Summary
Hemolytic uremic syndrome (HUS) is a thrombotic microangiopathy, a condition in which microthrombi, consisting primarily of platelets, form and occlude the microvasculature. HUS is characterized by microangiopathic hemolytic anemia (MAHA), thrombocytopenia, and acute kidney injury (AKI), referred to as the HUS triad. Shiga toxin-associated HUS (ST-HUS) is the most common form and predominantly affects children. It is most often caused by Shiga toxin-producing Escherichia coli (STEC) O157:H7 and usually manifests with diarrhea 5–14 days before the onset of HUS. Non-Shiga toxin-associated HUS (non-ST-HUS) is caused by complement pathway dysregulation (in complement-mediated HUS), infection, medication, transplant, or autoimmune disease. Diagnosis is made with laboratory studies that confirm the HUS triad and exclude disseminated intravascular coagulation (DIC) and thrombotic thrombocytopenic purpura (TTP). In patients with suspected HUS, stool studies should be performed to assess for STEC and Shiga toxin. Management is primarily supportive and includes administration of IV fluids, packed RBC transfusions, and renal replacement therapy as needed. Pharmacotherapy with complement inhibitors (eculizumab or ravulizumab) is recommended for complement-mediated HUS. Early management of STEC-positive illness that avoids antibiotics and antimotility agents can decrease the risk of developing HUS.
Thrombotic thrombocytopenic purpura (TTP) is discussed separately.
Epidemiology
-
ST-HUS
- Causes ∼ 90% of HUS cases in children [1]
- Most common in children 6 months to 5 years of age [1][2][3][4]
-
Non-ST-HUS
- Causes 10% of HUS cases in children; more common in adults [1][4][5]
- Can manifest at any age, depending on the underlying cause [6]
Epidemiological data refers to the US, unless otherwise specified.
Etiology
Shiga toxin-associated HUS [1][2][3]
ST-HUS is caused by bacterial production of Shiga toxin (i.e., verotoxin).
-
Enterohemorrhagic E. coli (EHEC) subset of STEC
- Serotype O157:H7 is the primary cause; of HUS in North America. [2][7]
- Usually transmitted via undercooked beef, raw fruits, leafy vegetables, and unpasteurized dairy products
- Shigella dysenteriae type 1
Up to 20% of children with STEC O157:H7 infection will develop HUS. [1]
Non-Shiga toxin-associated HUS [1][8][9]
Non-ST-HUS, sometimes called “atypical HUS,” is unrelated to Shiga-toxin. [6][9][10][11]
- Complement-mediated HUS: complement pathway dysregulation from genetic mutations and/or anti-complement antibodies
- Non-Shiga toxin infections: S. pneumoniae, influenza, HIV
-
Other causes
- Autoimmune diseases (e.g., SLE, antiphospholipid syndrome)
- Organ or bone marrow transplant
- Cytotoxic drugs (e.g., chemotherapeutic agents, calcineurin inhibitors)
S. pneumoniae-associated HUS mainly occurs in children < 2 years of age with invasive pneumococcal infections (e.g., meningitis, sepsis, complicated pneumonia). [1][12][13]
Pathophysiology
HUS is a thrombotic microangiopathy, a condition characterized by the formation of microthrombi that occlude the microvasculature. The other main thrombotic microangiopathy is TTP. The two conditions have some pathophysiology and clinical findings in common but different etiologies. HUS in children is most commonly caused by bacterial toxins. [14]
- Infection with enterohemorrhagic E. coli (EHEC) or another causative organism
- Mucosal inflammation facilitates bacterial toxins; entering systemic circulation.
- Toxins cause endothelial cell damage (especially in the glomerulus ).
- Damaged endothelial cells secrete cytokines that promote vasoconstriction and platelet microthrombus formation at the site of damage (intravascular coagulopathy) → thrombocytopenia (consumption of platelets)
- RBCs are mechanically destroyed as they pass through the platelet microthrombi occluding small blood vessels (i.e., arterioles, capillaries) → hemolysis (schistocytes), and end-organ ischemia and damage, especially in the kidneys → decreased glomerular filtration rate (GFR)
STEC O157:H7 infection → Shiga toxin in systemic circulation → toxin-mediated endothelial injury → microthrombus formation → blockage of small vessels → RBC fragmentation (hemolysis) and end-organ damage
Clinical features
See “Complications” for additional clinical features.
Gastrointestinal prodrome [1][2][15]
- Abdominal pain, nausea, vomiting, and/or diarrhea that typically progresses from watery to bloody
- Usually precedes the onset of HUS by 5–14 days [2][15]
- Fever is usually absent (low-grade if present).
- Often absent in non-ST-HUS
Symptoms of the HUS triad [1][2][15]
- Clinical features of anemia: fatigue, weakness, dyspnea, pallor, jaundice
-
Clinical features of AKI
- Hypertension (often severe)
- Oliguria or anuria (typically within 10 days of onset) [1]
-
Clinical features of thrombocytopenia (may be asymptomatic)
- Petechiae, purpura
- Mucosal bleeding
- Prolonged bleeding after minor cuts
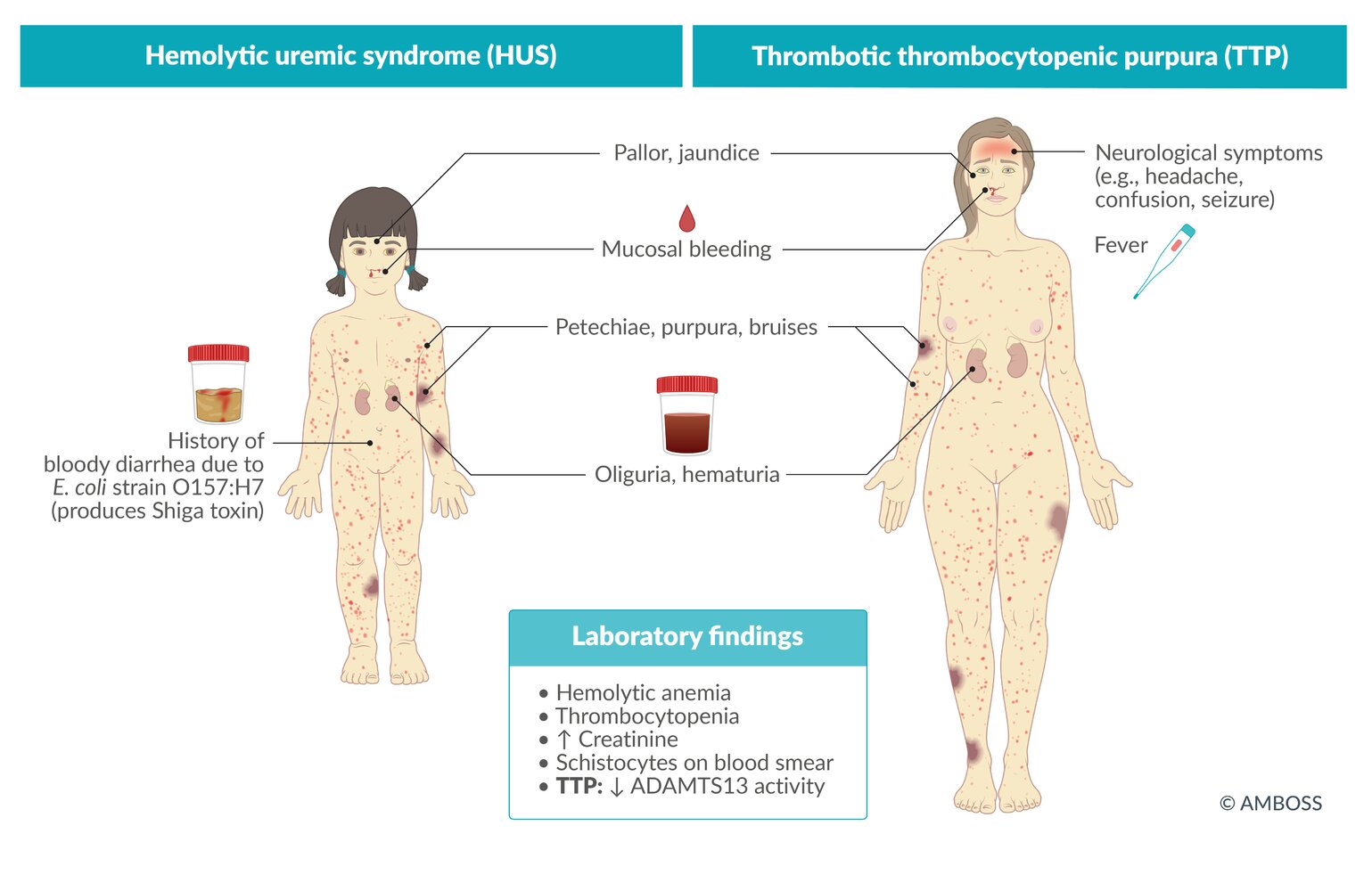
The typical HUS patient is a preschooler who has had a diarrheal illness within the past 5–14 days and presents with petechiae, jaundice, and oliguria.
The classic TTP pentad includes the HUS triad plus fever and neurological signs. [16]
Diagnosis
Approach [1][3][17]
Simultaneously begin diagnostic evaluation and management of HUS in consultation with nephrology and hematology.
- Obtain initial studies to:
- Confirm the HUS triad with CBC, BMP, hemolytic indices, and urinalysis.
- Assess for end-organ damage with liver enzymes, troponin, lactate, and lipase.
- Exclude DIC and TTP with coagulation studies and ADAMTS13 testing.
- Once the diagnosis is confirmed, determine the underlying cause.
- All patients: Collect stool studies to assess for Shiga-toxin. [1][2]
- Clinical signs of meningitis, sepsis, and/or pneumonia: Evaluate for S. pneumoniae infection.
- Specialists may recommend additional studies to assess for other causes.
Confirmation of HUS triad [1][3][17]
- Thrombocytopenia: typically the earliest laboratory abnormality and rapidly progresses [2]
-
Microangiopathic hemolytic anemia with laboratory evidence of intravascular hemolysis
- ↓ Hemoglobin (typically < 8 g/dL) [1]
- ↓ Haptoglobin
- ↑ Indirect bilirubin
- ↑ Reticulocytes
- ↑ LDH
- ↑ Schistocytes on blood smear
- Direct Coombs test: negative
-
Acute kidney injury
- ↑ BUN, ↑ creatinine, and electrolyte abnormalities
- Hemoglobinuria and/or proteinuria on urinalysis
The HUS triad includes thrombocytopenia, microangiopathic hemolytic anemia, and AKI, often manifesting in that order. [1][2][3]



Exclusion of differential diagnoses of HUS [1][2][3]
-
Coagulation studies to distinguish HUS from DIC [18]
- PT, aPTT, fibrin degradation products, and D-dimer levels are usually normal in HUS.
- See also “Differential diagnoses of DIC by laboratory findings.”
-
ADAMTS13 testing to distinguish HUS from TTP
- ADAMTS13 activity: > 10% in HUS [3]
- ADAMTS13 antibodies: absent in HUS [18]
Stool studies [2][15][19]
- Sample collection: stool sample (preferred) or rectal swab (alternative) [2][19]
-
Tests
- Stool culture to assess for STEC O157:H7 and S. dysenteriae pathogens
- Immunoassay for Shiga-toxin
- NAAT (e.g., with GI PCR) for Shiga-toxin genes
Additional studies for underlying cause [2][3]
-
Infectious studies based on clinical presentation
- Negative stool studies: Serological testing for STEC O157:H7 may be considered.
- Signs of invasive S. pneumoniae infection
- Obtain infectious studies (e.g., NAATs, cultures, and/or imaging).
- See “Diagnostics for pediatric CAP” and “Diagnostics for meningitis.”
- Other: influenza testing, HIV tests
-
Advanced studies are typically ordered by specialists.
- Suspected complement-mediated HUS: complement studies (e.g., C3 levels or genetic testing for complement gene variants)
- Other studies (e.g., SLE diagnostics) are obtained based on clinical presentation.
STEC infection and post-diarrheal HUS are nationally notifiable diseases in the US. Notify the CDC for suspected or confirmed cases. [20][21]
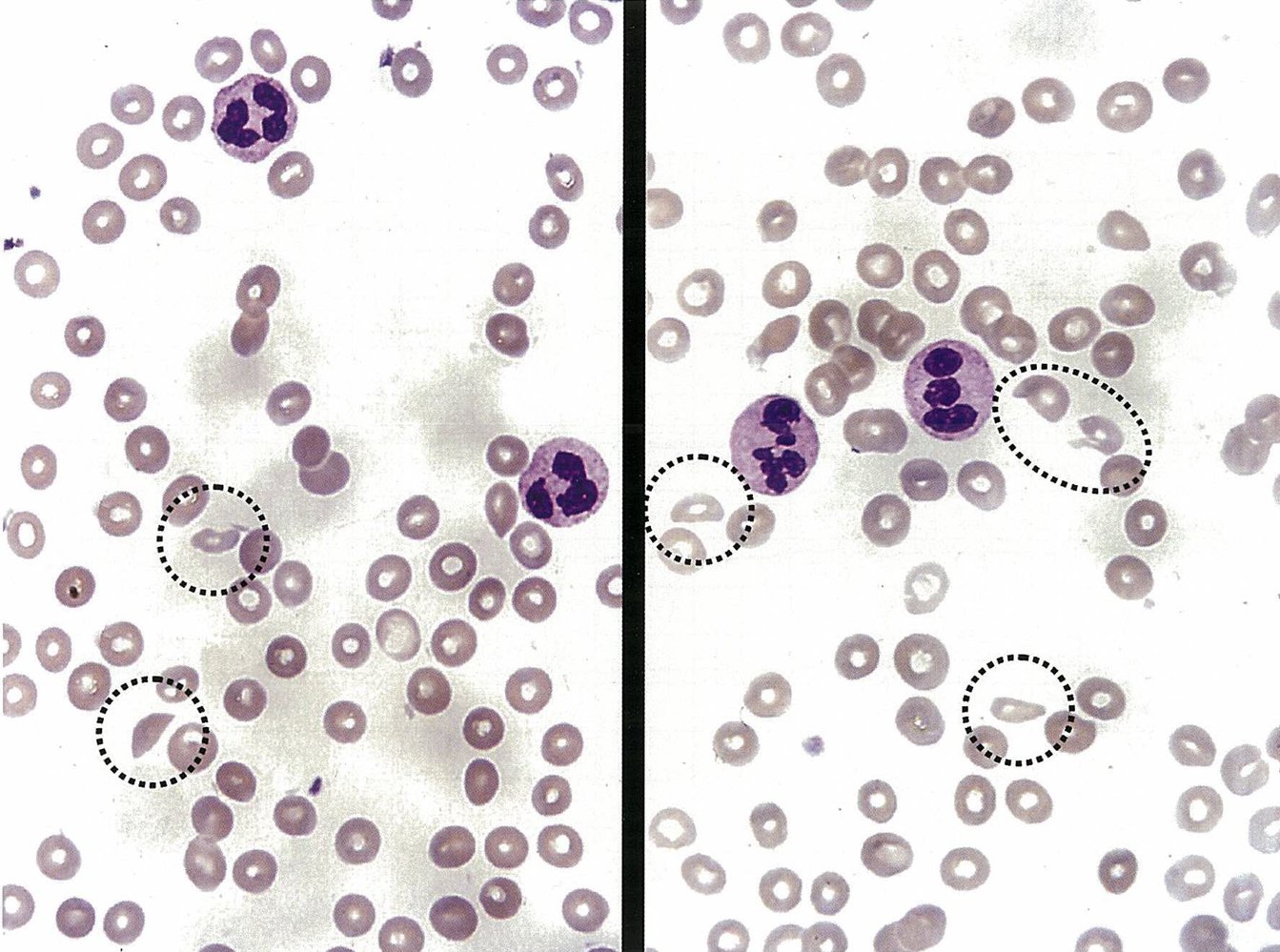
Photomicrographs of a peripheral blood smear
Erythrocytes with a convex and a concave side can be seen among the normal erythrocytes. These fragmented erythrocytes are known as schistocytes (black circles).
Schistocytes are a diagnostic finding of hemolytic uremic syndrome (HUS). They may also be caused by other forms of microangiopathic hemolytic anemia or mechanical damage to erythrocytes.
Source: © IMPP
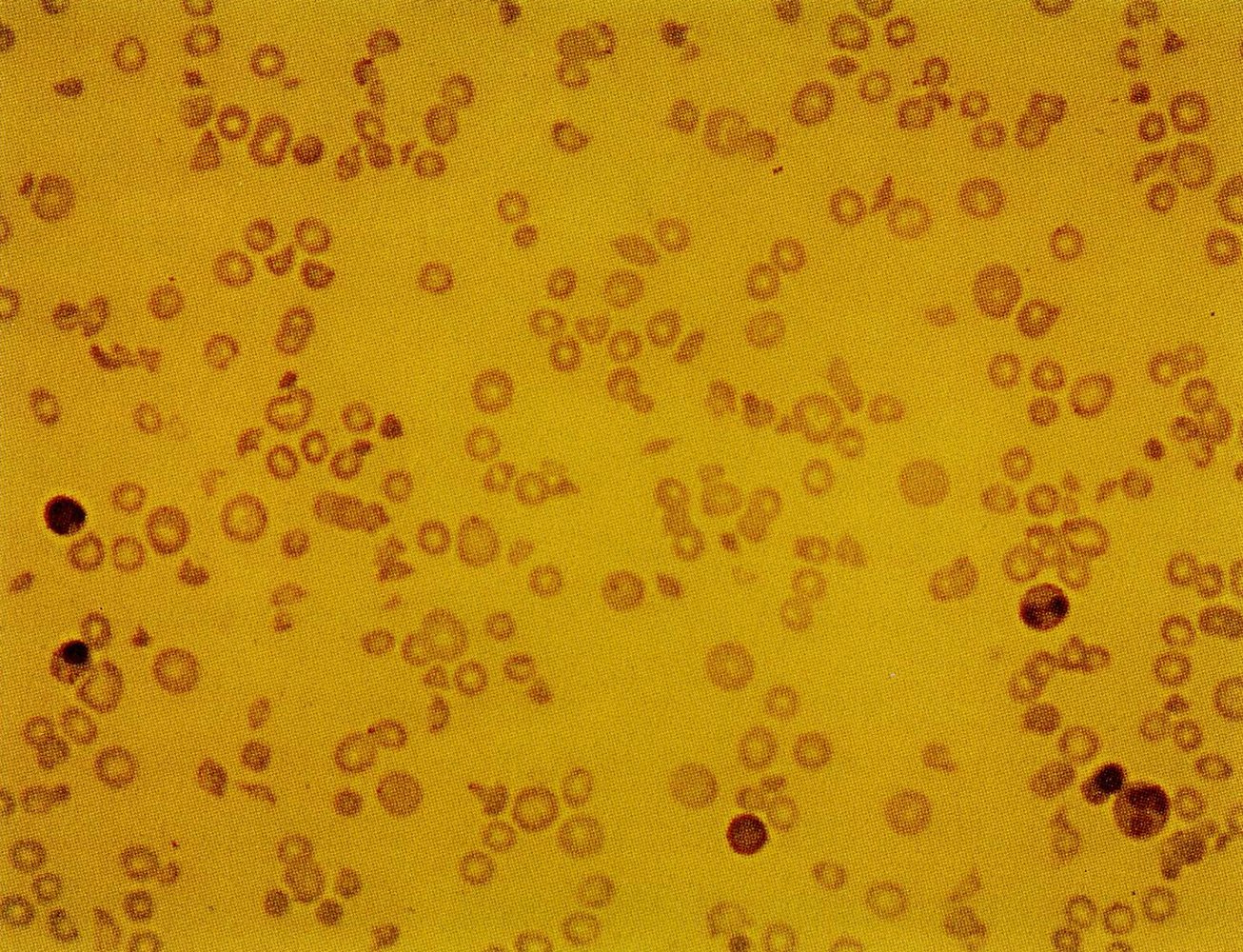
Photomicrograph of a peripheral blood smear (Giemsa stain; high magnification)
Fragmented erythrocytes (schistocytes) with a normal convex border on one side and concave or straight border on the other side (examples indicated by blue overlay) are visible. The majority of erythrocytes appear normal.
Schistocytes are a typical diagnostic finding in hemolytic uremic syndrome (HUS).
Source: © IMPP
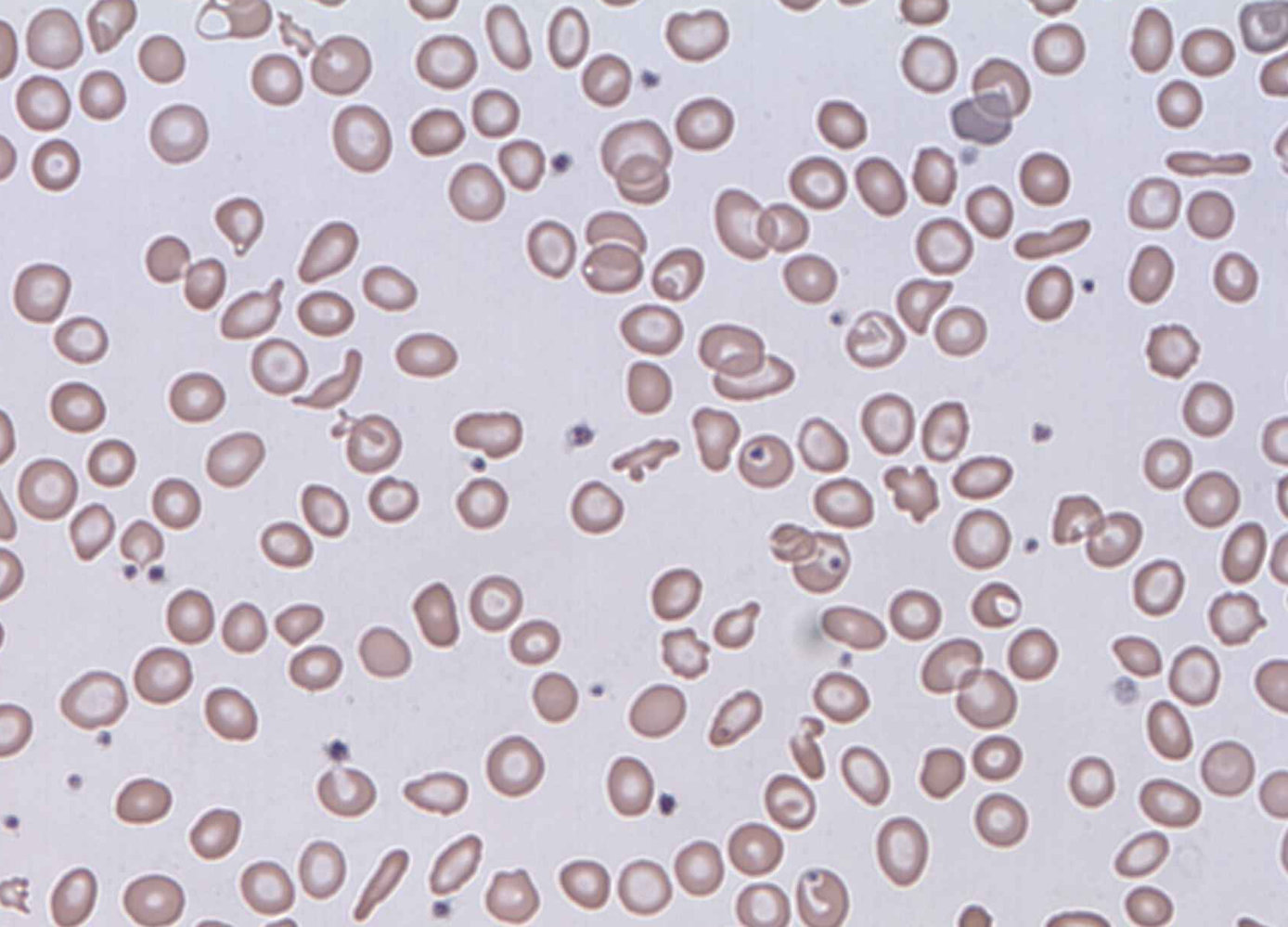
Photomicrograph of a peripheral blood smear
Fragmented erythrocytes, which are convex on one side (examples indicated by blue lines) and concave on the other (examples indicated by yellow lines), are visible among the normal erythrocytes. These fragmented erythrocytes are referred to as schistocytes.
Schistocytes are a diagnostic finding in patients with microangiopathic hemolytic anemias and those with mechanical damage to erythrocytes (e.g., from artificial heart valves).
Source: “Schistocytes” by Prof. Osaro Erhabor, Wikimedia Commons, licensed under CC0 1.0. Modifications: image cropped. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
{kind=link}
Differential diagnoses
- Other causes of microangiopathic hemolytic anemia and platelet destruction include:
- TTP [1][22]
- DIC
-
For additional information, see:
- “Differential diagnosis of platelet disorders”
- “Workup for underlying causes of MAHA”

The differential diagnoses listed here are not exhaustive.
© AMBOSS
Management
Initial management [1][2][3]
All patients with HUS should be admitted to a facility with dialysis support in consultation with nephrology and hematology. [23][24]
- Provide IV fluid therapy; with isotonic saline (see “Hemodynamic support in patients with AKI”).
- Replete serum electrolytes and correct acid-base disorders.
- Administer transfusions if clinically indicated.
- Indications for pRBC transfusion: packed RBC transfusions (multiple may be required)
- Hemodynamically significant bleeding: platelet transfusions
- Indications for renal replacement therapy: Initiate RRT.
- Assess for and manage complications of HUS (e.g., hypertension) as needed.
Avoid platelet transfusions unless patients have significant bleeding or require an invasive procedure, as transfusions can exacerbate microangiopathy. [2]
Cause-specific management [1][2][3]
-
ST-HUS
- Does not require additional management
- Avoid antibiotics.
-
S. pneumoniae-associated HUS [12][13]
- Treat ongoing S. pneumoniae infection with antibiotics (e.g., ceftriaxone, vancomycin).
- See “Empiric antibiotic therapy for pediatric CAP” and “Treatment for meningitis in children.”
-
Complement-mediated HUS
- Preferred treatment: terminal complement inhibitors (eculizumab or ravulizumab)
- Alternative treatment: plasma exchange therapy
Terminal complement inhibitors increase the risk of meningococcal infection; coordinate appropriate prophylaxis (e.g., immunization, antibiotics) as indicated. [8][25]
Ongoing management [1][2][3][19]
- Continue serial monitoring until symptoms resolve and laboratory parameters normalize.
- Inform patients with ST-HUS about the ongoing risk for transmission to others. Recommend:
- Hand hygiene to prevent transmission
- Monitoring of household contacts for symptoms
- Follow up throughout childhood to monitor for long-term renal complications (e.g., hypertension, chronic kidney disease).
Complications
Microthrombus formation in HUS can result in end-organ damage that affects various organs. [2]
-
CNS [26]
- Seizures
- Paresis
- Stroke
- Coma
-
GI tract
- Hemorrhagic colitis
- Bowel necrosis, perforation, stricture
- Peritonitis
- Intussusception
- Heart: cardiomyopathy, heart failure, pericardial effusion [27]
- Lung: respiratory distress syndrome, pulmonary hemorrhage, pleural effusion
- Pancreas: pancreatitis, insulin-dependent hyperglycemia
- Liver: hepatomegaly, elevated transaminases
-
Kidney
- Hypertension
- Chronic kidney disease
- End-stage renal disease
")
We list the most important complications. The selection is not exhaustive.
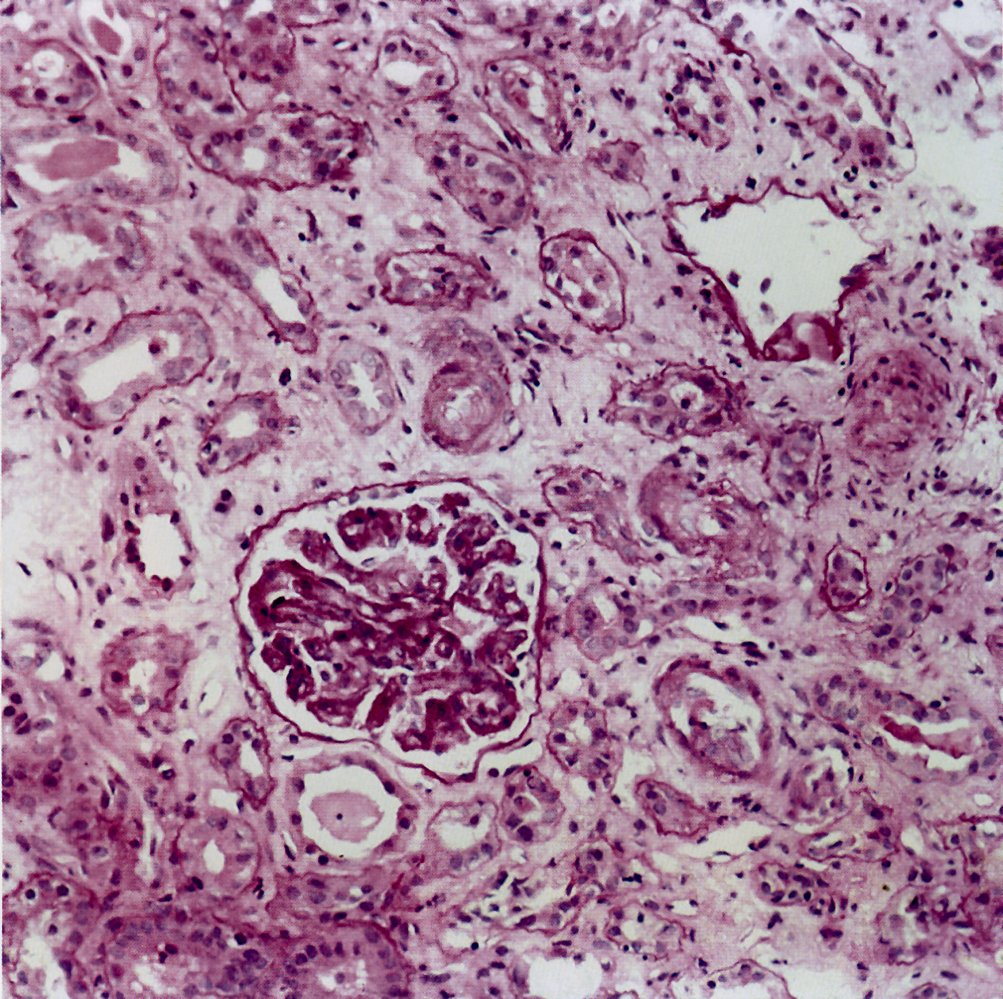
Photomicrograph of renal tissue (H&E stain; high magnification)
The renal corpuscle in the center of the image is surrounded by numerous atrophic tubules (examples indicated by blue overlay) and partly occluded vessels with eosinophil hyaline material (fibrin and platelet aggregates; indicated by green overlay). Also, interstitial fibrosis (examples indicated by red overlay) and interstitial edema (examples indicated by yellow overlay) can be seen within the surrounding tissue.
The amount of interstitial fibrosis indicates nephrosclerosis.
Source: © IMPP
Prognosis
The prognosis depends primarily on prompt initiation of treatment. Timely treatment can prevent acute complications (AKI, coma, and death) as well as progression to chronic renal failure.
- With treatment, the mortality rate of HUS is < 5%. [1]
- Renal involvement in children [28][29]
- During the acute phase, up to 50% of patients require RRT. [1]
- Up to 50% of patients develop long-term renal sequelae, with 5% becoming dialysis-dependent. [1]
- Non-ST-HUS has a less favorable prognosis and a higher risk of progressing to end-stage renal disease. [30]
Prevention
- Optimize management of STEC-positive illness, especially in patients with Shiga toxin 2 infection, to prevent progression to HUS. [1][2][19]
- Avoid antibiotics, narcotics, and antimotility agents. [2][3][19]
- Provide early isotonic IV fluids. [19]
- Reassess daily with clinical evaluation and laboratory studies until symptoms improve and laboratory parameters stabilize. [2][3][19]
Avoid antibiotics and antimotility agents in patients with diarrhea and STEC infection as they can increase the risk of HUS. [2][3]
References
- Fraustro M, Clemente Melissa. "An Overview of Pediatric Hemolytic Uremic Syndrome". Pediatr Rev. 46(1). :3-12. (2025)
- Stephen B. Freedman, Nicole C.A.J. van de Kar, Phillip I. Tarr. "Shiga Toxin-Producing Escherichia coli and the Hemolytic–Uremic Syndrome". N Engl J Med. 389(15). :1402-1414. (2023)
- Viteri B, Saland JM. "Hemolytic Uremic Syndrome". Pediatrics in Review. 41(4). :213-215. (2020)
- Loirat C, Frémeaux-Bacchi V. "Atypical hemolytic uremic syndrome". Orphanet J Rare Dis. 6(1). :60. (2011)
- Fremeaux-Bacchi V, Fakhouri F, Garnier A, et al. "Genetics and outcome of atypical hemolytic uremic syndrome: a nationwide French series comparing children and adults.". Clin J Am Soc Nephrol. 8(4). :554-62. (2013)
- Afshar-Kharghan V. "Atypical hemolytic uremic syndrome". Hematology. American Society of Hematology. Education Program. 2016(1). :217-225. (2016)
- "FoodNet Fast". https://web.archive.org/web/20241223215518/https://wwwn.cdc.gov/FoodNetFast/HUS. [2023-06-28]
- Loirat C, Fakhouri F, et al. "An international consensus approach to the management of atypical hemolytic uremic syndrome in children". Pediatr Nephrol. 31(1). :15-39. (2015)
- Kavanagh D, Ardissino G, Brocklebank V, et al. "Outcomes from the International Society of Nephrology Hemolytic Uremic Syndromes International Forum". Kidney Int. 106(6). :1038-1050. (2024)
- Nester CM, Feldman DL, Burwick R, et al. "An expert discussion on the atypical hemolytic uremic syndrome nomenclature—identifying a road map to precision: a report of a National Kidney Foundation Working Group". Kidney Int. 106(3). :326-336. (2024)
- Jokiranta TS. "HUS and atypical HUS". Blood. 129(21). :2847-2856. (2017)
- Agarwal HS, Latifi SQ. "Streptococcus Pneumoniae-Associated Hemolytic Uremic Syndrome in the Era of Pneumococcal Vaccine". Pathogens. 10(6). (2021)
- Young HL, Brown CC, Crawford B, Blaszak RT, Prodhan P. "Streptococcus pneumoniae associated hemolytic uremic syndrome in children". Front Pediatr. 11. (2023)
- Zoja C, Buelli S, Morigi M. "Shiga toxin-associated hemolytic uremic syndrome: pathophysiology of endothelial dysfunction". Pediatr Nephrol. 25(11). :2231-2240. (2010)
- "CDC Yellow Book 2024". https://web.archive.org/web/20241220194104/https://wwwnc.cdc.gov/travel/yellowbook/2024/infections-diseases/escherichia-coli-diarrheagenic. [2023-05-01]
- Joly BS, Coppo P, Veyradier A. "Thrombotic thrombocytopenic purpura". Blood. 129(21). :2836-2846. (2017)
- Phillips J, Henderson AC. "Hemolytic Anemia: Evaluation and Differential Diagnosis". Am Fam Physician. 98(6). :354-361. (2018)
- Boral BM, Williams DJ, Boral LI. "Disseminated Intravascular Coagulation". Am J Clin Pathol. 146(6). :670-680. (2016)
- Shane AL, Mody RK, Crump JA, et al. "2017 Infectious Diseases Society of America Clinical Practice Guidelines for the Diagnosis and Management of Infectious Diarrhea". Clin Infect Dis. 65(12). :e45-e80. (2017)
- "Shiga Toxin-producing Escherichia coli (STEC) 2018 Case Definition". https://web.archive.org/web/20250227224341/https://ndc.services.cdc.gov/conditions/shiga-toxin-producing-escherichia-coli/. [2021-04-16]
- "National Notifiable Diseases Surveillance System". https://web.archive.org/web/20241224174625/https://ndc.services.cdc.gov/conditions/hemolytic-uremic-syndrome-post-diarrheal/. [2021-04-16]
- Chiasakul T, Cuker A. "Clinical and laboratory diagnosis of TTP: an integrated approach". Hematology Am Soc Hematol Educ Program. 2018(1). :530-538. (2018)
- Walls R, Hockberger R, Gausche-Hill M, Erickson TB, Wilcox SR. "Rosen's Emergency Medicine 10th edition- Concepts and Clinical Practice E-Book". Elsevier Health Sciences. (2022). ISBN: 9780323757904
- American Academy of Pediatrics. "Textbook of Pediatric Care". American Academy of Pediatrics. (2016). ISBN: 9781610020473
- "Clinical Guidance for Managing Meningococcal Disease Risk in Patients Receiving Complement Inhibitor Therapy". https://web.archive.org/web/20241226155413/https://www.cdc.gov/meningococcal/hcp/clinical-guidance/complement-inhibitor.html. [2024-11-26]
- Costigan C, Raftery T, Carroll AG, et al. "Neurological involvement in children with hemolytic uremic syndrome". Eur J Pediatr. 181(2). :501-512. (2021)
- Sanders E, Brown CC, Blaszak RT, Crawford B, Prodhan P. "Cardiac Manifestation among Children with Hemolytic Uremic Syndrome". J Pediatr. 235. :144-148.e4. (2021)
- Siegler RL, Pavia AT, Christofferson RD, Milligan MK. "A 20-year population-based study of postdiarrheal hemolytic uremic syndrome in Utah". Pediatrics. 94(1). :35-40. (1994)
- Fitzpatrick MM, Shah V, Trompeter RS, Dillon MJ, Barratt TM. "Long term renal outcome of childhood haemolytic uraemic syndrome". BMJ. 303(6801). :489-492. (1991)
- "Atypical Hemolytic Uremic Syndrome". https://rarediseases.org/rare-diseases/atypical-hemolytic-uremic-syndrome/