Summary
Gout is an inflammatory crystal arthropathy caused by the precipitation and deposition of uric acid crystals in synovial fluid and tissues. Decreased renal excretion and/or increased production of uric acid leads to hyperuricemia, which is commonly asymptomatic but also predisposes to gout. Acute gout flares typically manifest with a severely painful big toe (podagra) and occur most often in men following triggers such as alcohol consumption. Diagnosis is based on clinical presentation and, ideally, by the demonstration of negatively birefringent monosodium urate (MSU) crystals on synovial fluid analysis. Acute attacks are treated with corticosteroids, NSAIDs (e.g., naproxen, indomethacin), or colchicine. The management of chronic gout includes lifestyle modifications and urate-lowering medications (e.g., allopurinol) to control hyperuricemia.
Acute calcium pyrophosphate crystal deposition (CPPD) disease, sometimes referred to as pseudogout, is another crystal arthropathy that resembles an acute gout flare and is managed similarly. It is covered in detail in a separate article.


© AMBOSS
Epidemiology
- Sex: : ♂ > ♀ (3:1) [1]
- Age of onset: 2 peaks of incidence (at 30–39 years and at 60 years of age) [2]
- Prevalence: ∼ 8 million people in the US [1]
Epidemiological data refers to the US, unless otherwise specified.
Etiology
Hyperuricemia
- Can be idiopathic (primary hyperuricemia) or secondary to insufficient excretion or increased production of purines
- Predisposes to gout and acute gout attacks
- Not obligatory for developing gout
Primary hyperuricemia
- Idiopathic extracellular supersaturation of uric acid
- No history of comorbidities or medications that affect uric acid formation or excretion [3]
Primary hyperuricemia can be aggravated by poor dietary habits.
Secondary hyperuricemia [4]
-
Decreased uric acid excretion: most common cause
- Medications (e.g., pyrazinamide, aspirin, loop diuretics, thiazides, niacin)
- Chronic renal insufficiency, lead nephropathy [5]
- Ketoacidosis (due to, e.g., starvation; , diabetes mellitus) and lactic acidosis
- Postmenopause
-
Increased uric acid production
-
High cell turnover, e.g.:
- Tumor lysis syndrome
- Hemolytic anemia [6]
- Psoriasis
- Myeloproliferative neoplasms
- Chemotherapy, radiation
-
Enzyme defects, e.g.: [5]
- Lesch-Nyhan syndrome
- Phosphoribosyl pyrophosphate synthetase overactivity
- von Gierke disease
- Diet rich in protein and especially purine (e.g., red meat, seafood)
- Obesity
- Hypercholesterolemia, hypertriglyceridemia
- Hypertension [7]
- Sleep apnea [8][9]
-
High cell turnover, e.g.:
-
Combined decreased excretion and overproduction: high alcohol consumption
- Organic acids from alcohol metabolism compete with uric acid to be excreted by the kidneys.
- Many alcoholic beverages contain a high level of purines.
Imagine drugs associated with gout: AS a Guy painfully walking THe NIce PYRamid LOOP trail: aspirin, thiazides, niacin, pyrazinamide, loop diuretics.
Pathophysiology
-
Gout
- An inflammatory crystal arthropathy that is caused by the precipitation and deposition of uric acid crystals in synovial fluid and tissues.
- It is typically associated with hyperuricemia, but can also occur if uric acid levels are normal.
-
Uric acid
- An end-product of purine metabolism that is excreted by the kidneys
- Has somewhat poor water solubility
- Predisposes to gout
-
Triggers of urate crystal deposition
- ↑ Uric acid levels (due to insufficient excretion or increased production of purines)
- Acidosis
- Low temperature (e.g., cool peripheral joints)
- Crystalline arthritis: supersaturation of uric acid in extracellular fluid → intraarticular uric crystal precipitation (coated by IgGs) → phagocytosis by polymorphonuclear cells → release of inflammatory mediators and enzymes → local joint inflammation
- Chronic effects: repeated attacks → aggregations of urate crystals and giant cells (tophi) → deformities and arthritis
Clinical features
Asymptomatic stage
- Hyperuricemia with no symptoms
- May last ≥ 10 years
Acute gouty arthritis
-
Triggers
- Sudden increase in uric acid, e.g.,: consuming a large amount of purine-rich foods or alcohol (see risk factors for gout)
- Trauma, surgery
- Diuresis
- Dehydration
-
Most common manifestation
- Acute severe pain with overlying erythema, decreased range of motion, swelling, warmth
- Possibly fever
- Symptoms are more likely to occur at night, typically waking the patient.
- Symptoms peak after 12–24 hours and regress over days to weeks. [10]
- Desquamation of the skin overlying the joint may be seen during the recovery from an acute gout flare.
-
Location
-
Usually monoarthritis during first attacks
- In < 20% of cases, patients present with polyarthritis during first attacks.
- Asymmetrical distribution is common if more than one joint is affected
- Peripheral small joints in the lower extremities are especially affected.
- Podagra: metatarsophalangeal joint (MTP joint) inflammation of the big toe (the most common site)
- Gonagra: inflammation of the knee
- Chiragra: inflammation of finger joints, especially metacarpophalangeal joint of the thumb
- Others: ankle; , tarsus, other toe joints, wrist, elbow
-
Usually monoarthritis during first attacks




Intercritical stage
- Asymptomatic
- May last up to several years
Chronic gouty arthritis
- Uncommon in these times
- Progressive joint destruction
-
Tophi formation
-
Multiple painless hard nodules with possible joint deformities [11]
- May appear yellow or white because of overlying attenuated skin
- Ulceration and discharge (chalky white substance) may occur
- Bone tophi: urate crystal deposition in bones (e.g., elbows, knees, extensor surfaces of forearms)
- Soft tissue tophi: urate crystal deposition in the pinna of the external ear, subcutis, tendon sheaths (e.g., at the Achilles tendon), or synovial bursae (e.g., olecranon bursa)
-
Multiple painless hard nodules with possible joint deformities [11]
- Renal manifestations with uric acid nephrolithiasis and uric acid nephropathy







Erythema and swelling can be seen in the area of the first metatarsophalangeal joint (MTPJ) of this patient's right foot.
First MTPJ inflammation (podagra) is a characteristic presentation of acute gouty arthritis.
Source: © IMPP

Erythema and swelling can be seen in the area of the first metatarsophalangeal joint (MTPJ) of this patient's left foot.
First MTPJ inflammation (podagra) is a characteristic presentation of acute gouty arthritis.
Source: © IMPP

Erythema and swelling can be seen in the area of the first metatarsophalangeal joint (MTPJ) of this patient's left foot.
First MTPJ inflammation (podagra) is a characteristic presentation of acute gouty arthritis.
Source: “Podagra” by Gonzosft, Wikimedia Commons, licensed under CC BY 3.0. Modifications: removal of arrow.
{kind=link}

Severe swelling of the proximal interphalangeal joint of the left middle finger
Source: © IMPP

Multiple gouty tophi can be seen bilaterally in the region of the metatarsophalangeal joint of the big toe.
In this patient, the tophi developed secondary to increased uric acid production in psoriasis.
Source: © IMPP

White chalky, nodules in the first and second toes (left)
Source: © IMPP

Tophi (monosodium urate crystal deposition in bones and soft tissues) are visible distributed irregularly in the fingers and metacarpus of this patient's left hand.
Source: © IMPP

The dorsum of both hands shows multiple gouty tophi in the area of the metacarpophalangeal joints (MCP). The proximal interphalangeal joints (PIP) appear swollen.
Source: “Fig. 1, in: The utility of dual energy computed tomography in the management of axial gout: case reports and literature review” by Jeremy X. Wang, Beverly Ng, Haesung Bak et al., BMC Rheumatology, licensed under CC BY 4.0. Modifications: - removed letter "a" - removed red arrow.

Painless, hard, soft, white chalky nodules in the bursa of the right elbow in a patient with gout.
Source: © IMPP

A 67-year-old male with an 8-year history of untreated gout
Both feet show unusually large gouty tophi in the area of the metatarsophalangeal (MTP), the interphalangeal, and the tarsometatarsal joints (Lisfranc joints). Some joints show signs of active inflammation (rubor).
Source: “Fig. 2, in: Nassira Aradoini et al. Chronic tophaceous gout with unusual large tophi: case report” by Nassira Aradoini, Sofia Talbi, Khadija Berrada et al., Pan African Medical Journal, licensed under CC BY 4.0.
Diagnosis
Identification of monosodium urate (MSU) crystals on synovial fluid analysis of the affected joint is the gold standard to diagnose gout but requires an invasive technique (i.e., arthrocentesis), trained personnel, and specialized instruments to perform the test. In patients with typical clinical features, a clinical diagnosis may be considered with/without supportive diagnostic evidence on imaging and laboratory studies.
Approach [8][12][13]
-
Acute gout (gout flare)
- Assess the clinical probability of septic arthritis.
- If relatively high, perform arthrocentesis for synovial fluid analysis
- Consult orthopedics as needed (see “Diagnosis of septic arthritis” for details).
- Assess the clinical probability of acute gout.
- If relatively low :
- Arthrocentesis with synovial fluid analysis is recommended.
- Consider differential diagnoses of gout.
- If relatively high : Diagnostic tests are not routinely required.
- If relatively low :
- Assess the clinical probability of septic arthritis.
- Chronic gout: A combination of history (e.g., recurrent episodes), examination and imaging findings (e.g., tophi), and evidence of MSU crystals on aspirates of tophi or synovial fluid analysis confirms the diagnosis of chronic gout. [14][15]
Arthrocentesis and synovial fluid analysis [8][12]
Synovial fluid analysis is the gold standard for diagnosing gout but should only be performed if polarized light microscopy is available and providers are trained in the procedure and interpretation.
-
Indications
- Uncertain clinical diagnosis
- Higher probability of septic arthritis
-
Characteristic findings
-
Polarized light microscopy: needle-shaped monosodium urate crystals that are negatively birefringent ; [10]
- Crystals appear yellow when their optical axis is oriented parallel to the polarizer.
- Crystals appear blue when their axis is perpendicular to the polarizer.
- Synovial fluid cell count: WBC > 2000/μL with > 50% neutrophils (see “Interpretation of synovial fluid analysis”)
- Gram stain: negative; useful for ruling out septic arthritis
-
Polarized light microscopy: needle-shaped monosodium urate crystals that are negatively birefringent ; [10]


Clinical diagnosis of acute gout [8][12]
There is a lack of consensus regarding strict diagnostic criteria for gout in clinical settings. [8][14][15][16]
- A clinical diagnosis of acute gout can be considered in patients who fulfill all of the following parameters:
- Typical clinical presentation
- Low suspicion for septic arthritis
- Monoarthritis
- The diagnostic rule for acute gout can improve diagnostic accuracy for patients with acute monoarthritis.
| Diagnostic rule for acute gout [17][18] | ||
|---|---|---|
| Criterion | Number of points | |
| Patient characteristics | Male | 2 |
| ≥ 1 of the following: hypertension, angina, MI, CHF, TIA, stroke, PVD | 1.5 | |
| History of previous arthritis attack | 2 | |
| Features of current attack | Onset within 24 hours | 0.5 |
| Joint erythema | 1 | |
| Affects 1stmetatarsophalangeal joint | 2.5 | |
| Serum uric acid level > 5.88 mg/dL (> 0.35 mmol/L) | 3.5 | |
Interpretation
| ||

Laboratory studies
-
Serum uric acid level ; [12][16]
- Acute gout flare: often elevated (hyperuricemia) ; may also be normal or low
- Intercritical stage or chronic gout
- Baseline levels are useful to determine the need for urate-lowering therapy.
- A normal or low level has a very low negative likelihood ratio for (but does not rule out) a diagnosis of gout.
- CBC and inflammatory markers: : WBC and ESR are typically elevated in an acute gout attack. [19]
- Urinary uric acid measurement (via 24-hour urine collection): not routinely recommended
Serum uric acid levels are not always elevated in acute gouty arthritis.
Imaging [8][12][16][20]
Imaging is indicated if synovial fluid analysis is unsuccessful or cannot be performed, and the diagnosis remains uncertain. It can be used to identify supportive findings of gout but cannot rule out septic arthritis.
-
Ultrasound
- Signs of acute joint inflammation
- Bone erosions
- Signs of urate crystal deposition
- Double contour sign: a hyperechoic band of crystals covering the surface of the hypoechoic articular cartilage, which is over the hyperechoic bone contour
- Tophi (pathognomonic for chronic gout)
-
X-ray
- Acute gout: typically normal; useful for ruling out a fracture in patients with posttraumatic joint inflammation
-
Chronic gout
- Punched-out lytic bone lesions with spiky periosteal appositions (overhanging edges), known as “rat-bite erosions”
- Radiopaque in surrounding soft tissue
- Joint space is preserved until late stages.
- Conventional CT and MRI: can identify erosions and tophi; used less frequently
- Dual-energy CT : can detect crystals within deeper anatomical structures (e.g., the spine) and extra-articular sites
Ultrasound or DECT are preferred imaging modalities to detect MSU crystal deposition within affected joints.


This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
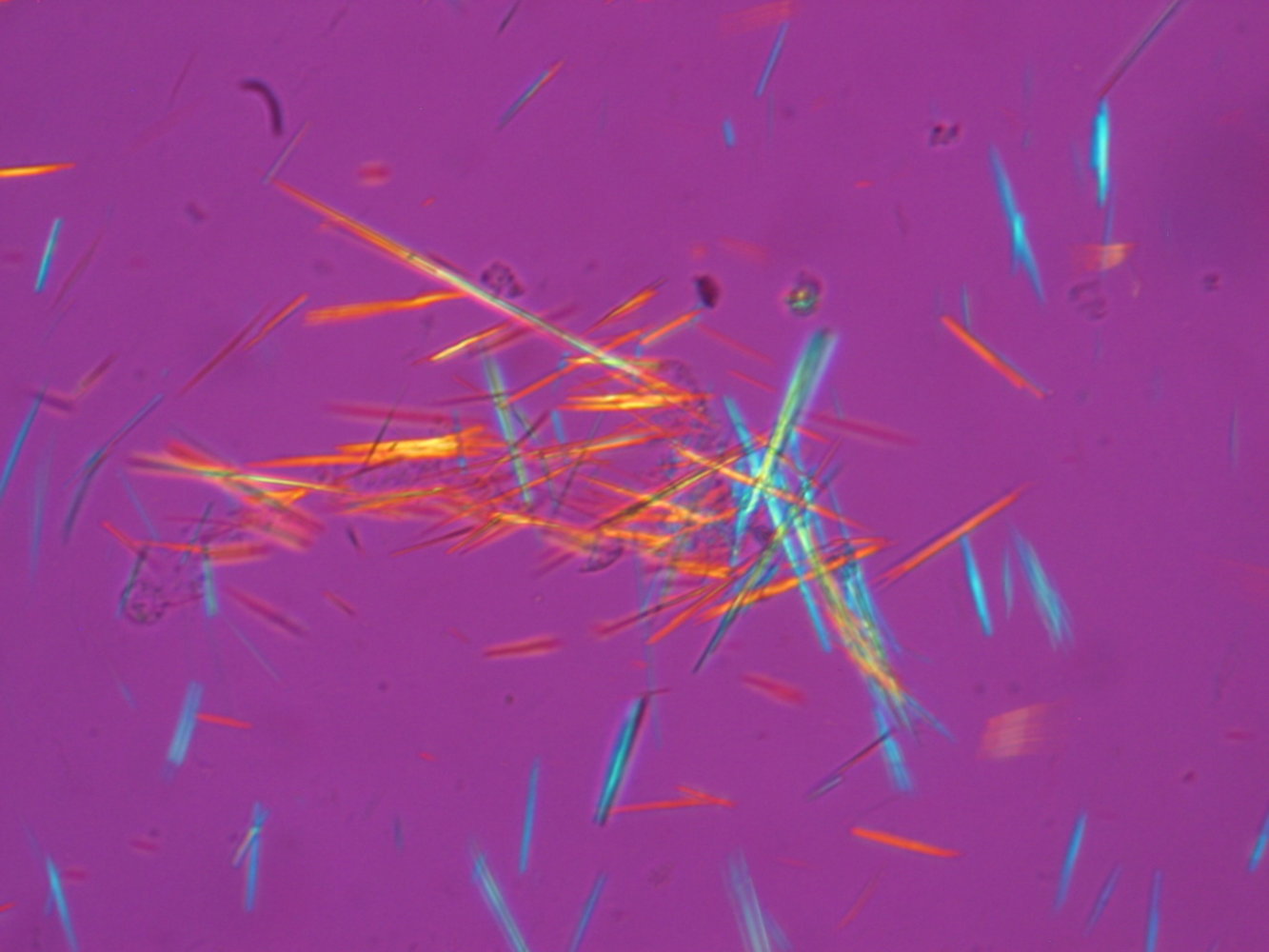
Sample of synovial fluid under polarizing light microscopy
Monosodium urate crystals are needle-shaped and appear yellow when their optical axis is oriented parallel to the polarizer. If their axis is perpendicular to the polarizer, they appear blue. The underlying physical principle is called negative birefringence.
Detection of negatively birefringent, needle-shaped crystals in synovial fluid confirms the diagnosis of gout.
Source: “Spiked rods of monosodium urate crystals photographed under polarized light from a synovial fluid sample.” by Bobjgalindo, Wikimedia Commons, licensed under CC BY-SA 4.0.
{kind=link}

Original title: “Guiding arthrocentesis with ultrasound”. Created by: Medmastery.

X-ray of a left foot (AP and lateral views)
Joint space narrowing of the first metatarsophalangeal joint with multiple spiky periosteal appositions (blue overlay). Both the first metatarsal bone and the first proximal phalanx also show the characteristic “punched-out” lesions (examples indicated by black arrowheads). There is marked soft tissue swelling on the lateral border of the foot (yellow overlay).
Source: “Gichtfuss im Roentgenbild 002” by Hellerhoff, Wikimedia Commons, licensed under CC BY-SA 3.0. Modifications: removed letters "P" and "F". The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}

X-ray knee (left: AP view; right: lateral view) of a patient with a history of gout
An eccentric lesion involves the lateral femoral condyle (green overlay) and adjacent soft tissues (red overlay). A sclerotic margin is seen along part of the lesion (arrowheads).
Source: “Figure 3 a and b, in: Radiology of crystal arthropathies” by Subbarao K, Journal of Medical and Scientific Research, licensed under CC BY 4.0. Modifications: Arrows removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
Pathology
Foreign body granuloma
- Caused by urate crystal deposition in cutis and subcutis
- Findings include:
- Clusters of crystal deposits
- Macrophages in the shape of epithelioid cells or polynuclear giant cells

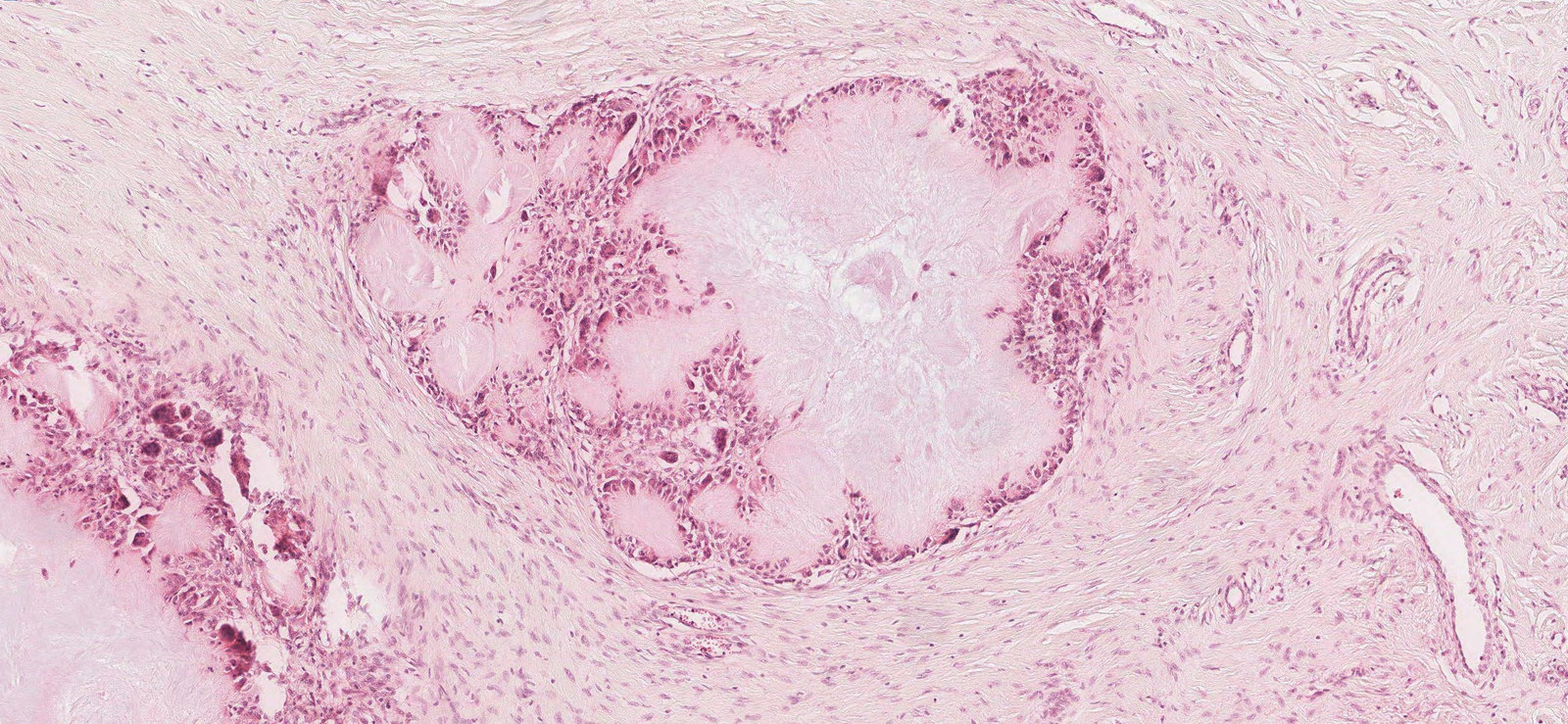
Photomicrograph of a subcutaneous tissue sample (H&E stain, medium power magnification)
Two foreign body granulomas can be seen (example indicated by black outline) and each with centrally located urate crystal deposits (examples indicated by green overlay), macrophages in the form of epithelioid cells (examples indicated by black arrows), and multinucleated giant cells (examples indicated by green arrowheads).
These findings indicate a gout tophus.
Click on the Smartzoom button to view the entire specimen through a virtual microscope.
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: PD Dr. med. Alberto Perez Bouza, Facharzt für Pathologie
Differential diagnoses
-
Septic arthritis
- Can occur concomitantly with gout [21]
- Joint damage from chronic gout may increase risk. [22]
-
Inflammatory arthritis (other types): See “Differential diagnoses of inflammatory arthritis.”
- Acute calcium pyrophosphate deposition disease (pseudogout)
- Rheumatoid arthritis
- Seronegative spondyloarthropathy (e.g. psoriatic arthritis, reactive arthritis)
- Basic calcium phosphate crystal deposition diseases
- Erosive osteoarthritis
The differential diagnoses listed here are not exhaustive.
Treatment
General measures [23]
- Lifestyle modifications may help reduce the risk of flares.
- Limit alcohol consumption
- Limit intake of purines (e.g., red meat and shellfish)
- Limit high-fructose corn syrup (e.g., sugary foods, juices, and non-diet sodas)
- Weight loss if patient is overweight
- Identify and treat sleep apnea. [24][25]
- Close management of comorbidities, such as diabetes and hypertension
- Adjust current antihypertensive regimen, if feasible: losartan preferred; avoid hydrochlorothiazide [23]
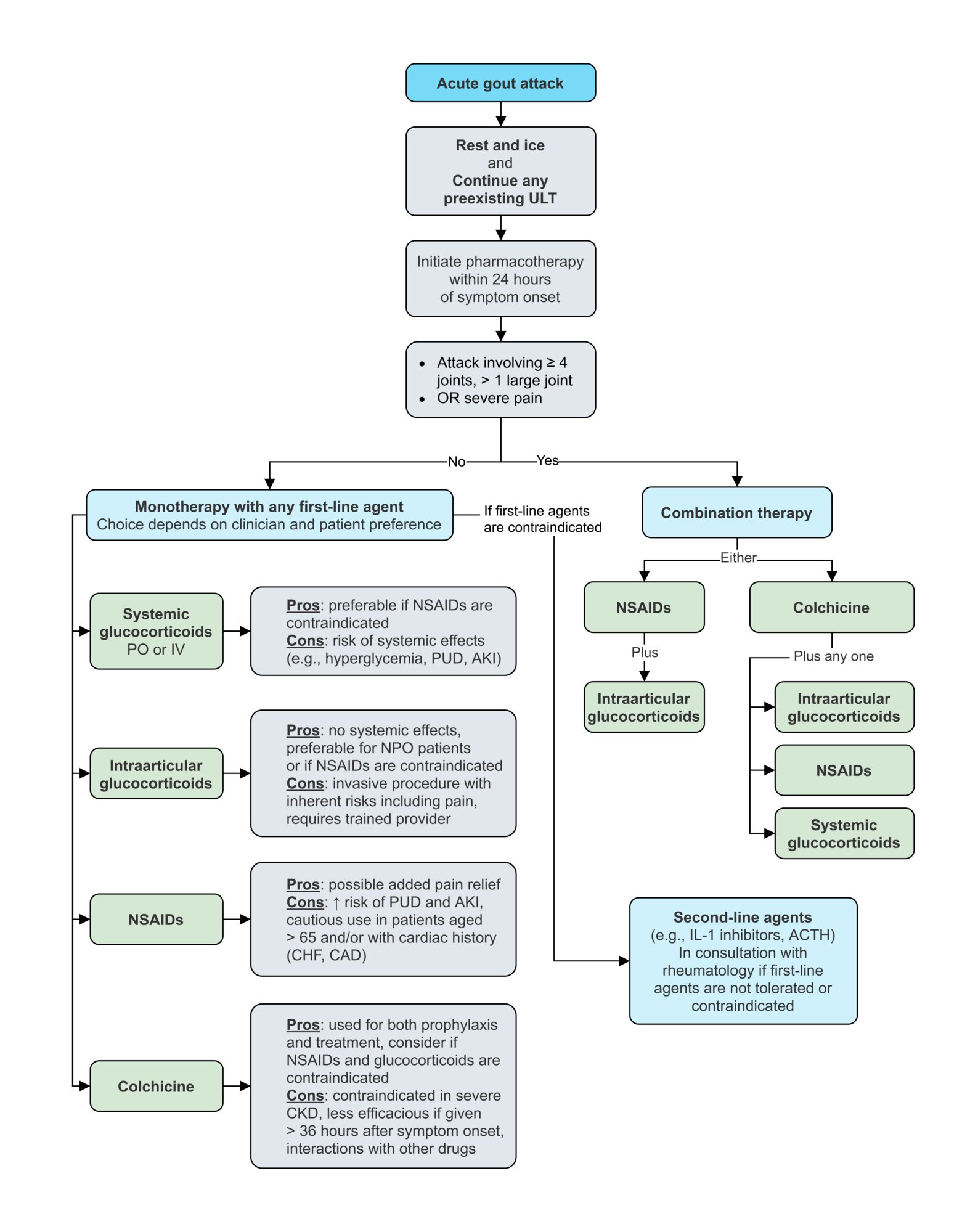
Acute gout flare
Approach [12][23][26][27][28]
- Nonpharmacological measures: Rest and ice the affected joint. [29]
-
Pharmacotherapy: Initiate within 24 hours of onset.
- First-line agents: glucocorticoids, NSAIDs, or colchicine (described in detail below) [23][27]
- Second-line agents : IL-1 inhibitors or ACTH
- Combination therapy options: indicated for attacks involving ≥ 4 joints, > 1 large joint, or severe pain
- Glucocorticoids (any formulation) PLUS colchicine
- NSAIDs PLUS colchicine
- Intraarticular glucocorticoids PLUS NSAIDs
- Consider initiating urate-lowering therapy in select patients (see “Indications” in “Urate-lowering therapy” for details).

If a patient is on long-term urate-lowering therapy, it should be continued during the treatment of an acute gout flare.
Avoid combining NSAIDs with systemic glucocorticoids. If prescribed together, add a proton pump inhibitor to reduce the risk of gastrointestinal ulcers.
Glucocorticoids [23][27]
-
Systemic administration
-
Oral (e.g., prednisone or prednisolone; or equivalent )
- Fixed-dose regimen: Treat for 5 days or until symptom resolution.
- A tapered regimen may reduce the risk of a rebound flare. [30]
- Parenteral or intramuscular (e.g., methylprednisolone ) if NPO
-
Oral (e.g., prednisone or prednisolone; or equivalent )
- Intraarticular administration: : Consider if there are 1–2 joints that are accessible and a trained provider is available.
Glucocorticoids are preferable if there are contraindications (e.g., CKD), intolerance, or inadequate response to colchicine or NSAIDs.
NSAIDs [23][27]
-
Naproxen: or an alternative (e.g., indomethacin, ibuprofen; see “Pain management” for details)
- Fixed-dose regimen: Treat for shortest duration necessary to resolve symptoms (often at least 3–5 days).
- Tapered regimen for patients with:
- Hepatic/renal impairment
- Comorbidities
- Severe symptoms
- Selective COX-2 inhibitors: Consider as an alternative to naproxen in patients without contraindications.
Low-dose aspirin can decrease uric acid excretion and trigger recurrent gout flares but it should not be stopped in patients taking it for specific indications (e.g., coronary artery disease, cerebrovascular disease), regardless of the severity of gout. [23][31]
Colchicine [23][27]
- Mechanism of action: binds and stabilizes tubulin subunits → inhibits microtubule polymerization → inhibits phagocytosis of urate crystals, neutrophil activation, migration, and degranulation [32]
-
Administration
- Administer within the first 12 hours of symptom onset to maximize efficacy.
- Reduce dose and monitor closely when prescribed in patients with hepatic impairment or mild-moderate CKD.
-
Adverse effects
- Gastrointestinal symptoms, e.g., diarrhea, nausea, vomiting, and abdominal pain, are the most common.
- Rhabdomyolysis , myopathy
- Polyneuropathy [33]
- Cardiac toxicity, arrhythmias
- Nephrotoxicity
- Myelosuppression
- CNS symptoms (e.g., fatigue, headache)
-
Contraindications
- Severe CKD
- Patients on prophylactic colchicine who received an acute gout dose of colchicine in the previous 14 days
-
Drug interactions
- Statins: Consider reducing dose of pravastatin, atorvastatin, or simvastatin when prescribed concomitantly.
- Potent cytochrome P450 3A4 substrates or inhibitors
- Reduce colchicine dose when prescribed concomitantly.
- Avoid in patients with CKD or hepatic impairment.
Colchicine is unlikely to be effective when initiated > 24–36 hours after symptom onset. Colchicine is preferable in patients who cannot tolerate NSAIDs or systemic glucocorticoids (e.g., patients with gastrointestinal ulcers)
Monitor for myotoxicity when prescribing colchicine with statins. Reduce dose of pravastatin, atorvastatin, and simvastatin when prescribed concomitantly.
© AMBOSS
Chronic gout
Approach [23]
-
Urate-lowering therapy (ULT) is recommended for chronic gout.
- First-line: xanthine-oxidase inhibitors (allopurinol)
- Second-line: uricosurics (probenecid)
- Third-line: recombinant uricase (pegloticase)
- Administer anti-inflammatory prophylaxis before initiating ULT as ULT may trigger, prolong, or worsen an acute gout flare.
Initial anti-inflammatory prophylaxis [23][26][28]
- Indication: pre-treatment in patients planned for ULT therapy
- Important consideration: should be initiated 1 week before starting ULT therapy
-
Options: low dose of any one of the following agents [12][23][26]
- Colchicine
- NSAIDs (e.g., naproxen )
- Glucocorticoids (e.g., prednisone )
- Treatment duration: Should be administered concomitantly with ULT for at least 3–6 months (or longer if flares continue).
Administering XOIs or uricosuric agents during an acute gout flare may worsen symptoms by mobilizing urate crystals. Anti-inflammatory prophylaxis with colchicine, NSAIDs, or glucocorticoids must be administered before initiating ULT.
Urate-lowering therapy (ULT) [23][26][27]
Indications
-
Absolute indications
- Damage due to chronic gout seen on imaging
- Tophi development
- Frequent gout attacks (≥ 2 per year)
-
Relative indications
- < 2 gout attacks per year
- First episode of acute gout flare in patients with any of the following risk factors:
- CKD ≥ stage 3
- Serum uric acid > 9 mg/dL
- History of urolithiasis
Contraindications
-
Common to all ULT agents
- Acute gout flare (in the absence of the above-mentioned risk factors)
- Asymptomatic hyperuricemia
- Specific contraindications: see the table below for details
Important considerations
- Timing of initiating ULT: at least one week after initiating anti-inflammatory prophylaxis (see above)
- Titration target: serum urate < 6 mg/dL [23]
- Treatment duration: Continue indefinitely if tolerated and in remission
- Patient adherence: typically low ; monitoring and counseling recommended [34]
Agents
| Urate-lowering therapy [23][27][35] | |||||
|---|---|---|---|---|---|
| Drugs | First-line Xanthine oxidase inhibitors (XOIs) |
Second-line Uricosurics |
Third-line Recombinant uricase |
||
| Allopurinol | Febuxostat | Probenecid | Pegloticase | ||
| Indications [23] |
|
|
|
|
|
| Mechanism of action |
|
|
|
||
| Specific contraindications |
|
|
|
|
|
| Side effects |
|
|
|
|
|
| Important drug interactions |
|
|
|
||
Test for the HLA-B*5801 allele before initiating allopurinol in black patients and patients of Southeast Asian descent.
The combination of allopurinol and azathioprine leads to increased bone marrow toxicity!

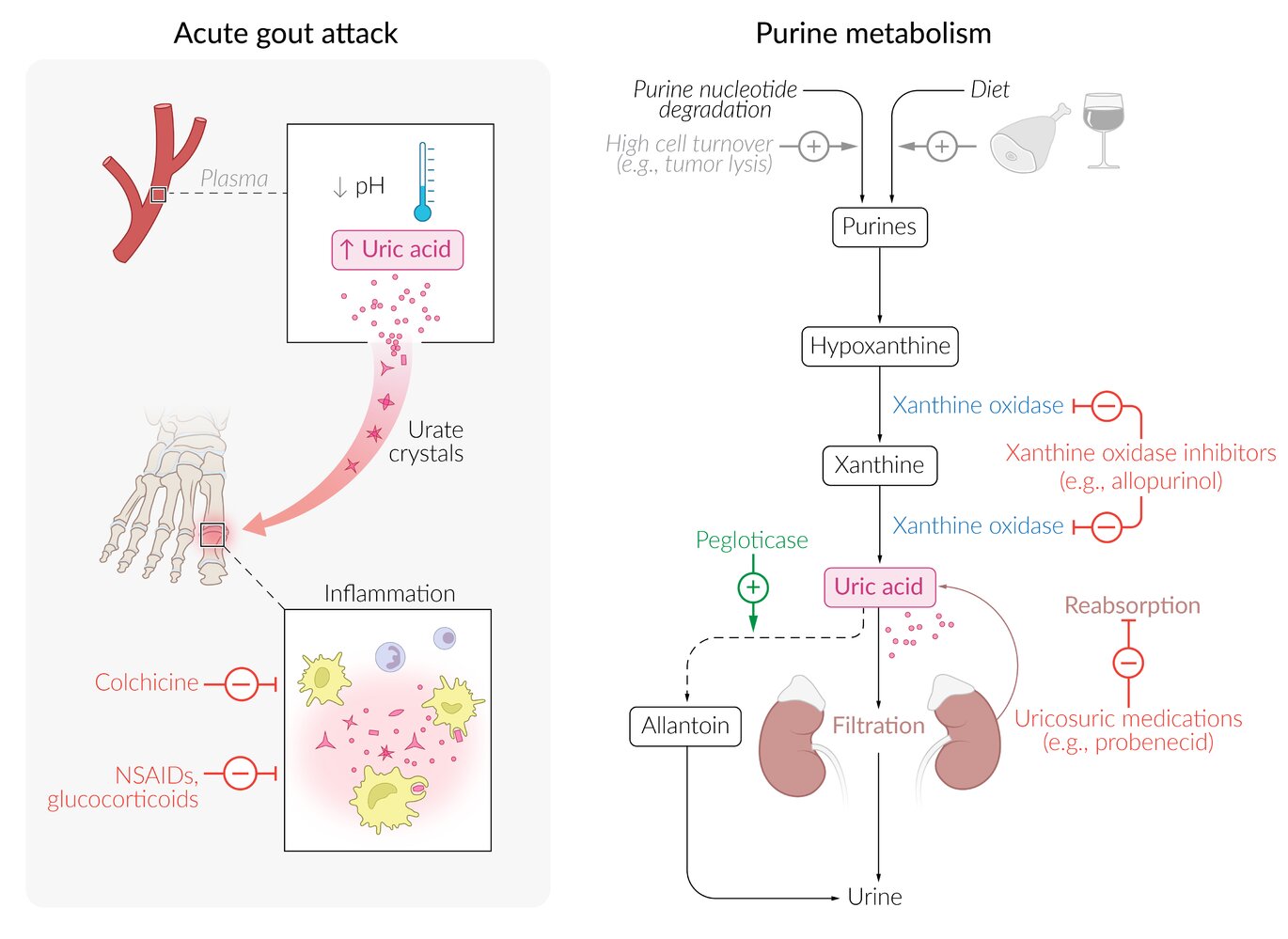
Acute gout attack: Increases in uric acid concentration or decreases in temperature/pH can lead to the accumulation of urate crystals in various tissues, triggering inflammation. First-line treatment options include NSAIDs, glucocorticoids, and colchicine.
Purine metabolism: Uric acid concentration can increase due to underexcretion (e.g., in chronic renal insufficiency) or over-production (e.g., in tumor lysis syndrome or high dietary purine intake). Xanthine oxidase inhibitors (e.g., allopurinol) inhibit the purine degradation pathway from hypoxanthine to uric acid. Uricosuric medications (e.g., probenecid) inhibit uric acid reabsorption in the proximal convoluted tubules, thus increasing renal excretion. Pegloticase (a recombinant uricase) catalyzes the breakdown of uric acid into allantoin, which is more water-soluble and, therefore, more readily excreted renally.
© AMBOSS
Acute management checklist for acute gout flare
- Consider limb-threatening differential diagnoses (e.g., septic arthritis).
- Assess need for diagnostic arthrocentesis, laboratory studies, and/or imaging.
- Consult rheumatology if diagnosis remains uncertain.
- Provide adequate analgesia.
- Rest the joint and use local ice therapy.
- If the patient is on long-term urate-lowering therapy, it should not be discontinued.
- Initiate pharmacotherapy for acute gout as early as possible; select one of the following based on patient-specific factors:
- Glucocorticoids
- NSAIDs
- Colchicine
- Consider indications for combination therapy.
- Ensure follow-up with the primary care provider or rheumatologist for complicated cases.
Complications
- Nephrolithiasis: uric acid stones
-
Uric acid nephropathy
-
Acute uric acid nephropathy
- Can occur in tumor lysis syndrome
- Causes tubular obstruction → acute renal failure
-
Chronic uric acid nephropathy: a form of chronic tubulointerstitial nephropathy with monosodium urate crystal deposition in the stroma of the kidney, which causes inflammation
- Clinical features
- Hypertension
- In rare cases, progressive renal failure
- Clinical features
-
Acute uric acid nephropathy
We list the most important complications. The selection is not exhaustive.
Related One-Minute Telegram
- One-Minute Telegram 97-2024-3/3: Two big toes up for SGLT2i in type 2 diabetes
Interested in the newest medical research, distilled down to just one minute? Sign up for the One-Minute Telegram in “Tips and links” below
External Resources
- One-Minute Telegram url:
- 2020 ACRE Guideline for the Management of Gout
- 2016 ACP Guideline for the Diagnosis of Acute Gout
- 2016 ACP Guideline for the Management of Acute and Recurrent Gout
- 2015 ACR/EULAR Gout Classification Criteria
- 2012 ACR Guidelines for the Management of Gout (Part 1)
- 2012 ACR Guidelines for the Management of Gout (Part 2)
- 2018 EULAR Recommendations for the Diagnosis of Gout
References
- "Arthritis: Gout". https://web.archive.org/web/20170518215721/https://www.cdc.gov/arthritis/basics/gout.html. [2016-07-22]
- Bingqing Zhang, Weigang Fang, Xuejun Zeng, et al. "Clinical characteristics of early- and late-onset gout". Medicine. (2016)
- Becker MA. "Asymptomatic hyperuricemia". UpToDate. UpToDate. http://www.uptodate.com/contents/asymptomatic-hyperuricemia. [2017-02-07]
- Choi HK, Mount DB, Reginato AM, American College of Physicians, American Physiological Society. "Pathogenesis of gout". Ann Intern Med. 143(7). :499-516. (2005)
- Curhan GC, Becker MA. "Uric acid renal diseases". UpToDate. UpToDate. http://www.uptodate.com/contents/uric-acid-renal-diseases. [2015-04-15]
- Pittman JR, Bross MH. "Diagnosis and Management of Gout". Am Fam Physician. 59(7). :1799-1806. (1999)
- Richard J. Johnson, Duk-Hee Kang, Daniel Feig, et al. "Is There a Pathogenetic Role for Uric Acid in Hypertension and Cardiovascular and Renal Disease?". Hypertension. (2003)
- Qaseem A, McLean RM, Starkey M, Forciea MA. "Diagnosis of Acute Gout: A Clinical Practice Guideline From the American College of Physicians". Ann Intern Med. 166(1). :52. (2016)
- Choi HK, Niu J, Neogi T, et al. "Nocturnal risk of gout attacks". Arthritis & rheumatology (Hoboken, N.J.). 67(2). :555-62. (2015)
- Richette P, Bardin T. "Gout". Lancet. 375(9711). :318-328. (2009)
- Becker MA. "Clinical manifestations and diagnosis of gout". UpToDate. UpToDate. http://www.uptodate.com/contents/clinical-manifestations-and-diagnosis-of-gout. [2017-02-07]
- Aslam F, Michet C. "My Treatment Approach to Gout". Mayo Clin Proc. 92(8). :1234-1247. (2017)
- Dalbeth N, Choi HK, Joosten LAB, et al. "Gout". Nature Reviews Disease Primers. 5(1). (2019)
- Neogi T, Jansen TLTA, Dalbeth N, et al. "2015 Gout Classification Criteria: An American College of Rheumatology/European League Against Rheumatism Collaborative Initiative". Arthritis Rheumatol. 67(10). :2557-2568. (2015)
- Aggarwal R, Ringold S, Khanna D, et al. "Distinctions between diagnostic and classification criteria?". Arthritis Care Res (Hoboken). 67(7). :891-7. (2015)
- Richette P, Doherty M, Pascual E, et al. "2018 updated European League Against Rheumatism evidence-based recommendations for the diagnosis of gout". Ann Rheum Dis. 79(1). :31-38. (2019)
- Janssens HJ, Fransen J, van de Lisdonk EH, et al. "A diagnostic rule for acute gouty arthritis in primary care without joint fluid analysis.". Arch Intern Med. 170(13). :1120-6. (2010)
- Kienhorst LBE, Janssens HJEM, Fransen J, Janssen M. "The validation of a diagnostic rule for gout without joint fluid analysis: a prospective study". Rheumatology (Oxford). 54(4). :609-614. (2015)
- Roseff R, Wohlgethan JR, Sipe JD, Canoso JJ. "The acute phase response in gout". J Rheumatol. 14(5). :974-7. (1987)
- Abdellatif W, Ding J, Khorshed D, Shojania K, Nicolaou S. "Unravelling the mysteries of gout by multimodality imaging". Semin Arthritis Rheum. 50(3). :S17-S23. (2020)
- Yu KH, Luo SF, Liou LB, et al. "Concomitant septic and gouty arthritis--an analysis of 30 cases.". Rheumatology (Oxford). 42(9). :1062-6. (2003)
- Goldenberg DL. "Infectious arthritis complicating rheumatoid arthritis and other chronic rheumatic disorders.". Arthritis Rheum. 32(4). :496-502. (1989)
- FitzGerald JD, Dalbeth N, Mikuls T, et al. "2020 American College of Rheumatology Guideline for the Management of Gout". Arthritis Care Res (Hoboken). 72(6). :744-760. (2020)
- Singh JA, Cleveland JD. "Gout and the Risk of Incident Obstructive Sleep Apnea in Adults 65 Years or Older: An Observational Study". J Clin Sleep Med. 14(9). :1521-1527. (2018)
- Blagojevic-Bucknall M, Mallen C, Muller S, et al. "The Risk of Gout Among Patients With Sleep Apnea: A Matched Cohort Study.". Arthritis & rheumatology (Hoboken, N.J.). 71(1). :154-160. (2019)
- Khanna D, Khanna PP, Fitzgerald JD, et al. "2012 American College of Rheumatology guidelines for management of gout: Part 2: therapy and antiinflammatory prophylaxis of acute gouty arthritis". Arthritis Care Res. 64(10). :1447-1461. (2012)
- Qaseem A, Harris RP, Forciea MA. "Management of Acute and Recurrent Gout: A Clinical Practice Guideline From the American College of Physicians". Ann Intern Med. 166(1). :58. (2016)
- Pillinger MH, Mandell BF. "Therapeutic approaches in the treatment of gout". Semin Arthritis Rheum. 50(3). :S24-S30. (2020)
- Schlesinger N, Detry MA, Holland BK, et al. "Local ice therapy during bouts of acute gouty arthritis". J Rheumatol. 29(2). :331-334. (2002)
- Hainer BL, Matheson E, Wilkes RT. "Diagnosis, treatment, and prevention of gout.". Am Fam Physician. 90(12). :831-6. (2014)
- Zhang Y, Neogi T, Chen C, et al. "Low-dose aspirin use and recurrent gout attacks". Ann Rheum Dis. 73(2). :385-390. (2013)
- Dalbeth N, Lauterio TJ, Wolfe HR. "Mechanism of action of colchicine in the treatment of gout". Clin Ther. 36(10). :1465-1479. (2014)
- Kuncl RW, Duncan G, Watson D, et al. "Colchicine Myopathy and Neuropathy". N Engl J Med. 316(25). :1562-1568. (1987)
- Abhishek A, Doherty M. "Education and non-pharmacological approaches for gout". Rheumatology. 57(suppl_1). :i51-i58. (2017)
- Khanna D, Fitzgerald JD, Khanna PP, et al. "2012 American College of Rheumatology guidelines for management of gout. Part 1: systematic nonpharmacologic and pharmacologic therapeutic approaches to hyperuricemia.". Arthritis Care Res (Hoboken). 64(10). :1431-46. (2012)
- Stamp LK, Barclay ML. "How to prevent allopurinol hypersensitivity reactions?". Rheumatology. 57(suppl_1). :i35-i41. (2018)
- Agabegi SS, Agabegi ED. "Step-Up To Medicine". Lippincott Williams & Wilkins. (2013). ISBN: 9781609133603
- Dalbeth N, Doyle AJ. "Imaging tools to measure treatment response in gout". Rheumatology. 57(suppl_1). :i27-i34. (2018)
- Dalbeth N, Bardin T, Doherty M, et al. "Discordant American College of Physicians and international rheumatology guidelines for gout management: consensus statement of the Gout, Hyperuricemia and Crystal-Associated Disease Network (G-CAN)". Nat Rev Rheumatol. 13(9). :561-568. (2017)
- Golenbiewski J, Keenan RT. "Moving the Needle: Improving the Care of the Gout Patient". Rheumatol Ther. 6(2). :179-193. (2019)
- McCarthy GM, Dunne A. "Calcium crystal deposition diseases — beyond gout". Nat Rev Rheumatol. 14(10). :592-602. (2018)
- Kelley JT, Agudelo CA, Sharma V, Holland NW. "Fever with Acute Arthritis in Calcium Pyrophosphate Dihydrate Deposition Disease: A Missed Explanation for Altered Mental Status in Elderly Patients?". J Clin Rheumatol. 7(5). :322-325. (2001)