Summary
Foreign body aspiration (FBA) is a potentially life-threatening emergency that most commonly occurs in children 1–3 years of age. A foreign body (FB) can become lodged in either the upper or lower airway and cause either a partial or complete airway obstruction. Complete obstruction of the larynx or upper trachea is a potentially life-threatening situation that causes severe respiratory distress, cyanosis, and suffocation; it should be managed with first-aid maneuvers (e.g., CPR in unresponsive patients or maneuvers to dislodge an aspirated FB in responsive patients) and, if needed, emergency airway procedures for FBA. Partial obstructions that do not cause significant respiratory distress can be removed via laryngoscopy, nasal endoscopy, or bronchoscopy if coughing fails to dislodge the FB. Lower airway FBA typically manifests with sudden-onset coughing and choking, followed by wheeze and dyspnea. Most commonly, the FB becomes lodged in the main and intermediate bronchi; approx. 60% of foreign bodies become lodged in the right main bronchus because of its more vertical orientation compared to the left main bronchus. If initial maneuvers fail to dislodge the FB and the patient is stable, imaging (e.g., x-ray of the neck or chest, CT chest, bronchoscopy) to localize the FB should be obtained, followed by a planned removal of the aspirated FB. If an FB remains undetected, it may result in chronic cough and recurrent pulmonary infections.
Epidemiology
-
Pediatric
- 80% of all cases occur in children < 3 years. [1]
- Peak incidence: 1–2 years
-
Adult
- FBA accounts for 0.16–0.33% of adult bronchoscopies. [2]
- Incidence: rises with age [3]
- Mortality rate: highest in patients 80–90 years of age [4]
Epidemiological data refers to the US, unless otherwise specified.
Etiology
-
Children and infants [5]
- Aspiration of a FB (e.g., of nuts, raisins, coins, toys) while chewing
- The risk of aspiration is higher if the infant or child is speaking, laughing, or playing while chewing.
- Toddlers are prone to examining objects with their mouth, and a sudden inspiration can result in aspiration. [1]
-
Adults
- Accidental aspiration
- Underlying conditions that increase the risk of aspiration [2]
- Neurological illnesses causing dysphagia
- Intoxication
- Altered mental status
- Neuromuscular disease
Pathophysiology
-
Aspiration of an FB → airway obstruction
- Complete airway obstruction → collapse of the respiratory structures distal to the obstruction (e.g., atelectasis)
- Partial airway obstruction: formation of a ball-valve obstruction with air trapping → build-up of pressure distal to the obstruction
-
Localization
- Upper airway obstruction: a minority of FB are lodged in the larynx or trachea
-
Bronchi: the right main bronchus is more often affected than the left main bronchus
- Aspirated particles are most likely to become lodged at the junction of the right inferior and right middle bronchi → right lower and middle lobe aspiration pneumonia
- Upper right lobe affected in bedridden patients, particularly while lying on their right side.
- In children, the two main bronchi are affected with similar frequency (compared to adults); however, there is still a slight right-sided predominance.
- Less severe than upper airway obstructions
Approximately 60% of foreign bodies become lodged in the right main bronchus because of its more vertical orientation compared to the left main bronchus.



References:[6][7]
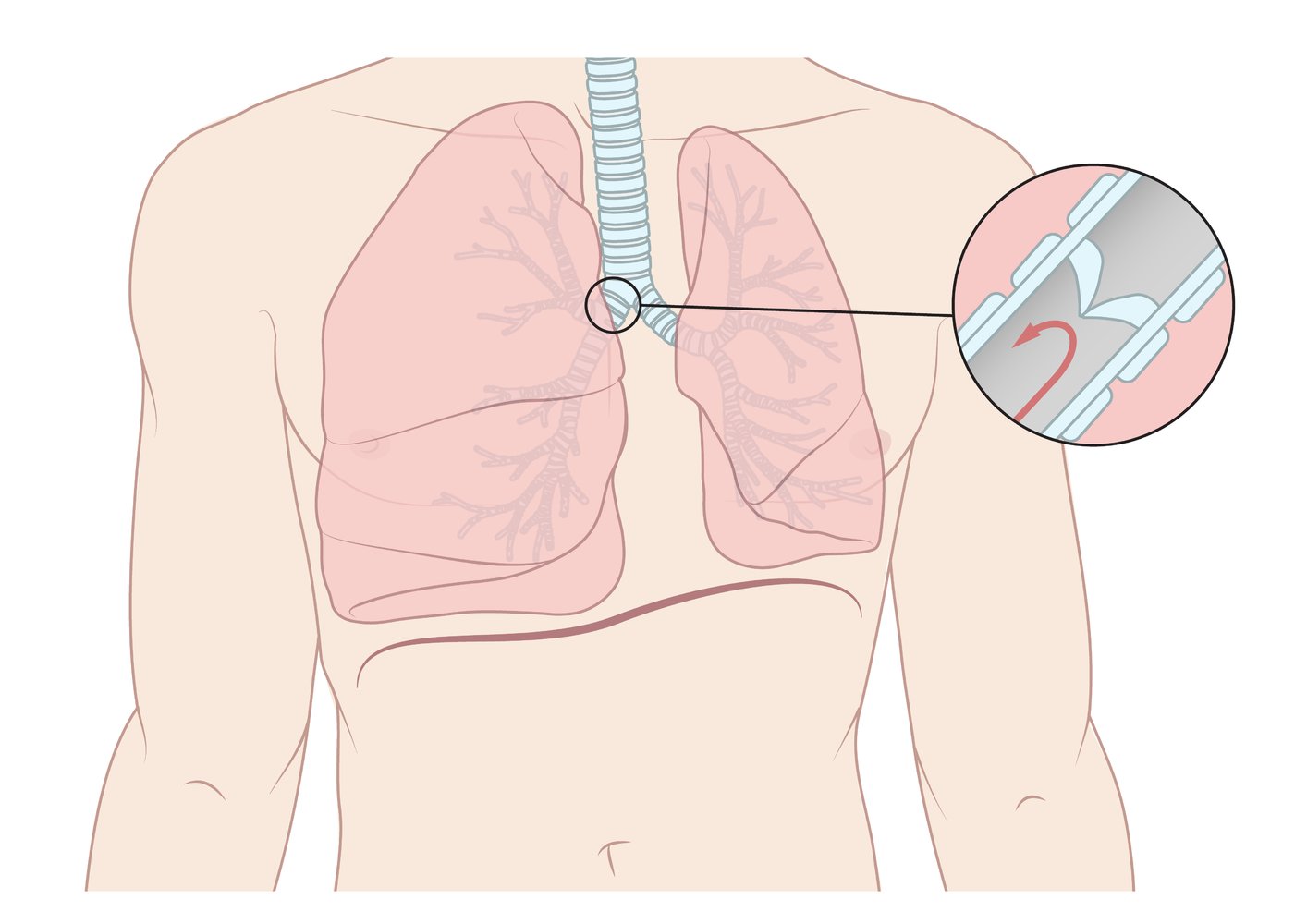
The foreign body functions as a one-way valve, allowing air to enter the lung during inspiration but blocking the passage of air back out during exhalation. This leads to hyperinflation of the lung on the side of the obstruction.
© AMBOSS
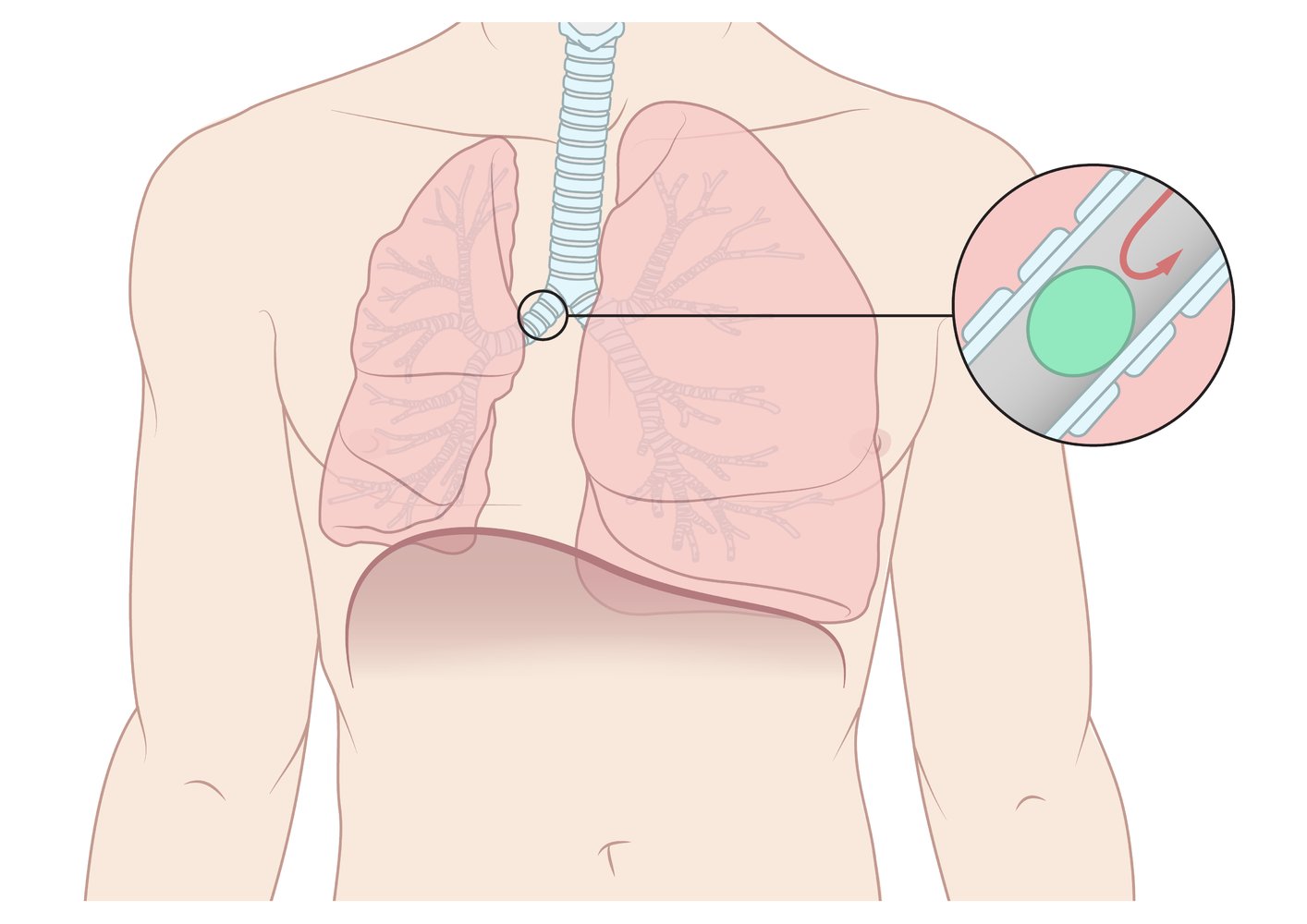
Complete obstruction with absence of ventilation
© AMBOSS
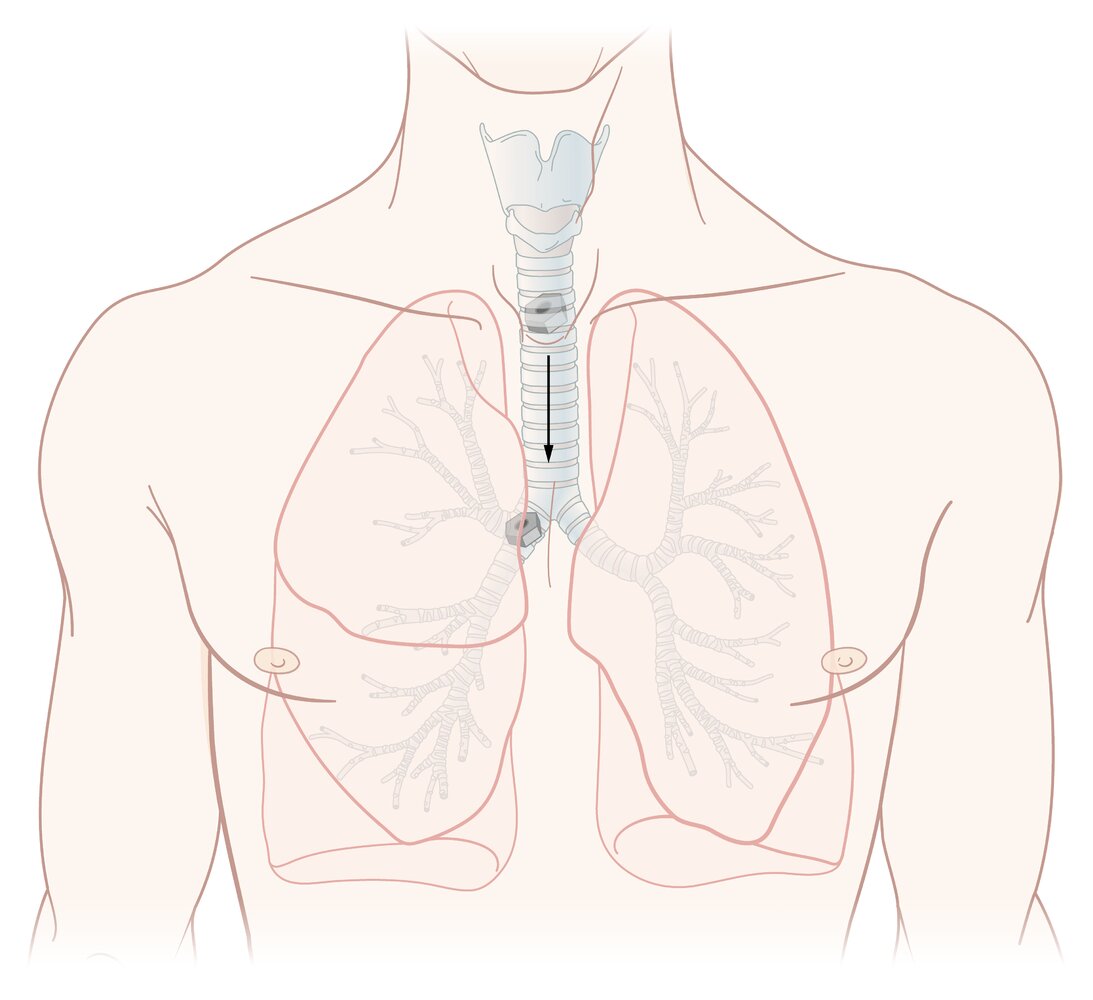
The right main bronchus is more commonly affected than the left main bronchus because it descends in a more vertical configuration.
© AMBOSS
Clinical features
Clinical features depend on the degree of airway obstruction and the duration of time since aspiration of the FB. See also “Upper airway FB obstruction” and “Lower airway FB obstruction” for differentiating features. [8]
| Clinical features in FBA | ||
|---|---|---|
| Complete airway obstruction [9] | Partial airway obstruction | Chronic FB airway obstruction |
|
|
|
Findings can change as organic foreign bodies absorb water and swell in the lung, converting a partial obstruction into a complete one. [6]
Differential diagnoses
-
Children
- See “Differential diagnoses of stridor”.
- See “Wheezing in children”.
- Acute obstructive bronchitis
- Laryngomalacia [10]
-
All ages [10]
- Tracheal blunt trauma, tumor, or stenosis
- Laryngeal trauma, tumor/papilloma
- Anaphylaxis
- Acute bilateral vocal cord paralysis
- Bronchial asthma (presents with bilateral wheezing, as opposed to the unilateral wheeze seen in FBA)
- Spontaneous pneumothorax
- Pneumonia
- Tracheobronchial tumor
- Extrinsic compression or infiltration of a large airway from an adjacent mass
The differential diagnoses listed here are not exhaustive.
Initial management (overview)
- Prioritize airway management and respiratory stabilization. [8]
- Defer diagnostic imaging if there are signs of respiratory distress or respiratory failure.
In patients with signs of life-threatening airway obstruction, immediately initiate critical interventions such as first aid (e.g., CPR), basic airway maneuvers, and emergency airway procedures for FBA (see “Unresponsive patients” below for details).
| Overview of diagnostic and therapeutic approach to FBA | ||
|---|---|---|
| Upper airway FB obstruction [11] | Lower airway FB obstruction [2] | |
| Physical findings |
|
|
| Initial imaging |
|
|
| Advanced imaging and/or dual diagnostic/therapeutic procedures |
|
|
| Management: unresponsive patient with suspected FBA |
|
|
| Management: responsive patient with suspected FBA |
|
|

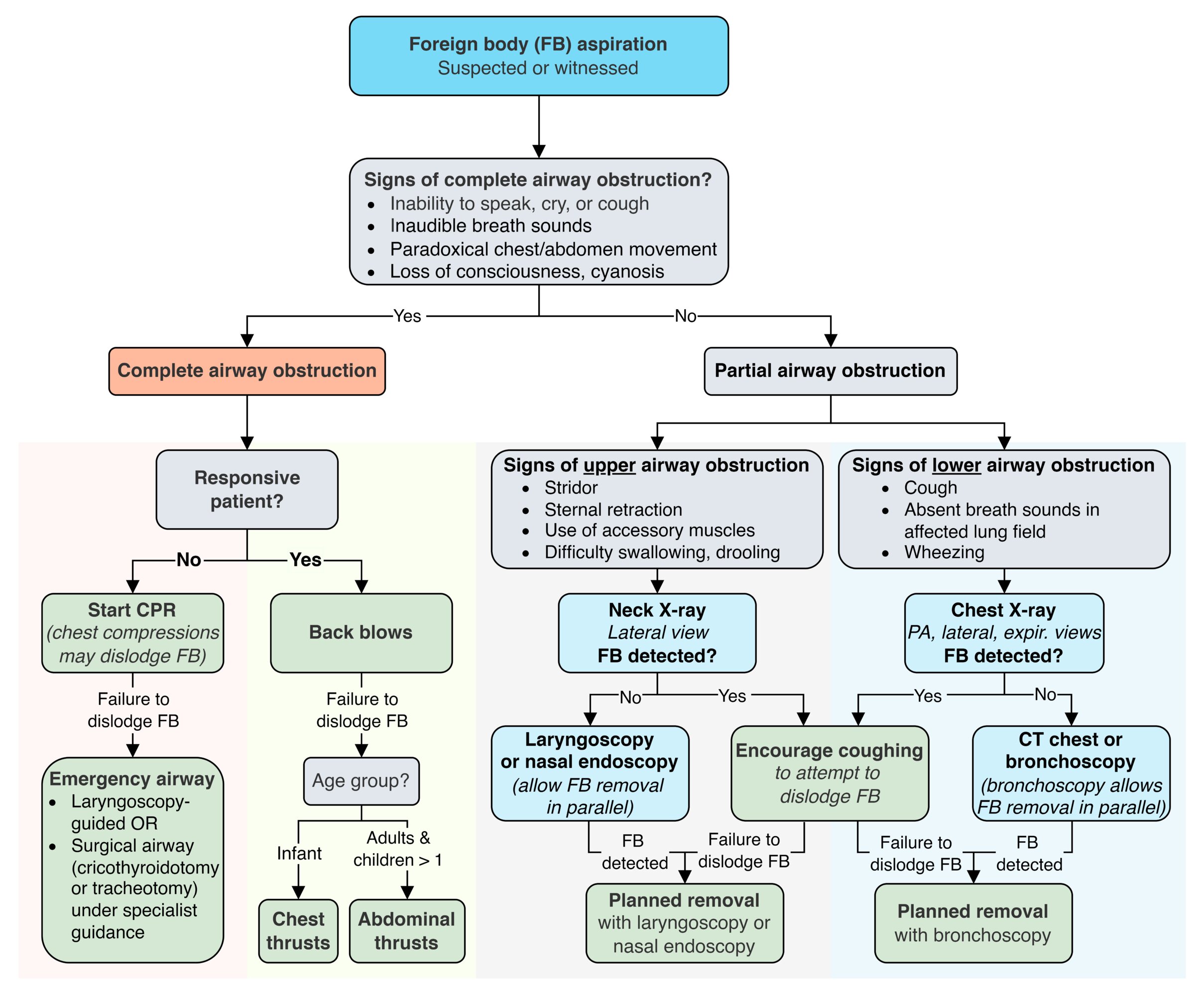
© AMBOSS
Unresponsive patient
Commence CPR
- Chest compressions may dislodge the object by raising intrapulmonary pressure. [12]
- Attempt to remove the FB while CPR is ongoing.
- Head-tilt/chin-lift maneuver to open the airway
- At every 2-minute pulse check, check the airway for a dislodged FB; remove if present.
- Do not perform blind finger sweeps if a FB is not visible. [13]
- Attempt laryngoscopy-guided FB retrieval.
Emergency airway procedures in FBA
- Indication: failed first-aid attempts to dislodge the FB
-
Anesthesia
- Unresponsive patients: none required
- Responsive patients: See “Planned removal of upper airway FB.”
Laryngoscopy [14]
- Laryngoscopy-guided FB retrieval: Under direct laryngoscopy, attempt to remove any visible FB with Magill forceps.
-
Inability to remove FB with forceps: Intubate using an endotracheal tube (ETT) to displace the FB as distally as possible into either main bronchus.
- Successful distal displacement: Withdraw the ETT to the standard tip-to-lip distance and ventilate if possible.
- Unsuccessful distal displacement: emergency surgical airway (see below)
Laryngoscopy risks converting a partial obstruction into a total obstruction by displacing the object or causing laryngeal trauma and/or hemorrhage [15]
Emergency surgical airway [16]
- Indication: failure of the above maneuvers to remove the FB in an unresponsive patient
-
Options
- Adults: scalpel cricothyroidotomy (or emergency tracheotomy if expertise is readily available) [17]
- Infants and children < 12 years old: needle cricothyroidotomy with percutaneous transtracheal ventilation [18]
-
Further management (after establishing an emergency airway)
- Planned removal of the aspirated FB.
- Urgently consult the relevant department (e.g., ENT, anesthesia) for a definitive airway as needed.



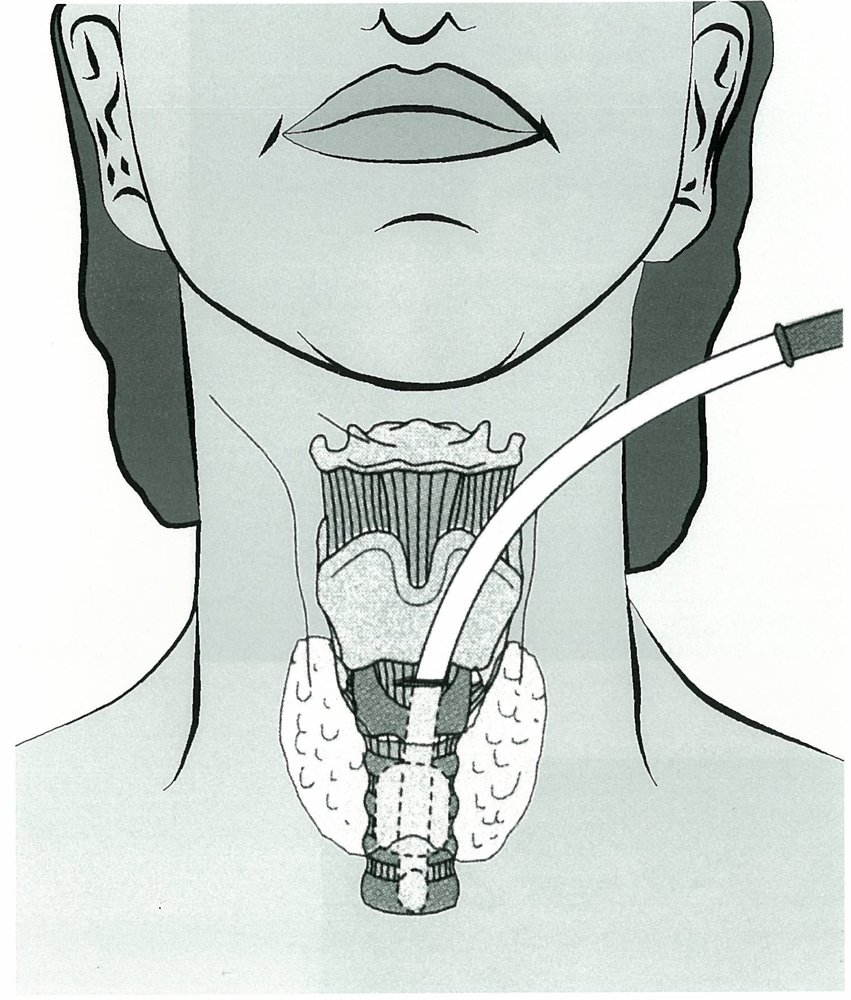
Diagram showing an emergency cricothyroidotomy, which is typically performed if attempts to intubate have been unsuccessful. An incision is made through the cricothyroid membrane, and a cuffed endotracheal tube is inserted through the incision site. Cricothyroidotomy allows ventilation of the patient until a more definitive airway is placed.
Source: © IMPP
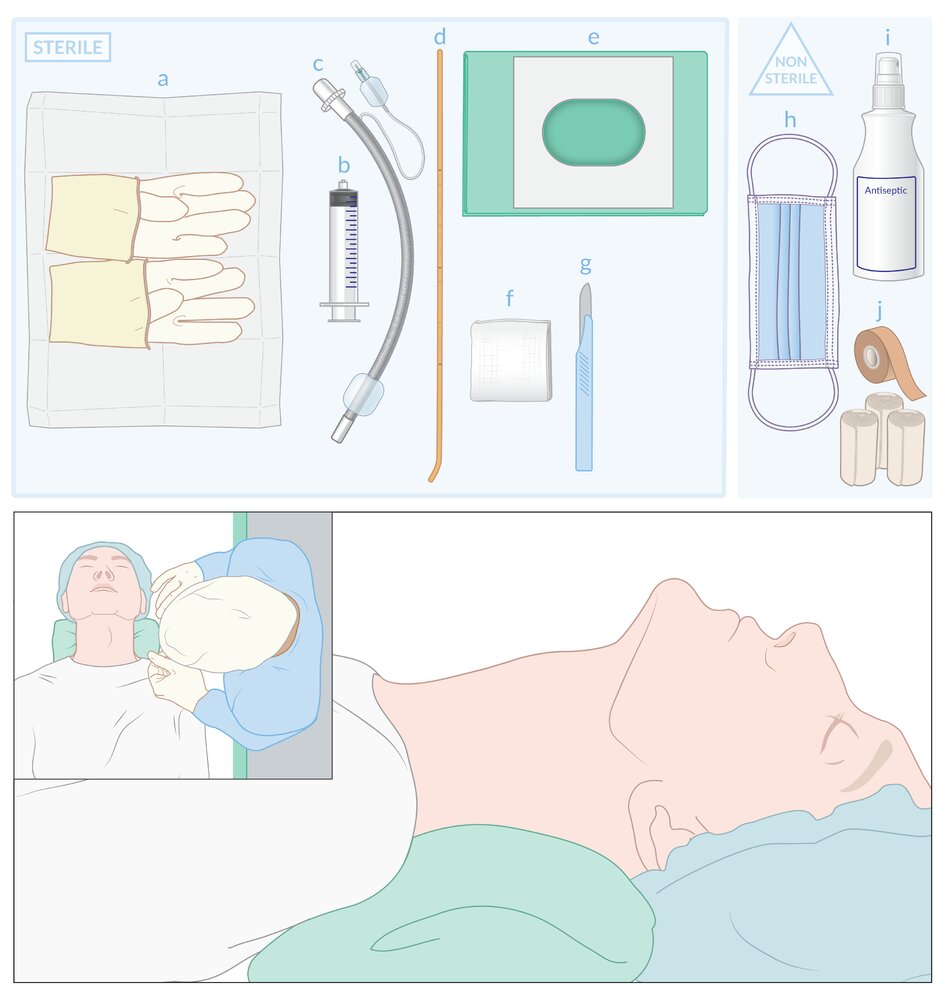
Preparation for surgical cricothyrotomy
Sterile equipment: (a) gloves, (b) syringe for cuff inflation, (c) endotracheal tube, (d) bougie with angled tip, (e) fenestrated drape, (f) gauze, (g) scalpel
Nonsterile equipment: (h) surgical mask, (i) antiseptic, (j) materials to secure the endotracheal tube (e.g., adhesive tape, bandage)
Patient and clinician positioning: The patient is positioned supine with their neck extended. Right-handed clinicians typically stand on the left side of the patient and left-handed clinicians typically stand on the right side.
© AMBOSS
Right-handed clinicians typically stand on the left side of the patient and left-handed clinicians typically stand on the right side.
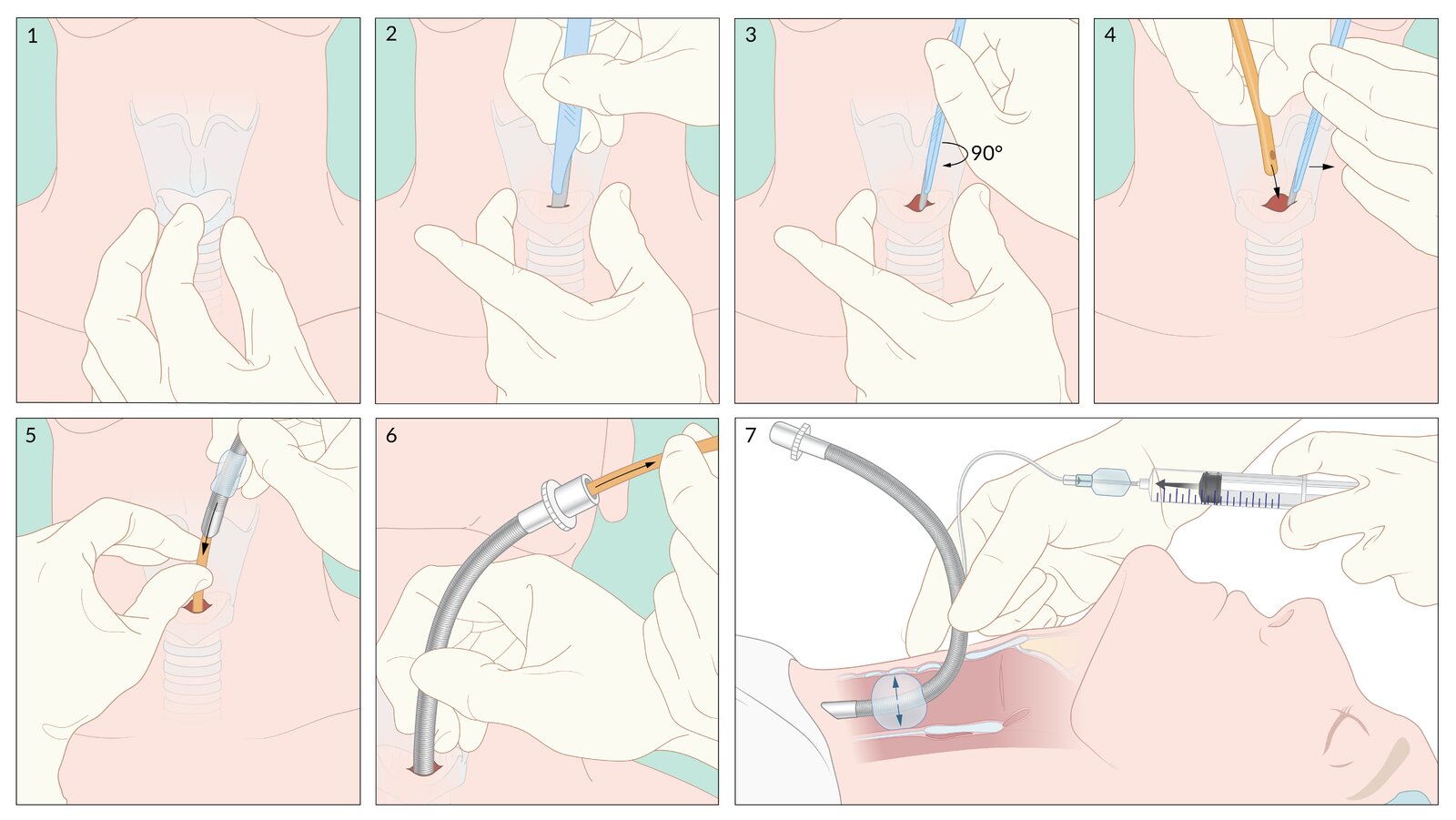
1. Landmark identification: With the nondominant hand, the larynx is stabilized between the thumb and middle finger, and the index finger palpates the cricothyroid membrane.
2. Stab: With the dominant hand, a transverse stab incision is made through the skin and cricothyroid membrane, with the cutting edge of the scalpel facing the clinician.
3. Twist: The scalpel is rotated 90° so that the cutting edge points toward the patient's feet.
4. Bougie: While keeping the scalpel in situ, the clinician swaps hands and holds the scalpel in the nondominant hand. The scalpel is kept vertical and is gently pulled toward the clinician to hold the incision open. Using the dominant hand, the tip of the bougie is inserted along the side of the scalpel into the trachea. After the bougie is advanced 10–15 cm into the trachea, the scalpel is removed.
5. Tube: The bougie is held firmly with the nondominant hand, ensuring it remains in place. With the dominant hand, the lubricated tracheal tube is threaded over the bougie and advanced into the trachea.
6. With the tube held firmly in place, the bougie is removed. Alternatively, the cuff may be inflated prior to bougie removal to stabilize the tube.
7. The cuff is inflated. Endotracheal tube position is then confirmed, the tube secured, and the patient ventilated using the same procedure and checks as for standard endotracheal intubation.
© AMBOSS
Responsive patient
Suspected complete airway obstruction (patient unable to speak, cry, or cough) [13]
If the patient can speak, cry, or cough, do not attempt back blows or abdominal thrusts, as these maneuvers risk dislodging the FB and converting a partial obstruction into a complete obstruction.
Approach
-
Initiate maneuvers to dislodge the aspirated FB (see table below for technique instructions).
- Back blows: preferred initial maneuver in all patients
-
If back blows are ineffective
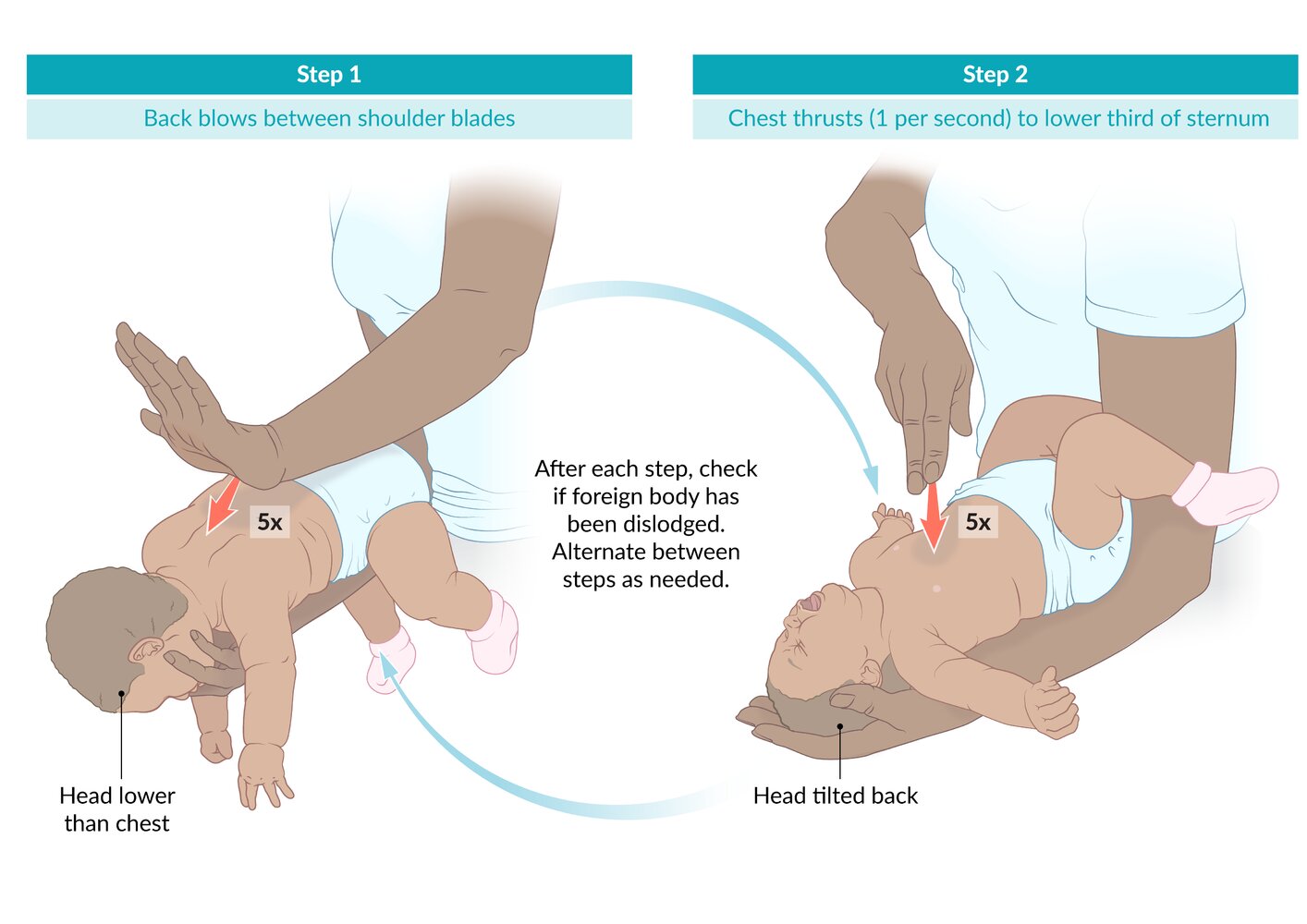
- Infants: Perform chest thrusts.
- Adults and children ≥ 1 year old: Perform abdominal thrusts (formerly known as the Heimlich maneuver). [19]
- Failure to dislodge the FB with repeated back blows and chest/abdominal thrusts
- If trained: Proceed with emergency airway procedures for FBA.
- Untrained or instruments not on hand: Continue maneuvers to dislodge the aspirated FB until help arrives.
-
Patient becomes unresponsive
- If trained, proceed to emergency airway procedures in FBA.
- If not trained, start CPR (see “Unresponsive patient”).
Technique
| Maneuvers to dislodge an aspirated foreign body | |
|---|---|
| Infants | Adults and children ≥ 1 year old |
| Initial maneuver: Back blows | |
|
|
| Next step: chest thrusts | Next step: abdominal thrusts [21][22] |
|
|


Suspected partial upper airway FBA
- Sit the patient upright.
- Encourage coughing to dislodge FB.
- Monitor for signs of deterioration.
- Signs of increased work of breathing
- Signs of poor gas exchange (e.g., cyanosis)
- Weak or ineffective cough
- Inability to dislodge the FB and patient remains stable: urgent ENT referral for planned removal of an upper airway FB
Suspected partial lower airway FBA
- Optimize oxygenation (see “Basic oxygen delivery systems”).
- Encourage coughing to dislodge the FB.
- Inability to dislodge the FB and patient remains stable: urgent pulmonology referral for planned removal of a lower airway FB
If at any time the patient becomes unresponsive despite treatment, start CPR, and, if trained, proceed to emergency airway procedures in FBA.
© AMBOSS
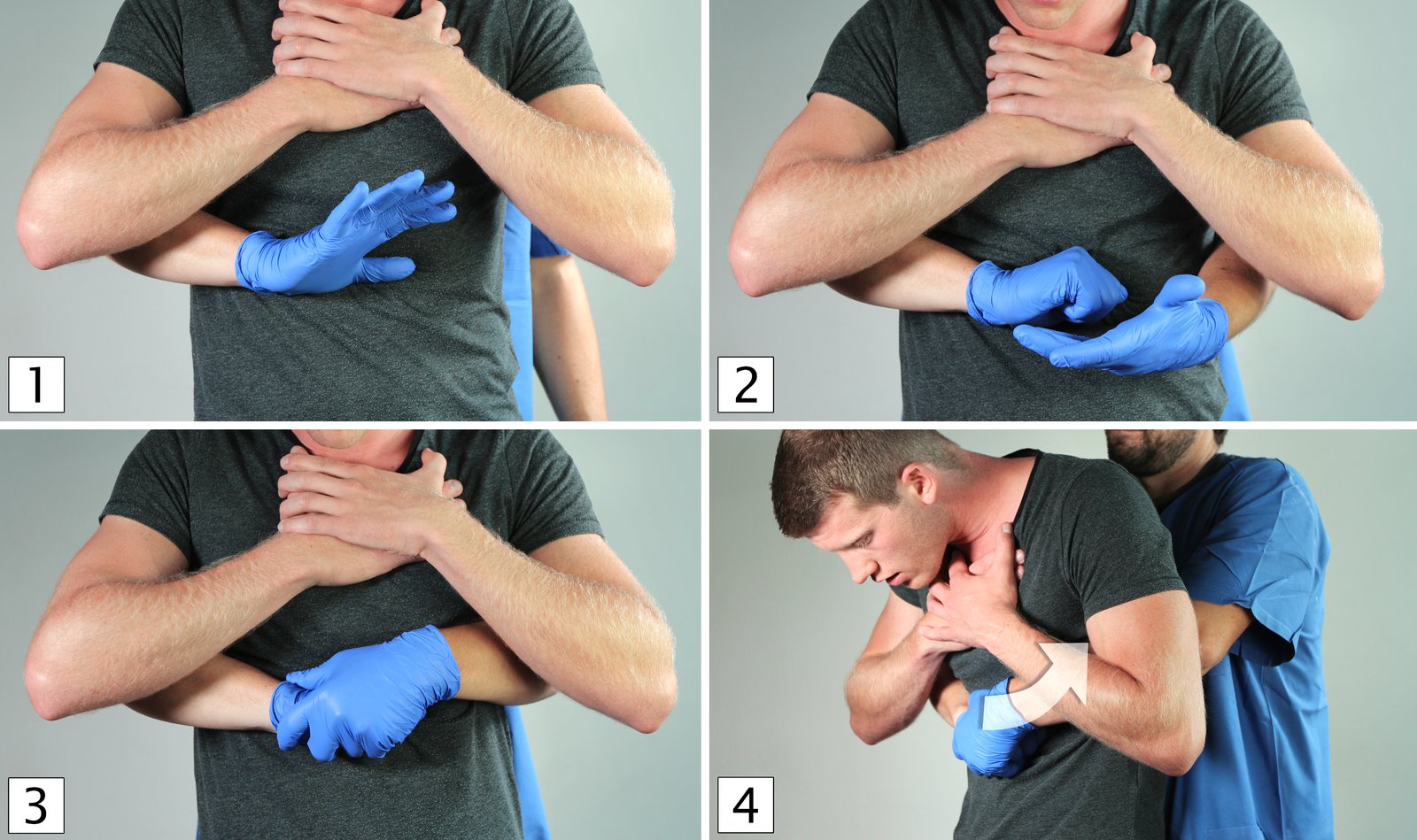
(1) The helper stands behind the patient and places their thumb under the xiphoid process, which is located on the upper abdomen.
(2) One hand is clenched into a fist.
(3) The fist is then grasped with the other hand.
(4) Several quick, upward abdominal thrusts are performed with both arms. This causes upward displacement of the diaphragm and, therefore, stimulates coughing. As a result, the foreign body can be mobilized and expectorated from the lower respiratory tract.
© AMBOSS
Diagnosis
Prioritize airway management and respiratory stabilization over diagnostics if there are any signs of respiratory distress or respiratory failure (see the “Initial management” sections above).
Imaging in suspected upper airway FBA
Neck x-ray (lateral view)
- Indications: suspected upper airway FB [23]
-
Findings
- Radiopaque foreign objects may be visible.
- Widened prevertebral shadow, loss of cervical lordosis (secondary signs) [24]
An x-ray may not detect a FB due to radiolucency or if the aspirated object is further down than suspected.

Laryngoscopy [25]
- Indications: next management step after failed first-aid attempts to dislodge an upper airway FB
-
Findings
- Direct visualization of the FB
- Potentially surrounding mucosal edema, abrasions, or blood
- Additional considerations: Nasal endoscopy can be used to remove a nasal FB or ensure there is no FB remnant in the upper airway that can be re-aspirated.
Imaging in suspected lower airway FBA
Chest x-ray [2]
-
Indications
- Initial screening modality in suspected lower airway FBA
- Exclusion of alternative diagnoses
-
Views
- PA, lateral, and expiratory
- Left and right lateral decubitus views in patients unable to cooperate with inspiratory/expiratory views [11]
-
Findings
- FB may be visualized if radiopaque (∼ 25%).
- Lung parenchyma changes suggestive of FBA are described in the table below.
-
Disadvantages
- False reassurance if chest x-ray is normal
- Insufficient detail for planning removal of FB; further imaging usually necessary
| Chest x-ray findings suggestive of FBA [2] | ||
|---|---|---|
| Early findings | Late findings | |
| Partial airway obstruction |
|
|
| Complete airway obstruction |
|
|



Chest x-ray may be normal in patients with FB aspiration.
If there is a high suspicion of FBA, CT chest or bronchoscopy should be performed even if the chest x-ray is inconclusive.
CT chest without contrast (∼ 100% sensitivity) [2]
-
Indications
- Second-line test in suspected lower airway FBA with a normal or inconclusive chest x-ray
- To guide planned removal of FB [2]
-
Findings
- Similar to chest x-ray
- Additionally includes: [27]
- Focal bronchial wall thickening adjacent to the FB
- Tree-in-bud opacities [28]
- Disadvantages: false-negative CT if the FB is very small or in patients with severe dyspnea [27]
Bronchoscopy [2]
Bronchoscopy is the gold standard diagnostic and therapeutic modality for a suspected lower airway FBA.
-
Indications
- Preferred modality in patients with signs of respiratory distress suspected to be due to a lower airway FB [2]
- Next step in stable patients high clinical suspicion of lower airway FBA despite inconclusive imaging.
-
Findings
- Direct visualization of the FB
- Granulation tissue if localized irritation has occurred
- Disadvantages: requires sedation and/or anesthesia
Investigation of the underlying causes
In adults with suspected neurological or neuromuscular abnormalities, consider a clinical swallow evaluation and other diagnostics for dysphagia. [29][30]
© AMBOSS

X-ray neck (lateral view)
An irregular opacity in the subglottic region (red overlay) is accompanied by airway narrowing (green overlay). The aspirated foreign body (a single tablet foil) is depicted in the top-right corner.
Source: “A Reclusive Foreign Body in the Airway: A Case Report and a Literature Review” by Ajay Philip, V. Rajan Sundaresan, Philip George, Satyabrata Dash, Regi Thomas, Anand Job, and V. K. Anand, Case Reports in Otolaryngology, licensed under CC BY 3.0. Modifications: Photo collage of two pictures. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).

X-ray chest (AP views; left: inspiratory; right: expiratory) of an infant with a history of suspected plastic toy aspiration
The mid and lower zones of the right lung appear hyperlucent on inspiration (green overlay). Hyperlucency persists on expiration, whereas the normal left lung and apical and upper zones of the right lung become more opaque on expiration. A foreign body in the bronchus intermedius was later retrieved by bronchoscopy.
Aspirated foreign bodies are often not radiopaque on chest radiography. The hallmark radiographic finding is a lung volume that does not appreciably change during the respiratory cycle (postobstructive emphysema; green overlay). The affected lung may appear overinflated and hyperlucent as a result of a check valve mechanism that allows air to enter but not exit. The hyperlucency may be accompanied by rib flaring or diaphragmatic depression.
Other findings that may indicate foreign body aspiration include atelectasis, mediastinal shift, and pneumonia. Lateral decubitus radiographs, fluoroscopy, and CT are also utilized to help diagnose foreign body aspiration.
Source: “Figure 1A+B, in: Subtle Crucial X-Ray Findings in Pediatric Foreign Body Aspiration” by Sekioka A, Koyama M, Fukumoto K, Nomura A, Urushihara N, Cureus, licensed under CC BY 4.0. Modifications: Images cropped, left/right images swapped, arrows and "A" and "B" markers removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
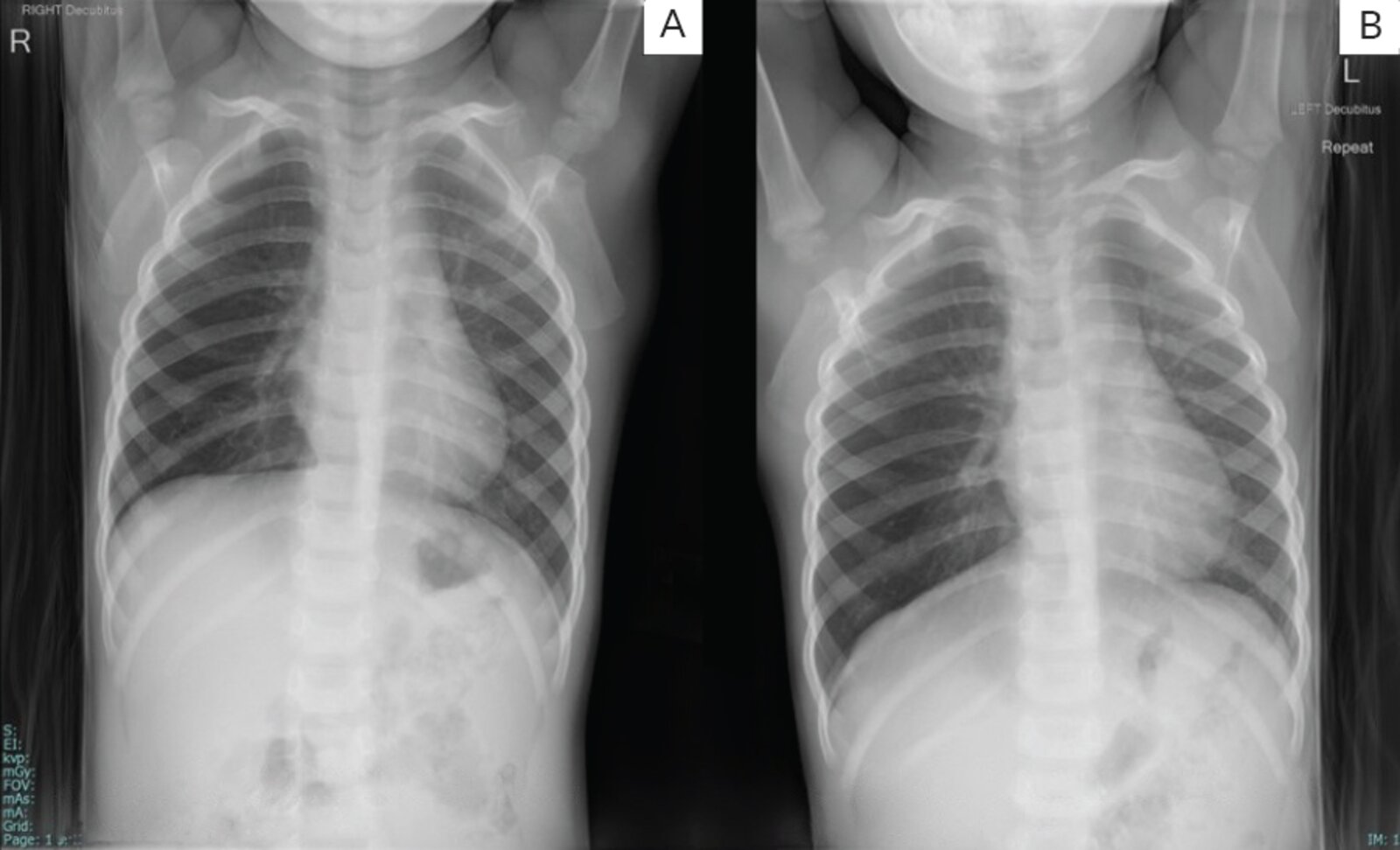
X-ray chest (lateral decubitus view; A: right lateral decubitus, B: left lateral decubitus) of a child who aspirated an almond
No radiopacity demonstrating the foreign body is seen. However, the right lung (red outlines) remains hyperinflated when the patient is positioned with the right side down on the radiographic table. The hyperinflation reflects air trapping from foreign body aspiration into the right main bronchus.
Decubitus radiographs are sometimes used to evaluate for the presence of an inhaled foreign body. The expectation is that a dependent lung will partially collapse in a normal patient, but will remain hyperinflated in the setting of an obstructive foreign body.
Green outlines: left lung
Source: “Fig. 15, in: Clinical presentation, diagnosis and management of aerodigestive tract foreign bodies in the paediatric population: Part 2” by Mathew R P, Liang T I, Kabeer A, Patel V, Low G, SA Journal of Radiology, licensed under CC BY 4.0. Modifications: Image was cropped, white area in between the images was recolored.. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
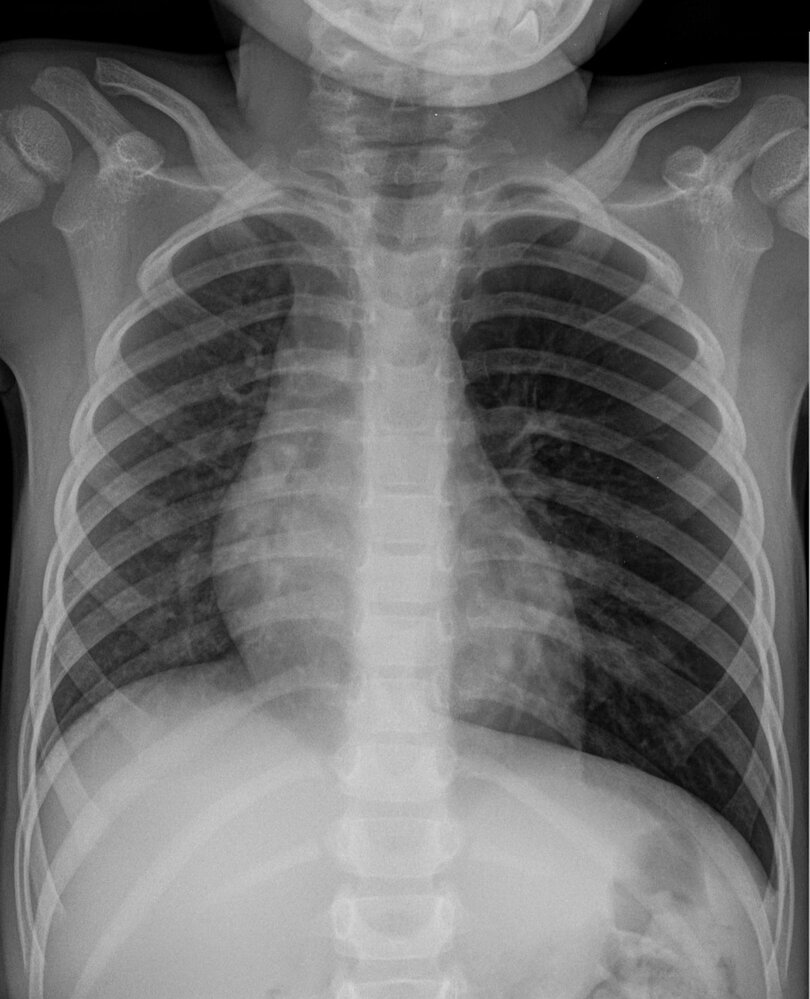
X-ray chest (PA view)
Hyperinflation of the left lung appears hyperlucent, with depression of the left hemidiaphragm (indicated by red lines and red arrow) and contralateral shift of the mediastinum (indicated by green outline, green hatched overlay, and green arrows). There is no pneumothorax or pneumomediastinum. The left main bronchus and its branches are not well seen in this patient as they project over the spine.
Hyperinflation of a lung due to a ball valve effect is a common presentation of foreign body aspiration.
Source: “Erdnussaspiration 3j - Roe pa - 001.jpg” by Hellerhoff, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
Treatment
Emergency management of suspected FBA is covered in the “Initial management” sections above.
This section describes procedures to remove a FB in stable/stabilized patients if CPR or initial maneuvers to dislodge the aspirated FB have failed.
Planned removal of an upper airway FB
- Indication: stable patients with an upper airway FB if attempted maneuvers to dislodge an aspirated FB have failed
-
Anesthetic considerations [15][31]
- Local anesthesia (1% topical lidocaine) can be considered in alert, cooperative patients with an oropharyngeal FB.
- If general anesthesia is required, IV induction with spontaneous breathing or smooth mask inhaled anesthesia is preferred. [5]
- Modalities: laryngoscopy (or nasal endoscopy)
- Procedure: Under direct visualization, the object is grasped and removed with forceps.
- Risks: Dislodgement of the object can lead to complete airway obstruction; keep equipment on hand to create an emergency surgical airway if needed.
Avoid positive pressure ventilation (e.g., bag-mask ventilation) during anesthesia induction in patients with suspected upper airway FBA as it can dislodge the FB more distally. [31]
Planned removal of a lower airway FB
Bronchoscopy (gold standard) [2]
- Indication: stable patients with confirmed/suspected lower airway FB if first-aid attempts to dislodge the FB have failed
- Type: flexible bronchoscopy or rigid bronchoscopy (see “Bronchoscopy choice in FBA”)
- Procedure: retrieval of the FB under direct vision [2]
-
Risks [32]
- Complete airway obstruction during removal; keep equipment on hand to create an emergency surgical airway if needed.[2]
- Pneumothorax
- Bleeding
- Infection (see “Aspiration pneumonia”)
- Injury of the tracheal/bronchial wall
-
Additional considerations: management of granulation tissue [2]
- Consider parenteral corticosteroids (e.g., methylprednisolone ) prior to bronchoscopy to reduce inflammation and assist FB removal. [2][33]
- Removal of granulation tissue during bronchoscopy may be required to prevent airway stenosis.
| Bronchoscopy choice in FBA [2][34] | |||
|---|---|---|---|
| Indications | Advantages | Disadvantages | |
| Flexible bronchoscopy |
|
|
|
| Rigid bronchoscopy |
|
|
|
Surgical management [2][33]
-
Indications
- Failure of bronchoscopy to remove the FB
- Destruction of surrounding lung tissue (e.g., bronchiectasis) in delayed presentations [35][36]
- Procedure: thoracotomy with bronchotomy or segmental resection
Acute management checklist
All patients
- Assess for signs of complete airway obstruction.
- Prioritize airway management and oxygenation.
Suspected complete airway obstruction
Unresponsive patient
- Start CPR
- Failure to dislodge FB with CPR: Proceed to emergency airway procedures for FBA.
Responsive patient
- Initiate maneuvers to dislodge the aspirated FB.
- Initial maneuver (all ages): Perform back blows.
- If ineffective
- Adults and children ≥ 1 year old: Perform abdominal thrusts.
- Infants: Perform chest thrusts.
Suspected partial upper airway FB obstruction or suspected lower airway FBA
- Encourage coughing.
- Provide oxygen if hypoxic.
- Urgent ENT consult (upper airway) or pneumology (lower airway)
- Stable patients: Obtain imaging to assist in planned removal of FB.
- All patients will require removal of the FB.
- Upper airway: laryngoscopy or nasal endoscopy
- Lower airway: bronchoscopy or rarely surgical resection
- Consider steroid therapy in lower airway FBA with granulation tissue.
- Adult patients with FBA should receive a workup for an underlying cause.
Complications
- Atelectasis
- Postobstructive pneumonia, lung abscess
- In complete obstruction
- Suffocation, asystole, and death
- Hypoxia: brain damage
References:[37]
We list the most important complications. The selection is not exhaustive.
References
- Wang K-P, Mehta AC, Turner JF, Jr. JF. "Flexible Bronchoscopy". John Wiley & Sons. (2012). ISBN: 9781405175876
- Hewlett JC, Rickman OB et al. "Foreign body aspiration in adult airways: therapeutic approach". J Thorac Dis. 9(9). :3398-3409. (2017)
- Boyd M, Watkins F, Singh S, et al. "Prevalence of flexible bronchoscopic removal of foreign bodies in the advanced elderly". Age Ageing. 38(4). :396-400. (2009)
- "Preventable-injury-related deaths by age and cause, United States, 1999-2018". https://injuryfacts.nsc.org/all-injuries/deaths-by-demographics/deaths-by-age/data-details/
- Fidkowski CW, Zheng H, Firth PG. "The anesthetic considerations of tracheobronchial foreign bodies in children: a literature review of 12,979 cases.". Anesth Analg. 111(4). :1016-25. (2010)
- Dikensoy O, Usalan C, Filiz A. "Foreign body aspiration: clinical utility of flexible bronchoscopy". Postgrad Med J. 78(921). :399-403. (2002)
- Blanco Ramos M, Botana-Rial M, García-Fontán E, Fernández-Villar A, Gallas Torreira M. "Update in the extraction of airway foreign bodies in adults". J Thorac Dis. 8(11). :3452-3456. (2016)
- Walls R, Hockberger R, Gausche-Hill M. "Rosen's Emergency Medicine". Elsevier Health Sciences. (2018). ISBN: 9780323354790
- Paradis NA, Halperin HR, Kern KB, Wenzel V, Chamberlain DA. "Cardiac Arrest". Cambridge University Press. (2007). ISBN: 9781139465700
- Darras KE, Roston AT, Yewchuk LK. "Imaging Acute Airway Obstruction in Infants and Children". Radiographics. 35(7). :2064-2079. (2015)
- Karnwal A, Ho EC, Hall A, Molony N. "Lateral soft tissue neck X-rays: are they useful in management of upper aero-digestive tract foreign bodies?". J Laryngol Otol. 122(8). :845-847. (2007)
- Chaffin PL, Grischkan JM, Malhotra PS, Jatana KR. "Endoscopic Management of Pediatric Airway and Esophageal Foreign Bodies". InTech. (2015). ISBN: 9789535121725
- Grillo HC. "Surgery of the Trachea and Bronchi". PMPH USA. (2004). ISBN: 9781550090581
- Abiramalatha T, Bansal A, Sudha S, Jhamb U. "Unusual Presentation of Foreign Body Aspiration as Pleural Effusion in an Infant". Indian J Pediatr. 81(3). :305-305. (2014)
- Colt H, Murgu S. "Bronchoscopy and Central Airway Disorders E-Book". Elsevier Health Sciences. (2012). ISBN: 9781455733316
- Miller WT, Panosian JS. "Causes and Imaging Patterns of Tree-in-Bud Opacities". Chest. 144(6). :1883-1892. (2013)
- McGinnis CM, Homan K, Solomon M, et al. "Dysphagia: Interprofessional Management, Impact, and Patient-Centered Care". Nutr Clin Pract. 34(1). :80-95. (2018)
- Ricci Maccarini A, Filippini A, Padovani D, et al. "Clinical non-instrumental evaluation of dysphagia.". Acta Otorhinolaryngol Ital. 27(6). :299-305. (2007)
- Llewelyn H, Ang HA, Lewis K, Al-Abdullah A. "Oxford Handbook of Clinical Diagnosis". Oxford University Press. (2014). ISBN: 9780199679867
- Walls R, Hockberger R, Gausche-Hill M. "Rosen's Emergency Medicine - Concepts and Clinical Practice". Elsevier Health Sciences. (2013). ISBN: 9780323390163
- Kendigelen P. "The anaesthetic consideration of tracheobronchial foreign body aspiration in children". J Thorac Dis. 8(12). :3803-3807. (2016)
- Papadimos T, Stahl D, Richard K. "Complications of bronchoscopy: A concise synopsis". Int J Crit Illn Inj Sci. 5(3). :189. (2015)
- Sehgal IS, Dhooria S, Ram B, et al. "Foreign Body Inhalation in the Adult Population: Experience of 25,998 Bronchoscopies and Systematic Review of the Literature". Respir Care. 60(10). :1438-1448. (2015)
- Yoon J-S, Kim K, Lee H, et al. "Foreign body removal by flexible bronchoscopy using retrieval basket in children". Ann Thorac Med. 13(2). :82. (2018)
- Lammy S, Pringle E, Carnochan F, et al. "Right lower lobectomy following inhalation of a toy traffic cone". JRSM Short Rep. 4(10). :204253331347669. (2013)
- Hasdiraz L, Oguzkaya F, Bilgin M, Bicer C. "Complications of bronchoscopy for foreign body removal: experience in 1035 cases". Ann Saudi Med. 26(4). :283-287. (2006)
- Jenkins B, McInnis M, Lewis C. "Step-Up to USMLE Step 2 CK". Lippincott Williams & Wilkins. (2015). ISBN: 9781496309747
- Berg RA, Hemphill R, Abella BS, et al. "Part 5: Adult Basic Life Support: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care". Circulation. 122(18_suppl_3). :S685-S705. (2010)
- Nolan JP, Maconochie I, Soar J, et al. "Executive Summary: 2020 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations". Circulation. 142(16_suppl_1). (2020)
- Walls, RM, Murphy MF. "Manual of Emergency Airway Management". Lippincott Williams & Wilkins. :317. ISBN: 9781451144918
- Lamberg JJ, Donahue KS. "Near-complete Upper Airway Obstruction from a Grape". Anesthesiology. 122(2). :435. (2015)
- DeVore EK, Redmann A, Howell R, Khosla S. "Best practices for emergency surgical airway: A systematic review". Laryngoscope Investigative Otolaryngology. 4(6). :602-608. (2019)
- American College of Surgeons and the Committee on Trauma. "ATLS Advanced Trauma Life Support". American College of Surgeons. (2018). ISBN: 9780996826235
- Lee SL, Kim SS, Shekherdimian S, Ledbetter DJ. "Complications as a Result of the Heimlich Maneuver". The Journal of Trauma: Injury, Infection, and Critical Care. 66(3). :E34-E35. (2009)
- Olasveengen TM, Mancini ME, Perkins GD, et al. "Adult Basic Life Support: 2020 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations". Circulation. 142(16_suppl_1). (2020)
- Berg MD, Schexnayder SM, Chameides L, et al. "Part 13: Pediatric Basic Life Support: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care". Circulation. 122(18_suppl_3). :S862-S875. (2010)
- American Heart Association. "Part 9: Pediatric Basic Life Support- International Guidelines 2000 for CPR and ECC". Circulation. 102(Suppl_1). :I-253-I-290. (2000)