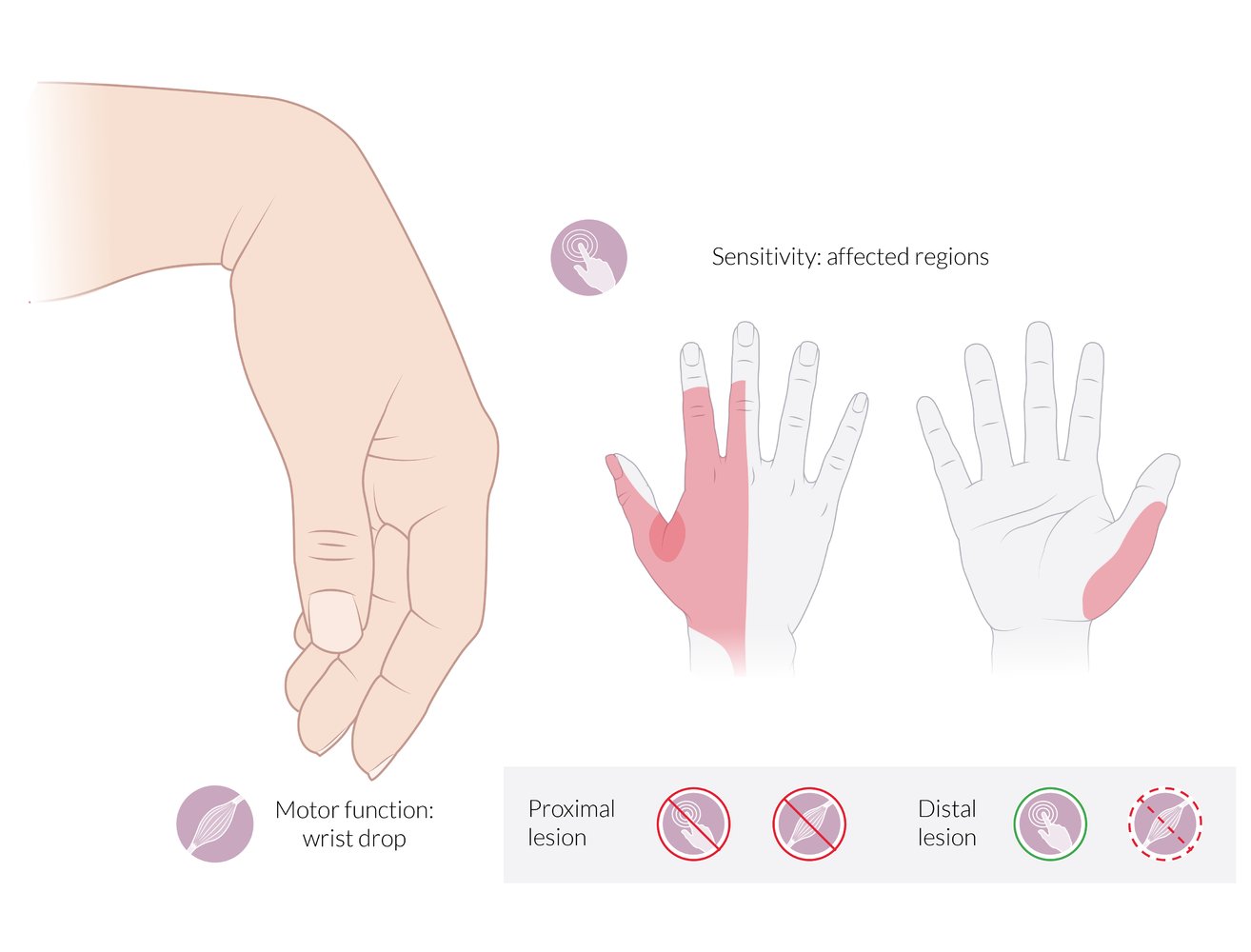
Motor deficits:
- Wrist drop: inability to extend (dorsiflex) the wrist
- Inability to extend the fingers at the MCP joints
Sensory deficits:
- Dorsal aspect: radial 2½ fingers (less commonly, 3½ fingers), excluding the tips of the 2nd and 3rd fingers. The 1st web space is the autonomous sensory zone of the radial nerve and is highlighted in red.
- Palmar aspect: the radial border of the thumb
Proximal lesion: complete loss of motor and sensory function
Distal lesion (radial tunnel syndrome): partial loss of motor function; preservation of sensory function
© AMBOSS
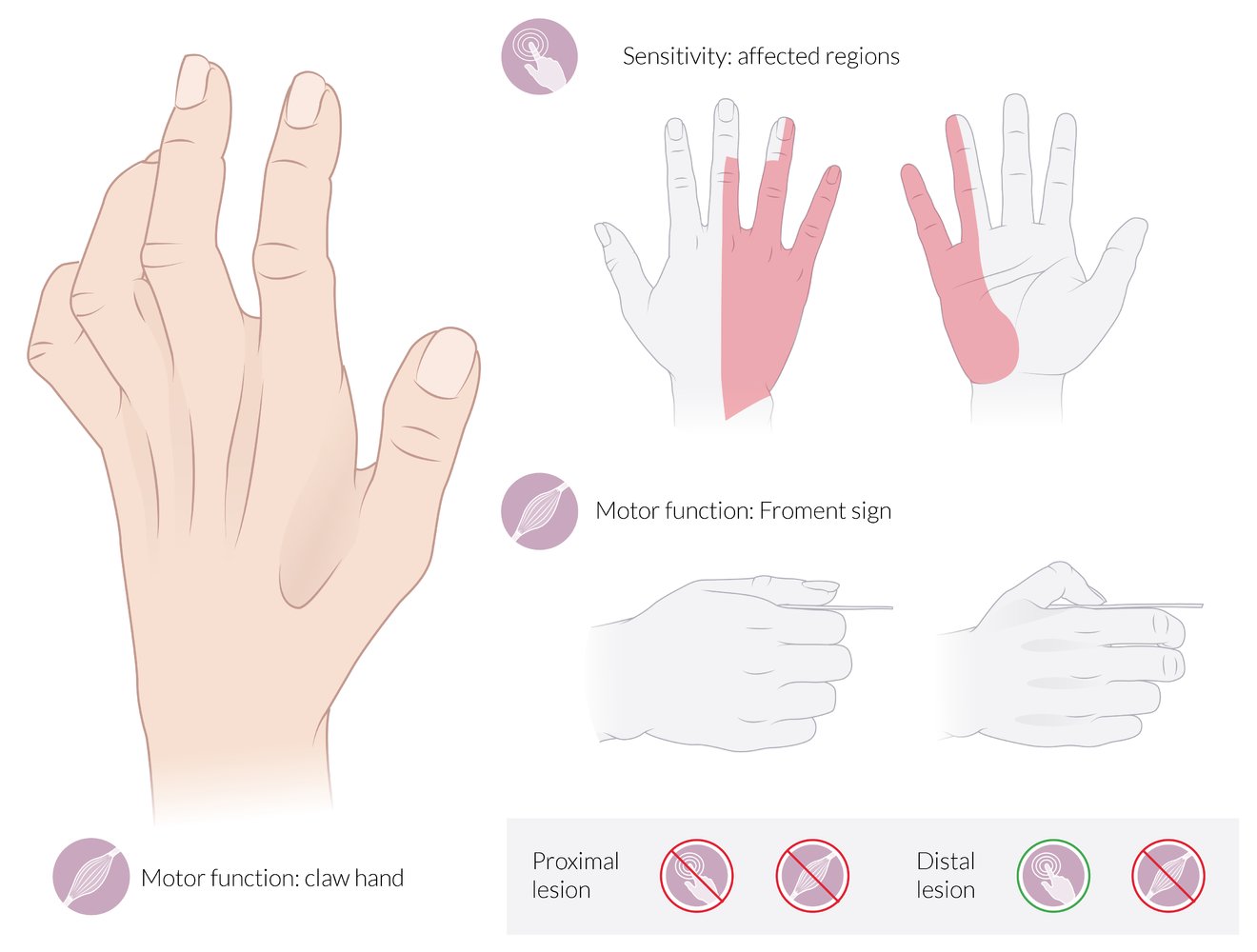
Motor deficits:
- Claw hand: The 4th and 5th joints are hyperextended at the MCP and flexed at the IP joints at rest (neutral position).
- Froment sign: The patient is asked to grasp a piece of paper between the thumb and the index finger. When the examiner tries to pull the paper away, the thumb flexes at the IP joint because the flexor pollicis longus (supplied by the median nerve) compensates for the paralyzed adductor pollicis (supplied by the ulnar nerve).
Also depicted here is hollowing of the intermetacarpal spaces and the 1st web space due to the atrophy of the interossei, which is seen in chronic ulnar nerve palsy.
Sensory deficits:
- Dorsal aspect: ulnar 2½ fingers (less commonly, 1½ fingers), excluding the tips of the 3rd and 4th fingers
- Palmar aspect: ulnar 1½ fingers
Proximal lesion: complete loss of motor and sensory functions
Distal lesion: complete loss of motor function; preservation of sensory function
© AMBOSS
Complete forearm fractures
- Definition: fracture of both the radial shaft and ulnar shaft
- Epidemiology: more common in children [2]
- Etiology: FOOSH injury (common in children), high-energy trauma (e.g., MVC) [2]
-
Clinical features [2]
- Pain and swelling of the mid-forearm
- Gross deformity
- Nerve injury is uncommon with closed fractures.
-
Diagnostics: x-ray [2][5]
- May show nondisplaced, displaced, or greenstick fractures of both shafts of the radius and ulna
- Injury from high-energy trauma: may show angulation > 10° and/or comminution
-
Management: Begin general management of forearm fractures. [2][3][5]
-
Fracture-dislocations with signs of skin tenting or neurovascular compromise
- Consult orthopedics for emergency reduction.
- If timely access to orthopedics is unavailable, consider closed reduction by an experienced emergency physician.
-
Open fractures
- Begin irrigation and IV antibiotics for open fractures.
- Consult orthopedics for emergency operative management.
-
Closed fractures without reasons for urgent orthopedic consultation for fractures
- All patients
- Immobilize with a long-arm AP splint or sugar tong splint.
- Refer for prompt follow-up with orthopedics, e.g., within 3–5 days.
- Children: closed reduction under sedation and immobilization
- Adults
- Nondisplaced (uncommon): long-term immobilization
- Displaced : typically requires ORIF
- All patients
-
Fracture-dislocations with signs of skin tenting or neurovascular compromise
Thoroughly evaluate patients with complete forearm fractures for signs of compartment syndrome. [5]



X-ray distal forearm (left: AP view; right: lateral view) of a child
Angulated mid-diaphyseal fractures of the radius (green arrowheads) and ulna (red arrowheads) are seen on the lateral view. The cortex of the radius is disrupted on the convex side, but intact on the concave side (greenstick fracture). The fracture on the convex side of the ulna is conspicuous, but the concave side of the ulna is not well-evaluated due to overlap with the radius. The fractures are well-aligned on the AP view.
Source: “Fig 1, from: Functional Outcome of Closed Reduction and Extension Casting in Forearm Fractures in Children” by Yadav P, Phalak MO, Patel S et al., Cureus, licensed under CC BY 4.0. Modifications: Green tone attenuation. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).

X-ray right wrist (A: lateral view; B: PA view)
Comminuted fractures (indicated by arrows and red lines) of the distal radius and ulna are accompanied by dorsal angulation and displacement (indicated by dashed and solid lines and curved arrow). Intraarticular extension of the radial fracture (green line) is best seen on the PA view.
D: dorsal; P: pisiform bone; V: volar
Source: “Fig 2, In: Simultaneous Fractures of Distal and Proximal Ends of Radius and Ulna: Four Fractures in One Forearm” by Hashem M, AlMohaini RA, Cureus, licensed under CC BY 4.0. Modifications: placed lateral view (A) to face the opposite way, with volar facing to our left. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
Monteggia fracture
- Definition: proximal (or middle) ulnar fracture with concomitant dislocation of the radial head
-
Etiology
- Fall on outstretched and pronated forearm (low-energy trauma)
- Direct blow to the forearm, high-energy trauma (e.g., MVC)
-
Clinical features [2][5]
- Pain, crepitus, and limited range of motion at the elbow
- Radial head palpable in antecubital fossa
- Shortened forearm
-
Posterior interosseous nerve injury can occur.
- Paresthesias to the dorsal aspects of the thumb, second, and third fingers
- Loss of thumb extension
-
Diagnostics: x-ray [2]
- Shows a fracture of the proximal (or middle) ulna with dislocation of the radial head (dislocation can be anterior, posterior, or lateral)
- Lateral view: The radiocapitellar line does not intersect the middle of the capitellum, suggesting elbow dislocation.
-
Treatment Begin general management of forearm fractures. [2]
- Children with uncomplicated fractures: Closed reduction by an orthopedic surgeon is often successful.
- Adults and patients with complicated fractures
- Initial: Immobilize in a posterior long arm splint.
- Definitive: ORIF (e.g., plating, K-wire fixation) required for most injuries
- Disposition: Consult orthopedics urgently.
Adults with displaced Monteggia fractures require urgent ORIF. [3]
In patients with ulnar fractures, evaluate the radiocapitellar line to check for disruption of the proximal radioulnar joint. [2]

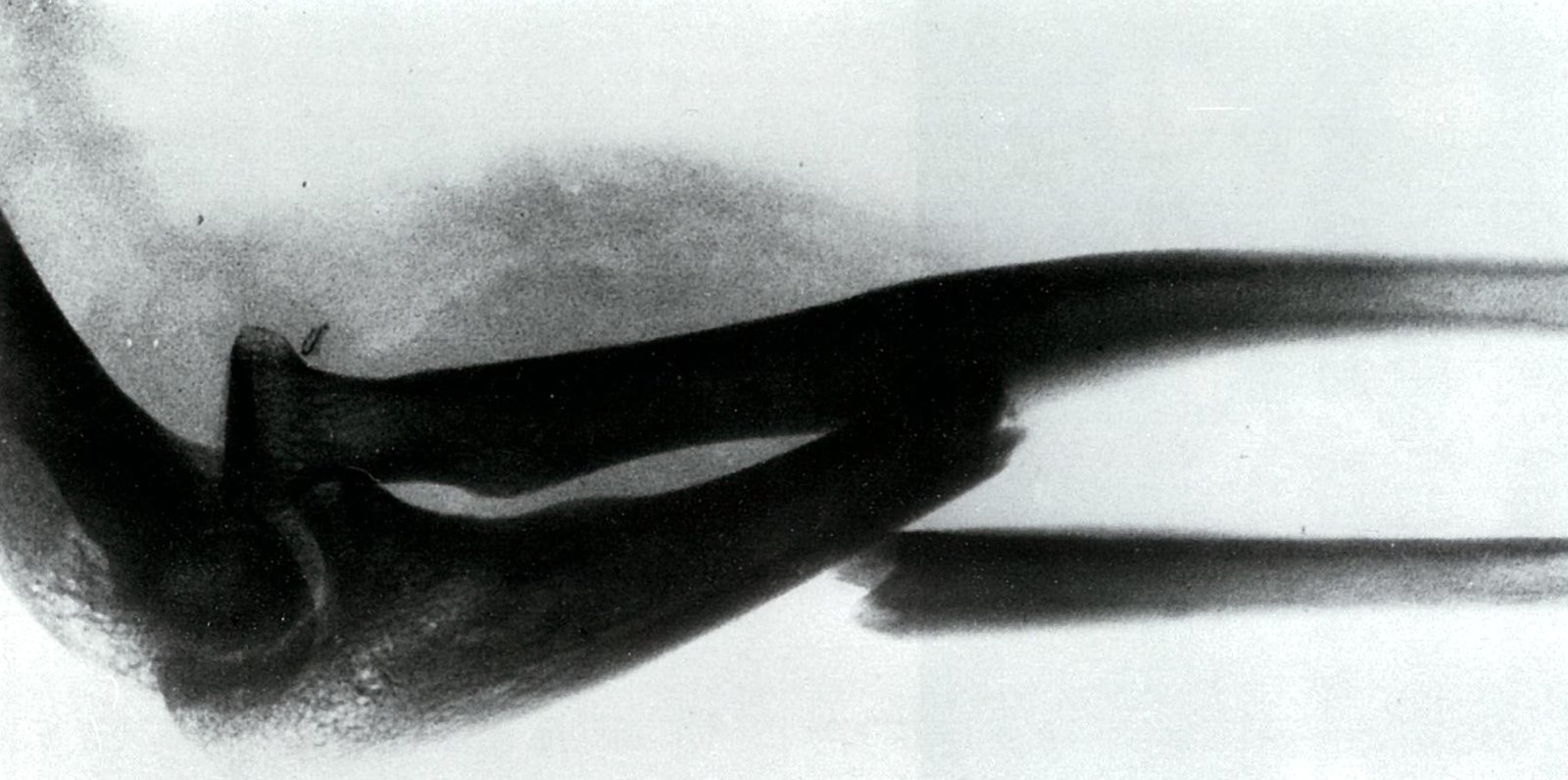
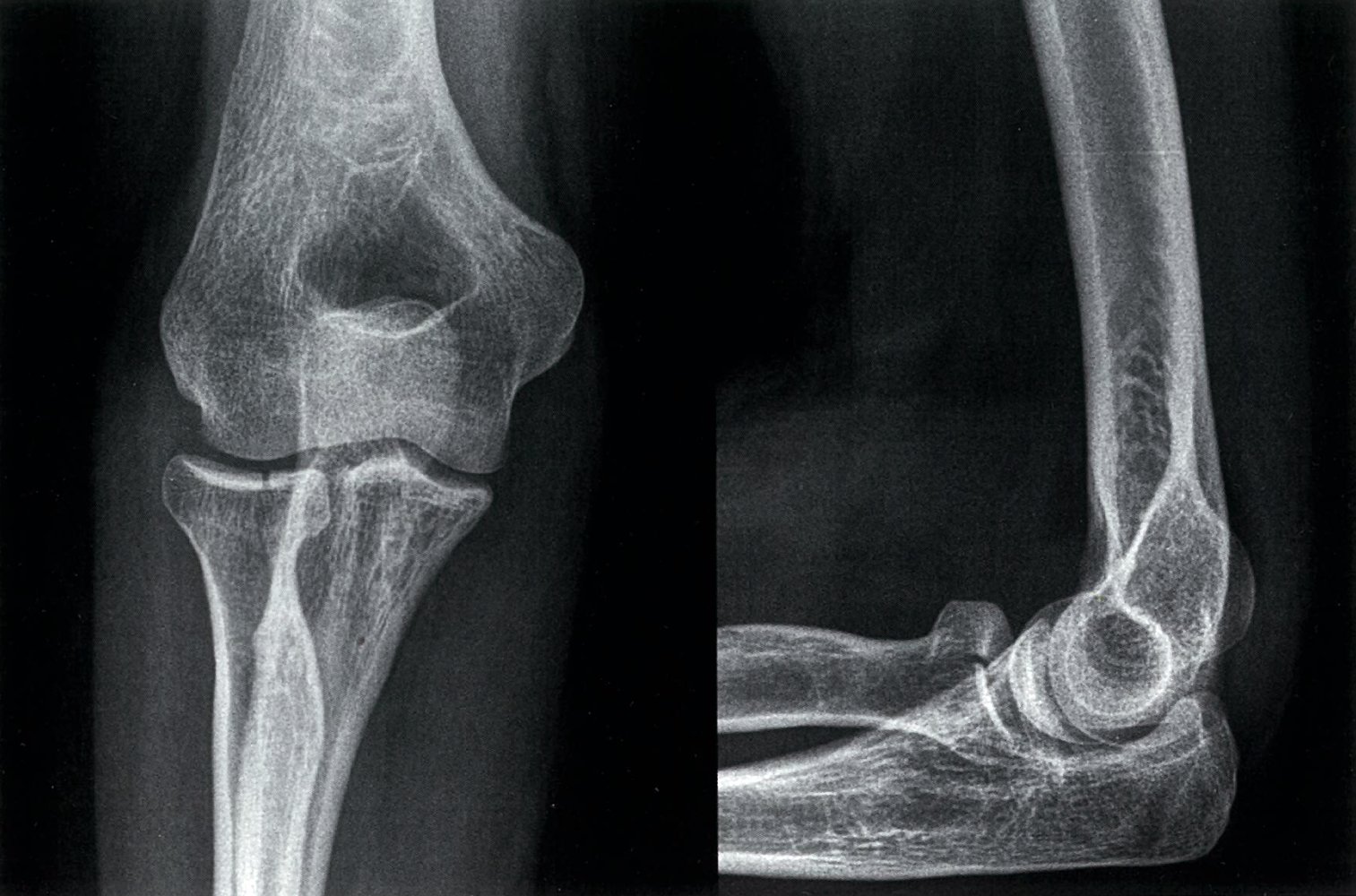
X-ray of the elbow (lateral view, positive mode)
Fracture of the proximal ulna with anterior dislocation of the head of the radius.
The radiodensity of soft tissue anterior to the elbow joint is also increased.
Source: © IMPP
Right forearm; medial/ulnar view.
Monteggia fracture is defined as a fracture of the ulna (most commonly proximal) with concomitant dislocation of the radial head.
This fracture is more common in children, therefore the illustration depicts the distal humerus, radius, and ulna with epiphyseal (growth) plates (dark blue) and incompletely ossified epiphyses (light blue).
© AMBOSS
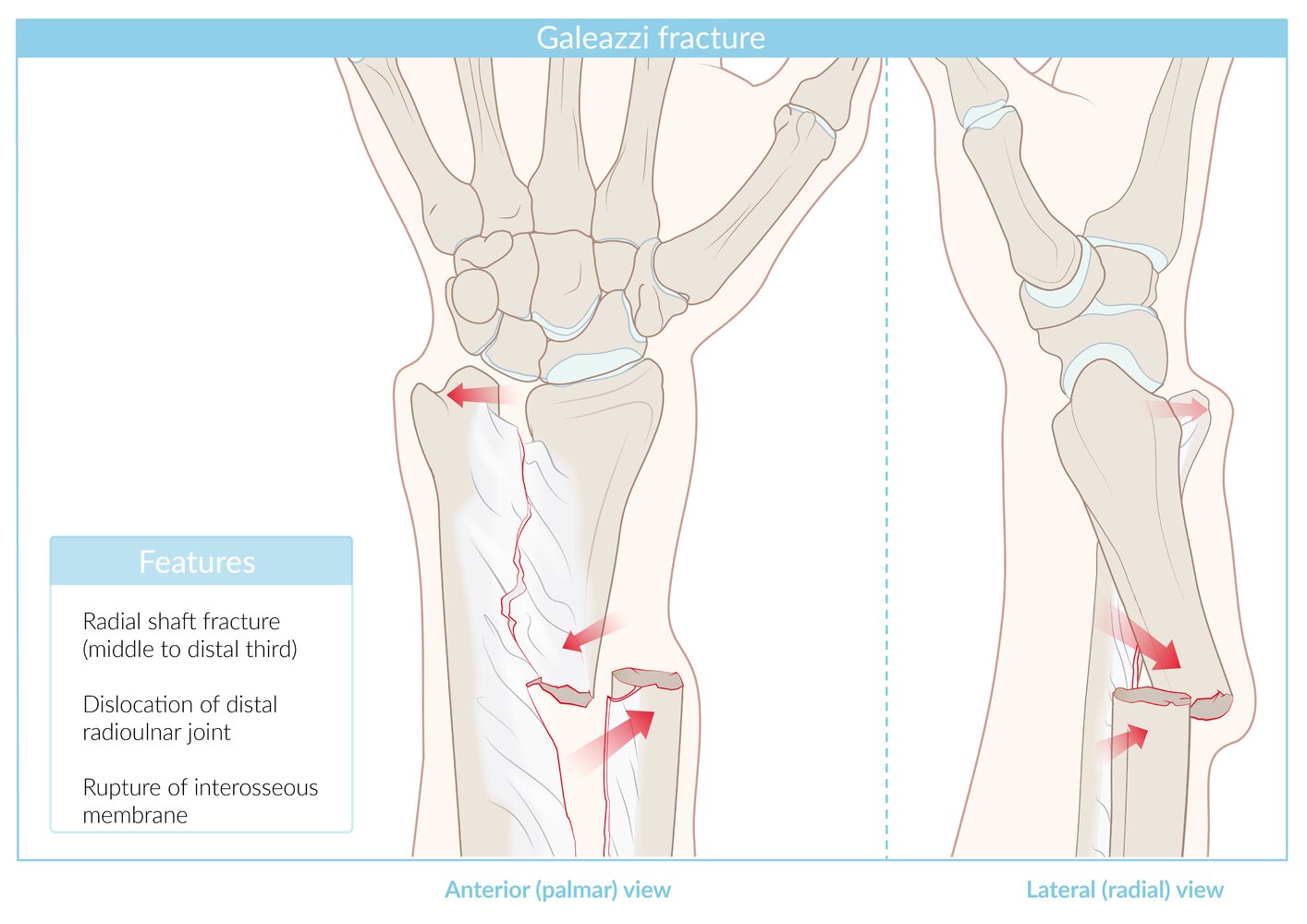
Galeazzi fracture
- Definition: radial shaft fracture with disruption of the distal radioulnar joint
- Epidemiology: more common in children
- Etiology: fall on outstretched and pronated forearm, MVC [2][3]
-
Clinical features [2][3][6]
- Pain and deformity at the distal radius
- Limited range of motion at the wrist
- Palpable displacement of the ulnar head
- Neurologic injury is rare.
-
Diagnostics: x-ray [3][7]
- Shows a fracture at the mid to distal radial shaft, with subluxation or dislocation of the distal radioulnar joint (DRUJ)
- A tear in the interosseous membrane can only be seen indirectly on x-ray.
- Signs of DRUJ instability (e.g., widening of the space between the distal radius and ulna)
-
Treatment: Begin general management of forearm fractures. [2][3]
- Children with uncomplicated fractures: Closed reduction by an orthopedic surgeon followed by casting
- All adult patients and all patients with complicated fractures
- Initial: Immobilize in a posterior long arm splint.
- Definitive: ORIF (e.g., plating, K-wire fixation) required for most injuries
- Disposition: Consult orthopedics urgently.
Almost all Galeazzi fractures require open reduction and repair of the distal radioulnar joint. [3]

Right distal forearm
© AMBOSS

X-ray of the distal lower arm (left, lateral view; right, PA view)
A distal third radius fracture (green outline, bottom left) and distal ulnar head dislocation (green dashed line) can be seen; this fracture pattern is referred to as a Galeazzi fracture. Fracture of the first metacarpal bone (green outline, top right) is also visible.
Source: © IMPP
Radial head fracture
- Definition: fracture of the radial head
- Epidemiology: more common in adults than radial head subluxation or dislocation [8]
-
Etiology
- FOOSH with the elbow partially flexed and pronated [9]
- Stress fracture (e.g., in throwing sports)
-
Clinical evaluation [9]
- Perform a neurovascular exam. [10]
- Radial head region is tender to touch.
- Pronation and supination of the forearm are painful.
- Effusion or hemarthrosis of the elbow joint may be present.
-
Diagnostics: x-ray elbow (AP, lateral and oblique) [3][9][10]
- Fracture through the radial head is not always visible.
- Evidence of effusion (sail sign and/or posterior fat pad sign) may be the only finding.
- Comminuted fractures: Consider imaging the wrist, as these fractures may be associated with additional injuries. [10]
-
Treatment: Begin general management of forearm fractures.
- Fractures with > 60 degrees of angulation often require open reduction and orthopedic consult. [3]
-
Nondisplaced fractures: conservative treatment
- Immobilize in a sling or posterior long arm splint for 24–72 hours. [3][11]
- Start early ROM exercises. [9][12]
- Complex fractures: typically surgical treatment [9]
-
Pain management
- Consider hemarthrosis aspiration only as an adjunct to splinting in select patients. [3][13]
- Avoid intraarticular local anesthetic infiltration. [3]
- Disposition: typically outpatient management with short-term orthopedic follow-up [3]
- Complication: cubitus valgus
Treat a positive elbow fat pad sign with corresponding bony tenderness as an occult fracture. [3]

X-ray left elbow (left: AP view; right: lateral view)
The radial head fracture shows intraarticular extension and slight distraction (widening) at the fracture line (red overlay).
Source: © IMPP
Olecranon fracture
- Definition: fracture of the olecranon process
-
Etiology [2]
- Direct blow to the elbow: more likely to cause comminuted fractures
- FOOSH with the elbow in flexion: more likely to cause transverse or oblique fractures
-
Clinical evaluation [2][3]
- Perform a neurovascular exam. [10]
- Assess for ulnar nerve injury and document ulnar nerve function. [3]
- Findings
- Olecranon and surrounding soft tissue are swollen and tender to touch.
- Hemarthrosis of the elbow joint
- Inability to extend the forearm against resistance or gravity if there is concurrent triceps injury
-
Diagnostics: x-ray elbow (AP, lateral)
- Fractures and displacement are best visualized with lateral views of the elbow in 90° flexion.
- An elbow fat pad sign is indicative of a fracture.
-
Management: Begin general management of forearm fractures. [2][3][5]
- Open fracture and/or neurovascular compromise: orthopedics consult within 30–60 minutes
- Patients without reasons for urgent orthopedic consultation for fractures: Admission is typically not necessary.
- Nondisplaced or minimally displaced (< 2 mm) fractures: conservative treatment
- Immobilize with a posterior long-arm splint. [2]
- Refer for orthopedic follow-up within 5–7 days, including repeat x-rays to exclude delayed displacement.
- ROM exercises can begin 3 weeks after the injury.
-
Fractures displaced > 2 mm and/or loss of extensor mechanism
- ORIF required
- Orthopedics consult within 24–48 hours
- Nondisplaced or minimally displaced (< 2 mm) fractures: conservative treatment
-
Complications [5]
- Ulnar nerve injury
- Decreased range of motion
- Posttraumatic arthritis
- Nonunion
Ensure rapid orthopedic follow-up for all patients with olecranon fractures, as most are considered intraarticular and require near-perfect reduction to preserve full ROM. [2][5]
External Resources
References
- Sherman SC. "Simon's Emergency Orthopedics, 8th edition". McGraw Hill Professional. (2018). ISBN: 9781259860836
- Walls R, Hockberger R, Gausche-Hill M, Erickson TB, Wilcox SR. "Rosen's Emergency Medicine 10th edition- Concepts and Clinical Practice E-Book". Elsevier Health Sciences. (2022). ISBN: 9780323757904
- Roettges P, Turker T. "Ulnar Nerve Injury as a Result of Galeazzi Fracture: A Case Report and Literature Review". Hand. 12(5). :NP162-NP165. (2017)
- Matthias R, Wright T. "Interosseous Membrane of the Forearm". J Wrist Surg. 05(03). :188-193. (2016)
- Eiff MP, Hatch RL. "Fracture Management for Primary Care and Emergency Medicine". Elsevier. (2019). ISBN: 9780323496346
- Walls R, Hockberger R, Gausche-Hill M. "Rosen's Emergency Medicine". Elsevier Health Sciences. (2018). ISBN: 9780323354790
- Pappas N, Bernstein J. "Fractures in Brief: Radial Head Fractures". Clin Orthop Relat Res. 468(3). :914-916. (2010)
- Swensen SJ, Tyagi V, Uquillas C, et al. "Maximizing outcomes in the treatment of radial head fractures". J Orthop Traumatol. 20(15). (2019)
- Wolfson AB. "Harwood-Nuss' Clinical Practice of Emergency Medicine". LWW. (2014). ISBN: 9781451188813
- de Muinck Keizer RJO, Walenkamp MMJ, Goslings JC, Schep NWL. "Mason Type I Fractures of the Radial Head". Orthopedics. 38(12). (2015)
- Foocharoen T, Foocharoen C, Laopaiboon M, Tiamklang T. "Aspiration of the elbow joint for treating radial head fractures". Cochrane Database Syst Rev. 22(11). (2014)
- Logan AJ, Lindau TR. "The management of distal ulnar fractures in adults: a review of the literature and recommendations for treatment". Strategies in Trauma and Limb Reconstruction. 3(2). :49-56. (2008)
- "Contributor Disclosures - Forearm fractures. None of the individuals in control of the content for this article reported relevant financial relationships with ineligible companies. For details, please review our full conflict of interest (COI) policy:"