Quick guide
Diagnostic approach
- Neurovascular exam
- Assess for features requiring urgent orthopedic consult.
- X-rays in ≥ 2 orthogonal views
- Consider x-rays of adjacent joints.
- CT or MRI if x-ray findings are inconclusive
- Preoperative diagnostics if urgent surgery is likely
Splint fractures with gross deformity and/or crepitus prior to imaging.
Red flag features
- Neurovascular compromise
- Open fractures
- Unstable fractures
- Skin tenting
- Gross deformity
- Crepitus
- Signs of compartment syndrome
Management checklist
- Analgesia for acute fractures (e.g., tramadol , ketorolac )
- Acute wound management for open fractures
- Antibiotic prophylaxis for open fractures
- Immobilize the affected extremity.
- Ice pack for 20–30 minutes every 1–2 hours
- Consider procedural sedation and/or regional anesthesia before interventions.
Summary
A fracture is a partial or complete interruption in the continuity of bone. The most common cause is trauma, followed by diseases that result in weakened bone structure. Fractures are named and classified according to a variety of characteristics, including location, extent, and orientation. Evaluation of a suspected fracture includes obtaining a patient history and assessing the skin, soft tissue, and sensory and motor function of the affected area. Fractures are typically diagnosed on x-ray; CT scan and MRI are helpful adjuncts for surgical planning and diagnosis of subtle or occult fractures. Acute management consists of analgesia, wound care, fracture reduction, and immobilization. Surgery may be necessary. Open fractures, in which the bone is exposed due to severe soft tissue injury, require urgent surgical management and antibiotic therapy. Acute complications include nerve and vascular injury, hemorrhage, and acute compartment syndrome (ACS); long-term complications include avascular necrosis and nonunion.
The specific management of different fracture types is covered in separate articles; see “Overview of common fractures” for links. See also “Management of trauma patients” and “Conservative management of fractures.”
Etiology
- Trauma: mechanical stress and/or loading
- Weakened bone structure: osteoporosis, bone tumors, metastasis, Paget disease
References:[1]
Classification
Fractures are typically classified based on the following characteristics: [2]
-
Anatomy
- Location: affected bone (proximal, distal)
- Position: diaphysis, metaphysis, epiphysis
-
Extent
- Complete
- Incomplete
- Orientation: transverse, oblique, spiral
-
Displacement
- Rotated: rotation around the longitudinal axis
- Angulated: angulation of the axis
- Translated: lateral movement of the bone fragments
- Longitudinal displacement of bone fragments
- Distraction: elongation
- Impaction: shortening
-
Fragmentation
- Comminuted fracture: more than two fracture lines resulting in multiple bone fragments
- Segmental fracture: two fracture lines with a bone fragment between the proximal and distal portions of the bone
-
Soft tissue involvement
- Closed fracture (simple fracture; does not come into contact with the outside environment)
- Open fracture
-
Stability [3]
-
Stable fractures
- Bone fragments remain in their normal anatomical alignment without significant displacement from their original position.
- Low risk of progression to dislocation or conversion to open fractures
-
Unstable fractures
- Bone fragments are significantly displaced, misaligned, or shifted from normal anatomical position.
- High risk of displacement after reduction and of complications or compromised healing
-
Stable fractures
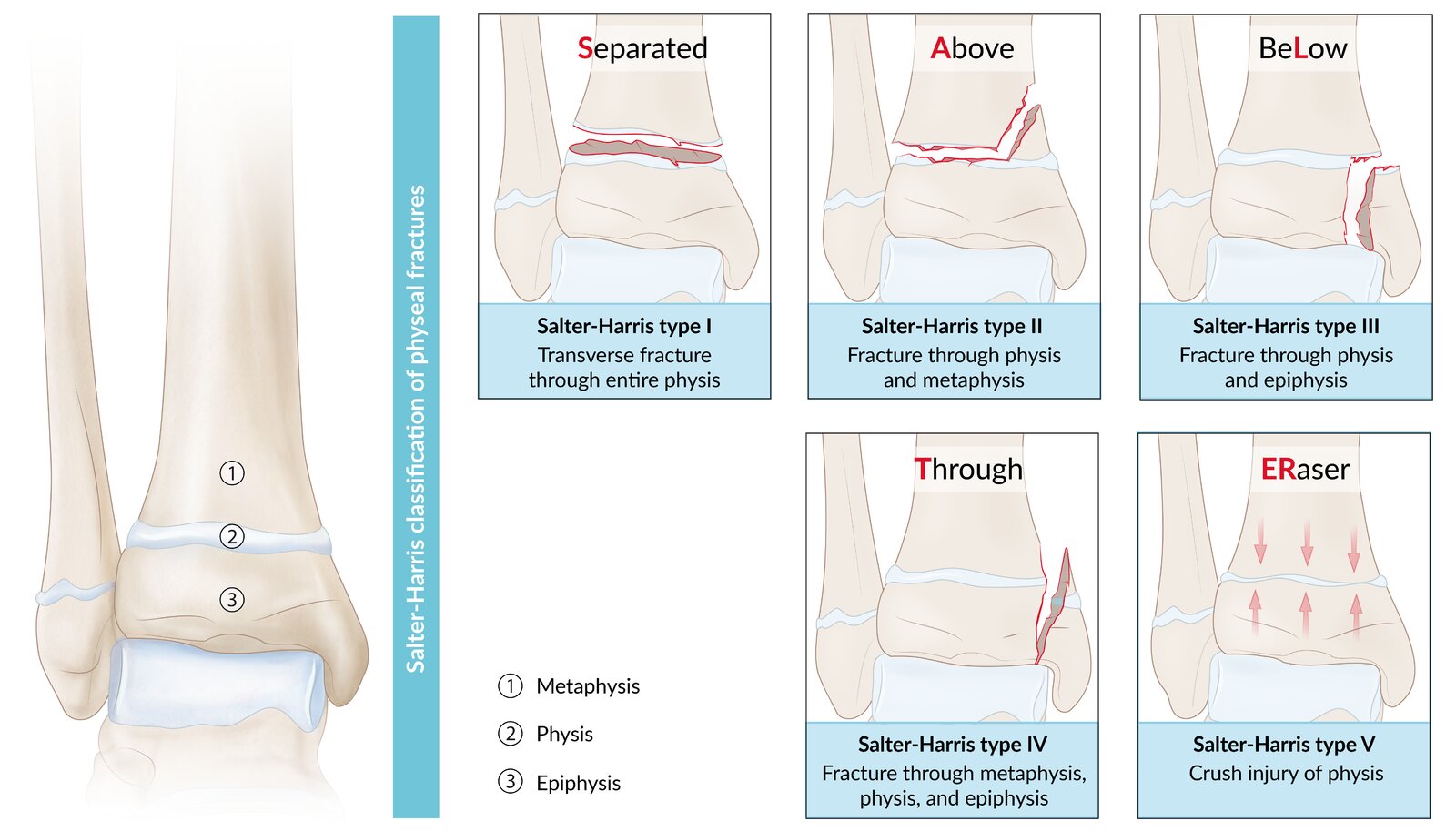
- Growth plate involvement (pediatric fractures): Salter-Harris fractures
To describe the features of a fracture, think NOLARD: Neurovascular status, Open vs. closed, Location, Angulation-Alignment-Articular, Rotation, Displacement. [2]
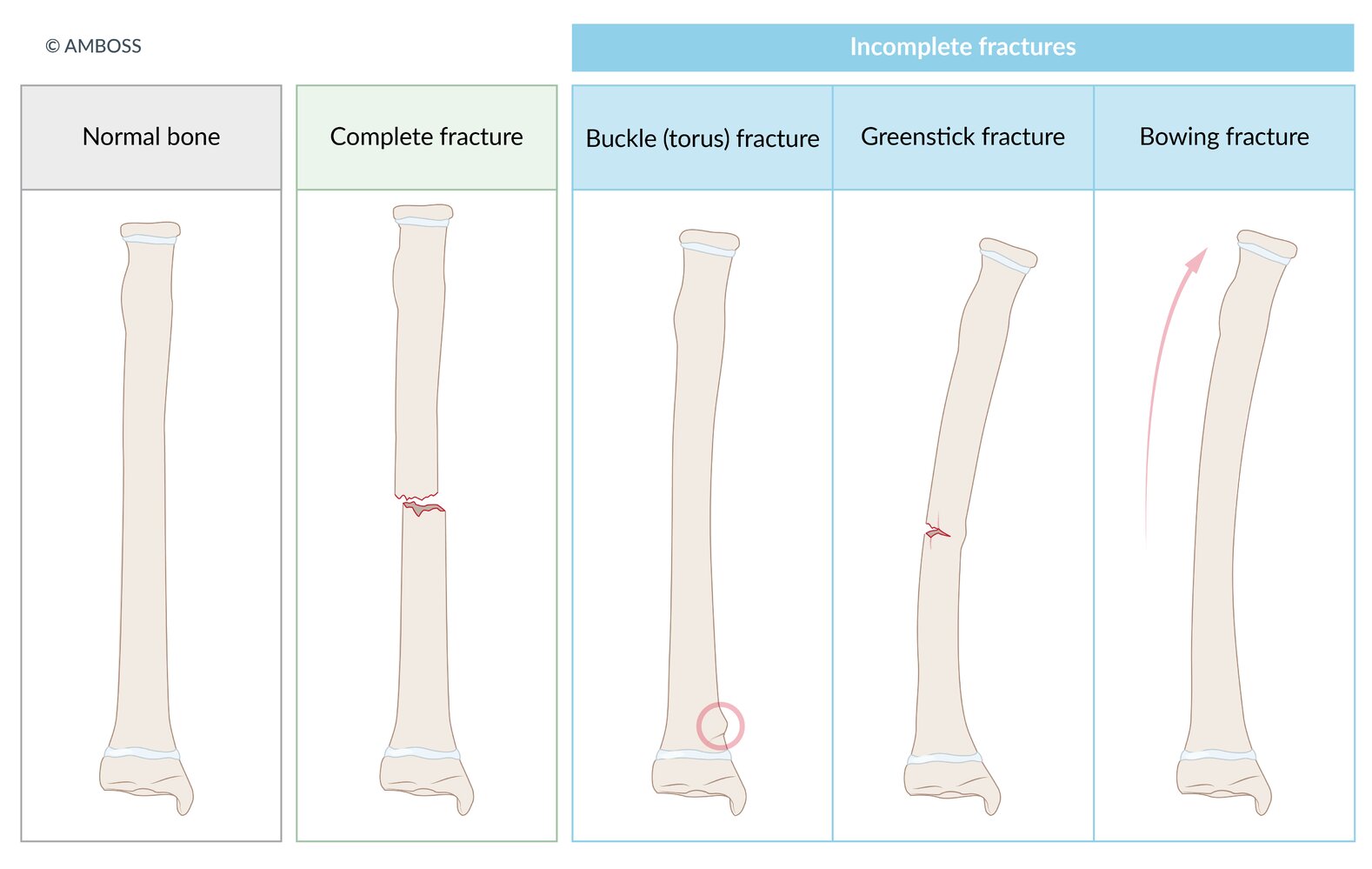
In a complete fracture, there is a discontinuity between the bone fragments, whereas in incomplete fractures, the fracture line is either absent or does not completely traverse the entire bone. Incomplete fractures are more common in children due to their thicker, stronger periosteum and the greater elasticity of growing bones. Types of incomplete fractures include:
Buckle (torus) fracture: A compressive force results in bulging, i.e., buckling of the cortex. More specifically, a buckle fracture is characterized by bulging of only one side of the cortex (the concave side), while a fracture in which the bulge is circumferential is referred to more precisely as a “torus fracture.” However, the terms are frequently used interchangeably.
Greenstick fracture: There is discontinuity of the cortex and periosteum on the convex (tension) side of the fracture, but bending occurs only on the concave (compression) side.
Bowing fracture: There is angulation but no discontinuity of the cortex or periosteum.
© AMBOSS
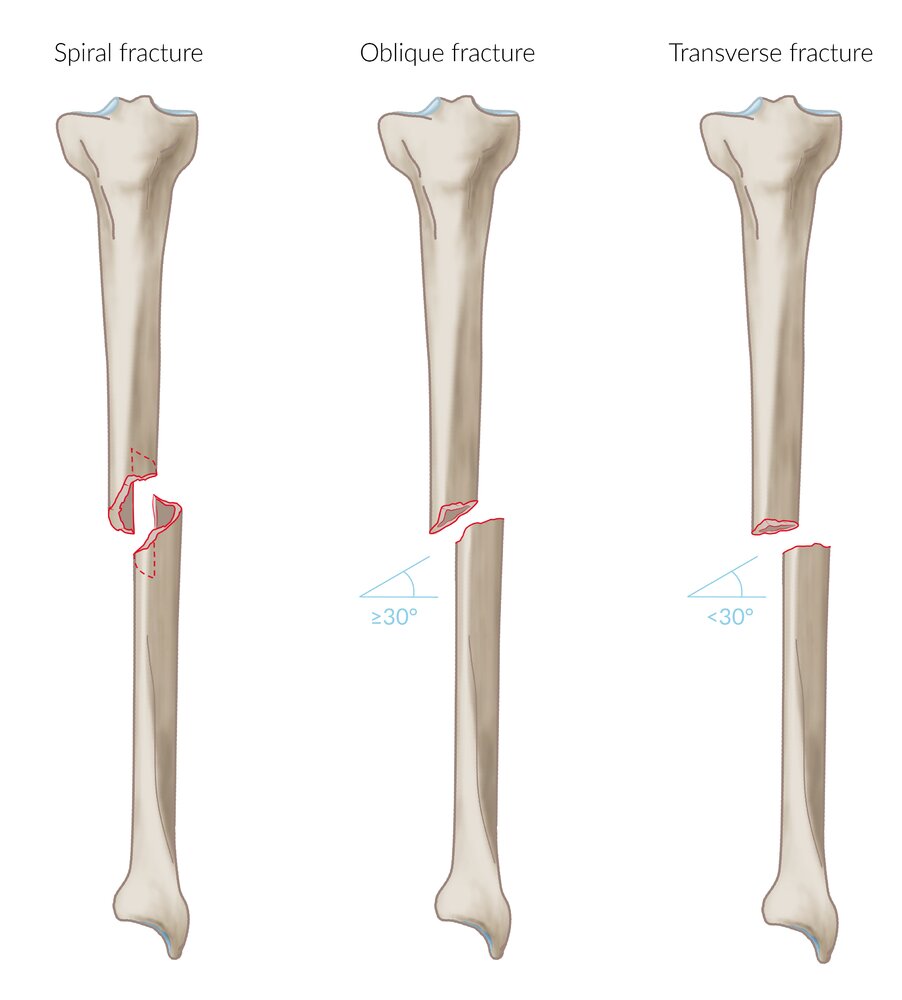
Right tibia, anterior view
Note that in a transverse fracture, the fracture line runs at an angle < 30°, while in an oblique fracture the angle is ≥ 30°.
© AMBOSS
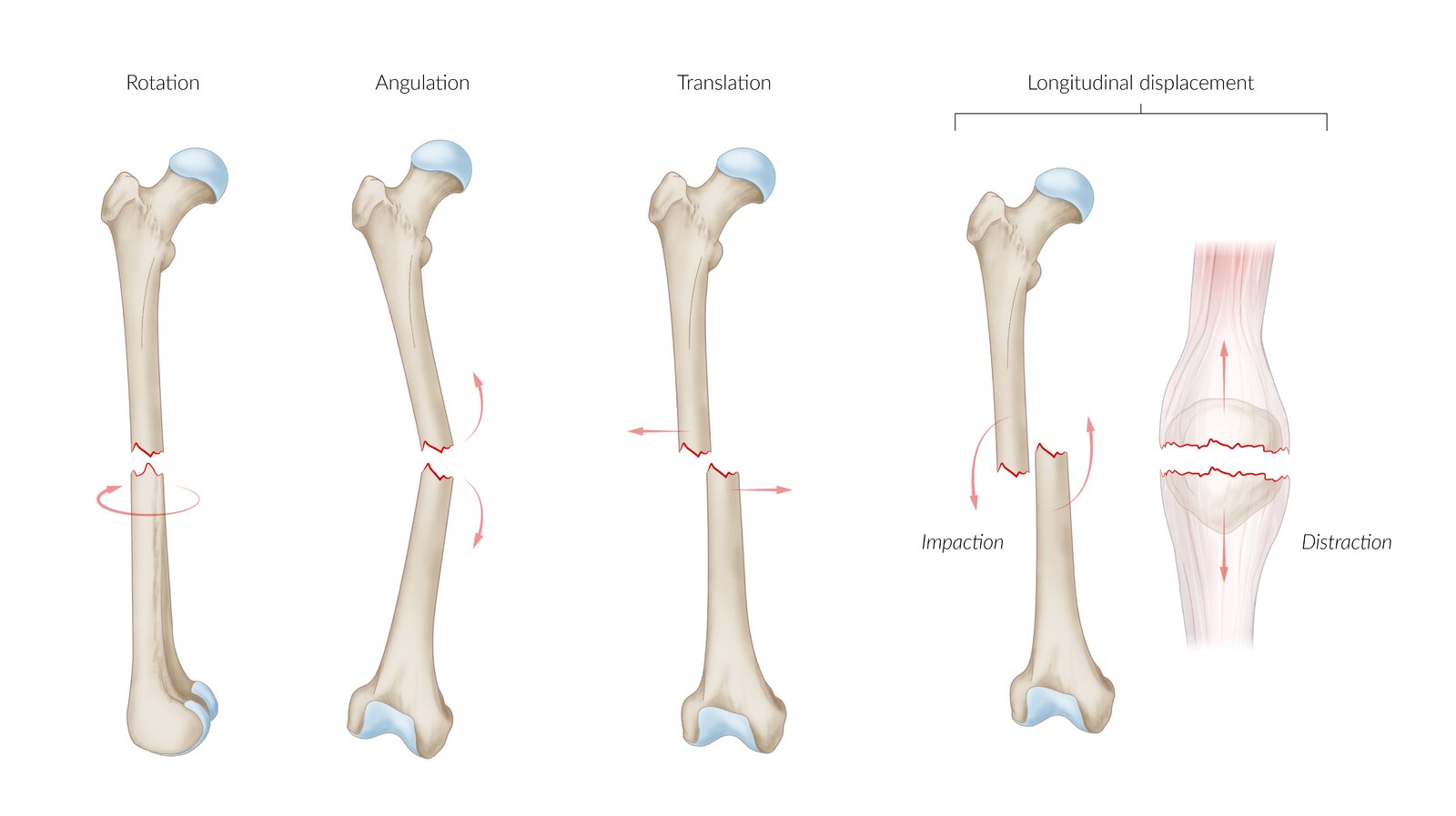
The most common types of fracture displacement, using the example of the femur and patella. The fracture sites are marked in red; the arrows indicate the directions the fracture fragments move.
© AMBOSS
© AMBOSS
Overview of common fractures
For common fractures in children (e.g., greenstick fractures), see “Pediatric fractures.”
Upper extremity fractures
- Humerus fractures
- Elbow fractures
-
Forearm fractures
- Monteggia fracture
- Galeazzi fracture
- Wrist fractures (distal radius fractures)
- Colles fracture
- Smith fracture
- Hand fractures
- Metacarpal fractures (e.g., boxer's fracture)
- Scaphoid fracture
- Phalangeal fractures
Lower extremity fractures
-
Hip fractures
- Femoral head fracture
- Femoral neck fracture
- Femoral shaft fracture
- Tibial fracture
- Ankle fracture
- Foot fractures
- Midfoot fracture (Lisfranc fracture): a tarsometatarsal fracture; may involve damage to the cartilage of the midfoot joints
- Jones fracture: fracture at the base of the shaft of the fifth metatarsal bone
- Talus fracture
- Calcaneal fracture
Truncal fractures
- Clavicle fracture
- Sternal fracture
- Rib fracture
- Vertebral fractures (including compression fracture)
- Pelvic fracture
Head and neck fractures
-
Skull fractures
- Basilar skull fracture
- Temporal bone fracture
-
Facial fractures
- Le Fort fractures
- Nasal bone fracture
- Mandibular fracture
Clinical features
- Pain localized to the fracture site
- Redness and swelling
- Limb deformity
- Palpable step-off or gap
- Bone crepitus
- Ecchymosis
- Possible neurovascular compromise below the site of injury
- Possible signs of an open fracture
Diagnosis
Approach [2][4]
- Conduct a thorough history and physical examination.
- Perform a neurovascular assessment to check for neurovascular injury and compartment syndrome.
- Obtain x-rays of the affected extremity in at least two orthogonal views.
- Consider advanced imaging (CT or MRI) in consultation with orthopedics (e.g., for suspected occult fractures).
- Obtain preoperative diagnostics if fractures are likely to require urgent operative treatment.
Any findings that suggest neurovascular injury or open fracture should prompt urgent orthopedic consultation.
Fractures associated with gross deformities and/or crepitus should be splinted prior to imaging. [2]
Neurovascular assessment [5][6]
- Purpose: detecting early signs of limb ischemia, peripheral nerve injury, or compartment syndrome
-
Components
- Sensation
- Motor function
- Perfusion
-
Findings
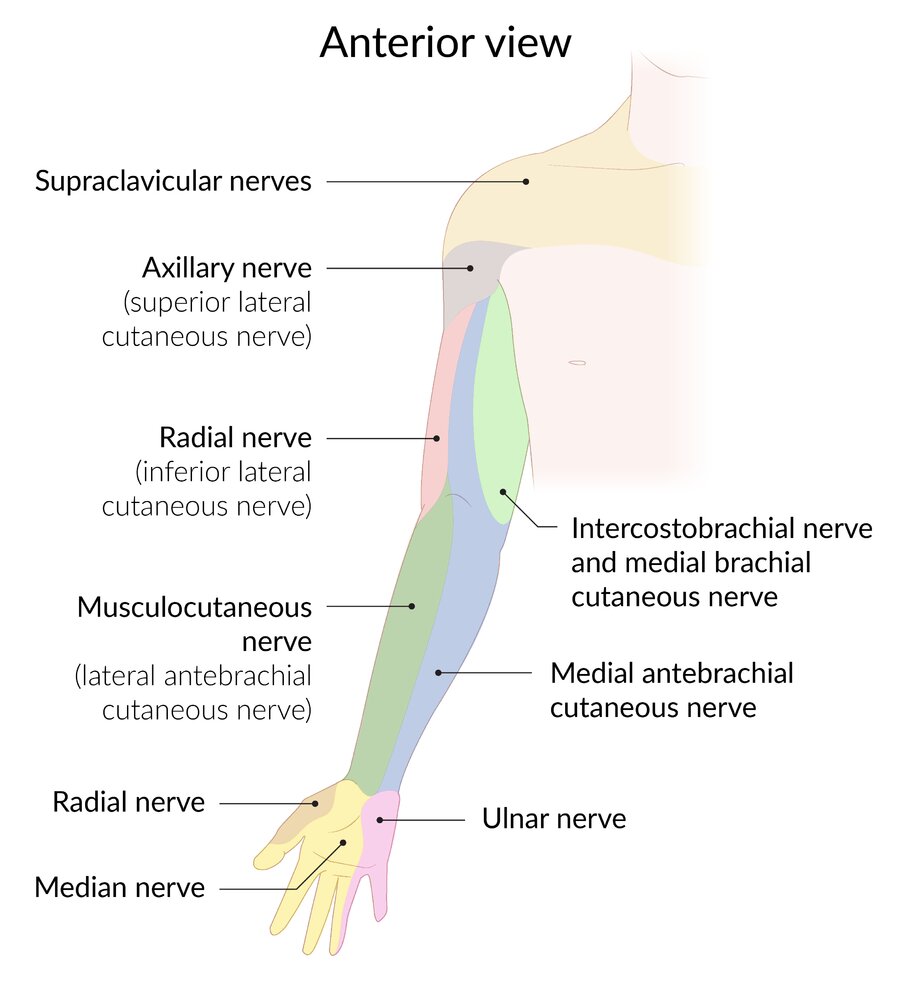
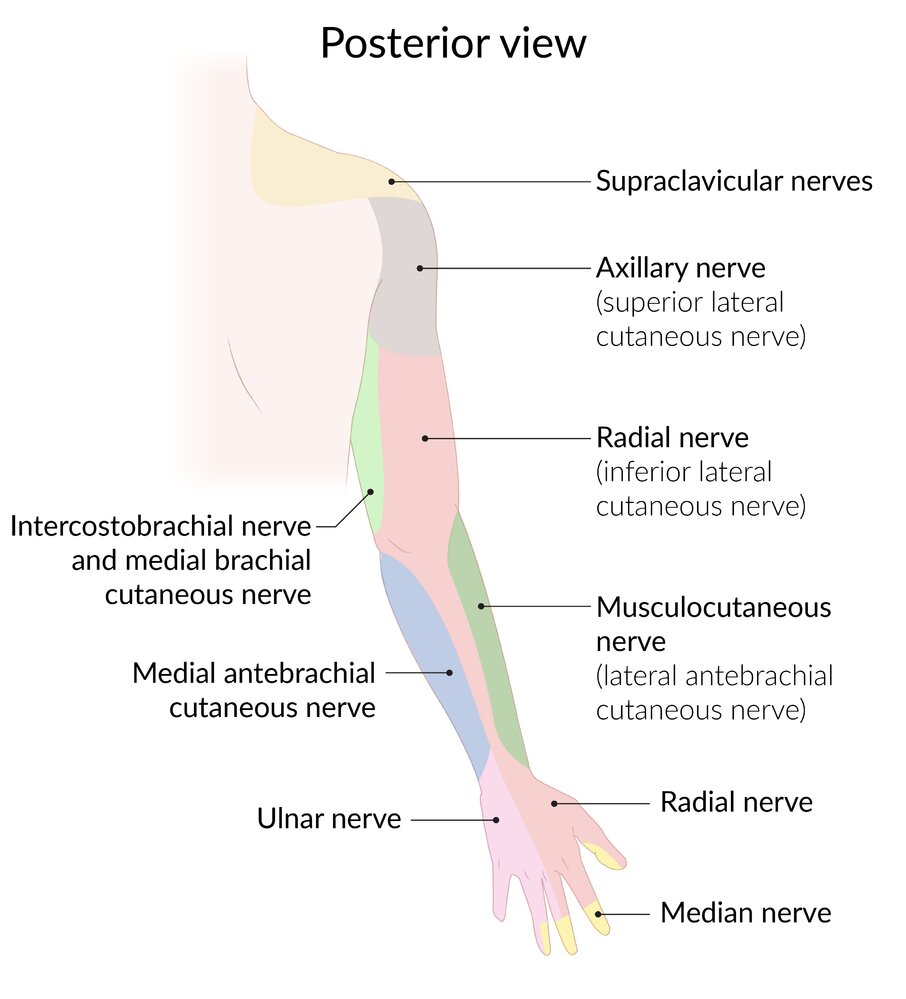
- See “Nerve injuries in the upper body.”
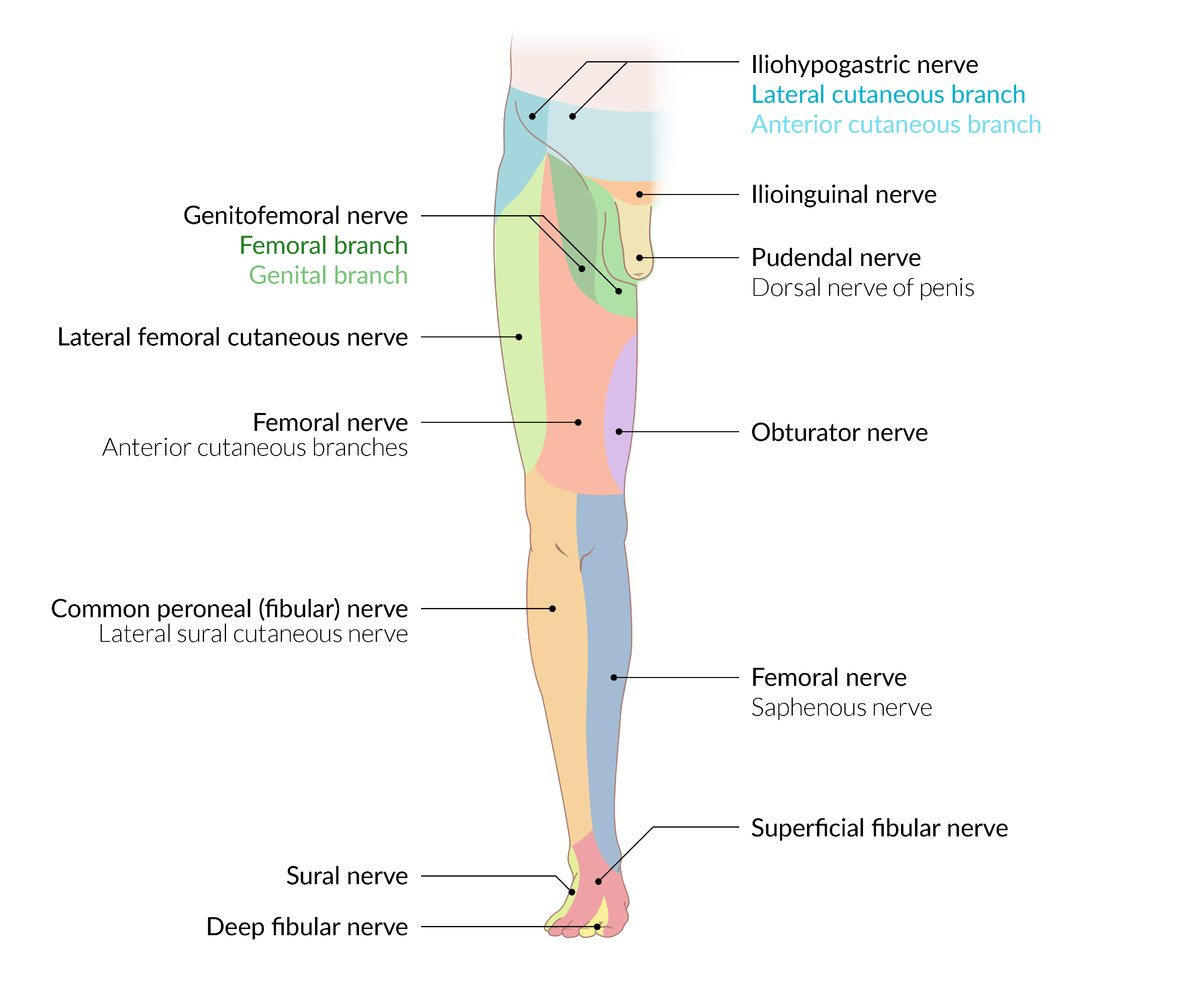
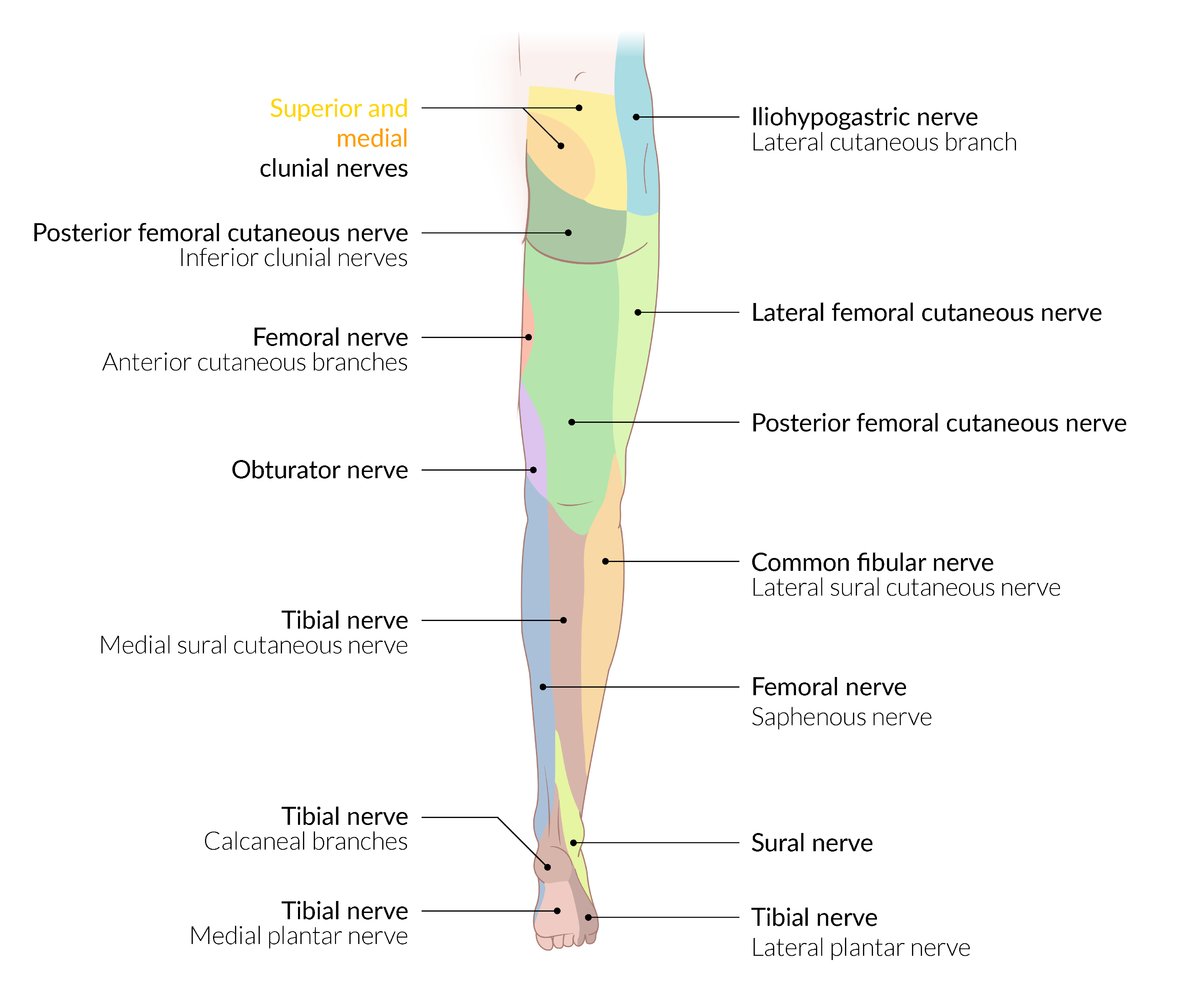
- See “Nerve injuries in the lower body.”
- Acute ischemia/ACS: 6 Ps of ALI
A neurovascular assessment should be performed in all patients with extremity injuries and repeated after every intervention (e.g., reduction or immobilization). [5]
")
")
")
")
Imaging [2][7]
X-ray
- Indication: all suspected fractures (before and after reduction)
-
Views
- All extremities: at least two orthogonal views (e.g., AP and lateral)
- Some sites may benefit from a dedicated third view (e.g., oblique view, notch view of the knee)
- Consider imaging of joints above and below a suspected fracture.
-
Radiographic fracture signs
- Disruption of bony cortex
- Radiolucent fracture line
- Fracture fragments in comminuted fractures
- Specific fracture findings, e.g. elbow fat pad signs , height loss in vertebral fractures
As fractures may not be visible on x-rays for up to two weeks after an injury, any focal bony tenderness after a severe injury should initially be treated as a fracture. [2]

")
")
")





Additional imaging modalities [4]
- Point-of-care ultrasound (POCUS): potential alternative to x-ray in patients who wish to avoid radiation or when x-ray is unavailable [8]
-
CT
- Inconclusive x-ray findings: may be indicated
- Assessment of associated injuries
- Preoperative planning for complicated fractures
- MRI: may be indicated to diagnose associated tendon/ligament injuries or occult fracture


© AMBOSS
© AMBOSS
© AMBOSS
© AMBOSS

X-ray distal forearm (PA view)
A comminuted fracture (red lines) of the distal radius shows intraarticular extension and radial displacement (indicated by green lines and arrows) of the main distal fragment (F). The ulnar styloid process (USP; normal position indicated by yellow dashed outline) is also fractured and displaced medially (indicated by yellow overlay and arrow).
Source: © IMPP

X-ray distal forearm (lateral view)
A comminuted fracture (red lines) of the distal radius shows intraarticular extension. Dorsal angulation of the main distal fragment has altered the bony alignment (indicated by green lines and arrows).
Source: © IMPP

X-ray ankle (left; lateral view)
A comminuted fracture of the distal fibula (green overlay) is well seen on this view, including a posterior fragment projected over the distal tibia (red outline) on the AP view. There is no fracture of the posterior aspect of the tibial plafond (posterior malleolus) as would be expected in a trimalleolar fracture. The shape of the talus (yellow overlay and dashed line) appears abnormal, consistent with its displacement on the AP view.
Red line: distal tibia
Source: © IMPP

X-ray ankle (left; AP view)
A transverse fracture of the medial malleolus (dashed white line) is seen along with a comminuted fracture of the distal fibula (green outlines) at the level of the ankle syndesmosis (Weber B fracture; blue overlay). The ankle mortise is disrupted, with lateral displacement of both the talus (yellow overlay) and the tibial fragment (red overlay) in relation to the tibial shaft.
Red outline: distal tibia
Source: © IMPP

Radiograph of the right hand: scaphoid fracture (arrow) following a fall on the outstretched hand.
(1 = scaphoid; 2 = lunate; 3 = triquetrum; 4 = pisiform; 5 = trapezium; 6 = trapezoid, 7 = capitate; 8 = hamate; I–V = metacarpals; R = radius; U = ulna)
Source: © IMPP

X-ray (posteroanterior view) of the humerus
Fracture of the humerus into multiple fragments. The overlay highlights the points of fracture belonging together in green and red. White-filled overlay highlights the ulna. White outline highlights the humerus. White dashed outline highlights the radius.
Source: © IMPP

X-ray of the elbow joint, lateral view
13-year-old girl who fell on an outstretched hand. The bones show no fracture, but a fat pad sign can be seen ventral and dorsal to the humeral shaft. The fat pad sign indicates elbow joint effusion. It arises when the fatty tissue usually attached to the distal humerus is lifted off the bone because of the joint effusion; while the fatty tissue is usually visible as a lucency parallel to the humerus, it becomes crescent-shaped if there is an effusion.
Our great thanks to PD Dr. M. Jergas (Center for Diagnostic and Interventional Radiology, St. Elizabeth Hospital, Cologne) for kindly providing this image.

X-ray lumbar spine (lateral view)
There is a chronic compression deformity (red dimension line) of the L4 vertebral body, with displacement (red overlay) toward the spinal canal beyond the posterior vertebral lines of L3 and L5 (white dotted line). Exuberant anterior osteophyte formation is visible at L3–4 (red dotted lines).
Source: © IMPP

X-ray sternum (lateral view)
A slightly displaced sternal fracture (arrow) is visible in the middle third of the sternum.
Created by: Dr. med. Kerstin Bohse. Organization providing image: Klinikum Pfeiffersche Stiftungen. Modifications to original image: Image cropped. Further notes: Many thanks to Dr. med. Kerstin Bohse (Klinikum Pfeiffersche Stiftungen) for kindly providing this case.

Ultrasound of the sternum (longitudinal plane) of an 83-year-old patient with sternal pain after falling on a bus and hitting her chest against the edge of a seat
Two sites of disruption of the cortex of the anterior sternum are seen.
Source: “Fig 1A, from: Point-of-Care Ultrasound for Diagnosis and Pain Control of Sternal Fracture” by Masoudi A, Naraghi L, Cureus, licensed under CC BY 4.0. Modifications: image cropped.
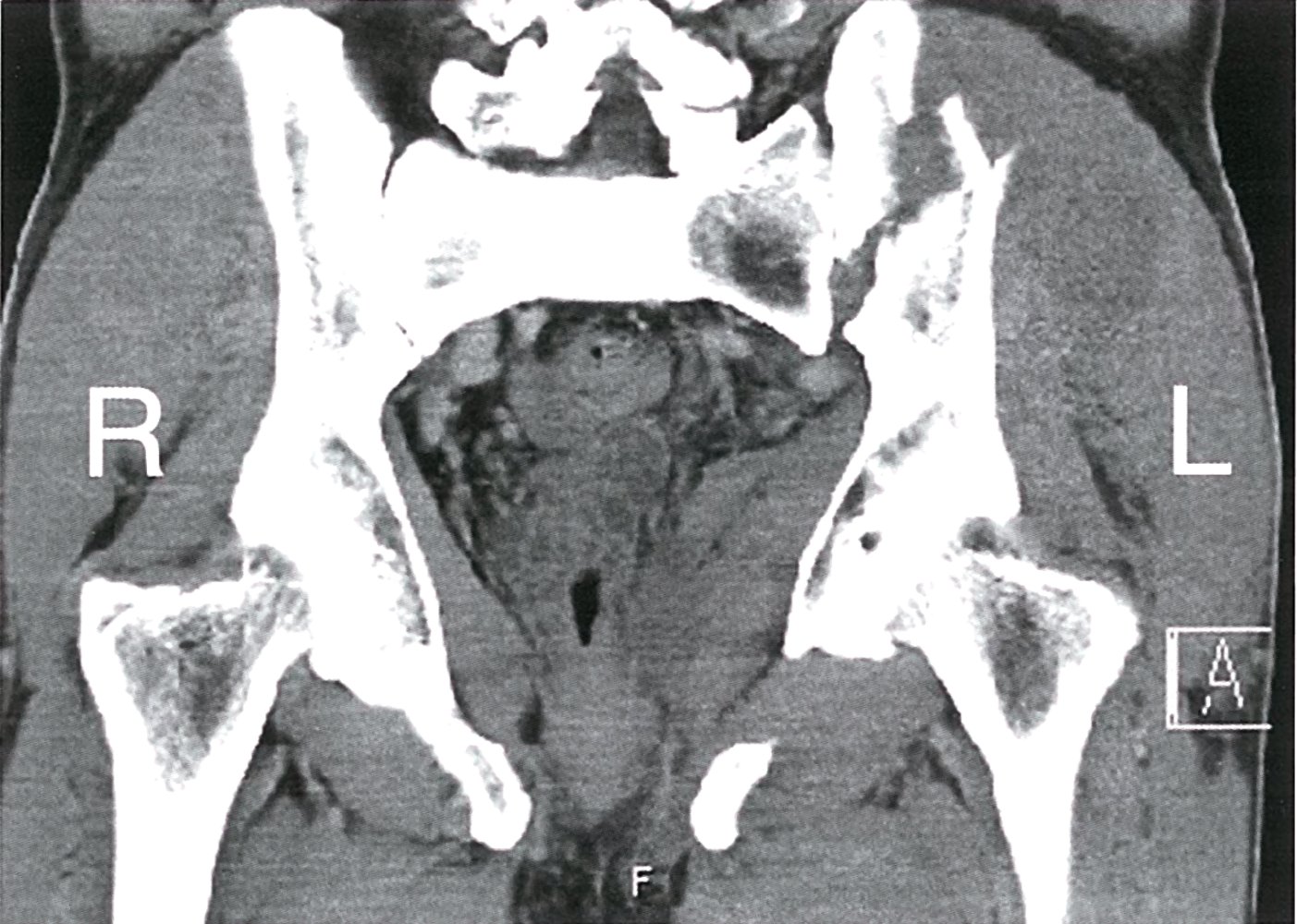
CT pelvis (soft tissue window; coronal section)
An obliquely oriented fracture, communicating with the left sacroiliac joint, is visible through the left iliac wing (green line).
Source: © IMPP
Treatment
Initial fracture management [2][4]
-
Immobilization
- Immobilize joints above and below for most extremity fractures.
- Splint in the position of function (if not otherwise specified).
- See “Conservative treatment of fractures” for details.
-
Indications to consult orthopedics for fractures [7]
- Any signs of neurovascular compromise or compartment syndrome
- Open fractures
- Displaced intraarticular fractures
- Fracture-dislocations
- Associated tendon injury
-
Supportive care
- Provide adequate analgesia.
- Perform wound care (see “Acute wound management”).
- Initiate antibiotic prophylaxis for open fractures.
- Admit or discharge with proper follow-up (see “Disposition” below).
Fractures with skin tenting should be reduced promptly to prevent conversion to an open fracture. [7]
Analgesia for acute fractures [7][9]
-
Nonoperative and/or outpatient management
-
Non-opioid analgesics
- Acetaminophen [9]
- NSAIDs: e.g., ibuprofen [9]
- Gabapentin [9]
-
Opioid analgesics: typically reserved for long bone fractures and/or severe pain
- Tramadol [9]
- Hydrocodone/acetaminophen [9]
- For prescribing principles and risk mitigation strategies, see “Opioids for acute pain.”
-
Non-opioid analgesics
-
Operative and/or inpatient management
- NSAIDs, e.g. ketorolac IV followed by ibuprofen PO [9]
- Combination analgesics, e.g. oxycodone/acetaminophen [9]
- Opioids for severe pain, e.g. hydromorphone [9]
-
Additional interventions
- Cryotherapy: Ice pack for 20–30 minutes every 1–2 hours. [2]
- Consider procedural sedation and/or regional anesthesia before interventions.
- Ensure proper immobilization of the fracture to reduce pain associated with movement.
Analgesics are typically only needed for 2–5 days following an injury. Consider a fracture complication if significant pain persists beyond this time frame. [7]
Nonoperative fracture management [2]
-
Indications
- Stable fractures without neurovascular compromise
- Most pediatric fractures
-
Procedure
- Closed reduction
- Long-term immobilization with a cast or splint
- See “Conservative treatment of fractures” for supportive care and additional considerations.
Surgical fracture management
-
Indications [2]
- Open fractures
- Associated arterial injury
- Severe displacement (e.g., rotational deformities) with displaced fragments
- Inadequate manual reduction and fixation
- Unstable fractures
- Displaced intraarticular fractures
- Fracture within metastatic lesion
-
Procedure: anatomical reduction of the fracture and subsequent fixation and immobilization
-
External fixation
- Immobilization of a fracture using pins or screws that are secured outside of the skin
- Commonly performed as a temporary measure in severely injured patients or contaminated open fractures
-
Internal fixation
- Immobilization of a fracture using implants (e.g., plates, screws, wires)
- Can be performed in combination with closed or open reduction
- See “Osteosynthetic procedures” for details.
-
External fixation
Disposition [4]
-
Discharge considerations
- Consider discharge with supportive care for:
- Stable nonoperative fractures
- Stable fractures after successful closed reduction
- Arrange follow-up with orthopedics in 3–5 days.
- Consider discharge with supportive care for:
-
Indications for admission
- Urgent operative management needed
- Severe intractable pain
- Inability to safely ambulate or perform activities of daily living
-
Specialist referral
- Orthopedics: casting, reassessment, and operative planning
- Podiatry: management of foot fractures
- Physical medicine and rehabilitation: postfracture rehabilitation
Complications
Acute complications [2][7]
- Acute compartment syndrome
- Neurovascular injury (e.g., nerve injury, bleeding, hematoma, seroma)
-
Fracture blisters
- Clear or hemorrhagic blister that can develop between 6 hours and 3 weeks after injury; most commonly after 24–48 hours
- May delay intervention because of increased risk of infection and wound dehiscence and should be left intact
- Wound infection
- Osteomyelitis
- Secondary dislocation
- Fat embolism
Closed femur fractures and pelvic fractures may be associated with significant hemorrhage requiring transfusion. [7]
Suspect compartment syndrome in patients with intense or disproportionate pain (e.g., pain with passive stretch), even in the absence of additional symptoms. [2]



Complications due to immobilization [10][11]
- Thrombosis (e.g., DVT, pulmonary embolism)
- Muscle atrophy
- Joint contractures
- Cardiovascular deconditioning
- Decubitus ulcer
- Infections, e.g.:
- Pneumonia
- Urinary tract infection
Complications of nonweightbearing
- Muscle atrophy
- Crutch palsy
Compromised fracture healing
Nonunion [12]
- Definition: incomplete healing of a fracture; can result in the creation of a false joint (pseudarthrosis)
-
Risk factors
- Poor vascular supply
- Inadequate immobilization
- Chronic diseases (e.g., diabetes mellitus, osteoporosis)
- Open fractures
- Infection
- Smoking
-
Types [13]
- Hypertrophic nonunion: callus formation in the fracture zone
- Atrophic nonunion: atrophic bone without callus formation
-
Clinical features
- Pain and swelling
- Limited weight-bearing capacity
- Reduced range of motion that persists
- Diagnosis: Imaging shows lack of fracture consolidation 6–9 months after injury.
-
Treatment [14]
- Debridement and resection
- Osteosynthesis (fixation)
- Culture-directed antibiotics for infected nonunion


")
")
Malunion [2][15]
- Definition: healing of a fracture in a pathological position
-
Risk factors
- Inadequate immobilization
- Inaccurate reduction
- Unsuccessful surgical fixation
-
Clinical features
- Pain and swelling
- Impairment of function
- Limb shortening (poorly tolerated in the lower extremities)
- Treatment: surgical correction (osteotomy) in symptomatic patients
Long-term complications
- Growth disturbances after growth plate fracture in children
- Chronic osteomyelitis
- Avascular necrosis
- Posttraumatic osteoarthritis
- Complex regional pain syndrome
- Joint stiffness/contracture
- Joint instability
- Heterotopic ossification
We list the most important complications. The selection is not exhaustive.

Lower leg of a patient with severe pain, interdigital dysesthesias, and ankle dorsiflexion weakness one day following closed reduction and intramedullary fixation of a lower leg fracture
The leg is swollen; the skin is taut, shiny, and partially erythematous; the sutures are visibly under tension.
These symptoms and findings are consistent with compartment syndrome. Immediate fasciotomy is indicated.
Source: © IMPP

Left foot and ankle of a patient with Weber type B fracture
Multiple hemorrhagic blisters are seen on the medial side of the ankle. The area around the blisters is swollen and shows an extensive hematoma.
These findings are characteristic of fracture blisters, which typically form over the fracture site.
Source: "Fracture blisters", Cindy L. Budge, Wikimedia Commons licensed under Public Domain
{kind=link}

Photograph of the right ankle of a patient who underwent an osteosynthesis procedure after an ankle fracture.
There is swelling and erythema, and pus is discharging from the proximal end of the wound.
Source: © IMPP

AP radiograph of the ankle joint and lower leg: hypertrophic pseudarthrosis of the distal fibula
Source: © IMPP

X-ray pelvis (AP view)
Abnormal healing has occurred at the site of a fracture through the left femoral neck, with development of a pseudarthrosis. The fracture line (green overlay) remains visible, and sclerosis (red overlay) has developed along its margins. The femoral neck has widened. There are also degenerative changes, with medial joint space narrowing (indicated by arrowheads).
Source: © IMPP

X-ray left humerus (AP view)
The humeral diaphyseal fracture remains conspicuous following internal fixation using an intramedullary nail with locking screws. Callus (green overlay) has developed, although it does not bridge the fracture line (red overlay). The appearance is compatible with hypertrophic nonunion.
Source: © IMPP

X-ray left humerus (coned AP view)
The humeral diaphyseal fracture remains conspicuous following internal fixation using an intramedullary nail with locking screws. Callus (green overlay) has developed, although it does not bridge the fracture line (red overlay). This appearance is compatible with hypertrophic nonunion.
Source: © IMPP
Subtypes and variants
Specific types of fractures that require modified approaches to diagnostics and treatment include open fractures and pathologic fractures.
Open fracture [2][7]
Definition
- A fracture with direct communication to the outside environment via a break in the skin and soft tissue
- Typically caused by high-energy trauma
Clinical features of open fractures
- Soft tissue injuries: open wound or puncture
- Visible bone fragments in an open wound
- Visibly greasy, fatty, or oily blood loss


Diagnostics
-
Clinical evaluation
- Examine fractures closely for signs of skin and soft tissue compromise.
- Perform a thorough neurovascular examination.
-
Imaging
- X-ray of the fracture and surrounding joints: Air may be detected in the soft tissue. [2]
- Consider CT (e.g., for periarticular injuries).
Treatment [2][4]
-
Acute wound management and immobilization
- Remove visible foreign bodies and debris.
- Irrigate wound with sterile saline if operative irrigation will be performed > 2 hours postinjury.
- Cover with moist, sterile dressing and splint the fractured extremity.
- Perform tetanus prophylaxis if vaccine status is outdated or unknown.
-
Emergent orthopedic referral
- Operative irrigation and debridement within 24 hours of injury
- Tuft fractures with small, clean wounds may be managed in the ED with irrigation and debridement.
-
Antibiotic prophylaxis for open fractures: Initiate as soon as possible after injury. [16][17]
- Most injuries without gross contamination: Gram-positive coverage suffices.
- First-generation cephalosporins, e.g., cefazolin [17]
- For patients with penicillin allergy: e.g., clindamycin [17]
- Severe/extensive injuries: Consider broader coverage, e.g., with ceftriaxone. [16][17][18]
- Duration: 24 hours unless active infection develops [16]
- Most injuries without gross contamination: Gram-positive coverage suffices.
Fractures associated with wounds directly over the site, even if minor, should be treated as open fractures.
Operative management of open fractures should be performed promptly because of the high risk of osteomyelitis.
Pathologic fracture [2]
Definition
- A fracture due to abnormal bone weakness caused by an underlying condition; may be spontaneous or secondary to minor trauma [19]
Etiology
- Disorders affecting bone metabolism, e.g., osteoporosis (most common cause), hyperparathyroidism
- Bone lesions
- Malignant bone tumors and bone metastases [20]
- Benign bone tumors (including bone cysts)
- Malignant blood diseases (e.g., multiple myeloma)
- Infection: chronic osteomyelitis
Common locations [19]
- Proximal femur
- Proximal humerus
- Spine (vertebral compression fractures)
Clinical features
- Pain localized over fracture site
- Occasionally painless swelling over fracture site
- Systemic symptoms (e.g., fatigue, unexplained weight loss)
- Generalized bone pain
Diagnostics
-
X-ray findings (depending on the underlying cause)
- Bone lesions
- Thinning of the cortices
- Generalized osteopenia
- Other imaging modalities: CT, MRI


Treatment
- Initial treatment aligns with general fracture care.
- Further management depends on location and etiology.
Other
-
Avulsion fracture [2][21]
- A fracture caused by bone shearing at the insertion point of a tendon or ligament
- Most commonly due to ligamentous traction; can be acute or chronic
- May be associated with joint instability due to ligament injury
- Surgical management may be necessary for significantly displaced fracture fragments or injury to other structures.
-
Periprosthetic fracture [22]
- A fracture directly adjacent to an orthopedic implant; most commonly due to low-energy trauma
- Stable fractures with fixed hardware are managed with immobilization and restricted weight-bearing.
- Unstable fractures and/or loose prostheses require surgical revision.
-
Occult fracture
- A fracture that is not radiographically evident following an injury
- Common locations include the scaphoid and hip.
- If an occult fracture is suspected, general fracture care (including immobilization) should be initiated.
-
Stress fracture
- Fracture of structurally normal bone due to repetitive microtrauma
- See “Stress fractures” for details.
-
Greenstick fracture
- Type of incomplete fracture; common in children
- See “Pediatric fractures” for details.
- Fractures suggesting abuse: See “Injuries suggestive of child abuse” for patterns that may indicate physical child abuse.
Accessory ossicles are sometimes mistaken for avulsion fractures, but they can be differentiated by their smooth borders. [2]



Part of the distal tibia can be seen protruding from the wound at the medial malleolus.
Source: © IMPP

The distal tibia protrudes from a wound at the medial malleolus. There is soft tissue swelling of the distal part of the lower leg and the fracture forces the foot into a slightly pronated position.
Source: “Offene Luxation.jpg” by Xy01, Wikimedia Commons, licensed under CC BY-SA 2.0.
{kind=link}

X-ray right shoulder (AP view; external rotation) of a patient with metastatic renal cell carcinoma
A fracture (dashed lines) traverses a lytic lesion (green overlay) involving the surgical neck of the humerus. The lesion margin is ill-defined (wide zone of transition) and cortical breakthrough is present.
Source: “Pathologische Fraktur des Humerus bei einer Metastase eines Nierenzellkarzinoms.” by Hellerhoff, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}

AP radiograph of the hip: the osteolytic metastasis (reduced bone density with thinning of the cortical bone and the medullary cavity, highlighted in green) of the proximal femur weakened the bone, and led to a pathological, displaced, subtrochanteric femoral fracture.
Source: © IMPP

X-ray left foot (oblique view)
An avulsion fracture is present at the base of the 5th metatarsal.
Other entities that occur at the base of a 5th metatarsal and must be distinguished from a fracture are an apophysis and an os vesalianum. The orientation of an avulsion fracture is typically transverse to the metatarsal shaft. An apophysis is longitudinally oriented and generally fuses during adolescence. An os vesalianum resides within the peroneus brevis tendon, can appear rounded or triangular, and may articulate with the cuboid bone.
Green overlay: fracture fragment
Source: “FractureBaseof5th” by James Heilman, MD, Wikimedia Commons, licensed under CC BY-SA 4.0. Modifications: - arrow removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 4.0.
{kind=link}

Left hip (anteroposterior view) of a patient with a modular total hip arthroplasty
A fracture (overlay) involves the femoral trochanters and the diaphysis at the level of the prosthetic stem. Loosening is seen along the stem.
The term periprosthetic fracture is used to describe a fracture that occurs in the region of an orthopedic prosthesis, typically a hip or knee arthroplasty.
Source: “Periprosthetic fracture of left femur, case 1, before treatment” by Jmarchn, Wikimedia Commons, licensed under CC BY-ND 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
{kind=link}
External Resources
References
- Wick JY. "Spontaneous fracture: multiple causes". Consult Pharm. 24(2). :100-113. (2009)
- Sherman SC. "Simon's Emergency Orthopedics, 8th edition". McGraw Hill Professional. (2018). ISBN: 9781259860836
- Foster AL, Moriarty TF, Zalavras C, et al. "The influence of biomechanical stability on bone healing and fracture-related infection: the legacy of Stephan Perren". Injury. 52(1). :43-52. (2021)
- Walls R, Hockberger R, Gausche-Hill M, Erickson TB, Wilcox SR. "Rosen's Emergency Medicine 10th edition- Concepts and Clinical Practice E-Book". Elsevier Health Sciences. (2022). ISBN: 9780323757904
- Faraz A, Qureshi AI, Noah H Khan M, et al. "Documentation of neurovascular assessment in fracture patients in a tertiary care hospital: A retrospective review". Ann Med Surg. 79. (2022)
- Judge NL. "Neurovascular assessment". Nurs Stand. 21(45). :39-44. (2007)
- Eiff MP, Hatch RL. "Fracture Management for Primary Care and Emergency Medicine". Elsevier. (2019). ISBN: 9780323496346
- Chartier LB, Bosco L, Lapointe-Shaw L, Chenkin J. "Use of point-of-care ultrasound in long bone fractures: a systematic review and meta-analysis". CJEM. 19(2). :131-142. (2016)
- Hsu JR, Mir H, Wally MK, Seymour RB. "Clinical Practice Guidelines for Pain Management in Acute Musculoskeletal Injury". J Orthop Trauma. 33(5). :e158-e182. (2019)
- Krishnagopalan S, Johnson EW, Low LL, Kaufman LJ. "Body positioning of intensive care patients: Clinical practice versus standards". Crit Care Med. 30(11). :2588-2592. (2002)
- Reichman EF. "Emergency Medicine Procedures, Second Edition". McGraw-Hill Education / Medical. (2013). ISBN: 9780071613507
- Reahl GB, Gerstenfeld L, Kain M. "Epidemiology, Clinical Assessments, and Current Treatments of Nonunions". Curr Osteoporos Rep. 18(3). :157-168. (2020)
- Morshed S. "Current Options for Determining Fracture Union". Adv Med. 2014. :1-12. (2014)
- Nauth A, Lee M, Gardner MJ, et al. "Principles of Nonunion Management: State of the Art". J Orthop Trauma. 32(3). :S52-S57. (2018)
- Weber D, Borisch N, Weber M. "Treatment of malunion in ankle fractures". Eur J Trauma Emerg. 36(6). :521-524. (2010)
- Buckman SA, Forrester JD, Bessoff KE, et al. "Surgical Infection Society Guidelines: 2022 Updated Guidelines for Antibiotic Use in Open Extremity Fractures". Surg Infect (Larchmt). 23(9). :817-828. (2022)
- Garner MR, Sethuraman SA, Schade MA, Boateng H. "Antibiotic Prophylaxis in Open Fractures". J Am Acad Orthop Surg. 28(8). :309-315. (2020)
- Suzuki T, Inui T, Sakai M, et al. "Type III Gustilo–Anderson open fracture does not justify routine prophylactic Gram-negative antibiotic coverage". Sci Rep. 13(1). (2023)
- Marshall RA, Mandell JC, Weaver MJ, et al. "Imaging Features and Management of Stress, Atypical, and Pathologic Fractures". Radiographics. 38(7). :2173-2192. (2018)
- "Pathologic Fractures: What the Radiologist Needs to Know"
- Choi C, Lee SJ, Choo HJ, Lee IS, Kim SK. "Avulsion injuries: an update on radiologic findings". Yeungnam University Journal of Medicine. 38(4). :289-307. (2021)
- Capone A, Congia S, Civinini R, Marongiu G. "Periprosthetic fractures: epidemiology and current treatment.". Clin Cases Miner Bone Metab. 14(2). :189-196