Summary
Renal glomeruli excrete urinary substances and excess water as an ultrafiltrate into the urine by selectively filtering the blood. Any damage to the glomeruli disrupts the filtration process and results in the appearance of blood components (proteins and red blood cells) in the urine. Glomerular damage is commonly caused by immune-mediated processes, which often lead to glomerulonephritis. Non-inflammatory causes, such as metabolic disease (e.g., diabetes, amyloidosis), can also result in significant damage to the glomeruli. The pathophysiology of glomerular diseases is complex; most patients present with either nephritic syndrome (low-level proteinuria, microhematuria, oliguria, and hypertension) or nephrotic syndrome (high-level proteinuria and generalized edema). All glomerular diseases can progress to acute or chronic renal failure. Thus, quick diagnosis and immediate initiation of therapy are required to prevent irreversible kidney damage.
Definitions
Terminology of glomerular diseases
- Primary: a kidney disease specifically affecting the glomeruli (e.g., minimal change glomerulonephritis)
- Secondary: a disease affecting the glomeruli in the context of a systemic disease (e.g., lupus nephritis in SLE) or a disease affecting another organ (e.g., diabetic nephropathy)
- Diffuse: > 50% of glomeruli affected (e.g., diffuse proliferative glomerulonephritis)
- Focal: < 50% of glomeruli affected (e.g., focal segmental glomerulosclerosis)
- Global: entire glomerulus is affected
- Segmental: only part of the glomerulus is affected
- Proliferative: an increased number of cells in the glomerulus
- Membranous: thickening of the glomerular basement membrane (e.g., membranous nephropathy)
- Sclerosing: scarring of the glomerulus
- Necrotizing: cell death within the glomerulus
- Crescentic: accumulation of cells such as macrophages, fibroblasts, and epithelial cells in Bowman space
Pathophysiology
- The glomerular filtration barrier consists of 3 parts
- Initial segment: Fenestrated glomerular capillary endothelium prevents large proteins from passing through.
- Second segment: The glomerular basement membrane (GBM) contains a negative charge produced by heparan sulfate.
- Final segment: Visceral epithelial cells produce/maintain the GBM and contain intercellular junctions created by podocytes that prevent further protein loss.
-
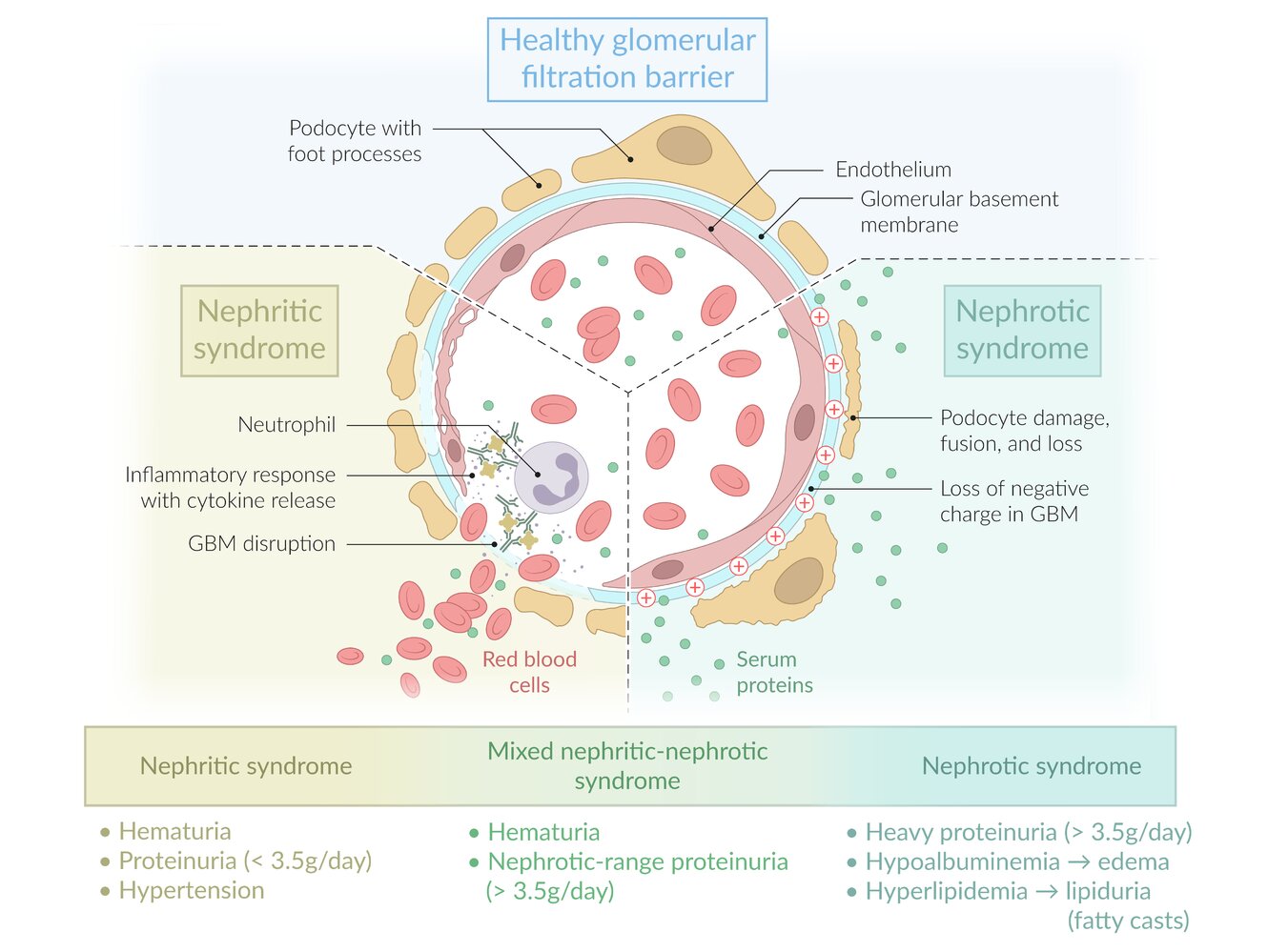
Damage to the glomeruli → disruption of the glomerular filtration barrier → can lead to nephritic or nephrotic syndrome
- See “Pathophysiology” in “Nephritic syndrome.“
- See “Pathophysiology” in “Nephrotic syndrome.“

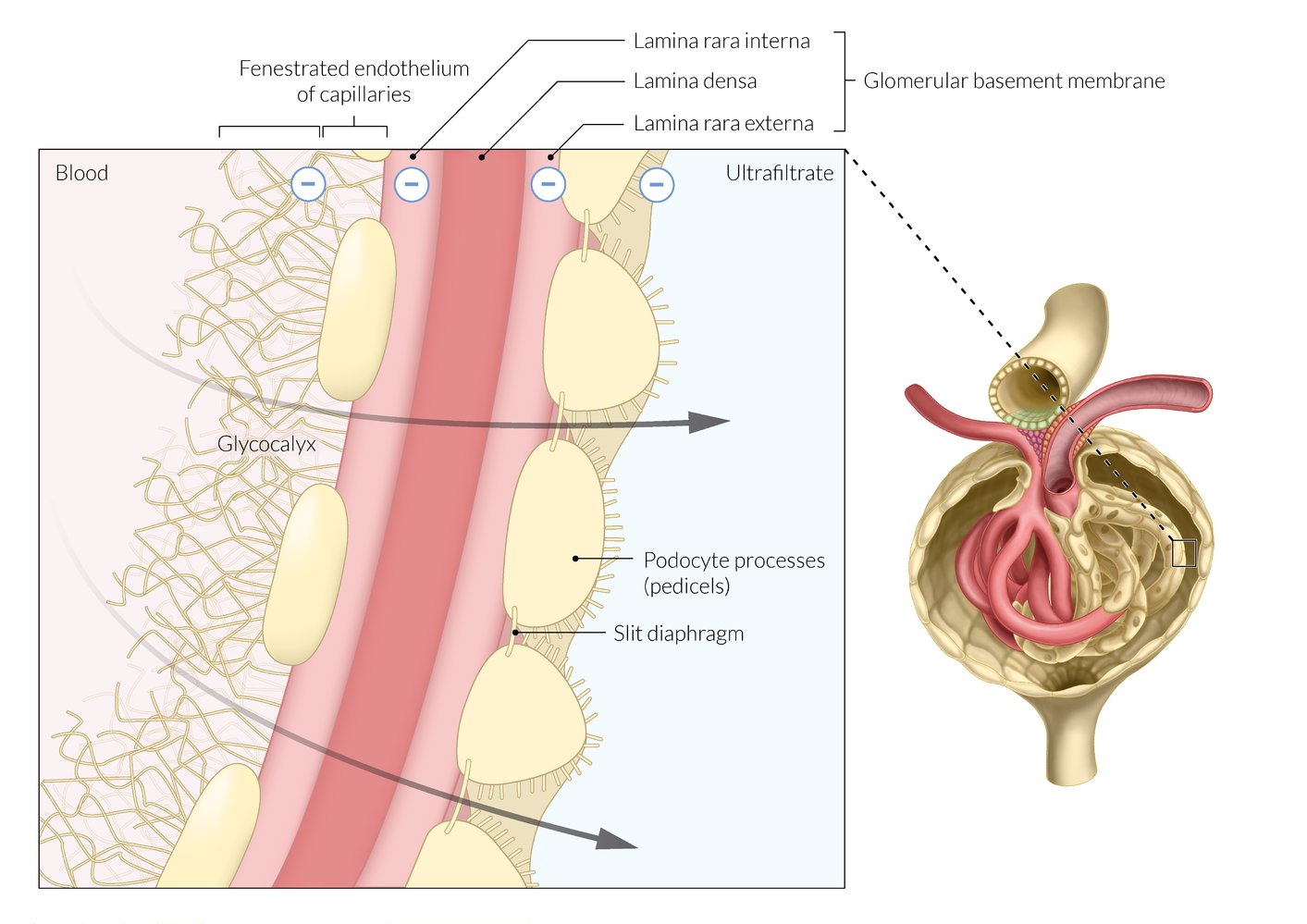
The glomerular filtration barrier filters the blood to form primary urine.
The filtration barrier is composed of three layers: the fenestrated endothelium of capillaries, the glomerular basement membrane, and the podocytes. All three layers selectively allow the passage of particles of a specific size.
Both the podocytes and the negative glycocalyx of the fenestrated endothelium are permeable to neutral and cationic particles.
© AMBOSS
Nephritic-nephrotic syndrome
Nephritic-nephrotic syndrome
- Some diseases that manifest with nephritic syndrome can simultaneously cause nephrotic-range proteinuria (; > 3.5 g/24 h), the main feature of nephrotic syndrome.
- When the criteria for both syndromes are fulfilled, the findings are referred to as mixed nephritic-nephrotic syndrome.
- Most common causes of nephritic-nephrotic syndrome:
- Membranoproliferative glomerulonephritis
- Diffuse proliferative glomerulonephritis
- Classifying the patient's presentation as nephritic, nephrotic, or mixed nephritic-nephrotic can help narrow down the list of likely differential diagnoses.
Nephrotic vs. nephritic syndrome [1][2]
- Nephritic syndrome and nephrotic syndrome are both common clinical manifestations of glomerular diseases.
- Both syndromes are composed of characteristic clinical (e.g., edema, hypertension) and laboratory findings (e.g., glomerular hematuria, massive proteinuria), which result from damage to the glomeruli.
- Glomerular diseases are usually categorized by the syndrome they cause, which is either nephritic or nephrotic.
| Nephritic syndrome | Nephrotic syndrome | |
|---|---|---|
| Presentation |
|
|
| Pathophysiology |
|
|
| Causes |
|
|
All glomerular diseases can lead to acute and chronic kidney failure.

© AMBOSS
Membranoproliferative glomerulonephritis (MPGN)
| Overview of membranoproliferative glomerulonephritis [3][4][5][6] | |||
|---|---|---|---|
| Immunoglobulin-mediated MPGN | Complement-mediated MPGN | ||
| Epidemiology |
|
||
| Definition |
|
||
| Pathophysiology |
|
|
|
| Etiology |
|
|
|
| Clinical features |
|
||
| Laboratory studies |
|
||
| Biopsy findings | LM |
|
|
| EM [3] |
|
||
| Management[6] |
|
||
| LM = light microscopy, EM = electron microscopy | |||
MPGN is characterized by deposition of antibodies and/or complement factors in the mesangium and along capillary walls.

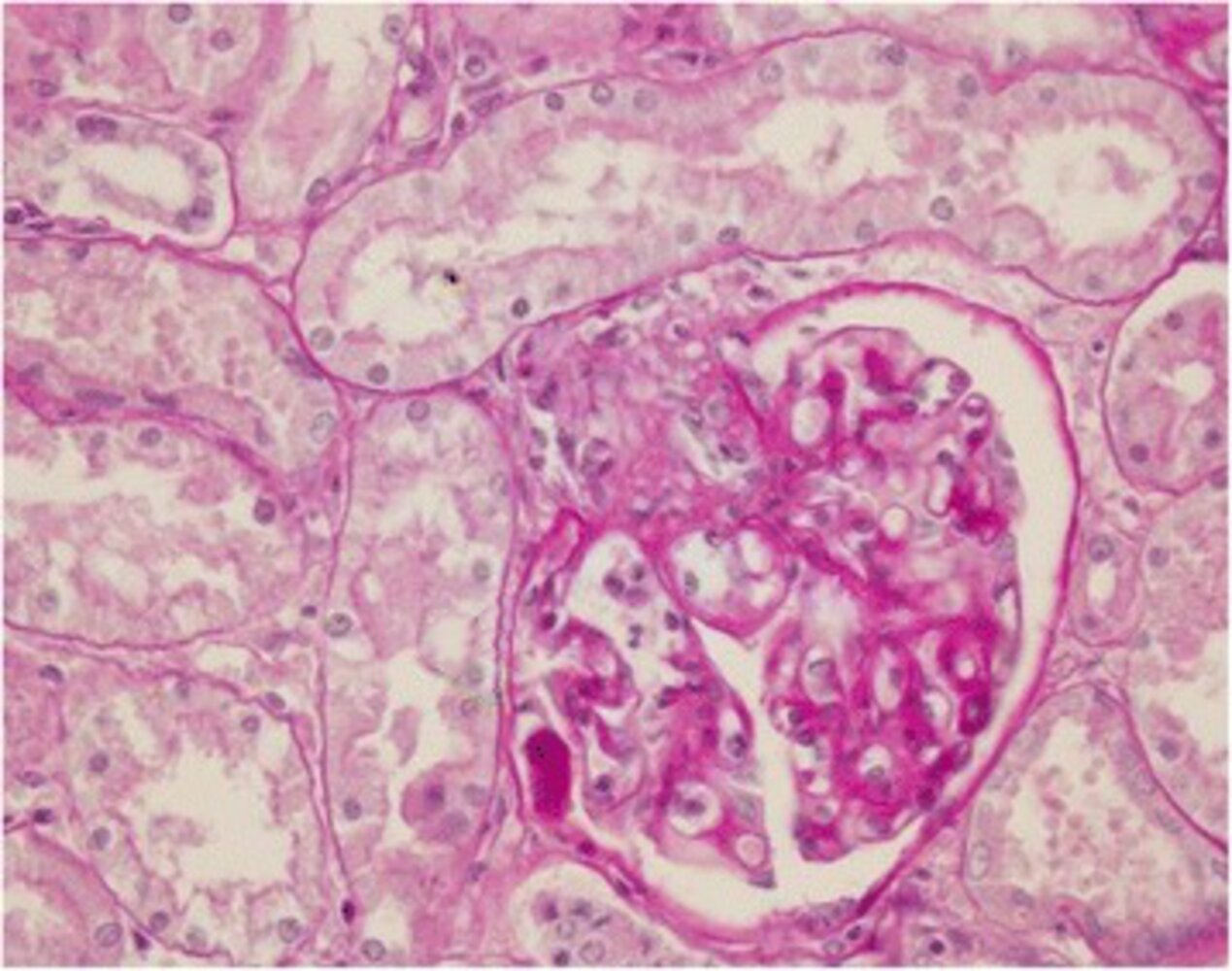
Photomicrograph of a kidney biopsy specimen (PAS stain; high magnification)
The glomerulus shows slightly increased mesangial cellularity (examples indicated by circles) and duplication of the glomerular basement membrane (GBM). The latter displays in the form of a double contour of the GBM (tram-track appearance; examples indicated by yellow lines).
As a secondary finding, there is an Angiostrongylus larva within the glomerulus (blue overlay).
Duplication of the GBM is a typical finding in membranoproliferative glomerulonephritis.
Source: “Figure 8: Kidney” by Laura Rinaldi, Laura Cortese, Leonardo Meomartino et al., BMC Veterinary Research, licensed under CC BY 4.0. Modifications: - arrow removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
Diffuse proliferative glomerulonephritis
-
Definition
- A histopathological pattern of glomerular injury characterized by increased cellularity in > 50% of the glomeruli
- Most common and severe manifestation of lupus nephritis in systemic lupus erythematosus (SLE)
- Also seen in IgA nephropathy and in other inflammatory, autoimmune, and infectious diseases
-
Clinical features
- Nephritic syndrome
- Nephritic-nephrotic syndrome (i.e., nephritic with nephrotic-range proteinuria)
- Can lead to immune complex-mediated RPGN
-
Diagnostics
-
Laboratory studies
- ↓ Serum C3 complement levels
- In lupus nephritis: positive ANA, anti-dsDNA antibodies
- Microscopy
-
LM
- Thickening of glomerular capillaries (resembling wire loops)
- Characterized by increased cellularity in more than half of the glomeruli
- IM: granular appearance
-
EM
- More commonly: subendothelial immune deposits (IgG immune complexes, C3, and C1q)
- Less commonly: subepithelial or intramembranous deposits
-
LM
-
Laboratory studies
- Management: depends on underlying cause

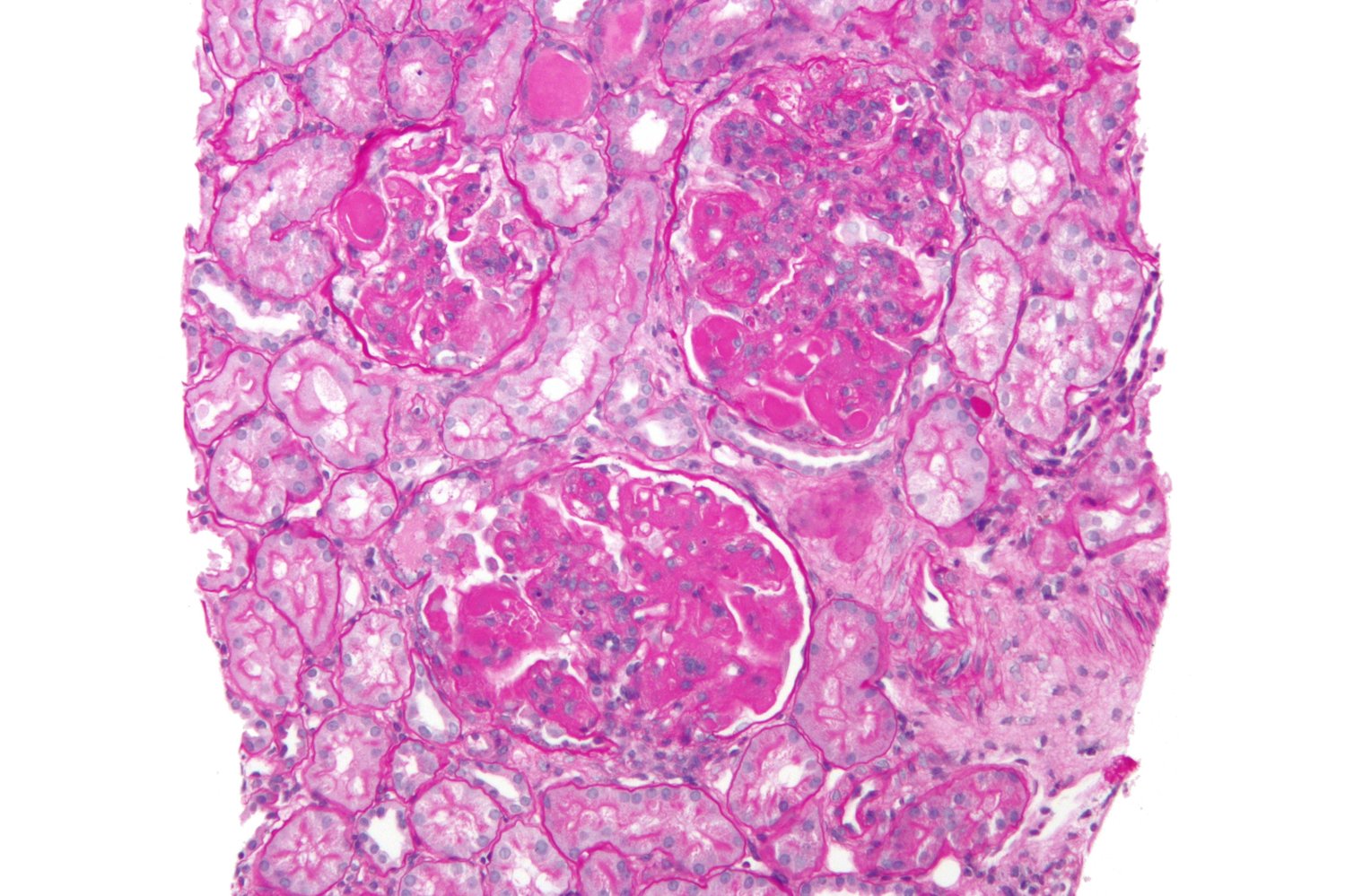
Photomicrograph of a renal cortex biopsy specimen (PAS stain; 250x magnification)
Sections of numerous tubules and vessels and three centrally located renal glomeruli (blue outlines) are visible. The latter show a partially increased mesangial cell density (examples indicated by black outlines), thickened capillary loops (due to subepithelial immune complex deposits; examples indicated by blue overlay), extracapillary epithelial proliferation (examples indicated by yellow overlay), and diffuse glomerulosclerosis (examples indicated by arrowheads).
These findings are characteristic of diffuse proliferative glomerulonephritis, the most common form of lupus nephritis, in which more than half of the glomeruli are affected.
Source: “Diffuse proliferative lupus nephritis” by Michael Bonert ("Nephron"), Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
Inherited glomerular disorders
| Overview of inherited glomerular disorders | |||
|---|---|---|---|
| Alport syndrome[7] | Thin basement membrane disease (benign familial hematuria) [8] | ||
| Epidemiology |
|
|
|
| Pathophysiology |
|
|
|
| Distinguishing features |
|
|
|
| Laboratory studies |
|
|
|
| Renal biopsy | LM |
|
|
| IM |
|
|
|
| EM |
|
|
|
| Management |
|
|
|
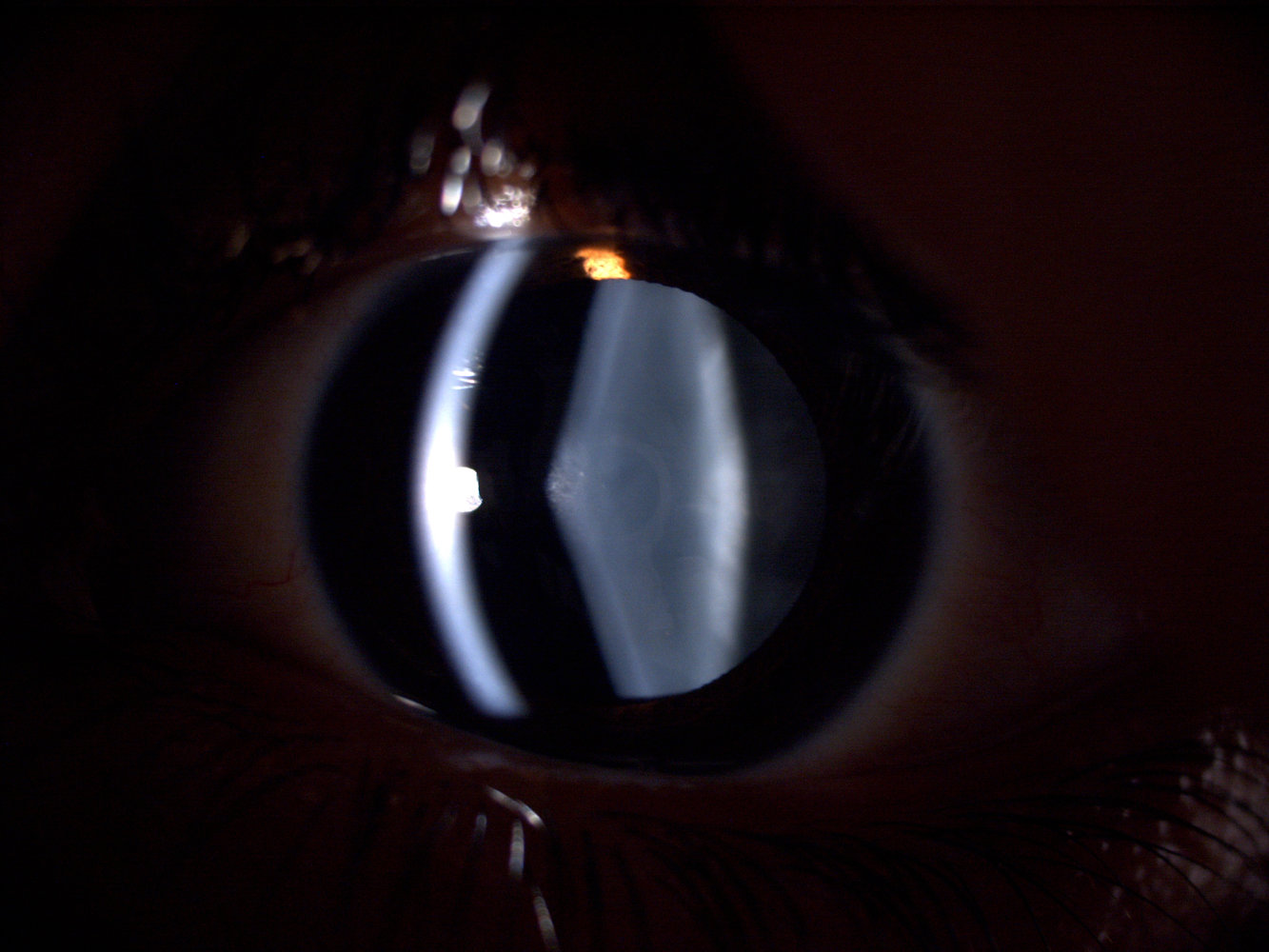
Slit-lamp photograph of the right eye (mydriatic pupil)
The light of the slit-lamp produces an optical cross section of the cornea (left optical cross section) and the lens (right optical cross section). Compared to the cornea, the anterior surface of the lens appears conical (normal physiological shape is indicated by the dashed line).
This protrusion of the anterior cortex of the lens is referred to as “anterior lenticonus” and it is associated with Alport syndrome.
Source: “Figure 1. in: Clear lens phacoemulsification in the anterior lenticonus due to Alport Syndrome: two case reports” by Ghassem Amir Aslanzadeh, Davoud Gharabaghi & Niloofar Naderi, Journal of Medical Case Reports, BioMed Central, licensed under CC BY 2.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
References
- Goldman L, Schafer AI. "Goldman-Cecil Medicine, 25th Edition". Elsevier. (2016). ISBN: 9781455750177
- Longo D, Fauci A, Kasper D, et al. "Harrisons's Principles of Internal Medicine, 18th Edition, 2011". McGraw-Hill Medical. (2011). ISBN: 9780071748896
- Sethi S, Fervenza FC. "Membranoproliferative Glomerulonephritis — A New Look at an Old Entity". N Engl J Med. 366(12). :1119-1131. (2012)
- Bassam Alchi and David Jayne. "Membranoproliferative glomerulonephritis". Pediatric Nephrology. (2010)
- Gilbert SJ, Weiner DE, Bomback AS, Perazella MA, Rifkin DE. "National Kidney Foundation's Primer on Kidney Diseases". Elsevier. (2022). ISBN: 9780323791229
- Rovin BH, Adler SG, Barratt J, et al. "KDIGO 2021 Clinical Practice Guideline for the Management of Glomerular Diseases". Kidney Int. 100(4). :S1-S276. (2021)
- Kashtan CE. "Alport Syndrome: Achieving Early Diagnosis and Treatment". Am J Kidney Dis. 77(2). :272-279. (2021)
- Tryggvason K, Patrakka J. "Thin Basement Membrane Nephropathy". Journal of the American Society of Nephrology. 17(3). :813-822. (2006)
- Judy Savige, Deb Colville, Frances Flinter. "Alport Syndrome in Women and Girls". Clinical Journal of the American Society of Nephrology. (2016)
- Dische FE, Anderson VE, Keane SJ, et al. "Incidence of thin membrane nephropathy: morphometric investigation of a population sample.". J Clin Pathol. 43(6). :457-60. (1990)
- Goljan EF. "Rapid Review Pathology". Elsevier Saunders. (2013). ISBN: 9780323087872