CME information and disclosures
To see contributor disclosures related to this article, hover over this reference: [1]
Physicians may earn CME/MOC credit by searching for an answer to a clinical question on our platform, reading content in this article that addresses that question, and completing an evaluation in which they report the question and the impact of what has been learned on clinical practice.
AMBOSS designates this Internet point-of-care activity for a maximum of 0.5 AMA PRA Category 1 Credit(s)™. Physicians should claim only credit commensurate with the extent of their participation in the activity.
For answers to questions about AMBOSS CME, including how to redeem CME/MOC credit, see "Tips and Links" at the bottom of this article.
Quick guide
Diagnostic approach
- ABCDE survey
- Targeted clinical evaluation
- CBC
- BMP
- Blood gas analysis
- Lactate
- Abdominal x-ray (upright or lateral decubitus)
- CT abdomen and pelvis with IV contrast
GI tract perforation is a surgical emergency. In some cases, clinical features alone are sufficient to warrant emergency explorative laparotomy.
Management checklist
- Consult general surgery
- NPO
- Two large-bore peripheral IVs
- IV fluid resuscitation
- Nasogastric tube with suction
- Start empiric antibiotic therapy for intra-abdominal infection.
- Electrolyte repletion
- Parenteral analgesics (e.g., morphine )
- Parenteral antiemetics (e.g., ondansetron )
- Manage complications (e.g., peritonitis, sepsis, multiorgan dysfunction, shock).
Most patients with GI tract perforation should be managed with urgent explorative laparotomy.
Summary
Gastrointestinal perforation is a full-thickness loss of bowel wall integrity that results in perforation peritonitis. Perforation of a duodenal ulcer is the most common cause of perforation peritonitis. Patients typically present with an acute onset of severe abdominal pain associated with nausea, vomiting, and fever. Signs of peritoneal irritation are evident on examination and include decreased bowel sounds and diffuse or localized abdominal guarding and rebound tenderness. CT abdomen with IV contrast is the preferred imaging modality to confirm the presence of free air within the peritoneal cavity (pneumoperitoneum) and localize the site of the perforated viscus. Most patients will require an emergency exploratory laparotomy. Patients with evidence of a well-contained perforation (e.g., a small localized appendicular or diverticular perforation) and no signs of sepsis may be given a trial of conservative management with antibiotics, bowel rest, close monitoring of vital signs, and serial abdominal examination. The prognosis depends on the etiology, degree of intraabdominal contamination, and other comorbidities.
See also esophageal perforation.
Etiology
-
Ulcerative/erosive disease [2]
-
Peptic ulcer disease:
- Most common cause of stomach and duodenal perforation [3]
- Duodenal ulcers of the anterior wall are more likely to perforate.
- Malignancy
- Inflammatory bowel disease: ulcerative colitis, Crohn disease
-
Peptic ulcer disease:
-
Infections
- Diverticulitis (colonic diverticula, Meckel diverticulum)
- Acute appendicitis
- Typhoid
- Gastrointestinal tuberculosis
- Toxic megacolon
-
Bowel ischemia
- Bowel obstruction (i.e., adhesions, volvulus, malignancy)
- Acute mesenteric ischemia
-
Trauma
- Penetrating trauma (e.g., stab injury, iatrogenic perforations): e.g., post-ERCP duodenal perforation
- Blunt abdominal trauma
-
Miscellaneous
- Foreign body ingestion
- Drug-induced (e.g., NSAIDs, glucocorticoids, cocaine)
- Radiation therapy to the abdominopelvic or lower thoracic region
- Post renal transplant [4]
Clinical features
-
General signs and symptoms
- Sudden onset of abdominal pain and abdominal distention
- Nausea, vomiting, obstipation
- Fever, tachycardia, tachypnea, hypotension
- Signs of peritonitis or shock
- Decreased or absent bowel sounds
- Loss of liver dullness on RUQ percussion
-
History suggestive of specific locations
-
Perforated PUD:
- Sudden onset of intense, stabbing pain, followed by diffuse abdominal pain and distention (beginning peritonitis)
- Referred pain to the shoulder due to irritation of the diaphragm, which is innervated by the phrenic nerve (C3-C5); the shoulder skin is innervated by supraclavicular nerves (C3-C4) (see referred pain)
- History of recurrent epigastric pain, chronic use of NSAIDs
- Perforation of chronic ulcers may only cause mild symptoms.
- Perforated diverticulitis: constipation, previous LLQ pain
- Perforated appendicitis: progressively worsening RLQ pain, migratory pain
- Perforated malignancy or IBD: anorexia, weight loss, melena, change in bowel habits
-
Perforated PUD:
-
Localization of pain
- Diffuse: in patients with free intraperitoneal perforation
- Localized RLQ pain: contained perforated appendicitis
- Localized LLQ pain: contained perforated diverticulitis
Bowel perforation is a surgical emergency. In some cases, clinical features alone are sufficient to warrant emergency explorative laparotomy.

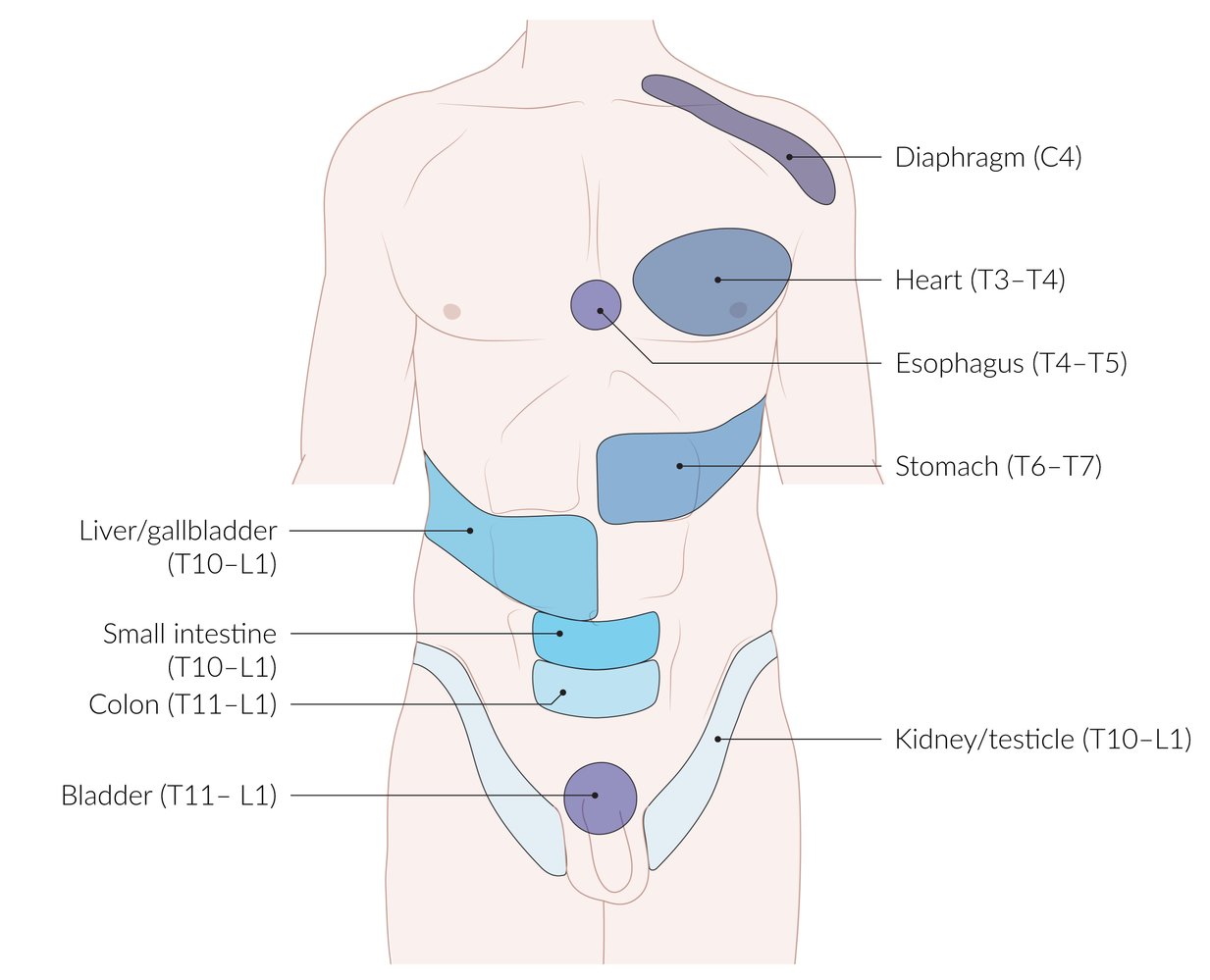
Visceral fibers from internal organs may project pain onto a specific dermatome or myotome, which can be misinterpreted as somatic pain. Commonly, the pain is not projected onto the whole dermatome, but is more intense at specific points in the corresponding dermatome (blue areas).
© AMBOSS
Diagnosis
Laboratory analysis
- CBC: neutrophilic leukocytosis
- BMP: ↑ BUN, ↑ creatinine
- Blood gas analysis: lactic acidosis (in ischemic perforation) [5]
Imaging [6][7]
Immediate studies
- Indications: Consider only for patients too unstable to safely undergo CT scanning.
-
X-ray abdomen (upright or lateral decubitus) ; [8]
- Combine lateral decubitus with upright CXR to increase sensitivity.
- Findings: free intraperitoneal air (pneumoperitoneum) under the diaphragm and/or between liver and lateral abdominal wall
-
Point of care ultrasound (POCUS) for which characteristic findings include: [9][10]
- Enhanced peritoneal stripe sign: a hyperechogenic focal thickening of the peritoneum
- Horizontal reverberation artifacts: horizontal stripes resulting from the interface of free air and fascia
Before an upright x-ray, patients must be sitting up for at least 10 minutes in order to allow free air to move upward and collect under the diaphragm. [8]
Confirmatory studies
-
First line: CT abdomen and pelvis with IV contrast (most sensitive)
- Indications: acute nonlocalized abdominal pain
- Findings
-
Pneumoperitoneum: the presence of air in the peritoneal cavity
- An abdominal x-ray showing radiolucent air under the diaphragm and/or the delineation of the bowel wall by radiolucent air is diagnostic.
- Can occur after perforation of a hollow abdominal viscus (e.g., perforated peptic ulcer) or after surgery in which air is introduced into the abdominal cavity.
- Signs of perforated bowel: loss of bowel wall continuity, localized mesenteric fat stranding
-
Pneumoperitoneum: the presence of air in the peritoneal cavity
-
Alternative: formal ultrasound abdomen
- Indication: preferred in patients with contraindications to radiation exposure (e.g., pregnancy)
- Findings: pneumoperitoneum, localized fluid collection, localized thickening of a bowel segment.









IV contrast is preferred if bowel perforation is suspected. If oral contrast must be used, a water-soluble contrast agent is preferred.
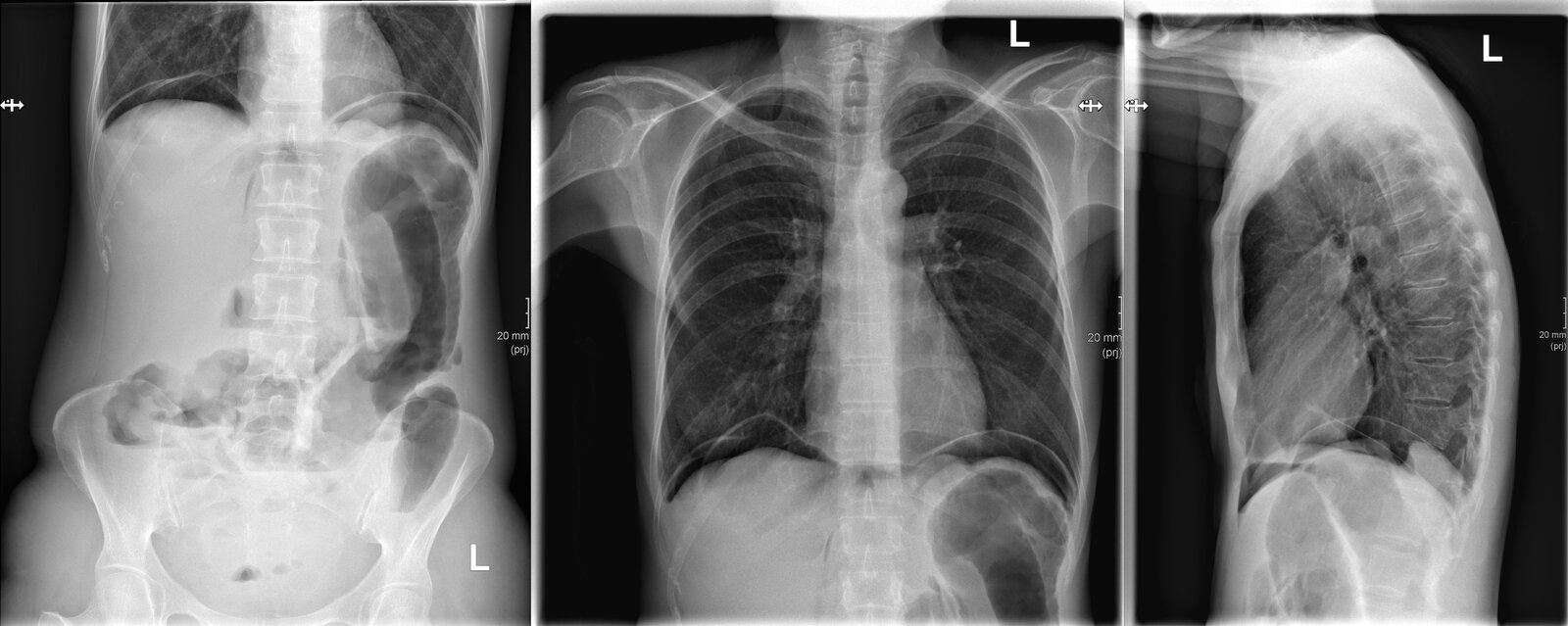
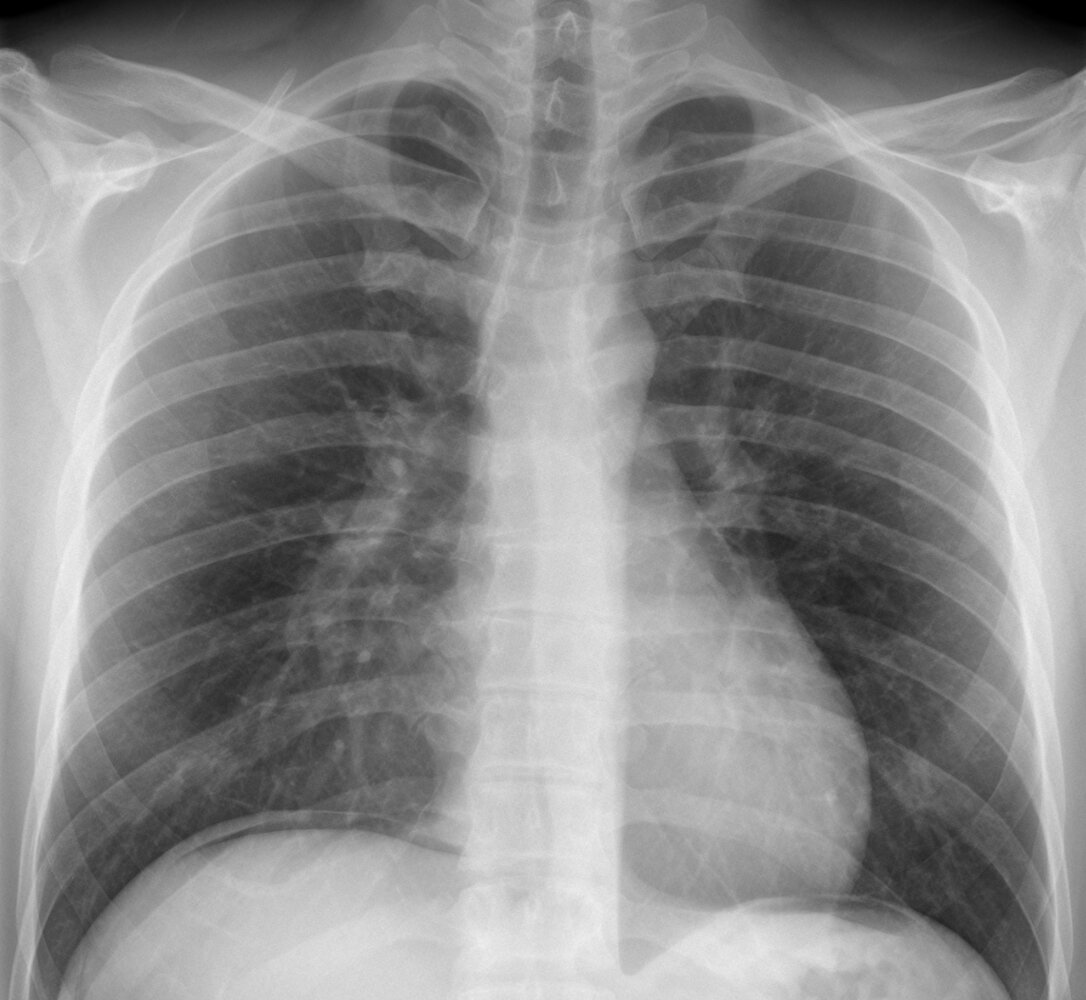
X-ray abdomen (AP erect view) and chest (PA and lateral views)
Multiple air-fluid levels are seen in the colon and small bowel (examples indicated by black lines). Some dilated segments of left colon are seen and gas is present in the peritoneal space as a result of bowel perforation. Gas is primarily located beneath the diaphragms (green overlay) because of the erect positioning of the patient. Additional gas has dissected into the retroperitoneum (examples indicated by red overlay) and is visible as linear collections parallel to the spine.
Our great thanks to Kerstin Bohse, MD (Klinikum Pfeiffersche Stiftungen), for kindly providing this case.
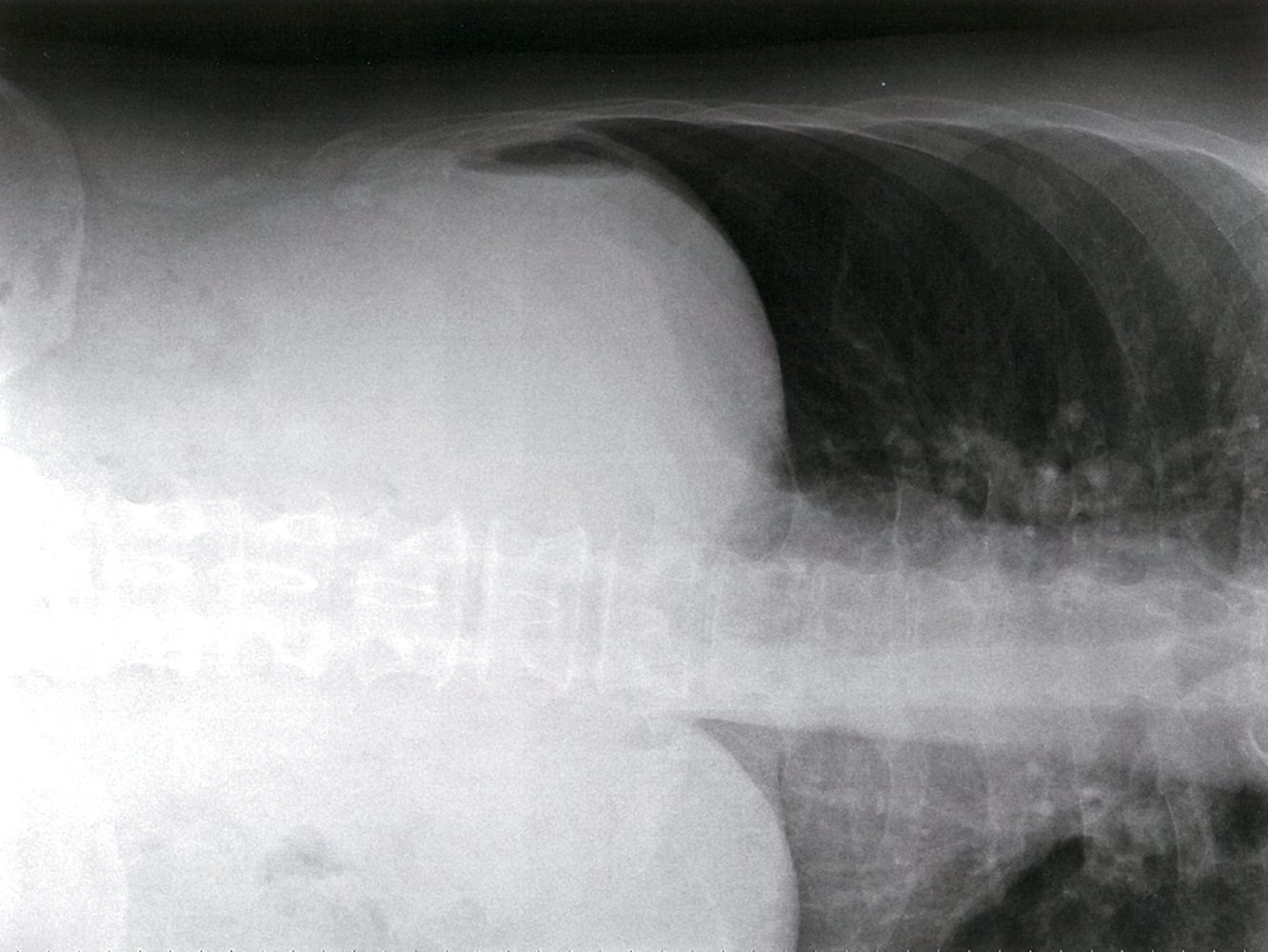
X-ray abdomen (AP view in left lateral decubitus position)
The left lateral decubitus, or left side down decubitus, radiograph was obtained with the patient's left (L) side dependent on the x-ray table. The image is centered on the nondependent right (R) hemidiaphragm. Free intraperitoneal air (pneumoperitoneum; green overlay) is interposed between the right hemidiaphragm and liver.
Source: © IMPP
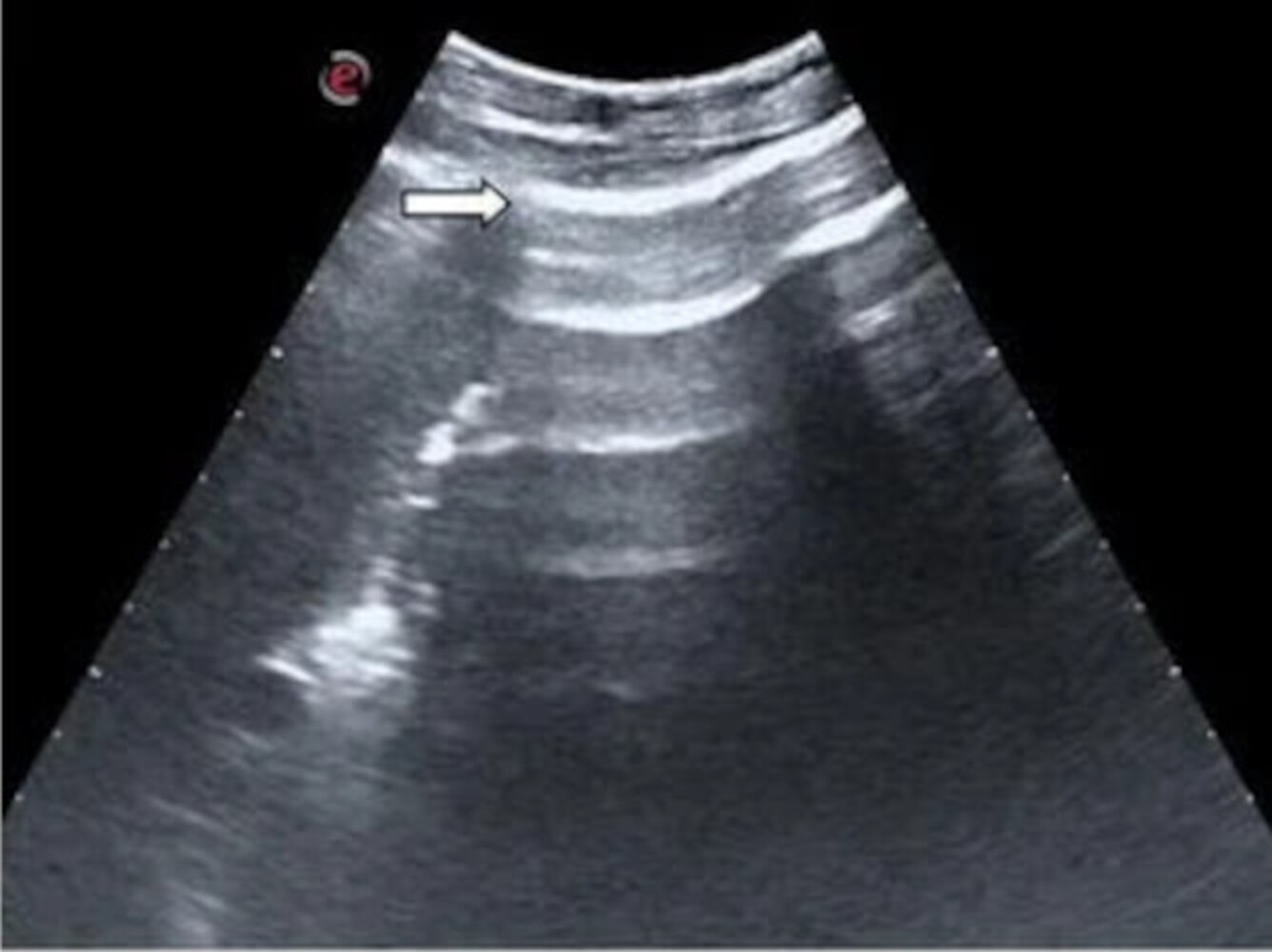
Ultrasound right upper quadrant
Increased echogenicity and thickening of the peritoneal stripe (white arrow) is accompanied by reverberation artifacts (green overlay).
Free air has collected anteriorly in the prehepatic space in this supine patient and abuts the parietal peritoneum creating a very reflective interface. The enhanced peritoneal stripe sign (EPSS) is helpful in the detection of pneumoperitoneum.
Source: “Figure 2, in: Accuracy of abdominal ultrasound for the diagnosis of pneumoperitoneum in patients with acute abdominal pain: a pilot study” by Peiman Nazerian, Camilla Tozzetti, Simone Vanni, Maurizio Bartolucci, Simona Gualtieri, Federica Trausi, Marco Vittorini, Elisabetta Catini, Gian Alfonso Cibinel, Stefano Grifoni, Springer Open, licensed under CC BY 4.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).

Click on the overlay icon below the taskbar on the left to toggle the overlay on and off.
CT abdomen (with IV and oral contrast; portal venous phase; axial plane) of a patient with abdominal pain after a colonoscopy
A large amount of free intraperitoneal gas (examples indicated by green dashed outlines) is present in the anterior abdomen. It is the result of perforation of the anterior wall of the colon (red overlay) in the region of the rectosigmoid transition. There are several small gas bubbles (examples indicated by green dashed outlines) within the mural defect and within nearby pelvic fatty tissue. A small amount of free fluid (blue overlay) is present in the right hemipelvis along with inflammatory fatty and fascial stranding.
Surgical clips (yellow arrowheads) in the gallbladder fossa are the result of a previous cholecystectomy. There is slight post-surgical pneumobilia (green arrowheads). A calcified uterine leiomyoma (green overlay) is seen in the pelvis.
Image source of original image: Clinic Pfeiffersche Stiftungen. Original title: “Hohlorganperforation”. Created by: Dr. med. Kerstin Bohse. Further notes: Our great thanks to Dr. med. Kerstin Bohse (Clinic Pfeiffersche Stiftungen) for kindly providing this case.
X-ray chest (PA view)
Free intraperitoneal gas (green overlay) is visible under both the right and left hemidiaphragms.
Source: “34-01-Freie Luft nach LH-OP” by Hellerhoff, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
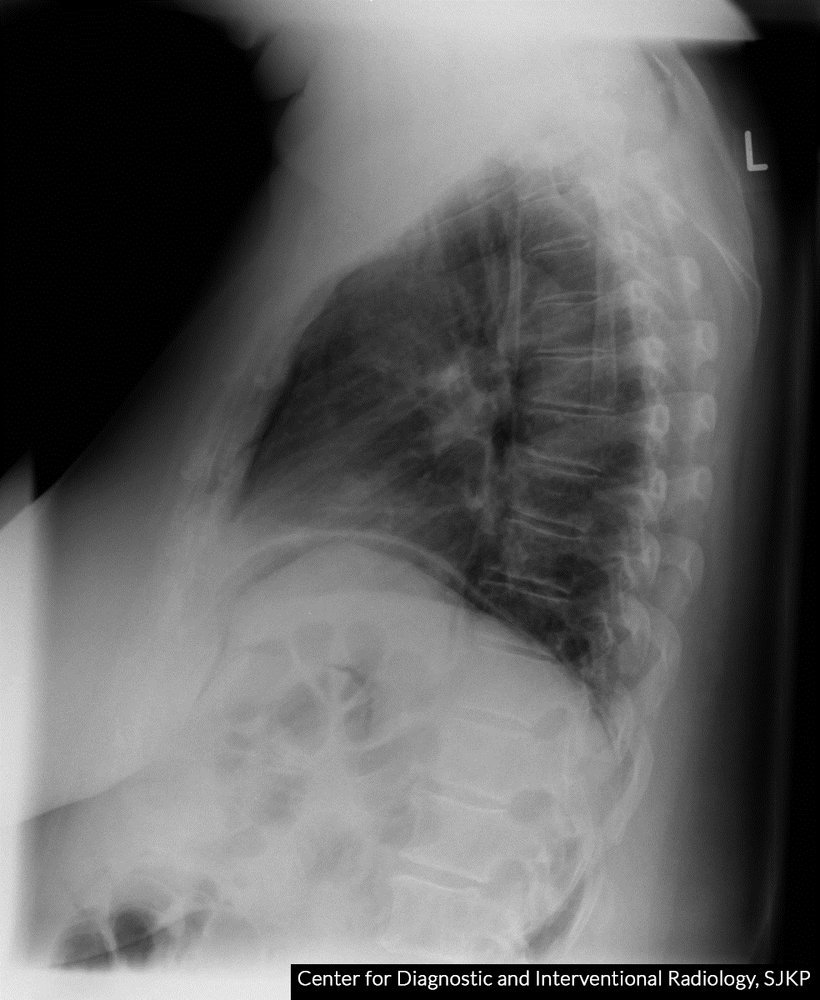
X-ray chest (upright position; left lateral view) of a female patient presenting with acute abdominal pain
Air is seen as a radiolucent column (green overlay) underneath the diaphragm (white dashed line), which appears as a thin semicircular radiopacity immediately inferior to the pulmonary shadow.
Air underneath the diaphragm is typically seen on x-rays of patients with pneumoperitoneum and indicates the perforation of a hollow viscus.
Our great thanks to Dr. Kissig (Center for Diagnostic and Interventional Radiology, Hedwigshöhe, St. Hedwig, Berlin, and St. Josefs Hospital, Potsdam) for kindly providing this image.

X-ray abdomen (supine; AP view)
Lucencies indicating free air in the retroperitoneal space dissect along numerous tissue planes (examples indicated by green overlay) and outline the right kidney (margin indicated by blue lines) and the psoas muscle (margin indicated by red line). In addition, the liver edge (yellow outline) is outlined by free air in the peritoneal space, which is also seen along several loops of bowel (examples indicated by arrows).
Our great thanks to Dr. Kissig (Center for Diagnostic and Interventional Radiology, Hedwigshöhe, St. Hedwig, Berlin, and St. Josefs Hospital, Potsdam) for kindly providing this image.

CT abdomen (with oral and IV contrast; axial plane) of a patient with abdominal distention
A large amount of free air is seen in the peritoneal cavity (indicated by arrows) anterior to the liver (L) and stomach (St). A perforation site was not identified by CT.
Pneumobilia (example indicated by green overlay) is due to a biliary stent (not shown). Cysts in the right kidney are partially visible on this image (red overlay).
Sp: spleen
Source: “Fig 1, In: Massive Pneumoperitoneum Presenting as an Incidental Finding” by Wang H, Batra V, Cureus, licensed under CC BY 3.0. Modifications: - arrow removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).

Abdomen CT (IV and oral contrast; coronal section)
The appendix (green overlay) is markedly distended, as evidenced by its distinctly visible hypodense lumen. A localized hypodense fluid collection (hatched area) with a well-defined hyperdense rim is visible at the cecal end of the appendix, indicating a periappendiceal abscess that is partially compressing the bladder.
This image was created by AMBOSS and is licensed under CC BY-SA 3.0. It is based on the image “Perityphlitischer Abszess in der CT - cor” by Hellerhoff, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
Differential diagnoses
See “Differential diagnoses” in “Acute abdomen”.
The differential diagnoses listed here are not exhaustive.
Treatment
Initial management
- Bowel rest (NPO)
- IV access with two large-bore peripheral IVs
- Start broad-spectrum IV antibiotics: See “Severe infection” in “Empiric antibiotic therapy for intraabdominal infection.”
- Obtain an urgent surgical consult to determine whether surgery or conservative management is appropriate.
- Patients with signs of sepsis and/or shock additionally require:
- Immediate hemodynamic support, e.g., aggressive IV fluid resuscitation
- Urgent critical care consult
- Begin supportive care (e.g., analgesics, antiemetics).
- Reevaluate frequently (serial abdominal examination, vital signs), as the patient's condition may rapidly deteriorate.
Supportive care
- NG tube with continuous or intermittent suction
- Consider IV PPI, e.g., pantoprazole for patients with suspected perforated peptic ulcer. [11]
-
Parenteral analgesics
-
Opioid analgesics [12]
- Morphine
- Meperidine
- Hydromorphone
- Tramadol
- NSAIDs: Diclofenac
-
Opioid analgesics [12]
- Parenteral antiemetics (see “Antiemetics”)
- Ondansetron
- Promethazine
Ketorolac is contraindicated in patients with suspected bowel perforation.
Opioids are contraindicated in patients with suspected bowel obstruction.
Surgical management [13]
Most patients with GI tract perforation should be managed with urgent explorative laparotomy.
-
Indications:
- Signs of generalized peritonitis
- Signs of sepsis
-
Procedure: Exploratory laparotomy with midline incision is usually preferred.
- Obtain peritoneal fluid for cultures.
- Thorough peritoneal lavage with saline [14]
- Closure of the perforation, if feasible
- Primary closure with/without an omental pedicle
- Resection of the perforated segment of bowel with primary anastomosis or temporary stoma creation
- If perforated appendix identified: Perform an appendectomy.
- If malignancy is identified (e.g., perforated colon cancer):
- Consider curative resection.
- Obtain intraoperative biopsies of the mass if resection is not possible.
- Place peritoneal drains and close the abdomen.
-
Postoperative care
- Continue bowel rest, IV fluids, and NG tube with suction until normal bowel function returns (see “conservative management” below).
- Identify and treat the underlying condition. [15]
Conservative management [11][15]
Patients with only localized peritonitis and no signs of sepsis may be candidates for conservative (nonsurgical) management.
- NPO, maintenance IV fluids, and IV PPI (see “Supportive care” above)
- IV broad-spectrum antibiotics: See “Severe infection” in “Empiric antibiotic therapy for intraabdominal infection”
- If imaging shows evidence of an abscess: Consider image-guided percutaneous drainage of abscess. [16]
- Serial abdominal examination
- Further management:
- If there are clinical signs of improvement : Obtain an abdominal x-ray with water-soluble contrast to confirm that the perforation has sealed.
- No leakage of contrast: Initiate enteral feeds and switch to oral antibiotics.
- If there are clinical signs of deterioration : exploratory laparotomy
- If there are clinical signs of improvement : Obtain an abdominal x-ray with water-soluble contrast to confirm that the perforation has sealed.
Traumatic hollow viscus injury
See “Primary survey” for the general approach to trauma patients; see also “Blunt abdominal trauma” (BAT) and “Penetrating abdominal trauma.”
Diagnosis [17][18]
-
Emergency surgery consult (prior to imaging) in patients with :
- Suspected GI perforation due to penetrating abdominal trauma
- Suspected traumatic GI perforation with hemodynamic instability
-
Maintain high index of suspicion: Clinical features may be subtle.
- Patients with BAT are at elevated risk, especially if they also have : [18]
- High-energy injury: e.g., resulting from high-speed motor vehicle collision
- Seat belt sign (typical injury after a vehicle collision with ecchymoses on the neck or on the flank caused by the seat belt strap) with pain and guarding
- Other injuries associated with hollow viscus injury: e.g., abdominal aortic injury, L-spine transverse fracture
- Iatrogenic injury: Suspect in patients with clinical features of GI perforation following recent liver biopsy, paracentesis, peritoneal dialysis or lavage, or GI endoscopy.
- Patients with BAT are at elevated risk, especially if they also have : [18]
-
CT abdomen: test of choice for all stable patients
- In patients with BAT, evidence of hollow viscus injury may be absent on the initial CT abdomen.
- Consider repeat imaging in at-risk patients with BAT, especially if they have:
- Persistent pain
- Pain out of proportion
- Delayed peritoneal signs
Maintain a high index of suspicion for hollow viscus injury in patients with blunt abdominal trauma as clinical features may initially be very subtle. [18]
Management
- All patients: Administer broad-spectrum IV antibiotics and provide supportive care and monitoring identical to that for nontraumatic GI perforation.
- Patients with sepsis, peritonitis, or hemodynamic instability: Operative management is indicated.
- Stable patients with penetrating abdominal trauma: Operative management is typically indicated. [19][20]
- Stable patients with any other traumatic etiologies: Consult surgery to determine if operative or nonoperative management is most appropriate. [18][21][22][23]
Complications
- Peritonitis
- Bacteremia
- Sepsis
- Multiorgan dysfunction
- Intraabdominal abscess
- Intraabdominal adhesions
- Subhepatic abscess
- Pyogenic liver abscess
- Pelvic abscess
- Postoperative complications
We list the most important complications. The selection is not exhaustive.
External Resources
References
- "Bowel Perforation"
- Behrman SW. "Management of Complicated Peptic Ulcer Disease". Arch Surg. 140(2). :201. (2005)
- Helderman H, Goral S. "Gastrointestinal Complications of Transplant Immunosuppression". Journal of the American Society of Nephrology. 13(1). (2002)
- Mayumi T, Yoshida M, Tazuma S, et al. "Practice Guidelines for Primary Care of Acute Abdomen 2015". Journal of Hepato-Biliary-Pancreatic Sciences. 23(1). :3-36. (2015)
- "American College of Radiology ACR Appropriateness Criteria® Acute Nonlocalized Abdominal Pain". https://acsearch.acr.org/docs/69467/Narrative/. [2018-01-01]
- Kuzmich S, Burke CJ, Harvey CJ, Kuzmich T, Fascia DTM. "Sonography of Small Bowel Perforation". American Journal of Roentgenology. 201(2). :W283-W291. (2013)
- Eisenberg RL, Johnson NM. "Comprehensive Radiographic Pathology - E-Book". Elsevier Health Sciences. (2015). ISBN: 9780323370257
- Bacci M, Kushwaha R, Cabrera G, Kalivoda EJ. "Point-of-Care Ultrasound Diagnosis of Pneumoperitoneum in the Emergency Department.". Cureus. 12(6). :e8503. (2020)
- Khor M, Cutten J, Lim J, Weerakkody Y. "Sonographic detection of pneumoperitoneum.". BJR case rep. 3(4). :20160146. (2017)
- Chung KT, Shelat VG. "Perforated peptic ulcer - an update". World Journal of Gastrointestinal Surgery. 9(1). :1. (2017)
- Rushfeldt CF, Sveinbjørnsson B, Søreide K, Vonen B. "Risk of anastomotic leakage with use of NSAIDs after gastrointestinal surgery". Int J Colorectal Dis. 26(12). :1501-1509. (2011)
- Weledji EP, Ngowe MN. "The challenge of intra-abdominal sepsis". International Journal of Surgery. 11(4). :290-295. (2013)
- Sartelli M, Catena F, Di Saverio S, et al. "Current concept of abdominal sepsis: WSES position paper". World Journal of Emergency Surgery. 9(1). (2014)
- Søreide K, Thorsen K, Harrison EM, et al. "Perforated peptic ulcer". Lancet.. 386(10000). :1288-1298. (2015)
- Khalil HA, Yoo J. "Colorectal emergencies: perforated diverticulitis (operative and nonoperative management).". J Gastrointest Surg. 18(4). :865-8. (2014)
- Walls R, Hockberger R, Gausche-Hill M. "Rosen's Emergency Medicine". Elsevier Health Sciences. (2018). ISBN: 9780323354790
- Bège T, Brunet C, Berdah SV. "Hollow viscus injury due to blunt trauma: A review". Journal of Visceral Surgery. 153(4). :61-68. (2016)
- Como JJ, Bokhari F, Chiu WC, et al. "Practice Management Guidelines for Selective Nonoperative Management of Penetrating Abdominal Trauma". Journal of Trauma: Injury, Infection & Critical Care. 68(3). :721-733. (2010)
- De Moya M, Goldstein AL. "Non-operative Management of Penetrating Abdominal Injuries: An Update on Patient Selection". Current Surgery Reports. 7(6). (2019)
- Paspatis G, Dumonceau J-M, Barthet M, et al. "Diagnosis and management of iatrogenic endoscopic perforations: European Society of Gastrointestinal Endoscopy (ESGE) Position Statement". Endoscopy. 46(08). :693-711. (2014)
- Lohsiriwat V. "Colonoscopic perforation: Incidence, risk factors, management and outcome". World Journal of Gastroenterology. 16(4). :425. (2010)
- Putcha RV, Burdick JS. "Management of iatrogenic perforation". Gastroenterol Clin North Am. 32(4). :1289-1309. (2003)
- "Contributor Disclosures - Gastrointestinal perforation. All of the relevant financial relationships listed for the following individuals have been mitigated: Jan Schlebes (medical editor, is a shareholder in Fresenius SE & Co KGaA). None of the other individuals in control of the content for this article reported relevant financial relationships with ineligible companies. For details, please review our full conflict of interest (COI) policy:"
- Mavroudis CD, Kucharczuk JC. "Acute Management of Esophageal Perforation". Curr Surg Rep. 2(1). (2013)
- Kaman L. "Management of Esophageal Perforation in Adults". Gastroenterol Res. (2011)
- Mazuski JE, Tessier JM, May AK, et al. "The Surgical Infection Society Revised Guidelines on the Management of Intra-Abdominal Infection". Surg Infect (Larchmt). 18(1). :1-76. (2017)
- Søreide J, Viste A. "Esophageal perforation: diagnostic work-up and clinical decision-making in the first 24 hours". Scand J Trauma Resusc Emerg Med. 19(1). :66. (2011)
- Sartelli M, Viale P, Catena F, et al. "2013 WSES guidelines for management of intra-abdominal infections". World Journal of Emergency Surgery. 8(1). :3. (2013)
- "Bowel perforation". https://radiopaedia.org/articles/bowel-perforation-1
- Sepesi B, Raymond DP, Peters JH. "Esophageal perforation: surgical, endoscopic and medical management strategies". Curr Opin Gastroenterol. 26(4). :379-383. (2010)
- Akgul GG, Yenidogan E, Ozsoy Z, et al. "Conservative Management of Large Rectosigmoid Perforation under Peritoneal Reflection: Case Report and Review of the Literature". Case Reports in Surgery. 2015. :1-4. (2015)