Summary
Gestational trophoblastic disease (GTD) is a class of neoplastic conditions characterized by abnormal trophoblast-cell growth in the uterus. GTD is classified into hydatidiform moles (molar pregnancy), which are subclassified into complete and partial moles, and gestational trophoblastic neoplasia (GTN), which is subclassified into choriocarcinoma, invasive moles, placental site trophoblastic tumors, and epithelioid trophoblastic tumors. Hydatidiform moles are benign but have a malignant potential, whereas GTN are malignant lesions with a tendency to metastasize, especially to the lungs. Typical symptoms of GTD are vaginal bleeding and pelvic tenderness. Additional features of complete moles include enlarged uterus, hyperemesis gravidarum, and preeclampsia. Diagnosis of GTD is established on the basis of significantly elevated serum β-HCG and ultrasound findings. If GTN is suspected, workup must include x-ray of the chest to screen for lung metastases. Hydatidiform moles are typically treated via suction evacuation and curettage, whereas GTN treatment typically starts with chemotherapy.
Overview
Hydatidiform mole
A type of GTD resulting from abnormal fertilization of an egg that can invade the uterus and metastasize
- Complete mole: a type of hydatidiform mole typically resulting from fertilization by a single sperm of an abnormal egg that lacks maternal chromosomes
- Partial mole: a type of hydatidiform mole typically resulting from fertilization of an egg by two sperm or a diploid sperm
Gestational trophoblastic neoplasia (GTN)
A type of malignant GTD characterized by a high risk of local invasion and metastasis
- Choriocarcinoma: a highly malignant GTN characterized by invasive, highly vascular, and anaplastic trophoblastic tissue without villi
- Invasive mole: a type of GTN characterized by edematous chorionic villi and direct invasion of the myometrium by abnormal trophoblastic cells
- Placental site trophoblastic tumor: a rare type of potentially malignant GTN that is characterized by the absence of villi, decreased syncytiotrophoblast cells, and proliferation of intermediate trophoblast cells
- Epithelioid trophoblastic tumor: a type of GTN that is characterized by nests, cords, and/or sheets of intermediate trophoblastic cells with eosinophilic to clear cytoplasm
| Overview of gestational trophoblastic disease | |||||
|---|---|---|---|---|---|
| Hydatidiform mole | Gestational trophoblastic neoplasia | ||||
| Partial mole | Complete mole | Invasive mole | Choriocarcinoma | ||
| Risk |
|
|
|
||
| Etiology |
|
|
|
||
| Clinical features |
|
|
|
|
|
| Diagnostics | β-hCG |
|
|||
| Imaging |
|
|
|
|
|
| Histopathological exam | Microscopy |
|
|
|
|
| P57 staining |
|
|
|
||
| Treatment |
|
|
|||
| Prognosis |
|
|
|||
The risk of malignant GTN is higher in complete mole than in partial mole.
")



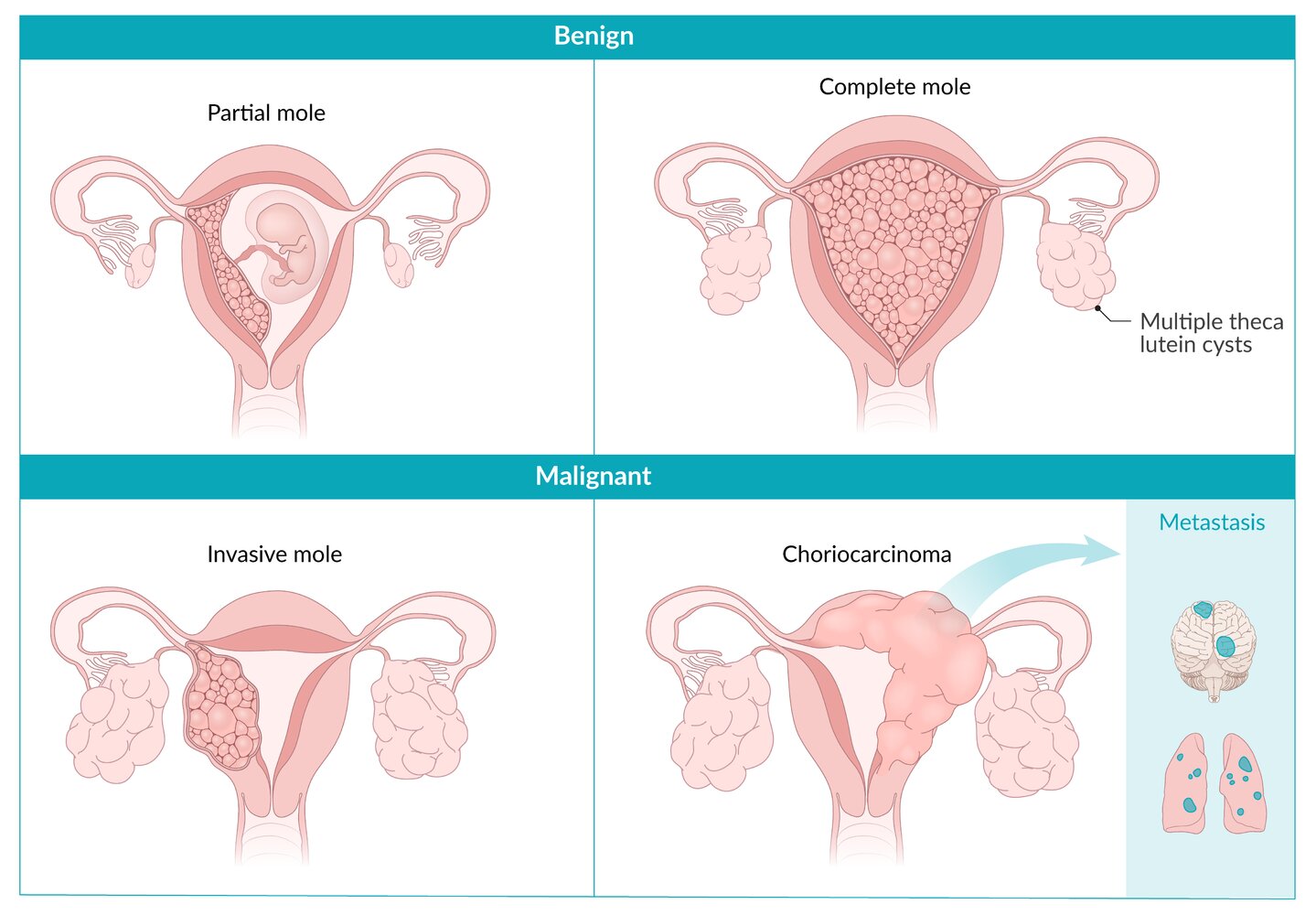
GTD is a group of diseases that originate in the placenta and typically result from abnormal fertilization of the ovum. Complete and partial moles may develop malignant traits and become invasive. Choriocarcinoma may be preceded by hydatidiform moles (50% of cases), ectopic pregnancy or miscarriages, or normal pregnancy.
Theca lutein cysts result from exaggerated stimulation of the theca interna cells of the ovarian follicles due to excessive amounts of beta-hCG.
© AMBOSS

Ultrasound pelvis (transvaginal) of pregnant patient with abnormally elevated β-hCG level
There is no intrauterine gestation. An intrauterine mass (green outline) contains multiple cystic spaces (examples indicated by red overlay), which correspond to hydropic trophoblastic villi.
This vesicular appearance seen in a molar pregnancy has been described as a “snowstorm pattern”.
Source: “Molar pregnancy” by Mikael Häggström, Wikimedia Commons, licensed under CC0 1.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
{kind=link}

X-ray chest (PA view) of a patient with lung metastases
Multiple pulmonary nodules with circumscribed margins can be seen in both lungs (examples indicated by green overlays). Differential diagnoses include malignant etiologies (metastatic disease, primary lung cancer, lymphoma) and benign etiologies (infection, embolism, autoimmune disease). An old healed fracture of the right clavicle (white arrow) is also visible.
Source: “The appearance of lung metastasis in patient that was reported” by Ghaemmaghami F, Zarchi MK, Early Onset of Metastatic Gestational Trophoblastic Disease after Full-Term Pregnancy, International Journal of Biomedical Science, licensed under CC BY 2.5. Modifications: removed yellow arrow. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
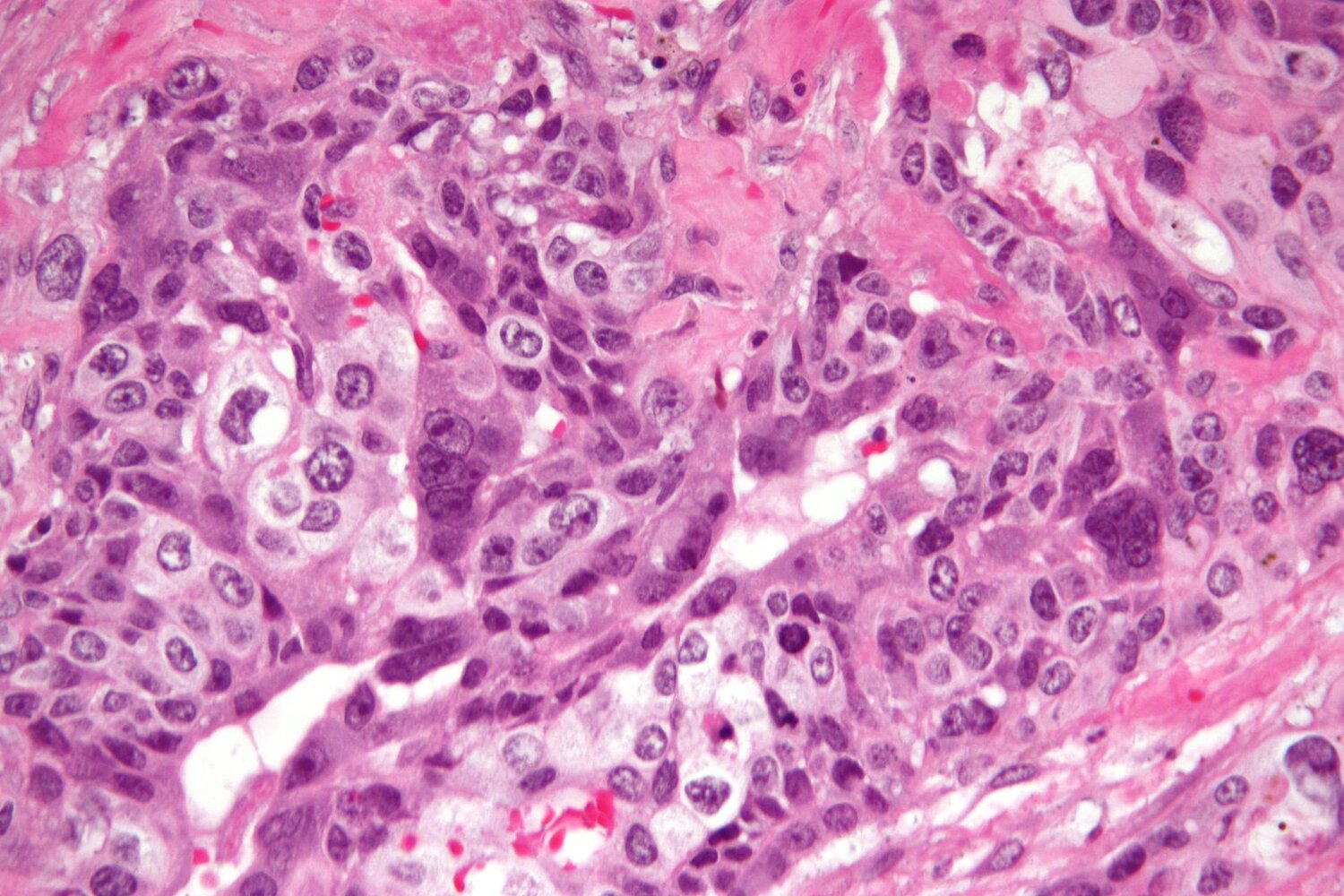
Photomicrograph of testicular tumor specimen (H&E stain; very high magnification)
Cytotrophoblasts are visible throughout the tumor in the form of polygonal-shaped cells with pale cytoplasm, enlarged oval nuclei, and distinct cell borders (examples indicated by arrowheads). Syncytiotrophoblasts are visible as multinucleated cells with eosinophilic cytoplasm (examples indicated by green overlay) surrounding the mononuclear cytotrophoblasts.
These findings are suggestive of choriocarcinoma. The diagnosis was confirmed by immunohistochemical findings (positive for β-hCG).
Source: “Choriocarcinoma -2- very high mag” by Nephron, Wikimedia Commons, licensed under CC BY 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
{kind=link}
Hydatidiform mole
General principles [2]
-
Risk factors
- Prior molar pregnancy
- Age ≤ 15 and ≥ 35 years
- History of miscarriage and infertility
-
Characteristics
- Proliferates within the uterus without myometrial infiltration or hematogenic dissemination
- May undergo malignant transformation to an invasive mole
-
Approach to management [2]
- Initial evaluation
-
β-hCG level measurement (initial test of choice)
- Markedly elevated (higher than expected for the gestational age)
- Higher in complete mole compared to partial mole
- Blood type and antibody screen
- Further laboratory tests: CBC, PT and PTT, renal, thyroid, and liver function tests
- Complete pelvic examination
- Imaging: obtained if β-hCG levels are elevated
- Pelvic ultrasound
- Chest x-ray (performed in individuals with pulmonary symptoms)
-
β-hCG level measurement (initial test of choice)
- Uterine evacuation (both diagnostic and therapeutic) [3]
- Suction dilation and curettage
- Diagnosis is based on histopathological evaluation, karyotype, and the presence of fetal parts.
- Surveillance [2]
-
Monitor β-hCG levels until undetectable, stable, or elevated levels are detected.
- Obtained within 48 hours of uterine evacuation
- Followed every 1–2 weeks while elevated
- Oral contraceptives during β-hCG surveillance period
-
Monitor β-hCG levels until undetectable, stable, or elevated levels are detected.
- Initial evaluation
-
Prognosis [1][4]
- Most patients achieve normal reproductive function after recovery.
- Risk of subsequent GTN is 15–20%
- The recurrence risk of hydatidiform mole in a subsequent pregnancy is 1.8%.
Preeclampsia at < 20 weeks should raise suspicion for GTD.
Complete mole is the result of paternal disomy. Partial mole is the result of triploidy.
Complete mole [2]
-
Etiology
- Fertilization of an empty egg that does not carry any chromosomes by a single sperm
- The (physiological) haploid chromosome set contributed by the sperm is subsequently duplicated.
-
Fetal karyotypes
- 46XX (more common; ∼ 90% of cases)
- 46XY (less common; ∼ 10% of cases)
- 46YY (has never been observed because it is nonviable)
- Pathophysiology: Hydropic degeneration of chorionic villi with concomitant proliferation of cytotrophoblasts and syncytiotrophoblasts → death of the embryo
-
Clinical features
- Vaginal bleeding during the first trimester
- Uterus size greater than normal for gestational age
- Pelvic pressure or pain
- Passage of vesicles with grape-like appearance
-
β-hCG-mediated endocrine conditions
- Theca lutein cysts
- Preeclampsia (before the 20th week of gestation)
- Hyperemesis gravidarum
- Hyperthyroidism: Very high amounts of hCG may lead to hyperthyroidism because the α-subunit of hCG structurally resembles TSH. [5][6]
-
Diagnostics
- See “Approach to management” in “General principles” above.
-
Pelvic ultrasound [2]
- No fetal parts or heartbeat
- Absence of amniotic fluid
- Echogenic mass interspersed with many hypoechogenic cystic spaces representing hydropic villi (referred to “honeycomb”, “bunch of grapes”, or “snowstorm” appearance)
- Ovarian theca lutein cysts (bilateral, large, cystic, adnexal masses)
- Uterine dilation and evacuation (D&E)
- Histopathological examination: diffuse hydropic villi, marked circumferential trophoblastic proliferation [7]
- Immunohistochemical marker: p57-negative
-
Treatment
- Uterine dilation and evacuation (D&E)
- Monitor β-HCG levels: until within reference range (usually 8–12 weeks)
-
Chemotherapy (usually methotrexate) if unresolved, as indicated by either of the following:
- β-HCG values do not decrease.
- Features of malignant GTN on histology or imaging

Partial mole
-
Etiology
- Fertilization of an egg containing a haploid set of chromosomes with two sperms
- A haploid ovum with reduplication of the paternal haploid set from a single sperm
-
Fetal karyotypes
- 69XXY
- 69XXX
- 69XYY (rare)
-
Clinical features
- Vaginal bleeding
- Pelvic tenderness
- No change in uterine size
- β-hCG-mediated endocrine conditions (less common)
-
Diagnostics
- See “Approach to management” in “General principles” above.
-
Pelvic ultrasound
- Fetal parts may be visualized.
- Fetal heartbeat may be detectable.
- Amniotic fluid may be visualized.
- Increased placental thickness
- Multicystic avascular hypoechoic or anechoic spaces (referred to as “Swiss cheese” appearance) [8]
- Uterine dilation and curettage (D&C)
- Histopathological examination: partial occurrence of hydropic villi, minimal trophoblastic proliferation
- Immunohistochemical marker: p57-positive
Fetal parts may be present in partial moles.
Some moles may not produce HCG at all. [9]

Water immersion gross photograph of formalin-fixed hysterectomy specimen with a complete mole
There is an accumulation of small vesicles in the placenta with a typical clusters-of-grapes appearance.
Source: “Complete Hydatidiform Mole” by Ed Uthman, Flickr, licensed under CC BY 2.0.
Ultrasound pelvis (transvaginal) of pregnant patient with abnormally elevated β-hCG level
There is no intrauterine gestation. An intrauterine mass (green outline) contains multiple cystic spaces (examples indicated by red overlay), which correspond to hydropic trophoblastic villi.
This vesicular appearance seen in a molar pregnancy has been described as a “snowstorm pattern”.
Source: “Molar pregnancy” by Mikael Häggström, Wikimedia Commons, licensed under CC0 1.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
Gestational trophoblastic neoplasia
Choriocarcinoma [2]
-
Definition
- A highly malignant GTN characterized by invasive, highly vascular, and anaplastic trophoblastic tissue without villi.
- Has the tendency to metastasize to the lungs, vagina, CNS, liver, pelvis, GI tract, and kidneys
-
Etiology: Choriocarcinoma is preceded by: [2]
- Hydatidiform mole
- Spontaneous abortion or ectopic pregnancy
- Term or preterm gestation
-
Pathophysiology
- Malignant transformation of cytotrophoblastic and syncytiotrophoblastic tissue
- Destructive growth into myometrium without chorionic villi → risk of hemorrhage and early metastasis (lung, vagina, brain, liver)
-
Clinical features: depend on disease extension and metastases location
- Postpartum vaginal bleeding and inadequate uterine regression after delivery
-
Additional symptoms according to the site of metastasis e.g.:
- Dyspnea, cough, or hemoptysis from metastases in the lungs
- Seizures, headaches from metastases in the brain
- Visible vascular lesions from metastases to the vagina
- β-hCG-mediated endocrine conditions (e.g., hyperthyroidism, theca lutein cysts)
-
Diagnostics [10]
- Pelvic examination
- Laboratory tests
- β-HCG levels: very high (initial test of choice)
- Renal, thyroid, and liver function tests
- Imaging
-
Pelvic ultrasound [11]
- Mass of varying appearance (suggestive of hemorrhage and necrosis)
- Hypervascular on color Doppler
- Multiple theca lutein cysts
-
Chest x-ray
- Asses for lung metastases
- “Cannonball metastases” (hematogenous spread → multiple nodules in the lung)
-
Pelvic ultrasound [11]
- Uterine dilation and curettage (D&C): Both diagnostic and therapeutic (but only limited diagnostic value)
- Histopathologic examination: shows anaplastic cytotrophoblasts and syncytiotrophoblasts without chorionic villi
- Immunohistochemical markers: HCG, inhibin, cytokeratin, and Ki-67
-
Treatment [12]
-
Treatment of choice: methotrexate or dactinomycin [13]
- Low-risk : monotherapy with methotrexate or actinomycin D
- High-risk : multiagent chemotherapy consisting of methotrexate, actinomycin D, etoposide, cyclophosphamide, or vincristine
- Surgical treatment (e.g., hysterectomy): may be indicated to stop bleeding from cancerous lesions or to excise distant metastases
- Monitor β-HCG levels for at least 12 months.
-
Treatment of choice: methotrexate or dactinomycin [13]
-
Prognosis [2]
- Risk of recurrence < 1%
- Worse prognosis in the case of advanced-stage disease
Invasive mole [2]
- Definition: a form of GTD characterized by the malignant transformation of an incomplete or complete mole
-
Etiology: The risk of progression to an invasive mole depends on the type of initial hydatidiform mole. [1]
- Complete mole: 15–20% risk of subsequent invasive mole
- Incomplete mole: < 5% risk of subsequent invasive mole
-
Pathophysiology
- Trophoblasts infiltrate the myometrium → increased risk of uterine perforation, intraperitoneal hemorrhage, or infection
- Hematogenic dissemination leads to metastatic growth (including in the brain, lungs, and liver).
-
Clinical features
- Often detected on routine posttreatment surveillance following a hydatidiform mole
- Less likely to cause hemorrhage from a metastatic site than choriocarcinoma
-
Diagnostics
- Laboratory tests: persistently high β-HCG (after evacuation of hydatidiform mole)
- Imaging
- Pelvic ultrasound: poorly defined uterine mass with potential invasion into the myometrium
- Consider chest x-ray if metastasis is suspected.
- Uterine dilation and curettage (D&C): Histopathologic examination shows direct myometrial invasion by abnormal trophoblastic cells with hydropic chorionic villi.
-
Treatment [2]
- See “Treatment” in “Choriocarcinoma” above.
- Predominantly detected at an earlier stage and responsive to monotherapy (with methotrexate or actinomycin D)
-
Prognosis [2]
- Risk of recurrence < 1%
- Evaluate future pregnancies for signs of molar disease
X-ray chest (PA view) of a patient with lung metastases
Multiple pulmonary nodules with circumscribed margins can be seen in both lungs (examples indicated by green overlays). Differential diagnoses include malignant etiologies (metastatic disease, primary lung cancer, lymphoma) and benign etiologies (infection, embolism, autoimmune disease). An old healed fracture of the right clavicle (white arrow) is also visible.
Source: “The appearance of lung metastasis in patient that was reported” by Ghaemmaghami F, Zarchi MK, Early Onset of Metastatic Gestational Trophoblastic Disease after Full-Term Pregnancy, International Journal of Biomedical Science, licensed under CC BY 2.5. Modifications: removed yellow arrow. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
Photomicrograph of testicular tumor specimen (H&E stain; very high magnification)
Cytotrophoblasts are visible throughout the tumor in the form of polygonal-shaped cells with pale cytoplasm, enlarged oval nuclei, and distinct cell borders (examples indicated by arrowheads). Syncytiotrophoblasts are visible as multinucleated cells with eosinophilic cytoplasm (examples indicated by green overlay) surrounding the mononuclear cytotrophoblasts.
These findings are suggestive of choriocarcinoma. The diagnosis was confirmed by immunohistochemical findings (positive for β-hCG).
Source: “Choriocarcinoma -2- very high mag” by Nephron, Wikimedia Commons, licensed under CC BY 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
References
- Soper JT. "Gestational Trophoblastic Disease". Obstetrics & Gynecology. 137(2). :355-370. (2021)
- Ngan HYS, Seckl MJ, Berkowitz RS, et al. "Update on the diagnosis and management of gestational trophoblastic disease". International Journal of Gynecology & Obstetrics. 143. :79-85. (2018)
- Lurain JR. "Gestational trophoblastic disease I: epidemiology, pathology, clinical presentation and diagnosis of gestational trophoblastic disease, and management of hydatidiform mole". Am J Obstet Gynecol. 203(6). :531-539. (2010)
- Sebire NJ, Fisher RA, Foskett M, et al. "Risk of recurrent hydatidiform mole and subsequent pregnancy outcome following complete or partial hydatidiform molar pregnancy". BJOG: An International Journal of Obstetrics and Gynaecology. 110(1). :22-26. (2003)
- Yoshimura M, Hershman JM. "Thyrotropic action of human chorionic gonadotropin". Thyroid. 5(5). :425-434. (1995)
- Cole LA. "Biological functions of hCG and hCG-related molecules". J Endocrinol Reprod. 8(1). :102. (2010)
- "Placenta - Gestational trophoblastic disease - Complete hydatidiform mole". http://www.pathologyoutlines.com/topic/placentacompletemole.html. [2020-08-13]
- Jauniaux E. "Ultrasound diagnosis and follow-up of gestational trophoblastic disease". Ultrasound in Obstetrics and Gynecology. 11(5). :367-377. (1998)
- Nodler JL, Kim KH, Alvarez RD. "Abnormally low hCG in a complete hydatidiform molar pregnancy: The hook effect". Gynecologic Oncology Case Reports. 1(1). :6-7. (2011)
- "Uterine choriocarcinoma". https://radiopaedia.org/articles/uterine-choriocarcinoma
- "Complete Molar Gestation: Role of Ultrasound". https://sonoworld.com/ArticleDetails/Complete_Molar_Gestation__Role_of_Ultrasound.aspx?ArticleId=15
- Berkowitz RS, Goldstein DP, Horowitz NS. "Initial management of high-risk gestational trophoblastic neoplasia". UpToDate. UpToDate. https://www.uptodate.com/contents/initial-management-of-high-risk-gestational-trophoblastic-neoplasia. [2017-04-06]
- Berkowitz RS, Goldstein DP, Horowitz NS. "Initial management of low-risk gestational trophoblastic neoplasia". UpToDate. UpToDate. https://www.uptodate.com/contents/initial-management-of-low-risk-gestational-trophoblastic-neoplasia. [2016-09-12]
- Getrajdman J, Kolev V, Brody E, Chuang L. "Case of maternal and infantile choriocarcinoma following normal pregnancy". Gynecologic Oncology Case Reports. 2(3). :102-104. (2012)