Summary
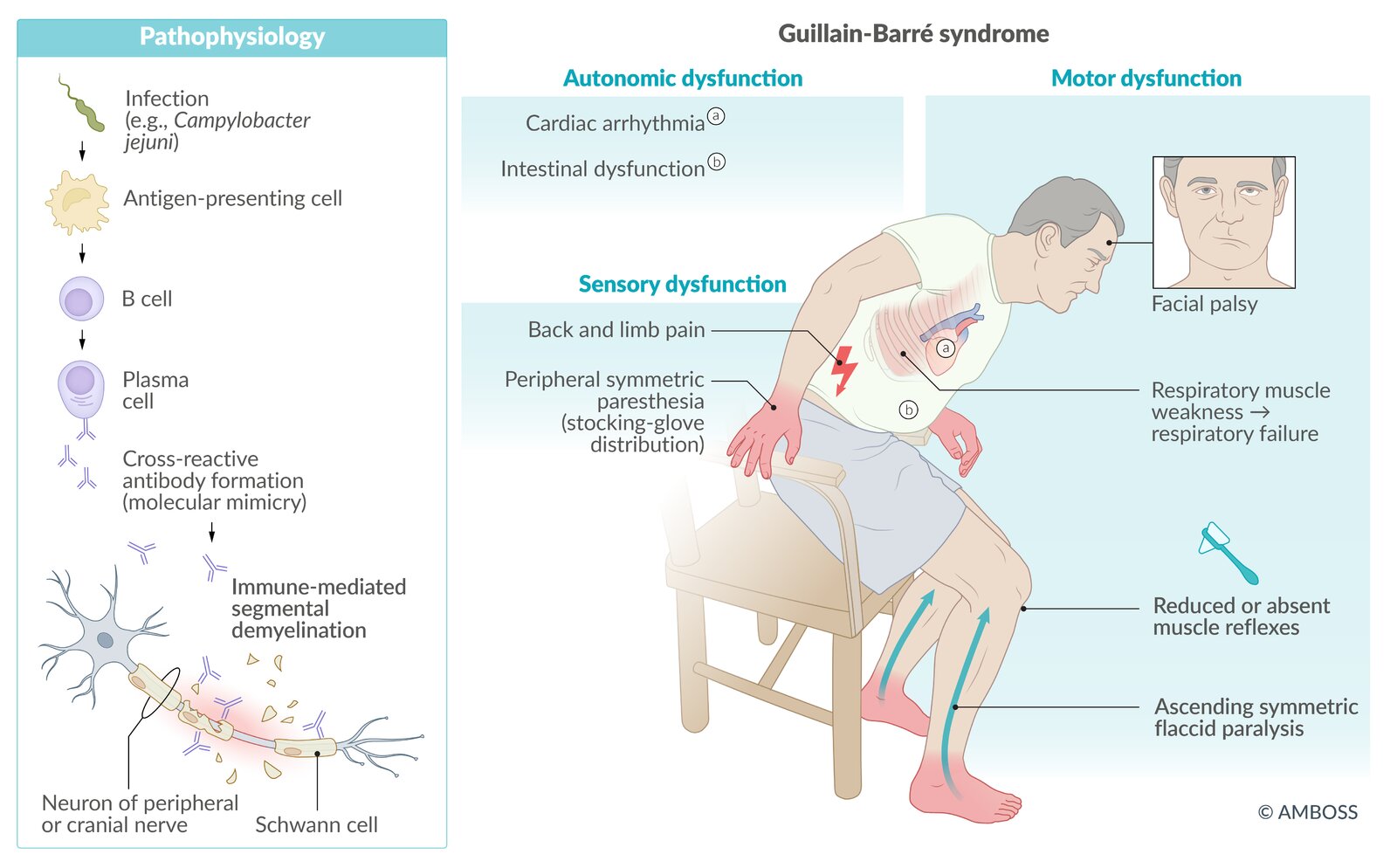
Guillain-Barré syndrome (GBS) is an acute immune-mediated polyradiculoneuropathy that typically manifests with bilateral ascending flaccid paralysis and sensory involvement, e.g., paresthesia. The pathogenesis of GBS involves autoantibodies against antigens in the myelin sheath, other Schwann-cell antigens, and axon membranes. Approximately 65% of patients have an upper respiratory tract or gastrointestinal infection before the onset of GBS symptoms. Diagnosis is primarily clinical; alternative diagnoses should be considered especially in patients with atypical presentations. Cerebrospinal fluid (CSF) analysis showing albuminocytologic dissociation and electrodiagnostic study findings help support the diagnosis. Medical treatment depends on the severity of symptoms; available treatment options are intravenous immunoglobulin (IVIg) and plasmapheresis. Close monitoring is required for all patients. Complications such as respiratory failure, pulmonary embolism, and/or cardiac arrest increase mortality. Up to 20% of patients remain severely disabled and approximately 5% of patients die despite medical treatment.
Epidemiology
-
Incidence [1]
- ∼ 1 case per 100,000 individuals
- Adults are affected more frequently than children.
- Sex: ♂ > ♀ (1.5:1) [2]
Epidemiological data refers to the US, unless otherwise specified.
Etiology
-
Overview
- About two-thirds of GBS patients experience symptoms of an upper respiratory or gastrointestinal tract infection up to 6 weeks prior to onset of GBS. [2][3]
- The causal connection between pathogens and GBS is still undetermined.
-
Associated pathogens [1][4][5]
- Campylobacter jejuni: Campylobacter enteritis is the most common disease associated with GBS.
- Cytomegalovirus (CMV)
- HIV
- Influenza
- Zika virus
- Epstein-Barr virus
- SARS-CoV-2
- Mycoplasma pneumoniae
-
Vaccination
- There have been reports of small increases in incidence after administration of certain vaccines. [6]
- In the US, GBS is listed as a vaccination injury for the seasonal influenza vaccines.
Pathophysiology
- Postinfectious autoimmune reaction that generates cross-reactive antibodies (molecular mimicry) [7]
- Infection triggers humoral response → formation of autoantibodies against gangliosides (e.g., GM1, GD1a) or other unknown antigens of peripheral Schwann cells → immune-mediated segmental demyelination → axonal degeneration of motor and sensory fibers in peripheral and cranial nerves (CN III–XII) [7]

© AMBOSS
Clinical features
Disease extent and severity in GBS vary widely, from mild muscle weakness to quadriplegia and respiratory failure.
Typical disease progression
- Onset is acute or subacute, and symptoms progress rapidly.
- Symptoms peak at ∼ 2–4 weeks and then plateau over months or years, followed by partial or complete resolution. [2][3]
Typical presentation
Classic sensorimotor features are observed in most patients with GBS (see also “Variants of GBS”). [3]
-
Limb involvement: typically bilateral and ascending from the lower limbs
- Progressive flaccid paresis or paralysis
- Paresthesia: stocking‑glove distribution [3]
- Hyporeflexia or areflexia typically begins in the lower limbs. [2]
-
Back and limb pain (often an early symptom)
- Involves nociceptive and neuropathic pain
- Affects approx. two-thirds of patients [8]
-
Autonomic dysfunction
- Cardiac arrhythmias, blood pressure fluctuations [2]
- Urinary retention and/or intestinal dysfunction
- Respiratory muscle involvement: may lead to respiratory failure.
-
Cranial nerve involvement
- Facial diplegia: due to bilateral facial nerve involvement (most frequently affected cranial nerve in GBS)
- Bulbar dysfunction
GBS can affect respiratory muscle function; life-threatening respiratory failure occurs in approx. 20% of patients. [8][9]
© AMBOSS
Subtypes and variants
Subtypes of Guillain-Barré syndrome
Classification into subtypes is based on electrodiagnostic study findings; each subtype is associated with specific autoantibodies.
| Overview of subtypes of Guillain-Barré syndrome | ||||||
|---|---|---|---|---|---|---|
| Subtype | Pathophysiology | Epidemiology | Characteristic features | |||
| Acute inflammatory demyelinating polyneuropathy (AIDP) |
|
|
|
|||
| Axonal loss | Acute motor axonal neuropathy (AMAN) |
|
|
|
||
| Acute motor and sensory axonal neuropathy (AMSAN) | ||||||
Classification into subtypes does not affect treatment decisions but may inform prognosis. [2][3]
Variants of Guillain-Barré syndrome
Variants of the classic sensorimotor presentation are characterized by the involvement of a specific group of muscles or nerves; overlap between variants is common.
-
Miller-Fisher syndrome (MFS) [2][3]
-
Limited involvement; characteristic features include: [2]
- Cranial nerve involvement, typically ophthalmoplegia
- Bulbar palsy
- Ataxia
- Areflexia
- Anti‑GQ1b antibodies and anti‑GT1a antibodies are detected in 90% of patients. [7]
- Nerve conduction studies are normal in most patients. [7]
-
Limited involvement; characteristic features include: [2]
-
Other variants include:
-
Bickerstaff brainstem encephalitis (BBE) [9]
- Typical features include ophthalmoplegia, ataxia, and signs of brainstem dysfunction.
- Associated with anti‑GQ1b antibodies
- Pure motor variant
- Pharyngeal-cervical-brachial variant
- Paraparetic variant
- Bilateral facial palsy with paresthesia variant
-
Bickerstaff brainstem encephalitis (BBE) [9]
Diagnosis
General principles [9][10]
- A diagnosis of GBS is based on:
- Typical clinical features, e.g., rapidly progressive bilateral limb paresis and/or sensory involvement, with hyporeflexia or areflexia
- CSF analysis
- Electrodiagnostic studies
- Diagnostic criteria may be considered to support the diagnosis, e.g., the National Institute of Neurological Disorders and Stroke or Brighton criteria. [9][10]
- Evaluate patients for differential diagnoses of GBS, especially those with atypical presentations. [9]
- Consult a neurologist for all patients.
A complete neurological examination is required for all patients.
CSF analysis [2][7]
- Obtained to support diagnosis and rule out infectious and malignant causes
- Findings
- May be normal in the first 1–2 weeks of the disease [2]
- Typical: albuminocytologic dissociation, i.e., increased protein levels with WBCs normal or slightly elevated (typically < 10 cells/mcL) in CSF [11]
CSF cell count is typically normal in patients with GBS; consider other diagnoses in patients with a count > 50 cells/mcL. [11]
Electrodiagnostic studies
Nerve conduction studies [7][8]
- Obtained to support diagnosis and/or to classify GBS into subtypes
- Findings vary according to the subtype of GBS and may be normal during the early stages of disease.
- Signs of demyelination; in AIDP (e.g., ↓ nerve conduction velocity, conduction block, ↑ F‑wave latency)
- Signs of axonal damage in AMAN and AMSAN subtypes (e.g., ↓ CMAP amplitude)
- Sural nerve function is typically intact.
Nerve conduction study findings may be normal in the week following symptom onset or in patients with certain GBS clinical variants, e.g., Miller-Fisher syndrome. [9]
Electromyography
- Findings help differentiate between neuropathy and myopathy.
- Pathological spontaneous activity is a sign of an unfavorable prognosis.
- See “EMG findings of neuropathy vs. myopathy.”
Additional studies [7][9]
-
Routine laboratory studies
- CBC, CMP: to exclude differential diagnoses, e.g., infection or electrolyte disturbances
- See “Diagnostic workup for polyneuropathy” for further details.
-
Serological studies may be obtained to: [7]
- Identify the causative pathogen for epidemiological data, e.g., during outbreaks
- Detect specific autoantibodies, e.g., anti-GM1 antibodies, anti-GQ1b antibodies
-
Imaging studies: not routinely required but may help rule out differential diagnoses [2][9]
-
MRI spine with contrast
- Consider in patients with abrupt acute onset of paralysis and urinary retention to rule out a spinal cause. [2]
- Nerve root enhancement on gadolinium-enhanced MRI can support the diagnosis of GBS [9]
- MRI brain with contrast: Consider in patients with suspected CNS involvement.
-
MRI spine with contrast
Differential diagnoses
Differential diagnoses of Guillain-Barré syndrome [3][9]
See “Etiology of polyneuropathy” and “Differential diagnoses of polyneuropathy” for further details.
-
Peripheral polyneuropathies
- Chronic inflammatory demyelinating polyneuropathy
- Multifocal motor neuropathy
- Critical illness polyneuropathy
- Diabetic polyneuropathy
-
CNS-related
- Multiple sclerosis
- Transverse myelitis
- Poliomyelitis
- Spinal cord compression
- Brainstem syndrome
- Lyme disease
-
Metabolic or electrolyte disorders
- Hypokalemia
- Hypophosphatemia
- Hypoglycemia
- Hypothyroidism
- Porphyria
-
Vitamin deficiency
- Vitamin B1 deficiency
- Vitamin B12 deficiency
-
Muscle-related
- Myasthenia gravis
- Lambert-Eaton myasthenic syndrome
- Drug-induced myopathy
- Toxic myopathy (botulism, tetanus)
-
Other
- Vasculitides
- Diphtheria
- HIV
- Tick paralysis
- West Nile virus
Clinical features of Guillain-Barré syndrome vs. transverse myelitis
| Clinical features of Guillain-Barré syndrome vs. transverse myelitis | ||
|---|---|---|
| Guillain-Barré syndrome | Transverse myelitis | |
| Etiology |
|
|
| Symptom onset |
|
|
| Motor findings |
|
|
| Reflexes |
|
|
| Sensory findings |
|
|
| Autonomic dysfunction |
|
|
| Cranial nerve involvement |
|
|
| CSF examination |
|
|
| Imaging and findings |
|
|
| Electrophysiological findings |
|
|
The differential diagnoses listed here are not exhaustive.
Management
Approach [9]
- Screen for predictors of respiratory failure in GBS and provide respiratory support early if indicated.
- Consult neurology.
- Admit all patients for close monitoring and supportive management.
- Start medical treatment (IVIg or plasmapheresis) promptly in patients with indications.
- Monitor for symptom progression and provide management as needed, e.g., management of respiratory failure, bradycardia, dysphagia.
Even though many patients recover without treatment, hospital admission and multidisciplinary care are necessary because of the unpredictable course of the disease and risk of death.
Medical treatment [3][8][9]
-
Indications [9]
- Inability to walk > 10 meters unaided
- Severe autonomic dysfunction, e.g., cardiac arrhythmia
- Oropharyngeal dysphagia
- Respiratory failure
-
Options
- Intravenous immunoglobulin (IVIg) [3]
- Plasmapheresis
-
Special considerations: patients with clinical variants of GBS [9]
- Treatment decisions should be made by a specialist.
- Very limited variants, e.g., MFS, may not require medical treatment.
- In severe variants, e.g., BBE, treatment with IVIg or plasmapheresis may be indicated.
Glucocorticoids are not recommended for the treatment of GBS, as they have not been proven to hasten recovery or affect the prognosis. [9]
Monitoring for individuals with Guillain-Barré [9][12]
The frequency of reassessment should be based on clinical severity; follow local protocols when available.
-
Monitor respiratory muscle function frequently.
- Assess for clinical features of respiratory distress.
- Perform bedside pulmonary function tests (PFTs): vital capacity (VC), maximal inspiratory pressure (MIP), and maximal expiratory pressure (MEP)
-
Monitor autonomic function.
- Initiate continuous cardiac monitoring.
- Patients with cardiac autonomic dysfunction, e.g., severe bradycardia, may require a cardiac pacemaker.
- Assess regularly for bladder and/or bowel dysfunction, e.g., urinary retention, paralytic ileus.
- Frequently assess paresis and/or paralysis progression and swallowing function.
ICU-level care and intubation may be indicated.
Patients with bulbar palsy, involvement of the upper extremities, or autonomic dysfunction have an increased risk of respiratory failure. [3]
Respiratory support
Identify predictors of respiratory failure in GBS early to guide decisions about intubation, mechanical ventilation, and ICU admission. Manage respiratory failure urgently.
-
Predictors of respiratory failure in GBS [13][14]
- Clinical features at presentation
- Rapid progression (e.g., onset-to-peak disability interval < 7 days)
- Bulbar palsy
- Facial nerve palsy (especially bilateral)
- Neck weakness
- Autonomic dysfunction
- Bedside PFTs
- VC < 20 mL/kg or > 30% decline from baseline
- MIP less negative than -30 cm H2O or > 30% decline from baseline
- MEP < 40 cm H2O or > 30% decline from baseline
- Clinical features at presentation
- Clinical prediction rule: The Erasmus GBS Respiratory Insufficiency Score (EGRIS) can be used to predict the need for mechanical ventilation. [15]
-
Management: See “Management of respiratory failure” for a general approach.
-
Endotracheal intubation
- Consider early intubation: e.g., for airway protection in at-risk patients or to prevent complications of unplanned intubation.
- Avoid succinylcholine; use nondepolarizing NMJ blockers (e.g., rocuronium) if paralytic agents for intubation are indicated.
- Mechanical ventilation: Use a ventilation strategy for neuromuscular weakness.
-
Endotracheal intubation
Classic signs of respiratory distress and signs of impending respiratory failure typically occur late in GBS. Identify predictors of respiratory failure in GBS as early as possible. [13][14]
Succinylcholine is contraindicated in patients with GBS as it can cause life-threatening hyperkalemia and cardiac arrest. [16]
")
Supportive management [9]
- Manage neuropathic pain.
- NSAIDS and opioids are usually not effective.
- Consider gabapentin or carbamazepine.
- See “Analgesia for peripheral neuropathy” for dosage suggestions.
- Prevent complications.
- Prevention of decubitus ulcers
- Thromboprophylaxis for patients confined to bed: LMWH or low dose UFH, compression stockings [9]
- Early physiotherapy, physical rehabilitation, and psychosocial support
Disposition [9][12]
- All patients with suspected or confirmed GBS require inpatient evaluation and monitoring.
- Admit to ICU for any of the following life-threatening features of Guillain-Barré syndrome:" [9]
- Predictors of respiratory failure in GBS
- Signs of impending respiratory failure
- Rapid progression of paralysis
- Severe autonomic dysfunction, e.g., arrhythmia
- Severe dysphagia, reduced cough reflex, or signs of airway compromise
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
Prognosis
- Approx. 80% of patients with GBS regain the ability to walk unaided 6 months after symptom onset. [9]
- Consider calculating the modified Erasmus GBS Outcome Score (mEGOS) to predict the patient's ability to walk unaided.
-
3–7% of patients with GBS die as a result of complications, e.g.: [2][8]
- Respiratory muscle paralysis
- Sepsis
- Pulmonary embolism
- Cardiac arrest
- Patient factors associated with an increased risk of long-term disability include: [3]
- Rapid symptom progression
- Severe symptoms at peak of the disease
- Older age
- Axonal damage (e.g., in AMAN)
- It may take > 5 years for symptoms to improve and/or resolve. [9]
Death can occur as many as > 30 days after onset of symptoms, during the recovery phase.
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
Guillain-Barré syndrome in children
The etiology of Guillain-Barré syndrome is similar in children and adults. [17]
Clinical features [17]
- Clinical features of Guillain-Barré syndrome that often occur within 6 weeks after a GI infection or URTI [9]
- Children < 6 years of age may present with nonspecific symptoms, e.g.: [9][18]
- Nonlocalized pain
- Irritability
- Refusal and/or inability to bear weight
- Meningismus
- Unsteady gait
Diagnosis [9][17]
-
Diagnosis of Guillain-Barré syndrome is similar in adults and children and is typically based on the following:
- Clinical features of Guillain-Barré syndrome
- CSF analysis that demonstrates albuminocytologic dissociation
- Electrodiagnostic studies
- Diagnostic considerations in young children
- Electrodiagnostic studies may not be feasible.
-
MRI spine with contrast may be used to:
- Assess for nonspecific nerve root enhancement to support the diagnosis
- Rule out alternative diagnoses
Differential diagnoses [3][9][19]
See "Differential diagnoses of Guillain-Barré syndrome." Important conditions to consider in children include the following:
- Acute cerebellar ataxia [9][20]
- Acute flaccid myelitis
- Acute disseminated encephalomyelitis
- Myositis
- Spinal cord tumor
- Botulism (especially in infants)
- Tick paralysis
- Functional neurological disorder
- Metabolic disorders
Management [9][17][18]
- Signs of pediatric respiratory distress: Provide immediate pediatric respiratory support.
- Admit all patients and consult neurology.
- Patients with life-threatening features of Guillain-Barré: Admit to ICU.
- Other patients: Ensure close monitoring for individuals with Guillain-Barré.
- Assess the need for immunomodulatory therapy and administer if indicated.
- Recommended for an acute inability to walk and/or life-threatening features of Guillain-Barré
- Considered for mild disease presenting within 2 weeks of symptom onset [18]
- Options: IVIg (preferred, off-label) OR plasma exchange [9][18]
- Provide supportive care during hospitalization and after discharge, including:
- Pediatric pain management
- Physical therapy
Up to 20% of children with Guillain-Barré syndrome require mechanical ventilation; monitor respiratory status closely. [17]
Due to the risk of reduced vaccine efficacy, avoid administering live vaccines until 8–11 months after receiving IVIG treatment at doses recommended for Guillain-Barré syndrome. [21]
References
- "Guillain-Barré Syndrome". https://web.archive.org/web/20201229211121/https://www.cdc.gov/campylobacter/guillain-barre.html. [2019-12-20]
- Yuki N, Hartung HP. "Guillain–Barré Syndrome". N Engl J Med. 366. :2294-2304. (2012)
- Walling AD, Dickson G. "Guillain-Barré syndrome". Am Fam Physician. 87(3). :191-7. (2013)
- Uncini A, Vallat J-M, Jacobs BC. "Guillain-Barré syndrome in SARS-CoV-2 infection: an instant systematic review of the first six months of pandemic". Journal of Neurology, Neurosurgery & Psychiatry. 91(10). :1105-1110. (2020)
- Hartung HP. "Infections and the Guillain-Barré Syndrome". J Neurol Neurosurg Psychiatry. 66. :277. (1999)
- Nelson KE. "Invited Commentary: Influenza Vaccine and Guillain-Barre Syndrome--Is There a Risk?". Am J Epidemiol. 175(11). :1129-1132. (2012)
- Van Den Berg B, Walgaard C, Drenthen J, et al. "Guillain–Barré syndrome: pathogenesis, diagnosis, treatment and prognosis". Nature Reviews Neurology. 10. :469–482. (2014)
- Willison HJ, Jacobs BC, van Doorn PA. "Guillain-Barré syndrome". Lancet. 388. :717-727. (2016)
- Leonhard SE, Mandarakas MR, Gondim FAA, et al. "Diagnosis and management of Guillain–Barré syndrome in ten steps". Nat Rev Neur. 15(11). :671-683. (2019)
- Asbury AK, Cornblath DR. "Assessment of current diagnostic criteria for Guillain-Barré syndrome". Ann Neurol. 27(S1). :S21-S24. (1990)
- Al-Hakem H, Doets A, Stino A, et al. "CSF Findings in Relation to Clinical Characteristics, Subtype, and Disease Course in Patients With Guillain-Barré Syndrome". Neurology. 100(23). (2023)
- Matthew Harms. "Inpatient Management of Guillain-Barré Syndrome". The Neurohospitalist. 1(2). :78-84. (2011)
- Umer SR, Nisa Q, Kumari M, et al. "Clinical Features Indicating the Need for Mechanical Ventilation in Patients with Guillain Barre Syndrome". Cureus. (2019)
- Lawn ND, Fletcher DD, Henderson RD, Wolter TD, Wijdicks EFM. "Anticipating Mechanical Ventilation in Guillain-Barré Syndrome". Arch Neurol. 58(6). :893. (2001)
- Doets AY, Walgaard C, Lingsma HF, et al. "International Validation of the Erasmus Guillain–Barré Syndrome Respiratory Insufficiency Score". Ann Neurol. 91(4). :521-531. (2022)
- Martyn JAJ, Richtsfeld M, Warner DO. "Succinylcholine-induced Hyperkalemia in Acquired Pathologic States". Anesthesiology. 104(1). :158-169. (2006)
- Ryan M. "Pediatric Guillain-Barré syndrome". Curr Opin Pediatr. 25(6). :689-693. (2013)
- van Doorn P, Van den Bergh P, Hadden R, et al. "European Academy of Neurology/Peripheral Nerve Society Guideline on diagnosis and treatment of Guillain–Barré syndrome". Eur J Neurol. 30(12). :3646-3674. (2023)
- Kliegman RM, Geme JS. "Nelson Textbook of Pediatrics, 2-Volume Set". Elsevier. :3623-3633. (2019). ISBN: 9780323529501
- Overby P, Kapklein M, Jacobson R. "Acute Ataxia in Children". Pediatr Rev. 40(7). :332-343. (2019)
- Committee on Infectious Disease, American Academy of Pediatrics. "Red Book: 2024-2027 Report of the Committee on Infectious Diseases, 33rd Edition". American Academy of Pediatrics. (2024). ISBN: 9781610027373