Summary
Glucose-6-phosphate dehydrogenase (G6PD) deficiency leads to an impaired regeneration of reduced glutathione, an important antioxidant, which makes RBCs more susceptible to oxidative stress and can result in episodic hemolytic anemia. The condition is inherited in an X-linked recessive pattern and is the most common human enzyme deficiency worldwide. It primarily affects males of African, Asian, and Mediterranean descent. G6PD deficiency is usually asymptomatic, but a sudden surge in oxidative stress (e.g., after infection, consumption of fava beans, or various drugs) may lead to a life-threatening hemolytic crisis. Diagnostic findings include signs of intravascular hemolysis (e.g., normocytic anemia, ↑ LDH, and ↓ haptoglobin), Heinz bodies, and bite cells on blood smear. Management mainly consists of preventing hemolysis by avoiding triggers.
 deficiency fact sheet")
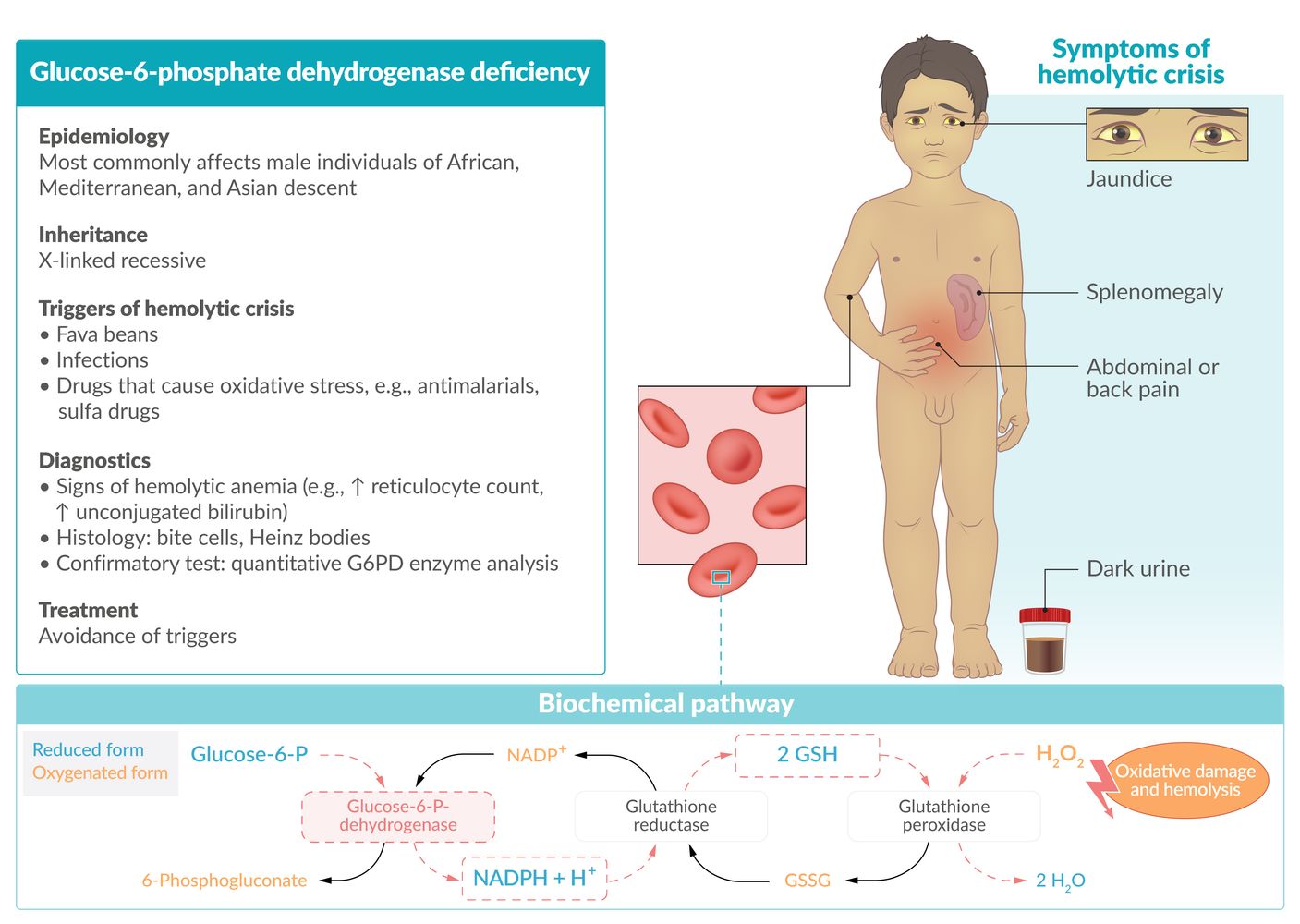
Glucose-6-phosphate dehydrogenase is the rate-limiting enzyme of the pentose phosphate pathway and oxidizes glucose-6-P to 6-phosphogluconate while reducing NADP to NADPH. NADPH is essential for converting oxidized glutathione back to its reduced form (GSH). The reduced glutathione is capable of neutralizing reactive oxygen species (e.g., hydrogen peroxide) and free radicals, thereby protecting red blood cells from oxidative damage.
In G6PD deficiency, glutathione cannot be reduced and erythrocytes become susceptible to oxidative stress, resulting in damage to the erythrocyte membrane, and thus intravascular and extravascular hemolysis.
© AMBOSS
Epidemiology
- G6PD deficiency is the most common human enzyme deficiency.
- Prevalence: ∼ 400 million worldwide [1]
- Affects primarily males of African, Mediterranean, and Asian descent [2]
Epidemiological data refers to the US, unless otherwise specified.
Pathophysiology
- X-linked recessive inheritance
- G6PD is the rate-limiting enzyme of the pentose phosphate pathway (also known as the hexose monophosphate shunt). This pathway yields NADPH, which is essential for converting oxidized glutathione back to its reduced form. Reduced glutathione is capable of neutralizing reactive oxygen species (ROS) and free radicals and therefore protecting RBCs from oxidative damage.
- In the absence of reduced glutathione (e.g., due to G6PD deficiency), RBCs become susceptible to oxidative stress that can damage erythrocyte membranes, resulting in intravascular and extravascular hemolysis.
-
Causes of increased oxidative stress are triggers of hemolytic crisis and include:
- Fava beans
- Drugs: antimalarial drugs (e.g., chloroquine, primaquine), sulfa drugs (e.g., trimethoprim-sulfamethoxazole), nitrofurantoin, isoniazid, dapsone, NSAIDs, ciprofloxacin, chloramphenicol
- Bacterial and viral infections (most common cause): Severe enzymatic deficiency can inhibit respiratory burst activity due to reduced NADPH production in phagocytes.
- Inflammation: During an inflammatory reaction free radicals are produced and can diffuse into RBCs.
- Metabolic acidosis

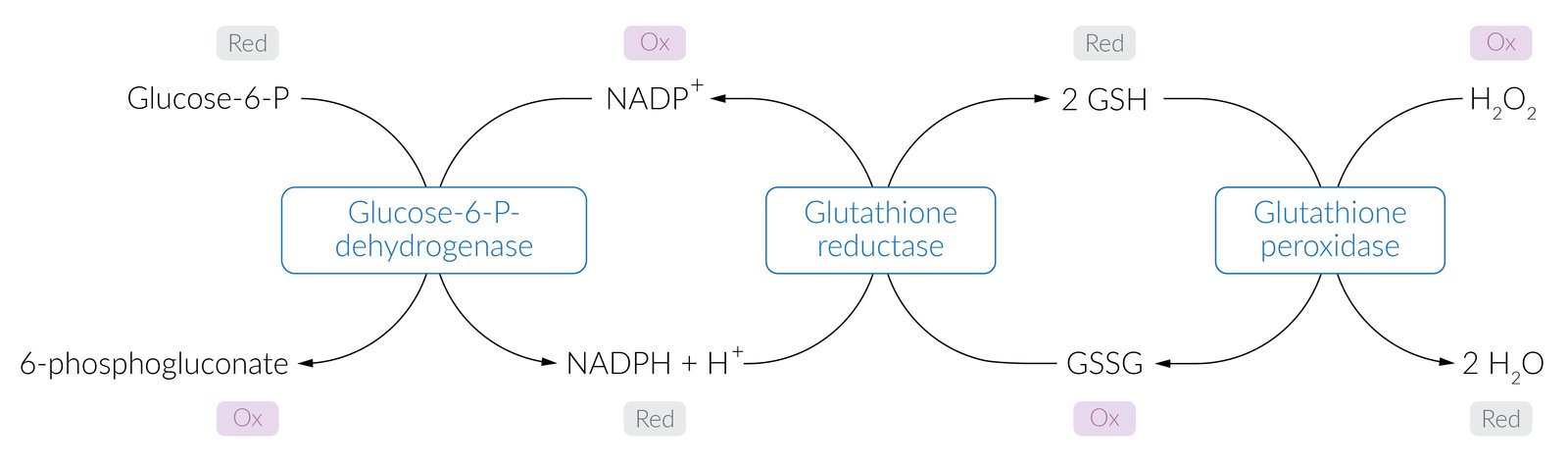
In its reduced form (GSH), glutathione detoxifies free radicals and peroxides (here hydrogen peroxide, H2O2, on the right). This reaction is catalyzed by the glutathione peroxidase and results in oxidized glutathione (GSSG) and water (H2O). To convert the GSSG back to GSH, the catalyzing enzyme glutathione reductase requires NADPH (nicotinamide adenine dinucleotide phosphate hydrogen). One possible pathway that yields NADPH for reductive reactions is the pentose phosphate pathway (hexose monophosphate shunt). The enzyme glucose-6-P-dehydrogenase (G6PD) oxidizes glucose-6-P to 6-phosphogluconate and reduces NADP to NADPH.
The reduced glutathione is particularly important for protecting RBCs from oxidative damage. In its absence (e.g., due to G6PD deficiency), RBCs become susceptible to oxidative stress, resulting in hemolytic anemia.
© AMBOSS
Clinical features
- Most patients are asymptomatic.
-
Recurring hemolytic crises may occur, especially following triggers
- Arise within 2–3 days after increased oxidative stress [3]
- Sudden onset of back or abdominal pain
- Jaundice
- Dark urine
- Transient splenomegaly
- Recurrent severe infections causing symptoms of chronic granulomatous disease
Diagnosis
-
Blood smear
- Heinz bodies: Oxidative stress causes hemoglobin denaturation. Hemoglobin then precipitates as small inclusions within the erythrocytes.
- Bite cells: due to macrophages selectively removing the denatured hemoglobin inclusions of RBCs
-
Signs of intravascular hemolysis
- Normocytic anemia
- ↑ Reticulocyte count
- ↑ Unconjugated bilirubin
- ↑ LDH
- ↓ Haptoglobin
- Hemoglobinuria [2]
-
Screening test: fluorescent spot test
- Add glucose-6-phosphate and NADP → measure NADPH fluorescence
- Normal G6PD activity produces fluorescent NADPH out of NADP, while in G6PD deficiency a lack of fluorescence is seen.
- Semi-quantitative
- Confirmatory test: : quantitative G6PD enzyme analysis
Ideally, both the screening and confirmatory tests should be performed during remission.
Stress makes me want to bite into some Heinz ketchup: ↑ Oxidative stress in patients with G6PD deficiency may lead to the detection of Heinz bodies and bite cells on the peripheral blood smear.


 deficiency")
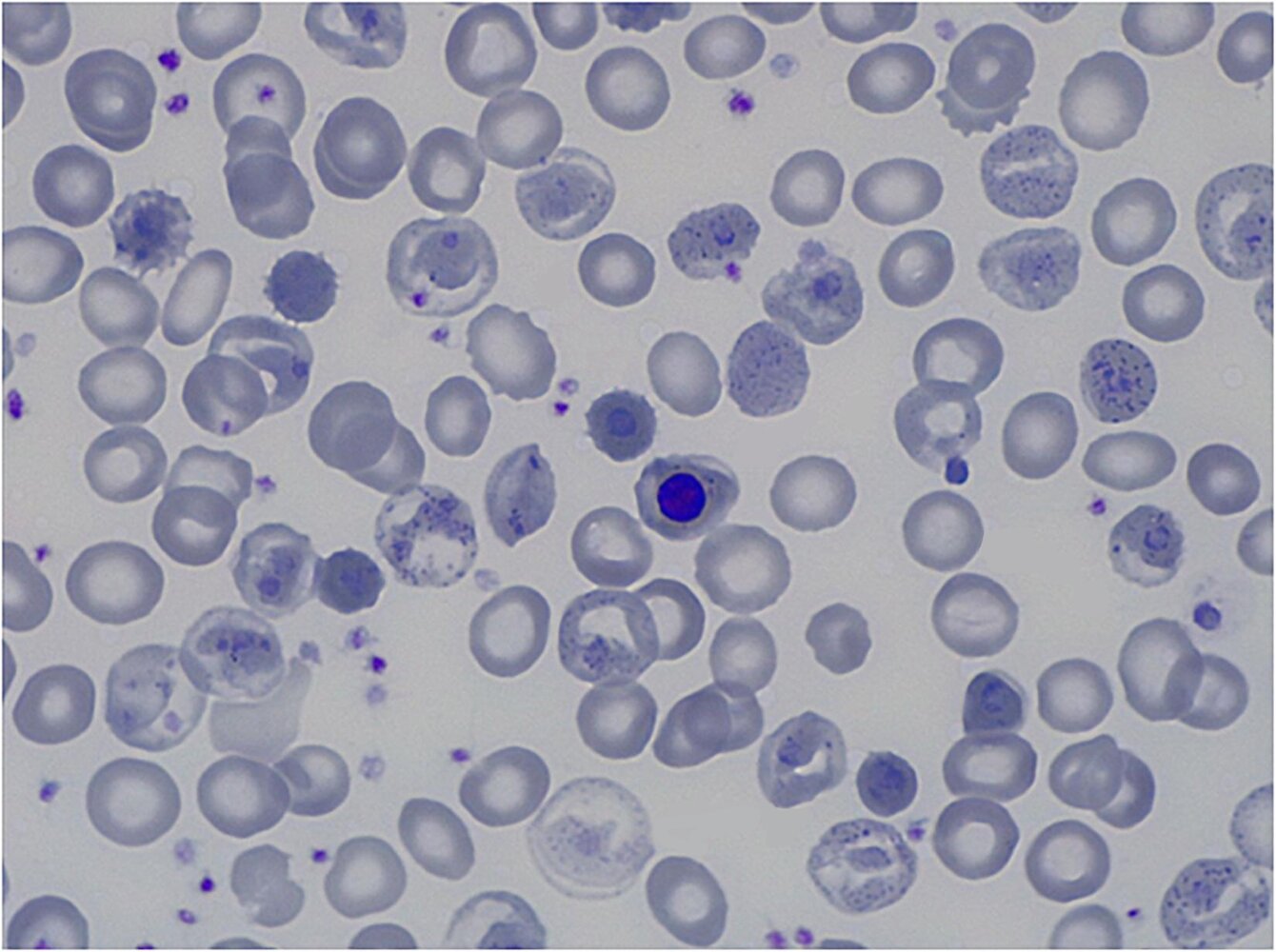
Photomicrograph of a peripheral blood smear (new methylene blue stain; high magnification)
Multiple erythrocytes are visible, some of which contain small, round inclusions (examples indicated by arrowheads) called Heinz bodies. Heinz bodies are composed of denatured hemoglobin and are typically associated with G6PD deficiency but are also seen in other conditions.
Source: “Fig 1, In: Usefulness of NGS for Diagnosis of Dominant Beta-Thalassemia and Unstable Hemoglobinopathies in Five Clinical Cases” by Rizzuto V, Koopmann TT, Blanco-Álvarez A et al., Frontiers in Physiology, licensed under CC BY 4.0. Modifications: removal of four arrows and the letters a, b, c, d. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
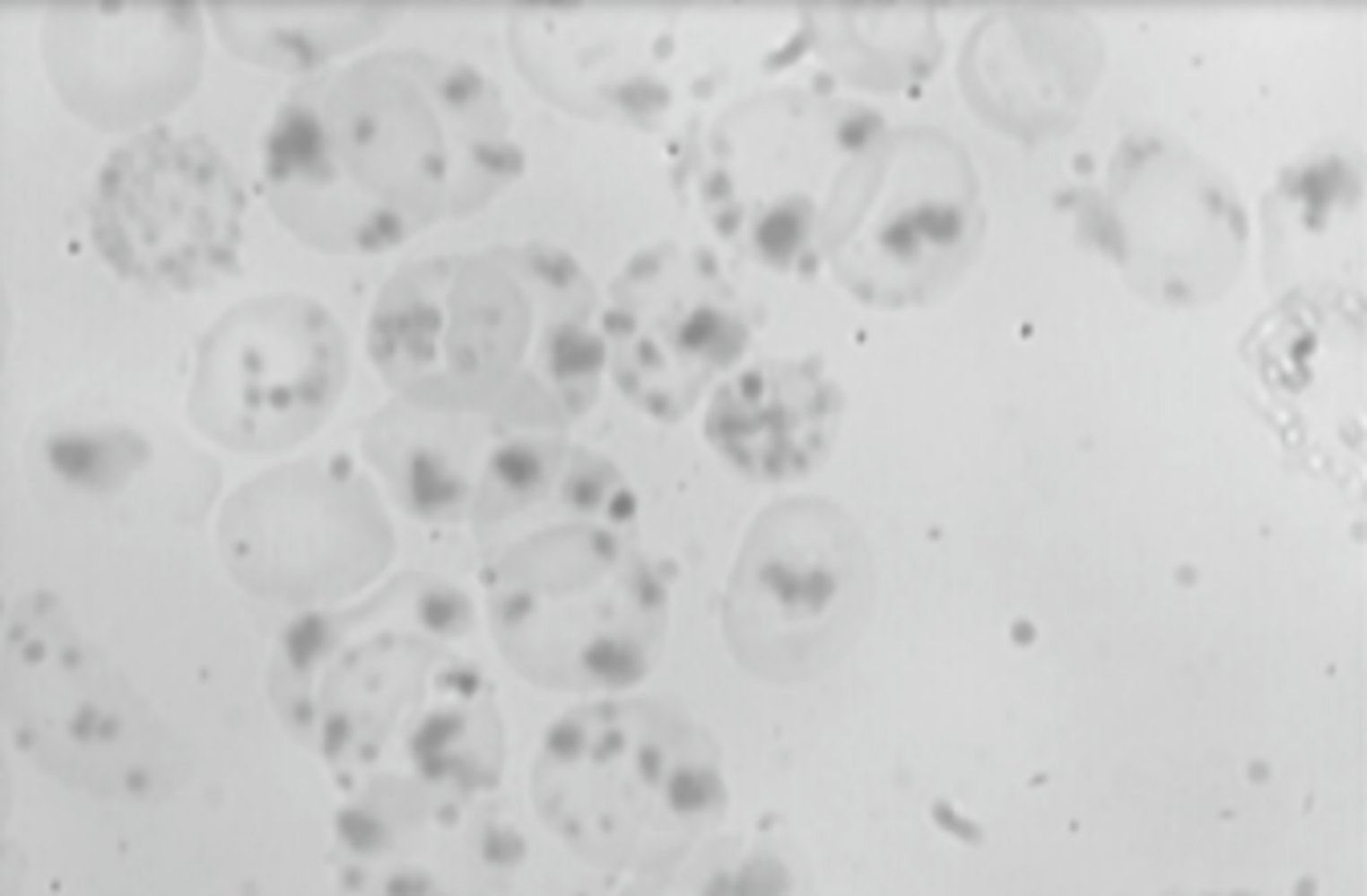
Photomicrograph of a peripheral blood smear
Numerous erythrocytes are visible. They contain dense aggregates of denatured hemoglobin (Heinz bodies; examples indicated by green overlay), which appear as dark spots.
Heinz bodies are found in a number of hematological disorders, most commonly in glucose-6-phosphate dehydrogenase deficiency.
Source: “Figure 1 (b): Peripheral blood smear depicting abundant Heinz bodies in our patient with hemoglobin H disease” by Panagiotis Andreadis, Stamatia Theodoridou, Marily Pasakiotou et al., Case Reports in Hematology Journal, licensed under CC BY 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
Photomicrograph of a peripheral blood smear (Wright-Giemsa stain; 600× magnification)
Multiple erythrocytes are visible, some of which have an abnormally shaped membrane due to macrophage-mediated removal of denatured hemoglobin that precipitated at the cell membrane (examples outlined in green). They appear smaller, denser, and more contracted than normal erythrocytes (example outlined in red).
These abnormally formed cells are called “bite cells” and result from oxidative hemolysis, which is seen in G6PD deficiency.
Source: “Fig 7, In: Anemias raras y fallos medulares hereditarios” by Vives Corrons J, Mañú Pereira MM, Trujillo JP, Surrallés J, Sevilla J, Arbor, licensed under CC BY 4.0. Modifications: overlay created. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
Treatment
- Avoid triggers (see “Pathophysiology” above)
- Blood transfusions should be performed only in rare, severe cases.
Miscellaneous
- Selective advantage in areas of endemic malaria: : As with sickle cell anemia, carriers of the G6PD deficiency may be less severely affected by malaria, especially if the disease is caused by Plasmodium falciparum. [4]
References
- Cappellini MD, Fiorelli G. "Glucose-6-phosphate dehydrogenase deficiency". Lancet. 371(9606). :64-74. (2008)
- Frank JE. "Diagnosis and management of G6PD deficiency". Am Fam Physician. 72(7). :1277-1282. (2005)
- "Glucose-6-Phosphate Dehydrogenase Deficiency". https://rarediseases.org/rare-diseases/glucose-6-phosphate-dehydrogenase-deficiency/. [2017-01-17]
- Roth EF, Ruprecht RM, Schulman S, Vanderberg J, Olson JA. "Ribose metabolism and nucleic acid synthesis in normal and glucose-6-phosphate dehydrogenase-deficient human erythrocytes infected with Plasmodium falciparum". J Clin Invest. 77(4). :1129-1135. (1986)
- Longmore M, Wilkinson IB, Davidson EH, Foulkes A, Mafi AR. "Oxford Handbook of Clinical Medicine (2010)". OUP Oxford. (2010). ISBN: 341114
- Dietel M, Suttorp N, Zeitz M, et al. "Harrisons Innere Medizin (2 Bände)". ABW Wissenschaftsverlagsgesellschaft (2005). (2005). ISBN: 9783936072297