Summary
Helminths (i.e., parasitic worms) are a group of macroparasites encompassing a variety of species that can infect their hosts in three different ways: ingestion of eggs or larvae (e.g., via contaminated food and water or fecal-oral route), direct penetration of the skin, and via vector bites (e.g., certain species of flies and mosquitoes). Helminths are classified based on their macroscopic appearance as nematodes (i.e., roundworms; genera include Ascaris, Enterobius, Trichuris, Toxocara, Trichinella, Ancylostoma, Necator, Strongyloides, Loa, Onchocerca, Wuchereria, Mansonella, Dracunculus, Gnathostoma, Anisakis, Capillaria, and Trichostrongylus), cestodes (i.e., tapeworms; genera include Taenia, Dibothriocephalus, Echinococcus, Hymenolepis, and Dipylidium), or trematodes (i.e., flukes; genera include Schistosoma, Clonorchis, Paragonimus, Fasciola, Dicrocoelium, and Opisthorchis). Most helminth species colonize the gastrointestinal tract of their hosts, causing symptoms such as abdominal pain, nausea, and diarrhea. The larvae of certain helminth species, such as those of the Ascaris and Ancylostoma genus, migrate from the intestines via the portal vein to the lungs, potentially causing asthma-like symptoms (e.g., dry cough, wheezing). Other species such as Taenia solium can colonize other human tissue, such as the brain or liver, which can lead to life-threatening complications (e.g., neurocysticercosis). Diagnosis of helminth infection is primarily based on eosinophilia in the blood and direct detection of worms, eggs, or larvae in stool samples. Serum IgE levels are often elevated. Treatment consists of anthelmintic agents, such as albendazole or praziquantel.
See also “Echinococcosis,” “Schistosomiasis,” and “Strongyloidiasis.” See “General parasitology” for an overview of all parasites.
Nematodes (roundworms)
Nematodes (roundworms) are long, thin, unsegmented, tube-like worms with a longitudinal digestive tract opening at both ends. Adult worms form separate sexes, and females are usually larger than males. Filarial nematodes are thread-like nematodes transmitted to humans through arthropod vectors.
| Overview of nematode infections [1] | ||||||
|---|---|---|---|---|---|---|
| Disease | Pathogen | Mode of transmission | Clinical features | Diagnostics | Treatment [2] | |
| Ascariasis |
|
|
|
|
|
|
| Enterobiasis (pinworm) |
|
|
|
|
||
| Trichuriasis (whipworm) |
|
|
|
|
||
| Toxocariasis |
|
|
|
|
||
| Trichinellosis |
|
|
|
|
|
|
| Hookworm (ancylostomiasis, necatoriasis) |
|
|
|
|
|
|
| Strongyloidiasis |
|
|
|
|
||
| Filariasis | Loiasis |
|
|
|
|
|
| Onchocerciasis |
|
|
|
|
|
|
| Lymphatic filariasis |
|
|
|
|
|
|
| Mansonellosis [3][4][5] |
|
|
|
|
|
|
| Dracunculiasis (Guinea worm disease) |
|
|
|
|
|
|
| Gnathostomiasis |
|
|
|
|
|
|
| Anisakiasis [7][8][9] |
|
|
|
|
|
|
| Intestinal capillariasis [10][11][12] |
|
|
|
|
|
|
| Trichostrongylosis [13][14] |
|
|
|
|
|
|
Eating a Toxic TrEAT: Toxocara, Trichiniella, Enterobius, Ascaris, and Trichiuris are transmitted by ingestion.
SANd on your Shins, Ancles, and Neck: Strongyloides, Ancylostoma, and Necator penetrate the skin while walking on sand.
The OWL bites: Onchocerca, Wuchereria, and Loa loa are transmitted by bites.
Ascariasis
-
Pathogen
- Ascaris lumbricoides (giant roundworm)
- Ascaris are nematodes.
- Epidemiology: : most common helminth infection worldwide (mainly affects children in tropical countries with low standards of hygiene)
- Mode of transmission: : fecal-oral (infection occurs in the larval state following the consumption of contaminated food, especially raw vegetables that have been contaminated by human waste used as a fertilizer)
- Life cycle: Host ingests eggs → Eggs hatch and release larvae → Larvae invade intestinal walls → Larvae migrate to lungs via portal vein → Larvae migrate into alveoli, trachea (“tracheal migration”), and larynx → Larvae are expectorated into the mouth and swallowed back into the intestine → Larvae return to the intestine → Larvae mature into adult worms, which then lay new eggs.
-
Clinical features
- Most patients are asymptomatic.
-
Early symptoms
- Dry cough, blood-tinged sputum, wheezing
- Loeffler syndrome: a transient respiratory disorder characterized by accumulation of eosinophils in the lungs due to certain infections (usually parasites) or allergic reactions to drugs. Symptoms are usually mild and resolve spontaneously
- Late symptoms : anorexia, abdominal discomfort, nausea, vomiting, and diarrhea
- Additional symptoms due to blockage by adult worms depend on the location of the obstruction:
- Bowel obstruction, especially at ileocecal valve (may lead to intestinal perforation)
- Obstruction of the appendix → features of appendicitis
- Obstruction of biliary and pancreatic ducts → features of cholestasis, pancreatitis
-
Diagnostics [1]
- CBC shows eosinophilia. [15]
- Confirmatory test: Stool samples show worms or visible oval eggs with a knobby appearance under the microscope.
-
Treatment [2]
-
Preferred
- Albendazole (off-label) [2]
- OR mebendazole [2]
- Alternative (all off-label): pyrantel pamoate, ivermectin, nitazoxanide
-
Preferred
-
Prevention [2]
- Proper disposal of human feces
- Thoroughly wash and cook vegetables.
- In high-prevalence areas, chemoprophylaxis for high-risk individuals [16]
")
")

")

A type of soil-transmitted helminth; 15-cm long specimen.
Source: © IMPP
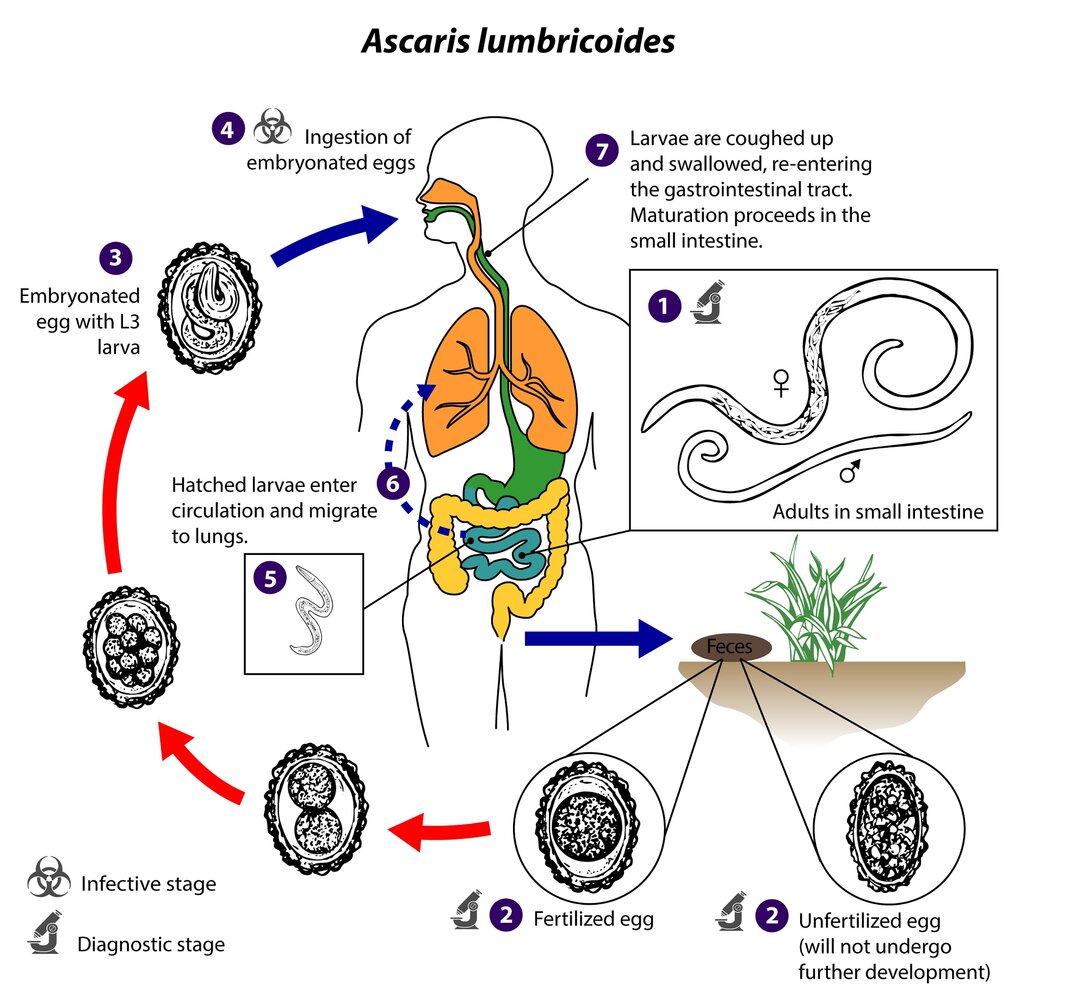
1. Diagnostic stage: Adult roundworms colonize the small intestine of the definitive host, where they produce approx. 200,000 eggs per day.
2. Diagnostic stage: The eggs are excreted with the feces.
3. Larvae develop within the embryonated eggs, becoming infective (L3) within approx. 18 days under optimal conditions (warm and moist soil protected from direct sunlight).
4. Infective stage: The end host ingests the embryonated eggs with poorly washed and/or undercooked produce.
5–6. The larvae hatch in the small intestine and enter the circulation via the intestinal mucosa, from where they migrate to the lungs.
7. In the lungs, the larvae continue to mature, penetrate the alveolar walls, and ascend the bronchial tree to the pharynx, from where they are coughed up and swallowed by the host, migrating back to the small intestine, where they mature into adult roundworms.
This image is an adaptation. Source of original image: CDC/ DPDx. Original title: “Ascariasis”. Created by: CDC/ DPDx. Licensed under Public Domain. Modifications to original image: CDC/DPDx logo removed by request.
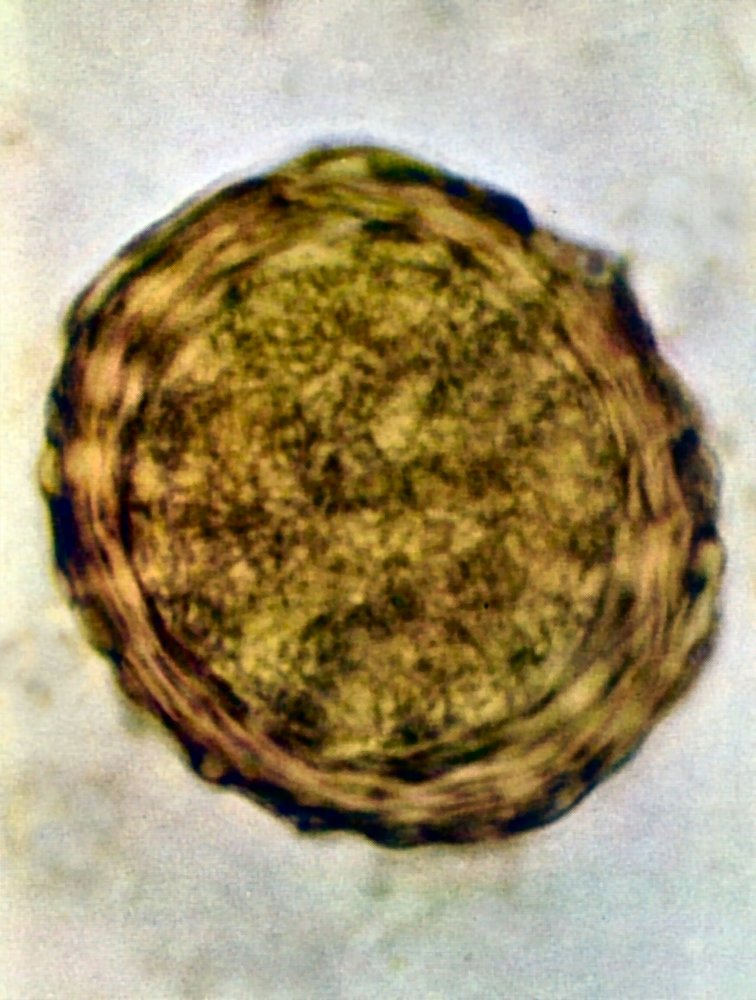
Photomicrograph of a wet mount of human feces
A yellowish-brown, round ovum with a knobby (mammillated) outer layer is visible.
This is the typical appearance of an Ascaris lumbricoides egg (the round shape indicates that it is fertilized).
Source: “Ascaris lumbricoides” by GrahamColm, Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}
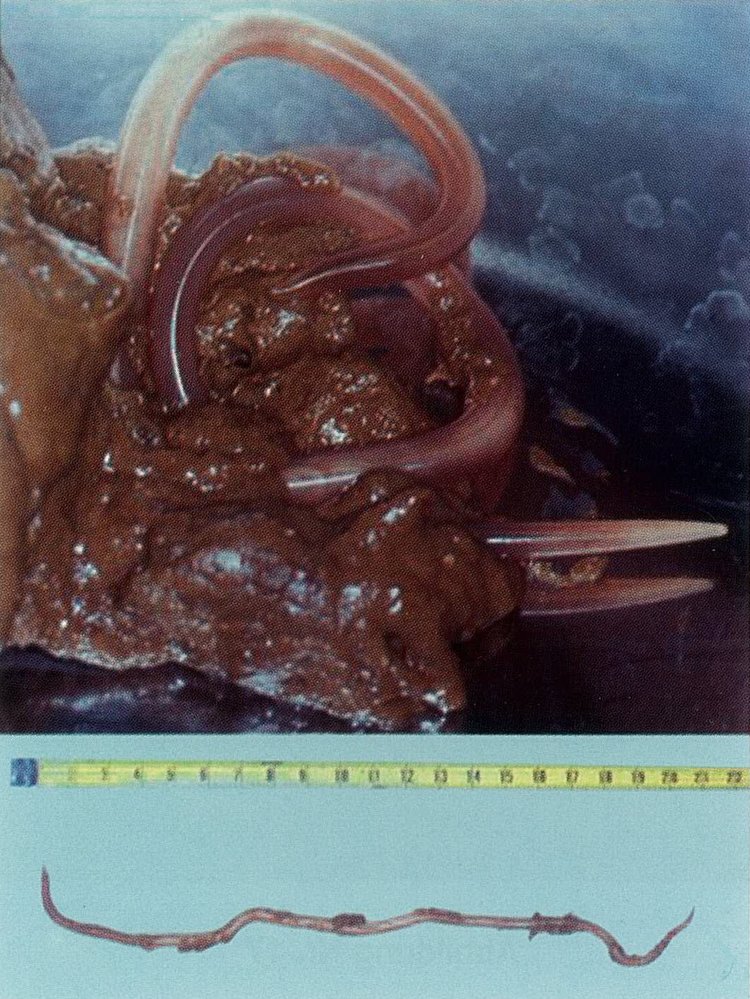
Stool sample with a 20-cm long specimen.
Source: © IMPP
Enterobiasis
-
Pathogen
- Enterobius vermicularis (pinworm)
- Pinworms are nematodes.
-
Epidemiology [17]
- Most common helminthic infection in the US
- Prevalence in the US: ∼ 12%
- Primarily affects children 5–10 years of age
-
Mode of transmission
- Initial infection: fecal-oral
- Reinfection: digital-oral after scratching anal region
-
Clinical features
- Anal pruritus (especially at night)
- Vulvovaginitis, especially in children
- Occasionally, symptoms of intestinal infection (i.e., nausea, vomiting, and abdominal pain which may become severe enough to mimic appendicitis)
-
Diagnostics [1]
- Tape test: microscopic detection of oval eggs (ova) and/or pinworms on tape that has been pressed against the perianal region
- Stool examination is not recommended because eggs and worms are rarely found in stool.
-
Treatment [2]
- Mebendazole (off-label) [2]
- OR pyrantel pamoate (off-label) [2]
- OR albendazole (off-label) [2]
-
Prevention [2]
- Consider treating the whole household to prevent reinfection.
- Encourage
- Daily hygiene (e.g., bathing, nail clipping, handwashing)
- Frequent washing of bedding and underwear
Enterobius commonly manifests with perianal pruritus.

")
")


Photomicrograph of a specimen prepared by applying cellulose tape to the anal region of a patient (very high magnification)
Eight transparent, elongated oval eggs, which are flattened asymmetrically on one side can be seen.
Source: "5229; Enterobius vermicularis", CDC, Centers for Disease Control and Prevention, Atlanta,USA licensed under Public Domain
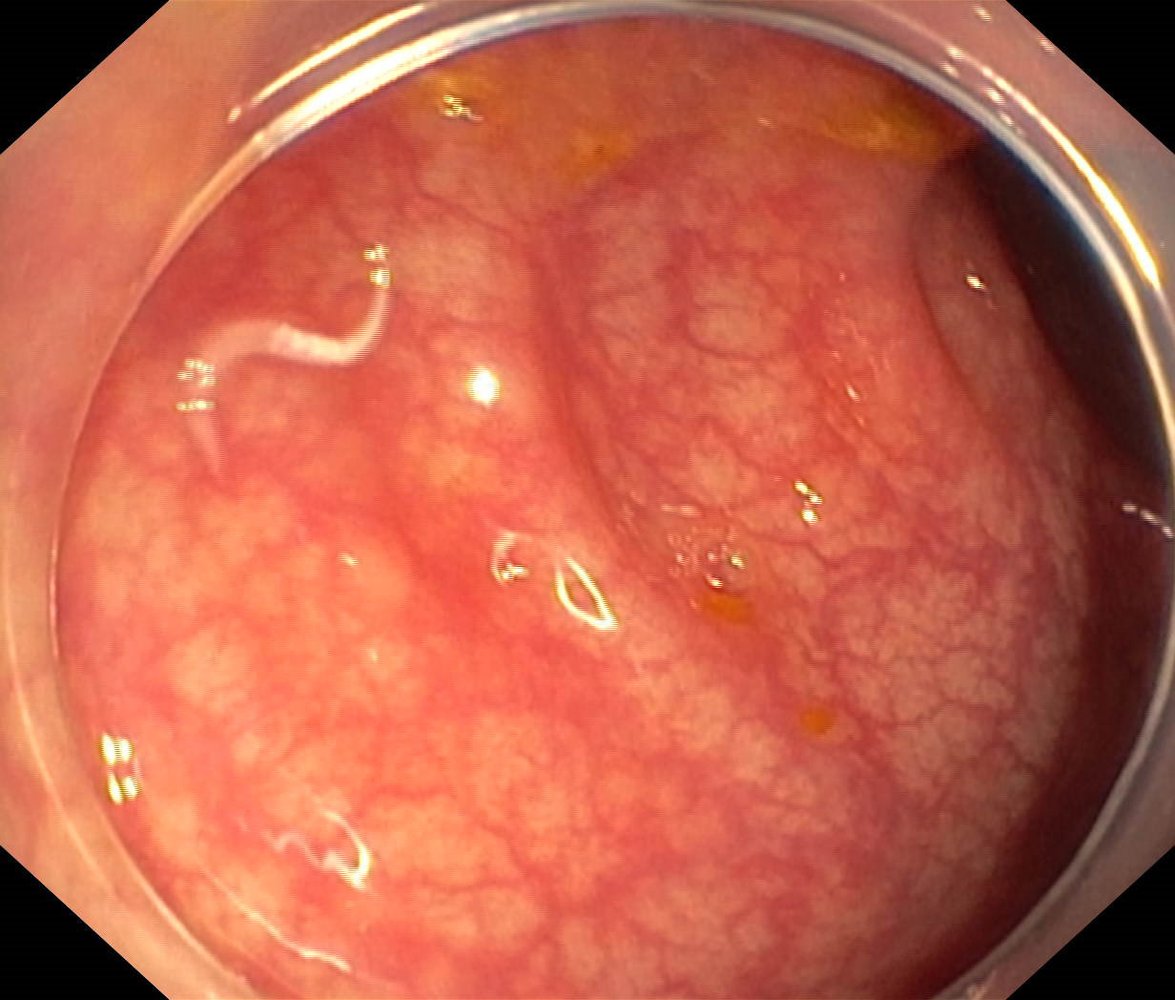
Endoscopic view of the colon
A worm is visible in the colon (green overlay). The surrounding mucosa's surface and vascular pattern appear normal.
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.
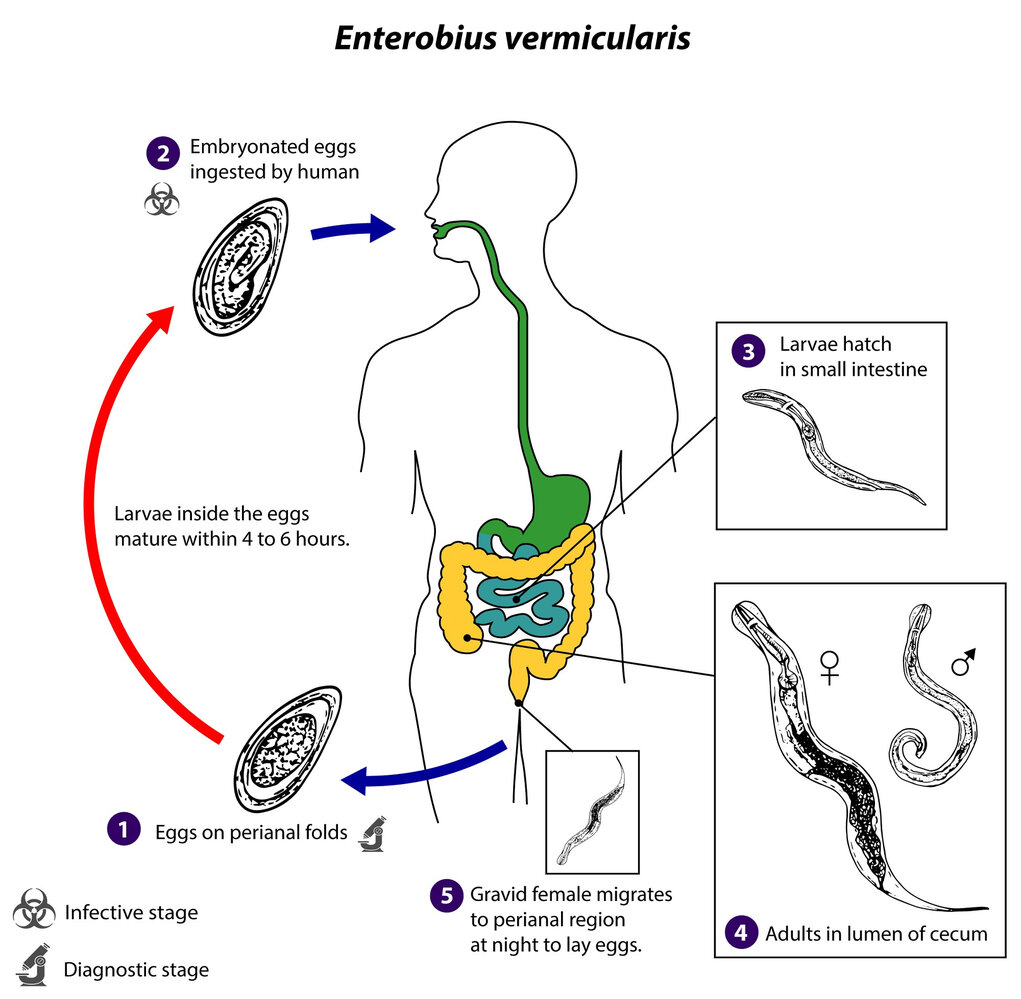
1. Diagnostic stage: Gravid, female pinworms deposit eggs on the perianal region of a human (definitive host). Under optimal conditions, the larvae in the eggs mature within 4–6 hours.
2. Infective stage: The eggs are spread in the environment (e.g., through contamination of clothing or bed sheets) and by the host scratching the perianal region and contaminating foods or surfaces. Infection occurs via ingestion of infective eggs. Autoreinfection occurs by transfer of eggs from the hands to the mouth.
3. The larvae hatch in the small intestine and migrate to the colon, where they mature (approx. 1 month).
4. Adult Enterobius vermicularis reside in the lumen of the cecum.
5. Gravid female Enterobius vermicularis migrate to the perianal region nocturnally to deposit eggs.
This image is an adaptation. Source of original image: CDC/ DPDx. Original title: “Enterobius vermicularis”. Created by: CDC/ DPDx. Licensed under Public Domain. Modifications to original image: CDC/DPDx logo removed by request.
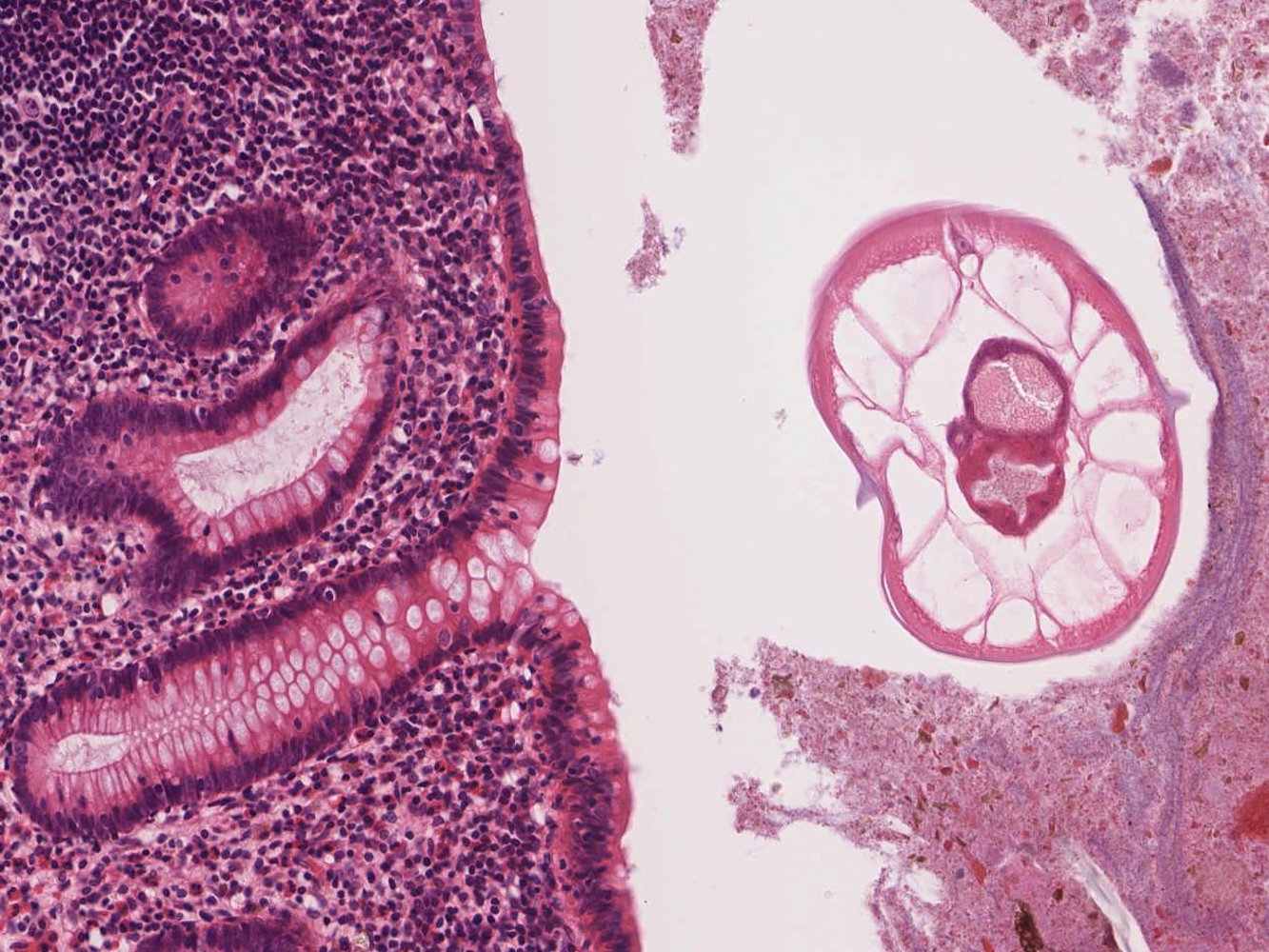
Photomicrograph of a tissue biopsy specimen of the appendix (H&E stain; high magnification)
Enterobius vermicularis (green overlay) with hooks (red overlay) for attachment to the intestinal wall is visible within the lumen of the appendix.
Click on the Smartzoom button to view the entire specimen through a virtual microscope.
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: PD Dr. Alberto Perez Bouza
Trichiuriasis
-
Pathogen
- Trichuris trichiura (whipworm)
- Whipworms are nematodes.
- Mode of transmission: : fecal-oral
- Life cycle: Host ingests eggs → Eggs hatch and release larvae in the small intestine → Larvae mature into adult worms in colon → Adult worms lay eggs, which are shed in feces.
-
Clinical features
- Mostly asymptomatic
- In children: severe infection causes diarrhea, iron deficiency anemia, growth retardation, rectal prolapse
-
Diagnostics [1]
- Microscopic examination of stool for eggs [1]
- Proctoscopy or colonoscopy may reveal adult worms.
-
Treatment [2]
- Mebendazole [2]
- OR albendazole (off-label) with or without ivermectin (off-label) [2]
-
Prevention [2]
- Proper hygiene and disposal of human waste
- In high-prevalence areas, chemoprophylaxis for high-risk individuals [16]
")

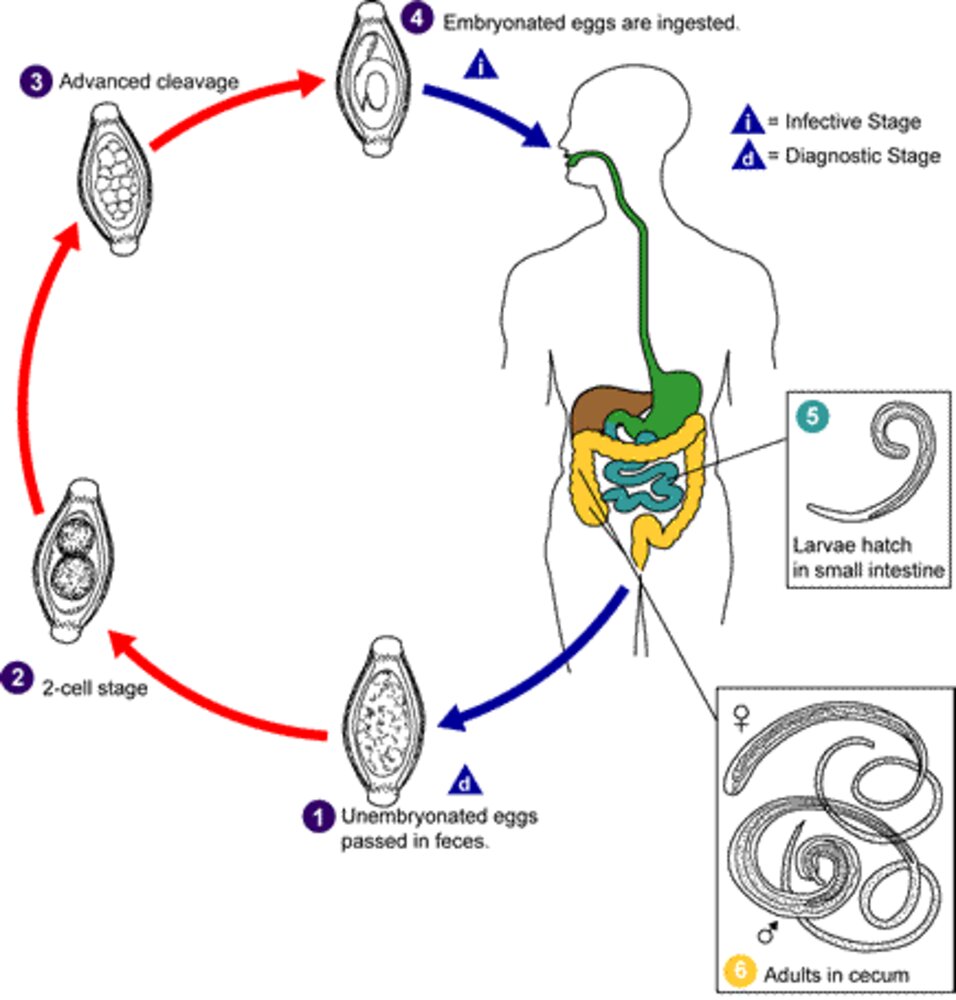
1. Diagnostic stage: Unembryonated eggs are excreted with the stool of an infected human (definitive host).
2–3. In soil, the eggs go through a 2-cell and an advanced-cleavage stage before they embryonate and become infective.
4. Infective stage: The infective, embryonated eggs are ingested with raw food or soil-contaminated hands.
5–6 . The larvae hatch in the small intestine and develop into adult worms that typically colonize the cecum.
This image is an adaptation. Source of original image: CDC/ DPDx. Original title: “Trichuriasis”. Created by: CDC/ DPDx. Licensed under Public Domain. Modifications to original image: CDC/DPDx logo removed by request.

Photomicrograph of a wet stool mount (very high magnification)
Barrel-shaped, thick-walled eggs with bipolar hyaline protuberances are visible, which are characteristic of Trichuris trichiura (whipworm).
Source: "ID#: 630", Centers for disease control and prevention, Centers for disease control and prevention licensed under Public Domain
Toxocariasis
-
Pathogen
- Toxocara canis (dog roundworm), Toxocara mystax/Toxocara cati (cat roundworm)
- Toxocara are nematodes.
- Mode of transmission: : fecal-oral (ingestion of Toxocara eggs from an infected dog or cat feces, e.g., in contaminated playground sand or garden soil) [18]
- Incubation period: 2–4 weeks
-
Clinical features
-
Visceral toxocariasis (also called visceral larva migrans): caused by larvae migrating through the intestinal wall into the blood and reaching other organs
- Fever and flu-like symptoms
- Additional symptoms depend on the affected organs
- Liver: hepatomegaly and abdominal pain
-
Lungs
- Dyspnea, wheezing, cough, pneumonia
- Loeffler syndrome
- Skin: rash
- Heart: myocarditis
- CNS (also called neural larva migrans): seizures, coma
-
Ocular toxocariasis (also called ocular larva migrans): caused by larvae migrating into the eye
- Unilateral impairment or loss of vision and resulting strabismus
- Leukocoria
- Inflammation, scarring, and possible detachment of the retina
-
Visceral toxocariasis (also called visceral larva migrans): caused by larvae migrating through the intestinal wall into the blood and reaching other organs
-
Diagnostics [1]
- CBC: leukocytosis with eosinophilia, anemia
- Hypergammaglobulinemia (↑ serum total IgE)
- Serology: ELISA for Toxocara antibodies in serum or vitreous fluid
- Advanced imaging (e.g., ultrasound, CT, MRI) may show diffuse nodular lesions on the liver.
-
Treatment [2]
- Albendazole (off-label) [2]
- OR mebendazole (off-label) [2]
- Specialist consult (e.g., ophthalmology) depending on affected organs
-
Prevention [2]
- Proper disposal of animal feces
- Deworm animals regularly.


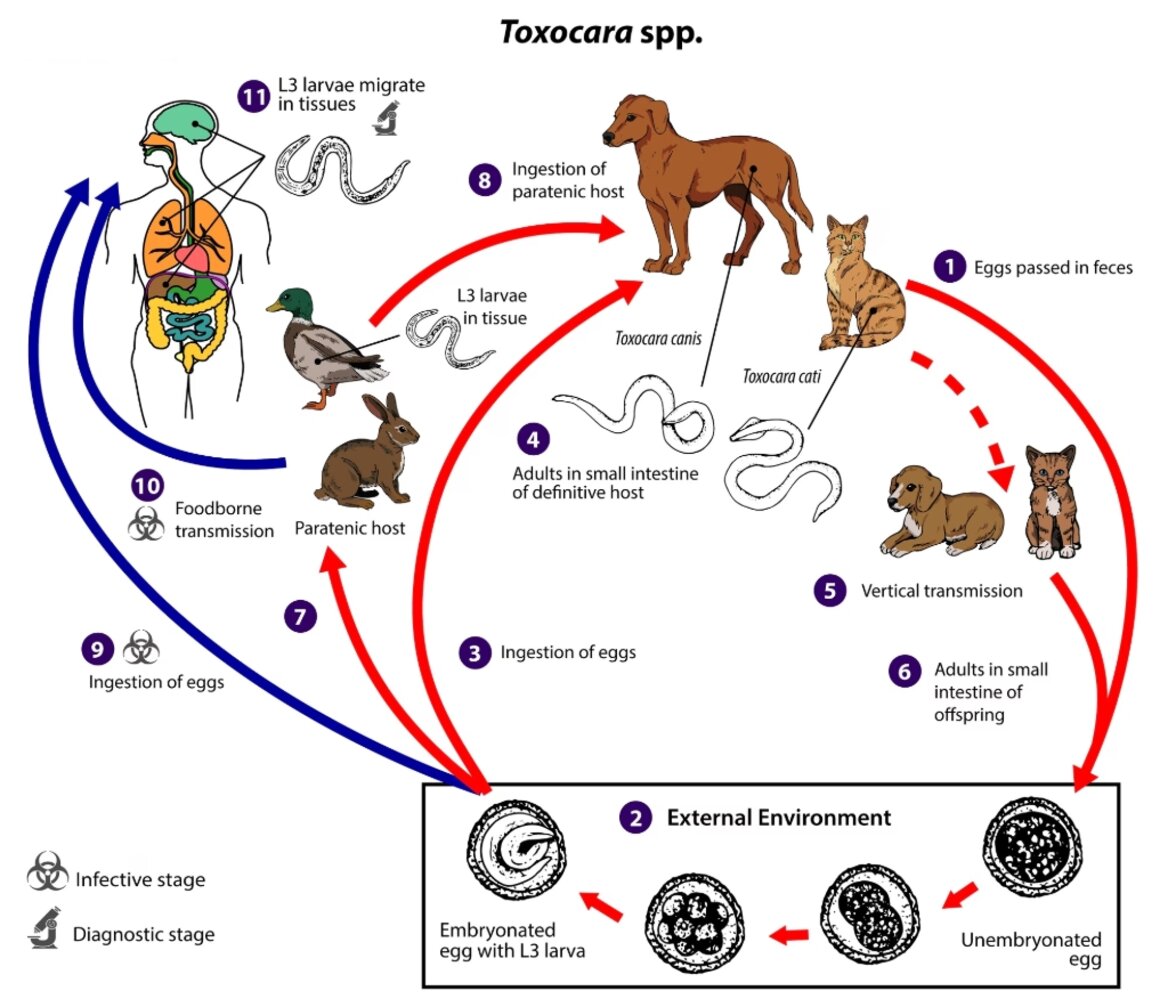
Toxocara spp. can follow a direct (one host) or indirect (multiple host) life cycle. Unembryonated eggs are shed in the feces of the definitive host (canids: T. canis; felids: T. cati) (1). Eggs embryonate over a period of 1 to 4 weeks in the environment and become infective, containing third-stage (L3) larvae (2). Following ingestion by a definitive host (3), the infective eggs hatch, and larvae penetrate the gut wall. In younger dogs (T. canis) and in cats (T. cati), the larvae migrate through the lungs, bronchial tree, and esophagus, where they are coughed up and swallowed into the gastrointestinal tract; adult worms develop and oviposit in the small intestine (4). In older dogs, patent (egg-producing) infections can also occur, but larvae more commonly become arrested in tissues. Arrested larvae are reactivated in female dogs during late gestation and may infect pups by the transplacental (major) and transmammary (minor) routes (5) in whose small intestine adult worms become established (6). In cats, T. cati larvae can be transmitted via the transmammary route (5) to kittens if the dam is infected during gestation, but somatic larval arrest and reactivation does not appear to be important as in T. canis.
Toxocara spp. can also be transmitted indirectly through ingestion of paratenic hosts. Eggs ingested by suitable paratenic hosts hatch and larvae penetrate the gut wall and migrate into various tissues where they encyst (7). The life cycle is completed when definitive hosts consume larvae within paratenic host tissue (8), and the larvae develop into adult worms in the small intestine.
Humans are accidental hosts who become infected by ingesting infective eggs (9) or undercooked meat/viscera of infected paratenic hosts (10). After ingestion, the eggs hatch and larvae penetrate the intestinal wall and are carried by the circulation to a variety of tissues (liver, heart, lungs, brain, muscle, eyes) (11). While the larvae do not undergo any further development in these sites, they can cause local reactions and mechanical damage that causes clinical toxocariasis. (Materials developed by CDC)
This image is an adaptation. Source of original image: CDC/ DPDx. Original title: “Toxocariasis”. Created by: CDC/ DPDx. Licensed under Public Domain. Modifications to original image: CDC/DPDx logo removed by request.
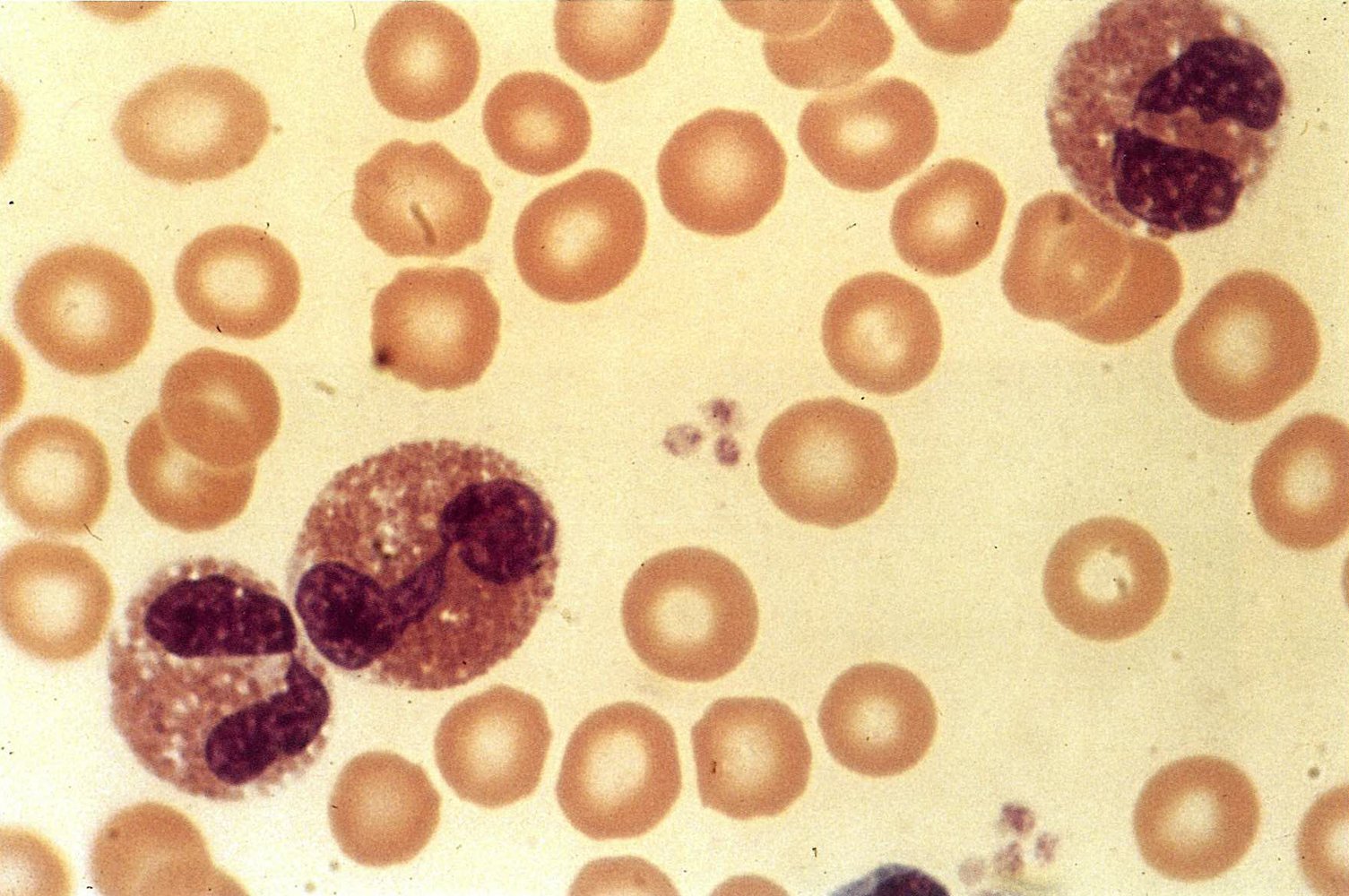
Blood smear showing many erythrocytes and three eosinophil granulocytes, which indicates eosinophilia in toxocariasis (T = thrombocytes, EG = eosinophil granulocytes).
Source: © IMPP
Trichinellosis
-
Pathogen
- Trichinella spiralis and other Trichinella spp.
- Trichinella are nematodes.
-
Mode of transmission
- Consumption of undercooked meat (especially pork) containing encysted larvae
- Fecal-oral (rarely)
- Life cycle: Host ingests meat that contains cysts → Larvae invade the small bowel mucosa → Larvae develop into adult worms → Adult worms release larvae, which then migrate to muscles, where they encyst.
- Incubation period: 7–30 days [19]
-
Clinical features
- Intestinal phase : abdominal pain, diarrhea, nausea, and vomiting
- Muscle phase
- Myositis: myalgia, muscle swelling, weakness
- Periorbital edema
- Other symptoms include: fever, rash, splinter hemorrhages, retinal and conjunctival hemorrhages, chemosis
-
Diagnostics [1]
- CBC: eosinophilia
- Elevated muscle enzymes (e.g., ↑ creatine kinase, ↑ lactate dehydrogenase)
- Serologic testing for antibodies
- Rarely: muscle biopsy
-
Treatment [2]
- Albendazole (off-label) [2]
- OR mebendazole (off-label) [2]
- Consider corticosteroids if symptoms are severe.
-
Complications
- Cardiac: ECG changes (e.g., arrhythmias)
- CNS: meningitis, encephalitis
- Pulmonary: myositis involving respiratory muscles, pneumonia
-
Prevention [2]
- Cook food thoroughly.
- Known exposure in the previous 6 days: prophylactic treatment
Consider trichinella infection in patients with myositis, periorbital edema, and eosinophilia.

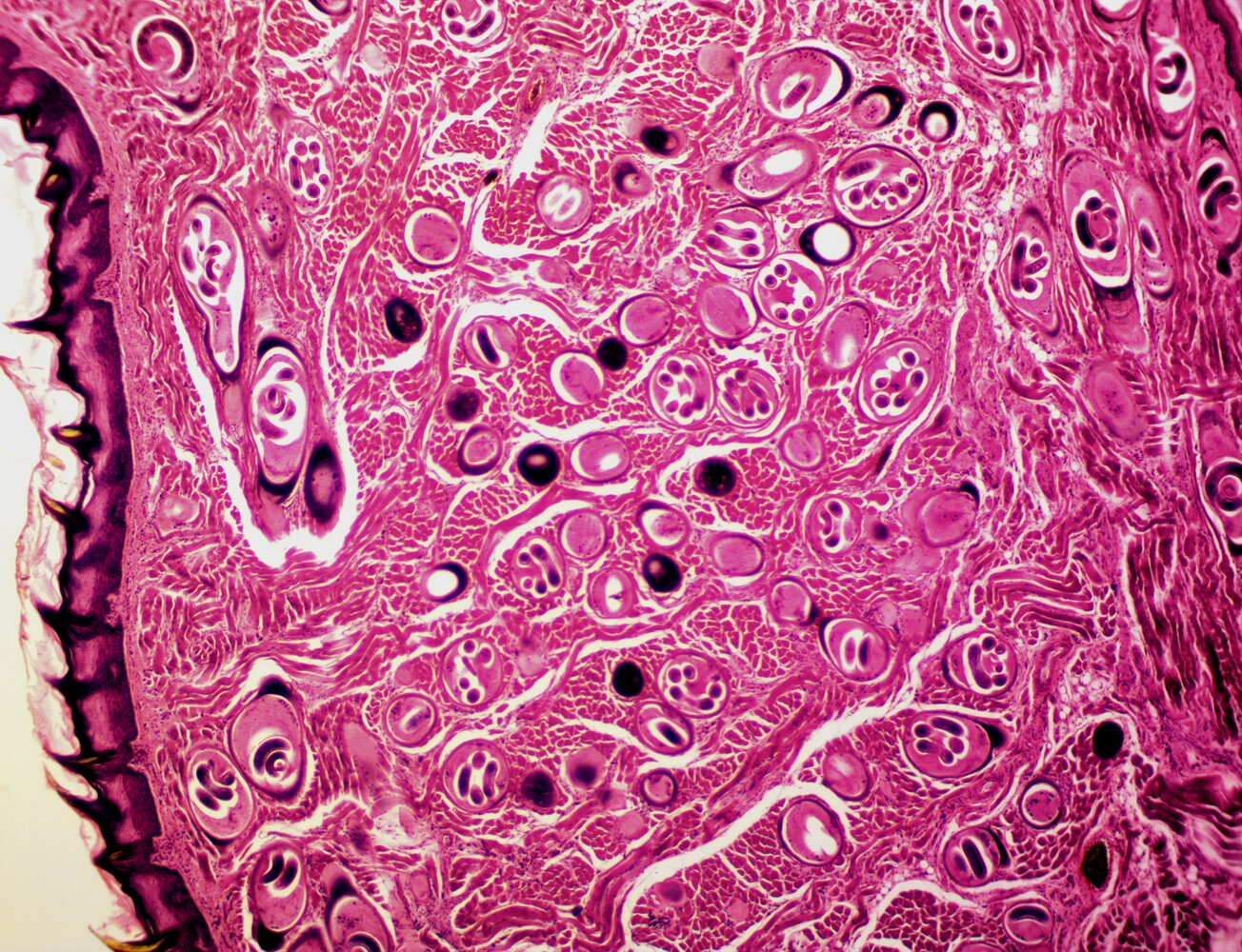
Photomicrograph of a striated muscle tissue specimen (H&E stain; low magnification)
Multiple encysted Trichinella spiralis larvae are visible throughout the sample. Most of the parasites are shown in cross-section (green overlay), some are visible in longitudinal section (green arrowhead).
Source: “Trichinella Spiralis x.s. & l.s. 40x.png” by TheMrGrove, Wikimedia Commons, licensed under CC BY-SA 4.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 4.0.
{kind=link}
Hookworm infections (ancylostomiasis; necatoriasis)
-
Pathogen [20]
- Human hookworms: Ancylostoma duodenale and Necator americanus
- Zoonotic hookworms, i.e., cat and dog hookworms ; (Ancylostoma braziliense; and Ancylostoma caninum) can also infect humans.
- Hookworms are nematodes.
- Mode of transmission: percutaneous penetration of larvae (primarily via the feet, e.g., while walking on a beach)
-
Life cycle
- Human hookworm: Soil is contaminated with human feces containing hookworm eggs → Eggs hatch and release larvae → Larvae penetrate skin (usually the feet) → Larvae migrate to lungs via blood and lymphatic vessels → Larvae migrate via bronchi and trachea to the larynx → Larvae are expectorated and swallowed back into the intestine → Larvae mature into adult worms that colonize the intestinal tract → Female hookworms lay eggs in the intestine → Eggs are eliminated with the feces.
- Zoonotic hookworms are usually unable to break through the basement membrane; after entering the human epidermis (humans are accidental intermediate hosts) → Migration through the epidermis for several weeks.
-
Clinical features
-
Cutaneous symptoms
- At entry site: pruritus, erythema, maculopapular rash
- Cutaneous larva migrans (CLM): serpiginous marks (cutaneous lesion with a progressive, creeping, snake-like border) representing larval tracks
- In zoonotic hookworm infections, only cutaneous symptoms are present.
- Respiratory tract: dry cough, wheezing, Loeffler syndrome
- Intestine: abdominal pain, weight loss, nausea, vomiting, diarrhea
- Microcytic anemia (hookworms ingest blood from the intestinal wall)
-
Cutaneous symptoms
-
Diagnostics [1]
- Human hookworms
- CBC may show eosinophilia and microcytic anemia. [21]
- Microscopic examination of stool for eggs [22]
- Zoonotic hookworms: clinical diagnosis based on visualization of cutaneous larva migrans
- Human hookworms
-
Treatment [2]
- Human hookworm
- Albendazole (off-label) [2]
- OR mebendazole (off-label) [2]
- OR pyrantel pamoate (off-label) [2]
-
Zoonotic hookworms (cutaneous larva migrans)
- Albendazole (off-label) [2]
- OR ivermectin (off-label) [2]
- Human hookworm
-
Prevention [2]
- Proper disposal of human and animal waste
- Wear shoes to protect feet from exposure to soil.
- In high-prevalence areas, chemoprophylaxis for high-risk individuals [16]
Consider hookworm infection in patients who present with a history of recent travel to a tropical country and microcytic anemia.


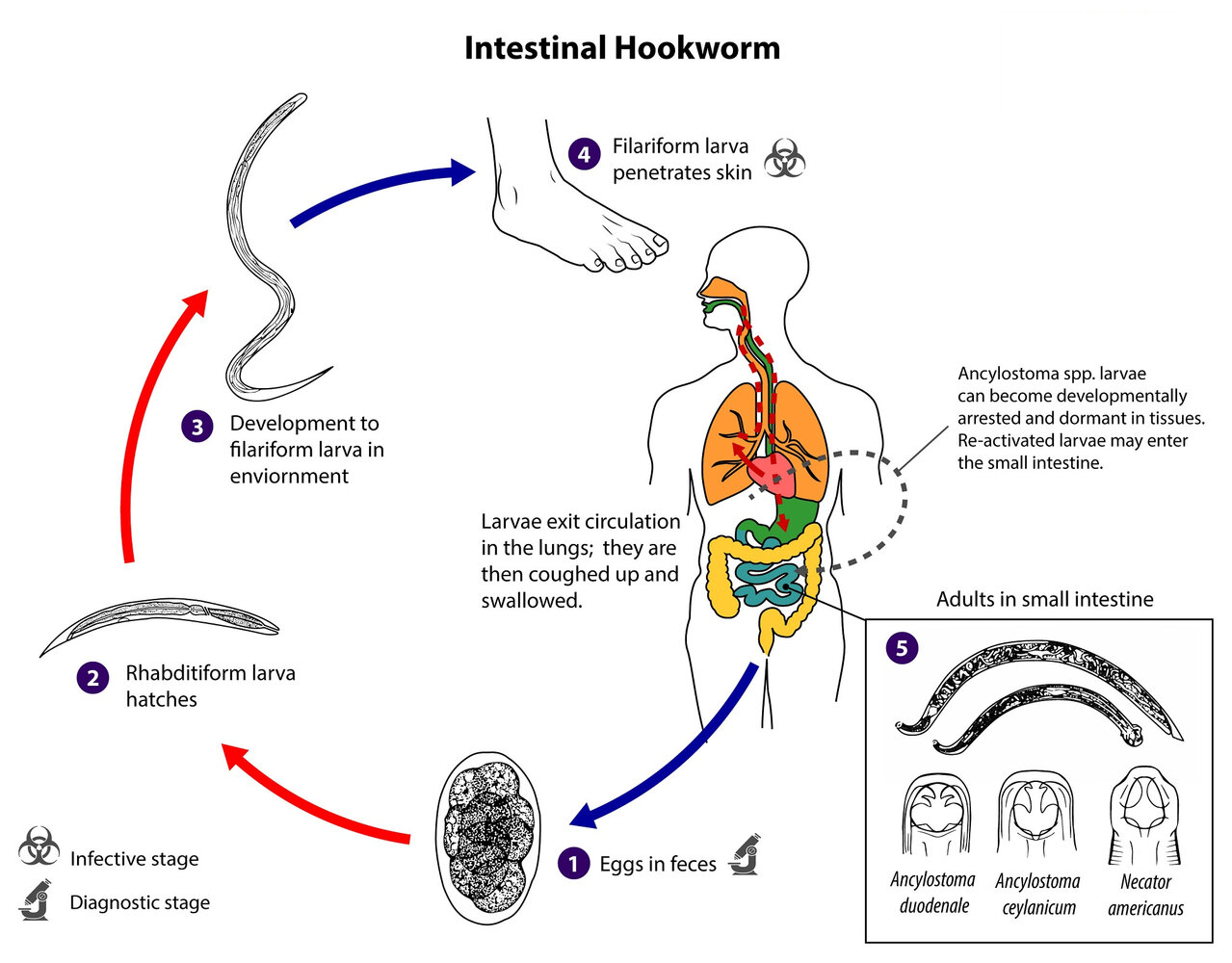
Species that infect humans are Ancylostoma duodenale, Ancylostoma ceylanicum, and Necator americanus.
1. Diagnostic stage: The host passes eggs in the feces.
2. Under optimal conditions (moist, warm soil without direct exposure to sunlight), rhabditiform larvae hatch within 2 days.
3. Within 5–10 days, the rhabditiform larvae develop into the infective filariform larvae, which can survive for 3–4 weeks in soil under favorable conditions.
4. Infective stage: The larvae penetrate the skin of the host (typically bare feet) and migrate to the heart and, then, the lungs via blood vessels. In the lungs, they penetrate the alveoli and ascend the bronchial tree to the pharynx, where they are swallowed.
5. The larvae mature into adults in the jejunum, where they attach to the intestinal wall.
This image is an adaptation. Source of original image: CDC/ DPDx. Original title: “Intestinal Hookworm”. Created by: CDC/ DPDx. Licensed under Public Domain. Modifications to original image: CDC/DPDx logo removed by request.

Ankle of a patient with cutaneous larva migrans
Serpiginous marks (larval tracks) are visible here. However, in the case of a strong local inflammatory response, these marks may not be visible.
Serpiginous marks together with pruritus establish the diagnosis of cutaneous larva migrans.
Source: "Larva Migrans Cutanea", WeisSagung, Wikimedia Commons licensed under Public Domain
{kind=link}
Loiasis
- Pathogen: Loa loa, a filarial nematode [23][24]
- Mode of transmission: bite from Chrysops (deer fly), horse fly, mango fly
- Life cycle: Introduction of larvae into bite wound → Larvae mature into adult worms → Adult worms reside in subcutaneous tissue, migrating through the body and causing symptoms → Adult worms produce microfilariae and release them into the bloodstream, where they are ingested by a female fly during a blood meal → Microfilariae mature into larvae, thus completing the cycle.
- Incubation period: 3–5 months
-
Clinical features
- Most infected individuals are asymptomatic.
- The two cardinal manifestations are:
- Calabar swelling: transient, localized swellings found commonly on the arms, legs, and around joints, which can cause pruritus and local pain
- Ocular manifestation (eye worm): Loa loa has a tendency to migrate to the subconjunctival tissue of the eye where it causes self-limiting congestion, pruritus, and pain.
-
Diagnostics [25]
- Initial test: CBC may show eosinophilia.
-
Confirmatory tests
- Blood smear: detection of microfilariae
- Visualization of adult worms in subcutaneous tissue or conjunctivae
- Treatment: diethylcarbamazine (off-label; prescribed by a specialist) [2]
-
Complications
- Encephalitis
- Cardiomyopathy
- Nephropathy
- Arthritis
- Lymphadenitis
-
Prevention
- Prevention of insect bites [26]
- Weekly prophylactic diethylcarbamazine for long-term travelers in endemic areas [27]


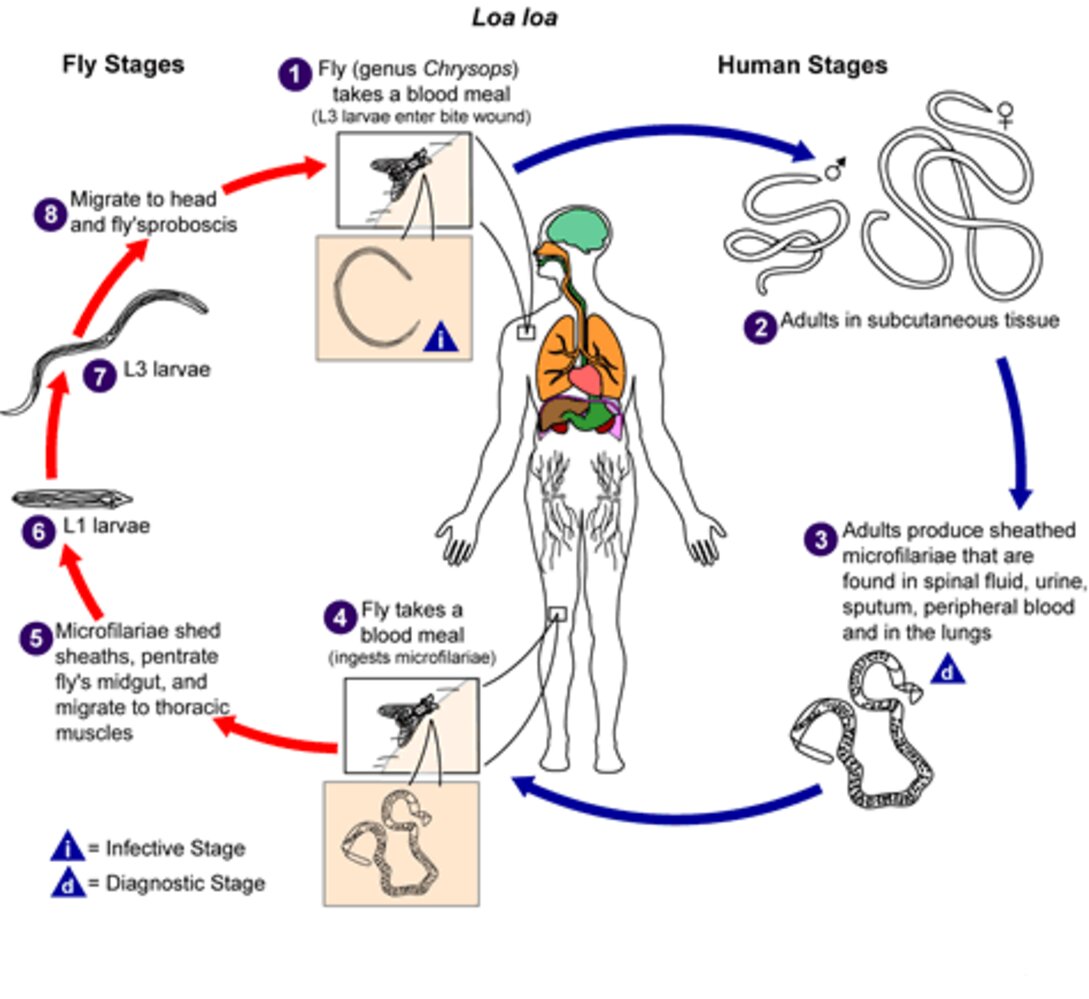
1. Infective stage: An infected day-biting fly of the species Chrysops silacea or Chrysops dimidiata deposits L3 filarial larvae from its mouthparts onto the skin of a human (definitive host), from where they migrate to microcuts or the bite wound to enter the bloodstream.
2. The larvae develop into adults in subcutaneous tissue.
3. Diagnostic stage: The adult worms produce sheathed microfilariae with diurnal periodicity, when they can be detected in the peripheral blood; at night, during the noncirculation phase, the worms can be detected in the lungs.
4. Microfilariae are ingested by a fly during a blood meal, infecting it in the process.
5. The microfilariae shed their sheaths and migrate through the intestinal wall into the fly's thoracic muscles.
6. The microfilariae develop into L1 larvae.
7. The microfilariae develop into L3 larvae.
8. The L3 larvae migrate to the mouthparts of the fly.
This image is an adaptation. Source of original image: CDC/ DPDx. Original title: “Loiasis”. Created by: CDC/ DPDx. Licensed under Public Domain. Modifications to original image: CDC/DPDx logo removed by request.
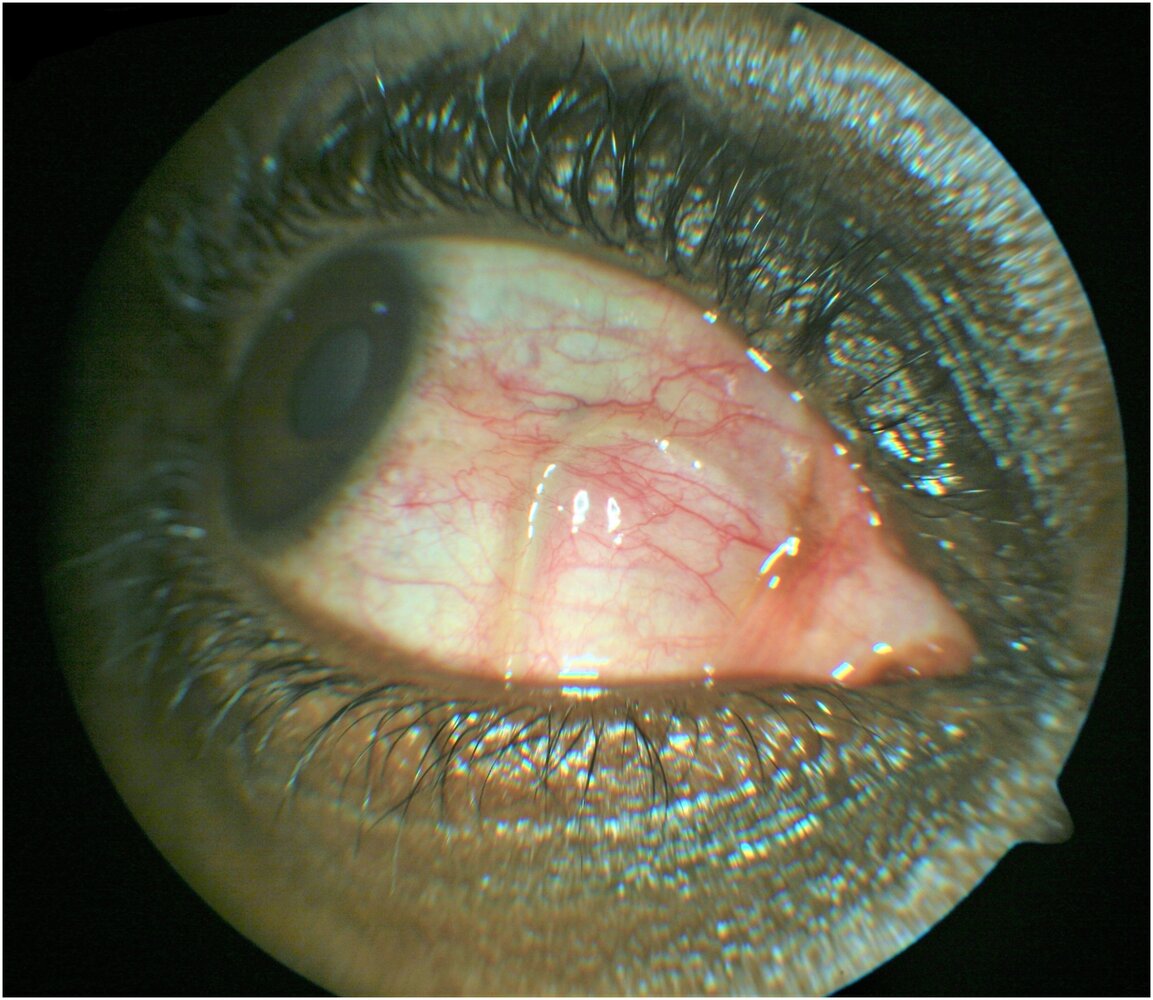
Right eye of a 35-year-old patient
A subconjunctival, filamentous mass can be seen nasally. Conjunctival injections are also visible.
This is the typical finding for a subconjunctival worm. The movement of a live worm can be observed with the slit lamp.
Source: “Fig 1, In: Removal of adult subconjunctival Loa loa amongst urban dwellers in Nigeria” by Okonkwo ON, Hassan AO, Alarape T et al., PLOS, licensed under CC BY 4.0.
Onchocerciasis
- Pathogen: Onchocerca volvulus [23][28]
- Mode of transmission: bite of the female blackfly
- Life cycle: Host is bitten by blackfly → Larvae are introduced into bite wound → Larvae mature into adult worms that reside in subcutaneous or intramuscular tissue → Adult worms produce microfilariae → Microfilariae migrate through subcutaneous tissue, causing clinical symptoms → Female fly consumes microfilariae during a blood meal → Microfilariae mature into larvae, thus completing the cycle.
-
Clinical features
-
Ocular onchocerciasis
- Keratitis
- Uveitis
- Optic atrophy
- Onchochorioretinitis
- Ocular lesions can progress to blindness (hence the common name river blindness)
-
Onchocercal skin disease
- Onchocercomata (subcutaneous nodules): deep, nonpalpable nodules containing adult worms that are found over various bony prominences
- Generalized pruritic lesions
- Hyperpigmented papules (sowda)
- Skin atrophy (due to loss of skin elasticity)
- Hanging groin
- Depigmentation (leopard-skin appearance)
- Systemic manifestations
- Allergic reactions to microfilariae may occur
- Weight loss
- Generalized musculoskeletal complaints (e.g., back and joint pain)
- Inguinal and femoral hernia
-
Ocular onchocerciasis
-
Diagnostics [1][29]
-
Skin snips (gold standard): superficial skin biopsies are taken from an inflamed area and incubated in salinefor 24 hours, causing microfilariae to leave the skin sample. Microfilarial load can be determined microscopically.
- At least two specimens are sampled and examined for motile microfilariae.
- Specimens of subcutaneous nodules can also be sampled and examined for adult worms.
- Slit-lamp examination: investigation of choice for ocular onchocerciasis
- Mazzotti test: a provocative test that involves administering diethylcarbamazine (DEC) to induce microfilarial death and exacerbate symptoms. A positive test is highly suggestive of onchocerciasis.
- Serology: unreliable for diagnosis as it cannot distinguish between active and past infection
-
Skin snips (gold standard): superficial skin biopsies are taken from an inflamed area and incubated in salinefor 24 hours, causing microfilariae to leave the skin sample. Microfilarial load can be determined microscopically.
-
Treatment [2]
- Microfilariae: ivermectin [2]
- Macrofilariae (adult worms): doxycycline (off-label) [2]
-
Prevention [2]
- Prevention of insect bites
- Mass treatment programs in endemic areas
Treating patients with onchocerciasis and loiasis coinfection places patients at risk for fatal encephalopathy; consult infectious diseases to help guide management. [1]
Everything turns black in onchocerciasis: black flies, black skin nodules, black vision (blindness).
Treat rIVER blindness with IVERmectin.
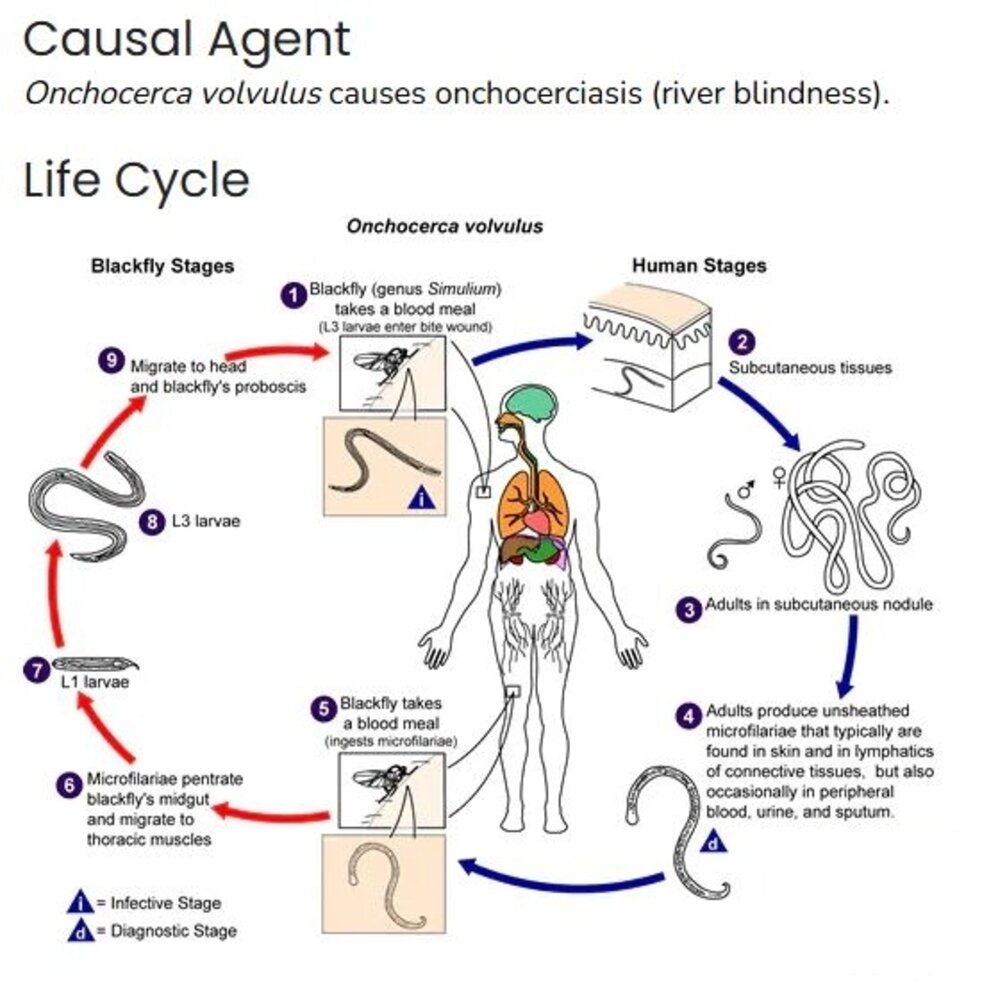
During a blood meal, an infected blackfly (genus Simulium) introduces third-stage filarial larvae onto the skin of the human host, where they penetrate into the bite wound (1). In subcutaneous tissues the larvae (2) develop into adult filariae, which commonly reside in nodules in subcutaneous connective tissues (3). Adults can live in the nodules for approximately 15 years. Some nodules may contain numerous male and female worms. Females measure 33 to 50 cm in length and 270 to 400 μm in diameter, while males measure 19 to 42 mm by 130 to 210 μm. In the subcutaneous nodules, the female worms are capable of producing microfilariae for approximately 9 years. The microfilariae, measuring 220 to 360 μm by 5 to 9 μm and unsheathed, have a life span that may reach 2 years. They are occasionally found in peripheral blood, urine, and sputum but are typically found in the skin and in the lymphatics of connective tissues (4). A blackfly ingests the microfilariae during a blood meal (5). After ingestion, the microfilariae migrate from the blackfly’s midgut through the hemocoel to the thoracic muscles (6). There the microfilariae develop into first-stage larvae (7) and subsequently into third-stage infective larvae (8). The third-stage infective larvae migrate to the blackfly’s proboscis (9) and can infect another human when the fly takes a blood meal (1). (Materials developed by CDC)
This image is an adaptation. Source of original image: CDC/ DPDx. Original title: “Onchocerciasis”. Created by: CDC/ DPDx. Licensed under Public Domain. Modifications to original image: CDC & DPDx Logo removed.
Lymphatic filariasis
-
Pathogens
- Wuchereria bancrofti: a nematode; responsible for most cases of lymphatic filariasis worldwide
- Brugia malayi and Brugia timori: found in Asia
- Mode of transmission: female mosquito bite (Aedes, Mansonia, Anopheles, and Culex)
- Incubation period: 9–12 months
- Life cycle: Mosquito introduces filarial larvae into host via bite wound → Larvae mature into adult worms that reside in the lymphatic system → Adult worms produce microfilariae (the blood circulating stage of filariasis-causing roundworms) → microfilariae move throughout vascular and lymphatic system → microfilariae are consumed by a female mosquito during a blood meal → microfilariae mature into larvae, thus completing the cycle.
-
Clinical features
- Fever
- Painful lymphadenopathy (due to worms invading lymph nodes, causing inflammation) ; and retrograde lymphangitis → lymphedema with disfiguration of the lower extremities (elephantiasis)
- Hydrocele
-
Diagnostics [1]
- Blood smear obtained at night (with Giemsa stain or H&E stain): detection of microfilariae
- Serology: elevated levels of antifilarial IgG4
-
Treatment [2]
- Diethylcarbamazine (off-label; prescribed by a specialist)
- Diethylcarbamazine can worsen eye disease in onchocerciasis and/or loiasis coinfection.
-
Complications [1]
- Lymphedema
- Hydrocele
-
Prevention [2]
- Prevention of insect bites
- Mass treatment programs in endemic areas


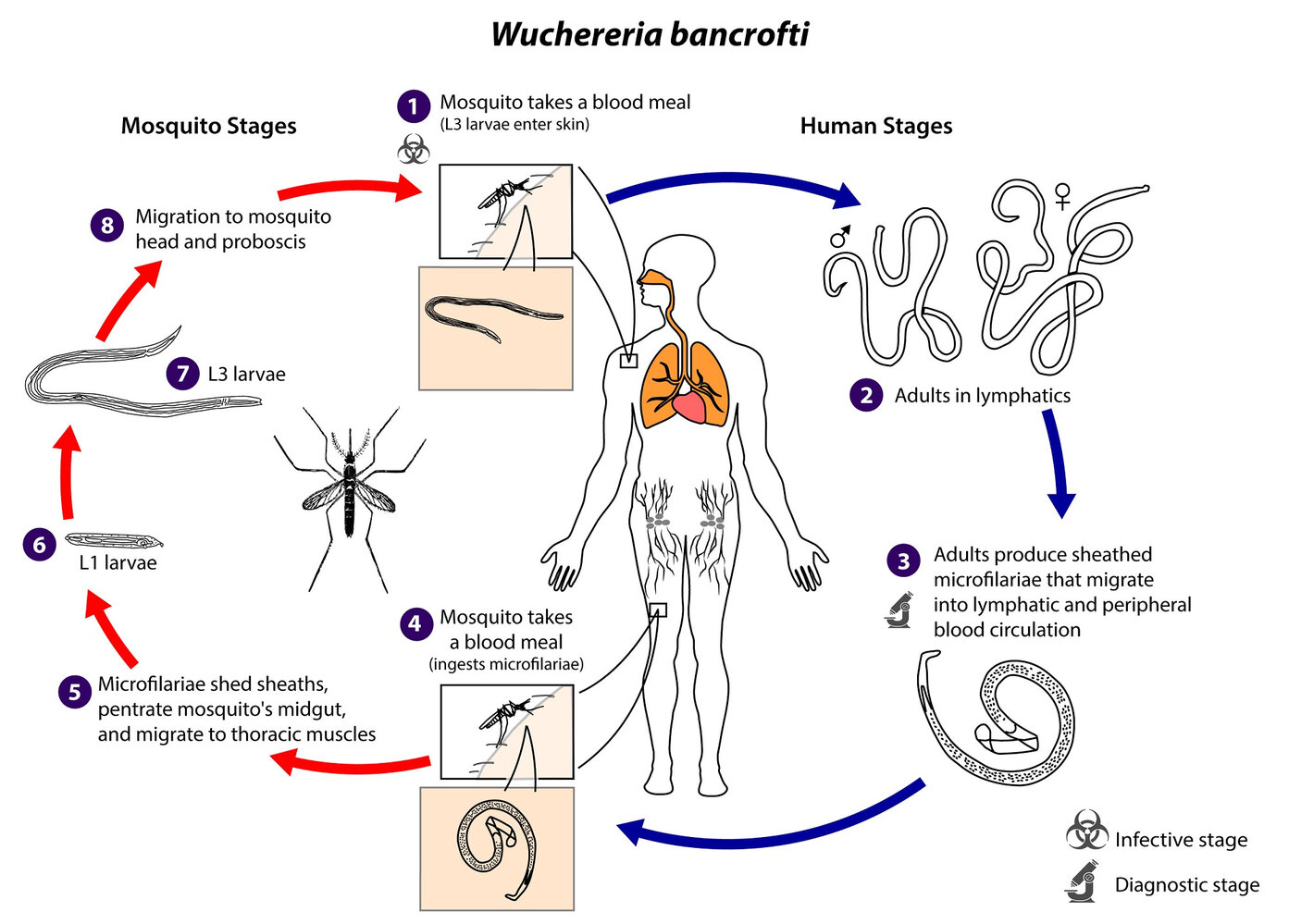
1. Infective stage: An infected mosquito (intermediate host; commonly of the Culex, Anopheles, Mansonia, and Aedes spp.) deposits L3 filarial larvae from its mouthparts onto the skin of a human (definitive host), from where they migrate to microcuts or the bite wound to enter the bloodstream.
2. The larvae develop into adults in the lymphatic system.
3. Diagnostic stage: The adult worms mate in the lymphatic system, and the female produces sheathed microfilariae that migrate into the bloodstream and lymphatic circulation. The microfilariae have nocturnal periodicity, except in the South Pacific, where W. bancrofti shows no periodicity.
4. Microfilariae are ingested by a mosquito during a blood meal, infecting it in the process.
5. The microfilariae shed their sheaths and migrate through the intestinal wall into the mosquito's thoracic muscles.
6. The microfilariae develop into L1 larvae.
7. The microfilariae develop into L3 larvae.
8. The L3 larvae migrate to the mouthparts of the mosquito.
This image is an adaptation. Source of original image: CDC/ DPDx. Original title: “Wucheria bancrofti”. Created by: CDC/ DPDx. Licensed under Public Domain. Modifications to original image: CDC/DPDx logo removed by request.

Photograph of the legs of an adult male
Severe edema of the lower legs.
This is likely due to an infection with tropical roundworms (lymphatic filariasis).
Source: "ID#: 373", CDC, Centers for Disease Control and Prevention, Atlanta, USA licensed under Public Domain
Mansonellosis
-
Pathogens [3]
- Mansonella perstans, M. ozzardi, M. streptocerca, and M. rodhaini (rare)
- Mansonella are filarial nematodes.
-
Epidemiology [4]
-
Prevalence increases with age.
- ♂ > ♀
- M. perstans has the highest prevalence. [5]
- Geographic distribution [3]
- M. perstans: West, East, and Central Africa (endemic); parts of Central and South America
- M. ozzardi: Central America, South America, and some Caribbean islands
- M. streptocerca: tropical regions of Central and West Africa
-
Prevalence increases with age.
-
Mode of transmission: transmitted by the bite of bloodsucking arthropods [4]
- Primary vectors (for all three species): biting midges (genus Culicoides)
- M. ozzardi can also be transmitted by blackflies (genus Simulium) in Latin America.
- Life cycle: infected biting midge or blackfly ingests blood meal from human host → deposition of infective L3 larvae on the skin and entrance through the bite site → maturation of larvae into adult worms in humans (body cavities for M. perstans, subcutaneous tissues for M. ozzardi, and dermis for M. streptocerca) → release of microfilariae (circulating in blood for M. perstans and M. ozzardi ; primarily in the skin for M. streptocerca) by adult worms → ingestion of microfilariae by the vector during a blood meal → migration of microfilariae from the vector midgut to thoracic muscles → development from first-stage larvae into L3 larvae → migration of L3 larvae to the vector’s proboscis → trasmission of larvae from the vector to another human during the next blood meal [3][4]
-
Clinical features [3]
- Often asymptomatic (especially in endemic regions)
- When present, symptoms are typically mild and nonspecific, e.g.:
- Fever, fatigue
- Lymphadenopathy
- Headache
- Arthralgia
- Pruritus, dermatitis, rash
- Features of M. perstans
- Transient subcutaneous nodules
- Neuropsychiatric symptoms
- Abdominal pain
- Ocular symptoms (e.g., impaired visual acuity)
- Features of M. ozzardi
- Peripheral edema
- Pulmonary symptoms
- Features of M. streptocerca: hyperpigmentation of the torso
-
Diagnostics [3][4]
- Eosinophilia (nonspecific)
- Microscopy: used to detect microfilariae in peripheral blood or skin
- Peripheral blood smear: M. perstans or M. ozzardi
- Skin snip biopsy : M. streptocerca, M. rodhaini [3]
- PCR-based assays: primarily used to differentiate M. streptocerca from Onchocerca volvulus in skin snip samples
-
Differential diagnoses [3][5]
- Onchocerciasis (Onchocerca volvulus)
- Loiasis (Loa loa)
- Lymphatic filariasis (Wuchereria bancrofti)
-
Treatment [4][5]
- There is no standardized treatment.
-
M. perstans
- Combination therapy with diethylcarbamazine plus mebendazole is commonly used.
- Alternative: doxycycline 6-week course (preferred if feasible)
- M. ozzardi: Single-dose ivermectin is effective against microfilariae but not against adult worms.
- M. streptocerca: diethylcarbamazine or single-dose ivermectin (not effective against adult worms)
-
Complications [3][4]
- Corneal lesions (associated with M. ozzardi in Brazil)
- Pericarditis and/or pleuritis (associated with M. perstans)
- Increased susceptibility to or severity of certain coinfections (associated with M. perstans), e.g.:
- Malaria
- Tuberculosis
- HIV
- Buruli ulcer
- Prevention: prevention of insect bites [3]
Dracunculiasis (Guinea worm disease)
- Definition: a parasitic infection caused by Dracunculus medinensis
- Epidemiology: endemic in West, Central, and East Africa
- Etiology: Dracunculus medinensis
- Hosts: copepods (intermediate host), humans (definitive host)
-
Mode of transmission
- Mainly consumption of water contaminated with infected copepods (water fleas)
- Consumption of raw infected aquatic animals (e.g., fish, frogs) can also lead to infection.
- Pathophysiology: Ingestion of contaminated water or food → dissolution of infected copepods in stomach acid → release of D. medinensis larvae → penetration of stomach and intestinal wall → dissemination of larvae throughout the abdominal cavity and retroperitoneal space → maturation of larvae and copulation → migration of female worms to skin surface (approx. 1 year after infection; male worms die) → induction of painful blister by female worm (from which it emerges to release eggs upon contact with water)
-
Clinical features: symptoms typically appear after 12 months [30]
- Systemic: fever, generalized pruritus, urticaria
- Gastrointestinal: nausea, vomiting, diarrhea
- Dermatological: painful papule, edema, blistering and/or ulcer where the worm emerges (usually on the legs and feet)
- Diagnostics: clinical diagnosis based on skin blister and visualization of adult worm [25]
-
Treatment: no effective medications available [25]
- Worm extraction: slow traction of the worm by wrapping with a stick or gauze (may take several days to weeks)
- Wound care and topical antibiotics
- Pain management (NSAIDs)
- Complications: cellulitis, abscess, sepsis, anaphylaxis
-
Prevention [31]
- Avoid submerging the affected limb in water until the worm is removed.
- Filter or treat drinking water with larvicide.
- Thoroughly cook aquatic animals and dispose of entrails safely.
")

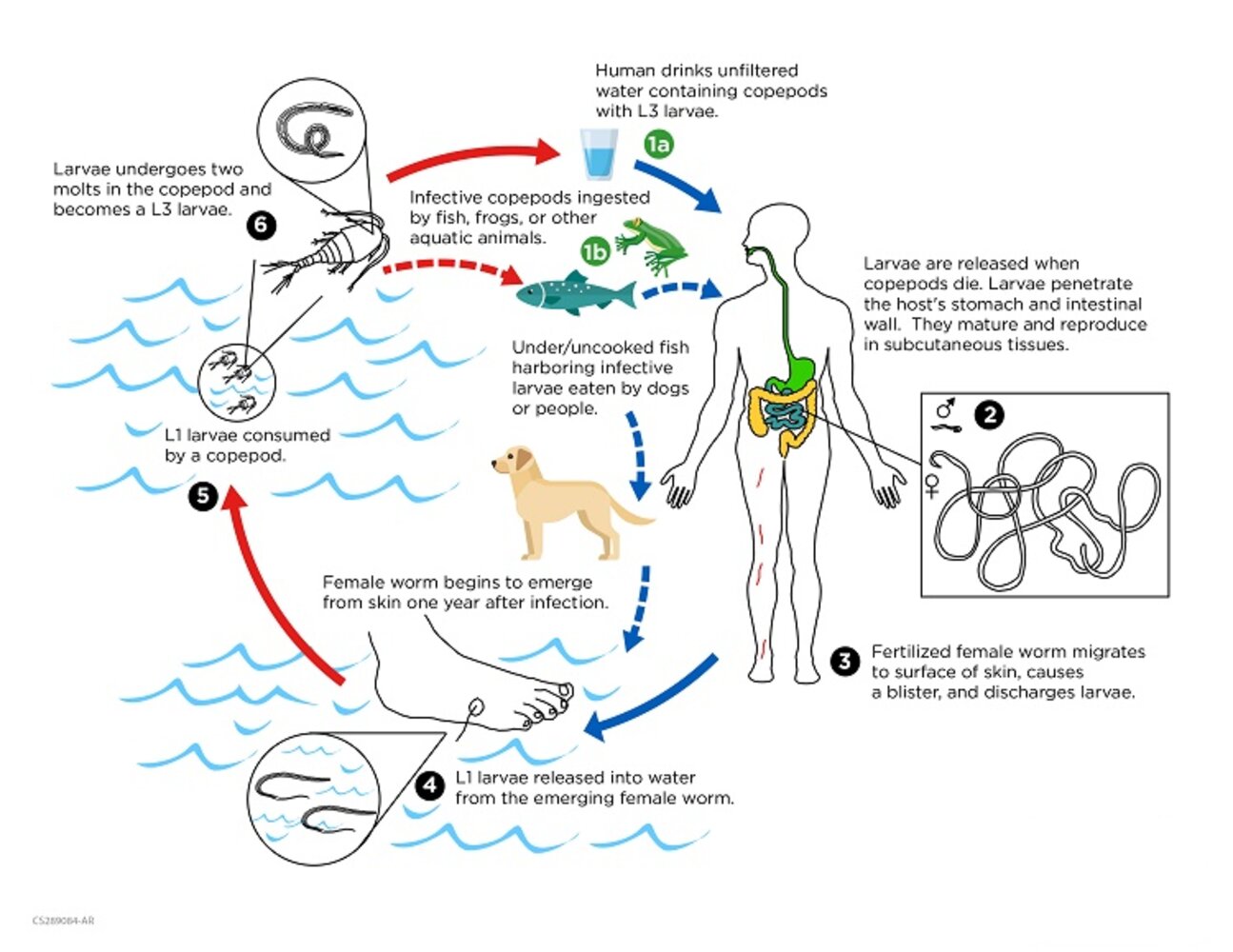
1. Infected copepods are ingested along with L3 larvae by aquatic animals or by dogs and humans with contaminated water. Ingestion of undercooked infected aquatic animals also cause infection.
2. L3 larvae are released upon the copepods' death and penetrate the host's stomach and intestinal wall, where they mature and reproduce.
3. The adult male worms die after copulation, while the fertilized female worms migrate towards the skin surface, esp. feet.
4. After approx. 1 year, the female worm forms a blister on the skin. Once the blister comes into contact with water, typically as a result of the host seeking to relieve discomfort, it ruptures and the worm emerges to release L1 larvae.
5. The L1 larvae are ingested by copepods, in which they molt twice to become infective L3 larvae.
This image is an adaptation. Source of original image: CDC/ DPDx. Original title: “Dracunculiasis”. Created by: CDC/ DPDx. Licensed under Public Domain. Modifications to original image: CDC/DPDx logo removed by request.

Inner ankle of the left foot of a patient with dracunculiasis (Guinea worm disease)
A burst blister with an emerging female Guinea worm (Dracunculus medinensis) is visible. A match stick is used to extract the worm, which can take days or weeks.
Source: "1342", CDC, CDC licensed under Public Domain
Anisakiasis
-
Pathogens [7][9]
- Anisakis simplex complex (e.g., A. simplex sensu stricto, A. pegreffii, A. berlandi)
- Pseudoterranova decipiens complex (e.g., P. decipiens sensu stricto, P. azarasi, P. cattani)
- Contracecum osculatum complex
- Also known as herringworm, sealworm, and codworm
-
Epidemiology [7]
- Incidence is highest in regions with high consumption of raw seafood.
- Most prevalent in Japan, regions of Northern Europe, and along the Pacific coast of South America
- Mode of transmission: ingestion of mature L3 larvae in raw or undercooked seafood (e.g., fish or squid) [8]
-
Life cycle [8]
- Marine mammals harbor adult L3 larvae → release of eggs into seawater with feces → development and hatching of eggs into free-swimming L3 larvae → ingestion of larvae by small crustaceans → consumption of infected crustaceans by fish or squid; larvae migrate to the viscera or body cavity → ingestion of infected fish or squid by marine mammals → maturation of larvae into adults in the stomach of marine mammals; adults produce eggs
- Humans are accidental hosts.
-
Incubation period [7][8]
- Gastric infection: 1–8 hours
- Intestinal infection: typically 5–7 days; may be up to 2 weeks
-
Clinical features [7][8]
- May be asymptomatic
- Symptoms depend on the site of infection.
- Gastric anisakiasis
- Abrupt-onset severe epigastric pain
- Nausea and vomiting
- Diarrhea
- Dyspepsia
- Intestinal anisakiasis
- Symptoms of bowel obstruction
- Symptoms of gastrointestinal perforation (e.g., fever, abdominal pain, abdominal distention)
- Symptoms and signs of secondary peritonitis (e.g., peritoneal signs)
- Gastrointestinal bleeding
-
Ectopic anisakiasis (rare)
- May affect, e.g., the throat, peritoneal cavity, or mesentery
- Symptoms depend on the location of the larvae (e.g., coughing up larvae from the respiratory tract).
- Symptoms of allergic reaction (e.g., urticaria, angioedema, anaphylaxis)
-
Diagnostics [7][8]
- Eosinophilia is uncommon.
-
Upper endoscopy
- Definitive method for diagnosing gastric anisakiasis
- Allows for direct visualization and removal of the larvae
- Findings: a filiform larva (∼ 15 mm) attached to swollen and inflamed mucosa
- Capsule endoscopy or double-balloon enteroscopy: initial diagnostic modality for intestinal anisakiasis
- An exploratory laparotomy may be required for confirmation.
- Histopathological diagnosis: from a tissue biopsy sample taken during EGD or laparotomy
- Serology: positive for anti-Anisakis-specific IgA/IgG and IgE antibodies
-
Differential diagnoses [7][8][9]
- Peptic ulcer disease
- Food poisoning
- Appendicitis
- Crohn disease
- Intestinal obstruction
- Peritonitis
- Cancer (e.g., gastric cancer, colorectal cancer, pancreatic cancer)
- Pancreatitis
- Ovarian cysts
- Gastroesophageal reflux disease
- Kounis syndrome
-
Treatment [7][8]
- Usually self-limited; symptoms resolve within 2–3 weeks
- Endoscopic removal is curative for gastric anisakiasis.
- Anthelmintics (e.g., albendazole) provide limited benefit.
- Surgery: for severe complications only
-
Complications [7][8]
- Intestinal perforation
- Intestinal obstruction
- Peritonitis
- Gastrointestinal bleeding
- Anaphylaxis
- Prevention: Cook seafood thoroughly. [7]
Intestinal capillariasis
- Pathogen: Capillaria philippinensis [11]
-
Epidemiology [12][32]
- Endemic in the Philippines and Thailand
- Sporadic cases reported in other parts of East and Southeast Asia and northern Egypt
- Mode of transmission: ingestion of raw or undercooked freshwater fish [10]
-
Life cycle [12]
- Humans ingest raw or undercooked freshwater fish containing larvae → release of larvae into the intestine → development of larvae into adult worms, which embed in the small intestinal mucosa → production of eggs by adult females, which may be passed into the environment via stool → maturation of eggs outside the host, which are eaten by freshwater fish → hatching and development of larvae in fish tissues → ingestion of infected fish by humans
- Some larvae hatch within the human intestine and reinvade the mucosa, leading to autoinfection and heavy worm burden.
-
Clinical features [10][11]
- Gastrointestinal symptoms
- Chronic watery diarrhea (most common symptom)
- Steatorrhea
- Chronic abdominal pain (often colicky)
- Borborygmi
- Bloating
- Anorexia
- Systemic symptoms
- Pronounced weight loss
- Anasarca
- Generalized weakness
- Fatigue
- Dizziness
- Gastrointestinal symptoms
-
Diagnostics [10][11][12]
-
Stool microscopy
- Eggs, larvae, and/or adult worms
- Poor sensitivity due to intermittent parasite shedding
-
Laboratory studies [11]
- Severe hypoalbuminemia (often < 2 g/dL)
- ↓ Total protein
- Hypokalemia
- Anemia
- Eosinophilia is uncommon.
- Endoscopy with biopsies: Histopathology confirms the diagnosis.
-
Stool microscopy
-
Differential diagnoses [10][11]
- Celiac disease
- Gastrointestinal cancer
- HIV infection
- Hyperthyroidism
- Strongyloidiasis hyperinfection
- Other causes of chronic diarrhea
-
Treatment
- Albendazole (off-label) [10]
- Mebendazole (off-label) [10]
-
Complications [10][12][32]
- Protein-losing enteropathy
- Severe malnutrition (emaciation, cachexia)
- Severe electrolyte abnormalities (e.g., hypokalemia)
- Paralytic ileus (can occur after treatment)
- Cardiomyopathy
- Prevention: Cook seafood thoroughly. [12]
Trichostrongylosis
-
Pathogens: nematodes (roundworms) of the genus Trichostrongylus that primarily infect herbivorous mammals [13][14]
- Common species that infect humans include T. colubriformis, T. orientalis, and T. axei.
- Other reported species that infect humans include T. capricola, T. probolurus, T. skrjabin, T. vitrinus, and T. longispicularis.
-
Epidemiology [13][14]
- Worldwide distribution
- Most common in rural communities with domesticated livestock in the Middle East and other parts of Asia
- Mode of transmission: ingestion of infective filariform larvae (e.g., in food or water contaminated with feces from infected host) [13][14]
- Life cycle: Eggs are excreted in feces → hatching of eggs in soil → development of larvae into infective L3 larvae on soil or vegetation → ingestion of infective larvae on contaminated food or plants by humans → migration of larvae into the small intestine → maturation of larvae into adult worms → production of eggs by adult worms, which are excreted in feces [13]
-
Clinical features [13][14]
- Typically asymptomatic
- Symptoms are associated with heavy worm burden and may include:
- Gastrointestinal symptoms (e.g., abdominal pain, anorexia, diarrhea)
- Systemic symptoms (e.g., fatigue, cachexia, developmental delays in children)
-
Diagnostics [13][14]
- Stool microscopy: The presence of Trichostrongylus eggs confirms the diagnosis.
- Peripheral eosinophilia or hypereosinophilia, mild anemia (nonspecific)
- Differential diagnosis: hookworm infection (e.g., Ancylostoma duodenale, Necator americanus) [13]
- Treatment: anthelmintic therapy [13]
-
Prevention [14]
- Avoid fecal contamination of food and water (e.g., wash, peel, and cook raw fruits and vegetables).
- Practice strict sanitation around livestock.
Cestodes (tapeworms)
Cestodes (tapeworms) are long, flat, ribbon-like worms composed of numerous segments and a single scolex at the head, which they use to anchor themselves to the intestine. Since they do not have a digestive tract, all nutrients are absorbed through the tegument. Cestodes are hermaphroditic.
| Overview of cestode infections [1] | ||||||
|---|---|---|---|---|---|---|
| Disease | Pathogen | Mode of transmission | Clinical features | Diagnosis | Treatment | |
| Taeniasis | Intestinal taeniasis |
|
|
|
|
|
| Cysticercosis |
|
|
|
|
|
|
| Diphyllobothriasis |
|
|
|
|
|
|
| Echinococcosis |
|
|
|
|
|
|
| Hymenolepiasis |
|
|
|
|
|
|
| Dipylidiasis [2][33][34] |
|
|
|
|
|
|

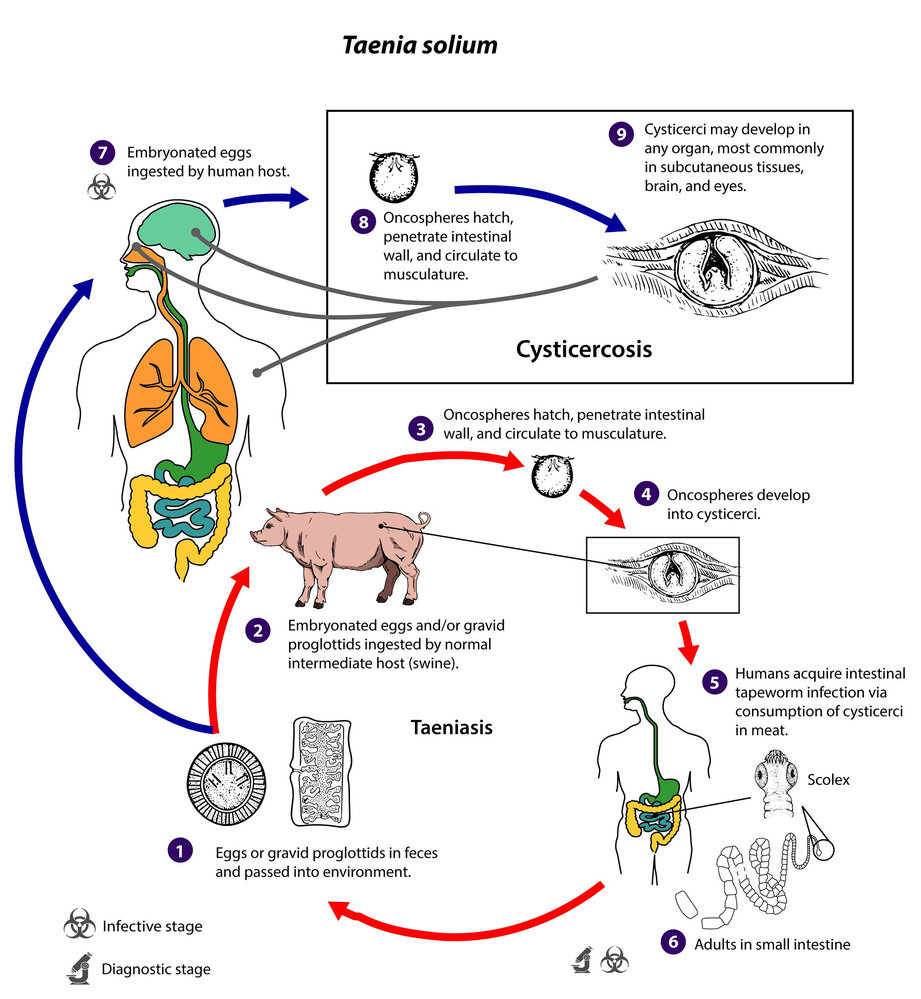
The distinct head (scolex) of a pork tapeworm. Characteristic of Taenia solium are two rows of hooks, which permit attachment to the host's intestinal wall. In contrast to pork tapeworms, beef tapeworms do not have hooks.
Source: "ID#: 14377", CDC/ Dr. Mae Melvin, Centers for Disease Control and Prevention (CDC) licensed under Public Domain
Taenia infections
| Overview of Taenia infections [2] | ||
|---|---|---|
| Intestinal taeniasis | Cysticercosis [35] | |
| Description |
|
|
| Pathogen |
|
|
| Mode of transmission |
|
|
| Life cycle |
|
|
| Clinical features |
|
|
| Diagnosis |
|
|
|
Treatment[2] |
|
|
|
Prevention[2] |
|
|
Cysticercosis can cause brain cysts and seizures.

A mature beef tapeworm. The tapeworm can develop in the human intestine over weeks to months after raw or undercooked beef containing the larvae is ingested. May reach lengths of up to 25 m.
Source: "ID#: 5260", CDC, Centers for Disease Control and Prevention (CDC) licensed under Public Domain
The distinct head (scolex) of a pork tapeworm. Characteristic of Taenia solium are two rows of hooks, which permit attachment to the host's intestinal wall. In contrast to pork tapeworms, beef tapeworms do not have hooks.
Source: "ID#: 14377", CDC/ Dr. Mae Melvin, Centers for Disease Control and Prevention (CDC) licensed under Public Domain
This image is an adaptation. Source of original image: CDC/ DPDx. Original title: “Taenia solium”. Created by: CDC/ DPDx. Licensed under Public Domain. Modifications to original image: CDC/DPDx logo removed by request.
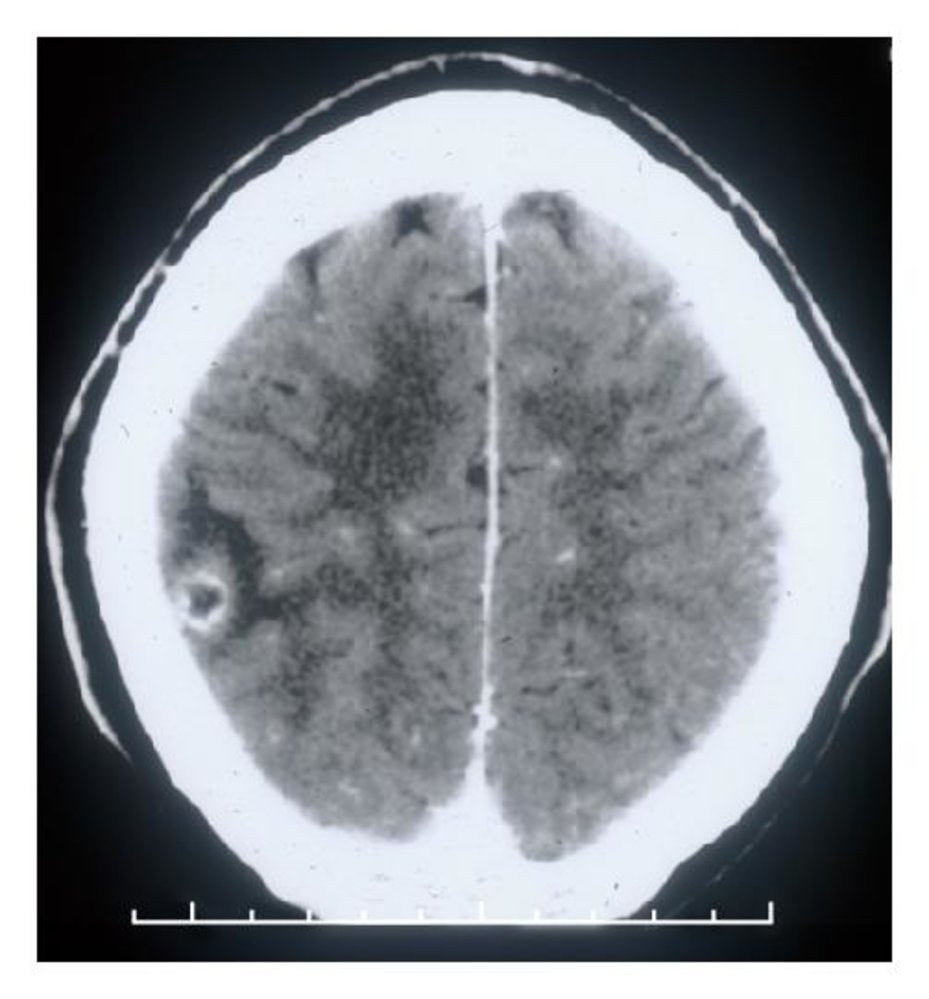
CT head (with contrast; axial plane) of a patient with neurocysticercosis
A rounded peripheral lesion in the right temporoparietal region has a hypodense center (yellow overlay) and thickened enhancing wall (red overlay). There is perilesional low-attenuation edema (green overlay).
These findings are typical of the colloidal-vesicular stage of neurocysticercosis.
Source: “Figure 2 (b) in: Diagnosis and Treatment of Neurocysticercosis” by Christina M. Coyle, Herbert B. Tanowitz, Interdisciplinary Perspectives on Infectious Diseases, licensed under CC BY 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
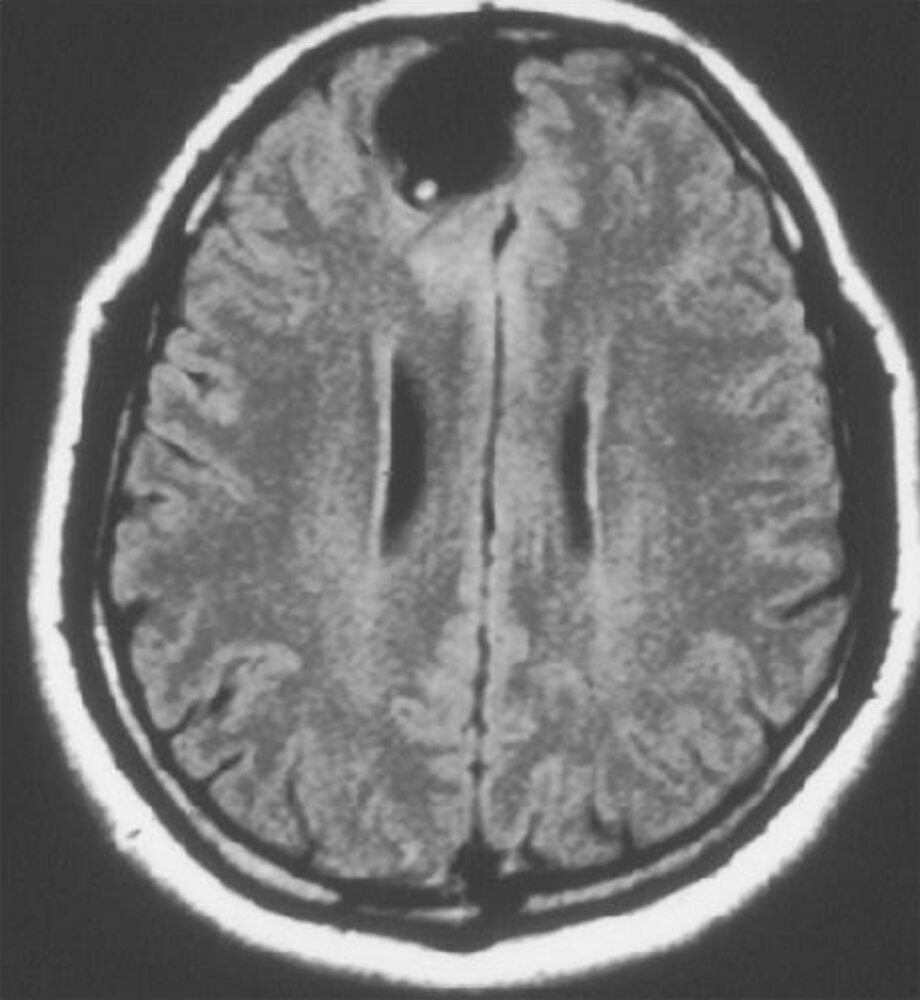
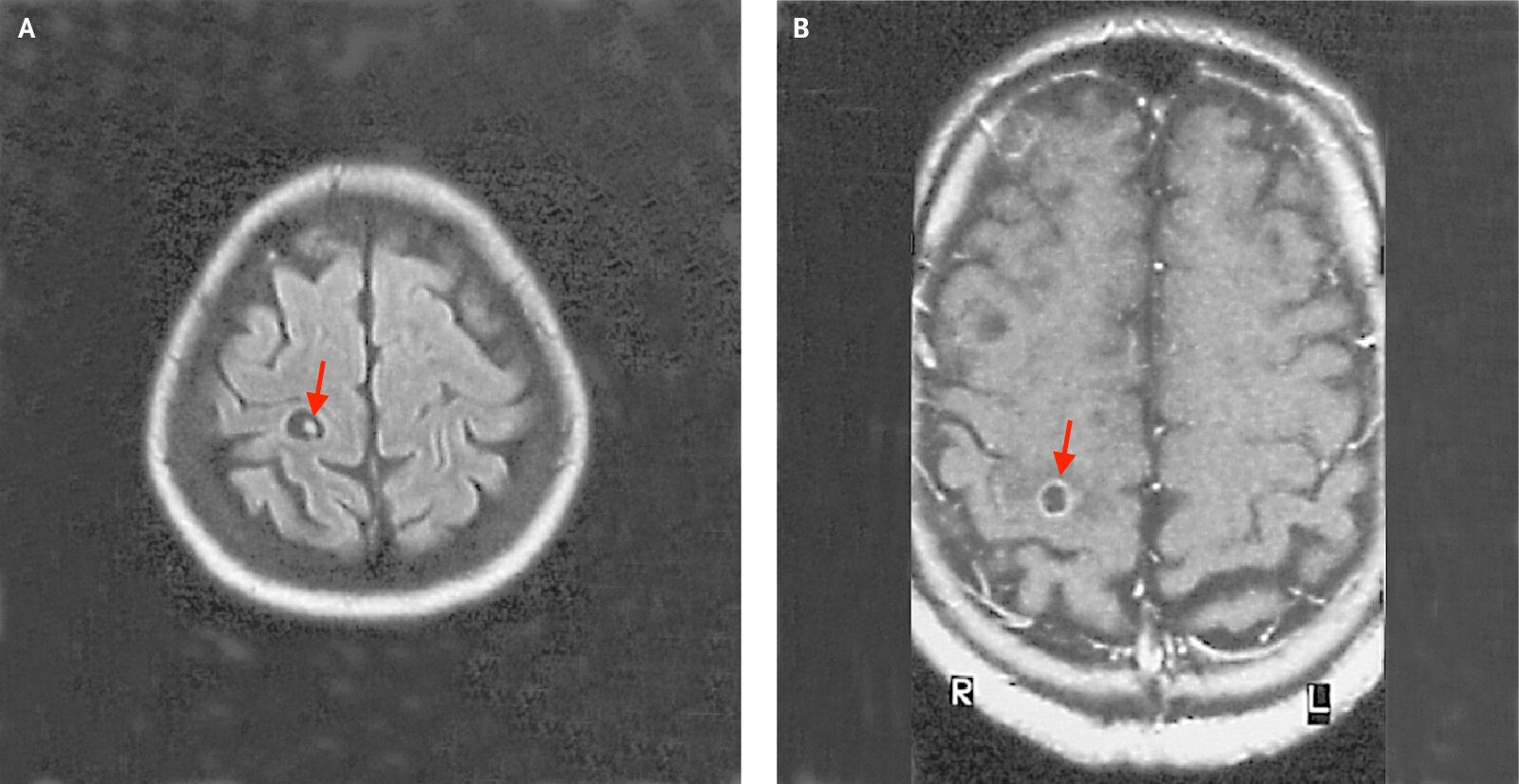
Cranial MRI (FLAIR sequence)
A hyperintense nodule is visible along the margin of a rounded lesion (hole-with-dot sign) in the right frontal lobe that is isointense to CSF.
The fluid-filled lesion (cysticercus; green overlay) is a larval cyst of the pork tapeworm, with the scolex (red overlay) seen as the hyperintense nodule. The finding is consistent with neurocysticercosis.
Source: “Figure 2 (a), in: Diagnosis and Treatment of Neurocysticercosis” by Christina M. Coyle, Herbert B. Tanowitz, Interdisciplinary Perspectives on Infectious Diseases, licensed under CC BY 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
© Massachusetts Medical Society. All rights reserved. AMBOSS SE, exclusive licensee.
Diphyllobothriasis
-
Pathogen [38]
- Dibothriocephalus latus (fish tapeworm; formerly Diphyllobothrium latum)
- Fish tapeworms are cestodes.
- Mode of transmission: consumption of raw or undercooked freshwater fish containing larvae
- Life cycle: Larvae develop into adult tapeworms in the small intestine → Adult worms produce proglottids, which can detach from the tapeworm and are passed in the feces.
-
Clinical features
- Usually asymptomatic
- Chronic infection leads to vitamin B12 deficiency: fish tapeworms compete with the host for dietary vitamin B12 in the intestine → anemia and/or neurological symptoms
-
Diagnostics [1]
- Initial test: CBC may show eosinophilia and megaloblastic anemia. [39]
- Confirmatory test: stool examination for eggs or proglottids (i.e., segments of adult tapeworms)
- Treatment: praziquantel (off-label) [2]
- Prevention: thoroughly cook fish [2]
Dibothriocephalus causes vitamin B12 deficiency.
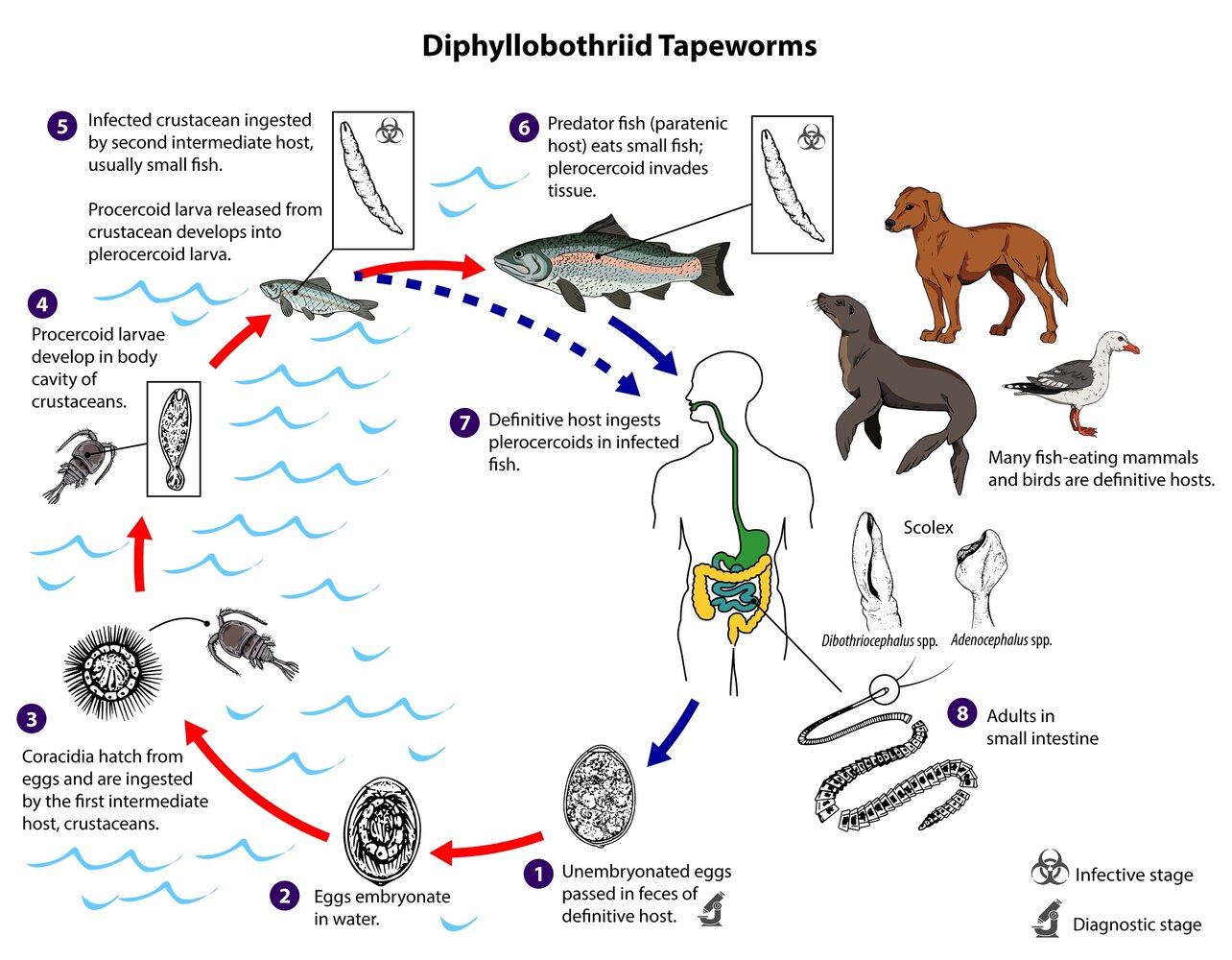
1. Diagnostic stage: Unembryonated eggs are shed in the feces of an infected definitive host (humans and most fish-eating mammals or birds).
2. The eggs embryonate in water, where they mature (18 to 20 days) and produce oncospheres that develop into coracidia.
3. The coracidia hatch from the eggs and are ingested by small crustaceans (first intermediate host).
4. The coracidia develop into procercoid larvae within the crustaceans.
5. Infective stage (mainly intermediate host): The infected crustacean is ingested by a small fish (second intermediate host), whereupon the procercoid larvae migrate into the deeper tissues and there develop into plerocercoid larvae. These small fish are rarely consumed raw by humans and, therefore, present a low risk of infection.
6. Infective stage (definitive host): Larger predatory fish ingest the smaller infected fish, which then serve as intermediate (paratenic) hosts. The pleroceroid larvae migrate to the muscle tissue of the paratenic host fish.
7. Infection of the definitive host occurs via ingestion of (undercooked) meat of the paratenic host fish.
8. The pleroceroid larvae develop into adult tapeworms in the small intestine, attaching to the intestinal mucosa via scolical bothria. Adult tapeworms produce over 3000 proglottids, which contain the unembryonated eggs. The proglottids release up to 1 million unembryonated eggs per day/tapeworm, which the definitive host passes in the feces.
This image is an adaptation. Source of original image: CDC/ DPDx. Original title: “Diphyllobothriid Tapeworms”. Created by: CDC/ DPDx. Licensed under Public Domain. Modifications to original image: CDC & DPDx Logo removed.
Hymenolepiasis
- Pathogen: Hymenolepis nana (dwarf tapeworm) [40]
-
Mode of transmission
- Ingestion of eggs from contaminated food or water
- Ingestion of cysticercoids from infected arthropods
- Life cycle: Ingestion of eggs → Develop into cysticercoid larvae in the small intestine villus (alternatively cysticercoids can be consumed from infected arthropods) → Cysticercoids (released upon rupture of the intestinal villus) develop into an adult worm in the intestinal lumen → Eggs are passed through the stool
-
Clinical features
- Mostly asymptomatic
- Severe infection with Hymenolepis nana manifests with:
- Anorexia, abdominal pain, diarrhea
- Weakness, headache
- Diagnostics: stool examination for eggs [1]
-
Treatment [1]
- Praziquantel (off-label) [2]
- OR nitazoxanide (off-label) [2]
- Prevention: proper hygiene and disposal of human waste [2]
Dipylidiasis
Pathogen: Dipylidium caninum (flea tapeworm) [33]
-
Epidemiology [33][34]
- Worldwide distribution
- Most common tapeworm in cats and dogs, but human infection is rare
- Children are more frequently infected than adults.
- Mode of transmission: ingestion of an intermediate host (flea or, less commonly, louse) containing infective cysticercoid larvae [33]
- Life cycle: egg packets released from gravid proglottids in stool → ingestion of egg packets by flea or louse larvae → hatching and development of oncospheres into cysticercoid larvae within the flea or louse as it matures → ingestion of an infected adult flea or louse by a human (accidental host) or animal (cat or dog) → release of cysticercoid in the small intestine and maturation into an adult tapeworm → excretion of proglottids in stool [33]
-
Clinical features [2][33][34]
- Typically asymptomatic in humans and animals
- Passage of proglottids is the most common sign.
- Found in the perianal region, in feces, on diapers, or in the environment
- Motile when initially passed
- Resemble rice kernels when dry and cucumber or pumpkin seeds when moist
- Symptoms may include:
- Anal pruritus and resulting excoriations
- Bloating
- Abdominal pain or discomfort
- Diarrhea
- Irritability
- Sleep disturbances
-
Diagnostics: stool examination [2][33]
- Macroscopic: identification of proglottids
- Microscopic (confirmatory): identification of characteristic egg packets
-
Differential diagnoses [2][33][34]
- Pinworm infection (Enterobius vermicularis)
- Other cestode infections (e.g., hymenolepiasis, taeniasis, Raillietina infection)
- Fly larvae (maggots)
- Undigested food (e.g., rice grains, vegetable seeds)
-
Treatment [2][34]
- Typically self-limited and may clear spontaneously within 6 weeks [2]
- First-line therapy: praziquantel (off-label) [34]
-
Prevention [2][34]
- Control fleas and lice on pets and in the environment.
- Wash hands after contact with cats and/or dogs.
Trematodes (flukes)
Trematodes (flukes) are small, flat, oval worms with two suckers (one located at the mouth and the other ventrally) and a blind-ending gut. Most species are hermaphroditic, but some also form separate male and female adults.
| Overview of trematode infections [1] | ||||||
|---|---|---|---|---|---|---|
| Disease | Pathogen | Mode of transmission | Clinical features | Diagnosis | Treatment [2] | |
| Schistosomiasis |
|
|
|
|
|
|
| Clonorchiasis |
|
|
|
|
|
|
| Paragonimiasis |
|
|
|
|
|
|
| Fascioliasis |
|
|
|
|
|
|
| Dicrocoeliasis [41][42] |
|
|
|
|
|
|
| Opisthorchiasis [43][44] |
|
|
|
|
|
|
Clonorchiasis
-
Pathogen
- Clonorchis sinensis (Chinese liver fluke)
- Clonorchis are trematodes (flukes).
- Endemic to certain parts of Asia
- Mode of transmission: consumption of raw/undercooked freshwater fish
- Incubation period: 10–26 days [45]
- Life cycle: Water is contaminated with human feces containing Clonorchis eggs → Eggs are ingested by freshwater snails and mature into larvae → Larvae are released to water and penetrate fish → Humans eat fish containing larvae → Larvae migrate to biliary tract and mature into adult worms → Eggs of adult worms are released into the bile ducts and carried to the intestinal tract → Eggs are eliminated with the feces, thus completing the cycle.
-
Clinical features
- Most infected individuals are asymptomatic.
- Acute symptoms
- Cholangitis
- Unspecific symptoms (e.g., right upper quadrant pain, diarrhea, fatigue)
- Chronic symptoms and complications
- Cholelithiasis with pigmented gallstones
- Hepatomegaly
- Malnutrition, weight loss
- Jaundice
- Risk factor for cholangiocarcinoma
-
Diagnostics [25]
- CBC: eosinophilia [46]
- Microscopic examination of stool for eggs
- Identification of adult worms on ERCP or during surgery
-
Treatment [2]
- Praziquantel [2]
- OR albendazole (off-label) [2]
- Prevention: thoroughly cook seafood [2]


")

Photomicrograph of a Clonorchis sinensis egg (400x magnification)
The miracidium (larval stage of C. sinensis; green overlay) is visible inside the egg. The narrow end of the egg is covered by an operculum (resembling a cap; blue overlay), which is separated from the egg when the miracidium hatches. At the opposite, abopercular end, a small, comma-shaped knob (red overlay) is visible.
This image is an adaptation. Source of original image: CDC. Original title: “PHIL ID#: 896”. Created by: Melvin M. Licensed under Public Domain. Modifications to original image: cropped.

Photomicrograph of an adult Clonorchis sinensis (H&E stain; low magnification)
The shape of the trematode is elongated and slim with the anterior region narrowing into an oral sucker which is connected to the two lateral tubes, called “caeca.” Vitelline glands are visible on either side of the caeca. Inside the body, the medial, brown-black, coiled uterus and the posterior, pink-red, branch-like testes appear prominently.
Source: “Figure 2, in: Liver Fluke Induces Cholangiocarcinoma” by Sripa B, Kaewkes S, Sithithaworn P, Mairiang E, Laha T, Smout M, et al., PLoS Med, licensed under CC BY 2.5. Modifications: Image cropped from diagram adapted from https://www.dpd.cdc.gov/DPDx/HTML/Opisthorchiasis.htm.
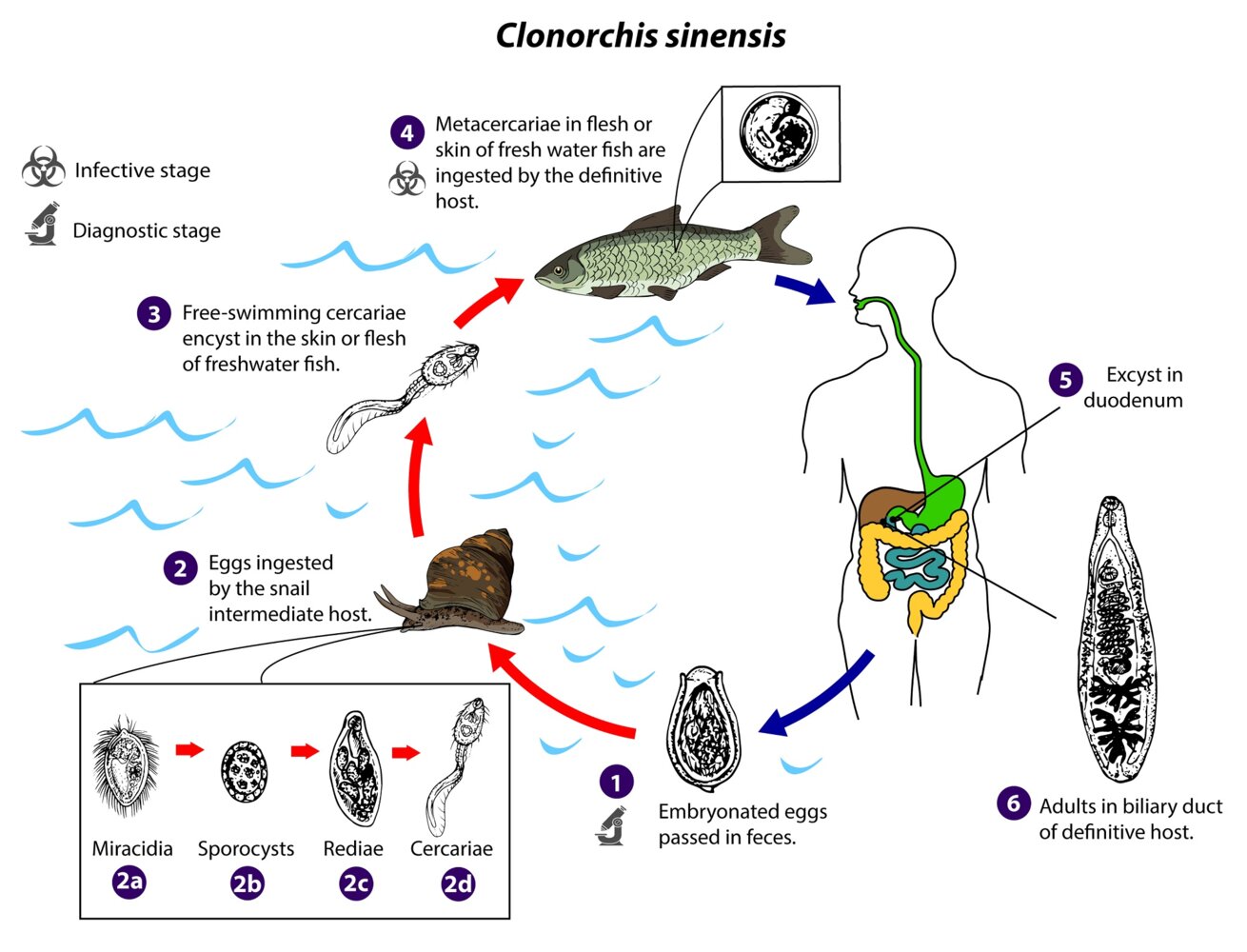
1. Diagnostic stage: The definitive host passes embryonated eggs with the feces.
2. Eggs are ingested by a freshwater snail (intermediate host), in which they release miracidia (2a). The miracidia develop into sporocysts (2b), then rediae (2c), before developing into cercariae (2d), which are excreted by the snail.
3. The free-swimming cercariae encyst in the skin or flesh of fish, in which they transform into metacercariae.
4. Infective stage: The metacercariae are ingested by humans via undercooked, smoked pickled, or salted fish.
5. The metacercariae excyst in the duodenum.
6. The parasites then migrate to biliary tract via the hepatopancreatic ampulla (of Vater) and mature there for approximately one month.
This image is an adaptation. Source of original image: CDC/ DPDx. Original title: “Clonorchis sinensis”. Created by: CDC/ DPDx. Licensed under Public Domain. Modifications to original image: CDC/DPDx logo removed by request.
Paragonimiasis
-
Pathogen
- Paragonimus westermani (responsible for most infections), less commonly P. mexicanus, P. kellicotti, P. heterotremus, P. africanus
- Paragonimus is a genus of trematodes that commonly infest the lung (lung flukes).
- Paragonimus species are endemic to Southeast Asia, Latin America, and Africa.
-
Mode of transmission
- Consumption of raw/undercooked crabs, crayfish, and contaminated seaweed
- Utilization of contaminated cooking utensils
- Incubation period: 2–16 weeks [47]
- Life cycle: Larvae in fresh water penetrate crabs, crayfish, and other crustaceans → Larvae encyst to metalarvae → Humans consume infected crustaceans → Metalarvae excyst and penetrate the intestinal wall, then migrate to the lungs → Larvae develop into adults in the lungs and eggs are expectorated with the sputum → Eggs are swallowed and eliminated with the feces, thereby reaching fresh water again.
-
Clinical features
- Rare prodromal signs (e.g., abdominal pain, fever, diarrhea)
- Possibly asymptomatic
- Pulmonary form
- Mild fever
- Night sweats
- Productive cough, hemoptysis
- Pleural effusions
- Extrapulmonary form
- Cerebral paragonimiasis
- Early symptoms resemble meningoencephalitis.
- Chronic symptoms include headache, vomiting, seizures, and weakness
- Possibly cyst, abscess, and granuloma formation in the intestine, spleen, peritoneum, and mesenteric lymph nodes
- Cerebral paragonimiasis
-
Diagnostics [1]
- CBC: eosinophilia
- CXR: pleural effusion, multiple small cysts, irregular linear densities, and/or nodular opacities [48]
- Microscopic examination of sputum, stool, pleural fluid, CSF, or other tissue specimens for eggs
- Serologic testing (e.g., ELISA, western blot)
- Differential diagnoses: tuberculosis
-
Treatment [2]
- Praziquantel (off-label) [2]
- OR triclabendazole (off-label) [2]
- Consider addition of corticosteroids in CNS infections.
-
Complications
- Pulmonary: secondary infections, bronchiectasis, lung abscess, empyema
- Cerebral: seizures, coma
- Skin: migratory allergic skin lesions
-
Prevention [2]
- Avoid eating raw or undercooked crustaceans.
- Cook pork thoroughly.
")
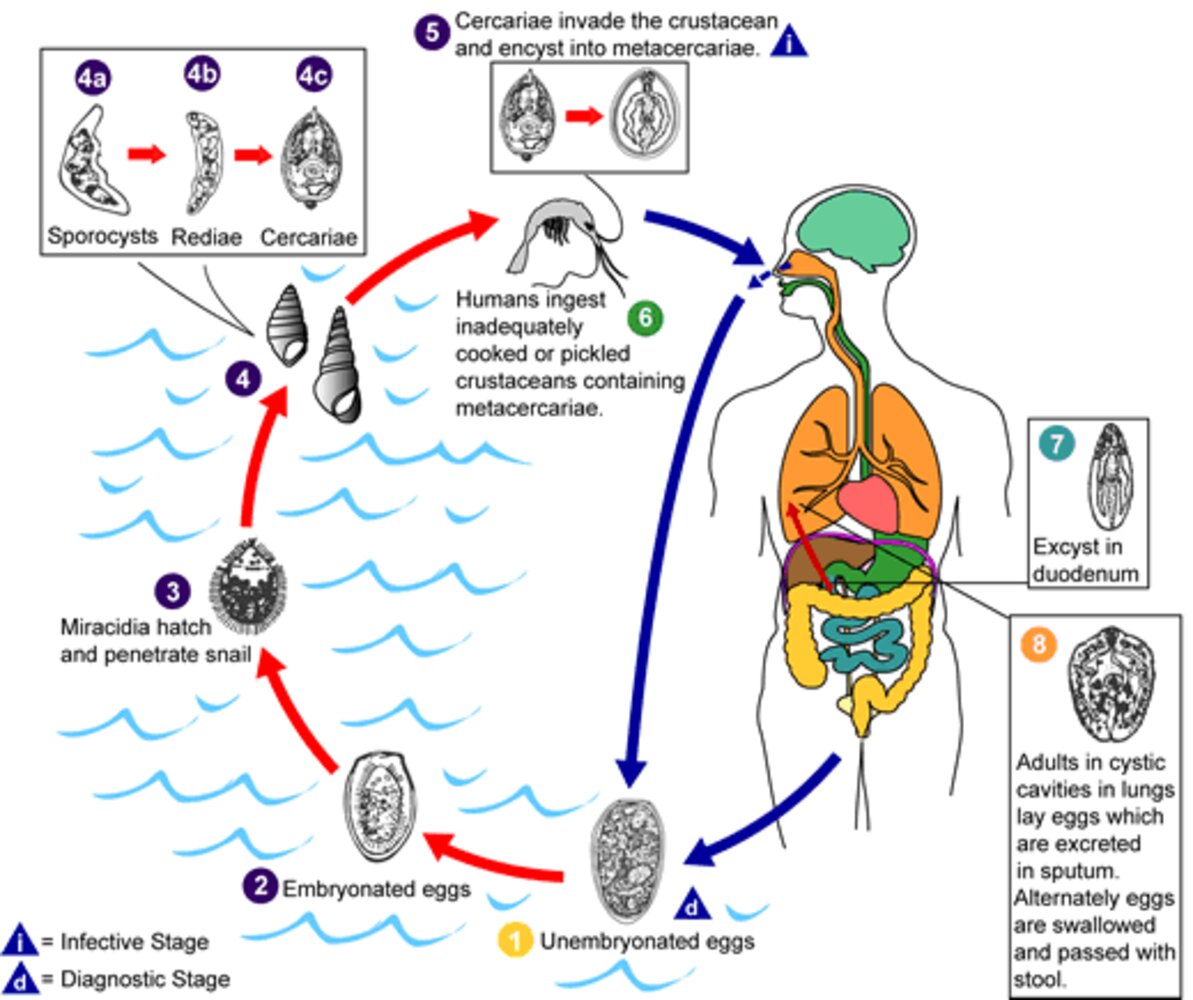
1. Diagnostic stage: Unembryonated eggs are excreted via the stool and sputum of an infected human (definitive host).
2. The unembryonated eggs are fertilized in the external environment.
3. Miracidia hatch and infect snails (1st intermediate host).
4.In the snail, the miracidia go through several developmental stages and then exit the snail as cercariae.
5. Infective stage: The cercariae infect crustaceans (2nd intermediate host) and transform into metacercariae.
6. The metacercariae enter the human gastrointestinal tract via inadequately cooked crustaceans.
7. The metacercariae are released in the small intestine and penetrate the intestinal wall, migrating from the peritoneal cavity, through the abdominal wall and diaphragm, into the lungs. Here they encaspulate and develop into adults.
8. Adults lay eggs, which are passed in the sputum.
Paragonimiasis may become chronic, in which case symptoms mimic those of tuberculosis.
This image is an adaptation. Source of original image: CDC/ DPDx. Original title: “Paragonimus”. Created by: CDC/ DPDx. Licensed under Public Domain. Modifications to original image: CDC/DPDx logo removed by request.
Fascioliasis
- Pathogen: Fasciola hepatica, Fasciola gigantica
-
Mode of transmission
- Consumption of contaminated freshwater plants (e.g., watercress)
- Drinking contaminated freshwater
-
Life cycle
- Metacercariae on freshwater plants are ingested by herbivorous mammals, e.g., sheep, cattle (both definitive hosts), or humans (incidental hosts) → Migration of the organism through the intestinal wall, then liver parenchyma, and into the biliary ducts → Adult fluke release eggs into the biliary ducts, which are then passed in the stool of the host.
- Snails serve as the intermediate hosts.
-
Clinical features
- Acute phase: fever, right upper quadrant pain, and hepatomegaly
- Chronic biliary phase: abdominal pain, nausea, vomiting, and diarrhea
- Features of biliary obstruction: biliary colic, cholangitis, cholelithiasis, and obstructive jaundice
-
Diagnostics [25]
- CBC: eosinophilia [49]
- Microscopic examination of stool, bile, or duodenal aspirates for eggs
- Serologic testing (e.g., ELISA, western blot)
- Lesions seen on imaging (e.g., CT, MRI)
- Endoscopy: adult flukes in the biliary tract
-
Treatment [2]
- Triclabendazole [2]
- OR nitazoxanide (off-label) [2]
- Biliary obstruction: GI consult and ERCP [50]
-
Prevention [2]
- Drink filtered water.
- Avoid eating contaminated freshwater plants (e.g., bamboo shoots, watercress).

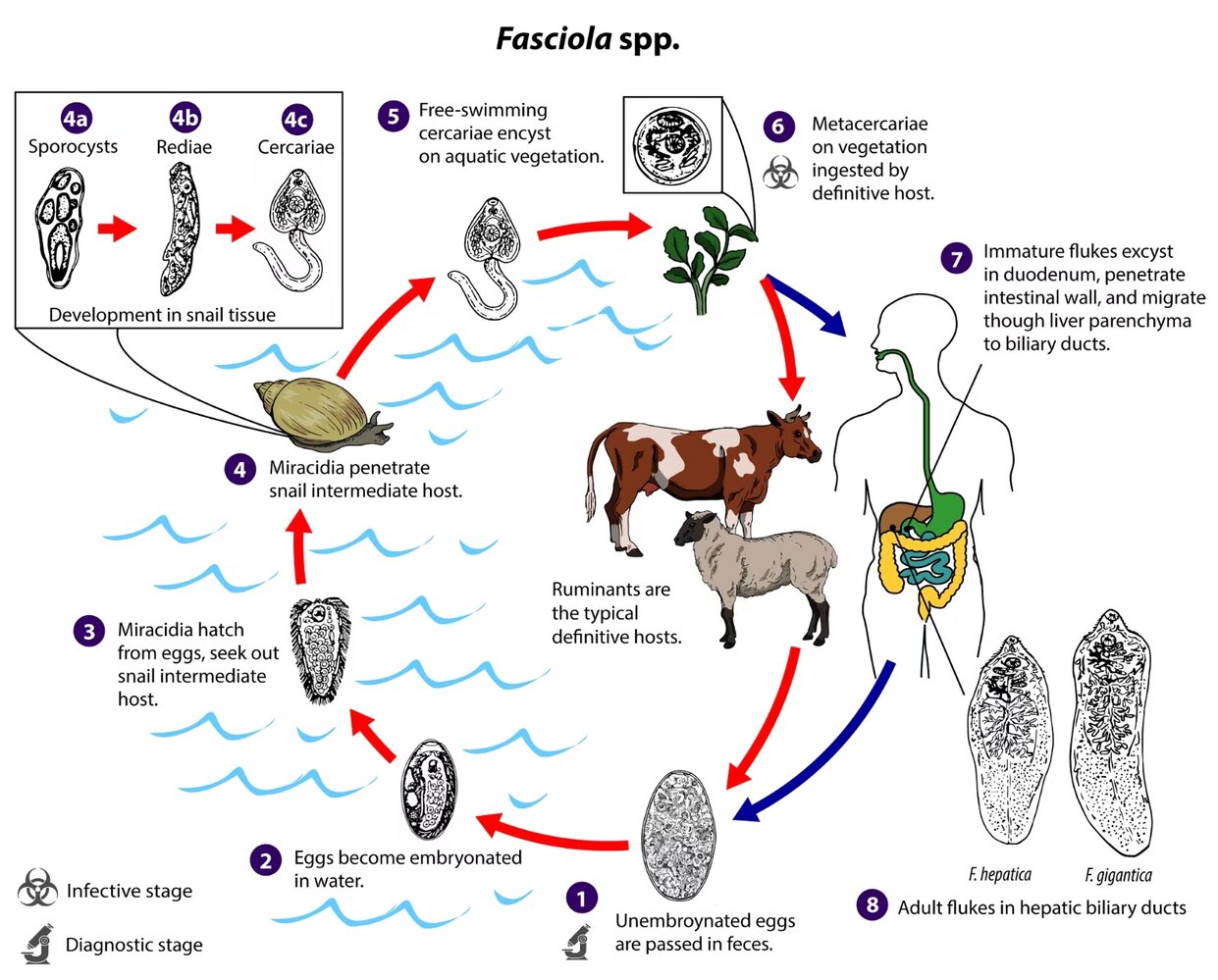
Immature eggs are discharged in the biliary ducts and passed in the stool (1). Eggs become embryonated in freshwater over ~2 weeks (2); embryonated eggs release miracidia (3), which invade a suitable snail intermediate host (4). In the snail, the parasites undergo several developmental stages (sporocysts, rediae, and cercariae). The cercariae are released from the snail (5) and encyst as metacercariae on aquatic vegetation or other substrates. Humans and other mammals become infected by ingesting metacercariae-contaminated vegetation (e.g., watercress) (6). After ingestion, the metacercariae excyst in the duodenum (7) and penetrate through the intestinal wall into the peritoneal cavity. The immature flukes then migrate through the liver parenchyma into biliary ducts, where they mature into adult flukes and produce eggs (8). In humans, maturation from metacercariae into adult flukes usually takes about 3–4 months; development of F. gigantica may take somewhat longer than F. hepatica. (Materials developed by CDC)
This image is an adaptation. Source of original image: CDC/ DPDx. Original title: “Fascioliasis”. Created by: CDC/ DPDx. Licensed under Public Domain. Modifications to original image: CDC & DPDx Logo removed.
Dicrocoeliasis
-
Pathogens [41][42]
- Dicrocoelium dendriticum (lanceolate, lancet fluke, or lancet liver fluke)
- D. hospes
-
Epidemiology [41]
- D. dendriticum: present in Europe, Asia, and North Africa, with sporadic cases in North America
- D. hospes: endemic to Sub-Saharan West Africa (e.g., Ghana, Senegal, Mali, Sierra Leone)
- Mode of transmission: consumption of infected ants [41]
- Life cycle: eggs released in the feces of ruminants (definitive hosts such as sheep, cattle, or humans) are eaten by land snails (first intermediate host) → development of larval stages within the snail, which are expelled as cercariae in slime balls → ingestion of slime balls by ants (second intermediate host), and the parasites encyst as metacercariae → ingestion of infected ants by grazing animals or humans → excystation of metacercariae in the intestine and migration directly to the bile ducts, where adult flukes mature and produce eggs that are excreted in stool [41]
-
Clinical features [41][42]
- Typically asymptomatic
- Symptoms of high fluke burden include:
- Abdominal pain
- Symptoms related to chronic cholangitis (e.g., weight loss, fatigue)
- Symptoms of acute cholecystitis (e.g., fever, RUQ pain, nausea, vomiting)
- Subcutaneous nodules containing flukes (rare)
-
Diagnostics [41][42]
- Stool microscopy: The presence of fully embryonated eggs confirms the diagnosis.
- Spurious infection (i.e., pseudoparasitism) can occur from consuming infected animal liver, resulting in the passage of eggs in the stool.
- Repeat stool examination after a liver-free diet for at least 3 days.
- Persistence of eggs: true infection
- Absence of eggs: spurious infection
-
Treatment [42]
- Indication: true parasitism (spurious infections do not require treatment)
- Pharmacological treatment options include:
- Praziquantel (off-label) [42]
- OR triclabendazole (off-label) [42]
-
Complications [41][42]
- Cholecystitis
- Liver abscess
- Chronic cholangitis
- Bile duct dilation
- Pancreatitis [51]
Opisthorchiasis
-
Pathogens [43]
- Opisthorchis viverrini (Southeast Asian liver fluke)
- Opisthorchis felineus (cat liver fluke)
-
Epidemiology [43][44]
- Geographic distribution
- O. viverrini: Southeast Asia (e.g., Thailand, Laos, Cambodia, Vietnam)
- O. felineus: Germany, Italy, Russia, Belarus, Kazakhstan, and Ukraine
- Worldwide prevalence: estimated > 27 million infections [44]
- ♂ > ♀
- Prevalence increases with age.
- Geographic distribution
- Mode of transmission: consumption of raw or undercooked freshwater fish [43]
- Life cycle: metacercariae encysted in freshwater fish are consumed by fish-eating mammals, which serve as definitive hosts (e.g., cats, dogs, humans) → excystation of metacercariae in the duodenum and migration upward into the biliary ducts, where they mature into adult flukes → production of eggs by adults, which drain into bile and are excreted in stool → uptake of eggs by freshwater snails (first intermediate host), where larval development occurs → exit of free-swimming stages from the snail and infection of freshwater fish (second intermediate host), encysting as metacercariae [43]
-
Clinical features [43][44]
- Typically asymptomatic
- Can manifest with an acute phase similar to Katayama fever (primarily with O. felineus infection)
- Mild or early infection: nonspecific symptoms (e.g., RUQ abdominal pain, dyspepsia, anorexia)
- Chronic or severe infection: hepatomegaly, malnutrition, jaundice, tenderness on liver palpation
-
Diagnostics [43][44]
- Stool microscopy: The presence of eggs confirms the diagnosis.
- PCR of stool samples may be used for species differentiation.
- Cross-sectional imaging (e.g., ultrasound, CT scan, or MRI) may be used to assess for organ damage and complications.
- Adult flukes may be recovered during surgery.
-
Differential diagnoses [43]
- Clonorchiasis (Clonorchis sinensis infection)
- Acute schistosomiasis (Katayama fever)
- Other causes of cholangitis, cholecystitis, or biliary obstruction (e.g., gallstones)
-
Treatment [44]
- Preferred: praziquantel [44]
- Alternative: albendazole
-
Complications [43][44]
- Cholangitis
- Cholecystitis
- Cholelithiasis (typically pigment stones)
- Periductal fibrosis
- Fatty liver
- Cholangiocarcinoma
-
Prevention [44]
- Annual mass drug administration (e.g., with praziquantel) in endemic areas with high prevalence
- Measures to avoid fecal contamination of water supply
- Avoidance of raw or undercooked freshwater fish
External Resources
References
- "Parasites - Toxocariasis (also known as Roundworm Infection) - Epidemiology & Risk Factors". https://web.archive.org/web/20170405065516/https://www.cdc.gov/parasites/toxocariasis/epi.html. [2013-01-10]
- AAP Committee on Infectious Diseases. "Red Book: 2021–2024 Report of the Committee on Infectious Diseases". American Academy of Pediatrics. (2021). ISBN: 9781610025218
- Committee on Infectious Disease, American Academy of Pediatrics. "Red Book: 2024-2027 Report of the Committee on Infectious Diseases, 33rd Edition". American Academy of Pediatrics. (2024). ISBN: 9781610027373
- "Parasites - Enterobiasis (also known as Pinworm Infection) - Epidemiology & Risk Factors". https://web.archive.org/web/20170318002930/https://www.cdc.gov/parasites/pinworm/epi.html. [2013-01-10]
- Weller PF. "Eosinophilia in travelers". Med Clin North Am. 76(6). :1413-1432. (1992)
- WHO. "Guideline: Preventive Chemotherapy to Control Soil-Transmitted Helminth Infections in At-Risk Population Groups". WHO. (2018). ISBN: 9789241550116
- Vu Thi N, Trung DD, Litzroth A, et al. "The hidden burden of trichinellosis in Vietnam: a postoutbreak epidemiological study.". BioMed Research International. (2013)
- "Parasites - Zoonotic Hookworm". https://web.archive.org/web/20170504011828/https://www.cdc.gov/parasites/zoonotichookworm/. [2012-10-11]
- Pearson MS, Tribolet L, Cantacessi C, et al. "Molecular mechanisms of hookworm disease: Stealth, virulence, and vaccines". J Allergy Clin Immunol. 130(1). :13-21. (2012)
- Loukas A, Hotez PJ, Diemert D, et al. "Hookworm infection". Nat Rev Dis Primers. 2(1). (2016)
- "Fish tapeworm infection". https://medlineplus.gov/ency/article/001375.htm. [2015-09-10]
- Tomáš Scholz, Hector H. Garcia, Roman Kuchta, Barbara Wicht. "Update on the Human Broad Tapeworm (Genus<i>Diphyllobothrium</i>), Including Clinical Relevance". Clin Microbiol Rev. 22(1). :146-160. (2009)
- "Parasites - Cysticercosis - Biology". https://web.archive.org/web/20170522101232/https://www.cdc.gov/parasites/cysticercosis/biology.html. [2010-11-02]
- Minciullo PL, Cascio A, Isola S, Gangemi S. "Different clinical allergological features of Taenia solium infestation". Clin Mol Allergy. 14(1). (2016)
- Garcia HH, Nash TE, Del Brutto OH. "Clinical symptoms, diagnosis, and treatment of neurocysticercosis". Lancet Neurol. 13(12). :1202-1215. (2014)
- Ralston SH, Penman ID, Strachan MWJ, Hobson R. "Davidson's Principles and Practice of Medicine". Elsevier. (2018). ISBN: 9780702070280
- "Parasites - Onchocerciasis (also known as River Blindness)". https://web.archive.org/web/20181113210542/https://www.cdc.gov/parasites/onchocerciasis/index.html. [2015-08-10]
- Thiele EA, Cama VA, Sleshi M, et al. "Detection of Onchocerca volvulus in Skin Snips by Microscopy and Real-Time Polymerase Chain Reaction: Implications for Monitoring and Evaluation Activities". Am J Trop Med Hyg. 94(4). :906-911. (2016)
- "Parasites - Loiasis". https://web.archive.org/web/20181206170245/https://www.cdc.gov/parasites/loiasis/index.html. [2015-01-20]
- Bennett JE, Dolin R, Blaser MJ. "Mandell, Douglas, and Bennett's Principles and Practice of Infectious Diseases". Elsevier Saunders. (2015). ISBN: 9781455748013
- Kelly-Hope L, Paulo R, Thomas B, et al. "Loa loa vectors Chrysops spp.: perspectives on research, distribution, bionomics, and implications for elimination of lymphatic filariasis and onchocerciasis". Parasit Vectors. 10(1). (2017)
- "CDC: Clinical Treatment of Loiasis". https://web.archive.org/web/20241218125240/https://www.cdc.gov/filarial-worms/hcp/clinical-care/loiasis.html
- CDC. "DPDx - Laboratory Identification of Parasites of Public Health Concern: Mansonellosis". (2019)
- Ta-Tang T, Crainey J, Post R, Luz S, Rubio J. "Mansonellosis: current perspectives". Res Rep Trop Med. Volume 9. :9-24. (2018)
- Ritter M, Hsu H, Lenz B, et al. "Mansonella perstans – the forgotten filaria". Trends Parasitol. 41(10). :909-921. (2025)
- Bravo F. "Emerging infections: mimickers of common patterns seen in dermatopathology". J Cutan Pathol. 33. :118-127. (2020)
- CDC. "Anisakiasis". (2019)
- Cong W, Elsheikha HM. "Biology, Epidemiology, Clinical Features, Diagnosis, and Treatment of Selected Fish-borne Parasitic Zoonoses.". Yale J Biol Med. 94(2). :297-309. (2021)
- Shamsi S, Barton D. "A critical review of anisakidosis cases occurring globally". Parasitol Res. 122(8). :1733-1745. (2023)
- Sadaow L, Sanpool O, Intapan P, et al. "A Hospital-Based Study of Intestinal Capillariasis in Thailand: Clinical Features, Potential Clues for Diagnosis, and Epidemiological Characteristics of 85 Patients". Am J Trop Med Hyg. 98(1). :27-31. (2018)
- Limsrivilai J, Pongprasobchai S, Apisarnthanarak P, Manatsathit S. "Intestinal capillariasis in the 21stcentury: clinical presentations and role of endoscopy and imaging". BMC Gastroenterol. 14(1). (2014)
- CDC. "Intestinal Capillariasis". (2020)
- CDC. " Laboratory Identification of Parasites of Public Health Concern: Trichostrongylosis". (2017)
- Bhat A, Tak H, Malik I, Ganai B, Zehbi N. "Trichostrongylosis: a zoonotic disease of small ruminants". J Helminthol. 97
- "Parasites - Guinea Worm". https://web.archive.org/web/20220409235417/https://www.cdc.gov/parasites/guineaworm/disease.html. [2022-02-04]
- Hopkins DR, Weiss AJ, Yerian S, Sapp SGH, Cama VA. "Progress Toward Eradication of Dracunculiasis — Worldwide, January 2022–June 2023". MMWR Morb Mortal Wkly Rep. 72(45). :1230-1236. (2023)
- Keiser J, Utzinger J. "Food-borne trematodiases.". Clinical Microbiology Reviews. (2009)
- O’Connell EM, Nutman TB. "Eosinophilia in Infectious Diseases". Immunol Allergy Clin North Am. 35(3). :493-522. (2015)
- James H. Diaz. "Paragonimiasis Acquired in the United States: Native and Nonnative Species". Clinical Microbiology Reviews. (2013)
- Kanpittaya J, Strobel M, Maleewong W, et al. "Different Chest Radiographic Findings of Pulmonary Paragonimiasis in Two Endemic Countries". Am J Trop Med Hyg. 83(4). :924-926. (2010)
- CDC. "Dicrocoeliasis". (2019)
- Moure Z, Zarzuela F, Espasa M, et al. "Dicrocoelium dendriticum: An Unusual Parasitological Diagnosis in a Reference International Health Unit". Am J Trop Med Hyg. 96(2). :355-357. (2017)
- CDC. "Opisthorchiasis". (2018)
- Qian M, Keiser J, Utzinger J, Zhou X. "Clonorchiasis and opisthorchiasis: epidemiology, transmission, clinical features, morbidity, diagnosis, treatment, and control". Clin Microbiol Rev. 37(1). (2024)
- CDC. "DPDx - Laboratory Identification of Parasites of Public Health Concern: Dipylidium caninum". (2019)
- Rousseau J, Castro A, Novo T, Maia C. "Dipylidium caninum in the twenty-first century: epidemiological studies and reported cases in companion animals and humans". Parasit Vectors. 15(1). :845-848. (2022)
- Tileklioglu et al. "The Importance of Eosinophilia in The Early Diagnosis of Fascioliasis, Toxocariasis and Hydatidosis". Journal of Health, Medicine and Nursing. (2020)
- Ha JS, Choi HJ, Moon JH, et al. "Endoscopic Extraction of Biliary Fascioliasis Diagnosed Using Intraductal Ultrasonography in a Patient with Acute Cholangitis.". Clinical endoscopy. 48(6). :579-82. (2015)
- "Hymenolepiasis". https://web.archive.org/web/20201017020318/https://www.cdc.gov/dpdx/hymenolepiasis/index.html. [2017-12-13]
- Paranjpe V, McCabe P, Mollah F, Bandy A, Hamerski C. "A fluke catch: biliary obstruction and pancreatitis from dicrocoeliasis". VideoGIE. 5(11). :567-568. (2020)
- Intirach J, Shu C, Lv X, et al. "Human parasitic infections of the class Adenophorea: global epidemiology, pathogenesis, prevention and control". Infect Dis Poverty. 13(1). (2024)
- Hong S-T, Fang Y. "Clonorchis sinensis and clonorchiasis, an update". Parasitol Int. 61(1). :17-24. (2012)