Summary
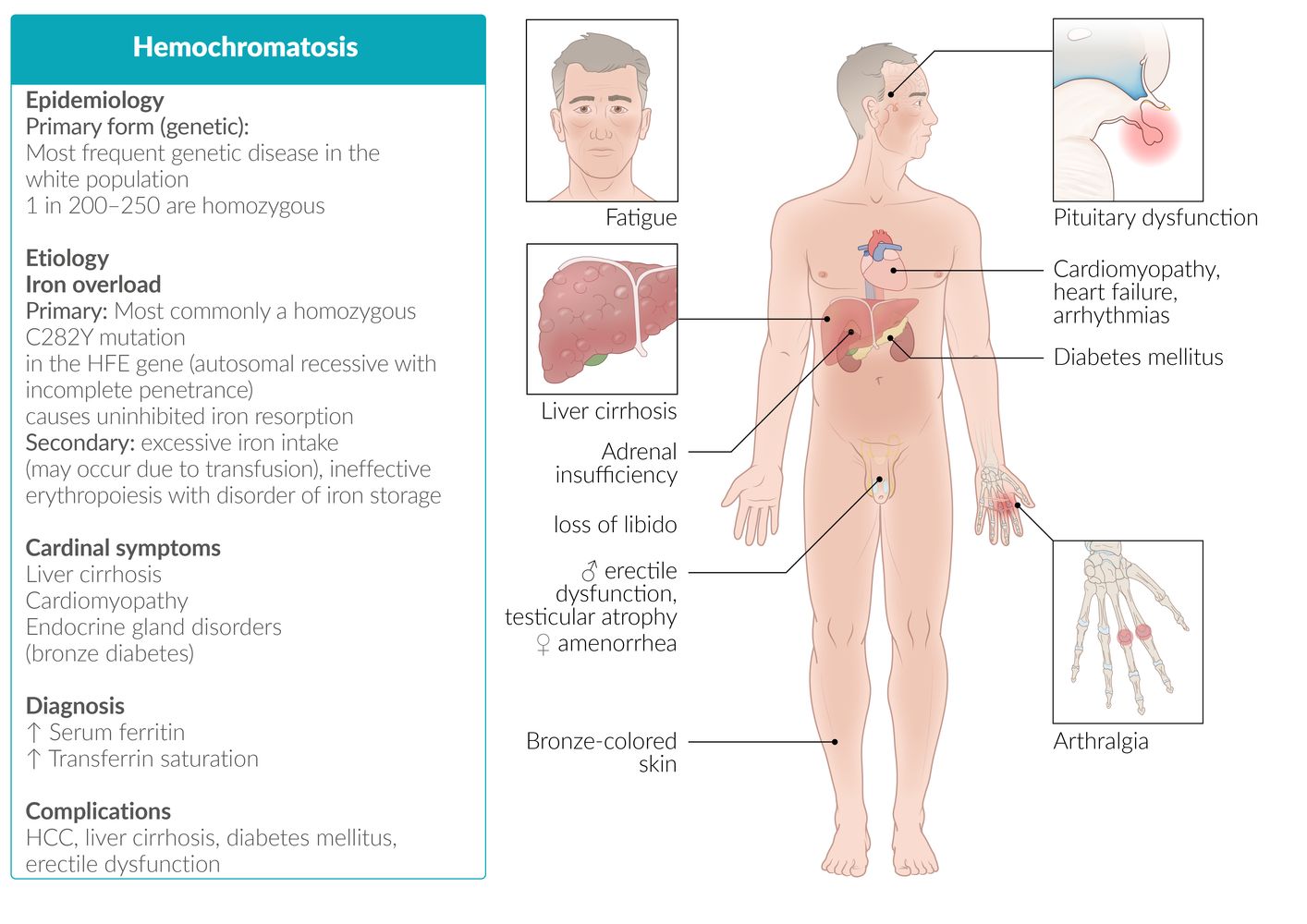
Hemochromatosis refers to a group of conditions characterized by excess iron deposition (or increased risk of excess deposition) in the body as a result of increased iron absorption. Increased iron absorption leads to iron overload as there is no physiologic method for iron excretion (except through menstrual bleeding). Primary iron overload (primary/hereditary hemochromatosis) is caused by mutations in genes involved in regulating gastrointestinal iron absorption, resulting in iron over-absorption. Secondary iron overload (sometimes referred to as secondary hemochromatosis) is caused by conditions affecting iron metabolism (e.g., chronic liver disease) or excessive iron ingestion or infusion (e.g., from repeated transfusions to treat beta-thalassemia major). Patients with primary iron overload often only become symptomatic after irreversible damage has occurred, commonly in the third to fifth decades of life. Early clinical features are often nonspecific (e.g., fatigue, decreased libido, hyperpigmentation, symptoms of diabetes mellitus, arthralgia). Laboratory findings of elevated serum ferritin combined with elevated transferrin saturation are highly suggestive of iron overload. Genetic testing, MRI abdomen, and, occasionally, liver biopsy may be used to confirm the diagnosis. Treatment with therapeutic phlebotomy or chelating agents (e.g., deferoxamine) can prevent or mitigate the downstream effects of parenchymal iron deposition (e.g., cardiomyopathy, arrhythmia). The liver is the most commonly affected organ, and the development of cirrhosis is associated with an increased risk of hepatocellular carcinoma. Patients with iron overload should be advised to avoid alcohol consumption and vitamin C supplementation, as they increase iron absorption, which may lead to disease progression.

© AMBOSS
Epidemiology
- Prevalence: the most frequent genetic disease in the white population
-
Age of onset: individuals > 40 years
- Symptoms start to show when body iron levels reach > 20 g.
- Before menopause, women lose iron via menstruation and pregnancy, which slows down iron accumulation within the body. As a result, symptom onset occurs later in women (typically postmenopausal) than in men.
References:[1][2][3]
Epidemiological data refers to the US, unless otherwise specified.
Etiology
Primary (hereditary) hemochromatosis
- Classical and most frequent form: adult hemochromatosis type I
-
Homozygous or heterozygous for the HFE gene defect
- Located on chromosome 6
- Most commonly affects C282Y and H63D
- Associated with HLA-A3 genotype
- Inheritance: autosomal recessive with incomplete penetrance
-
Homozygous or heterozygous for the HFE gene defect
- Further forms: Hemochromatosis types II–IV are also hereditary, but significantly less frequent.
HLA A3 as in HA3mochromatosis!
Secondary iron overload (secondary hemochromatosis)
-
Caused by iron overload
- Transfusion-related (e.g., in individuals with beta-thalassemia major or other forms of chronic anemia requiring chronic transfusion)
- Ineffective erythropoiesis
- Thalassemia
- Sickle-cell anemia
- Sideroblastic anemia (e.g., hereditary sideroblastic anemia; anemia of chronic disease)
- Excessive alcohol consumption
References:[2][4]
Pathophysiology
Hemochromatosis type I
- The HFE gene regulates iron homeostasis (see “Iron” in the articles on trace elements).
- HFE gene defect (homozygous) → defective binding of transferrin to its receptor → ↓ hepcidin synthesis by the liver → unregulated ferroportin activity in enterocytes → ↑ intestinal iron absorption → iron accumulation throughout the body → damage to the affected organs
In hereditary hemochromatosis, decreased hepcidin leads to iron overload. In secondary hemochromatosis, iron overload leads to increased hepcidin immediately after a blood transfusion (unless liver fibrosis or cirrhosis, which leads to decreased hepcidin synthesis, is present).




References:[5][6]
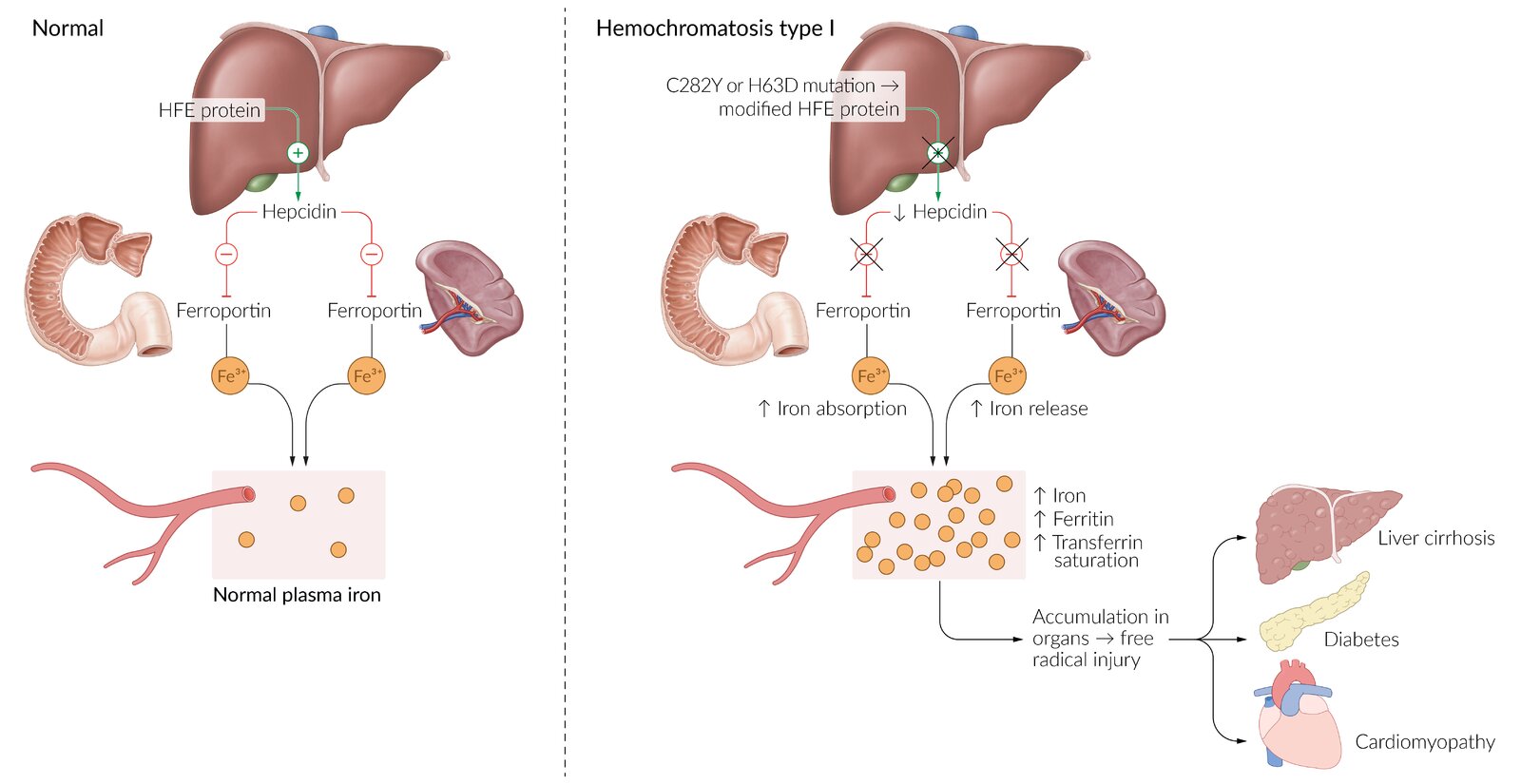
Left: Iron homeostasis is regulated by the HFE gene. HFE regulates levels of hepcidin, a protein that reduces the transport of iron from the cells to the bloodstream via the ferroportin transport protein.
Right: Hemochromatosis results from the mutation of the HFE gene → reduced hepcidin production → unregulated ferroportin activity → iron accumulation throughout the body → end-organ damage
© AMBOSS
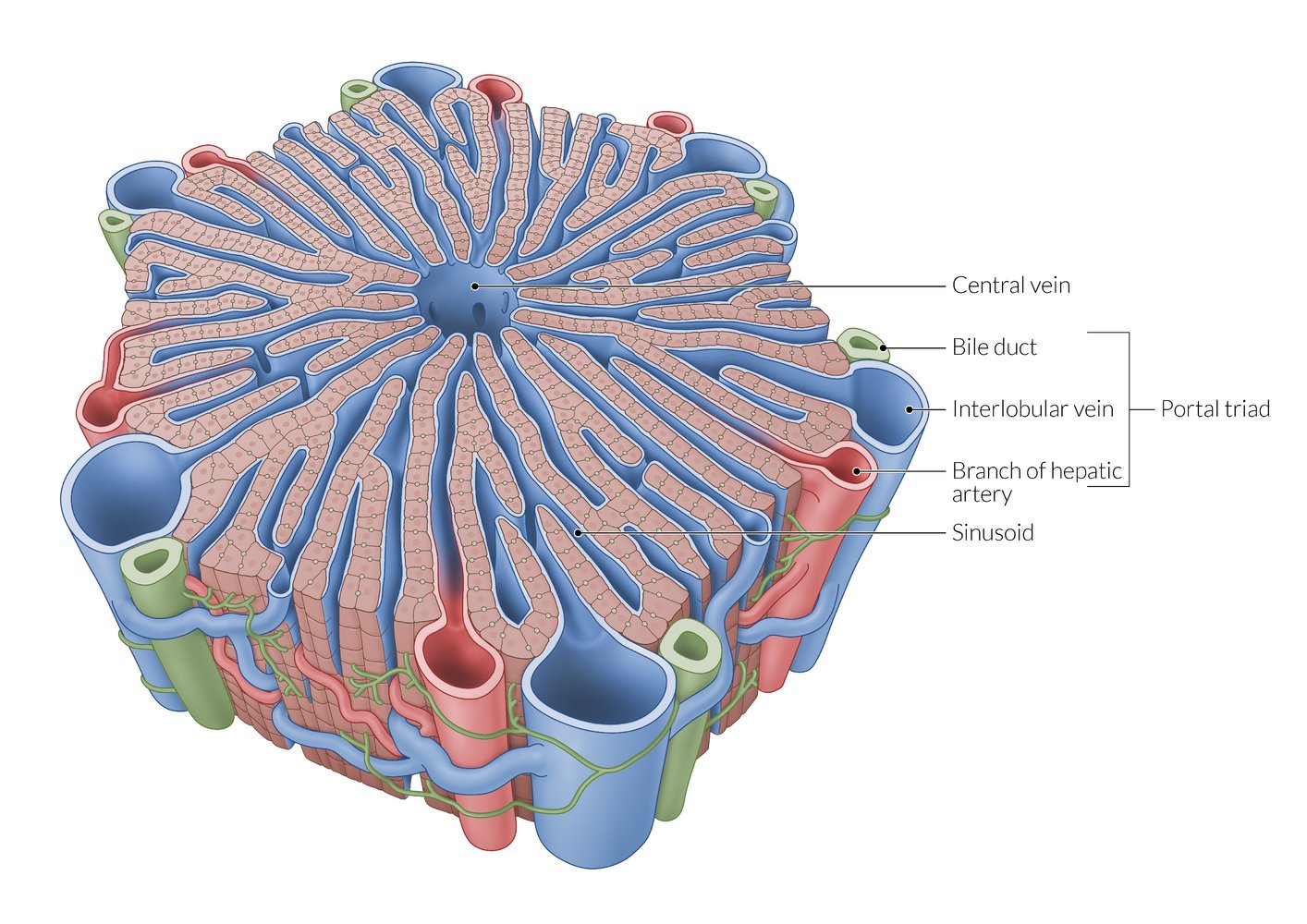
A lobule is a roughly hexagonal structural unit in the liver, separated from adjacent lobules by connective tissue. In each lobule, plates of hepatocytes are separated by hepatic sinusoids. At the vertices, branches of the hepatic artery and portal vein are arranged with bile ducts into portal triads. The flow of blood is from peripheral to central, as blood from the arteries and veins in the portal triads mixes in the sinusoids and drains via a central vein.
Note that sources differ regarding the distribution of portal triads, with some sources depicting them at every vertex of the hepatic lobules (as shown here) and others at only every second vertex.
© AMBOSS
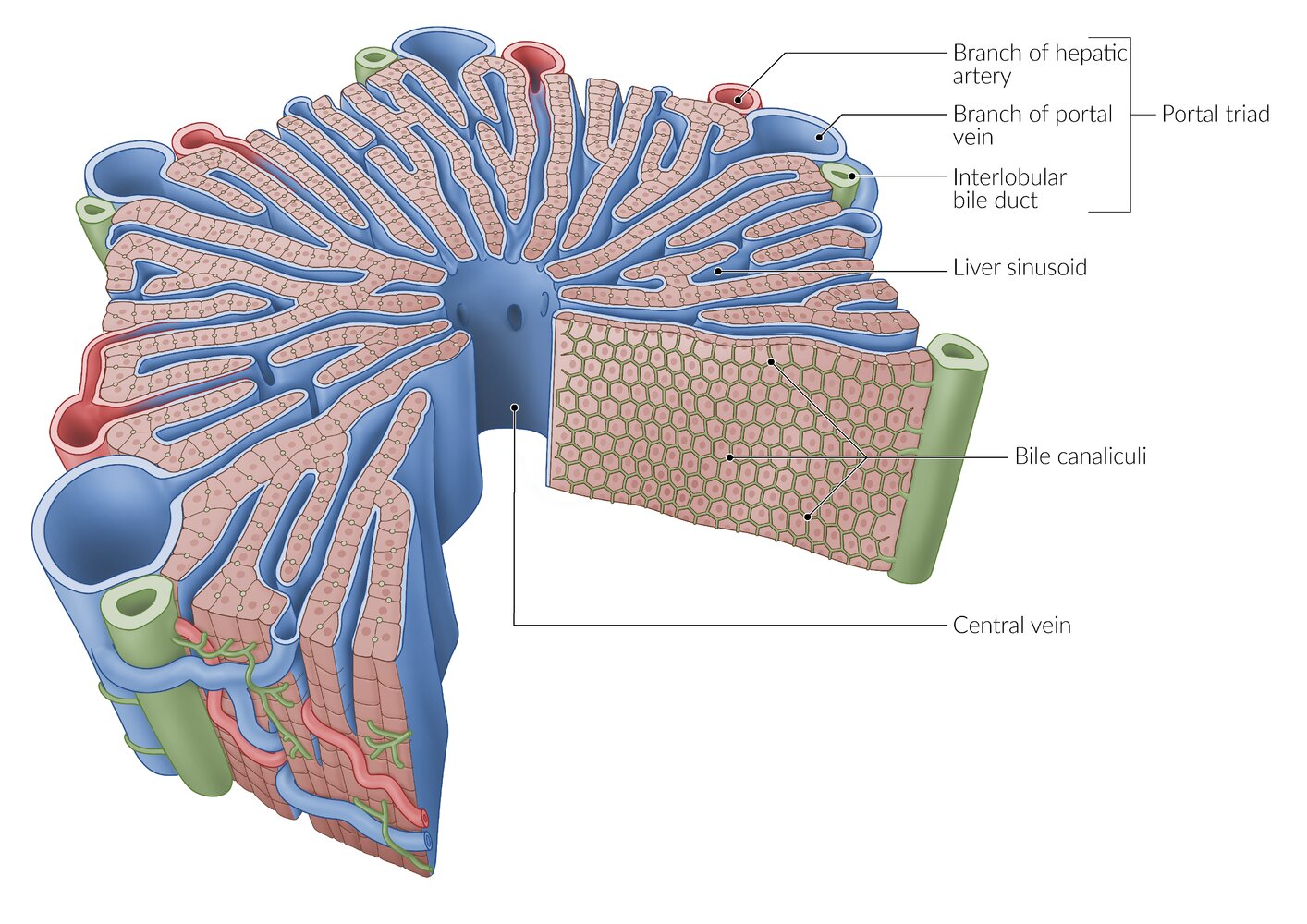
A lobule is a roughly hexagonal structural unit in the liver, separated from adjacent lobules by connective tissue. In each lobule, plates of hepatocytes are separated by hepatic sinusoids. At the vertices, branches of the hepatic artery and portal vein are arranged with bile ducts into portal triads. The flow of blood is from peripheral to central, as blood from the arteries and veins in the portal triads mixes in the sinusoids and drains via a central vein.
Between the hepatocytes is a network of bile canaliculi, which drains bile towards the interlobular bile ducts in the portal triads (the flow of bile is from central to peripheral, and thus opposite to the flow of blood).
© AMBOSS
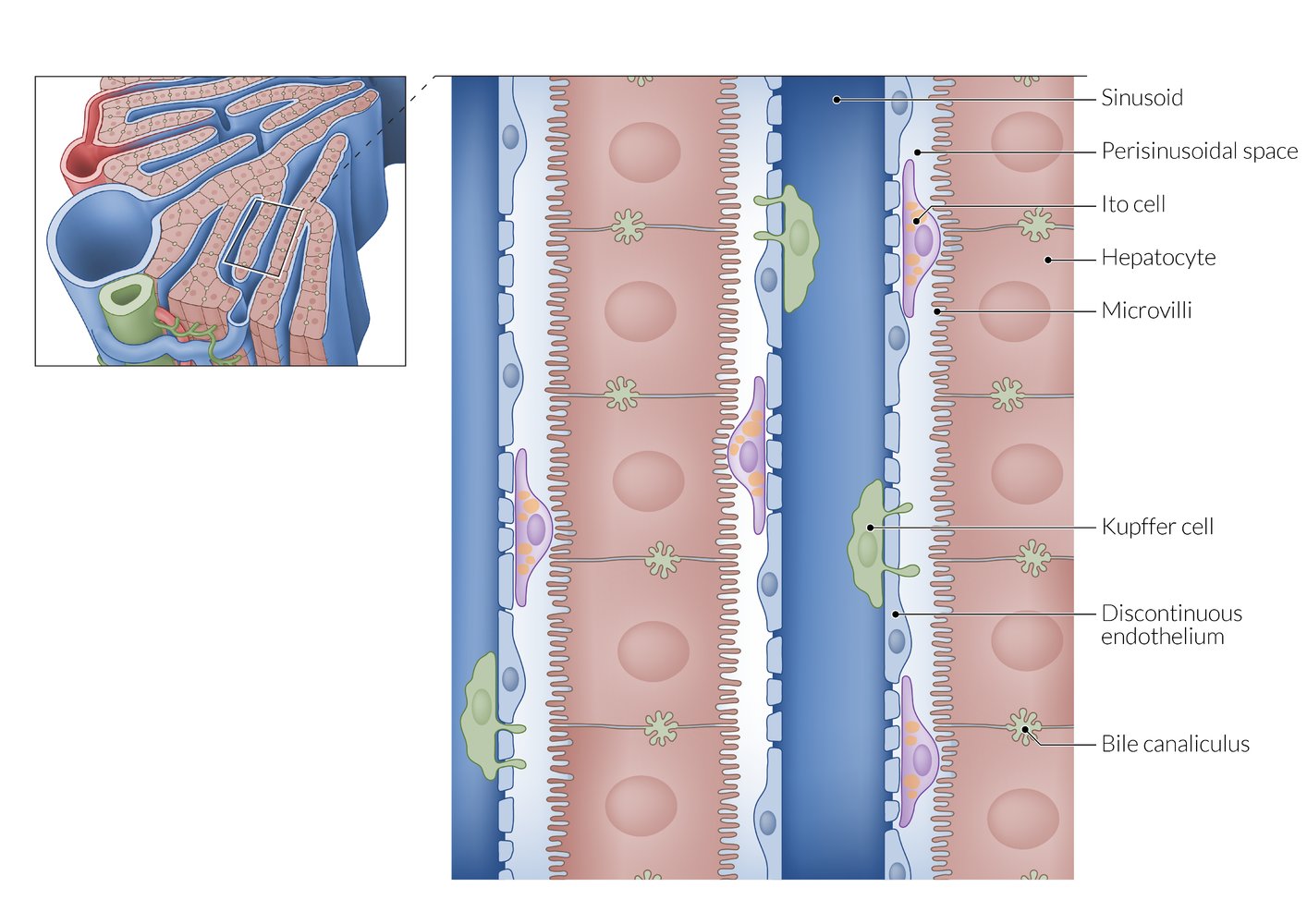
From the sinusoids, plasma can enter the perisinusoidal space through the highly fenestrated endothelium. Microvilli on the basolateral surface of the hepatocytes increase the surface area for efficient substance exchange. The apical surfaces of adjacent hepatocytes form the bile canaliculi, which drain into the peripherally located interlobular bile ducts.
© AMBOSS
Clinical features
Hemochromatosis is asymptomatic in 75% of cases. [2]
General symptoms
- Fatigue, lethargy
- Increased susceptibility to infections [7]
Organ-specific symptoms
-
Liver
- Abdominal pain
- Hepatomegaly
- Cirrhosis
- Increased risk of hepatocellular carcinoma (common cause of death) [8]
- Pancreas: signs of diabetes mellitus (polydipsia, polyuria)
- Skin: : hyperpigmentation, bronze skin
- Pituitary gland: hypogonadism, erectile dysfunction, testicular atrophy, loss of libido, amenorrhea [9]
- Joints: : arthralgia (typically symmetrical arthropathy of the MCP joints II and III); , chondrocalcinosis (accumulation of calcium pyrophosphate)
-
Heart
-
Cardiomyopathy due to cardiac siderosis
- Occurs in individuals with iron overload (e.g., due to hereditary hemochromatosis or repeated blood transfusions)
- Can lead to chamber remodeling and subsequent dilated (reversible); or restrictive cardiomyopathy
- The process of accumulation of iron in cardiac tissue.
- Cardiac arrhythmias: paroxysmal atrial fibrillation (most common), sinus node dysfunction, complete AV block, atrial and ventricular tachyarrhythmias, and sudden cardiac death
- Congestive heart failure
-
Cardiomyopathy due to cardiac siderosis
In combination with diabetes mellitus, bronze-colored skin pigmentation is also referred to as "bronze diabetes.”
© AMBOSS
Diagnosis
General principles [10]
- Early diagnosis and management are critical to avoid permanent organ damage and early mortality.
- Diagnosis is often incidental.
- Iron overload can progress slowly over decades.
- Patients with significant iron overload may be asymptomatic.
- Clinical features of advanced disease: organ dysfunction (e.g., of the liver, pancreas, or heart)
- Suggestive laboratory findings: elevated serum ferritin and transferrin saturation
- Genetic testing confirms hereditary hemochromatosis.
Laboratory studies [10]
-
Diagnosis of iron overload [10][11]
-
↑ Serum ferritin
- ≥ 200 ng/mL for premenopausal patients
- ≥ 300 ng/mL for all other patients
- ↑ Transferrin saturation (≥ 45%)
- ↑ Serum iron
- ↓ Total iron-binding capacity
-
↑ Serum ferritin
-
Genetic testing (HFE gene) [10]
- Indications: unexplained iron overload and/or first-degree relative with hereditary hemochromatosis
- Findings: Homozygous C282Y, homozygous H63D, or heterozygous C282Y/H63D mutation in the HFE gene confirms the diagnosis.
-
Additional studies
- ↑ Hepatocellular enzymes (e.g., AST, ALT)
- CBC may identify iron-loading anemia (e.g., sideroblastic anemia).
Elevated serum ferritin in conjunction with elevated transferrin saturation is highly suggestive of iron overload. The combination of normal serum ferritin and transferrin saturation has a 97% negative predictive value. [10]
Imaging [10]
-
MRI abdomen (without contrast)
- Used to estimate hepatic iron concentration (HIC)
- Hepatic iron pattern can help to distinguish between hereditary hemochromatosis and secondary iron overload.
-
Additional imaging: based on symptoms
- Echocardiogram, cardiac MRI, and/or X-ray chest to evaluate for cardiac manifestations (e.g., cardiomyopathy)
- Plain radiography to evaluate for joint manifestations (e.g., arthritis of the second and third MCPs)

Liver biopsy [10]
-
Indications
-
Homozygous HFE C282Y mutation plus either of the following:
- Serum ferritin level > 1000 ng/mL
- Additional risk factors for cirrhosis
- All other patients: if needed to stage fibrosis or investigate an alternative cause of liver disease [12]
-
Homozygous HFE C282Y mutation plus either of the following:
-
Histology findings
- Concentration and distribution pattern of hepatic iron
- Hemosiderin (normally golden yellow on microscopy) appears blue with the Prussian blue stain.
- Pattern of hereditary hemochromatosis: pronounced parenchymal siderosis (accumulation of hemosiderin within the tissue) in hepatocytes and bile duct epithelium
- Pattern of secondary iron overload: Kupffer cells (specialized macrophages) containing hemosiderin
- Presence and degree of hepatic fibrosis (see “Pathophysiology” in “Cirrhosis”)
- Concentration and distribution pattern of hepatic iron
The use of liver biopsy in hemochromatosis is limited, as the concentration and distribution pattern of hepatic iron can be assessed using noninvasive MRI. [13]



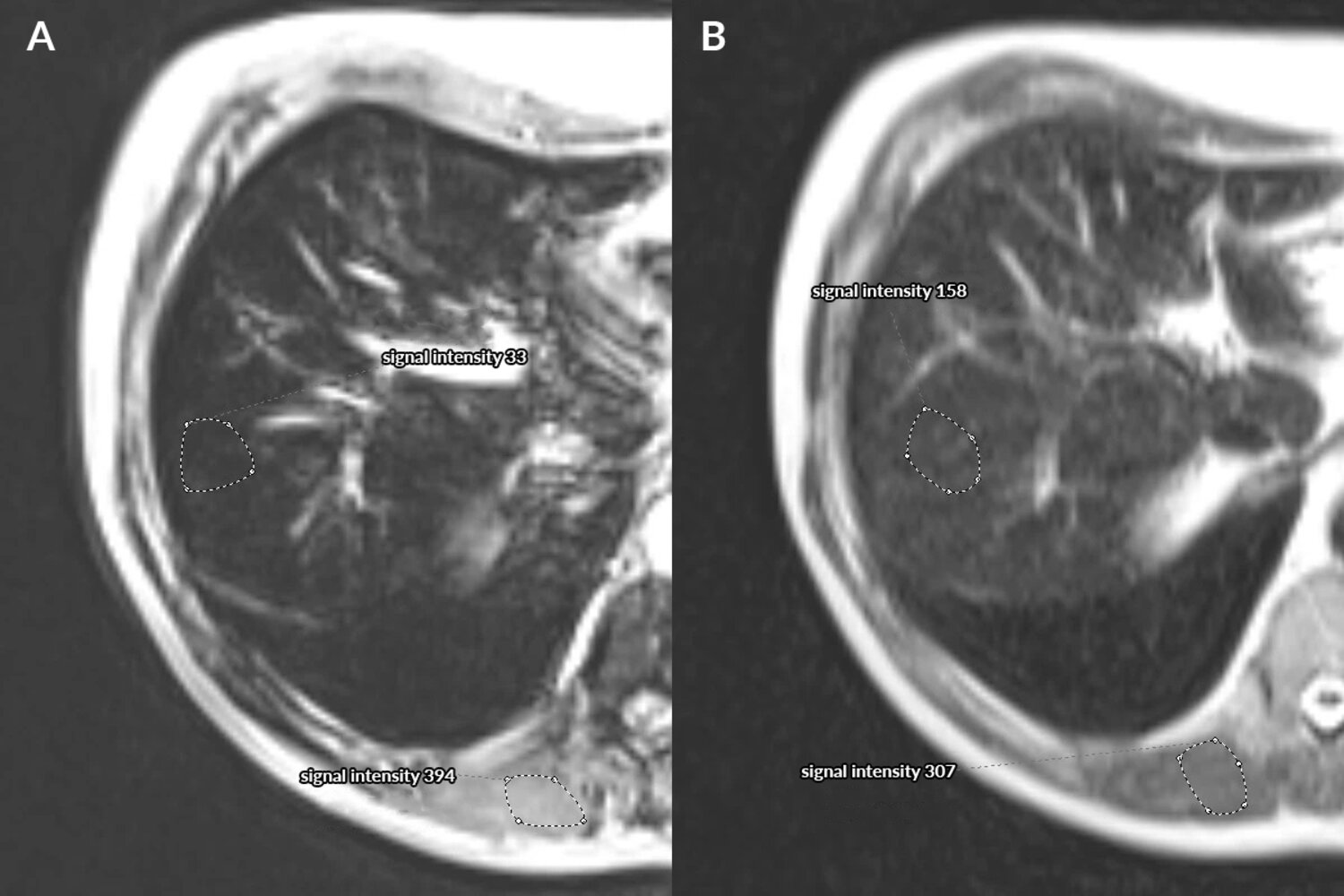
MRI abdomen (liver; a: T2-weighted gradient echo; b: Express; axial plane)
The liver is hypointense on both the gradient echo and Express sequences, with signal intensities of 33 and 158, respectively. These values are lower than those of the paraspinal musculature (394 and 307). Paraspinal musculature does not accumulate iron. Lower hepatic signal is consistent with hemochromatosis.
MRI can identify excessive hepatic iron accumulation and estimate iron concentration. A signal intensity ratio (liver to muscle) can be used to determine hepatic iron concentration.
Source: “Fig 3, In: The role of MR imaging in detection of hepatic iron overload in patients with cirrhosis of different origins” by Szurowska E, Sikorska K, Iżycka-Świeszewska E et al., BMC Gastroenterology, licensed under CC BY 2.0. Modifications: original letters replaced with Lato letters; translation and removal of parts of the in-image text.
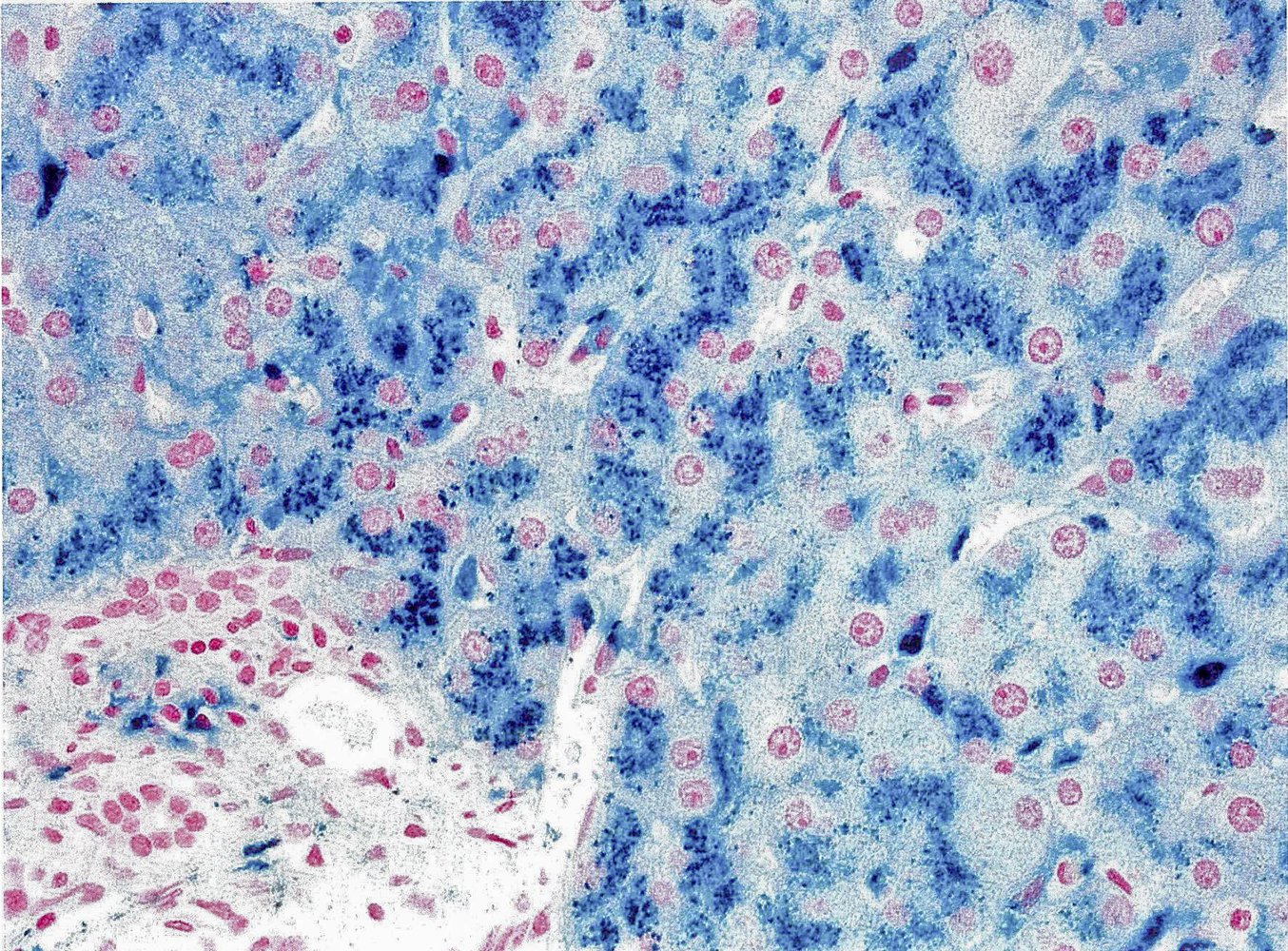
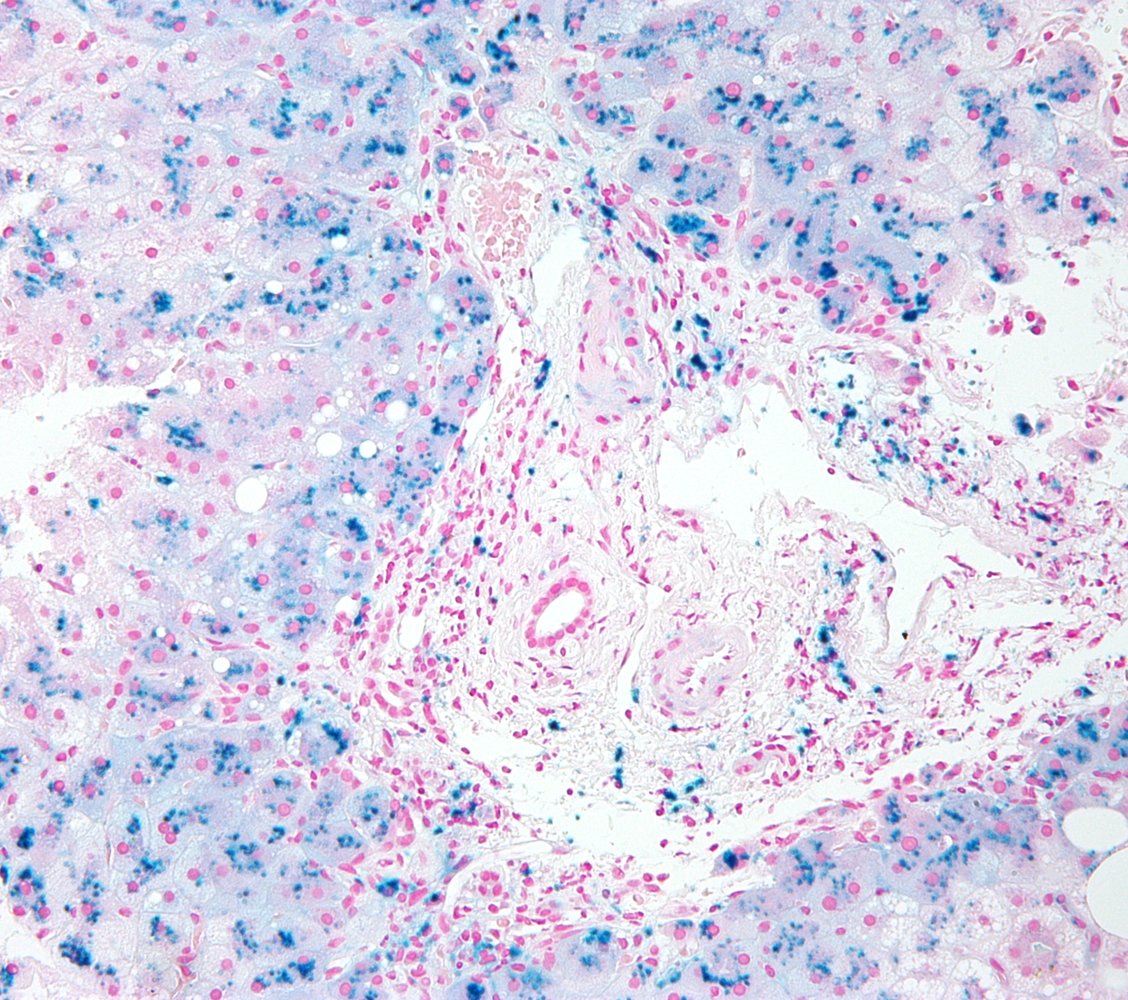
Photomicrograph of a liver tissue sample (Prussian blue stain)
Prussian blue stains the iron deposits dark blue (green arrows) and the nuclei bright red. A portal triad (P; green overlay) is visible in the lower left corner.
Source: © IMPP
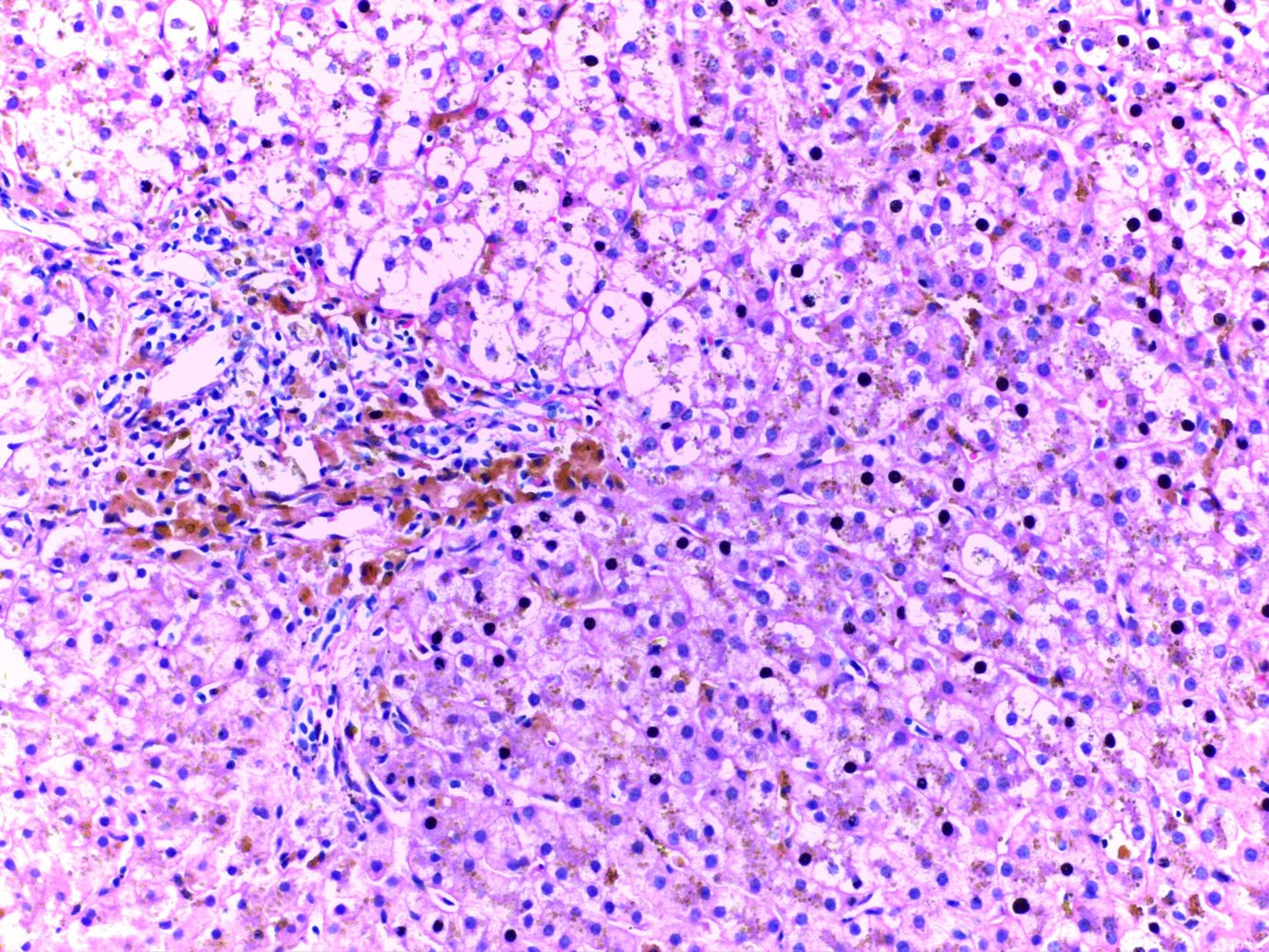
Photomicrograph of a liver biopsy (H&E stain, high magnification)
Deposits of coarse granular brown pigment are visible within the hepatocytes (examples indicated by blue circles). Further deposits also appear in portal tract macrophages (examples indicated by yellow circles).
These deposits stained positive with the iron stain (prussian blue stain; not shown here), which leads to the diagnosis of hemochromatosis.
Source: “Micrograph of hemochromatosis liver showing hepatocytes in brownish yellow color” by Department of Pathology, Calicut Medical College, Wikimedia Commons, licensed under CC BY-SA 4.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 4.0.
{kind=link}
Photomicrograph of a liver biopsy (Prussian blue stain)
Multiple hemosiderin deposits are visible within the hepatocytes.
This is the typical appearance of siderosis in hemochromatosis.
Source: “Hemosiderosis high mag” by Nephron, Wikimedia Commons, licensed under CC BY 3.0.
{kind=link}
Treatment
Approach [10]
Management is guided by a specialist (e.g., hepatologist, gastroenterologist, or hematologist).
- Hereditary hemochromatosis: Therapeutic phlebotomy and chelation therapy are the primary options for iron removal.
-
Secondary iron overload
- Address the underlying cause (e.g., alcohol use disorder) to stop iron loading.
- Consider iron removal on a case-by-case basis. [12]
- Counseling and education: Early treatment can stabilize organ damage, improve symptoms, and increase life expectancy.
Therapeutic phlebotomy [10][12]
-
Indications
- First-line treatment for hereditary hemochromatosis (including asymptomatic patients)
- Consider in patients with secondary iron overload (e.g., for patients with symptomatic porphyria cutanea tarda)
-
Contraindications
- Inability to tolerate the procedure (e.g., due to anxiety)
- Low hemoglobin (e.g., due to iron-loading anemia)
- Conditions sensitive to fluid shifts (e.g., end-stage liver disease, congestive heart failure)
-
Therapeutic regimen
- Initial phase: ∼ 500 mL of blood removed weekly over 1–2 sessions; serum ferritin goal of 50–100 ng/mL
- Maintenance phase: ∼ 500 mL of blood removed 3–4 times per year; serum ferritin goal of 50 ng/mL
Iron chelation therapy [10]
-
Indications
- First-line treatment for secondary iron overload due to iron-loading anemia
- Consider for hereditary hemochromatosis refractory to therapeutic phlebotomy and patients with contraindications to phlebotomy.
- Chelating agents: deferoxamine, deferasirox, or deferiprone [14][15][16]
-
Important considerations
- High cost
- Significant risk of adverse effects
Check renal function prior to administration of chelating agents because of the risk of nephrotoxicity and renal accumulation.
Drugs that delete iron (Fe) in hemochromatosis: deFeroxamine, deFerasirox, deFeriprone
Liver transplantation [10]
-
Indications
- Decompensated cirrhosis
- Hepatocellular carcinoma
- Important consideration: Untreated iron overload is not a contraindication to transplantation.
Additional therapies [10]
-
Dietary changes
- Advise avoidance of iron and vitamin C supplements.
- Encourage strict avoidance of alcohol.
- No need to reduce dietary iron
-
Proton pump inhibitors (PPIs)
- Can decrease iron absorption
- Consider as an adjunct to phlebotomy.
- Only recommended for patients with an indication for PPIs (e.g., GERD)
-
Erythrocytapheresis [17]
- Selective removal of red blood cells from the patient's circulation
- Useful for patients with thrombocytopenia or hypoproteinemia
In patients with iron overload, alcohol use significantly increases the risk of progression of both liver fibrosis and cirrhosis.
Patient counseling [10]
- Early treatment of iron overload may:
- Improve fatigue and skin hyperpigmentation
- Reverse early organ damage (e.g., elevated liver chemistries, early cardiomyopathy)
- Increase life expectancy
- It may be possible to prevent the progression of advanced complications , but they cannot be reversed.
Related One-Minute Telegram
One-Minute Telegram 114-2025-3/3: Hemochromatosis comorbidities: iron overload may not be the only link
Interested in the newest medical research, distilled down to just one minute? Sign up for the One-Minute Telegram in “Tips and links” below.
External Resources
References
- "Epidemiology and diagnostic testing for hemochromatosis and iron overload". http://onlinelibrary.wiley.com/doi/10.1111/ijlh.12347/full. [2015-05-14]
- "Recognition and Management of Hereditary Hemochromatosis". http://www.aafp.org/afp/2002/0301/p853.html. [2002-03-01]
- McLaren GD, Gordeuk VR. "Hereditary hemochromatosis: insights from the Hemochromatosis and Iron Overload Screening (HEIRS) Study". Hematology Am Soc Hematol Educ Program. 2009(1). :195-206. (2009)
- Schrier SL, Bacon BR, Mentzer WC, Raby BA, Tirnauer JS. "Genetics of Hereditary Hemochromatosis". UpToDate. UpToDate. https://www.uptodate.com/contents/genetics-of-hereditary-hemochromatosis. [2017-07-20]
- Fleming RE, Britton RS, Waheed A, Sly WS, Bacon BR. "Pathophysiology of hereditary hemochromatosis". Semin Liver Dis. 25(4). :411-419. (2005)
- Vela D. "Low hepcidin in liver fibrosis and cirrhosis; a tale of progressive disorder and a case for a new biochemical marker". Molecular Medicine. 24(1). (2018)
- Khan FA, Fisher MA, Khakoo RA. "Association of hemochromatosis with infectious diseases: expanding spectrum". International Journal of Infectious Diseases. 11(6). :482-487. (2007)
- Kowdley KV. "Iron, hemochromatosis, and hepatocellular carcinoma". Gastroenterology. 127(5). :S79-S86. (2004)
- "Hemochromatosis and sexual dysfunction". http://www.nature.com/ijir/journal/v15/n6/full/3901019a.html. [2003-03-31]
- Kowdley KV, Brown KE, Ahn J, Sundaram V. "ACG Clinical Guideline: Hereditary Hemochromatosis". Am J Gastroenterol. 114(8). :1202-1218. (2019)
- European Association For The Study Of The Liver. "EASL clinical practice guidelines for HFE hemochromatosis". J Hepatol. 53(1). :3-22. (2010)
- Bacon BR, Adams PC, Kowdley KV, Powell LW, Tavill AS. "Diagnosis and management of hemochromatosis: 2011 Practice Guideline by the American Association for the Study of Liver Diseases". Hepatology. 54(1). :328-343. (2011)
- Salomao MA. "Pathology of Hepatic Iron Overload". Clin Liver Dis. 17(4). :232-237. (2021)
- Caligiuri M, Levi MM, Kaushansky K, et al. "Williams Hematology, 9E". McGraw-Hill Education / Medical. (2015). ISBN: 9780071833004
- "Guidelines for the Management of Non Transfusion Dependent Thalassaemia (NTDT)". https://www.ncbi.nlm.nih.gov/books/NBK190453/. [2017-01-01]
- "Guidelines for the Management of Transfusion Dependent Thalassaemia (TDT)". https://www.ncbi.nlm.nih.gov/pubmed/25610943. [2014-01-01]
- Rombout-Sestrienkova E, van Kraaij MGJ, Koek GH. "How we manage patients with hereditary haemochromatosis". Br J Haematol. 175(5). :759-770. (2016)