Summary
Goiter is any abnormal enlargement of the thyroid gland. The condition has various causes, with the most common worldwide being iodine deficiency. In the US, however, Hashimoto's and Graves' disease are more common etiologies. Goiters can be classified based on their morphology, function, or dignity (benign or malignant). Symptoms depend on etiology and are often absent. However, patients may present with hyperthyroidism or hypothyroidism. Large goiters may also cause obstructive symptoms due to compression of the trachea and/or the esophagus. Diagnosis is established based on clinical examination, laboratory tests, and imaging techniques. Management depends on the underlying condition and may include administering iodine (for treating nontoxic euthyroid goiter) or performing surgery (e.g., for treating local compression or thyroid cancers).
Epidemiology
- Sex: ♀ > ♂ (4:1)
- Frequency: decreases with age
Epidemiological data refers to the US, unless otherwise specified.
Etiology
- Iodine deficiency (leading cause of goiter worldwide)
- Inflammation (e.g., Hashimoto thyroiditis, subacute granulomatous thyroiditis)
- Graves disease
- Thyroid cysts (e.g., thyroglossal cyst)
- Thyroid adenomas
- Thyroid carcinomas
- Ingestion of goitrogens (e.g., lithium carbonate)
- Elevated TSH production (e.g., pituitary adenoma, paraneoplastic syndrome)
- Congenital goiter
Classification
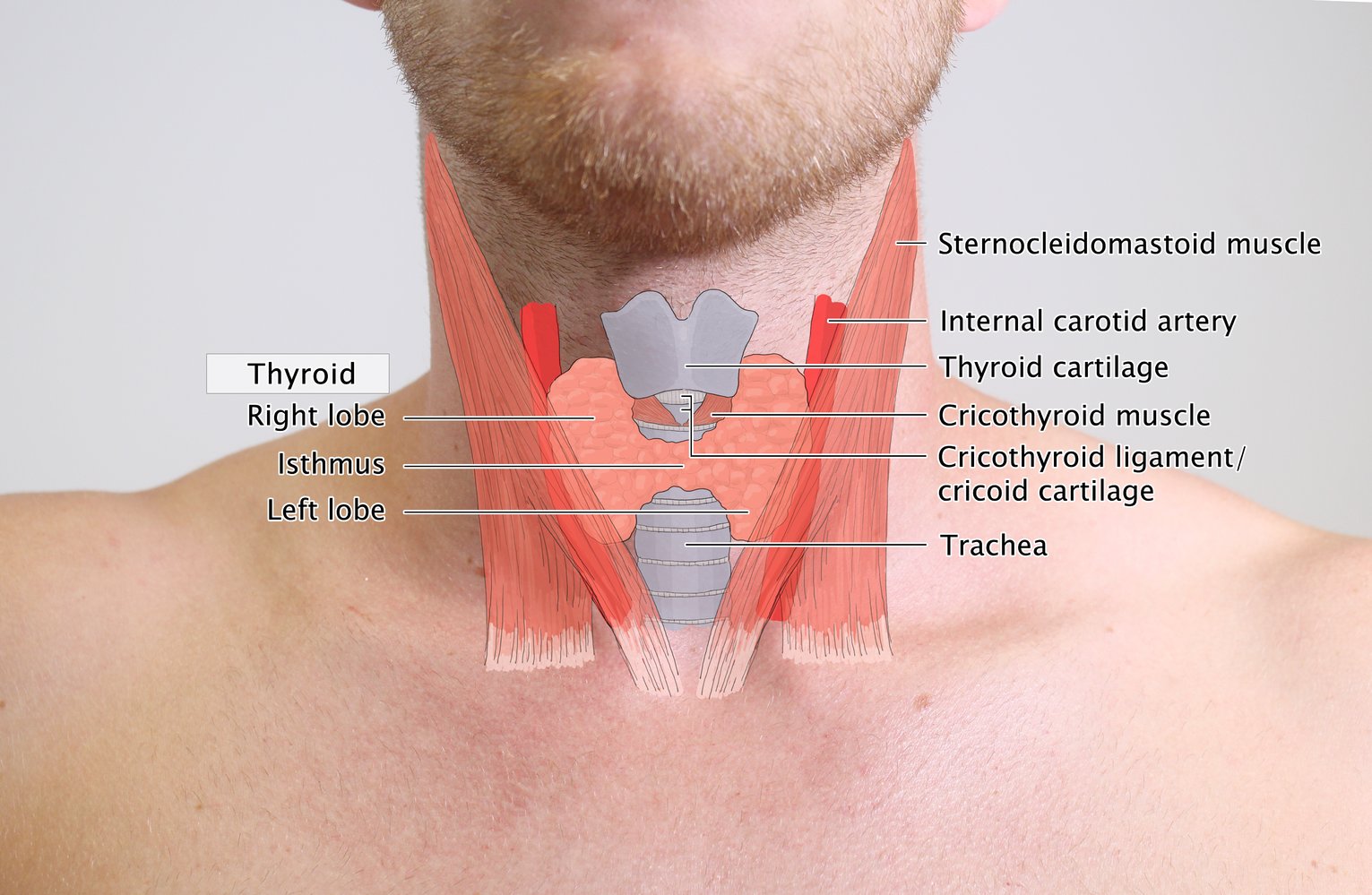
Thyroid gland versus goiter
-
Normal adult thyroid gland
- Weight: ∼ 20–30 g
- Volume: ∼ 7–10 mL
- Location: caudal to larynx surrounding the anterolateral part of the trachea
-
Goiter
- Enlarged volume of thyroid gland
- Goiters can be differentiated based on
- Morphology (growth pattern, size)
- Thyroid function
- Benignity/malignancy

Morphology
-
Growth pattern of goiter
-
Diffuse goiter: diffusely enlarged thyroid
- Graves disease
- Inflammation (e.g., Hashimoto thyroiditis)
- TSH-secreting pituitary adenoma
- Iodine deficiency
-
Nodular goiter: irregular enlarged thyroid due to nodule formation
- Uninodular goiter (e.g., cysts, adenoma, cancer)
- Toxic and nontoxic multinodular goiter
-
Diffuse goiter: diffusely enlarged thyroid
- Goiter size: see ”Classification of goiter by palpation” below.
Thyroid function of goiter
-
Nontoxic goiter: normal TSH, fT3, and fT4 levels
- E.g., Iodine deficiency
-
Toxic goiter: increased thyroid hormone production
- E.g., Graves disease, toxic multinodular goiter
-
Hypothyroid goiter: decreased thyroid hormone production
- E.g., Hashimoto's disease, congenital hypothyroid goiter
Dignity of goiter
- Malignant goiter: e.g., thyroid carcinoma
- Benign (bland) goiter: benign thyroid enlargement
References:[1][2]
© AMBOSS
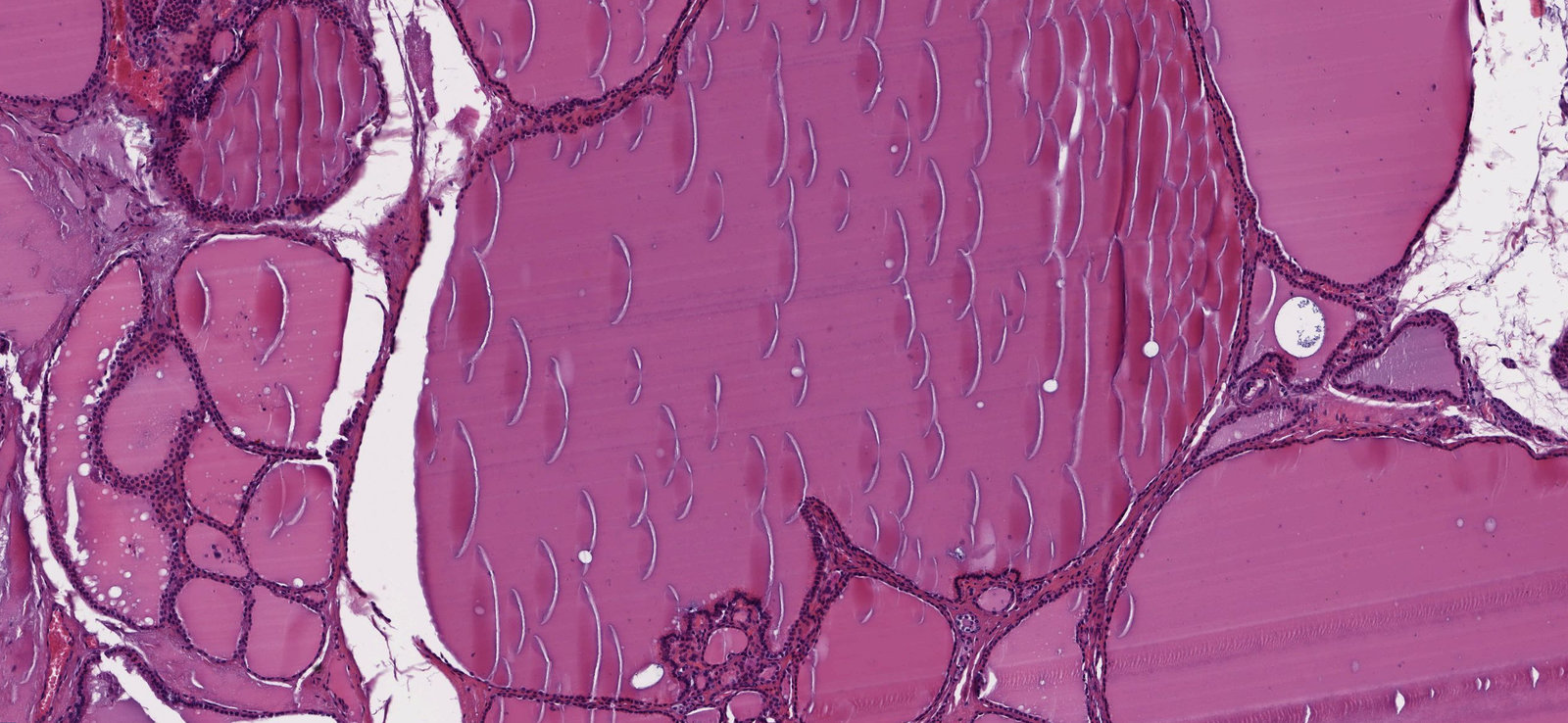
Photomicrograph of thyroid tissue (H&E stain, 250x magnification)
Green overlay: enlarged thyroid follicle
White overlay: small follicles
Black arrowheads: preparation artifacts in thyroid colloid
Click on the Smartzoom button to view the entire specimen through a virtual microscope.
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: PD Dr. med. Alberto Perez Bouza, Facharzt für Pathologie
Clinical features
- Patients are commonly asymptomatic.
- Altered hormone metabolism may occur
- Symptoms of hyperthyroidism
- Symptoms of hypothyroidism
- Obstructive symptoms
- Compression of the trachea → exertional dyspnea and, in severe cases, stridor or wheezing
- Compression of the esophagus → dysphagia
- Potentially:
- Lymph node enlargement (e.g., cervical lymph nodes) in malignant infiltration
- Pemberton sign: a physical examination finding in patients with goiter (bilateral arm elevation results in facial plethora due to an obstructed thoracic inlet that increases venous pressure)
Diagnosis
- Best initial step: palpation of thyroid gland (see “Classification of goiter by palpation” below)
-
Laboratory tests
- Initial workup: TSH levels
- Possible screen for thyroid antibodies (see thyroid antibodies)
- If medullary carcinoma is suspected, check calcitonin levels (see thyroid cancer).
-
Imaging: determination of goiter size, nodularity, and consistency
- Ultrasound
- Further evaluation may include: CT, MRI
-
Interventions
- Depend on the suspected pathology
- Fine-needle biopsy for cytology
Classification of goiter by palpation
According to the World Health Organization (WHO) classification:
- Grade 0: no goiter is palpable or visible.
- Grade 1: palpable goiter, not visible when neck is held in normal position
- Grade 2: a clearly swollen neck (also visible in normal position of the neck) that is consistent with a goiter on palpation


References:[3]

The neck is asymmetrical and the thyroid gland is enlarged. The green hatched overlay represents the normal size of a thyroid; the light green overlay is the estimated size of this patient's thyroid.
© AMBOSS

© AMBOSS
Treatment
-
Nontoxic goiter
- Treatment is not needed if the patient is asymptomatic.
- Schedule follow-ups for possible dysfunctional thyroid and/or obstructive symptoms.
-
Large goiter (> 80 mL)
- Surgery is preferred to avoid complications (e.g., obstructive symptoms).
- Alternatively, radioiodine therapy
- Iodine deficiency: iodine supplementation
- In other cases, goiter treatment varies depending on the exact etiology (see “Etiology” above).
References
- Lewinski A. "The problem of goitre with particular consideration of goitre resulting from iodine deficiency (I): classification, diagnostics and treatment". Neuro Endocrinol Lett. 23(4). :351-355. (2002)
- Pankow BG, Michalak J, McGee MK. "Adult human thyroid weight.". Health Phys. 49(6). :1097-103. (1985)
- Gómez JM, Maravall FJ, Gómez N, Gumà A, Soler J. "Determinants of thyroid volume as measured by ultrasonography in healthy adults randomly selected.". Clin Endocrinol (Oxf). 53(5). :629-34. (2000)