Summary
Oncology is the science of tumors. This article explains basic concepts relevant to the development, progression, spread, and diagnosis of cancer. Histological analysis helps to determine tumor type and grade, whereas the TNM classification system is used to assess staging. Because it is standardized and used internationally, the TNM classification helps unify oncological research and therapy protocols. Metastasis occurs via different pathways mainly by hematogenous or lymphatic spreading.
Principles of cancer care, paraneoplastic syndromes, and tumor markers are covered in detail in their respective articles.
Nomenclature
Terminology
| Basic terminology in oncology | |
|---|---|
| Term | Definition |
| Normal cell |
|
| Neoplasia |
|
| Tumor |
|
| Adenoma |
|
| Carcinoma |
|
| Sarcoma |
|
| Hamartoma |
|
| Choristoma |
|
| Dysplasia |
|
| Carcinoma in situ (CIS) |
|
| Invasive carcinoma |
|
| Metastasis |
|





 1/3")
")


Benign and malignant tumors
| Overview of benign and malignant tumors | ||
|---|---|---|
| Benign tumor | Malignant tumor | |
| Differentiation(grading) |
|
|
| Growth |
|
|
| Macroscopy |
|
|
| Microscopy |
|
|
| Metastasis and relapse |
|
|
Tumor origin
| Types of tumors based on cell origin | |||
|---|---|---|---|
| Type of tumors | Cell origin | Benign tumor | Malignant tumor |
| Epithelial tumors |
|
|
|
|
|
||
|
|
|
|
|
|
||
| Mesenchymal tumors |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| |||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| Special variants of mesenchymal tumors |
|
|
|
|
|
||
| Neuroectodermal tumors |
|
|
|
|
|
|
|
| Germ cell tumors |
|
|
|
| Embryonal tumors |
|
|
|
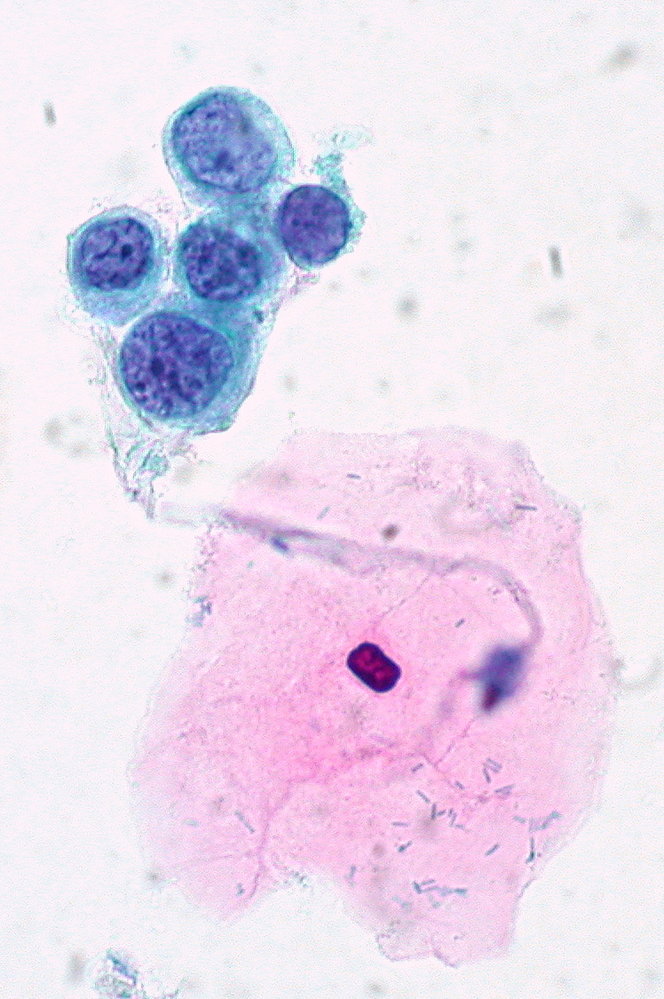
Photomicrograph of squamous cells of the cervix (Papanicolaou stain; very high magnification;)
There is a loosely connected group of abnormal squamous epithelial cells (blue-green cytoplasm). The nuclei are variable in size with a high nuclear-cytoplasmic ratio and there are course clumps of chromatin. The large cell with pink cytoplasm is a normal superficial squamous cell.
These findings are characteristic of severe dysplasia as seen in high-grade squamous intraepithelial lesion (HSIL).
Source: “High-Grade SIL, ThinPrep” by Ed Uthman, Flickr, licensed under CC BY 2.0.
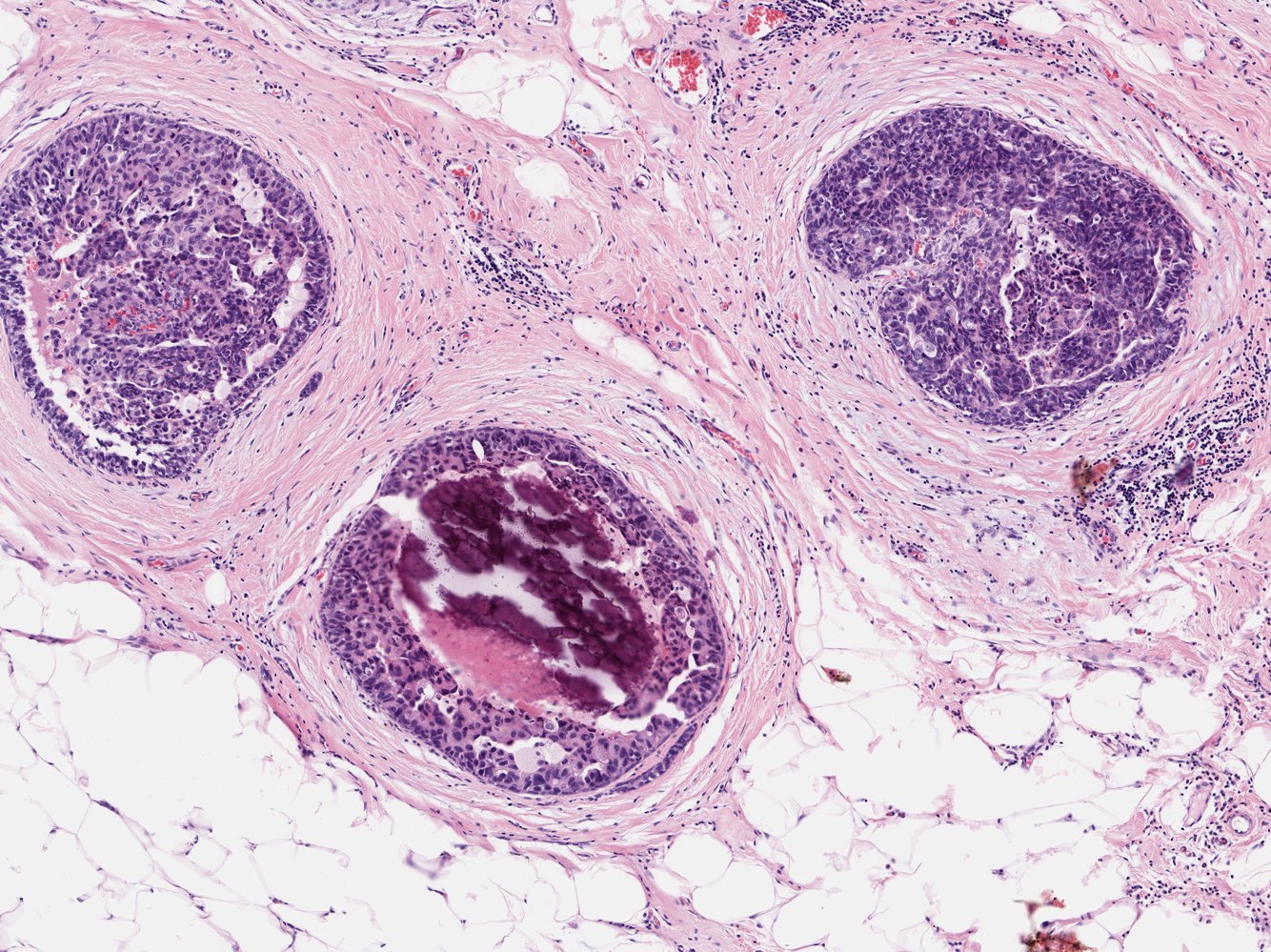
Photomicrograph of a breast tissue biopsy specimen (H&E stain; high magnification)
Intraductal tumor cells (green overlay) with a hyperchromatic nucleus are visible. Calcifications (red overlay) are visible in the lower duct.
These are characteristic histological features of ductal carcinoma in situ.
Click on the Smartzoom button to view the entire specimen through a virtual microscope.
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: PD Dr. Alberto Perez Bouza
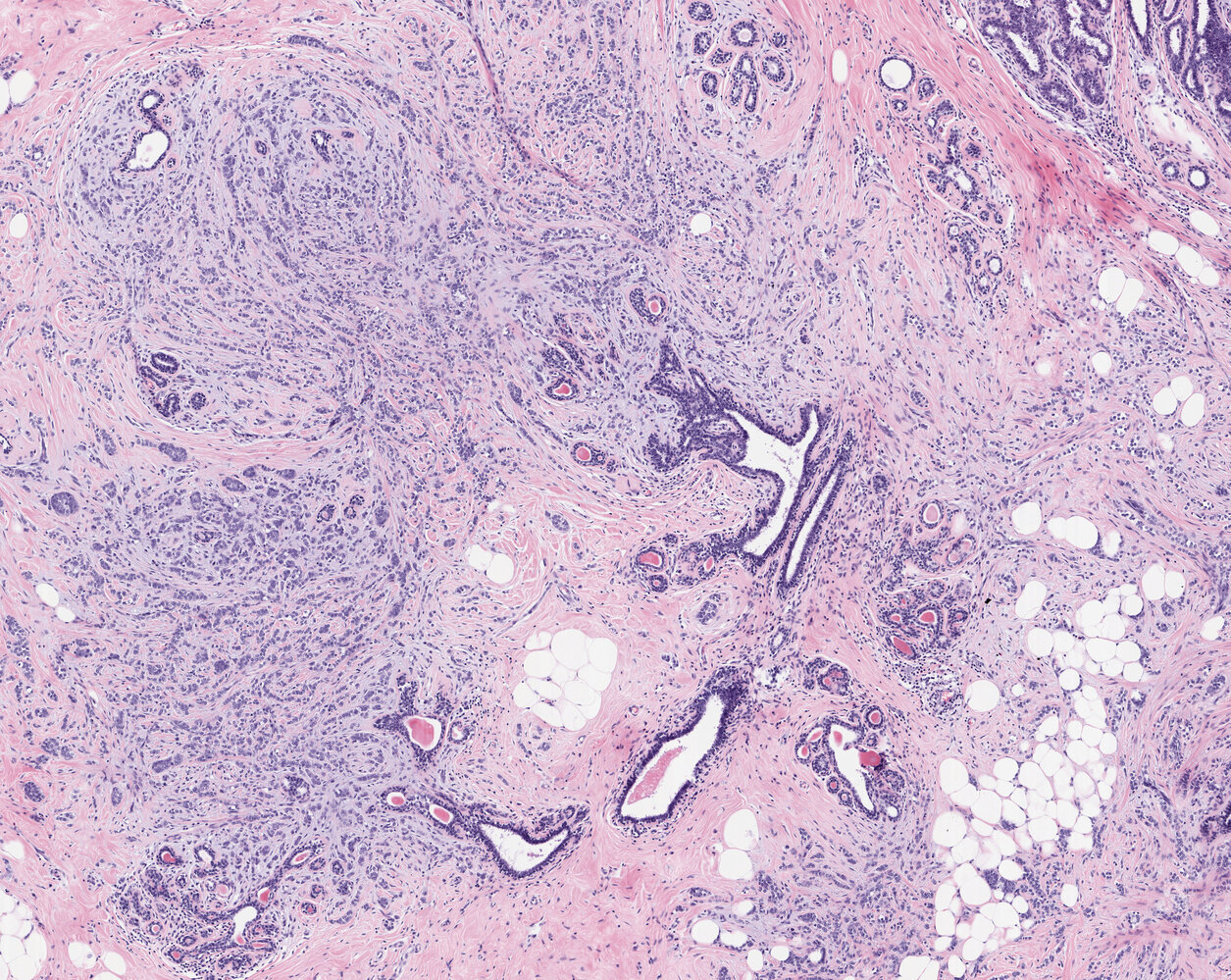
Photomicrograph of a breast tumor tissue specimen (H&E stain; 40x magnification)
Infiltrating malignant cells can be seen as single cells, narrow chords (examples indicated by green overlay), and characteristic single-file formations (examples indicated by blue overlay). The tumor cells are seen growing between distorted ductuli (D) and lobuli (L), surrounded by conspicuously pale connective tissue. There is no tubule formation of the tumor (as is commonly seen in other types of adenocarcinomas of the breast).
This is the typical appearance of invasive lobular carcinoma of the breast.
Click on the microscope icon (at the top) to view the entire specimen through a virtual microscope.
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: PD Dr. Alberto Perez Bouza
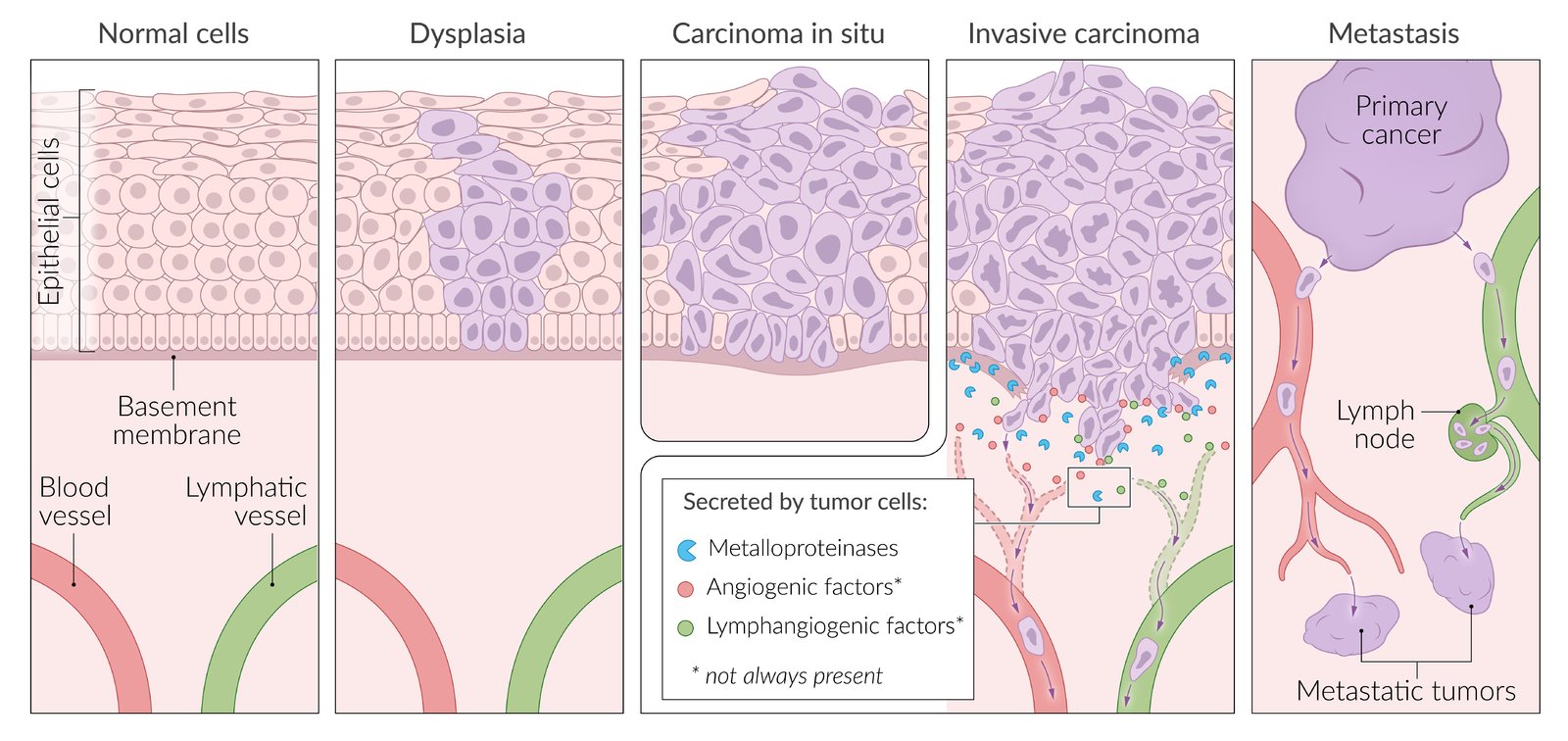
Typical neoplastic disease progression begins with the appearance of dysplastic cells, which have varying nuclei sizes and shapes, and disrupt surrounding tissue architecture. The cells continue to proliferate and become more dysplastic resulting in the formation of carcinoma-in-situ, which is still contained by the basement membrane (BM). Expression of metalloproteases enables the cells to break through the BM and the cancerous cells can then enter the vascular system and metastasize to distant locations. Expression of angiogenic or lymphangiogenic factors promote the recruitment of vessels, thereby facilitating metastasis.
© AMBOSS
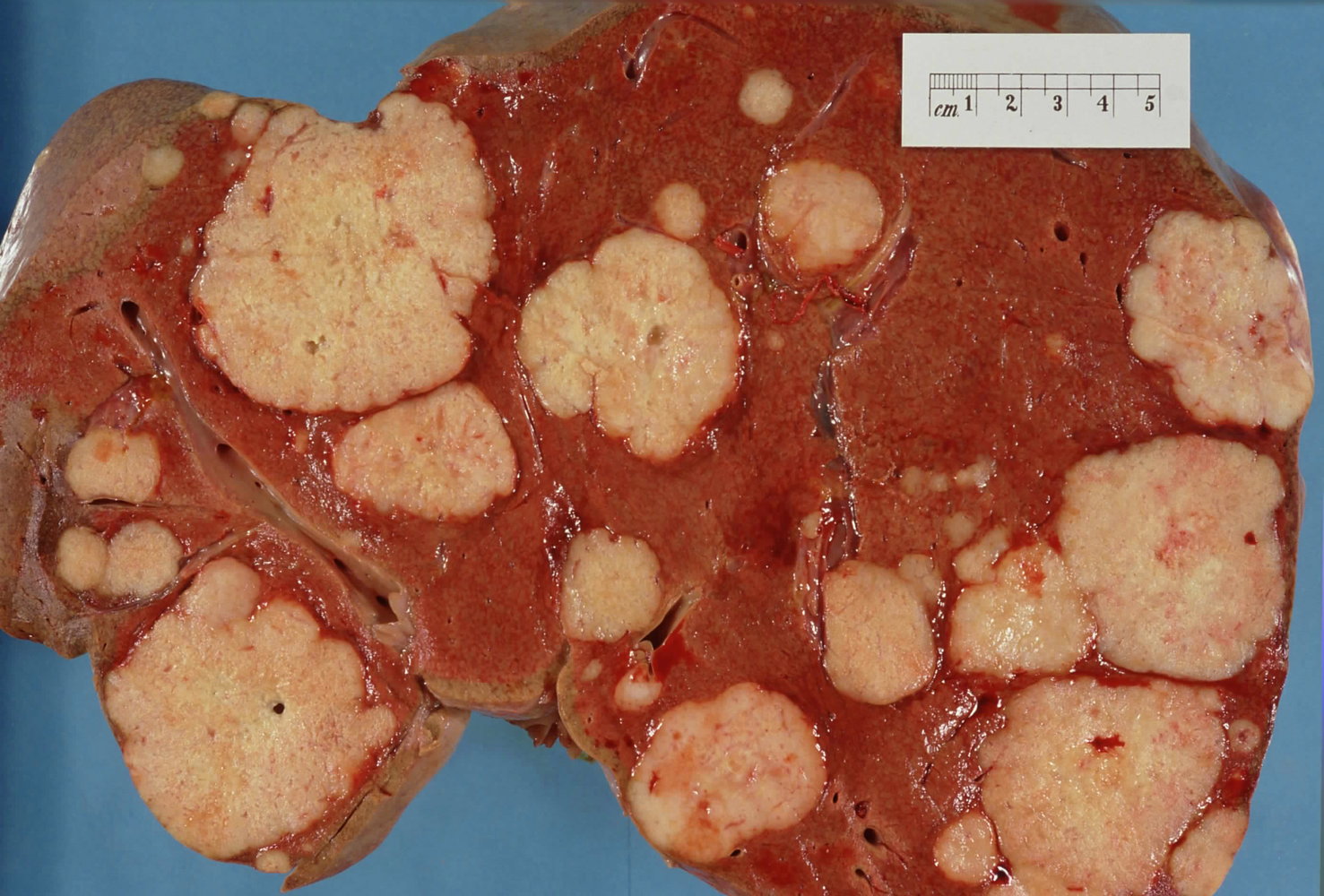
Cross section of autopsied human liver
Numerous variably-sized pale or white-tan nodules scattered throughout the liver. The tumor is an adenocarcinoma. One of the most primary sites for metastatic adenocarcinoma is the liver.
Source: "Secondary tumor deposits in the liver from a primary cancer of the pancreas", Haymanj, Wikimedia Commons licensed under Public Domain
{kind=link}
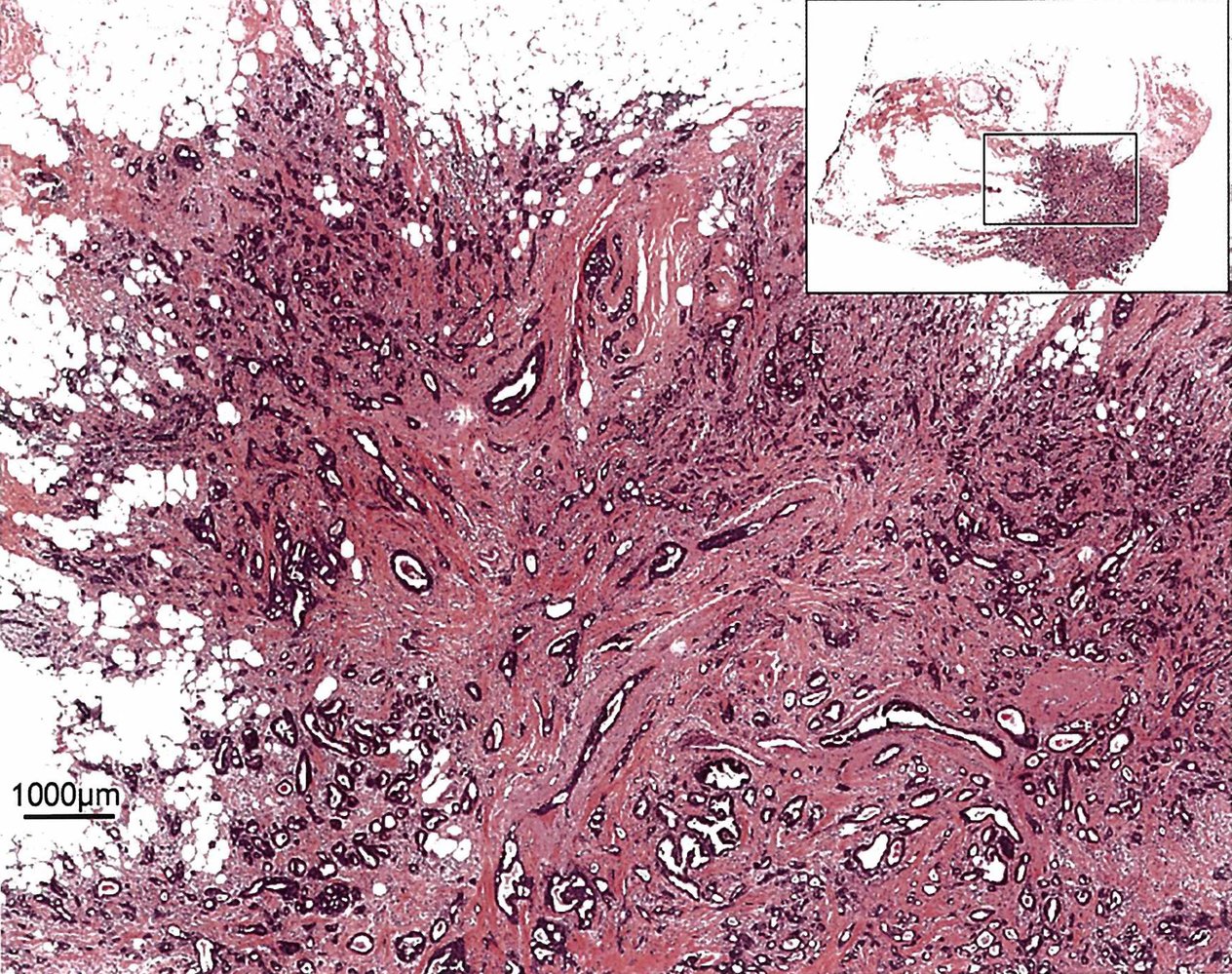
Photomicrograph of biopsy specimen (H&E stain; low magnification) from a mobile breast lump in 64-year-old female patient
Main image: At low magnification, a dense irregular mass (purple/pink) with poorly circumscribed borders can be seen infiltrating the mature adipose tissue of the breast (white). The mass is composed of disorganized tubular formations of the carcinoma (dark blue/basophilic staining) and surrounding collagenous connective tissue (pink/eosinophilic staining; also known as “desmoplastic stroma”).
Top right inset: very low magnification overview indicating the location of the main image on the specimen
Source: © IMPP
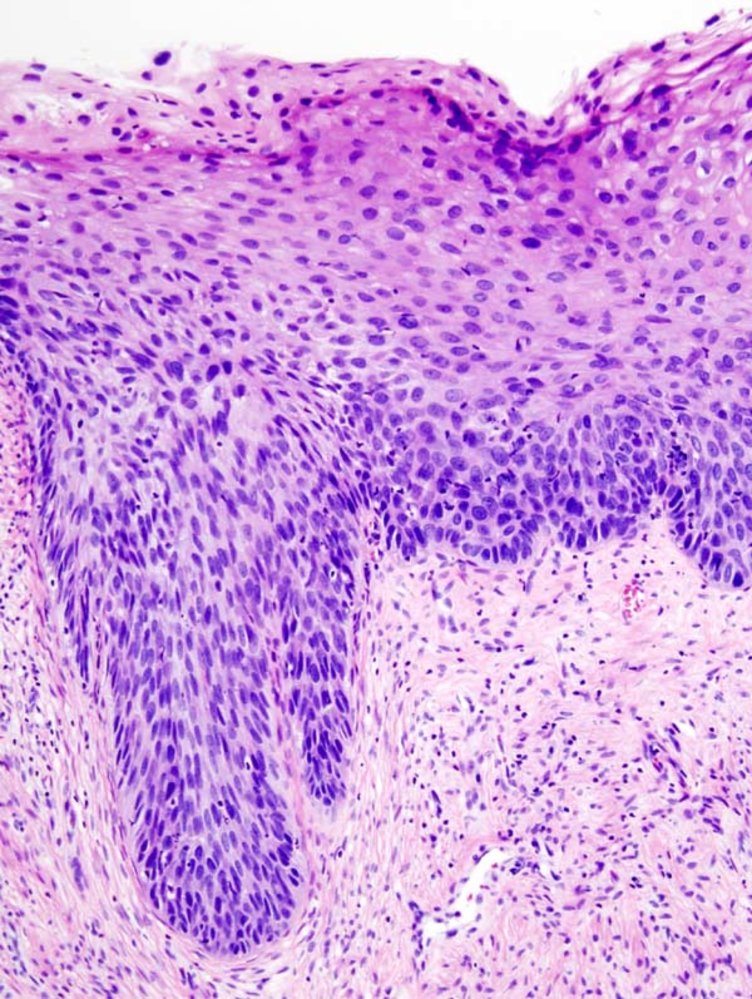
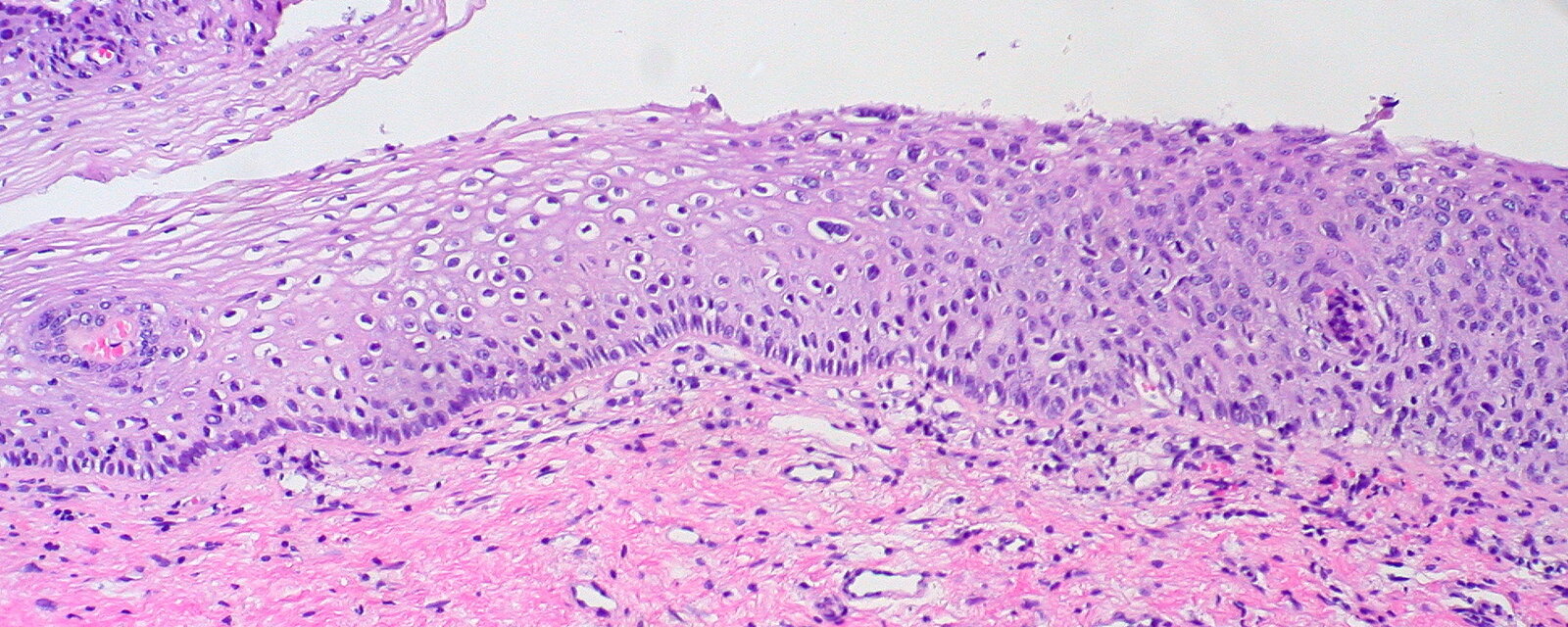
Photomicrograph of cervical tissue (H&E stain; very high magnification;)
There is a loss of epithelial architecture involving more than two-thirds of the epithelium, but the basement membrane is still intact. There is a high nuclear-to-cytoplasmic ratio, overlapping nuclei, and nuclear atypia. Mitotic figures can be seen. Epithelial cells with perinuclear halos are present in the superficial layers; these cells are koilocytes and indicate HPV infection.
These findings are consistent with severe dysplasia and (CIN III), and the changes are irreversible
Source: “Cervical intraepithelial neoplasia (4) CIN3” by KGH, Wikimedia Commons, licensed under CC BY-SA 3.0.
_CIN3.jpg){kind=link}
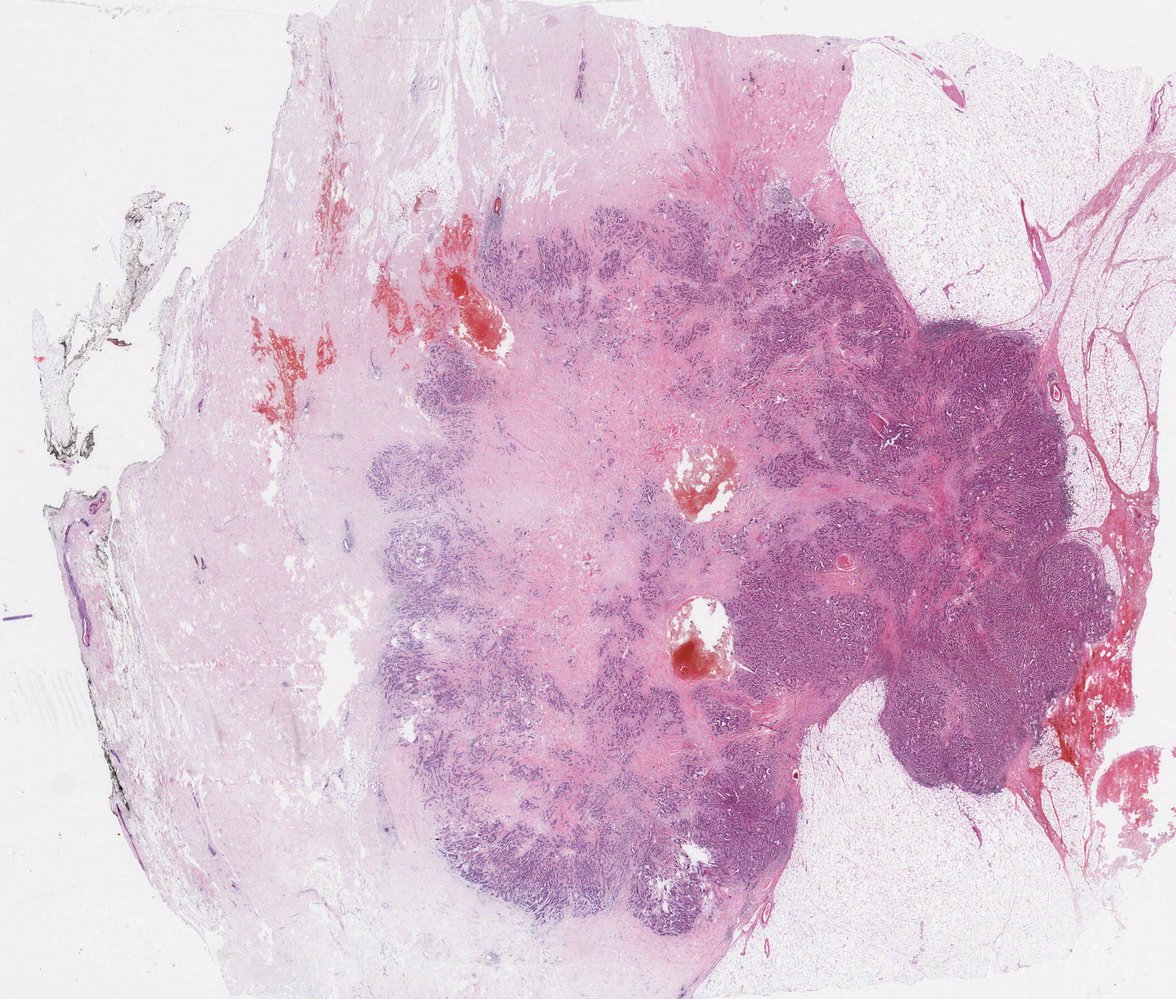
Photomicrograph of a surgical sample of breast tissue (H&E stain, low magnification)
An area of sclerosis (light purple) is visible in the center of the invasive ductal carcinoma (dark purple).
Click on the Smartzoom button to view the entire specimen through a virtual microscope.
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: PD Dr. Alberto Perez Bouza
Photomicrograph of a cervical biopsy specimen (H&E stain; high magnification)
1. Normal squamous epithelium (N; green overlay): normal nuclear-cytoplasmic ratio, intact cell polarity (epithelial cells have distinct lateral, apical, and basal membrane domains)
2. Mild dysplasia (1; yellow overlay): mild pleomorphism (loss of uniformity in cell size and shape), mild chromatin abnormalities (hyperchromatic), koilocytes (cells with perinuclear halos), dysplasia confined to the basal third of the epithelium
3. Moderate dysplasia (2; blue overlay): loss of cell polarity, moderate nuclear pleomorphism, moderate nuclear chromatin abnormalities, increased normal and abnormal mitosis, dysplasia confined to the basal two-thirds of the epithelium
4. Severe dysplasia (3; red overlay): irreversible high-grade dysplasia, irregular epithelial stratification, involves the entire thickness of the epithelium, clear demarcated basement membrane (no invasion)
Koilocytes in dysplastic cervical epithelium indicate an underlying persistent HPV infection as the cause of dysplasia.
Source: “Spectrum of SIL/Cervical Dysplasia” by Ed Uthman, Flickr, licensed under CC BY 2.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
General epidemiology
In 2020, approximately 1.8 million people will be diagnosed with cancer in the United States. Cancer is the 2nd leading cause of death; after heart disease. The most common type of cancer in both men and women is skin cancer, with basal cell carcinoma being more common than squamous cell carcinoma and melanoma. [1]
Epidemiology of common cancer types in 2020 [2]
The following numbers are an estimation of new cancer cases and their mortality in the United States (excluding skin cancer ).
| Epidemiology of most common cancer types | |||
|---|---|---|---|
| Type | Incidence/year in men | Incidence/year in women | Mortality/year |
| Breast cancer | 2,620 | 276,480 | 42,690 |
| Lung and bronchus cancer | 116,300 | 112,520 | 135,720 |
| Prostate cancer | 191,930 | N/A | 33,330 |
| Colorectal cancer | 78,300 | 69,650 | 53,200 |
| Bladder cancer | 62,100 | 19,300 | 17,980 |
| Kidney cancer | 45,520 | 28,230 | 14,830 |
| Uterine cancer | N/A | 65,620 | 12,590 |
| Pancreatic cancer | 30,400 | 27,200 | 47,050 |
| Thyroid cancer | 12,720 | 40,170 | 2,180 |
| Non-Hodgkin lymphoma | 42,380 | 34,860 | 19,940 |
| Leukemia | 35,470 | 25,060 | 23,100 |
-
The most common types of cancer in men (excluding skin cancer)
- Prostate cancer
- Lung and bronchus cancer
- Colorectal cancer
-
The most common cancer in women (excluding skin cancer)
- Breast cancer
- Lung and bronchus cancer
- Colorectal cancer
-
The types of cancer with the highest mortality rate in both men and women (in descending order)
- Cancer of lung and bronchus
- Prostate cancer (men), breast cancer (women)
- Colorectal cancer
-
The most common types of cancer that have the greatest mortality rate in children (< 15 years)
- Leukemia (ALL, AML)
- Brain and spinal cord tumors
- Neuroblastoma
")
")
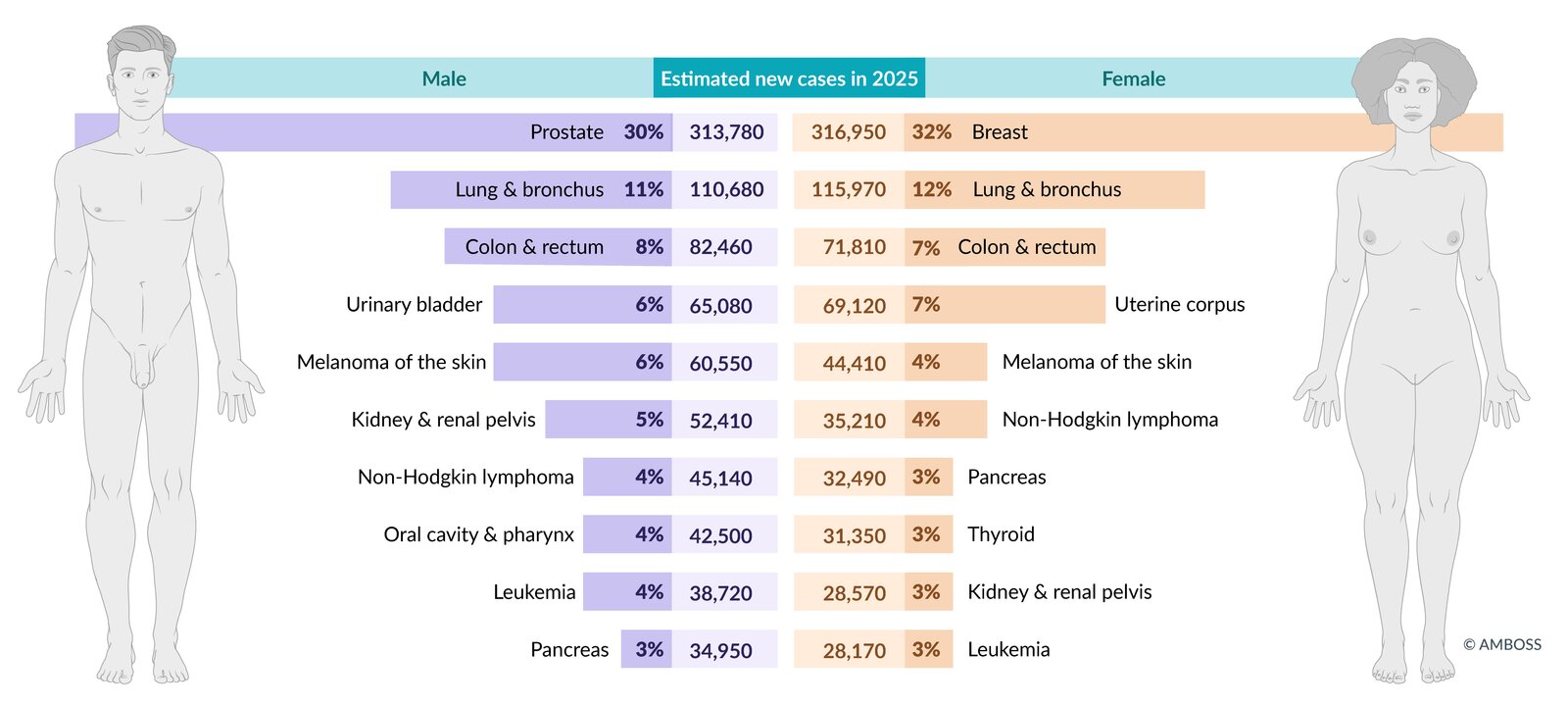
Estimated incidence of the most common cancers in the US in total figures and as a percentage of total cancer incidence (excluding non-melanoma skin cancers and in-situ carcinoma, except urinary bladder). Figures are prospective estimates of the American Cancer Society for 2025.
© AMBOSS. Data source: Cancer Facts & Figures 2024, American Cancer Society, access date 06/28/24 (https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/annual-cancer-facts-and-figures/2024/2024-cancer-facts-and-figures-acs.pdf)
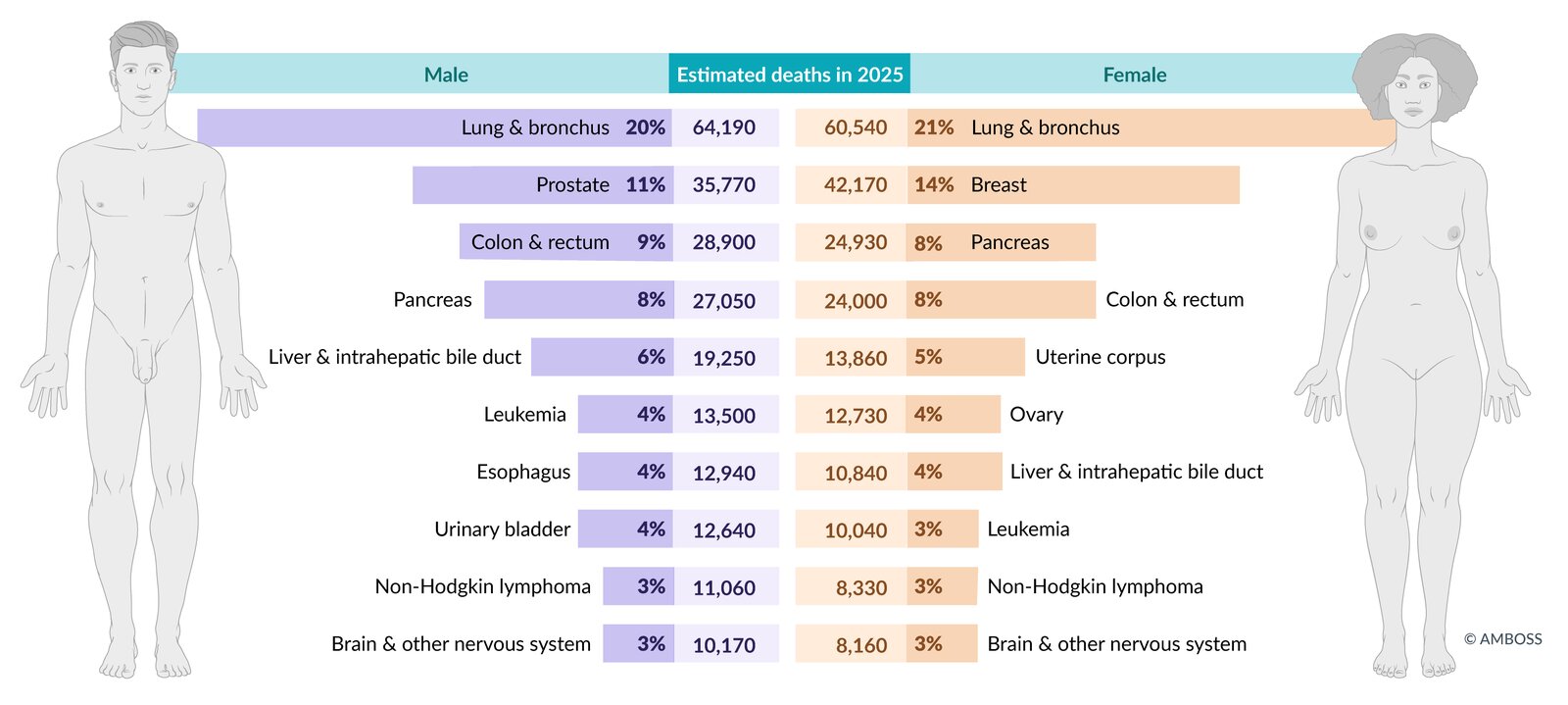
Estimated mortality from the most common cancers in the US in total figures and as a percentage of total cancer mortality. Figures are prospective estimates of the American Cancer Society for 2025.
© AMBOSS. Data source: Cancer Facts & Figures 2024, American Cancer Society, access date 06/28/24 (https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/annual-cancer-facts-and-figures/2024/2024-cancer-facts-and-figures-acs.pdf)
Carcinogenesis
Overview
- Definition: a multistep process by which normal cells develop and accumulate genetic mutations (inherited or acquired), resulting in a monoclonal expansion of mutated cells that can progress to the development of neoplasia
-
Process
- Initiation: DNA damage
- Promotion: DNA damage passed on
- Latency: the time between promotion and progression
- Progression: proliferation of the neoplastic cell line with the acquired DNA damage, leading to malignant transformation

Properties of malignant cells
-
Sustained proliferative signaling: due to mutation of genes regulating cell division and growth
- (Proto‑)oncogene: See “Proto-oncogene” below.
- Growth factor receptors (e.g., ERBB2, EGFR)
- Signaling molecules (e.g., Ras, B-Raf) [3]
- Transcription factors (e.g., MYC, TP53) [4]
- Cell cycle regulators (e.g., cyclins, CDKs)
-
Evade growth suppressors [5]
- Tumor suppressor genes: See “Tumor suppressor genes” below.
-
Loss of contact inhibition
- Mutated or absent E-cadherin → loss of growth inhibitory signals and contact inhibition of proliferation → excessive cell proliferation
- Due to mutations in genes that regulate contact inhibition (e.g., NF2 gene)
-
Genome instability and mutations
- Mutations: See “Gene mutations” and “Chromosomal translocation” in the “Basics of human genetics” article.
- Gene amplification: increased gene expression (e.g., overexpression of ERBB2 gene in several forms of breast cancer)
-
Resist cell death
- Occurs because of mutations in apoptosis regulatory genes
- Loss of regulatory genes (e.g., Bax, TP53, BCL-2) leads to cell immortality and increased proliferation.
- Enable replicative immortality: telomerase reactivation → ↑ length of telomeres → ↑ number of possible cell replication cycles
-
Deregulate cellular energetics: a shift in cellular metabolism from glycolysis and mitochondrial oxidative phosphorylation to glycolysis and preferential lactate generation, regardless of the oxygen supply (Warburg effect)
- In differentiated, non-malignant cells, glycolysis converts glucose to pyruvate, which then undergoes mitochondrial oxidative phosphorylation under aerobic conditions, or anaerobic glycolysis to generate lactate under anaerobic conditions.
- In malignant cells, the so-called Warburg effect occurs, in which pyruvate is preferentially converted to lactate, regardless of the cellular oxygen supply. This mechanism supplies rapidly dividing malignant cells with the necessary carbon to synthesize cellular structures. [6]
-
Induce angiogenesis [5]
- Angiogenesis helps maintain an adequate supply of oxygen and nutrients to the neoplastic cells.
- Regulated by angiogenic (e.g., VEGF, FGF) and inhibitory factors that are produced by neoplastic or supporting cells
- Occurs as:
- Vasculogenesis: de novo formation of blood vessels from bone marrow-derived endothelial cells
- Neoangiogenesis: formation of blood vessels from existing blood vessels and capillaries
- Newly formed blood vessels may be dilated or leaky.
- Activate invasion and metastasis: See “Metastasis” below.
- Avoid immune detection: See “Defense mechanisms of malignant cells” below.
- Tumor-promoted inflammation



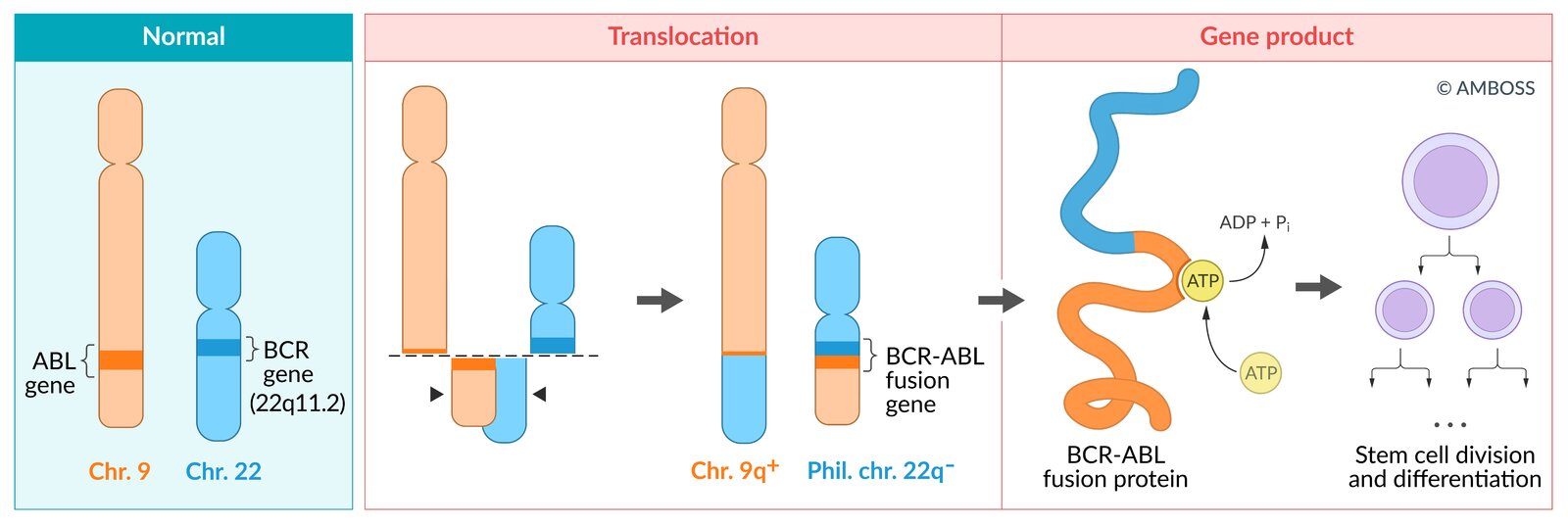
(q34;q11) Philadelphia chromosome")
Defense mechanisms of malignant cells [7]
-
Immune response modification
- ↓ MHC class I expression on malignant cells → inability of cytotoxic T-cells to recognize and mount an immune response against these cells
- Secretion of immunosuppressive molecules (e.g., TGF-β) → enhanced immune tolerance of malignant cells
- Enhanced regulatory T-cell activity → limited immune response
-
Immune checkpoints [8]
-
Cytotoxic T-lymphocyte-associated protein 4 (CTLA-4)
- Upregulation of CTLA-4 → promotion of binding to B7 protein (surface receptor on antigen-presenting cells, also called CD80 or CD86) → T-cell inactivation and simultaneous reduction of costimulation by binding of CD28 to B7
- CTLA-4 is inhibited by anti-CTLA-4 antibody ipilimumab.
-
Programmed death-ligand system
- Expression of programmed death-ligand 1 (PD-L1) and PD-L2 on tumor cells surface or environment → binding to programmed cell death protein 1 (PD-1) on T-cells → T-cell dysfunction
- PD-L1 and PD-L2 are inhibited by cancer immunotherapy agents atezolizumab, durvalumab, and avelumab.
- PD-1 is inhibited by cancer immunotherapy agents nivolumab and pembrolizumab.
-
Cytotoxic T-lymphocyte-associated protein 4 (CTLA-4)
-
Development of resistance to chemotherapeutic agents
- Expression of multidrug resistance protein 1 (MDR1; also called P-glycoprotein). [9]
- P-glycoproteins are transmembrane ATP-dependent efflux pump proteins that decrease intracellular concentrations of chemotherapeutics.
- Expressed in adrenocortical carcinoma as well as cancers of the colon, liver, pancreas, kidney, ovary, and breast


Etiologic field cancerization [10]
- Definition: a collection of factors (e.g., lifestyle, environmental, microbial, genetic) and their interactions that affect tissues and potentially predispose individuals to the development of disease
- Pathophysiology: carcinogenic exposure → transformation of normal cells → wide area of premalignant cells at the primary site and adjacent areas
-
Examples
- Interactions between the immune system, microbiome, and diet influence the development of ulcerative colitis and colorectal cancer.
- Prolonged exposure to tobacco smoke, alcohol consumption, and persistent HPV infection influence the development of head and neck cancer.
- Chronic sun exposure, UV radiation, and genetic predisposition influence the development of skin cancer.
- Exposure to industrial carcinogens, chronic inflammation, and genetic susceptibility influence the development of bladder cancer.
© AMBOSS
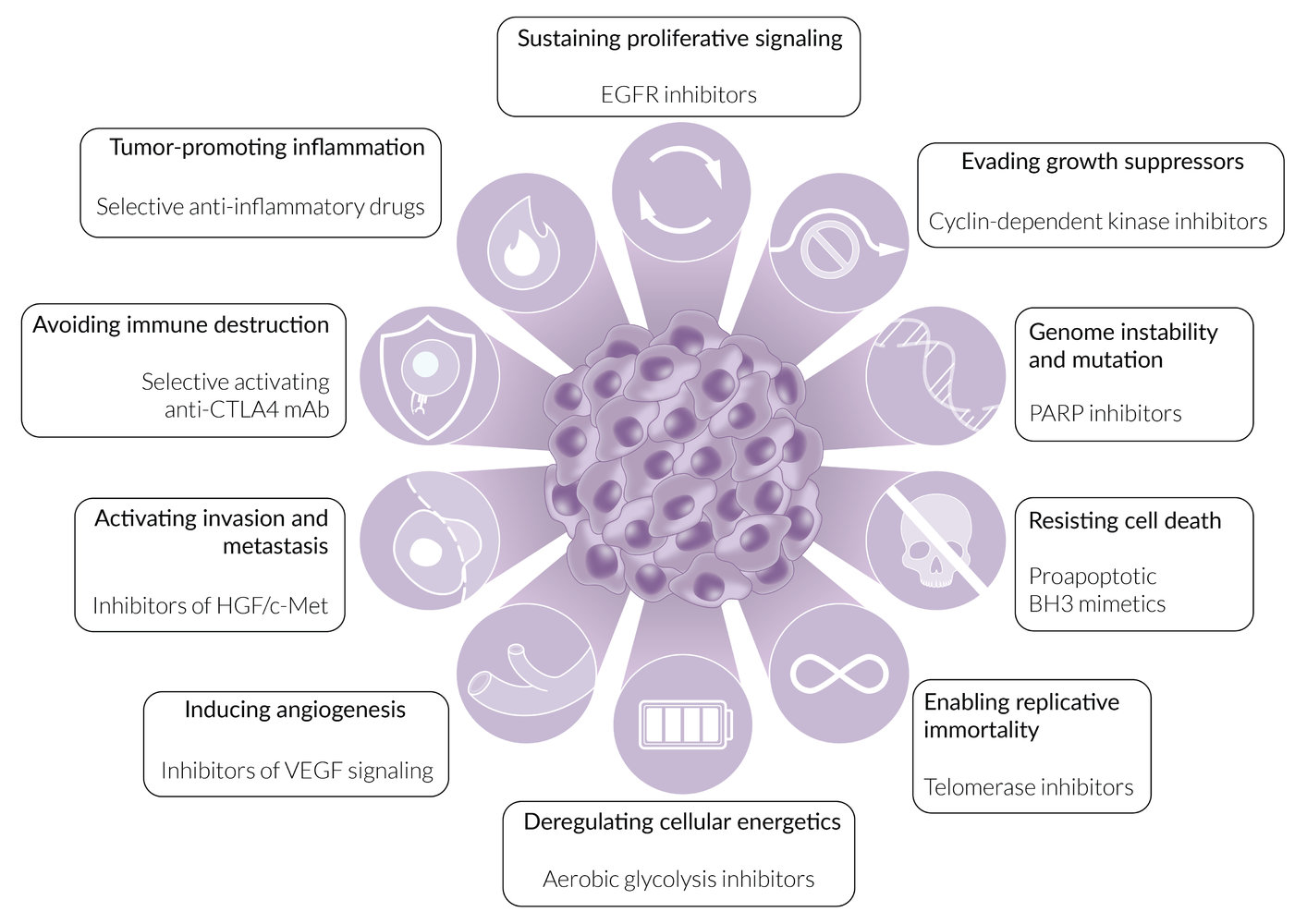
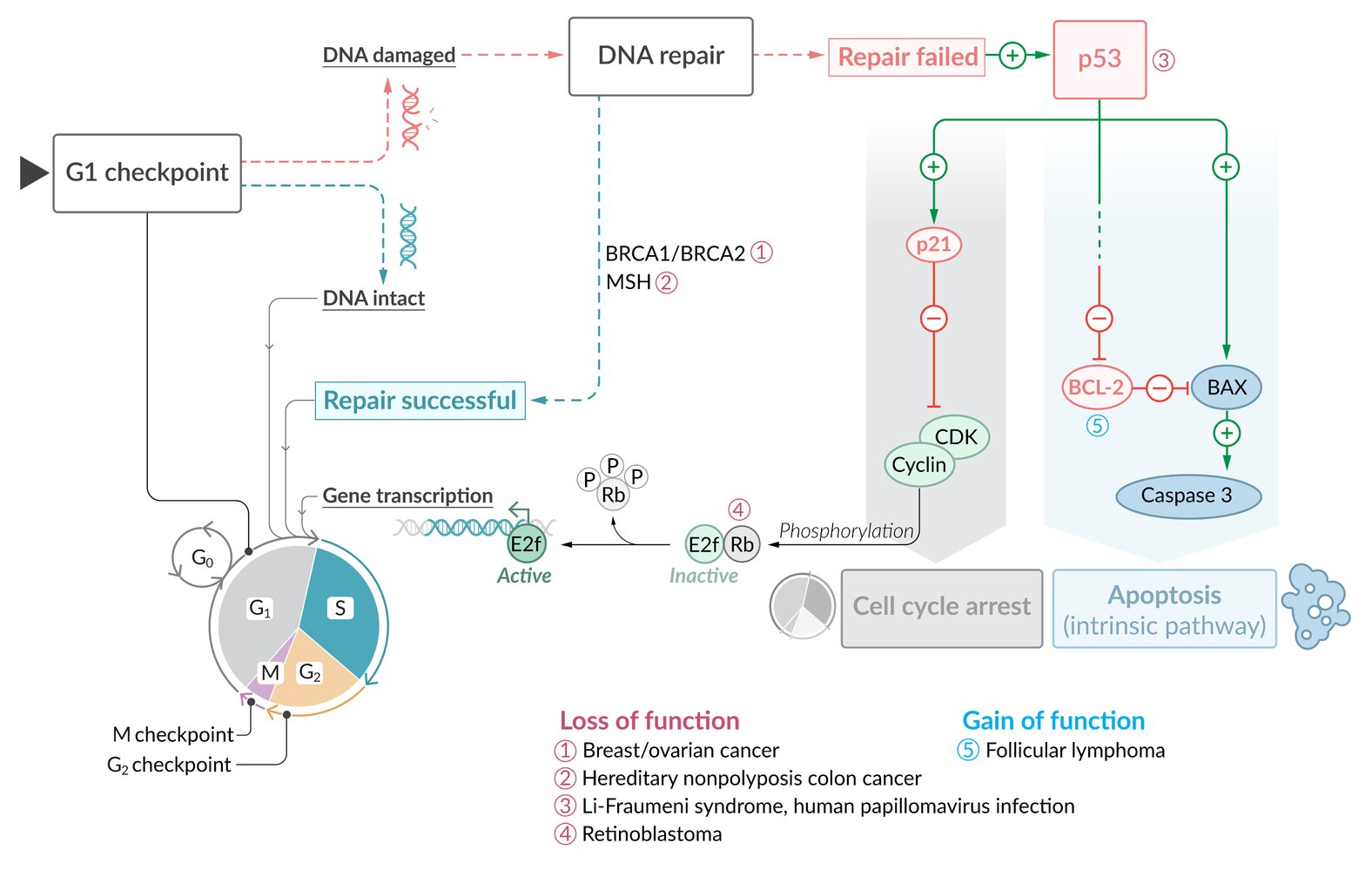
The hallmarks of cancer development and growth have been highlit in bold type, whereas the treatment options directed against the underlying mechanisms appear in plain type.
© AMBOSS
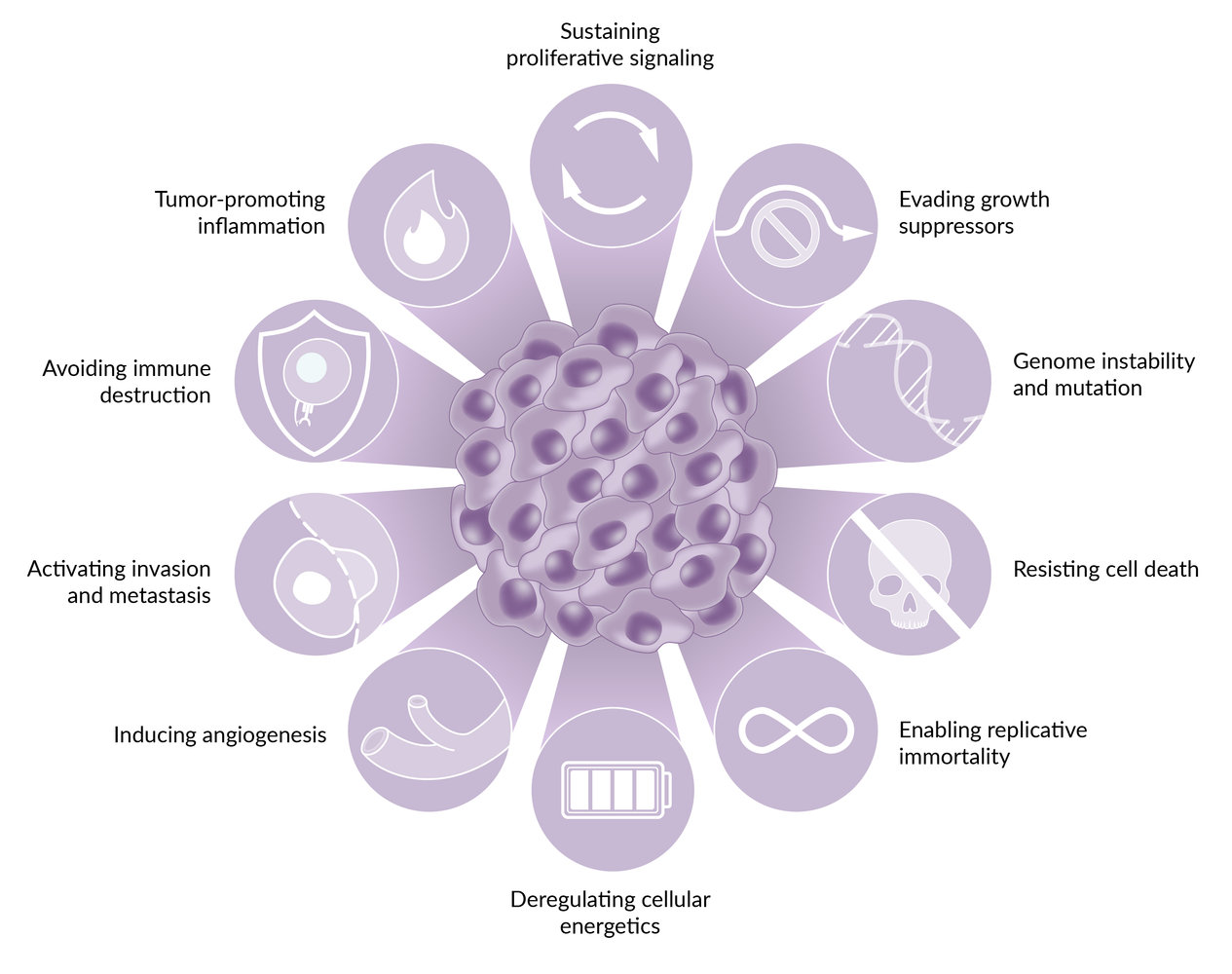
There are ten hallmarks of cancer acquired by cancer cells during human tumor development.
© AMBOSS
© AMBOSS

Karyogram and fluorescence in situ hybridisation (FISH) of a patient with chronic myeloid leukemia
In the karyogram (left image) and enlarged image (above right), the long arms of chromosome 9 and chromosome 22 are both of different size. This difference is caused by a translocation between both chromosomes, which resulted in an elongated chromosome 9 (9q+) and a shortened chromosome 22 (Philadelphia chromosome). The translocation can be also be detected using FISH (right image). A red probe is used to display the break on chromosome 9 (9q34) and a green probe to display the break on chromosome 22 (22q11). The red area reflects the intact chromosome 9; the pure green area the intact chromosome 22. The areas with a red-green signal signify the fusion of chromosome 9 and parts of chromosome 22.
Our great thanks to Dr. Wisplinghoff (Dr. Wisplinghoff's laboratory) for kindly providing this image.
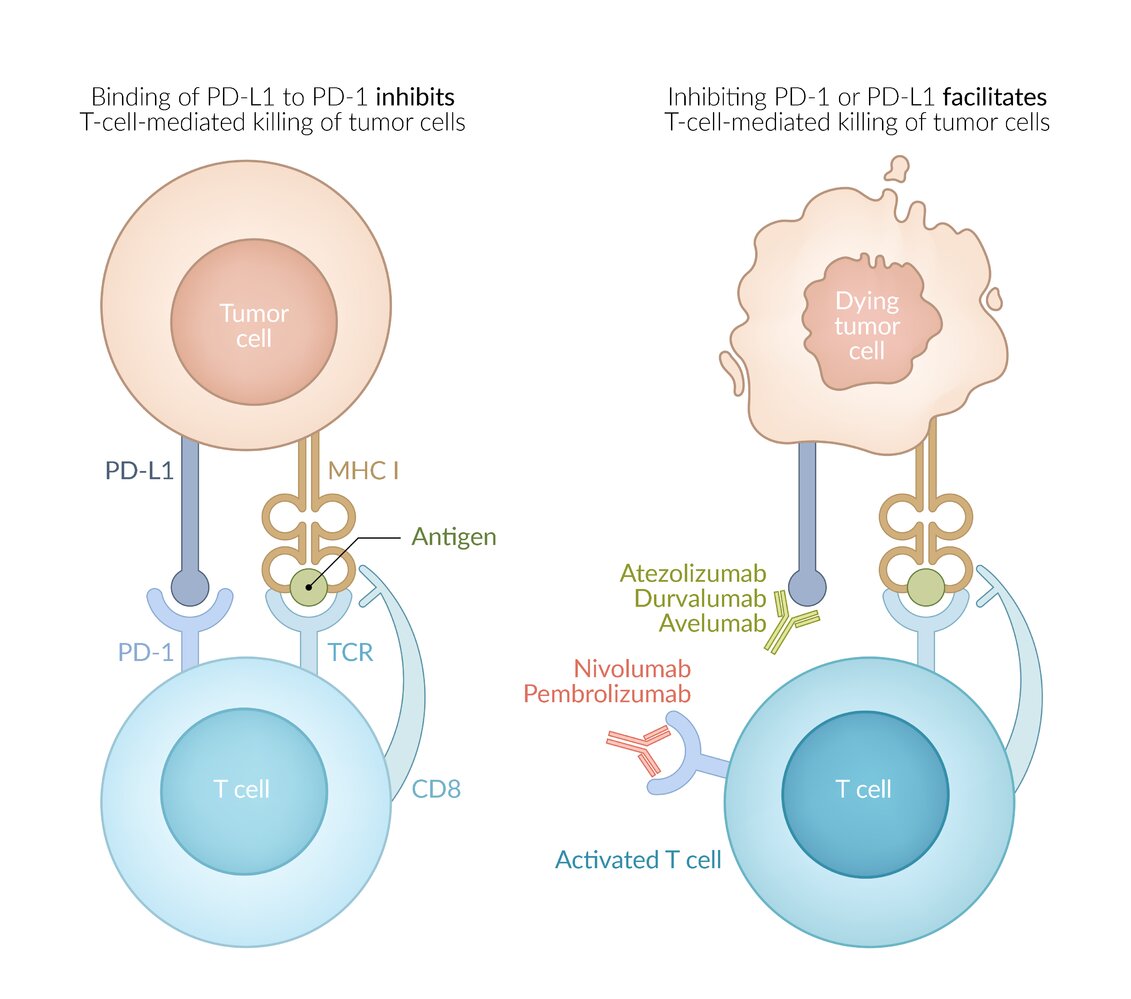
Anti-PD-1 antibodies remove negative signals and enhance the T cell-mediated killing of cancer cells.
© AMBOSS
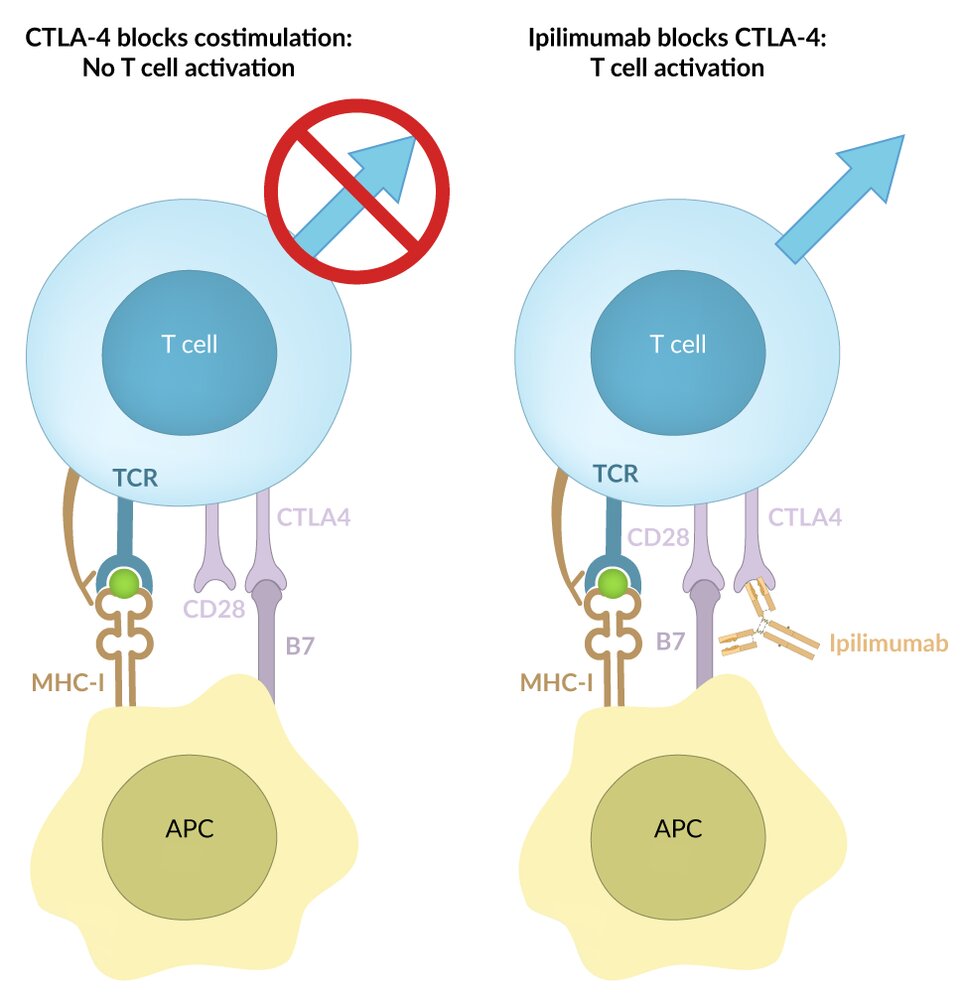
Anti-CTLA-4 antibodies block the molecule CTLA-4, thereby reducing negative signals that would otherwise prevent T-cell activation.
APC: antigen-presenting cell; MHC: major histocompatibility complex; TCR: T-cell receptor
© AMBOSS
Oncogene
-
Oncogene: the product of a gain-of-function mutation in a proto-oncogene which leads to overexpression of signaling proteins and growth factors, and thus, uncontrolled cellular proliferation (e.g., dysplasia, neoplasia)
- Only one allele of the proto-oncogene requires damage to form an oncogene.
- Often present in cancer cells
-
Proto-oncogene: Genes that encode proteins that are important in normal cell division and cell differentiation. Examples include:
- Protein kinases, e.g., protein kinase B (PKB)
- PKB activates and inhibits various substrates, regulates apoptosis, activates translation and, indirectly, cell division.
- PKB is activated by phosphatidylinositide 3-kinase (PI3K).
- Ligand-directed transcription factors (intracellular hormone receptors)
-
GTP-binding proteins
- G protein-coupled receptors
- Small G-proteins such as Ras
- Tyrosine kinase receptors
- Growth factors and cytokines
- Protein kinases, e.g., protein kinase B (PKB)
| Overview of proto-oncogenes [11] | |||
|---|---|---|---|
| Proto-oncogene | Chromosome | Gene product | Associated malignancies |
| BRAF |
|
|
|
| BCR-ABL |
|
|
|
| JAK2 |
|
|
|
| ERBB2 (HER2/neu) |
|
|
|
| ALK |
|
|
|
| RET |
|
|
|
| c-KIT |
|
|
|
| L-myc-1 (MYCL1) |
|
|
|
| N-myc (MYCN) |
|
|
|
| c-myc |
|
|
|
| KRAS |
|
|
|
| BCL-2 |
|
|
|
| CDK4 |
|
|
|
| CCND1 |
|
|
|
| ERBB1 |
|
|
|
“Adenocarcinoma of Lung Kinase”: Cancer (adenocarcinoma of lung) and the gene product (tyrosine kinase) are associated with ALK mutations.
L-myc is associated with lung cancer and n-myc with neuroblastoma.
c-KIT mutations affect CytoKIne recepTor production.
BCL-2 mutations are associated with diffuse large B-cell lymphoma.

© AMBOSS
Tumor suppressor genes
-
Tumor suppressor gene: a gene that normally controls and suppresses cell proliferation
- Loss of function or inactivation leads to an increased risk of developing cancer.
- Both alleles must be mutated in order for complete loss of function of the gene.
| Overview of tumor suppressor genes | |||
|---|---|---|---|
| Gene | Chromosome | Gene product | Associated malignancy |
| TP53 |
|
|
|
| Rb |
|
|
|
| CDKN2A |
|
|
|
| APC gene |
|
|
|
| PTEN [14] |
|
|
|
| BRCA1 |
|
|
|
| BRCA2 |
|
||
| MMR gene family |
|
|
|
| DCC (Deleted in colorectal cancer) |
|
|
|
| SMAD4 (DPC4) (Deleted in pancreatic cancer) |
|
|
|
| MEN 1 |
|
|
|
| NF1 |
|
|
|
| NF2 |
|
|
|
| TSC1 (Tuberous sclerosis complex 1) |
|
|
|
| TSC2 (Tuberous sclerosis complex 2) |
|
|
|
| VHL |
|
|
|
| WT1 (Wilms Tumor 1) |
|
|
|
| WT2 (Wilms Tumor 2) |
|
||
Mutations of the Rb (retinoblastoma) gene mutations cause Retinoblastomas and bone cancer (osteosarcoma).
PTEN mutation is associated with cancers of the Prostate, breasT, and ENdometrium.
Mutations in MEN 1 affect its gene product: MENin.

© AMBOSS
Carcinogens
Chemical carcinogens
| Examples of chemical carcinogens | ||
|---|---|---|
| Substance | Sources of exposure | Malignancy |
| Aflatoxin |
|
|
| Alkylating agents |
|
|
| Aromatic amines (β-naphthylamine, benzidine) |
|
|
| Arsenic |
|
|
| Asbestos |
|
|
| Benzene, benzol |
|
|
| Beryllium |
|
|
| Chromium |
|
|
| Cigarette smoke |
|
|
| Ethanol |
|
|
| Nickel |
|
|
| Nitrosamines |
|
|
| Radon |
|
|
| Silica |
|
|
| Vinyl chloride |
|
|
| Wood dust |
|
|
Radiation
| Overview of radiation | ||
|---|---|---|
| Type | Occurrence | Malignancy |
| Nonionizing radiation |
|
|
| Ionizing radiation |
|
|
Oncogenic infections
| Infective agent | Associated malignancies |
|---|---|
| DNA viruses | |
| EBV |
|
| HBV |
|
| HHV-8 |
|
| HPV 16 |
|
| HPV 18 | |
| RNA viruses | |
| HTLV-1 |
|
| HCV |
|
| Nonviral pathogens | |
| Schistosoma haematobium |
|
| Clonorchis sinensis (Chinese liver fluke) |
|
| H. pylori |
|
| Streptococcus bovis |
|
Cancer-Immunity cycle

© AMBOSS
Grading and staging
Tumor grading
- Definition: the process of classifying tumors based on their histological appearance (degree of cell differentiation)
-
Indicators of poor differentiation
- High-proliferation index
- Presence of nucleoli
- Giant cells with multiple nuclei
- Hyperchromasia and heterogeneous chromatin distribution
- Abnormal shape of cell or nucleus (nuclear atypia, enlarged nucleoli)
- Different cell polarity
- Different orientation of nuclei belonging to the same group of cells
- Increase in mitotic figures
- Anaplasia: loss of morphological features of malignant cells so that resemblance to normal cells of a particular tissue where tumor cell originated from is lost
Grading systems
-
AJCC grading system
- Most commonly used grading system for nonhematological malignancies
- Can be applied to a wide range of tumors
- Usually, higher-grade tumors are more aggressive than lower-grade tumors.
| Grading | Differentiation of malignant tissue |
|---|---|
| G1 | Well differentiated (low grade) |
| G2 | Moderately differentiated (intermediate grade) |
| G3 | Poorly differentiated (high grade) |
| G4 | Undifferentiated/anaplastic (high grade) |
| GX | Differentiation cannot be assessed. |
-
Cancer-specific grading systems
- Gleason score for prostate cancer
- Nottingham grading system for breast cancer


Tumor staging [20]
- Definition: a method of determining and classifying a tumor according to its spread throughout the body
- Prognosis: The stage of the tumor is typically more important than the grade in determining the prognosis.
Spread determines Stage, and Stage determines Survival more than grade.
TNM classification
-
T stage: size or direct extent of the primary tumor
- Tcis: carcinoma in situ (no basement membrane penetration and no infiltration of submucosa)
- T1–4 based on the size and/or extent of the primary tumor (T4 refers to the infiltration of neighboring organs)
-
N stage: involvement of regional lymph nodes
- N0: no lymph node involvement
- N1–3 based on type of tumor and lymph node involvement
-
M stage: presence of distant metastasis
- M0: no distant metastasis
- M1: present distant metastasis
- Mx: unknown if distant metastasis present or not
- By adding a "C" to any category, it is possible to express the certainty of the diagnosis:
- C1: routine procedure (clinical examination, x-ray)
- C2: special procedure (e.g. ERCP, CT)
- C3: based on biopsy, cytology or surgical exploration
- C4: based on surgery and additional histopathological workup
- C5: based on autopsy and histopathological workup
- By adding a prefix to TNM it is possible to indicate additional diagnostic or clinical information:
- cTNM: staging based on clinical criteria
- pTNM: histopathological staging
T, N, and M have independent prognostic values. N and M are typically the most important determinants of prognosis.

AJCC staging system
- Stage 0 (carcinoma-in-situ)
- Stage I–III: Tumor spread into nearby tissues.
- Stage IV: Tumor spread to distant parts of the body.
Cancer-specific staging systems
- Lugano staging system for lymphomas
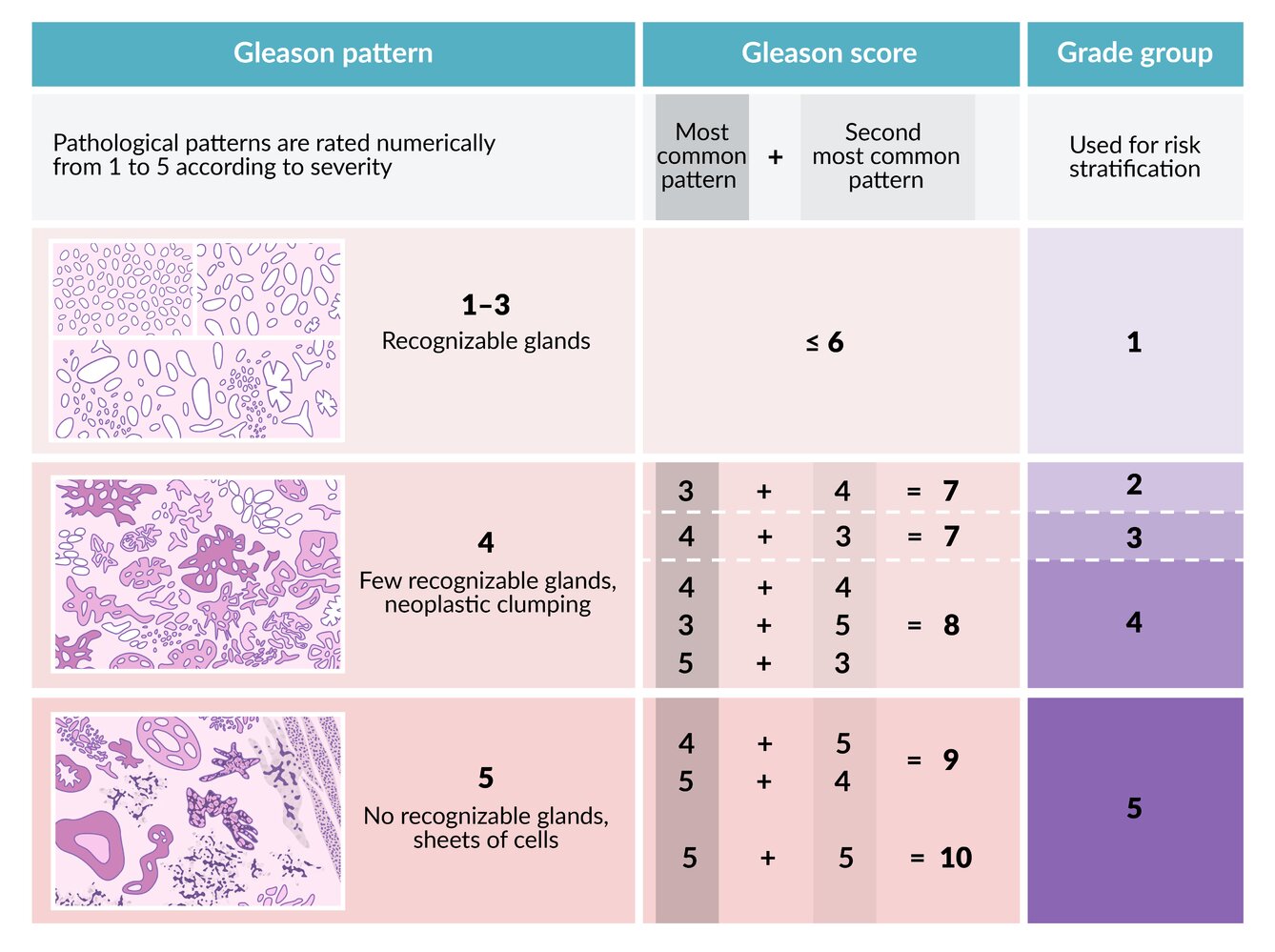
The pathological patterns of prostate CA in a biopsy sample are rated numerically according to severity. The scores of the most common and second most common patterns are added to obtain the Gleason score. This score is then used to determine the grade group, which is used for risk stratification.
© AMBOSS
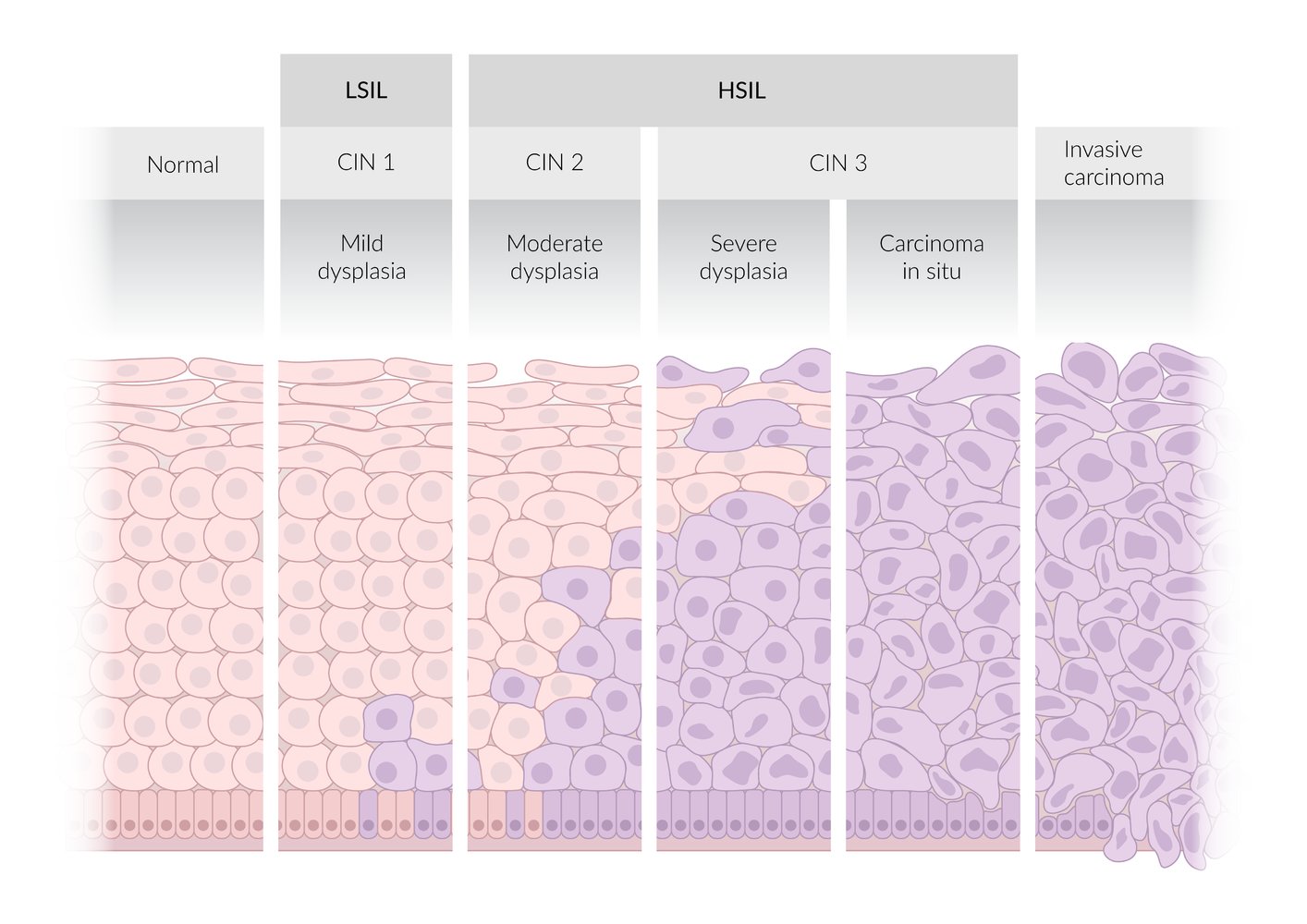
LSIL: low-grade squamous intraepithelial neoplasia
HSIL: high-grade squamous intraepithelial neoplasia
CIN: cervical intraepithelial neoplasia
© AMBOSS
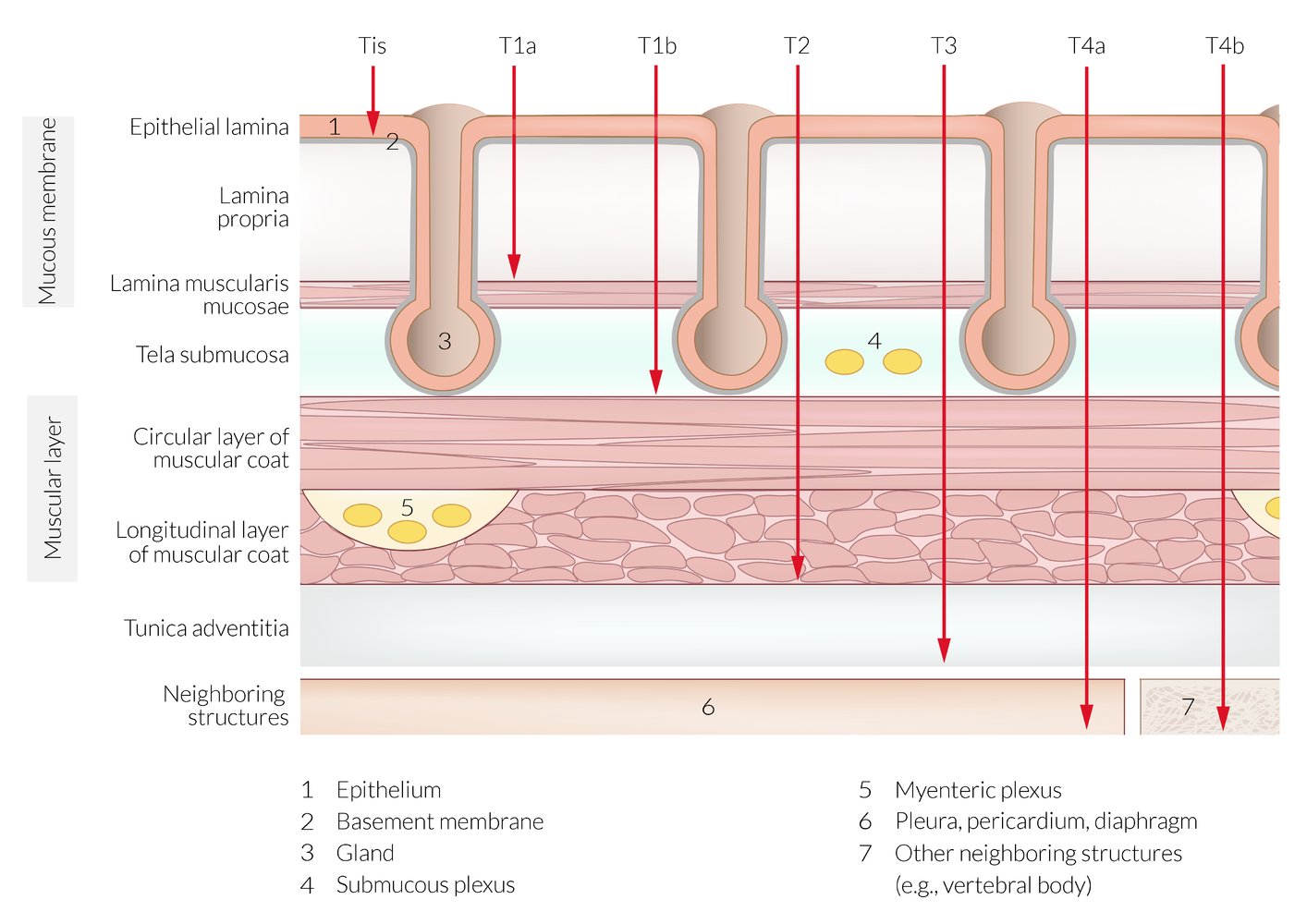
Cross-section of the esophageal wall showing the stages of infiltration by malignant tumors
© AMBOSS
Metastasis
Definition
- Metastasis: the spread of malignant cells to distant organs, tissues (e.g., colorectal cancer spreads to the liver)
Types of metastasis [21]
-
Lymphatic metastasis
- Dissemination of malignant cells via lymphatic vessels and lymph nodes
- Most common route of metastasis for most carcinomas
-
Hematogenous metastasis
- Dissemination of malignant cells via blood vessels
- Venous dissemination is more common than arterial dissemination because thin vein walls facilitate invasion.
- Most common route of metastasis for most sarcomas
- Seeding (oncology): spillage of malignant cells to neighboring structures → implants at a site adjacent to the primary tumor and subsequent growth (e.g., after a biopsy of cancer the cancer cells spill and implant along the biopsy canal)
- Transcoelomic metastasis: spread of malignant cells into body cavities by penetration of surfaces such as the pleura, pericardium, and peritoneum (e.g., ovarian cancer spread to the liver via the peritoneal cavity)
- Canalicular metastasis: spread of malignant cells via canalicular system (e.g. bile ducts, lactiferous ducts, urinary tract, and the subarachnoid space)
-
Cavitating pulmonary metastasis [22][23]
- Spread of malignant cells that form cavitary lesions in the lungs (e.g., gastrointestinal adenocarcinomas, renal cell carcinoma)
- Cavitary lesions are most commonly caused by squamous cell carcinoma (e.g., lung, head, and neck cancer)
- Cystic pulmonary metastasis: spread of malignant cells that form cystic lesions (contain a thin wall) in the lungs (e.g., colorectal cancer, soft tissue sarcomas, transitional cell carcinoma) [24][25]
“Four Carcinomas Route Hematogenously”: Follicular thyroid carcinoma, Choriocarcinoma, Renal cell carcinoma, and Hepatocellular carcinoma spread via the blood, compared to most carcinomas which spread lymphatically.


Mechanisms of metastasis
- Complex genetic changes are responsible for the selection of tumor subclones that are capable of metastasis.
- All metastases can be understood as arising from a two-part process: invasion of local extracellular tissue and dissemination and colonization.
-
Invasion of extracellular tissue: loss of adhesion to the basement membrane → invasion through basement membrane → passage through extracellular tissue
- Loss of E-cadherin expression is associated with tumor metastatic potential.
- Overproduction of proteases such as collagenase and matrix metalloproteinases degrade the basement membrane and interstitial matrix. Neoplastic cells encounter various chemotactic and angiogenic factors in the newly exposed extracellular matrix.
- Autocrine signaling via tumor-produced cytokines and paracrine signaling by cleaved matrix components and extracellular growth factors stimulate tumor cell locomotion towards vasculature or lymphatics.
-
Dissemination and colonization: encountering vascular or lymphatic routes → evasion of host defenses → implantation with distant tissue
- Host defenses destroy the majority of circulating cancer cells. Mechanisms to avoid this include tumor cell aggregation, formation of platelet-tumor complexes, and binding of active coagulation factors to form malignant emboli.
- Disruption of cellular adhesion molecules (laminins, cadherins) enables extravasation at distant tissues.
-
Invasion of extracellular tissue: loss of adhesion to the basement membrane → invasion through basement membrane → passage through extracellular tissue
Common sites for cancer metastasis [26]
- The target organ for metastasis is usually the first capillary bed encountered by the neoplastic cells during spread.
- Certain types of cancer have a tendency to spread to particular organs (organ tropism; e.g., prostate cancer to bone, lung cancer to adrenal glands)
| Common origins of cancer metastases | ||
|---|---|---|
| Organ with metastasis | Associated features | Primary tumor location |
| Liver |
|
|
| Bone |
|
|
| Brain |
|
|
| Lungs |
|
|
Approximately 50% of brain tumors and most bone tumors are not primary tumors but rather result from metastases.
“Cancers spread progressively to the liver”: Colon, Stomach, and Pancreas cancers metastasize to the liver.
“BLT with a kosher pickle and mayo on the bun”: Breast, Lung, Thyroid, Kidney, Prostate cancers, and Multiple myeloma metastasize to the bone.









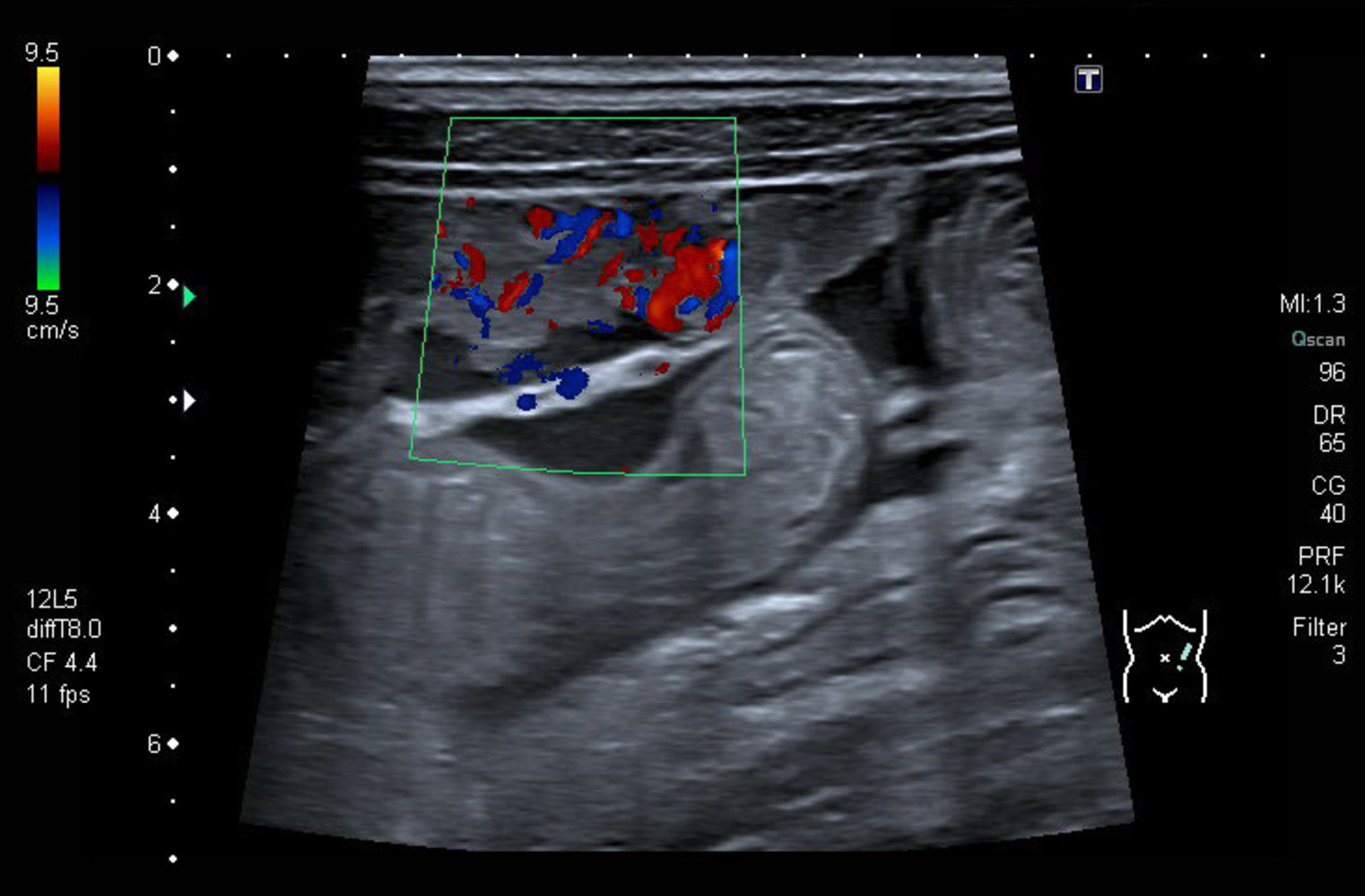
Abdominal ultrasound (longitudinal section)
A heteroechoic nodular mass is seen arising from the peritoneal surface of the anterior abdominal wall (green hatched overlay). The mass is well vascularized, as evident on color Doppler (red and blue areas within the green window).
Anechoic intraperitoneal free fluid, or ascites (light blue overlay), is seen between the mass and the adjacent intestinal loops (white outline).
These findings suggest peritoneal carcinomatosis.
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.

Intraoperative photograph of the small bowel of 48-year-old patient with ovarian cancer
Multiple white nodules of varying sizes are visible, predominantly on the mesentery and the segment of small bowel on the left side.
Source: “Tumor deposet” by haitham alfalah, Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}
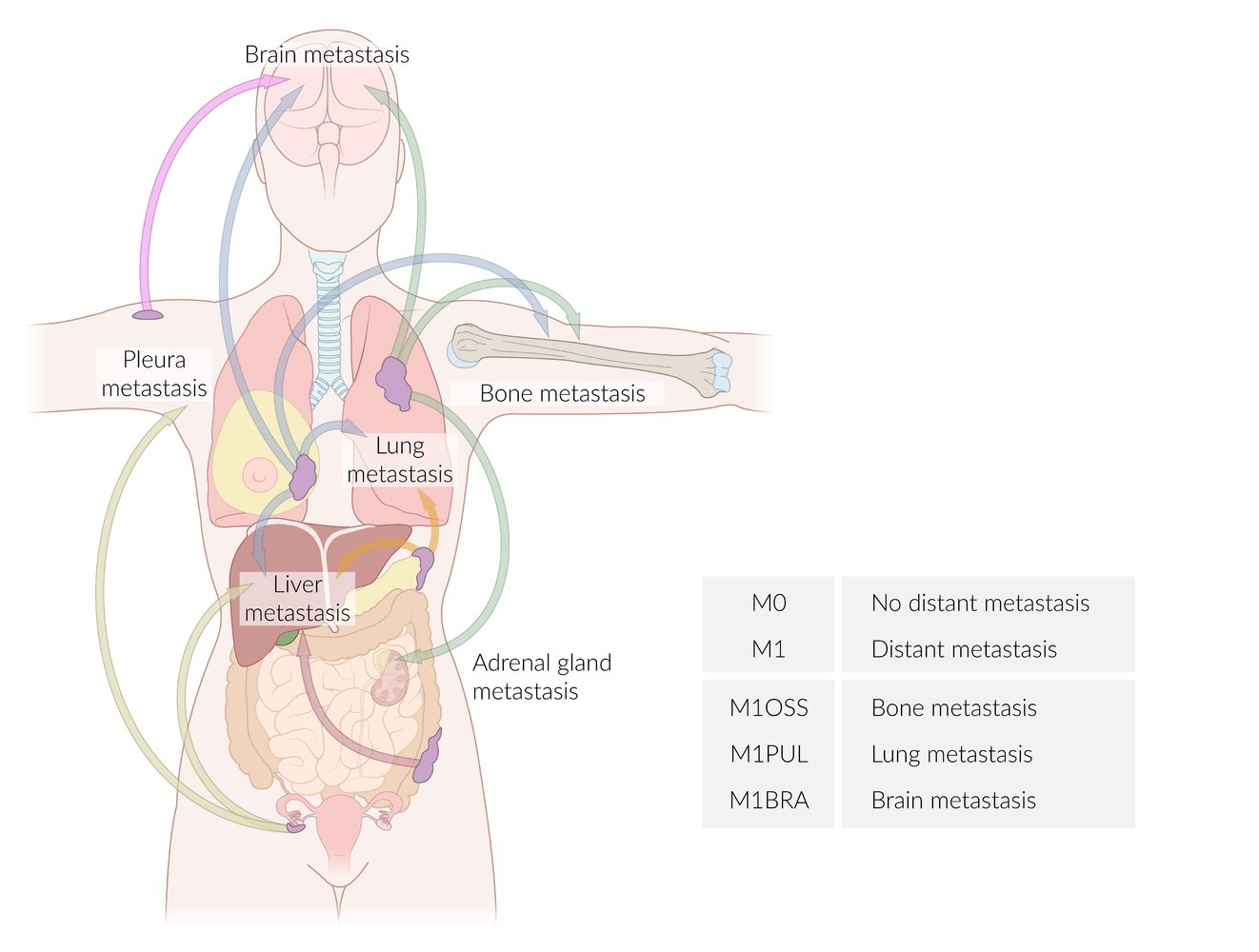
Arrows have been color-coded according to the site of the primary tumor:
Pink: skin cancer
Blue: breast cancer
Green: lung cancer
Orange: pancreatic cancer
Red: colon cancer
Lime: ovarian cancer
The table provides examples of suffixes used to specify the affected organs according to the TNM classification.
© AMBOSS

Ultrasound liver (oblique plane) of patient with pancreatic neuroendocrine tumor
Several rounded, hyperechoic lesions (green overlay) are seen in the right hepatic lobe.
Liver metastases from a pancreatic neuroendocrine tumor are usually circumscribed and round or oval in shape. They may appear hypoechoic, hyperechoic, or targetoid, and may contain cystic or necrotic areas.
Dashed line: diaphragm
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.

X-ray right shoulder (AP view; external rotation) of a patient with metastatic renal cell carcinoma
A fracture (dashed lines) traverses a lytic lesion (green overlay) involving the surgical neck of the humerus. The lesion margin is ill-defined (wide zone of transition) and cortical breakthrough is present.
Source: “Pathologische Fraktur des Humerus bei einer Metastase eines Nierenzellkarzinoms.” by Hellerhoff, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
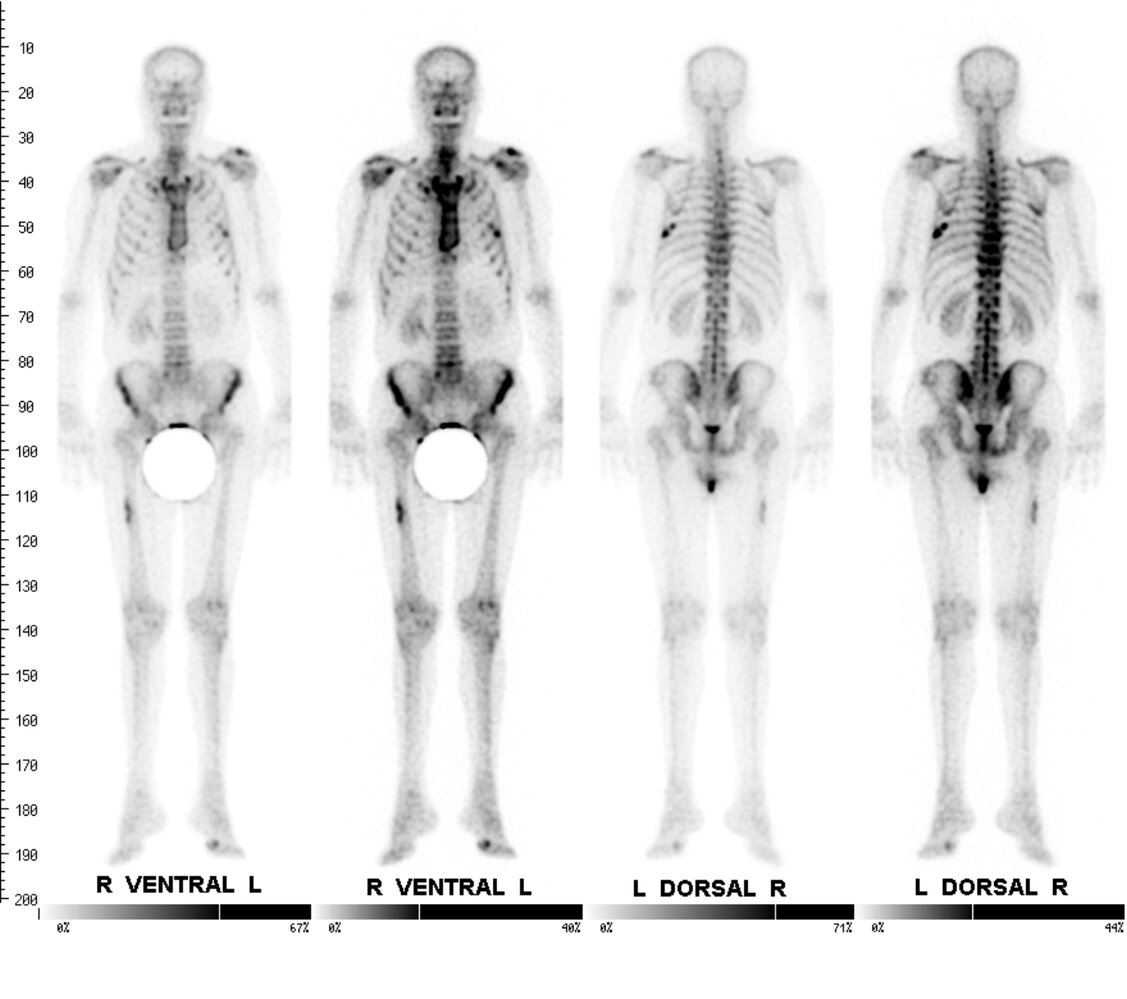
Bone scintigraphy in a 68-year-old patient with known lung carcinoma (tracer: technetium 99m, approximately 3 hours after injection)
Two images of the bony skeleton from a ventral view and two images from a dorsal view are shown (the second in each case with altered thresholds for contrast enhancement).
Zones of increased intensity can be seen in the right femur and one left rib (red arrowheads), which is a highly-suggestive of bone metastases.
Another zone of increased intensity is seen in the metatarsophalangeal joint of the left foot (blue arrowhead), which is most indicative of rhizarthrosis.
Our great thanks to PD Dr. M. Jergas (Center for Diagnostic and Interventional Radiology, St. Elizabeth Hospital, Cologne) for kindly providing this image.

X-ray femur (AP view) of a patient with bronchogenic carcinoma
A lytic cortical lesion (red overlay) involves the middle third of the femur.
Metastases can be lytic, sclerotic, or mixed-density lesions. Osteolytic lesions are the most common and are usually metastases from carcinomas of the kidney, lung, breast, gastrointestinal tract, or thyroid gland.
Our great thanks to PD Dr. M. Jergas (Center for Diagnostic and Interventional Radiology, St. Elizabeth Hospital, Cologne) for kindly providing this image.
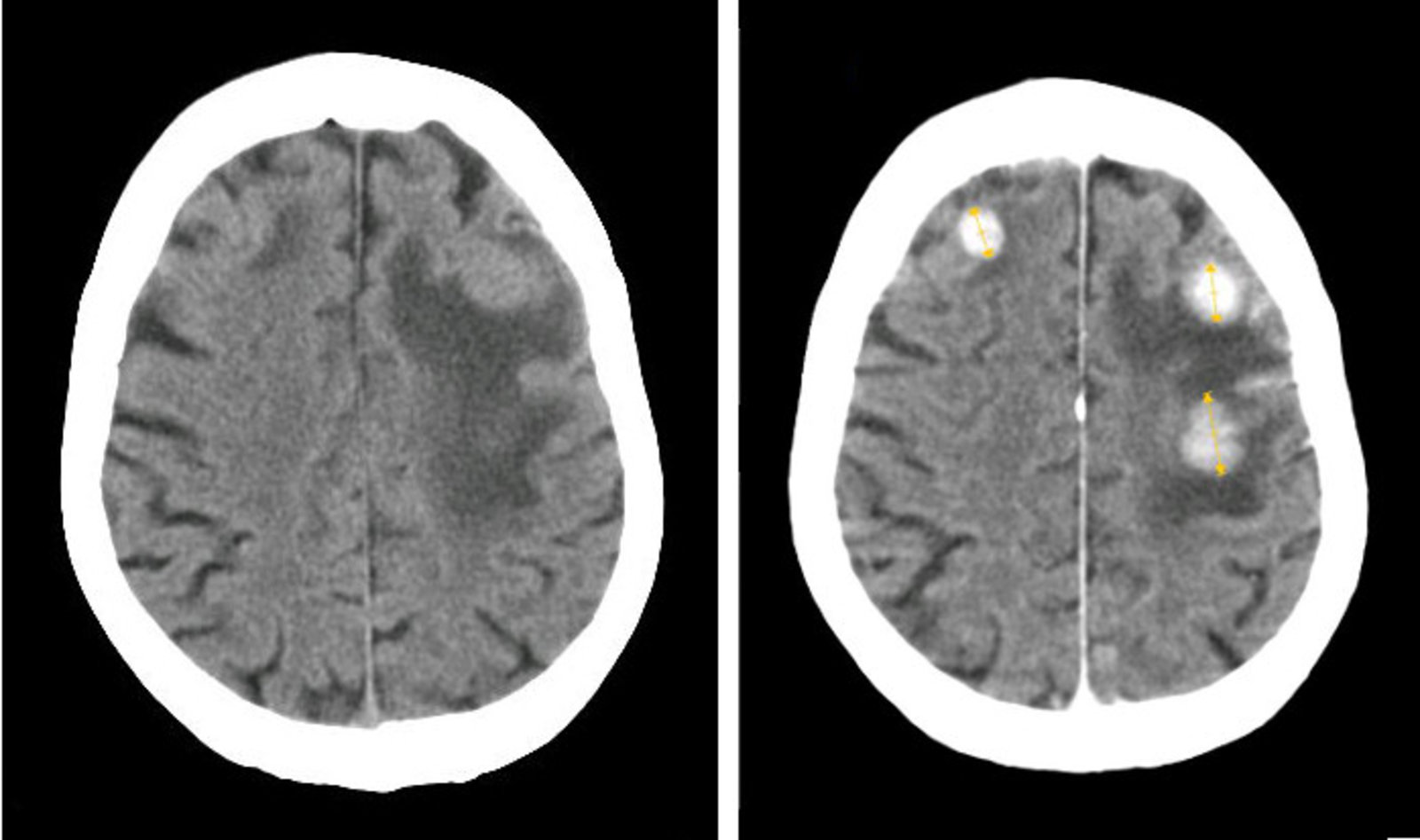
CT head (left: without contrast; right: with contrast; axial plane) of patient with breast cancer
Three intraparenchymal masses (left frontal lobe, right frontal lobe, and right parietal lobe) are accompanied by vasogenic edema (green overlay). The lesions (red overlay) are hyperdense and more conspicuous after IV contrast administration.
Source: “Brain Metastasis From Breast Cancer” by Jmarchn, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
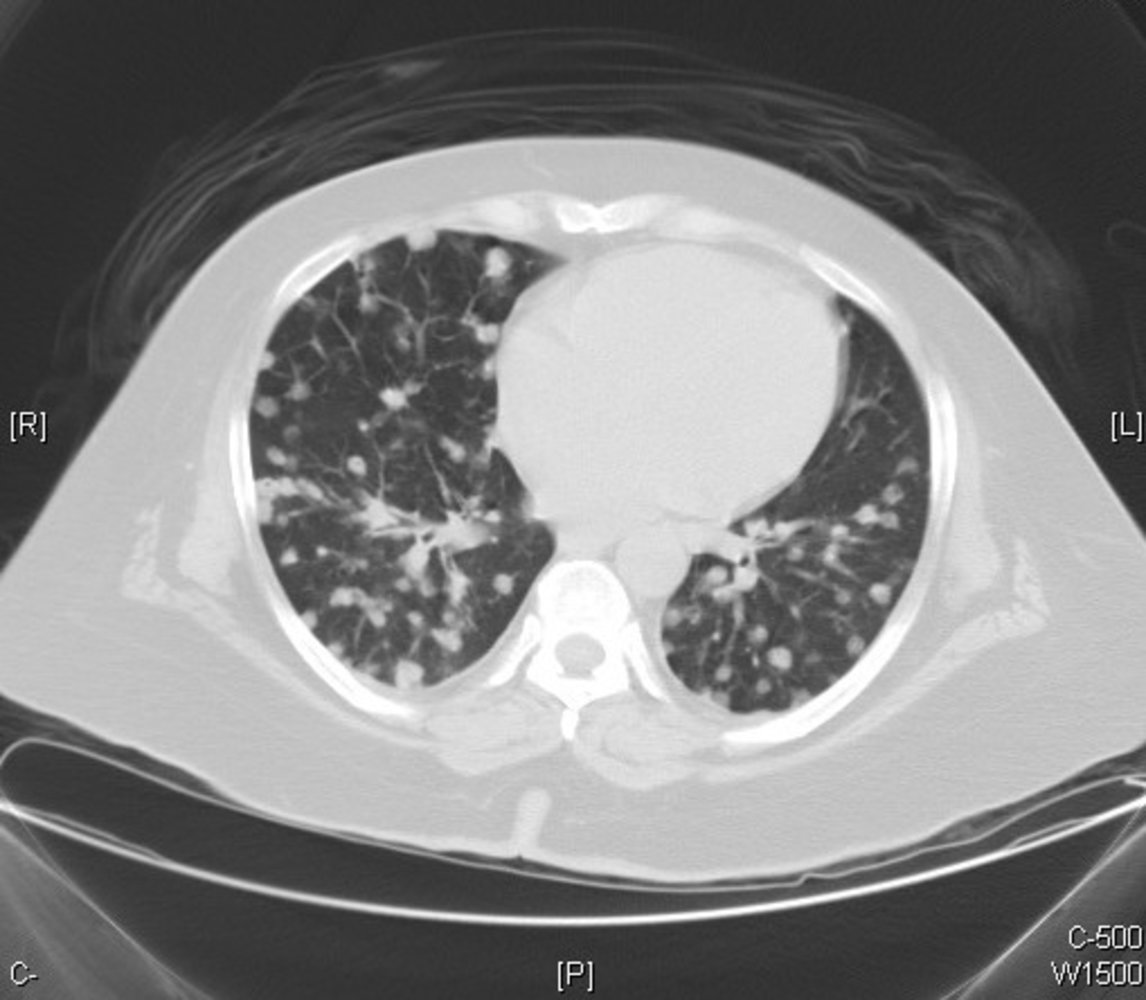
CT chest (axial plane; lung window) of a patient with lung metastases from colon carcinoma
Multiple small, circumscribed nodules of varying sizes (examples indicated by green overlays) can be seen in both lungs. A few nodules (examples indicated by red overlays) contain small foci of air, which may represent small bronchioles or sites of early cavitation.
Source: “Metastatic colonic adenocarcinoma - CT scan - Case 263” by Yale Rosen, Flickr, licensed under CC BY-SA 2.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 2.0.

X-ray chest (PA view) of a patient with lung metastases
Multiple pulmonary nodules with circumscribed margins can be seen in both lungs (examples indicated by green overlays). Differential diagnoses include malignant etiologies (metastatic disease, primary lung cancer, lymphoma) and benign etiologies (infection, embolism, autoimmune disease). An old healed fracture of the right clavicle (white arrow) is also visible.
Source: “The appearance of lung metastasis in patient that was reported” by Ghaemmaghami F, Zarchi MK, Early Onset of Metastatic Gestational Trophoblastic Disease after Full-Term Pregnancy, International Journal of Biomedical Science, licensed under CC BY 2.5. Modifications: removed yellow arrow. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
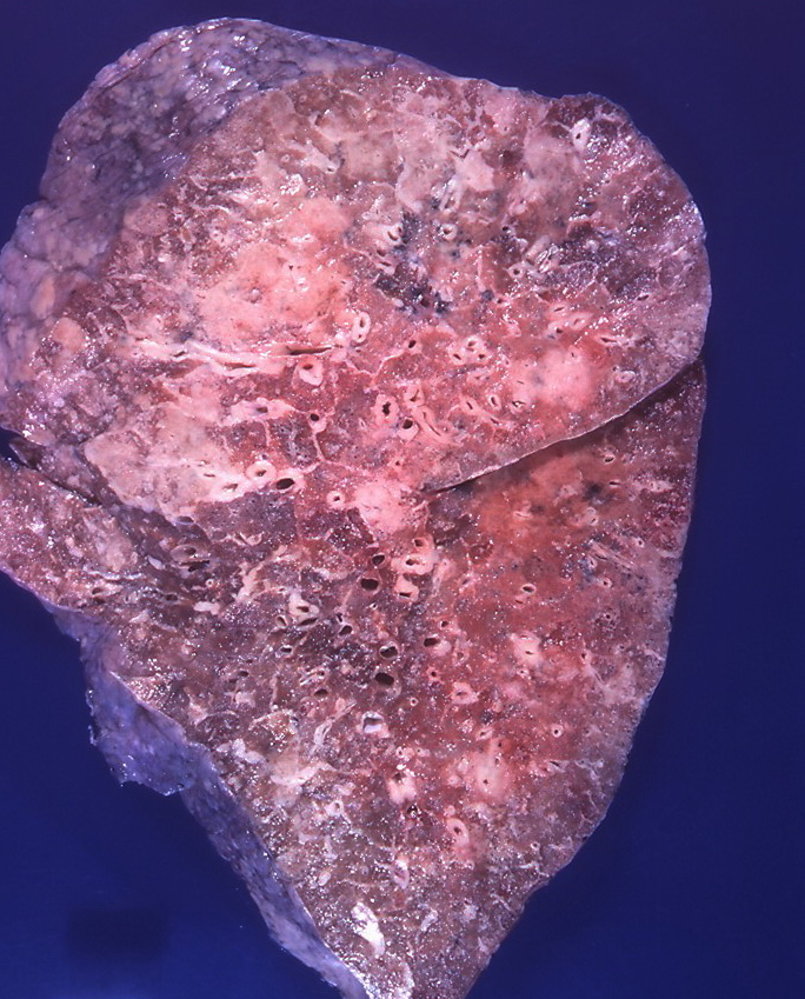
Photograph of a lung (longitudinal section) autopsied from a patient who died from metastatic prostate cancer
Multiple white nodules of varying sizes can be seen throughout the lung parenchyma, including the visceral surface.
Source: “Metastatic prostatic adenocarcinoma” by Yale Rosen, Flickr, licensed under CC BY-SA 2.0.
Tumor markers
Definition: Substances produced by cancer cells that are found in increased amount in the bloodstream, urine, or body tissues.
- The most commonly tested tumor markers include the following
- Alpha fetoprotein (AFP)
- β-HCG
- Carcinoembryonic antigen (CEA)
- Prostate-specific antigen (PSA)
- Calcitonin
- Alkaline phosphatase
- Placental alkaline phosphatase
- Lactate dehydrogenase
- Neuron specific enolase (NSE)
- CA 19–9
- CA 15–3
- CA 125
- Chromogranin A
- S-100 protein
- β2 microglobulin
- Thyroglobulin
- Monoclonal immunoglobulins
For more details for each tumor marker see the article on tumor markers.
Conditions associated with tumors
Neurocutaneous syndromes associated with neoplasms
| Overview of neurocutaneous syndromes associated with neoplasms | |||||
|---|---|---|---|---|---|
| Condition | Key features | Neoplasms | |||
| Neurofibromatosis type I |
|
|
|
||
| Neurofibromatosis type II |
|
|
|||
| Tuberous sclerosis |
|
|
|||
| von Hippel-Lindau syndrome |
|
|
|||
| Sturge-Weber syndrome |
|
|
|||
| Ataxia telangiectasia |
|
|
|||
Gastrointestinal conditions associated with neoplasms
| Overview of gastrointestinal conditions associated with neoplasms | |||||
|---|---|---|---|---|---|
| Condition | Key features | Neoplasms | |||
| Inflammatory bowel disease | Ulcerative colitis |
|
|
||
| Crohn disease |
|
||||
| Plummer-Vinson syndrome |
|
|
|||
| Barrett esophagus |
|
|
|||
| Atrophic gastritis | Autoimmune atrophic gastritis (AIG) |
|
|
|
|
| Environmental metaplastic atrophic gastritis (EMAG) |
|
|
|||
| Liver cirrhosis |
|
|
|||
Infectious conditions associated with neoplasms
| Overview of infectious conditions associated with neoplasms | |||||
|---|---|---|---|---|---|
| Condition | Key features | Neoplasms | |||
| DNA virus infections | EBV infection |
|
|
||
| HBV infection |
|
|
|||
| HHV-8 infection |
|
|
|||
| HPV 16 |
|
|
|||
| HPV 18 | |||||
| RNA virus infections | HTLV-1 infection |
|
|
||
| HIV infection |
|
||||
| HCV infection |
|
|
|||
| Nonviral pathogen infections | Schistosoma haematobium |
|
|
||
| Clonorchis sinensis (Chinese liver fluke) |
|
|
|||
| Streptococcus bovis |
|
|
|||
| Clostridium septicum |
|
||||
Miscellaneous conditions associated with neoplasms
| Miscellaneous conditions associated with neoplasms | |||||
|---|---|---|---|---|---|
| Condition | Key features | Neoplasms | |||
| Down syndrome |
|
|
|||
| Paget disease of the bone |
|
|
|||
Paraneoplastic conditions
| Overview of paraneoplastic conditions | |||||
|---|---|---|---|---|---|
| Condition | Key features | Neoplasms | |||
| Neuromuscular | Lambert-Eaton myasthenic syndrome |
|
|
||
| Myasthenia gravis |
|
|
|||
| Polymyositis |
|
|
|
||
| Dermatomyositis |
|
||||
| Neurological | Paraneoplastic encephalomyelitis |
|
|
|
|
| Paraneoplastic cerebellar degeneration |
|
|
|||
| Opsoclonus-myoclonus syndrome |
|
|
|||
| Endocrine | Cushing syndrome |
|
|
||
| Syndrome of inappropriate ADH secretion |
|
||||
| Hypercalcemia of malignancy |
|
|
|||
| Mucocutaneous | Malignant acanthosis nigricans |
|
|
||
| Necrolytic migratory erythema |
|
|
|||
| Paraneoplastic seborrheic keratosis (Leser-Trélat sign) |
|
|
|||
| Skeletal | Hypertrophic pulmonary osteoarthropathy (Bamberger-Marie syndrome) |
|
|
||
| Hematological | Polycythemia |
|
|
||
| Pure red cell aplasia |
|
|
|||
| Good syndrome |
|
||||
| Trousseau syndrome (thrombophlebitis migrans) |
|
|
|||
| Nonbacterial thrombotic endocarditis |
|
|
|||
| Miscellaneous | Neoplastic fever |
|
|
||
| Membranous glomerulonephritis |
|
|
|||

Multiple light brown macules with irregular borders (café-au-lait spots) are visible on the upper left arm, shoulder, and back.
This presence of multiple café-au-lait spots is highly suggestive of neurofibromatosis type 1.
Source: Courtesy of Dr. Gary M. White, MD
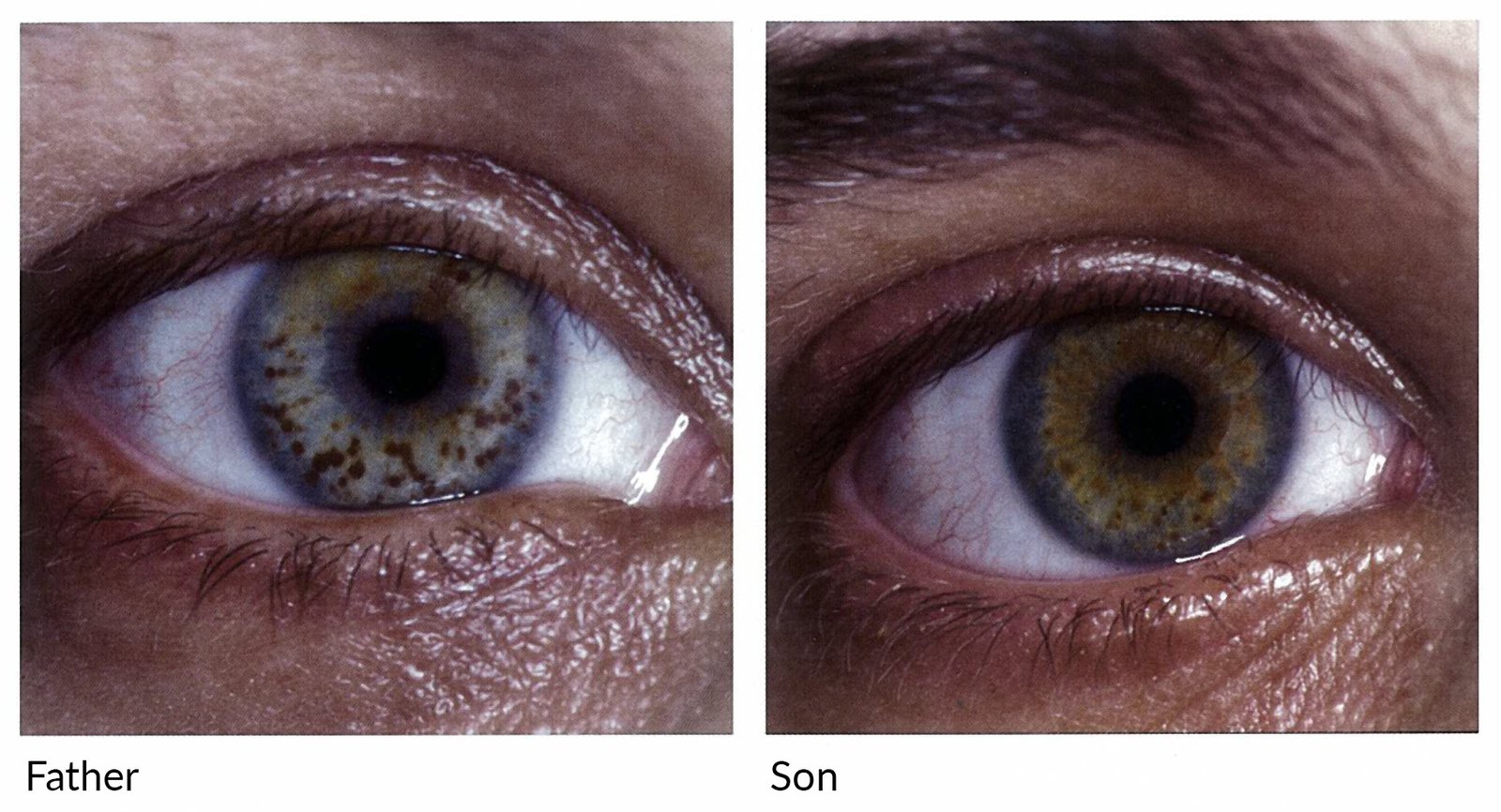
Right eyes of a father and son
Multiple brown-yellow, well-defined, and partly confluent papules (hamartomas) are visible on the iris.
These lesions are called Lisch nodules and can be seen in the vast majority of individuals with neurofibromatosis I.
Source: © IMPP

Multiple papules and nodules of varying sizes located on the upper back.
Numerous neurofibromas are pathognomonic of neurofibromatosis type 1 (von Recklinghausen disease).
Source: © IMPP
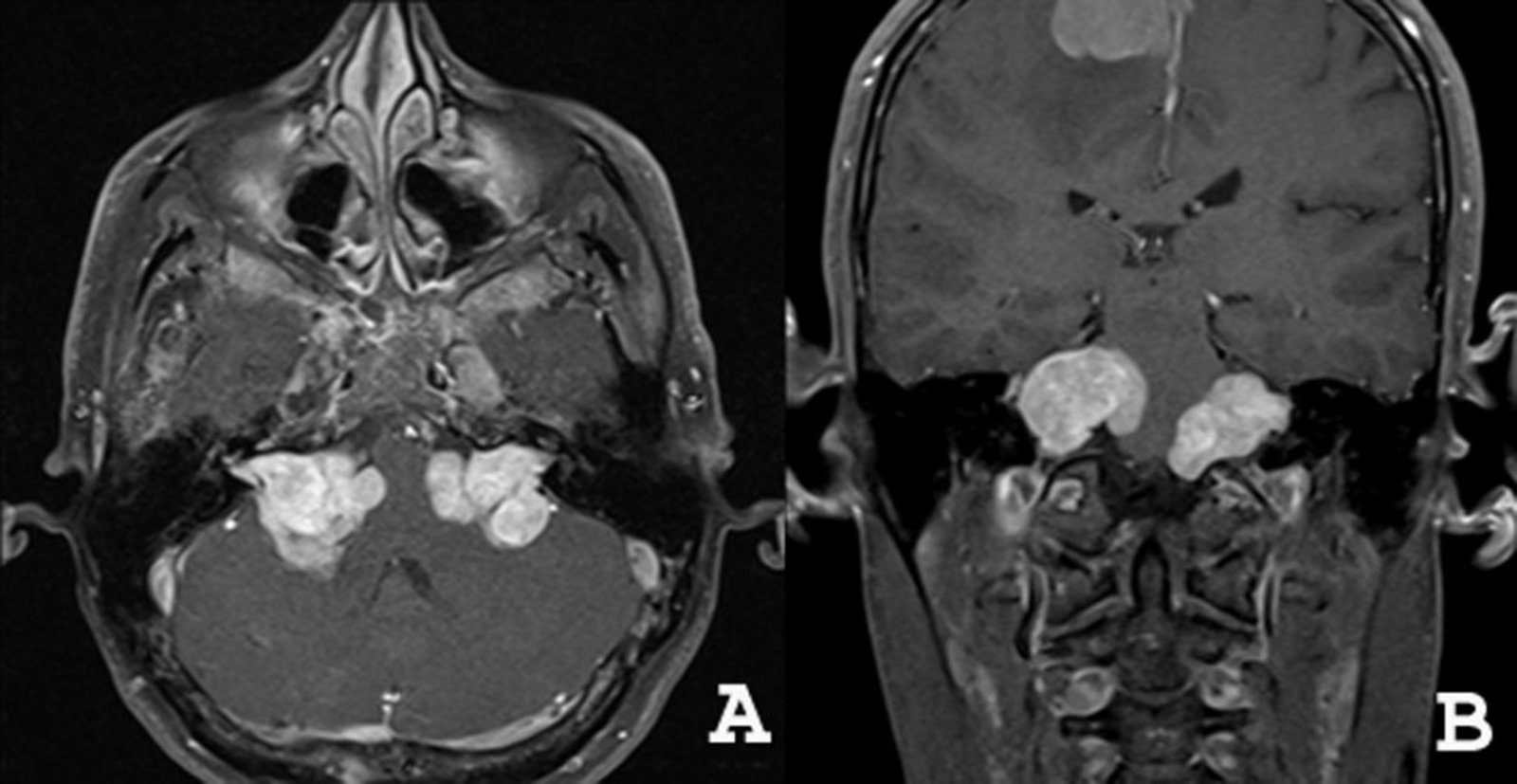
MRI head (T1-weighted; with contrast; A: axial plane; B: coronal plane) of a patient with neurofibromatosis type 2 (NF2)
The bilateral contrast-enhancing cerebellopontine angle masses (green overlay) represent vestibular schwannomas. The parasagittal location of the third intracranial mass (red overlay) suggests that it is a meningioma.
Bilateral vestibular schwannomas are the hallmark feature of NF2. Many patients also develop meningiomas and other tumors of the central nervous system.
Source: “Figure 1. in: Magnetic resonance findings of neurofibromatosis type 2: a case report” by Gabriela Spilberg et al., Cases Journal, licensed under CC BY 2.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).

Four ellipsoid, hypopigmented macules (ash-leaf spots) are located on the back of the patient (green overlay).
The presence of more than three ash-leaf spots is characteristic of tuberous sclerosis.
Source: Courtesy of Dr. Gary M. White, MD

Photograph of the back of a patient with tuberous sclerosis complex
A flesh-colored, irregularly shaped, slightly elevated patch can be seen on this patient's lumbosacral region. The fibrotic tissue gives it a bumpy appearance, which is often compared to that of orange peel.
Source: “Figure 1, in: Brain Proteomic Profiling in Intractable Epilepsy Caused by TSC1 Truncating Mutations: A Small Sample Study” by Liu Y-D, Ma M-Y, Hu X-B, Yan H, Zhang Y-K, Yang H-X, Feng J-H, Wang L, Zhang H, Zhang B, Li Q-B, Zhang J-C and Kong Q-X, frontiers in Neurology, licensed under CC BY 4.0. Modifications: image is cropped.

Multiple papules, resembling acne, can be seen on this patient's face.
These findings are suggestive of adenoma sebaceum, a cutaneous condition in patients with tuberous sclerosis characterized by the presence of angiofibromas.
Source: “A case of tuberous sclerosis showing facial angiofibromas in characteristic butterfly pattern.” by Herbert L. Fred, MD and Hendrik A. van Dijk, Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}
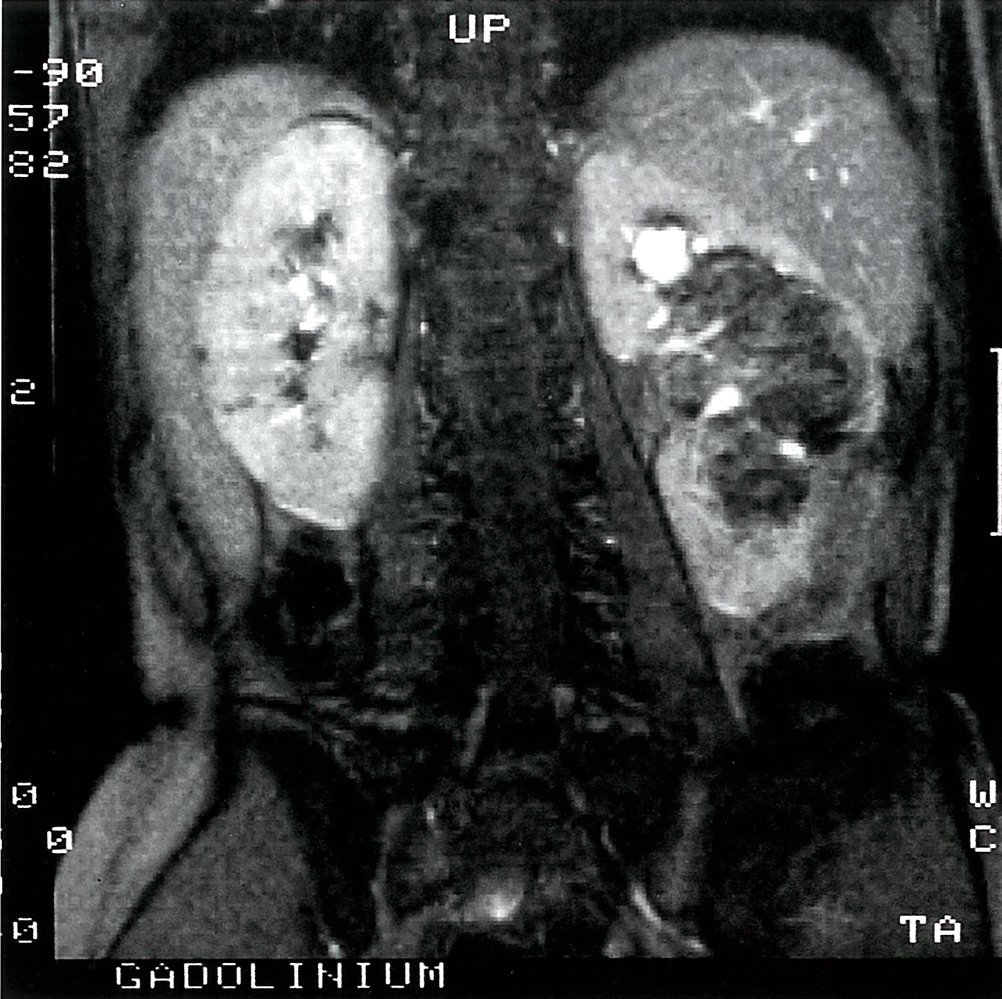
T2-weighted MRI of the abdomen with gadolinium-based contrast medium, frontal section: large angiomyolipoma of the left kidney (K) associated with tuberous sclerosis (L = liver, S = spleen)
Source: © IMPP
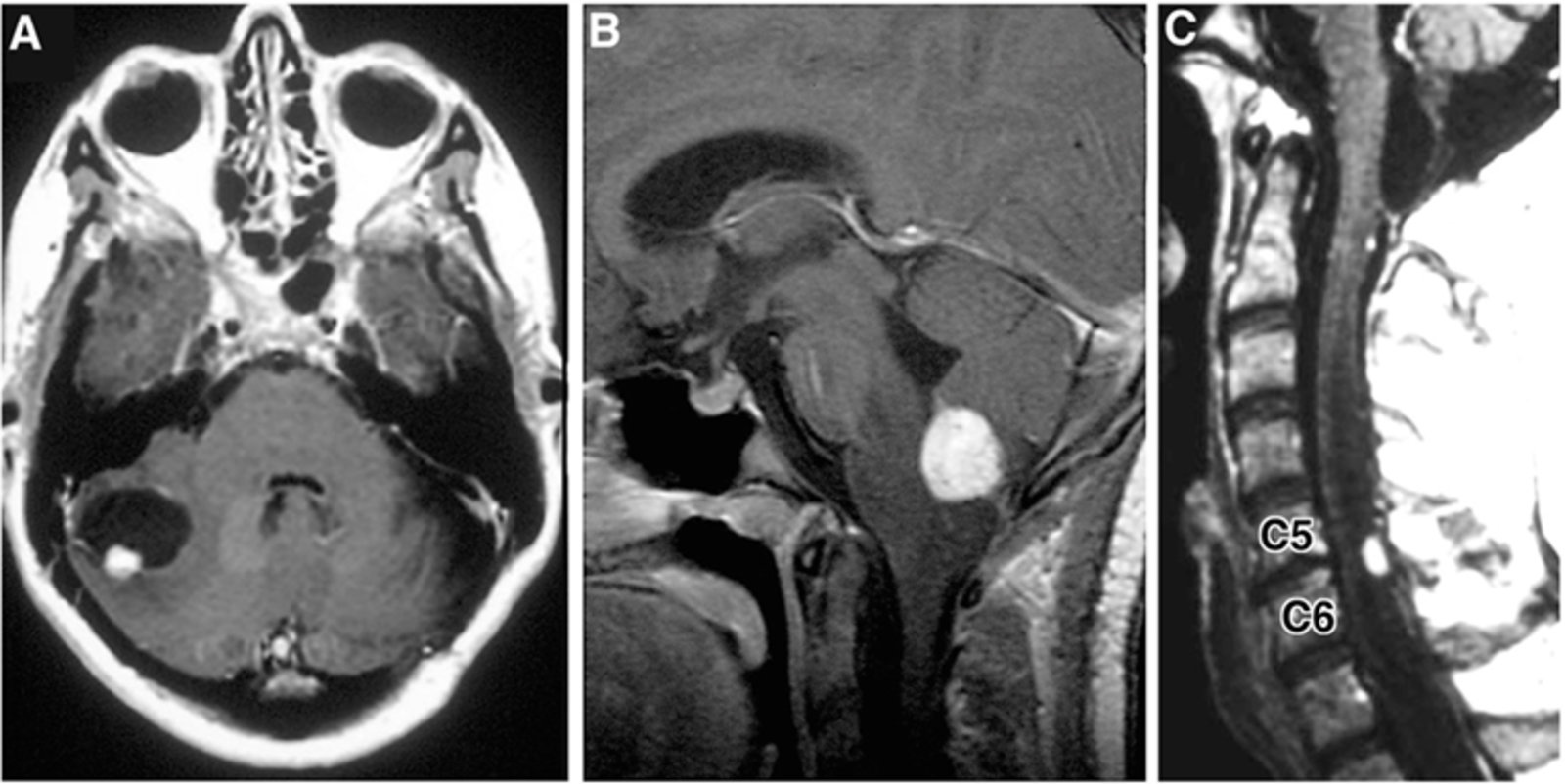
MRI images (contrast-enhanced; T1-weighted) of a patient with Von-Hippel-Lindau syndrome.
Image A (brain; axial view) shows a tumor within the lateral aspect of the right cerebellum. It consists of an enhancing solid component (red overlay) and a larger, hypointense part representing a cystic component (blue overlay).
Image B (brain; sagittal view) shows a contrast-enhancing tumor (green overlay) between medulla oblongata and cerebellum, within the region of the foramen of Magendie/median aperture.
Image C (spine MRI; sagittal view) shows a hyperintense tumor (yellow overlay) within the dorsal/posterior spinal canal at the level of vertebra C5-C6.
Von-Hippel-Lindau syndrome is a hereditary disorder characterised by the development of tumors in multiple parts of the body. This includes hemangioblastomas of the central nervous system, such as in this example. Hemangioblastomas are highly vascular tumours, resulting in the intense enhancement demonstrated on these post contrast images. Peritumoural cysts are common in these tumors, and result from plasma ultrainfiltrate passing through the permeable tumor blood vessels.
Source: “Figure 3. in: Personalized Medicine for Nervous System Manifestations of von Hippel–Lindau Disease” by Victoria Schunemann, Kristin Huntoon, Russell R. Lonser, Frontiers in Surgery Journal, Neurosurgery, licensed under CC BY 4.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
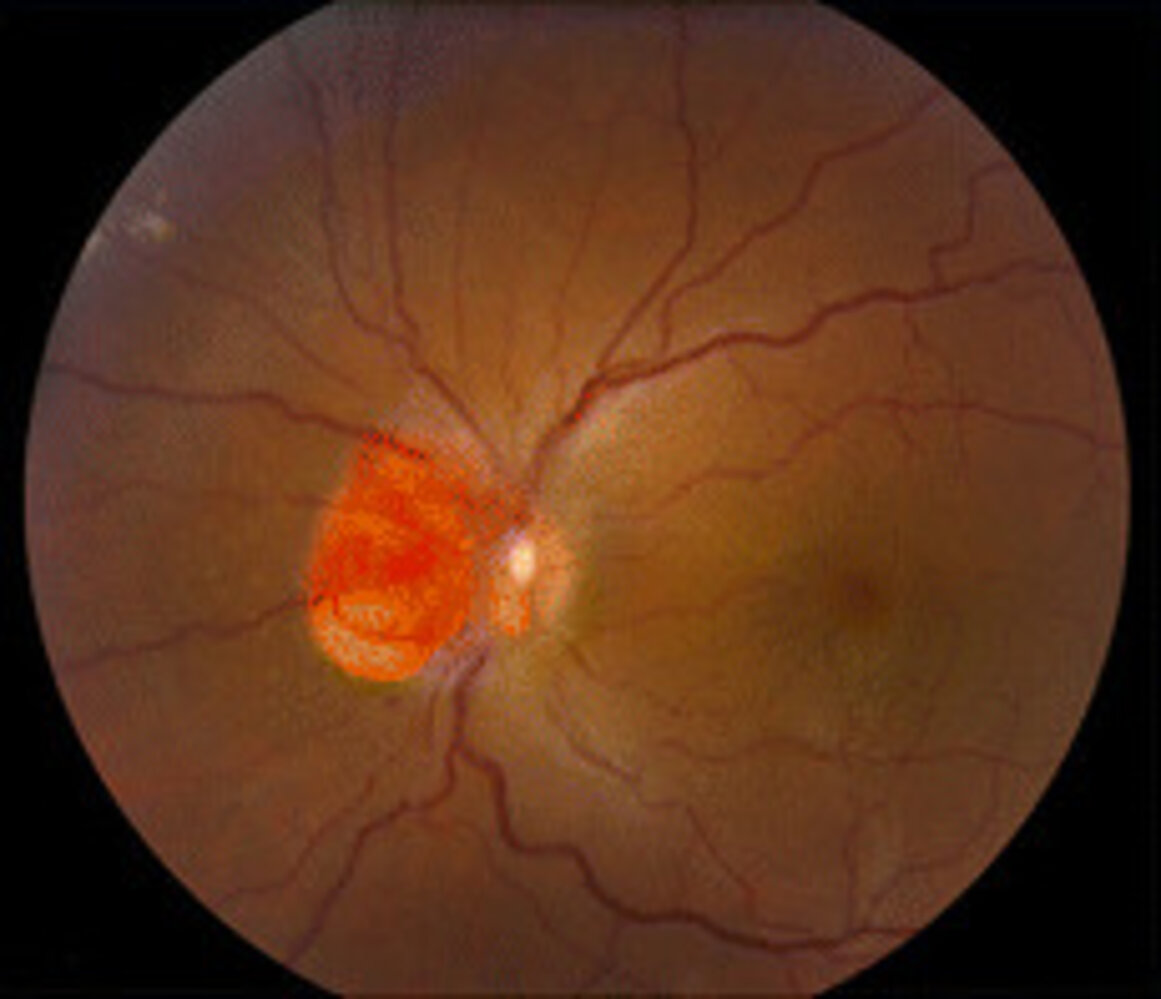
Fundus photography of a left eye
Adjacent nasally to the optic disc, a sharply demarcated orange lesion is visible.
This is the typical appearance of a retinal hemangioblastoma. Approx. 50% of patients with a solitary lesion will have von Hippel-Lindau disease. The vast majority of patients with multiple lesions will have von Hippel-Lindau disease.
Source: “Figure 1B. in: Pathology characteristics of ocular von Hippel-Lindau disease with neovascularization of the iris and cornea: a case report” by Shida Chen, Emily Y Chew & Chi-Chao Chan, Journal of Medical Case Reports, BioMed Central, licensed under CC BY 4.0. Modifications: image cropped & removal of the letter B.

A sharply demarcated, irregularly configured, erythematous area with a smooth surface on the left side of this 2-month-old infant's face is visible.
Image source of original image: www.paediatrie-in-bildern.de. Created by: Dr. Thomas Rautenstrauch. Modifications to original image: anonymized.
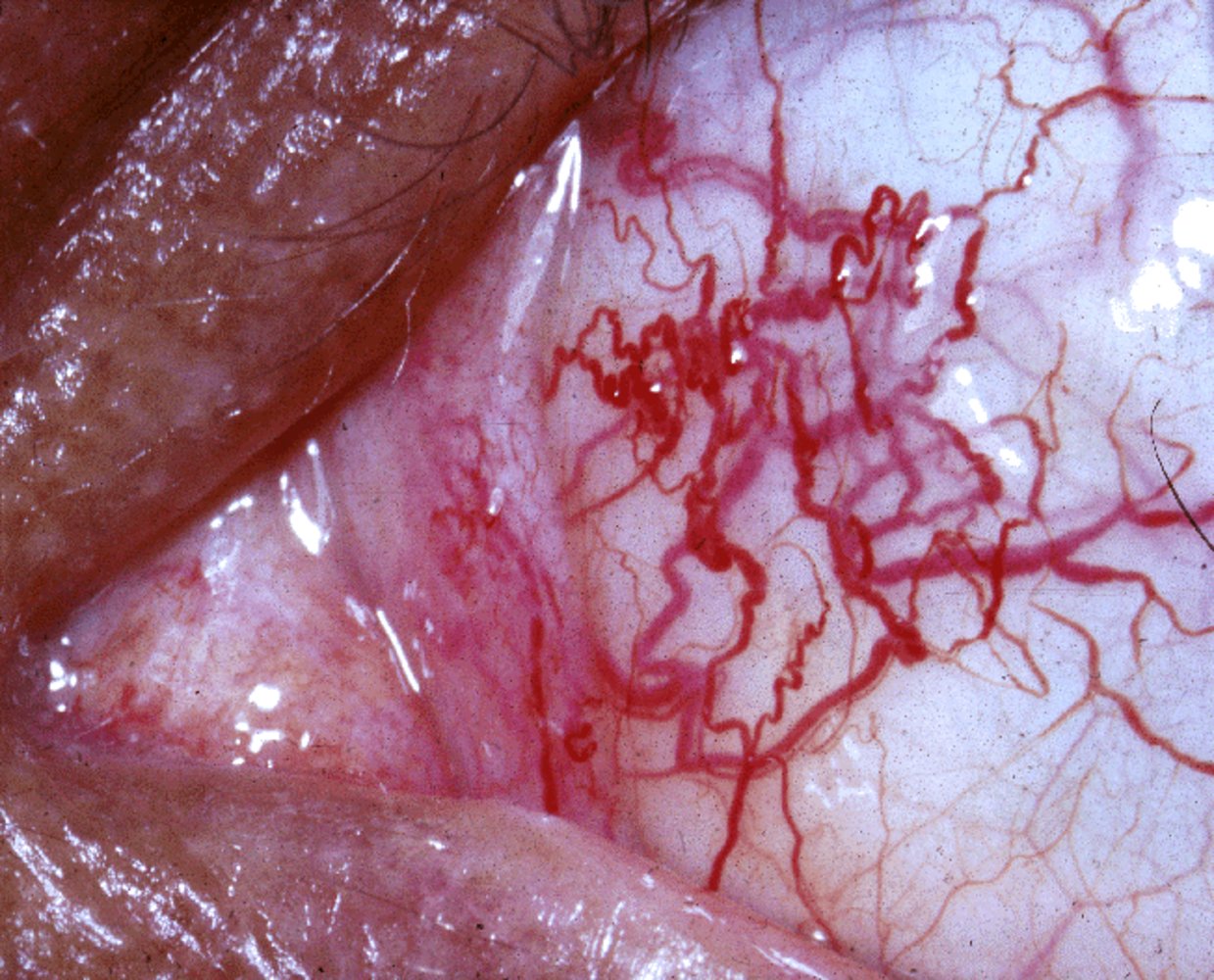
Medial angle of the left eye showing severely dilated blood vessels on the conjunctiva (conjunctival telangiectasia).
Conjunctival telangiectasias are a clinical finding of ataxia telangiectasia (Louis-Bar syndrome), a rare neurocutaneous syndrome
Source: "Ataxia-telangiectasia", National Eye Institute, Wikimedia Commons licensed under Public Domain
{kind=link}
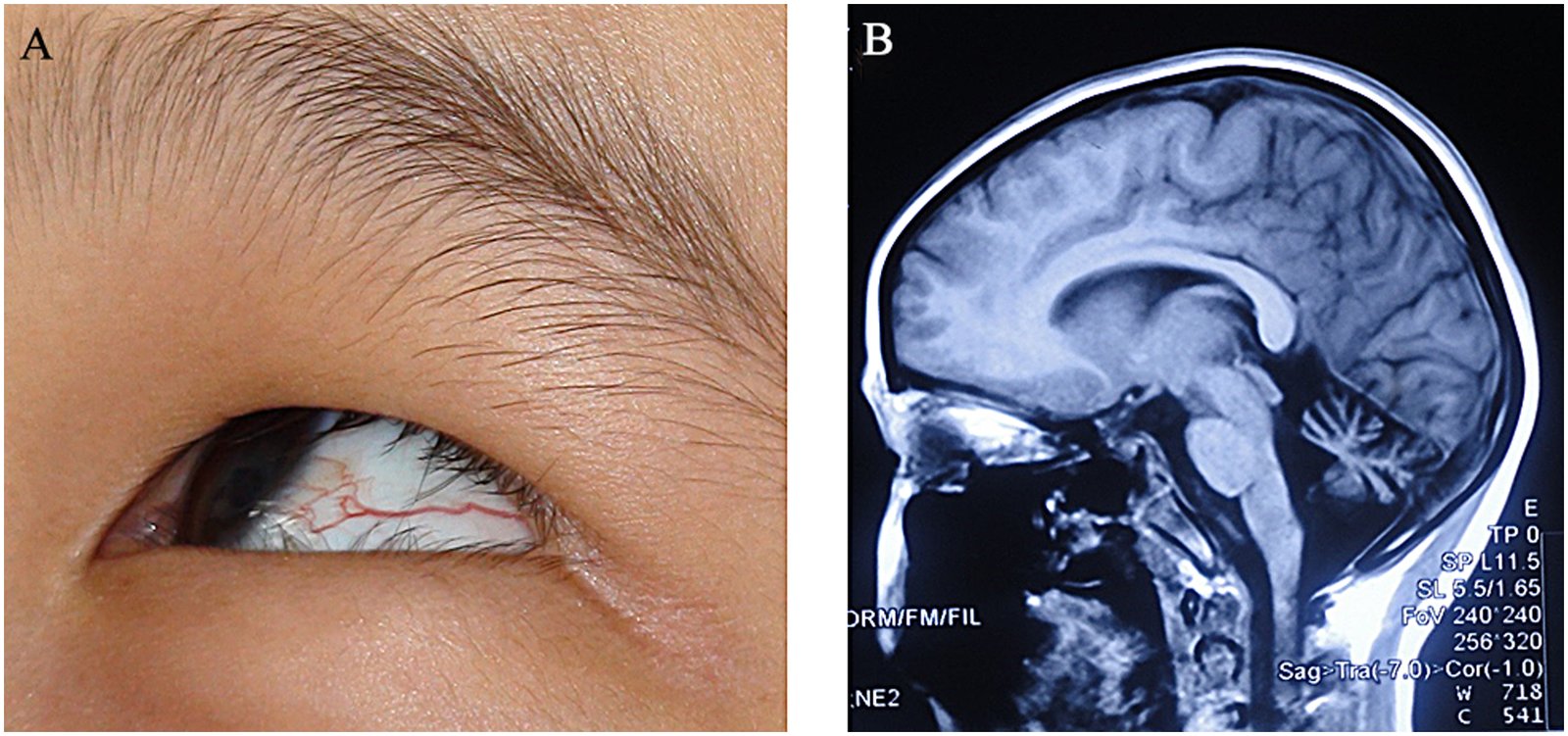
Image A: Close-up photograph of the left eye while the patient is looking to the right-top
A significantly dilated vessel of the conjunctiva can be seen (apart from that, the prominent epicanthic fold suggests an asian background of the patient).
Image B: Cranial MRI (T1w, sagittal view)
A remarkable atrophy of the cerebellum can be noted, leading to secondary enlargement of the cerebrospinal fluid system.
When put together, both findings are characteristics of neurocutaneous syndrome ataxia telangiectasia (Louis-Bar syndrome).
Source: “Figure 1: The clinical features of an AT patient” by Zhao Chen, Wei Ye, Zhe Long et al., Plos One, licensed under CC BY 4.0.
References
- "Cell Signaling in Cancer". https://www.technologynetworks.com/cancer-research/articles/cell-signaling-in-cancer-313171. [2018-12-17]
- Bhagwat AS, Vakoc CR. "Targeting Transcription Factors in Cancer". Trends in Cancer. 1(1). :53-65. (2015)
- Mendonsa AM, Na T-Y, Gumbiner BM. "E-cadherin in contact inhibition and cancer". Oncogene. 37(35). :4769-4780. (2018)
- Liberti MV, Locasale JW. "The Warburg Effect: How Does it Benefit Cancer Cells?". Trends Biochem Sci. 41(3). :211-218. (2016)
- Rabinovich GA, Gabrilovich D, Sotomayor EM. "Immunosuppressive Strategies that are Mediated by Tumor Cells". Annu Rev Immunol. 25(1). :267-296. (2007)
- Buchbinder EI, Desai A. "CTLA-4 and PD-1 Pathways: Similarities, Differences, and Implications of Their Inhibition.". Am J Clin Oncol. 39(1). :98-106. (2016)
- Flynn SD, Murren JR, Kirby WM, et al. "P-glycoprotein expression and multidrug resistance in adrenocortical carcinoma.". Surgery. 112(6). :981-6. (1992)
- Lochhead P, Chan AT, Nishihara R, et al. "Etiologic field effect: reappraisal of the field effect concept in cancer predisposition and progression". Modern Pathology. 28(1). :14-29. (2015)
- Cooper R, Harrison A. "The uses and adverse effects of beryllium on health". Indian Journal of Occupational and Environmental Medicine. 13(2). :65. (2009)
- "Beryllium Toxicity". https://www.atsdr.cdc.gov/csem/csem.asp?csem=5&po=6
- Hecht SS, Hoffmann D. "Tobacco-specific nitrosamines, an important group of carcinogens in tobacco and tobacco smoke". Carcinogenesis. 9(6). :875-884. (1988)
- "What Causes Lung Cancer". https://www.lung.org/lung-health-and-diseases/lung-disease-lookup/lung-cancer/learn-about-lung-cancer/what-is-lung-cancer/what-causes-lung-cancer.html. [2017-11-24]
- Deslauriers JR, Redlich CA. "Silica Exposure, Silicosis, and the New Occupational Safety and Health Administration Silica Standard. What Pulmonologists Need to Know.". Annals of the American Thoracic Society. 15(12). :1391-1392. (2018)
- Cowherd SM. "Tumor Staging and Grading: A Primer". Humana Press. :1-18. (2011). ISBN: 9781603272155
- Kumar V, Abbas AK, Aster JC. "Robbins & Cotran Pathologic Basis of Disease". Elsevier Saunders. (2014). ISBN: 9781455726134
- Yu X, Wang P, Liang Z. "Cavitary Pulmonary Metastases: CT Features and Their Correlation with the Pathology of the Primary Malignancy". The Chinese-German Journal of Clinical Oncology. 3(1). (2004)
- Gunasekaran K, Baskaran B, Rahi MS, Rudolph D, Parekh J. "Cavitating pulmonary metastases from a renal cell carcinoma". Clinics and Practice. 10(1). (2020)
- Sagar D, Adeni A. "Unusual cystic lung metastasis". BMJ Case Reports. :bcr-2018-224648. (2018)
- Fielli M, Avila F, Saino A, Seimah D, Fernández Casares M. "Diffuse cystic lung disease due to pulmonary metastasis of colorectal carcinoma". Respiratory Medicine Case Reports. 17. :83-85. (2016)
- Obenauf AC, Massagué J. "Surviving at a Distance: Organ-Specific Metastasis". Trends in Cancer. 1(1). :76-91. (2015)
- Lodish HF, Zipursky HF, Matsudaria HF, et al. "Molecular Cell Biology". Scientific American Library. (2000). ISBN: 0716731363
- Assi T, Kattan J, Rassy E, et al. "Targeting CDK4 (cyclin-dependent kinase) amplification in liposarcoma: A comprehensive review". Crit Rev Oncol Hematol. 153. :103029. (2020)
- Lee B, McArthur GA. "CDK4 inhibitors an emerging strategy for the treatment of melanoma". Melanoma Management. 2(3). :255-266. (2015)
- Coleman WB. "Molecular Pathogenesis of Prostate Cancer". Elsevier. :555-568. (2018). ISBN: 9780128027615
- "Skin Cancer". https://web.archive.org/web/20201231013700/https://www.cdc.gov/cancer/skin/statistics/index.htm
- "Cancer Stat Facts: Common Cancer Sites". https://seer.cancer.gov/statfacts/html/common.html. [2018-04-01]
- Chen C-Y, Peng H-C, Chen Y-Y, Chan C-C, Yu C-J. "Association of environmental heavy metals exposure and lung cancer incidence and prognosis". 11.1 Lung Cancer. (2016)