Summary
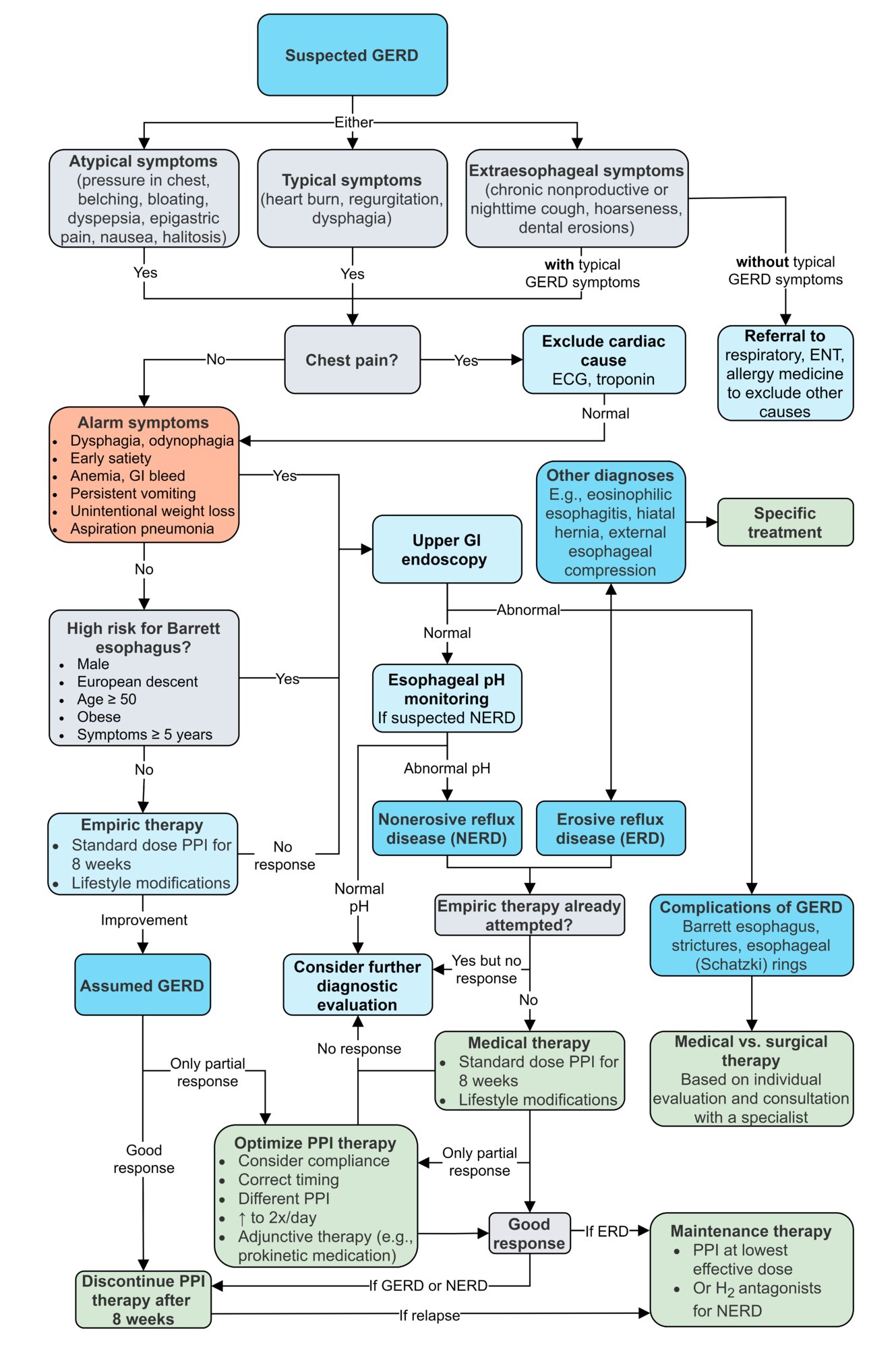
Gastroesophageal reflux disease (GERD) is a chronic condition in which stomach contents flow back into the esophagus, causing irritation to the mucosa. Reflux is primarily caused by an inappropriate, transient relaxation of the lower esophageal sphincter (LES). Risk factors include obesity, stress, certain eating habits (e.g., heavy meals or lying down shortly after eating), and changes in the anatomy of the esophagogastric junction (e.g., hiatal hernia). Typical symptoms are retrosternal burning pain (heartburn) and regurgitation, but the presentation is variable and may also include symptoms like chest pain and dysphagia. Most patients with suspected GERD should receive empirical treatment with proton pump inhibitors (PPIs). Diagnostic studies, e.g., esophagogastroduodenoscopy (EGD) and/or 24-hour pH test, may be indicated to confirm the diagnosis or to rule out other causes of symptoms. Management involves lifestyle modifications, medication, and, in some cases, surgery. Treating esophagitis is especially important because chronic mucosal damage can cause Barrett esophagus, a premalignant condition that can progress to adenocarcinoma.
Gastroesophageal reflux disease in children is detailed in a separate article.
Definitions
- Gastroesophageal reflux: regurgitation of stomach contents into the esophagus (can also occur in healthy individuals, e.g., after consuming greasy foods or wine)
-
Gastroesophageal reflux disease (GERD)
- A condition in which reflux causes troublesome symptoms (typically including heartburn or regurgitation) and/or esophageal injury/complications
- The most common endoscopic finding associated with esophageal mucosal injury is reflux esophagitis. [1]
- NERD (non-erosive reflux disease): characteristic symptoms of gastroesophageal reflux disease in the absence of esophageal injury, such as reflux esophagitis, on endoscopy (50–70% of GERD patients) [2]
- ERD (erosive reflux disease): gastroesophageal reflux with evidence of esophageal injury, such as reflux esophagitis, on endoscopy (30–50% of GERD patients) [2]
Epidemiology
- Prevalence: 15–30% in the US (increases with age) [3]
- Sex: ♀ = ♂
Epidemiological data refers to the US, unless otherwise specified.
Etiology
GERD develops when reflux-promoting factors, such as corrosiveness of the gastric juice, overcome protective mechanisms, such as the gastroesophageal junction and esophageal acid clearance.
Mechanisms
-
Gastroesophageal junction dysfunction can occur because of the following factors:
-
Increased frequency of transient lower esophageal sphincter relaxations (TLESRs) [4]
- TLESRs allow venting of accumulated gases to prevent distention of the stomach.
-
In individuals with GERD [5]
- About two-thirds of TLESRs are also accompanied by reflux of gastric content.
- The frequency of TLESRs increases.
-
Imbalance between intragastric and lower esophageal sphincter (LES) pressures [5]
- Reflux occurs when the intragastric pressure is higher than that created by the LES.
- LES tone can be decreased by substances such as caffeine and nitroglycerin, as well as by conditions that cause denervation of the muscle layer, such as scleroderma (see “Risk factors/associations” below).
- Intragastric pressure is increased in pregnancy, delayed gastric emptying, and obesity, among other conditions.
- Anatomic abnormalities of gastroesophageal junction (e.g., hiatal hernia, tumors)
-
Increased frequency of transient lower esophageal sphincter relaxations (TLESRs) [4]
- Impaired esophageal acid clearance [6]
- Normally, acid reflux is neutralized by salivary bicarbonate and evacuated back to stomach via esophageal peristalsis.
- Clearance can be disrupted by reduced salivation (e.g., due to smoking) and/or decreased peristalsis (e.g., due to inflammation).
Risk factors for GERD
- Smoking, caffeine and alcohol consumption [6][7][8]
- Stress [2]
- Obesity [9]
- Pregnancy [6]
- Angle of His enlargement (> 60°) [10]
- Iatrogenic (e.g., after gastrectomy)
- Inadequate esophageal protective factors (i.e., saliva, peristalsis) [6]
- Gastrointestinal malformations and tumors: gastric outlet obstruction, gastric cardiac carcinoma
- Scleroderma [6]
- Sliding hiatal hernia: ≥ 90% of patients with severe GERD [6]
- Asthma
Pathology
The histopathological findings include the following (may vary depending on the severity of mucosal damage): [11]
- Superficial coagulative necrosis in the nonkeratinized squamous epithelium
- Thickening of the basal cell layer
- Elongation of the papillae in the lamina propria and dilation of the vascular channels at the tip of the papillae (leading to hyperemia)
- Inflammatory cells (granulocytes, lymphocytes, macrophages)
- Transformation of squamous into columnar epithelium leads to Barrett metaplasia [12]



Click on the Smartzoom button to view the entire specimen through a virtual microscope.
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: PD Dr. med. Alberto Perez Bouza, Facharzt für Pathologie
Click on the Smartzoom button to view the entire specimen through a virtual microscope.
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: PD Dr. med. Alberto Perez Bouza, Facharzt für Pathologie
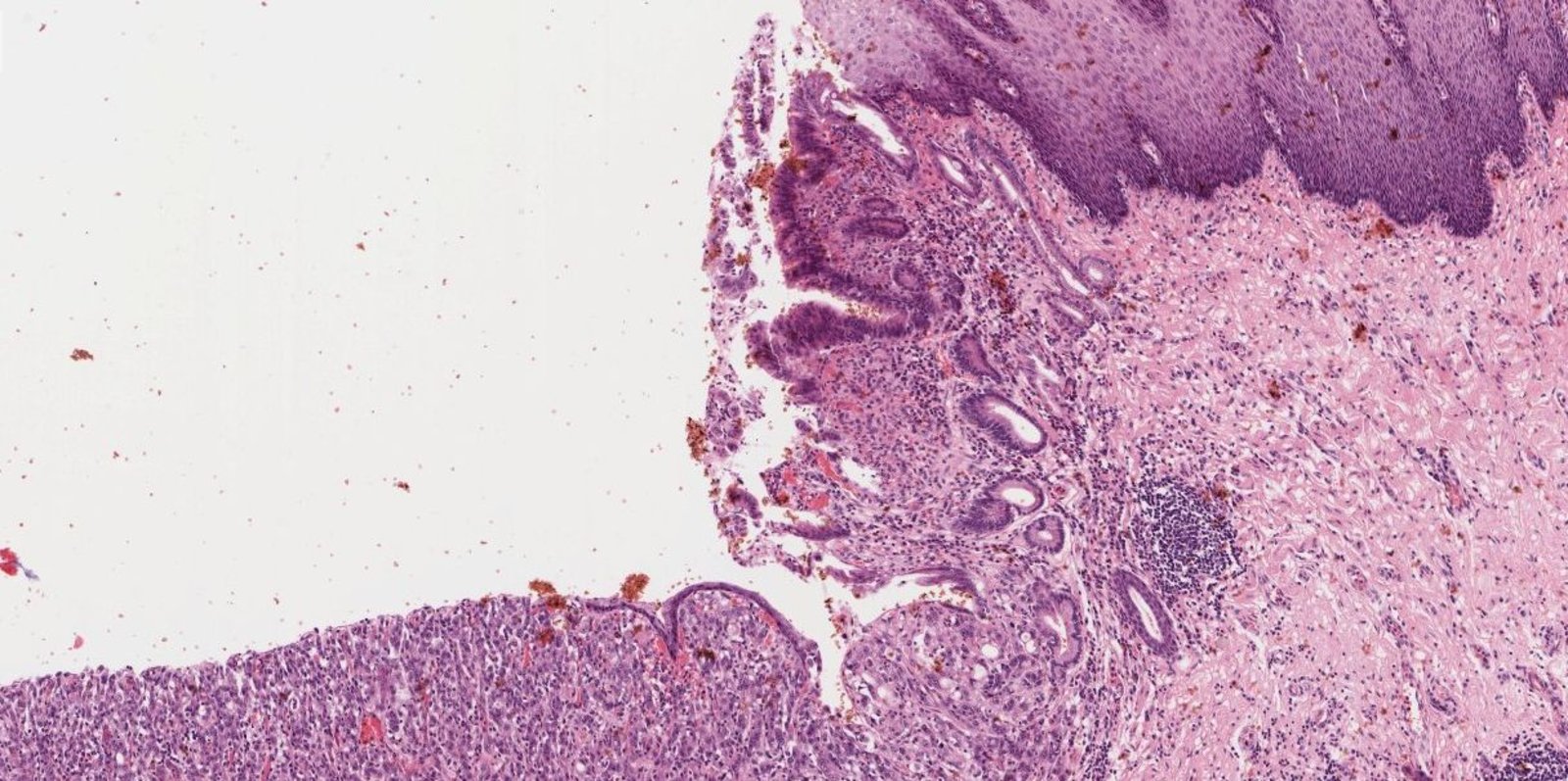
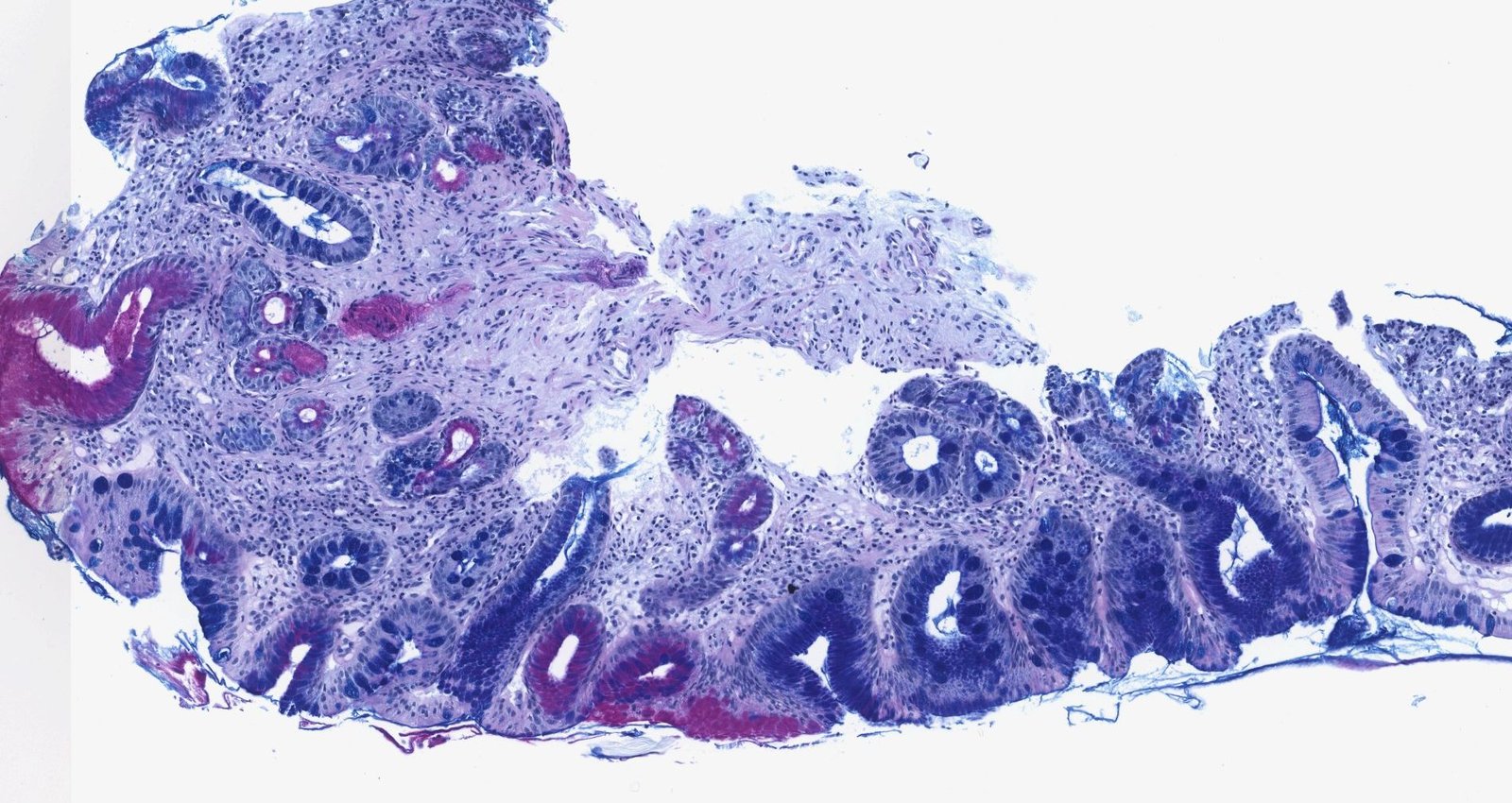
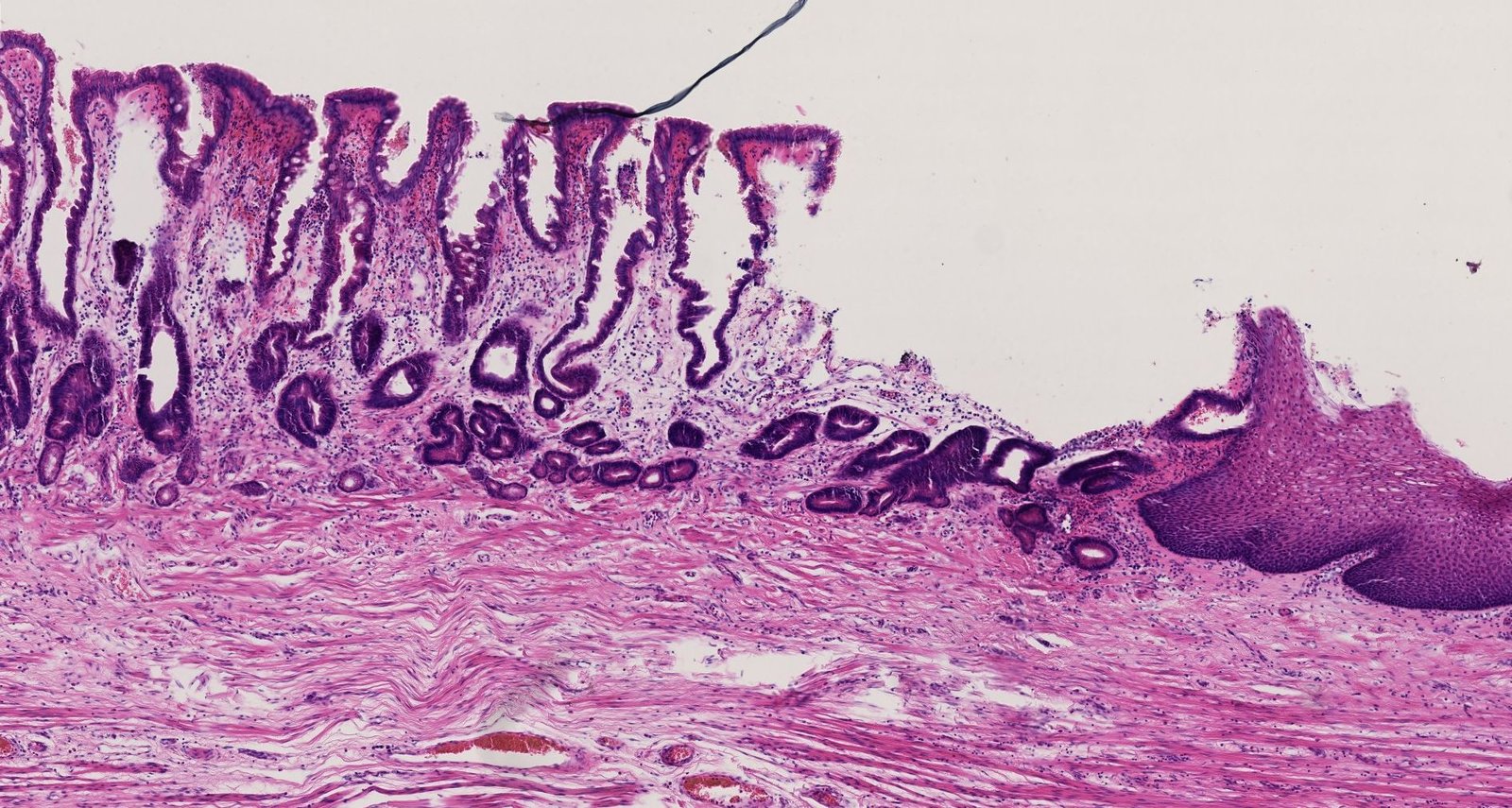
Photomicrograph of an esophageal tissue biopsy specimen (H&E stain; intermediate magnification)
The upper right edge of the image shows physiological multilayered squamous epithelium of the esophageal mucosa (white overlay), which changes into metaplastic prismatic epithelium with goblet cells (Barrett metaplasia; yellow overlay) toward the center of the image. Barrett metaplasia can eventually develop into epithelial dysplasia and, further, to adenocarcinoma of the esophagus (blue overlay). The carcinoma is characterized by loss of tissue architecture (atypical to absent gland formation) and invasive growth.
Click on the Smartzoom button to view the entire specimen through a virtual microscope.
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: PD Dr. med. Alberto Perez Bouza, Facharzt für Pathologie
Clinical features
Typical symptoms
- Retrosternal burning pain (heartburn)
- Regurgitation
- Dysphagia, odynophagia [13][14]
- Water brash: a symptom of excessive salivation triggered by refluxing of stomach acid
Atypical symptoms
- Pressure sensation in the chest/noncardiac chest pain
- Belching, bloating
- Dyspepsia, epigastric pain
- Nausea
- Halitosis
- Features of; GERD complications, e.g., aspiration pneumonia or aspiration pneumonitis
Extraesophageal symptoms [15]
- Chronic nonproductive cough and nighttime cough
- Hoarseness
- Bronchospasm
- Dental erosion
Aggravating factors
- Lying down shortly after meals
- Certain foods/beverages
Red flags in GERD [15]
- Dysphagia, odynophagia [13][14]
- Anemia and/or signs of GI bleeding (e.g., hematemesis, hematochezia)
- Unintentional weight loss
- Vomiting
- Presence of > 1 risk factors for Barrett esophagus
Consider investigating epigastric pain or burning lasting > 1 month (see “Approach to dyspepsia”). [15][16]
Differential diagnoses
-
Other causes of pain and discomfort
- See “Differential diagnoses of dyspepsia.”
- See “Differential diagnoses of chest pain.”
- See “Differential diagnoses of abdominal pain.”
-
Esophagitis
-
Infectious esophagitis (typically seen in immunocompromised patients)
- Esophageal candidiasis: Endoscopy shows white or yellow adherent plaques (pseudomembranes).
- Herpes esophagitis (mainly HSV-1): Endoscopy shows superficial, punched-out ulcers in the distal esophagus in the absence of plaques.
- CMV esophagitis: Endoscopy shows mucosal erosions and linear ulcers in the middle or lower esophagus, and viral inclusion bodies in cell nuclei on biopsy.
- Drug-induced esophagitis: Some medications may cause esophageal mucosal irritation, leading to erosions and ulcers. [17]
- Eosinophilic esophagitis
-
Infectious esophagitis (typically seen in immunocompromised patients)
Rule out acute coronary syndrome in patients with atherosclerotic risk factors before making a clinical diagnosis of GERD.





The differential diagnoses listed here are not exhaustive.
Endoscopic view of the esophagus
Multiple confluent, white-gray plaques in a longitudinal pattern are visible.
These findings are characteristic of Candida esophagitis.
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.
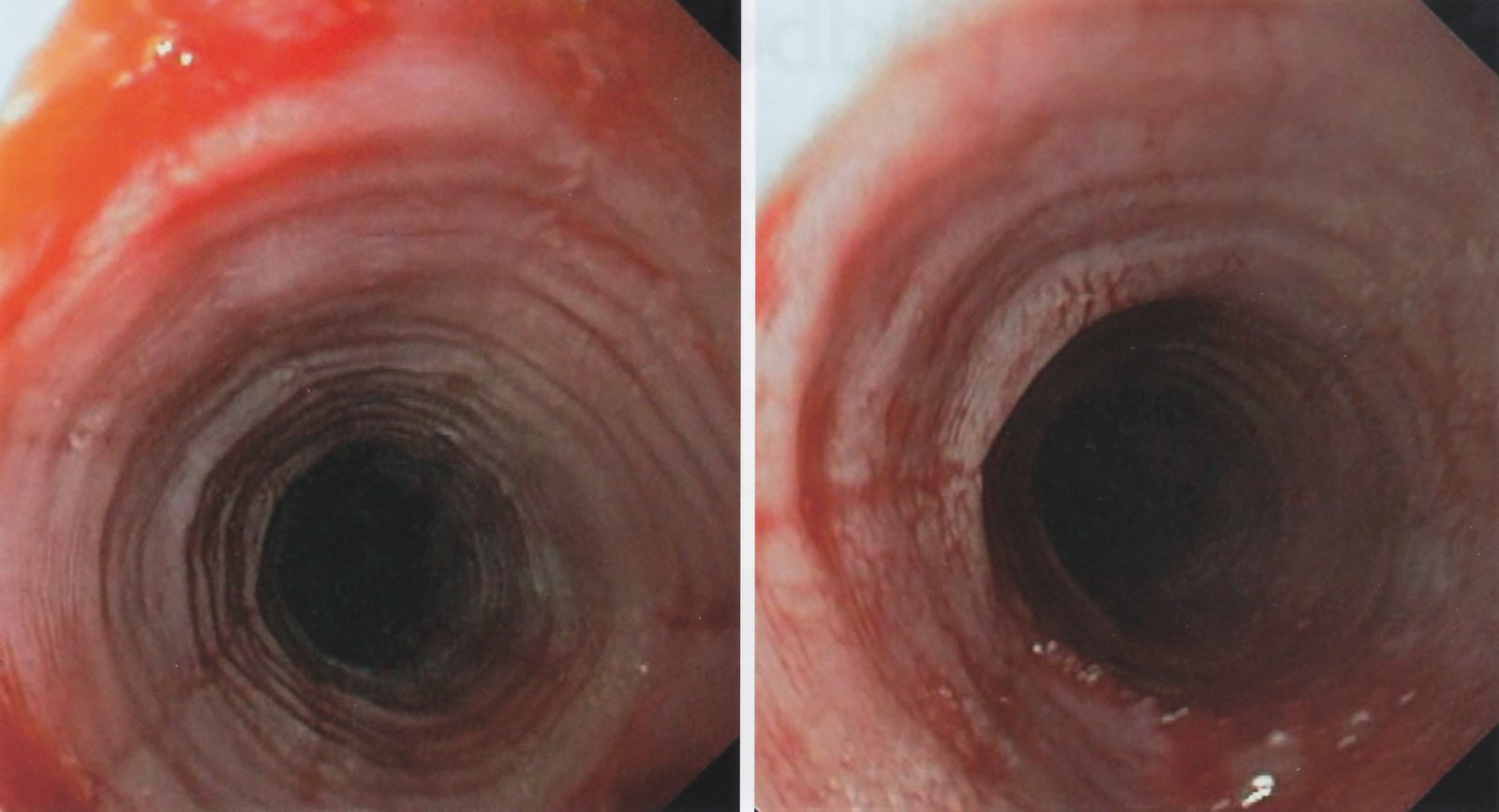
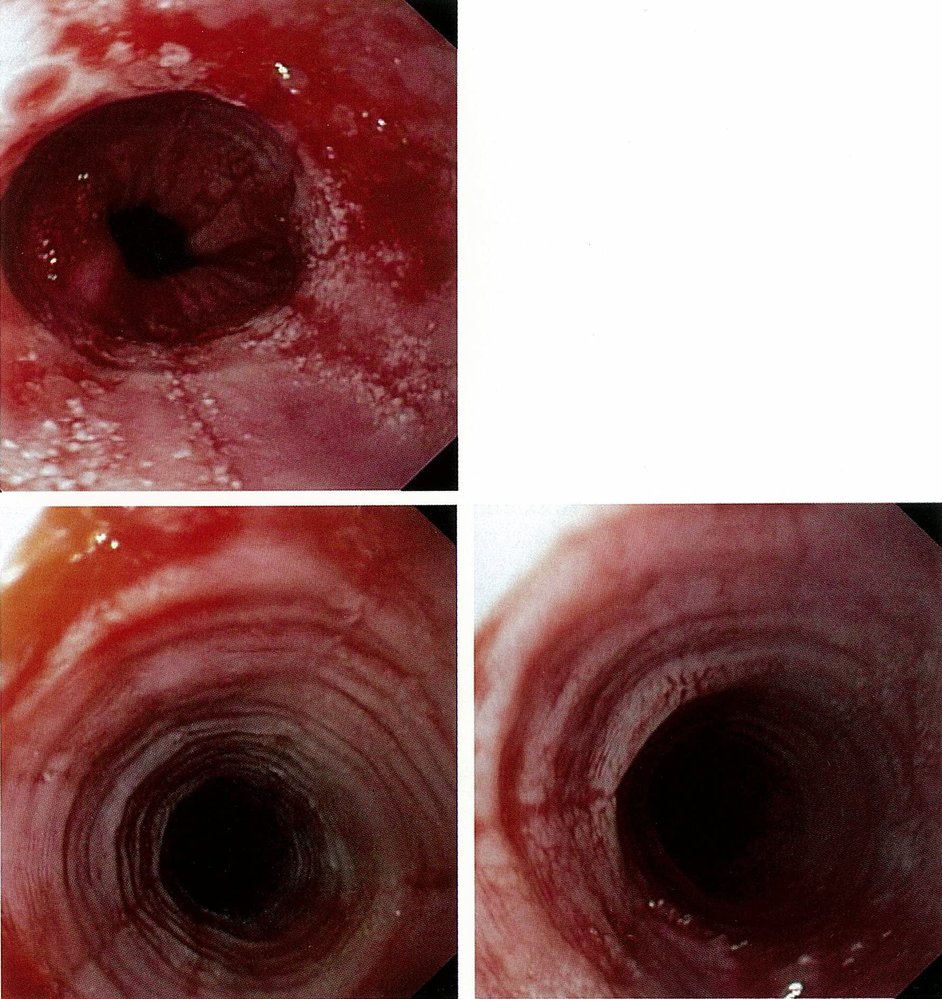
Endoscopic image of the esophagus
Circumferential lesions (examples indicated by green lines) and longitudinal furrows (examples indicated by blue lines) are visible along the esophageal mucosa. The pattern created by the repeated circumferential lesions is referred to as “trachealization” because it has a similar appearance to a trachea.
These are characteristic endoscopic features of eosinophilic esophagitis.
Source: © IMPP
Endoscopic image of the esophagus
Circumferential mucosal lesions (rings/corrugations; examples indicated by blue overlay) are visible.
Yellow lines: longitudinal furrows; Dashed encirclement: Z-line
Source: © IMPP
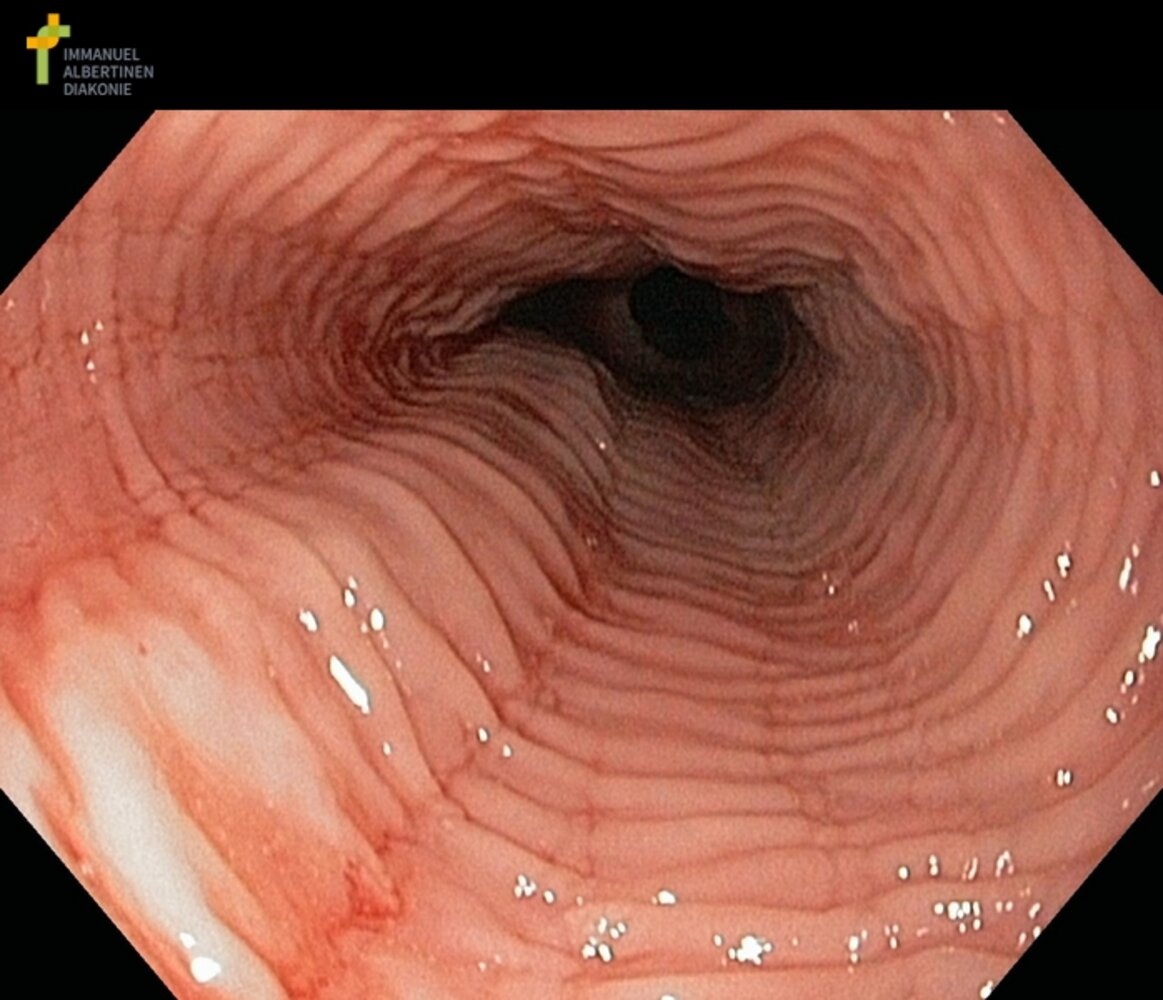
Endoscopic view of the esophagus
Circumferential rings (example indicated by green overlay) and longitudinal furrows (examples indicated by blue overlays) are visible along the esophageal mucosa.
These findings are characteristic of eosinophilic esophagitis.
Our great thanks to Albertinen Krankenhaus, Hamburg, Germany, for kindly providing this case.
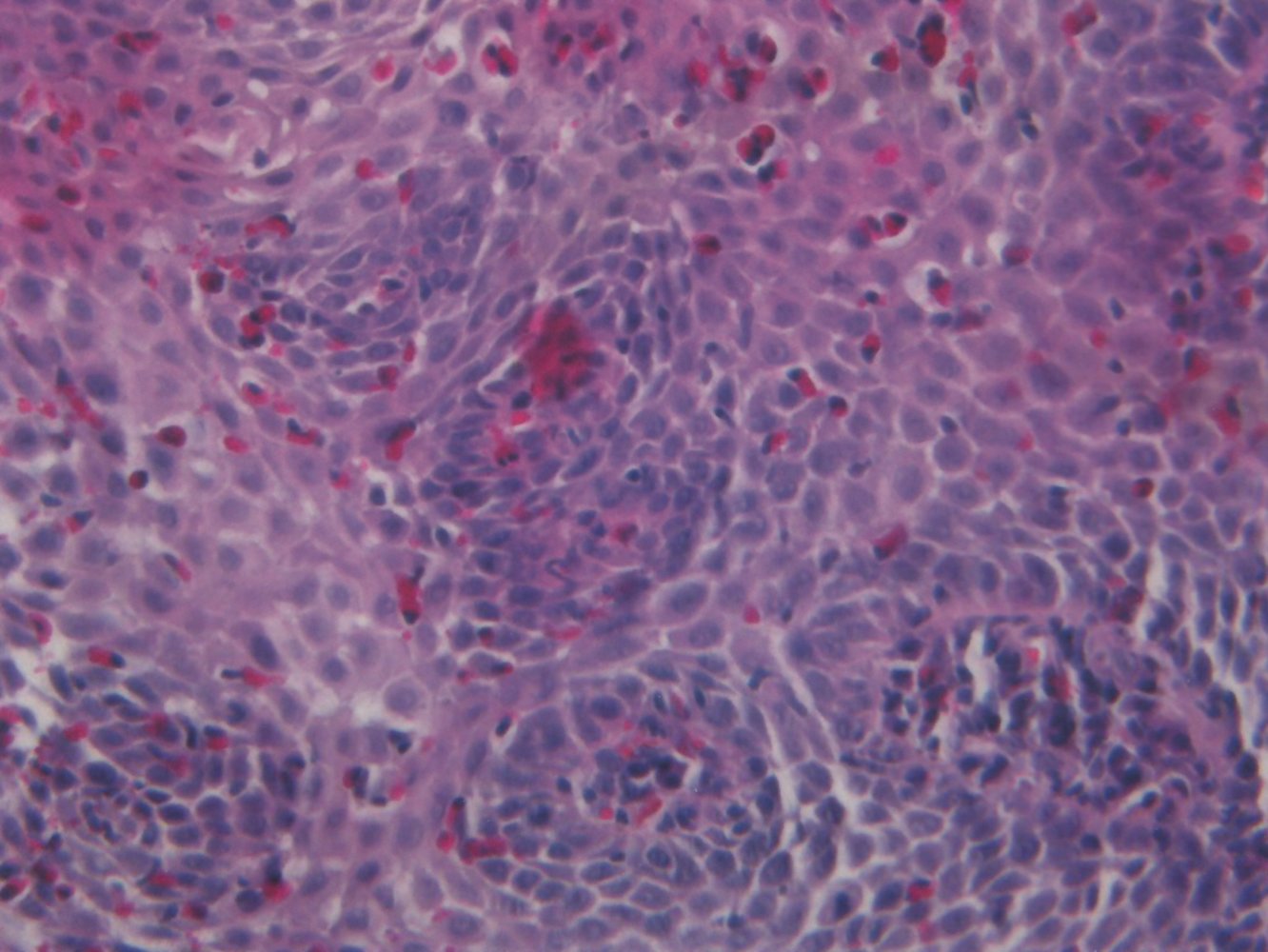
Photomicrograph of esophageal epithelial tissue (H&E stain, high magnification)
There are a large number of eosinophils present (examples indicated by green overlay). Some of these are clustered into eosinophilic microabscesses (white arrowheads), which are characteristic of eosinophilic esophagitis and help to differentiate it histologically from reflux esophagitis (in which there may also be many eosinophils present). The dilated intercellular spaces (black arrows) are a non-specific feature that is also present in reflux esophagitis.
Source: © IMPP
Diagnosis
There is no gold standard test for the diagnosis of GERD. The diagnosis is based on clinical presentation, endoscopic evaluation, reflux assessment, and therapeutic response. [15]
Approach [13][15]
-
All patients
- Perform a clinical evaluation, focusing on red flags in GERD and evaluating dyspepsia if present (see “Approach to dyspepsia”).
- Rule out life-threatening differential diagnoses of GERD and chest pain (e.g., acute coronary syndrome)
-
Typical symptoms without red flags in GERD: Initiate treatment for GERD; start an empiric once-daily PPI trial.
- If there is relief after 8 weeks of PPI: GERD is likely; PPI can be discontinued.
- If symptoms persist on PPI or recur after discontinuing PPI: Refer to gastroenterology for EGD. [15]
- Red flags in GERD: Refer to gastroenterology for EGD before initiating treatment.
- Extraesophageal symptoms: Rule out other diagnoses prior to initiating treatment for GERD.
-
Refractory symptoms: Optimize PPI therapy.
- If symptoms are relieved: Continue PPI.
- If symptoms persist: Refer to gastroenterology.
Resolution of chest pain with antacids is not diagnostic for GERD and does not rule out life-threatening causes of chest pain. [18]
GERD is common during pregnancy and usually subsides after delivery; diagnostic workup is rarely necessary.

EGD [15][19][20][21]
-
Indications
- Red flags in GERD
- Risk factors for Barrett esophagus
- No symptomatic improvement after PPI trial
- Red flags of dyspepsia
-
Supportive findings (typically in the lowest third of the esophagus) [22]
- Erythema, edema, friability
- Erosions, mucosal breaks, ulcerations
- Peptic strictures and rings
- Salmon pink mucosa (suggestive of Barrett esophagus)
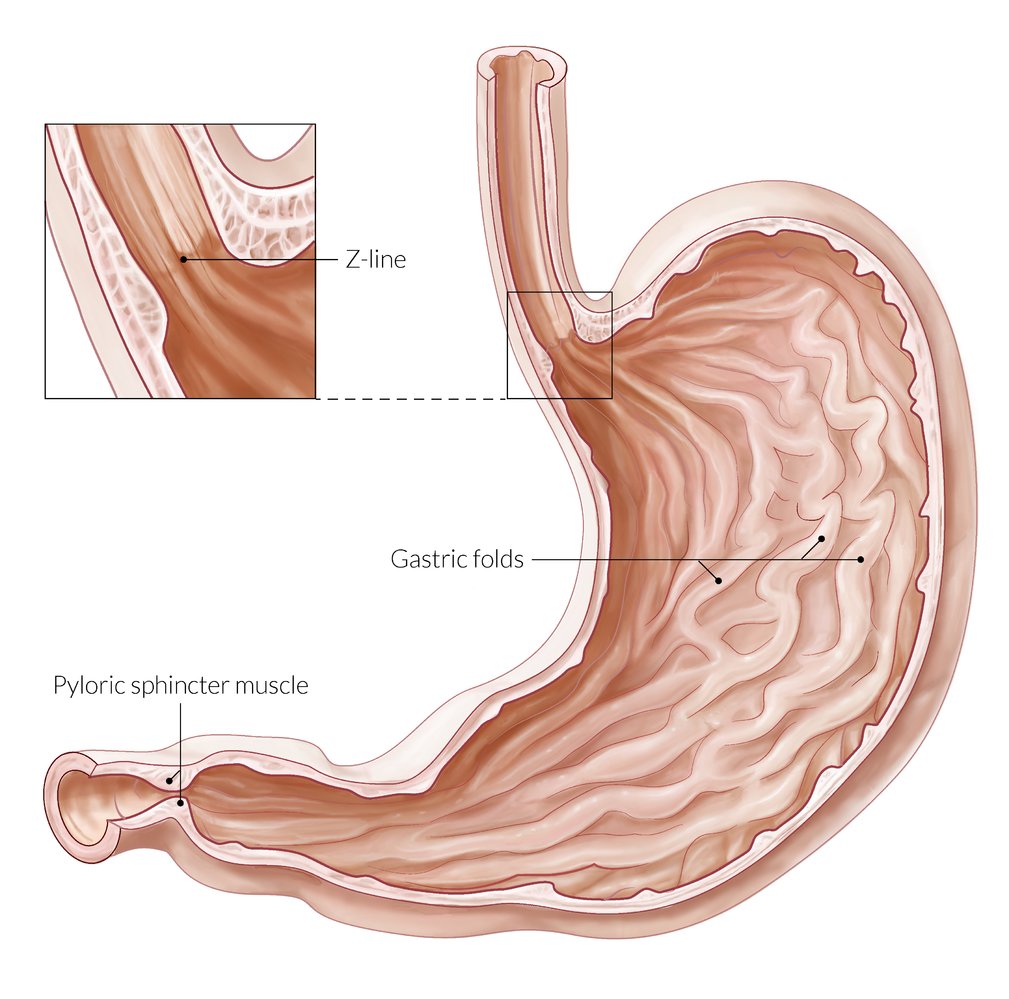
- Proximal migration of the gastroesophageal junction (Z line), e.g., in Barrett esophagus or hiatal hernia [23]
-
Biopsies
- Esophageal biopsies have little value as a diagnostic test for GERD. [15]
- Consider for exclusion of other diagnoses or complications (e.g., eosinophilic esophagitis, Barrett esophagus).
- See “Pathology” for histological findings.
> 50% of patients with GERD present with nonerosive reflux and normal endoscopic findings. [24]
Despite the limited value of esophageal biopsies in diagnosing GERD, they are necessary for establishing a diagnosis of eosinophilic esophagitis. [15]

Esophageal pH monitoring [15][22]
Esophageal pH monitoring can be used to objectively identify abnormal reflux of gastric content into the esophagus; however, it is not a routine diagnostic test. [15]
-
Indications
- Refractory GERD symptoms despite PPI therapy
- Confirmation of suspected NERD
- Evaluation before surgical or endoscopic antireflux procedure
-
Procedure
- Measurement of esophageal pH over 24–48 hours using a telemetry capsule or a transnasal catheter
- Documentation of relevant events by the patient
- Supportive finding: Drops in esophageal pH to 4 or less that correlate with symptoms of acid reflux and precipitating activities. [25]
Further diagnostic studies [15][22]
Not routinely indicated, as they play a limited role in the diagnosis of GERD; useful if endoscopy is inconclusive.
-
Esophageal barium swallow
- Consider if the main symptom is dysphagia or if there is suspicion of structural abnormalities (e.g., esophageal rings or webs) or motility disorders (e.g., achalasia, distal esophageal spasm)
- See “Diagnostics” in “Dysphagia”.
- Esophageal manometry: Consider if achalasia or esophageal hypermotility disorders are suspected. [26]
© AMBOSS
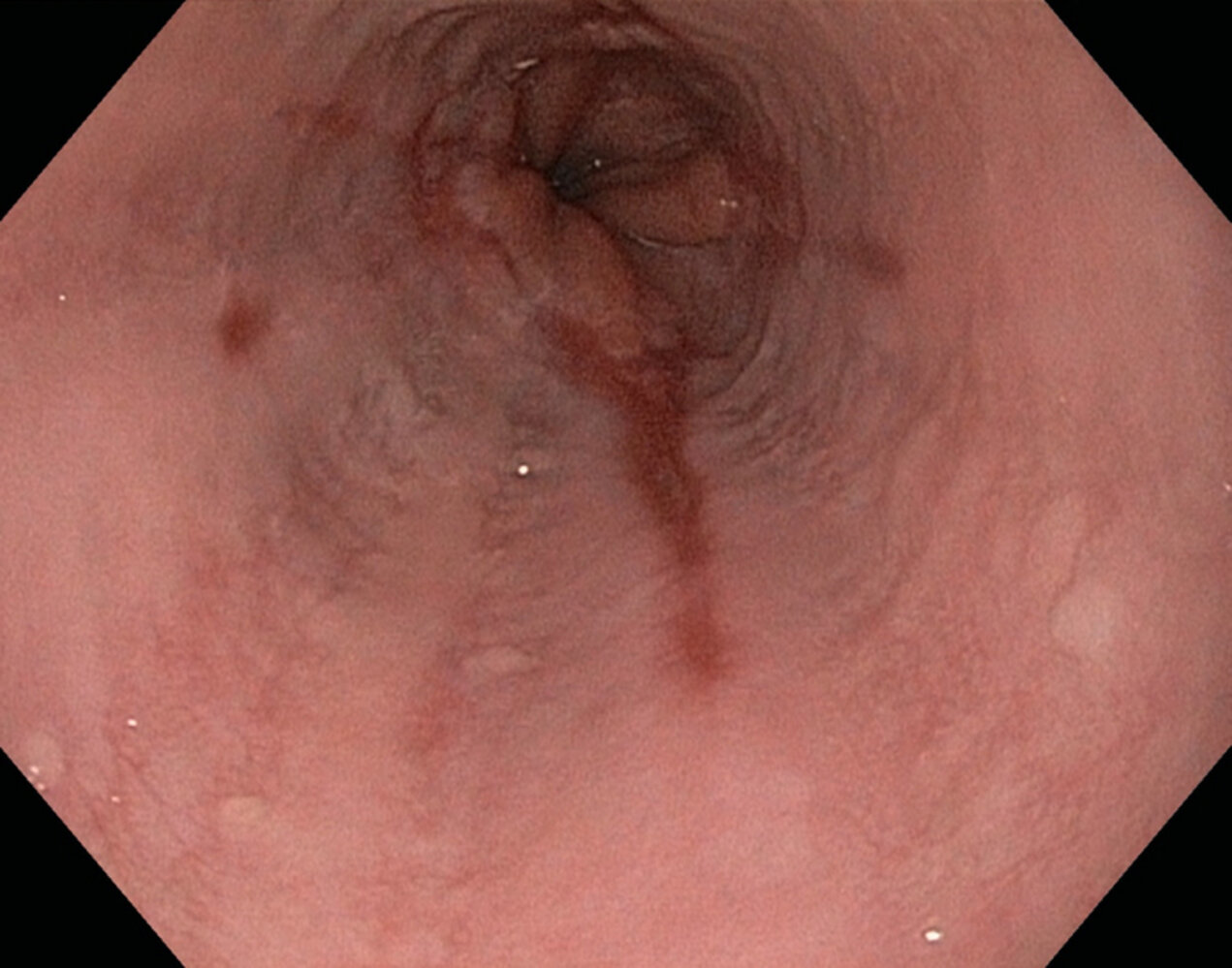
Endoscopic view of the esophagus
Several linear and round erosions (purple overlay) can be seen proximal to the Z-line (dashed outline).
These features are pathognomonic of erosive esophagitis.
Source: © IMPP
Treatment
The initial management of GERD consists of implementing lifestyle changes and initiating acid suppression therapy, preferably with PPIs. Surgical therapy is not routinely indicated and should only be considered in select cases, e.g., patients who develop complications despite receiving optimal medical therapy.
Pharmacological therapy [15][20]
See “Antacids and acid suppression medications” for agents, detailed dosages, and pharmacological considerations.
-
PPIs: standard dose of PPI for 8 weeks
- Indications
- Empiric PPI trial in patients with typical symptoms
- After EGD: ERD or presumed NERD
- Continuous management (based on the clinical response after 8 weeks) [27]
- Good response and no complications: Discontinue PPI.
- Good response in patients with complications : Continue PPI at maintenance dose. [15]
- Partial response: Increase dose (to twice-daily therapy), adjust timing, or switch to a different PPI.
- Recurrence of symptoms after discontinuation of PPI or during weaning: Consider confirming the diagnosis (e.g., with ambulatory esophageal pH monitoring) prior to continuing maintenance therapy.
- No response: further diagnostic evaluation
- There is controversy surrounding the risks of long-term PPI therapy [28][29][30][31]
- Indications
- H2 receptor antagonists: Consider as alternate maintenance therapy for NERD, or in addition to PPIs to control nighttime symptoms
- Maintenance therapy: lowest effective dose of acid suppression medication
-
Adjunctive therapy: Consider adding in patients with partial response to PPIs; Not recommended without confirmatory diagnostic studies
- Prokinetic medication for patients with gastroparesis: e.g., metoclopramide
- Baclofen (off-label) for refractory symptoms
A negative response to a PPI trial does not exclude GERD.
Lifestyle changes [15][20][32][33][34]
There is conflicting evidence as to which lifestyle modifications confer a significant benefit. The following recommendations are commonly mentioned in the literature but should be approached on a case-by-case basis, as they may offer relief only for some patients.
-
Dietary recommendations
- Small portions
- Avoid eating at least 2–3 hours before bedtime.
- Avoid foods and beverages that appear to trigger symptoms. [35]
-
Physical recommendations
- Weight loss in patients with obesity
- Elevate the head of the bed (10–20 cm) for patients with nighttime symptoms.
-
Reduce or avoid triggering substances
- Tobacco, alcohol, and/or caffeine if the patient experiences correlation with symptoms
- Medications that may worsen symptoms (e.g., CCBs, diazepam) [7]
Surgical therapy [9][15][20][36]
Antireflux surgery may be considered for select patients after careful evaluation. Predictors of successful outcomes include: [37][38]
- Symptoms that correlate objectively with reflux episodes using ambulatory esophageal pH monitoring
- Prior good response to PPIs
Indications
- Discontinuation of medical therapy (e.g., due to nonadherence or side effects)
- Symptoms refractory to medical therapy
- Complications despite optimal medical therapy, e.g., severe esophagitis, strictures, recurrent aspiration
- Large hiatal hernia
Fundoplication
- Definition: an antireflux procedure in which the gastric fundus is wrapped around the lower esophagus and secured with stitches to form a cuff; results in a narrowing of the distal esophagus and the gastroesophageal junction (GEJ), preventing reflux
- Approach: Laparoscopic and open fundoplication are possible.
-
Techniques [37]
- Partial fundoplication (fewer complications)
- 180° (Dor fundoplication)
- 270° (Toupet fundoplication)
- Complete fundoplication (Nissen fundoplication): 360°
- Partial fundoplication (fewer complications)
-
Complications [37]
- Gas bloat syndrome: inability to belch, leading to bloating and an increase in flatulence
- Dysphagia
- Recurrence of reflux esophagitis
-
Considerations for patients with comorbidities
- Patients with obesity and reflux undergoing bariatric surgery: Consider Roux-en-Y.
- Hiatal hernias: Combine fundoplication with hiatoplasty and, in some cases, gastropexy.

© AMBOSS
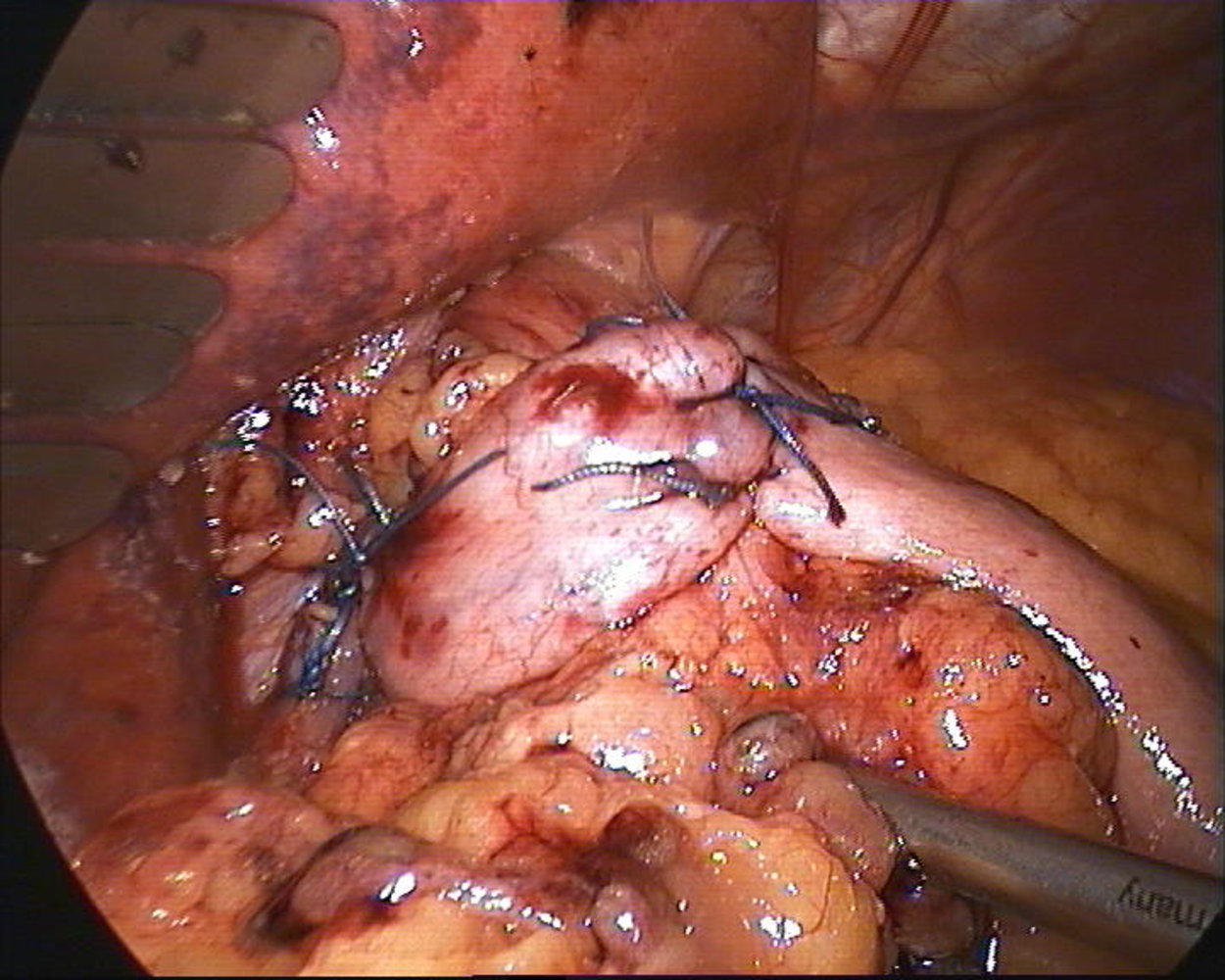
Photograph of the surgical site following laparoscopic 360° Nissen fundoplication, showing the stitches used to form the fundus cuff ventrally (center right of image) and to secure the fundus to the right crus of the diaphragm (left side of image).
Created by: Andreas Plamper, St. Franziskus-Hospital, Köln.
Complications
Barrett esophagus [20][39][40][41]
-
Definition: intestinal metaplasia of the esophageal mucosa due to chronic reflux esophagitis
- Columnar epithelium and goblet cells rather than esophageal squamous epithelium on histopathological examination
- A precancerous condition that requires close surveillance
- Incidence: up to 12% of patients with GERD [41]
-
Risk factors for Barrett esophagus [41]
- Chronic GERD symptoms (weekly symptoms for ≥ 5 years)
- Male sex
- Age > 50 years
- White race
- Smoking
- Obesity
- Family history of Barrett esophagus or esophageal adenocarcinoma in a first-degree relative
-
Pathophysiology
- Reflux esophagitis → stomach acid damages mucosa of distal esophagus → stratified squamous epithelium is replaced by nonciliated columnar epithelium and goblet cells (intestinal metaplasia, Barrett metaplasia) [12]
- The physiological transformation zone (Z line) between squamous and columnar epithelium is shifted upwards.
-
Diagnosis [41]
- Endoscopy
- Z line displacement < 1 cm and no visible lesions: no diagnosis of Barrett esophagus, biopsy not recommended
- Z line displacement ≥ 1 cm and/or visible lesions: diagnosis of Barrett esophagus, obtain ≥ 8 endoscopic biopsies
- Endoscopy
-
Management and surveillance [41]
- PPI therapy
- Endoscopic surveillance
-
If no dysplasia
- Barrett esophagus segment < 3 cm: Repeat endoscopy in 5 years.
- Barrett esophagus segment ≥ 3 cm: Repeat endoscopy in 3 years.
- If indefinite for dysplasia: Repeat endoscopy with biopsies after 3–6 months of optimized PPI therapy.
-
If low-grade dysplasia
- Endoscopic therapy of mucosal irregularities (usually including endoscopic mucosal resection and radiofrequency ablation) and follow-up endoscopy with biopsies after 1 year and every 2 years thereafter
- Alternatively: surveillance at 6 months and 1 year and annually thereafter with four-quadrant biopsies every 1 cm
- If high-grade dysplasia: endoscopic resection of all visible lesions and ablation of all remaining areas of Barrett epithelium (e.g., with radiofrequency ablation), and follow-up endoscopy with biopsies after 3, 6, and 12 months and annually thereafter
-
If no dysplasia
- Antireflux surgery to prevent progression to neoplasia is not routinely recommended.
- Complications: esophageal adenocarcinoma (see “Esophageal cancer”) [42]
Endoscopic examination of the esophagus is indicated to screen for Barrett esophagus in patients with chronic GERD symptoms (weekly for ≥ 5 years) and ≥ 3 additional risk factors: male sex, age > 50 years, White race, obesity, smoking, family history of Barrett esophagus or esophageal adenocarcinoma in a first-degree relative. [41]




Additional complications
- Reflux esophagitis: most common complication of GERD [43]
- Erosive esophagitis
- Iron deficiency anemia: mucosal erosions and ulcerations → chronic bleeding → anemia
-
Esophageal stricture
- Etiology
- Most common sequela of reflux esophagitis; or ingestion of caustic substances [43]
- Radiation
- Systemic sclerosis
- Clinical features: solid food dysphagia
- Diagnostics
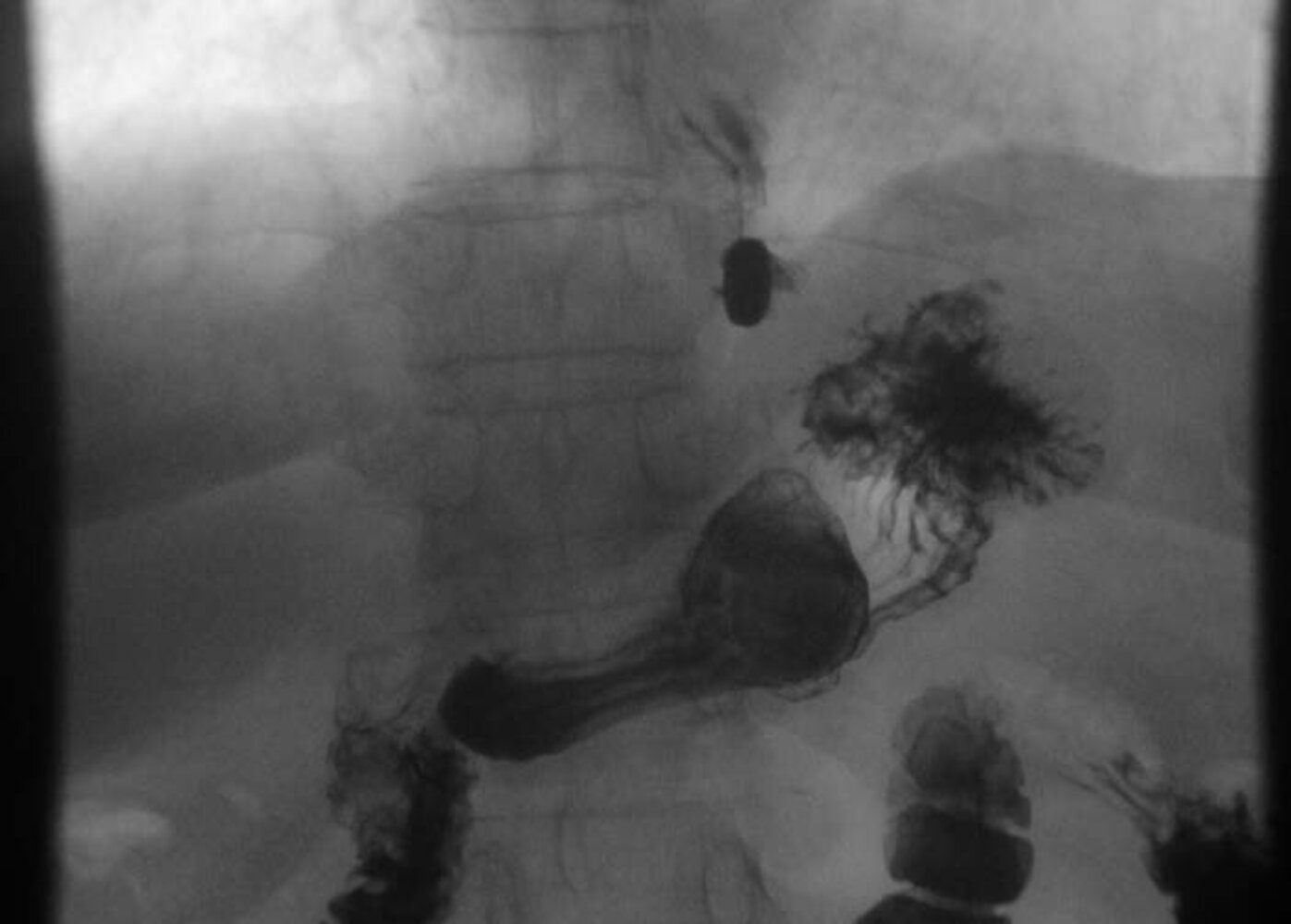
- Barium esophagram (best initial test): narrowing of the esophagus at the gastroesophageal junction
- Endoscopy with biopsies: to rule out malignancy and eosinophilic esophagitis
- Treatment
- First-line treatment: dilation with bougie dilator/balloon dilator and PPIs in patients with reflux
- In refractory cases (multiple recurrences): steroid injection prior to dilation; endoscopic electrosurgical incision
- Recurrence occurs in the majority of patients; multiple treatment attempts are often necessary.
- Etiology
- Esophageal rings: e.g., Schatzki rings
-
Complications due to aspiration of gastric contents
- Aspiration pneumonia and/or aspiration pneumonitis
- Chronic bronchitis
- Asthma (exacerbation)
- Reflux laryngitis: hoarseness (due to laryngopharyngeal reflux)
")



We list the most important complications. The selection is not exhaustive.
© AMBOSS
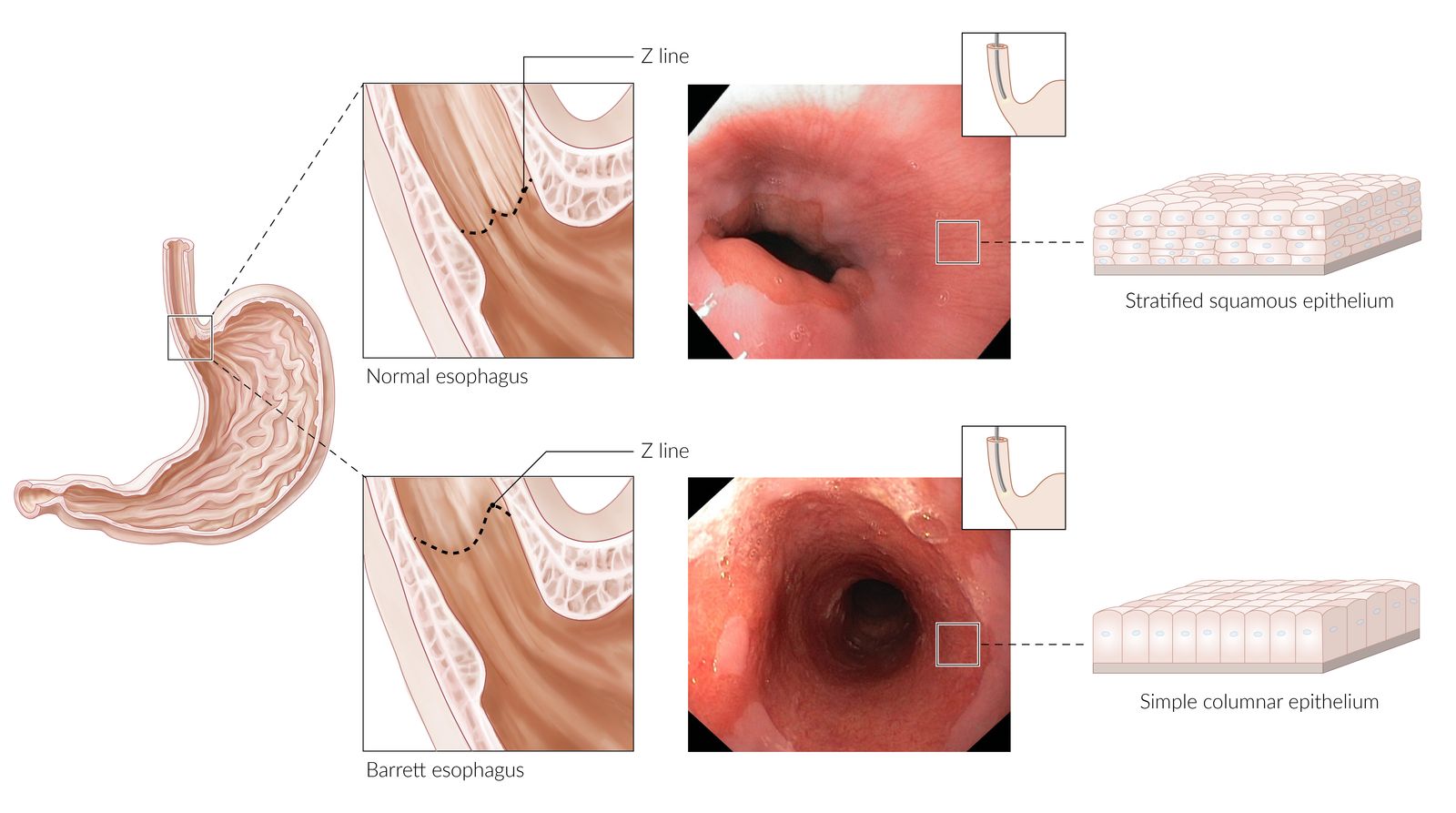
Visible in both photographs is the transformation zone (Z-line), where the stratified squamous epithelium of the esophagus (paler pink color) meets the columnar epithelium of the stomach (darker red color).
Normal esophagus: the Z-line is located at or just proximal to the gastroesophageal junction, which typically corresponds to the level of the diaphragmatic hiatus and the lower esophageal sphincter.
Barrett esophagus: chronic reflux esophagitis damages the stratified squamous mucosa of the distal esophagus (which is not adapted to tolerate gastric acid) → metaplastic replacement of stratified squamous epithelium by columnar epithelium → proximal displacement of the Z line
© AMBOSS. "Normal esophagus" endoscopy image kindly provided by Dr. J. Guntau - Albertinen Krankenhaus, Hamburg, Germany (endoskopiebilder.de). "Barrett esophagus" endoscopy image kindly provided by Dr. med. Merkel, Dr. med. Wiens, Dr. med. Kämmer - St. Hedwig Krankenhaus, Berlin, Germany.
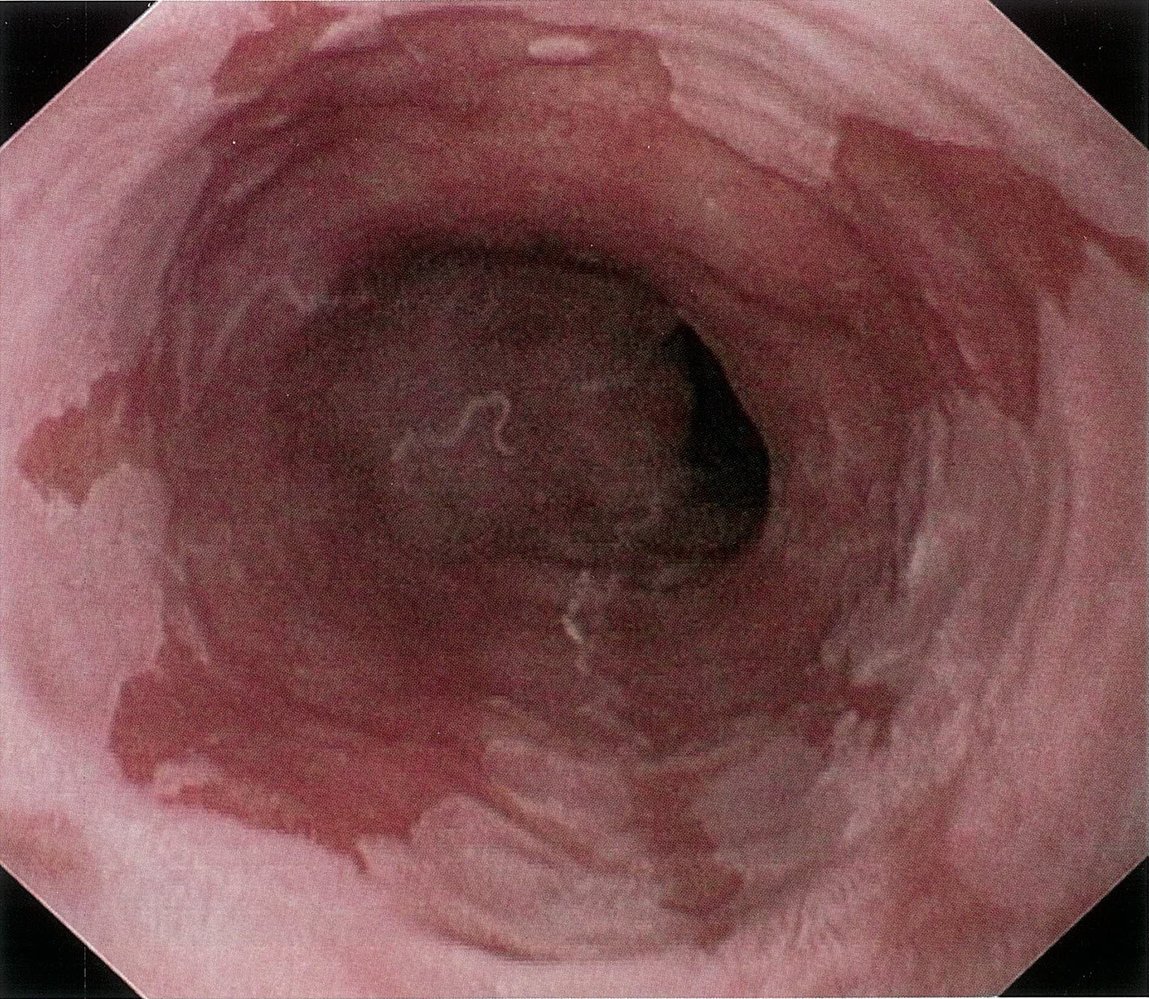
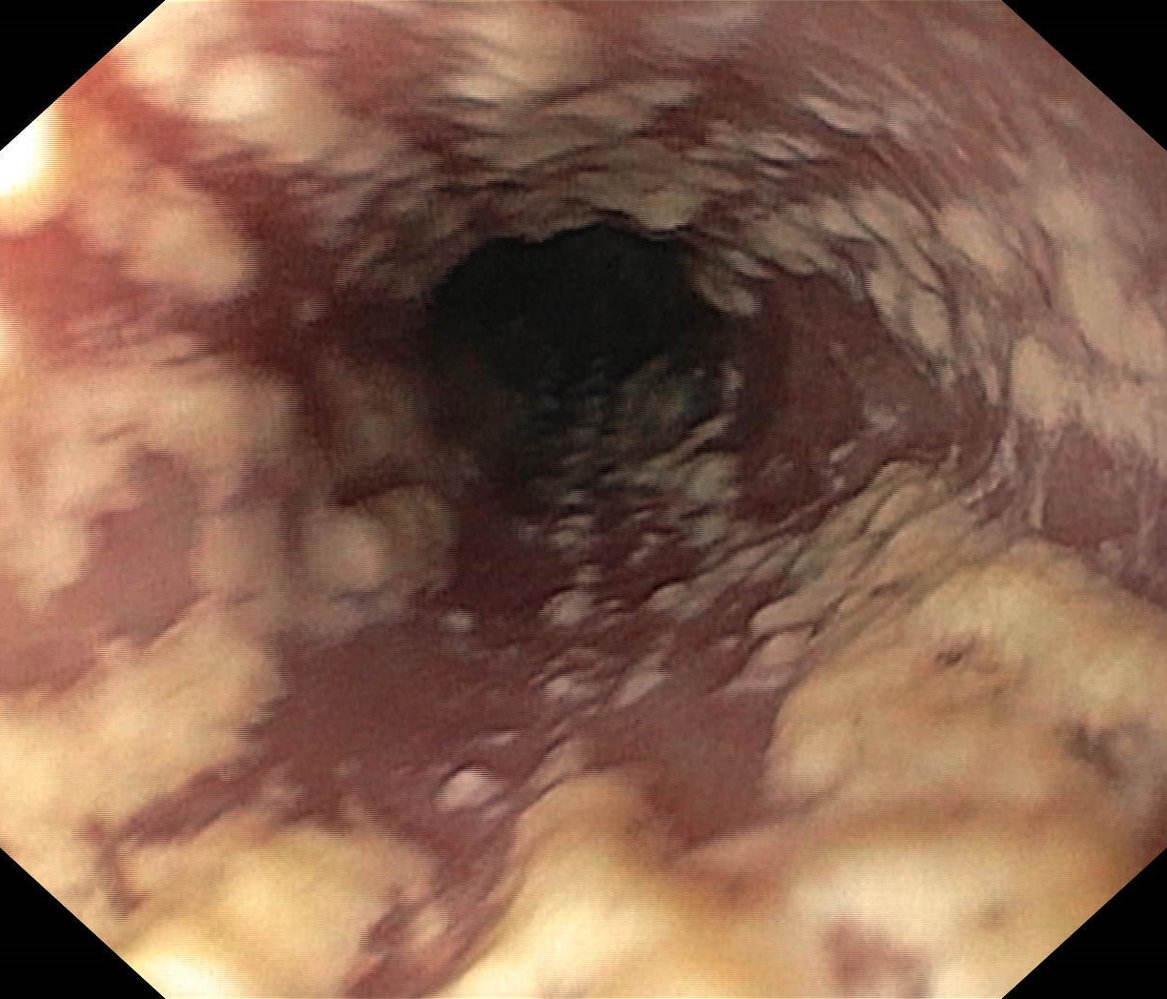
Endoscopic view of the esophagus
The distal esophagus is lined with salmon-pink metaplastic columnar epithelium. The distal parts involve the whole circumference (blue overlay). At the proximal end, tongue-shaped extensions of metaplastic columnar epithelium (yellow dotted line) are surrounded by normal (light) esophageal mucosa.
These findings are consistent with Barrett esophagus.
Source: © IMPP
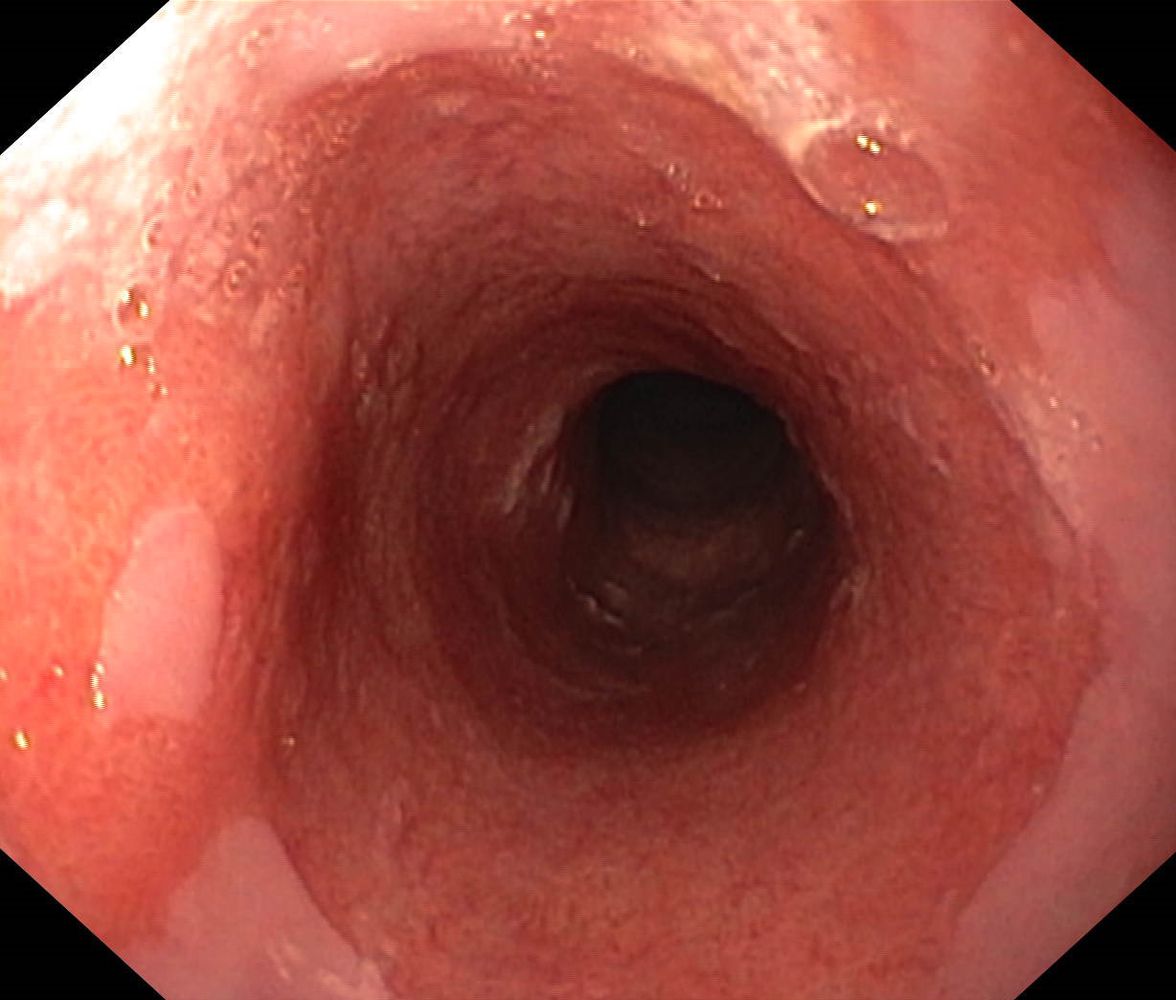
Endoscopic view of the esophagus
The distal esophagus is extensively lined with salmon-pink metaplastic columnar epithelium involving the entire circumference. At the proximal end, tongue-shaped extensions of metaplastic columnar epithelium are surrounded by normal squamous mucosa of the esophagus (green overlay). In one extension, a small squamous island (hatched overlay) is visible.
These findings are consistent with long-segment Barrett esophagus.
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.
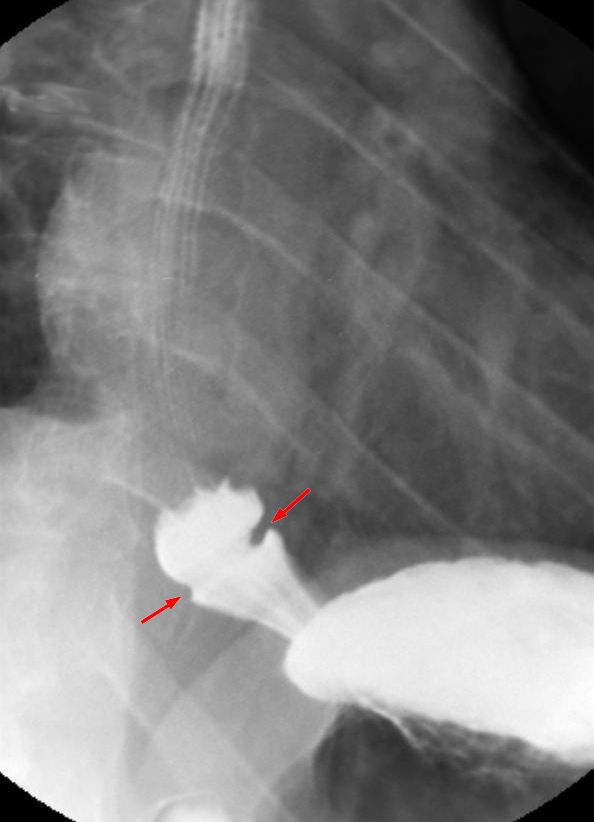
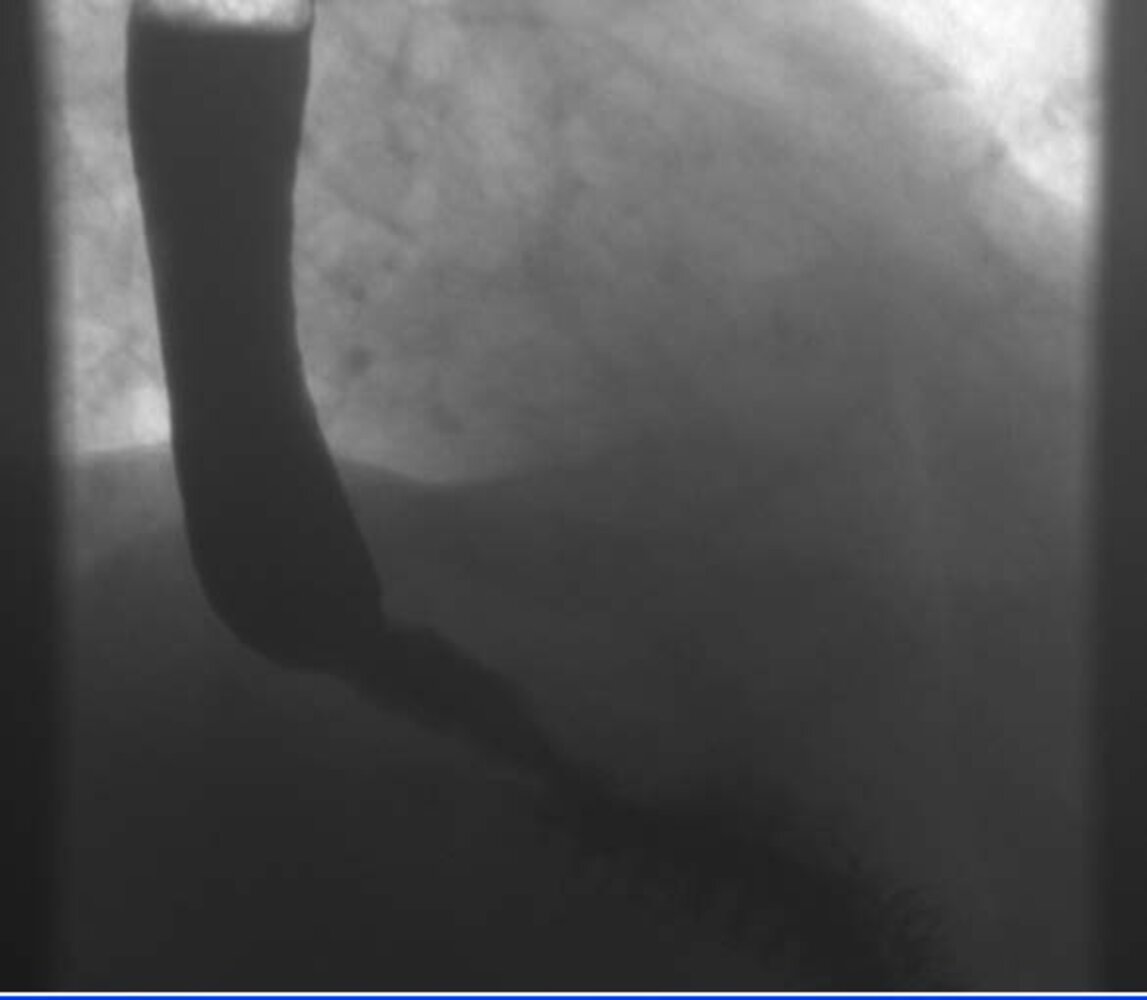
Barium swallow (lateral view): circular narrowing of the esophagus directly at the esophagogastric junction (Schatzki ring or B-ring). As opposed to A-rings (which are located just proximal to the EG junction), B-rings often can only be seen if there is a concomitant hiatal hernia, with which they are frequently associated (as is the case here).
Source: “Schatzkiring” by Hellerhoff, Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}

© Massachusetts Medical Society. All rights reserved. AMBOSS SE, exclusive licensee.
Related One-Minute Telegram
- One-Minute Telegram 46-2022-2/3: 2022 updated American College of Gastroenterology (ACG) guidelines for GERD
Interested in the newest medical research, distilled to just one minute? Sign up for the One-Minute Telegram in the “Tips and links” below.
External Resources
- 2013 ACG Guidelines for the Diagnosis and Management of GERD
- 2021 ACG Guidelines for the Diagnosis and Management of GERD
- 2017 AGA Best Practice Advice on Long-term Use of PPI
- 2010 SAGES Guidelines for the Surgical Treatment of GERD
- 2022 SAGES Guidelines for the Surgical Treatment of GERD
- 2022 ACG Guideline Update on the Diagnosis and Management of Barrett's Esophagus
- 2014 EAES Recommendations for the Management of GERD
- 2014 NICE Clinical Guideline on GERD and Dyspepsia in Adults
- 2017 WGO Global Perspective on GERD
- One-Minute Telegram
References
- Vakil N, Van Zanten SV, Kahrilas PJ et al. "The Montreal definition and classification of Gastro-esophageal Reflux Disease (GERD) – a global evidence-based consensus". Zeitschrift für Gastroenterologie. 45(11). :1125-1140. (2007)
- Hershcovici T, Fass R. "Nonerosive Reflux Disease (NERD) - An Update". J Neurogastroenterol Motil. 16(1). :8-21. (2010)
- Yamasaki T, Hemond C, Eisa M, Ganocy S, Fass R. "The Changing Epidemiology of Gastroesophageal Reflux Disease: Are Patients Getting Younger?". Journal of neurogastroenterology and motility. 24(4). :559-569. (2018)
- Schneider JH, Küper MA, Königsrainer A, Brücher BLDM. "Transient Lower Esophageal Sphincter Relaxation and Esophageal Motor Response". J Surg Res. 159(2). :714-719. (2010)
- Diamant N.. "Pathophysiology of gastroesophageal reflux disease". GI Motility online. (2006)
- De giorgi F, Palmiero M, Esposito I et al. " Pathophysiology of gastro-oesophageal reflux disease". Acta Otorhinolaryngol Ital. 26(5). :241-246. (2006)
- Börger HW, Schafmayer A, Arnold R et al. " [The influence of coffee and caffeine on gastrin and acid secretion in man (author's transl)]". Dtsch Med Wochenschr. 101(12). :455-457. (1976)
- Chen S, Wang J, Li Y. "Is alcohol consumption associated with gastroesophageal reflux disease?". Journal of Zhejiang University SCIENCE B. 11(6). :423-428. (2010)
- Katz PO, Gerson LB, Vela MF. "Guidelines for the diagnosis and management of gastroesophageal reflux disease". Am J Gastroenterol. 108(3). :308-328. (2013)
- Puri P. "Newborn Surgery". Hodder & Stoughton Ltd. (2011). ISBN: 9781444102833
- Walls R, Hockberger R, Gausche-Hill M. "Rosen's Emergency Medicine". Elsevier Health Sciences. (2018). ISBN: 9780323354790
- Altman KW, Prufer N, Vaezi MF. "A review of clinical practice guidelines for reflux disease: Toward creating a clinical protocol for the otolaryngologist". Laryngoscope. 121(4). :717-723. (2011)
- Katz PO, Dunbar KB, Schnoll-Sussman FH, et al. "ACG Clinical Guideline for the Diagnosis and Management of Gastroesophageal Reflux Disease". Am J Gastroenterol. 117(1). :27-56. (2021)
- Moayyedi PM, Lacy BE, Andrews CN, et al. "ACG and CAG Clinical Guideline: Management of Dyspepsia". Am J Gastroenterol. 112(7). :988-1013. (2017)
- Tintinalli JE, Stapczynski JS, Ma OJ, et al. "Tintinalli's Emergency Medicine: A Comprehensive Study Guide, 9th edition". McGraw Hill Professional. (2019). ISBN: 9781260019940
- DeVault KR, Castell DO. "Updated Guidelines for the Diagnosis and Treatment of Gastroesophageal Reflux Disease". Am J Gastroenterol. 100. :190-200. (2005)
- "Management of Gastroesophageal Reflux Disease". https://www.aafp.org/afp/2003/1001/p1311.pdf. [2003-01-01]
- Muthusamy VR, Lightdale JR, Acosta RD, et al. "The role of endoscopy in the management of GERD". Gastrointest Endosc. 81(6). :1305-1310. (2015)
- Fisichella PM, Schlottmann F, Patti MG. "Evaluation of gastroesophageal reflux disease". Updates in Surgery. 70(3). :309-313. (2018)
- Kahrilas PJ, Kim HC, Pandolfino JE. "Approaches to the diagnosis and grading of hiatal hernia". Best Practice & Research Clinical Gastroenterology. 22(4). :601-616. (2008)
- Vakil N, van Zanten SV, Kahrilas P, Dent J, Jones R. "The Montreal Definition and Classification of Gastroesophageal Reflux Disease: A Global Evidence-Based Consensus". Am J Gastroenterol. 101(8). :1900-1920. (2006)
- Tutuian, Castell. "Gastroesophageal reflux monitoring: pH and impedance". GI motility online. (2006)
- Klingler PJ, Hinder RA, Wetscher GJ, et al. "Accurate placement of the esophageal pH electrode for 24-hour pH monitoring using a combined pH/manometry probe". Am J Gastroenterol. 95(4). :906-909. (2000)
- Tripathi M, Streutker CJ, Marginean EC. "Relevance of histology in the diagnosis of reflux esophagitis". Ann N Y Acad Sci. 1434(1). :94-101. (2018)
- Peters Y, Al-Kaabi A, Shaheen NJ, et al. "Barrett oesophagus.". Nature reviews. Disease primers. 5(1). :35. (2019)
- Castell DO. "Medication-induced esophagitis". UpToDate. UpToDate. http://www.uptodate.com/contents/medication-induced-esophagitis. [2016-11-08]
- Freedberg DE, Kim LS, Yang Y-X. "The Risks and Benefits of Long-term Use of Proton Pump Inhibitors: Expert Review and Best Practice Advice From the American Gastroenterological Association". Gastroenterology. 152(4). :706-715. (2017)
- Moayyedi P, Eikelboom JW, Bosch J, et al. "Safety of Proton Pump Inhibitors Based on a Large, Multi-Year, Randomized Trial of Patients Receiving Rivaroxaban or Aspirin". Gastroenterology. 157(3). :682-691.e2. (2019)
- Ma C, Shaheen AA, Congly SE, et al. "Interpreting Reported Risks Associated With Use of Proton Pump Inhibitors: Residual Confounding in a 10-Year Analysis of National Ambulatory Data". Gastroenterology. 158(3). :780-782.e3. (2020)
- Corley DA. "Safety and Complications of Long-Term Proton Pump Inhibitor Therapy: Getting Closer to the Truth". Gastroenterology. 157(3). :604-607. (2019)
- Savarino V, Marabotto E, Furnari M, et al. "Latest insights into the hot question of proton pump inhibitor safety – a narrative review". Digestive and Liver Disease. 52(8). :842-852. (2020)
- Joelle Ayoub, Nicole D. White. "GERD Management". American Journal of Lifestyle Medicine. 11(1). :24-28. (2017)
- Kaltenbach T, Crockett S, Gerson LB. "Are Lifestyle Measures Effective in Patients With Gastroesophageal Reflux Disease?". Arch Intern Med. 166(9). :965. (2006)
- Commisso A, Lim F. "Lifestyle Modifications in Adults and Older Adults With Chronic Gastroesophageal Reflux Disease (GERD)". Crit Care Nurs Q. 42(1). :64-74. (2019)
- Becker DJ, Sinclair J, Castell DO, Wu WC. "A comparison of high and low fat meals on postprandial esophageal acid exposure". Am J Gastroenterol. 84(7). :782-786. (1989)
- Richter JE. "Gastroesophageal Reflux Disease Treatment: Side Effects and Complications of Fundoplication". Clin Gastroenterol Hepatol. 11(5). :465-471. (2013)
- John Cameron, Andrew Cameron. "Current Surgical Therapy 13th Edition". Elsevier. (2019). ISBN: 9780323640619
- "Guidelines for Surgical Treatment of Gastroesophageal Reflux Disease (GERD)". https://www.sages.org/publications/guidelines/guidelines-for-surgical-treatment-of-gastroesophageal-reflux-disease-gerd/. [2010-02-01]
- Shaheen NJ, Falk GW, Iyer PG, Gerson LB. "ACG Clinical Guideline: Diagnosis and Management of Barrett’s Esophagus". Am J Gastroenterol. 111(1). :30-50. (2015)
- Runge TM, Abrams JA, Shaheen NJ. "Epidemiology of Barrett’s Esophagus and Esophageal Adenocarcinoma". Gastroenterol Clin North Am. 44(2). :203-231. (2015)
- Shaheen NJ, Falk GW, Iyer PG, et al. "Diagnosis and Management of Barrett's Esophagus: An Updated ACG Guideline". Am J Gastroenterol. 117(4). :559-587. (2022)
- Sonja Kroep, Iris Lansdorp-Vogelaar, Joel H. Rubenstein, et al. "An Accurate Cancer Incidence in Barrett's Esophagus: A Best Estimate Using Published Data and Modeling". Gastroenterology. 149(3). :577-585.e4. (2015)
- Richter JE. "Peptic strictures of the esophagus". Gastroenterol Clin North Am. 28(4). :875-891. (1999)
- Clerico A, Giannoni A, Vittorini S, Emdin M. "The paradox of low BNP levels in obesity". Heart Fail Rev. 17(1). :81-96. (2011)
- "Gastroesophageal Reflux Disease". https://www.ncbi.nlm.nih.gov/books/NBK441938/. [2019-05-05]
- Genta RM, Spechler SJ, Kielhorn AF. "The Los Angeles and Savary-Miller systems for grading esophagitis: utilization and correlation with histology". Diseases of the Esophagus. 24(1). :10-17. (2011)
- Naini BV, Souza RF, Odze RD. "Barrett’s Esophagus". Am J Surg Pathol. 40(5). :e45-e66. (2016)
- Odze RD, Goldblum JR. "Surgical Pathology of the GI Tract, Liver, Biliary Tract, and Pancreas". Elsevier Health Sciences. (2009). ISBN: 9781416040590
- Roark R, Sydor M, Chatila AT, et al. "Management of gastroesophageal reflux disease". Disease-a-Month. 66(1). :100849. (2020)
- Siewert R, Lepsien G, Weiser HF, Schattenmann G, Peiper HJ. "[The telescope phenomenon. A complication possibility following fundoplication].". Chirurg. 48(10). :640-5. (1977)