Summary
Hemorrhoids are dilated submucosal vascular cushions within the anal canal that can be asymptomatic or manifest as painless perianal masses, pruritus, or intermittent scant hematochezia (bright red blood per rectum, typically at the end of defecation). Excessive straining during defecation or intraabdominal pressure (e.g., due to constipation, pregnancy, or prolonged periods sitting) increase the likelihood of developing hemorrhoids. Based on their anatomical location, hemorrhoids are internal (above the dentate line), external (below the dentate line), or mixed. Internal hemorrhoids are classified into four grades according to the extent of prolapse. The diagnosis is primarily clinical, based on a thorough history and examination that includes a digital rectal examination and anoscopy. Further investigation with proctoscopy, sigmoidoscopy, or colonoscopy may be required to rule out differential diagnoses of hemorrhoids, including colorectal cancer. All patients with symptomatic hemorrhoids should be counseled on lifestyle modifications (e.g., increased fiber and fluid intake, regular physical activity) to reduce straining during defecation. Medical management also includes stool softeners and short-term use of topical medications (e.g., anesthetics, corticosteroids, or vasoconstrictors) for symptomatic relief. Hemorrhoids refractory to medical management and larger (grades III and IV) internal hemorrhoids typically require procedures such as rubber band ligation, sclerotherapy, and infrared coagulation, or surgery. Thrombosed external hemorrhoids manifest with acute pain and a tender bluish-purple perianal nodule. Surgical excision of the thrombosed hemorrhoid may be beneficial in patients who present within 3–4 days of symptom onset. Those who present later should be managed conservatively.
Etiology
- Excessive straining; (e.g., from chronic constipation, frequent bowel movements, chronic cough, heavy lifting, benign prostatic hyperplasia)
- Extended periods of sitting (e.g., due to occupation or sedentary lifestyle)
- Pregnancy
- Older age
- Connective tissue disorder (e.g., Ehlers‑Danlos syndrome, scleroderma)
Pathophysiology
Anatomy of the anal canal
-
Anal cushions
- Areas of thickened anal mucosa that consist of arteriovenous blood vessels (corpus cavernosum recti), smooth muscle (e.g., Treitz muscle), and fibroelastic tissue (e.g., collagen, elastic fibers)
- Located at 11, 7 and 3 o'clock in the lithotomy position (right anterior, right posterior, and left lateral position)
- Play an important role in maintaining continence by enabling tight closure of the rectum
- Defecation causes contraction of supportive structures (e.g., Treitz muscle) → compression of anal cushions → increased diameter of the anal canal for adequate passage of stool
- Anal columns: longitudinal folds of mucous membrane that are fused at their inferior ends by transverse folds (anal valves)
- Anal sinuses: small, mucus-secreting pouches between the anal columns above the anal valves
-
Dentate line
- Circular separation line formed by the fusion of anal valves (hindgut-proctodeum junction)
- Divides anal canal into an upper and lower part (also see characteristics of the anal canal above and below the dentate line below)
-
External anal sphincter
- Composed of
- Subcutaneous external sphincter: surrounds lower third of anal canal
- Superficial external sphincter
- Deep external sphincter
- Consists of skeletal muscle and functions to open and close the anal canal and opening
- Innervated by the pudendal nerve and under voluntary control
- Composed of
-
Internal anal sphincter
- Surrounds upper two-thirds of anal canal
- Consists of involuntary circular smooth muscle and is responsible for ∼ 85% of the resting pressure of the anal canal
- Innervated by the enteric nervous system


| Characteristics of the anal canal above and below the dentate line [3][4] | ||
|---|---|---|
| Above the dentate line | Below the dentate line | |
| Embryological origin |
|
|
| Epithelium |
|
|
| Arterial supply |
|
|
| Venous drainage |
|
|
| Lymphatic drainage |
|
|
| Innervation |
|
|
| Clinical relevance |
|
|



Internal vs. external hemorrhoids
Hemorrhoids are classified as internal , external , or mixed .
-
Internal hemorrhoids
- Prolapse of internal hemorrhoids, with possible incarceration and strangulation, may cause pain by triggering an anal sphincter complex spasm. → possible ischemia and necrosis of internal hemorrhoids → worsening anal sphincter complex spasm → potential external hemorrhoid thrombosis → cutaneous pain
- Develop above the dentate line, which is not innervated by cutaneous nerves; distension does not cause pain.
- Bleeding and/or prolapsed internal hemorrhoids irritate sensitive perianal skin → perianal itching
-
External hemorrhoids
- Develop below the dentate line, which is innervated by cutaneous nerves; distention; of this innervated skin due to thrombosis results in severe pain.
- Acute thrombosis triggers cutaneous pain, lasting 7–14 days → thrombosis resolves → residual skin or skin tags of distended anal skin
Hemorrhoids are not varicose veins (dilated, tortuous veins). Anorectal varices occur, e.g., as a result of portal hypertension. The terms anorectal varices and hemorrhoids are often used interchangeably, but this is incorrect.
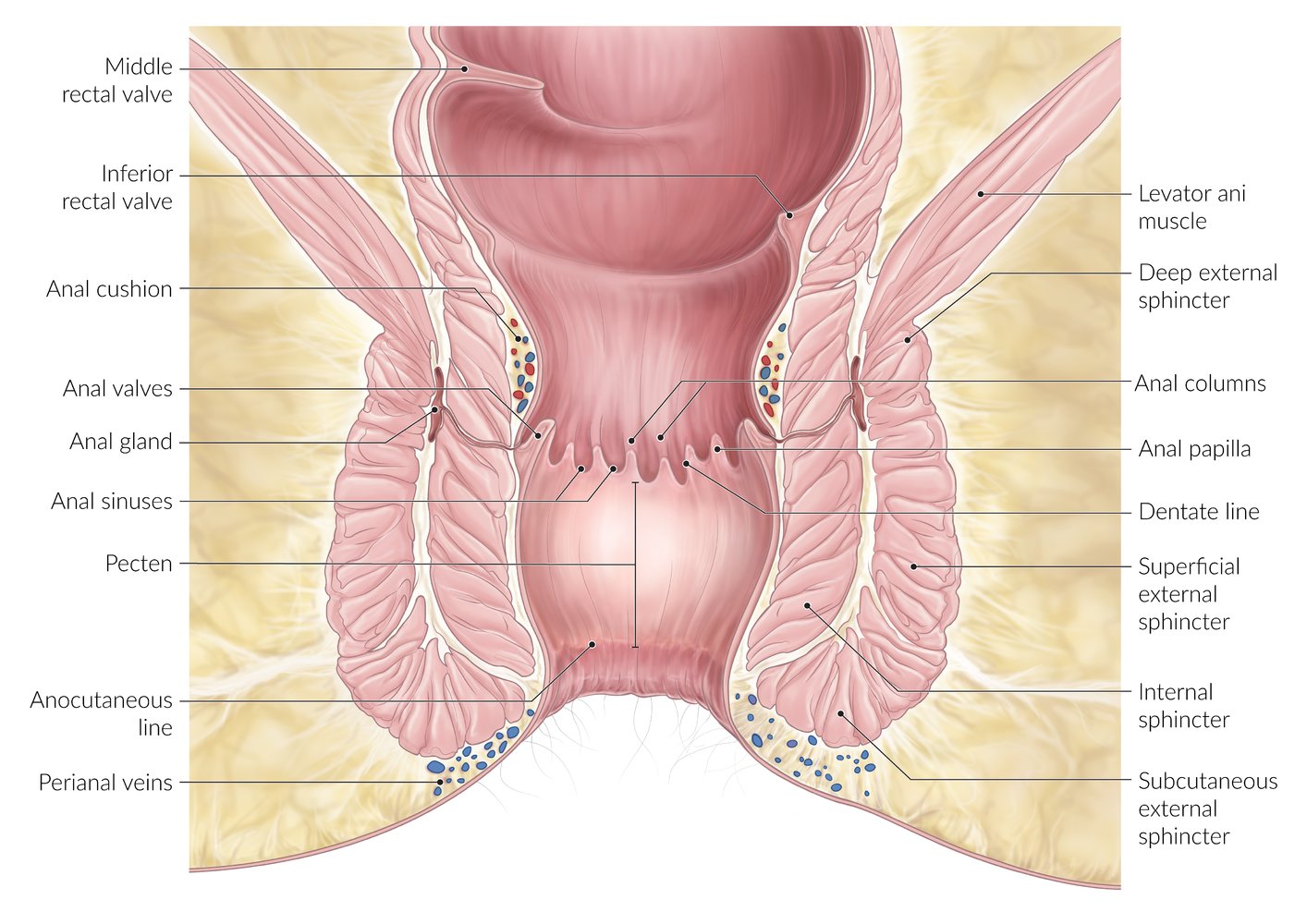
Coronal section of the anal canal
The anal canal extends from the rectum (inferior rectal valve) to the anal orifice.
Anal columns are longitudinal mucosal folds in the upper anal canal.
Anal valves are mucosal folds at the inferior end of the anal columns.
Anal sinuses are transverse mucosal furrows between anal valves.
Anal glands are located between the internal and external anal sphincters and drain into the anal sinuses.
The anal pecten (transitional zone) lies between the dentate line and the anocutaneous line.
Above the pecten, the epithelium is columnar. Below the pecten, it is keratinized squamous epithelium.
A complex sphincter system ensures fecal continence.
© AMBOSS
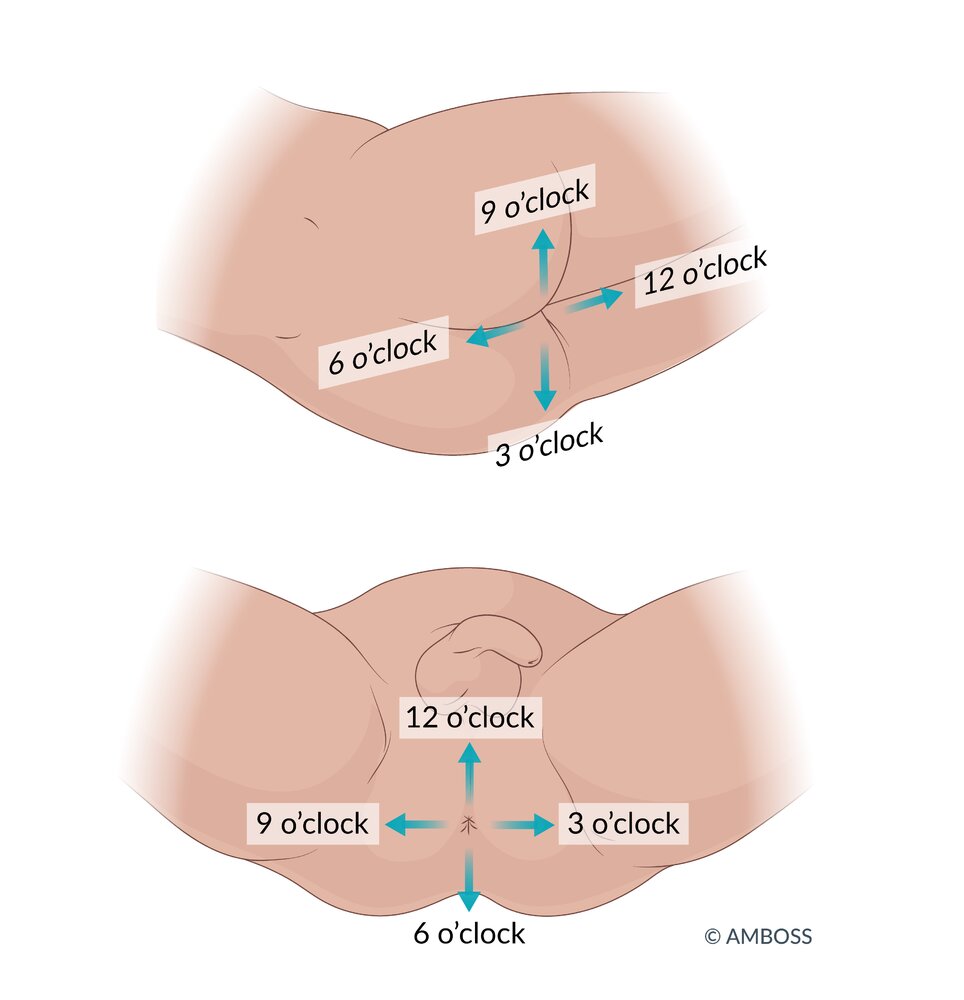
A clock face is commonly used to describe the location of findings during digital rectal examinations in lithotomy and left lateral positions.
– 12 o'clock: perineum
– 6 o'clock: anal rim
However, it is preferable to describe the location of findings relative to the patient (i.e., anterior, posterior, right, left).
© AMBOSS
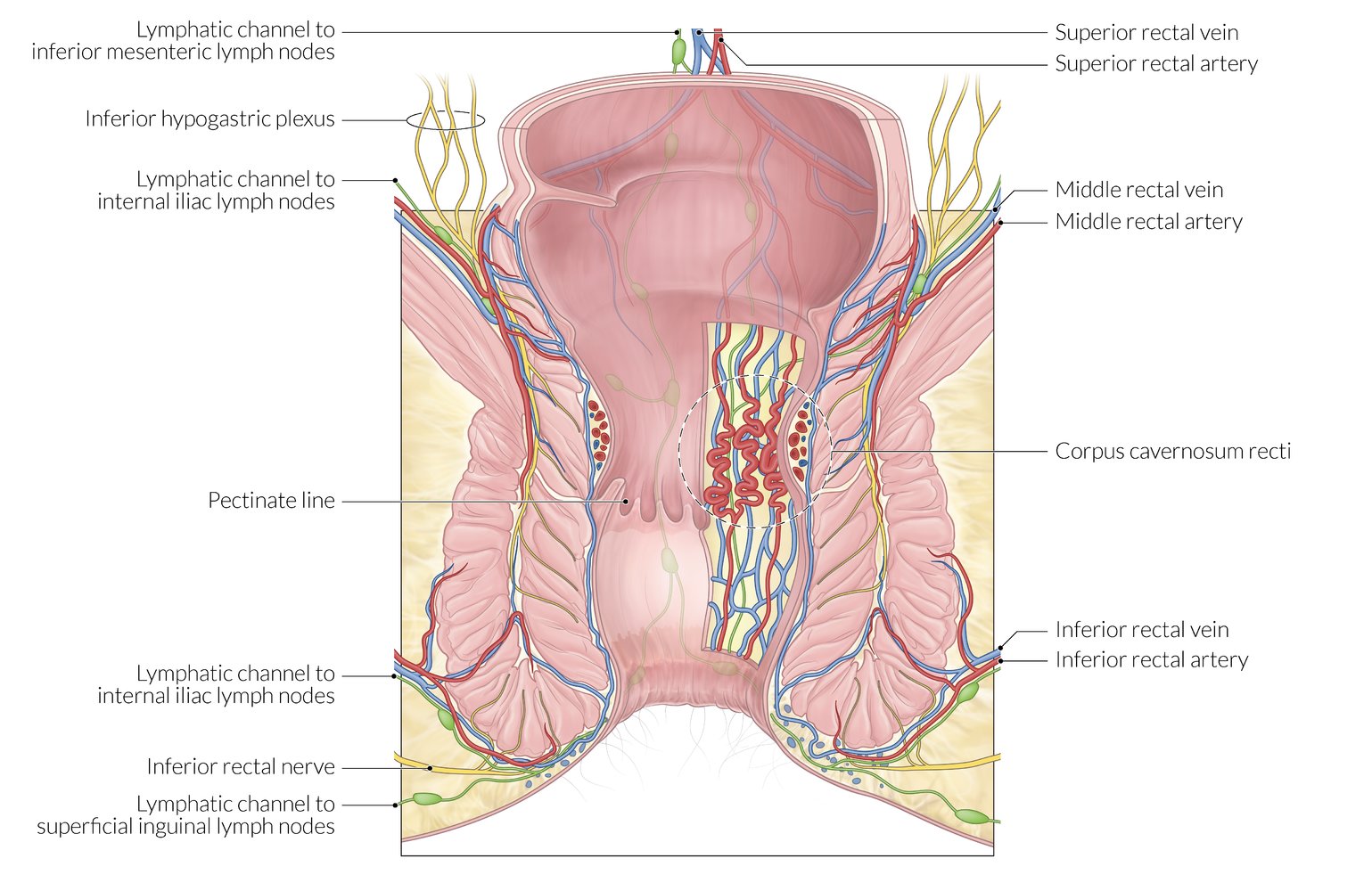
Illustration depicting the dual lymphovascular supply of the anal canal
The anal valves form the pectinate line (seen as a longitudinal scalloped line), which divides the anal canal into upper and lower parts.
Arterial supply
Above the pectinate line:
- Superior rectal artery (a branch of the inferior mesenteric artery)
- Middle rectal artery (a branch of the internal iliac artery)
Below the pectinate line: inferior rectal artery (a branch of the internal pudendal artery)
Venous drainage (site of porto-systemic anastomosis)
Above the pectinate line:
- Superior rectal vein (drains into the inferior mesenteric vein, which drains into the portal vein)
- Middle rectal vein (drains into the internal iliac vein, a systemic vein)
Below the pectinate line: inferior rectal vein (drains into the internal pudendal vein, a systemic vein)
Lymphatic drainage
Above the pectinate line: into the internal iliac and inferior mesenteric lymph nodes
Below the pectinate line: into the superficial inguinal lymph nodes
© AMBOSS
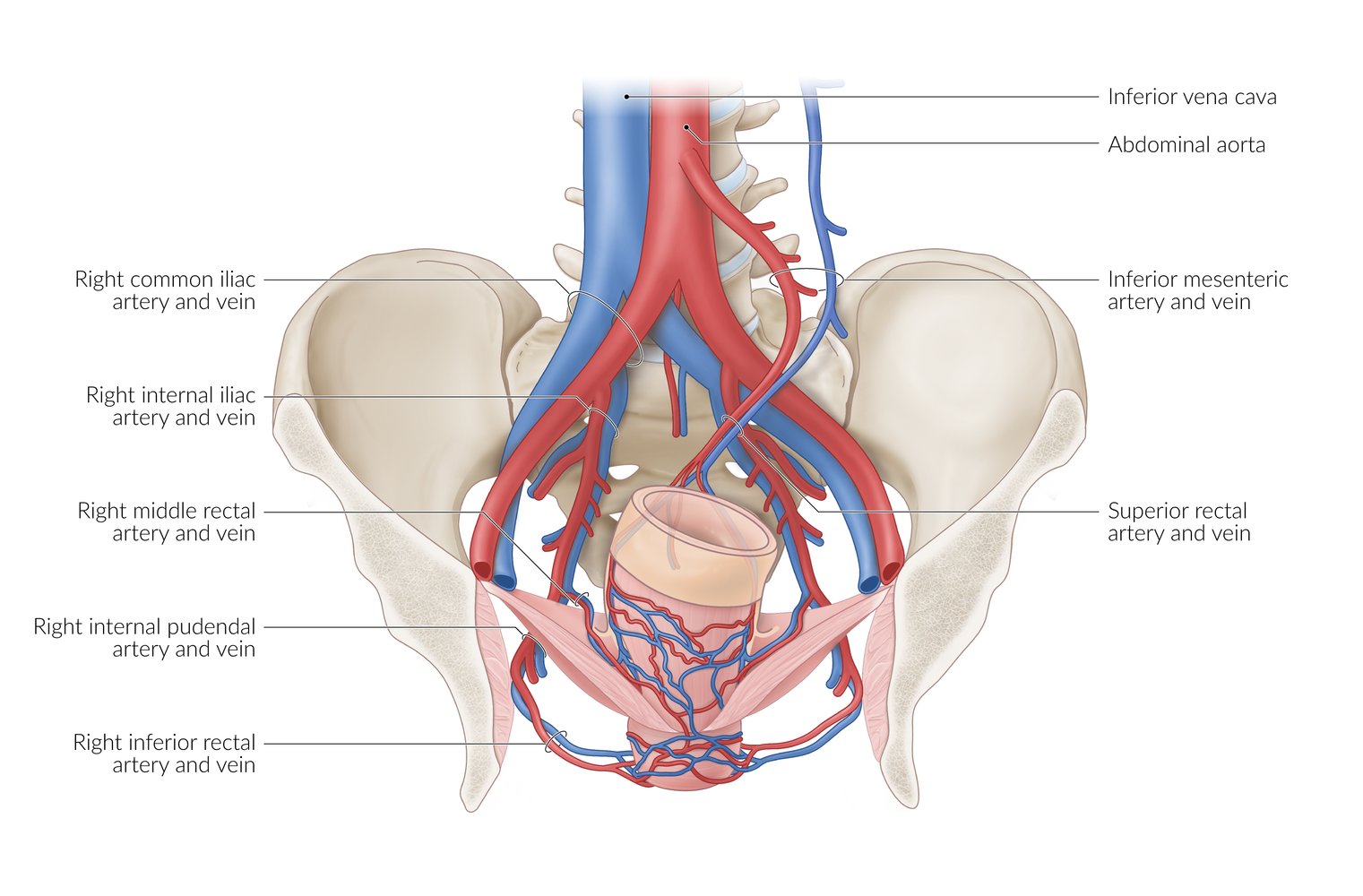
Illustration depicting the dual vascular supply of the anal canal
Arterial supply above the pectinate line:
- Superior rectal artery (a branch of the inferior mesenteric artery)
- Middle rectal artery ( a branch of the internal iliac artery)
Arterial supply below the pectinate line: inferior rectal artery (a branch of the internal pudendal artery)
Venous drainage (site of porto-systemic anastomosis)
Above the pectinate line:
- Superior rectal vein (drains into the inferior mesenteric vein, which drains into the portal vein)
- Middle rectal vein (drains into the internal iliac vein, a systemic vein)
Below the pectinate line: inferior rectal vein (drains into the internal pudendal vein, a systemic vein)
© AMBOSS
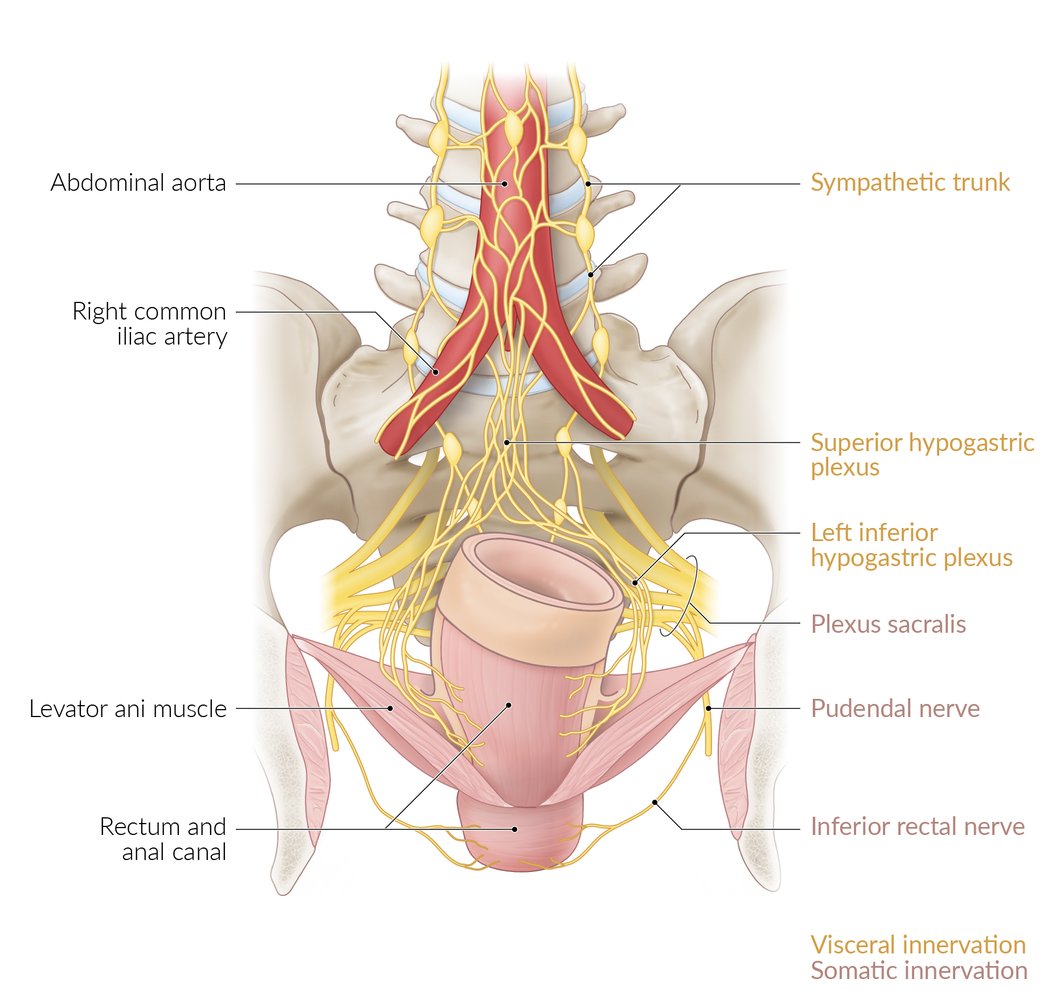
Illustration depicting the dual innervation of the anal canal
Above the pectinate line: autonomic innervation via the inferior hypogastric plexus (insensitive to pain, sensitive to stretch)
Below the pectinate line: somatic innervation via the inferior rectal nerve, a branch of the pudendal nerve that arises from the sacral plexus (sensitive to pain, pressure, touch, and temperature)
© AMBOSS
Clinical features
-
Internal hemorrhoids
- Often painless, bright red bleeding at the end of defecation
- Perianal mass in the event of prolapse
- Pruritus
- Anal discharge (containing mucus or fecal debris)
- Ulceration (in hemorrhoid stage IV)
-
External hemorrhoids
- Manifestations are similar to those of internal hemorrhoids (i.e., bright red bleeding, pruritus, perianal mass)
- A thrombosed external hemorrhoid manifests with severe perianal pain and a tender perianal mass.
Classification
Internal hemorrhoids are graded according to extent of prolapse. There is no widely used classification system for external hemorrhoids.
| Grading of internal hemorrhoids [5] | |
|---|---|
| Grade | Palpation findings |
| I | Hemorrhoids bleed but do not prolapse. |
| II | Prolapse when straining, but spontaneously reduce at rest |
| III | Prolapse when straining; only reducible manually |
| IV | Irreducible prolapse; may be strangulated and thrombosed with possible ulceration |


Perianal region with patient in lithotomy position
Hemorrhoids are visible in the anterior, posterior, and left lateral positions. Grade II hemorrhoids prolapse with straining, e.g., during defecation, but spontaneously reduce at rest.
Source: “Hemrrhoids 04” by Prof. Dr. A. Herold, End- und Dickdarm-Zentrum Mannheim, Wikimedia Commons, licensed under CC BY 3.0.
{kind=link}

Perianal region with patient in lithotomy position
Hemorrhoids are visible at the posterior and right and left lateral positions. Grade III hemorrhoids prolapse with straining, e.g., during defecation, and do not reduce spontaneously, requiring manual reduction. There are multiple anal skin tags, indicating previous episodes of inflamed or thrombosed hemorrhoids.
Source: © IMPP

Perianal region with patient in left lateral position
Multiple prolapsed hemorrhoids that were manually irreducible on examination are visible, indicating grade IV hemorrhoids. Several perianal skin tags can also be seen.
Source: “Grade IV Hemorrhoids” by Απόστολος Σταματιάδης, Wikimedia Commons, licensed under CC BY-SA 2.5.
{kind=link}

Perianal region with patient in lithotomy position
Multiple bleeding, prolapsed hemorrhoids that were manually irreducible on examination are visible, indicating grade IV hemorrhoids.
Source: “Piles 4th deg 01” by Dr. K.-H. Günther, Klinikum Main Spessart, Lohr am Main, Wikimedia Commons, licensed under CC BY 3.0.
{kind=link}
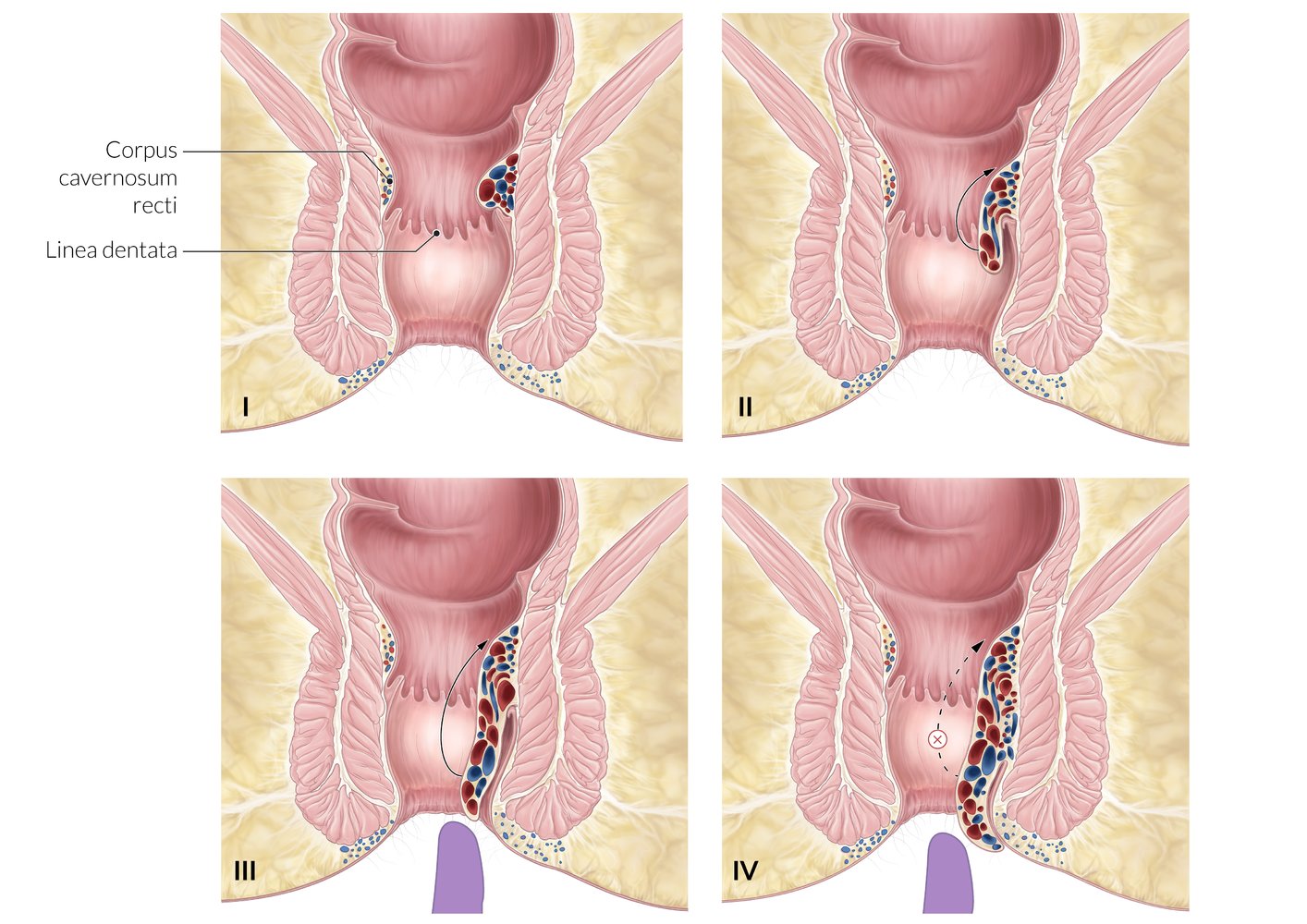
Internal hemorrhoids are located above the dentate line and are classified into the following grades based on the degree of prolapse:
Grade I: Hemorrhoids do not prolapse out of the anal verge.
Grade II: Hemorrhoids prolapse with straining, but reduce spontaneously.
Grade III: Hemorrhoids prolapse with straining and are only reducible manually.
Grade IV: Prolapse is irreducible.
© AMBOSS
Diagnosis
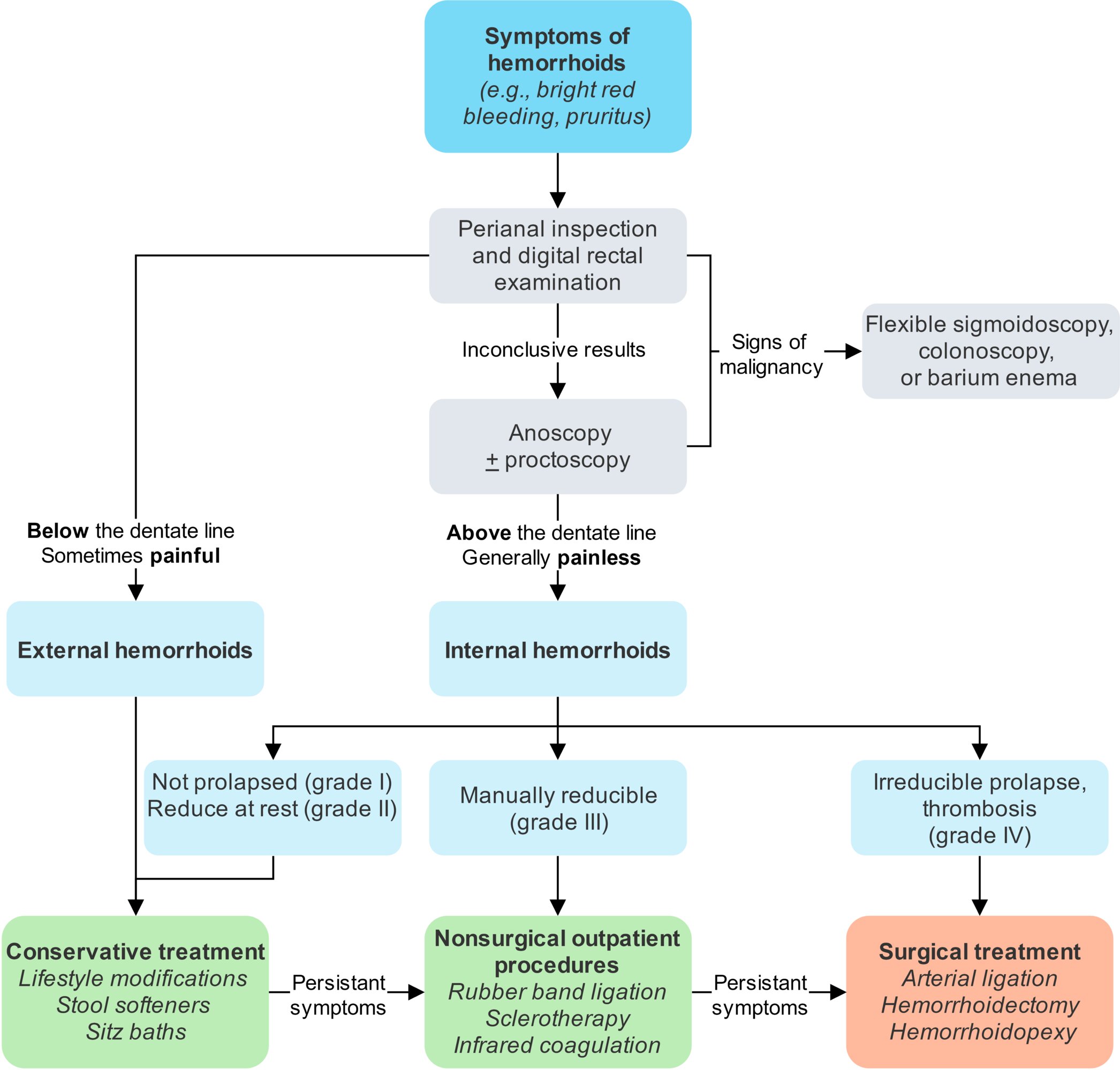
Approach [5][6][7]
- All patients with suspected hemorrhoids: Perform a perianal examination, digital rectal examination, and anoscopy.
- Inconclusive initial evaluation: Refer for proctoscopy or flexible sigmoidoscopy to evaluate the rectum and distal colon.
- Concern for malignancy (age ≥ 50 years; , risk factors for colorectal cancer, red flags for colorectal cancer): Colonoscopy (alternatively, CT colonography) is required to evaluate the entire colon. [6]
Hemorrhoids are a clinical diagnosis.
Physical examination [5][7][8]
- Evaluate in the prone jackknife position, lateral decubitus position, or lithotomy position. [8]
- Inspect the perianal area for external hemorrhoids and nonreduced internal hemorrhoids.
- Perform a digital rectal examination to evaluate for masses or tenderness.
- Ask the patient to perform the Valsalva maneuver in order to assess for any prolapse of grade II or III hemorrhoids or rectal mucosa.
- Rule out other potential sources of bright red blood per rectum or perianal masses (see “Differential diagnoses of hemorrhoids”).
Anoscopy [6][8]
- Insertion of an anoscope to directly visualize the anus and distal rectum [9]
- Perform in all patients with suspected hemorrhoids. [7][8]
- May show hemorrhoids or differential diagnoses, e.g., anal carcinoma or fissure




Further studies [6][8][10]
-
Indications
- Clinical uncertainty
- Inadequate visualization on anoscopy
- Concern for malignancy
-
Modalities
- High risk for malignancy : colonoscopy to visualize the entire colon; see “Initial workup” in “Approach to suspected colorectal cancer” for further information
- Low risk for malignancy : proctoscopy or flexible sigmoidoscopy
© AMBOSS
A clock face is commonly used to describe the location of findings during digital rectal examinations in lithotomy and left lateral positions.
– 12 o'clock: perineum
– 6 o'clock: anal rim
However, it is preferable to describe the location of findings relative to the patient (i.e., anterior, posterior, right, left).
© AMBOSS
Perianal region with patient in lithotomy position
Hemorrhoids are visible in the anterior, posterior, and left lateral positions. Grade II hemorrhoids prolapse with straining, e.g., during defecation, but spontaneously reduce at rest.
Source: “Hemrrhoids 04” by Prof. Dr. A. Herold, End- und Dickdarm-Zentrum Mannheim, Wikimedia Commons, licensed under CC BY 3.0.
Perianal region with patient in lithotomy position
Hemorrhoids are visible at the posterior and right and left lateral positions. Grade III hemorrhoids prolapse with straining, e.g., during defecation, and do not reduce spontaneously, requiring manual reduction. There are multiple anal skin tags, indicating previous episodes of inflamed or thrombosed hemorrhoids.
Source: © IMPP
Perianal region with patient in left lateral position
Multiple prolapsed hemorrhoids that were manually irreducible on examination are visible, indicating grade IV hemorrhoids. Several perianal skin tags can also be seen.
Source: “Grade IV Hemorrhoids” by Απόστολος Σταματιάδης, Wikimedia Commons, licensed under CC BY-SA 2.5.
Perianal region with patient in lithotomy position
Multiple bleeding, prolapsed hemorrhoids that were manually irreducible on examination are visible, indicating grade IV hemorrhoids.
Source: “Piles 4th deg 01” by Dr. K.-H. Günther, Klinikum Main Spessart, Lohr am Main, Wikimedia Commons, licensed under CC BY 3.0.
Differential diagnoses
- Anal skin tags: benign, painless folds of skin at the anal verge that are residues of previous episodes of inflammation or thrombosed hemorrhoids [5]
- Hypertrophied anal papillae
- Polyps
- Anal and colorectal carcinoma
- Anal fissures (cause painful bright red bleeding per rectum)
- Anorectal varices
- Proctitis
- Condyloma acuminata
- Inflammatory bowel disease (often associated with anal fistulas and abscesses)
- Rectal prolapse
- Perianal dermatitis

Always consider the possibility of concurrent colorectal carcinoma.
The differential diagnoses listed here are not exhaustive.

Perianal region with patient in lithotomy position
Multiple benign, painless folds of skin are visible at the anal rim.
Perianal skin tags are residues of previous episodes of inflammation or thrombosed hemorrhoids.
© AMBOSS. This image was adapted from the image “Anal skin tags without hemorrhoids present” by Tmalonetn, Wikimedia Commons, licensed under CC BY 3.0.
{kind=link}
Treatment
Approach [5][6][7]
- All patients with symptomatic hemorrhoids
- Lifestyle modifications to reduce straining during defecation
- Sitz baths and topical medications for short-term symptomatic relief
-
Internal hemorrhoids
- Grade I–III internal hemorrhoids unresponsive to conservative treatment: Refer for office-based procedures (e.g., rubber band ligation).
- Grade IV internal hemorrhoids and those unresponsive to other therapies: Refer for surgery (e.g., hemorrhoidectomy, stapled hemorrhoidopexy).
-
External hemorrhoids
- Symptomatic external hemorrhoids refractory to conservative management: Refer for surgery.
-
Thrombosed external hemorrhoids
- Presentation within 3–4 days of symptom onset: Consider excision of the thrombosed hemorrhoid.
- Delayed presentation: conservative management
Hemorrhoids should only be treated in symptomatic patients. [6]

Medical management of hemorrhoids [5][6][7]
- Indications: all patients with hemorrhoids
-
Interventions to reduce anorectal pressure and straining
-
Lifestyle modifications [5]
- High fiber diet (20–30 g/day)
- Increased fluid intake
- Avoidance of fatty foods
- Regular physical activity
- Avoidance of excessive straining [11]
- Limiting the amount of time spent on the toilet
- Treatment of constipation with short-term (up to 1 week) use of stool softeners (e.g., docusate) or laxatives (e.g., polyethylene glycol 3350) as needed. [5]
-
Lifestyle modifications [5]
-
Interventions to alleviate symptoms (e.g., pain, pruritus)
- Sitz baths: a bath in which the buttocks are immersed in warm water for short periods of time
- Topical medications for short-term symptomatic relief: topical anesthetics (e.g., lidocaine), corticosteroids (e.g., hydrocortisone), and/or vasoconstrictors (e.g., phenylephrine)
Conservative management is often the only intervention required for grade I–II internal hemorrhoids and external hemorrhoids.
Long-term use of topical medications for hemorrhoids can lead to sensitization and localized reactions and should be avoided. [6]
Office-based procedures for hemorrhoids [5][6][8]
- Indications: grade I–III internal hemorrhoids with symptoms refractory to medical management [6]
-
Interventions
-
Rubber band ligation: most common [5][6]
- A rubber band at the base of an internal hemorrhoid under vision through an anoscope
- Ligation leads to ischemic necrosis with subsequent fibrosis.
- Sclerotherapy: low risk of bleeding; consider for patients on anticoagulants [5]
- Infrared coagulation: application of infrared light waves to the base of the hemorrhoid under vision to induce necrosis and scar formation; typically performed for grade I–II internal hemorrhoids [6]
-
Rubber band ligation: most common [5][6]
- Potential complications: uncommon; can include bleeding, pain, or infection (including perianal sepsis) [6]
Sclerotherapy may be preferable in patients with actively bleeding hemorrhoids who are on anticoagulants. [5]
Surgery for hemorrhoids [6][7]
-
Indications [6][10]
- Symptomatic grade III and IV internal hemorrhoids
- Symptomatic external hemorrhoids or combined external and internal hemorrhoids with prolapse
- No improvement after; , or inability to tolerate, medical and office-based interventions
-
Options
-
Submucosal hemorrhoidectomy: surgical removal of hemorrhoids [12][13]
- Ferguson approach (closed approach): The mucosal defect is closed (healing by primary intention) after excision of the hemorrhoid. [6]
- Milligan‑Morgan approach (open approach): The mucosal defect is kept open (healing by secondary intention) after excision of the hemorrhoid.
-
Stapled hemorrhoidopexy (Longo procedure) [6][14]
- A circular stapling device is used to remove a circular wedge of mucosal tissue above the dentate line
- Only effective for internal hemorrhoids
- Doppler-guided hemorrhoidal arterial ligation: identification and ligation of the arteries supplying hemorrhoids
-
Submucosal hemorrhoidectomy: surgical removal of hemorrhoids [12][13]
- Potential complications: pain, bleeding, acute urinary retention, and rarely, anal stricture/stenosis
Pain is common after surgical treatment of hemorrhoids. Consider multimodal analgesia including local anesthesia and use of topical medications (e.g., diltiazem or nitroglycerin ointment) to reduce the need for opioid analgesics. [6]
Perianal sepsis can occur after surgical or office-based interventions for hemorrhoids and may manifest with worsening pain, fever, or dysuria. [6]
: steps")
: instruments and patient positioning")
© AMBOSS
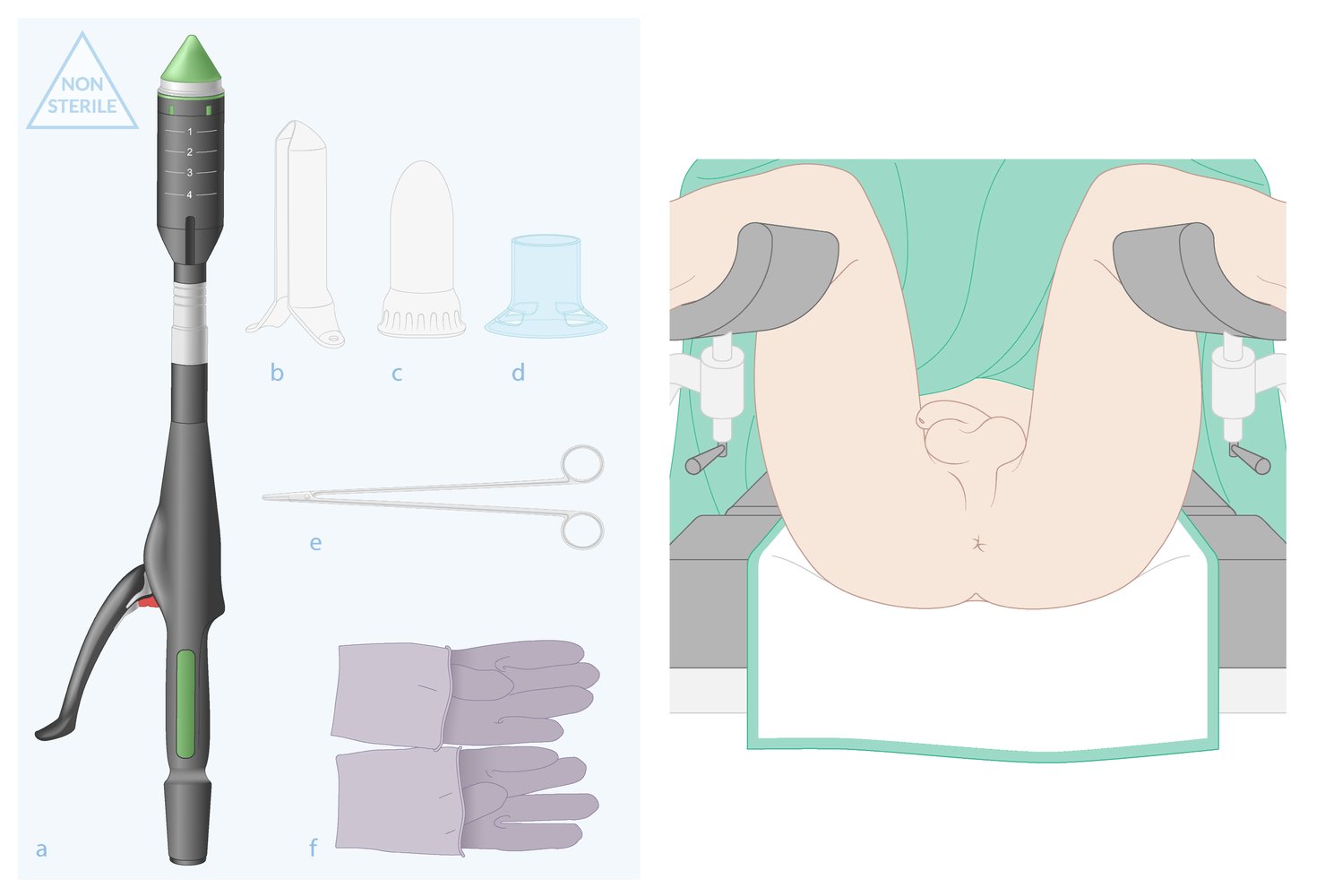
Instruments (left)
(a) Hemorrhoidal circular stapler
(b) Purse-string suture anoscope
(c) Obturator
(d) Circular anal dilator
(e) Needle holder
(f) Sterile gloves
Not depicted: sutures, surgical drapes, gauze
Patient positioning (right): The lithotomy position is usually preferred.
© AMBOSS
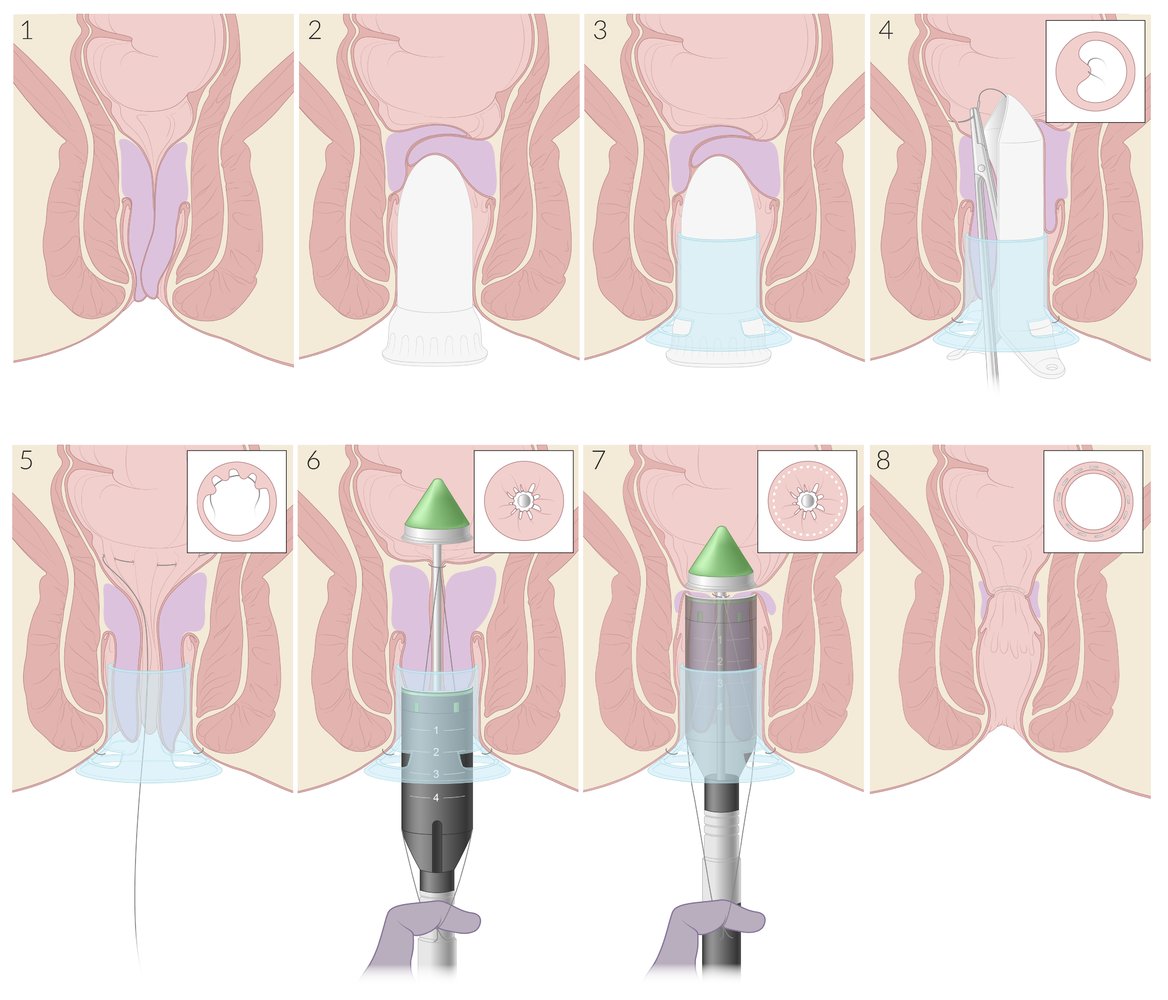
(1) Preoperative finding: grade III internal hemorrhoids
(2) Prior to insertion of the dilator, the obturator may be used to dilate the anal sphincter.
(3) The obturator is placed inside the circular anal dilator and both are inserted into the anal canal. The obturator is then removed and the anal dilator is secured to perianal skin with sutures (not depicted).
(4) The purse-string suture anoscope is inserted through the dilator. It allows for a circumferential submucosal purse-string suture to be placed proximal to the hemorrhoids, above the dentate line (transverse view inset).
(5) Longitudinal (large image) and transverse (inset) views of the partially completed purse-string suture
(6) The maximally opened stapler is inserted into the anal canal until the tip (anvil) is positioned proximal to the purse-string suture. The ends of the suture strings are tied and tightened around the stapler shaft (transverse view inset), pulled through the lateral openings of the stapler, and secured outside the anus. Tension on the suture pulls the prolapsed tissue into the stapler.
(7) The stapler is closed and fired, excising the enclosed tissue (including the purse-string suture) and stapling the cut ends together circumferentially (dotted line on transverse view inset). The stapler and dilator are removed.
(8) Postoperative: Excess hemorrhoidal tissue and prolapsed mucosa proximal to the hemorrhoids have been removed, and the circular staple line (transverse view inset) secures the remaining hemorrhoids in the anatomical position.
© AMBOSS
Thrombosed external hemorrhoid
Definition
A thrombus within the inferior hemorrhoidal venous plexus distal to the dentate line
Pathophysiology
- Stasis of blood within the external hemorrhoid → thrombus formation → inflammation and distention of the overlying perianal skin → severe pain
External hemorrhoids are located distal to the dentate (pectinate) line and are drained by the inferior hemorrhoidal (rectal) plexus. External hemorrhoid thrombosis occurs if a clot forms in the inferior hemorrhoidal plexus. [15]
Clinical features [6][8][16]
- Acute onset of severe perianal pain
- Painful perianal mass that may ulcerate and bleed
- Painful defecation



Diagnostics [6]
- Typically a clinical diagnosis
- Perianal examination: a palpable, tender, dark red to purplish nodule at the anal verge or just within the anal canal
Management [5][6][8]
Surgical excision [12]
- Indication: severe, acute perianal pain (< 3–4 days duration) [8]
- Procedure: : See “Excision of thrombosed external hemorrhoids.”
Medical management [6][8]
-
Indications
- Patients who present after > 3–4 days of symptom onset
- An alternative to surgery in patients with mild or moderate symptoms who present early
-
Methods
- Analgesia: warm sitz baths , antispasmodic agents (e.g., topical nitroglycerin or nifedipine) , analgesic creams (e.g., lidocaine)
- Topical antiinflammatories: e.g., hydrocortisone cream
- Improve passage of stool: stool softeners (e.g., docusate), increased intake of fluids and fiber

Perianal region with patient in lithotomy position
A pink-purple nodule with hemorrhagic blisters on the surface is visible in the right lateral position of the anal verge.
This is the characteristic appearance of a thrombosed hemorrhoid, which is an acutely painful complication of external hemorrhoids.
Source: “Perianalthrombose” by Braegel, Wikimedia Commons, licensed under CC BY 3.0.
{kind=link}

Perianal region with patient in left lateral position
A purplish bulging nodule is visible in the right lateral position of the anal verge, which is the characteristic appearance of a thrombosed external hemorrhoid. Additionally, an anal skin tag is visible in the posterior aspect of the anal verge.
Source: “Figure 1, in: Aetiology of thrombosed external haemorrhoids: a questionnaire study” by O. Gebbensleben, Y. Hilger, H. Rohde, BMC Research Notes, licensed under CC BY-SA 2.0.
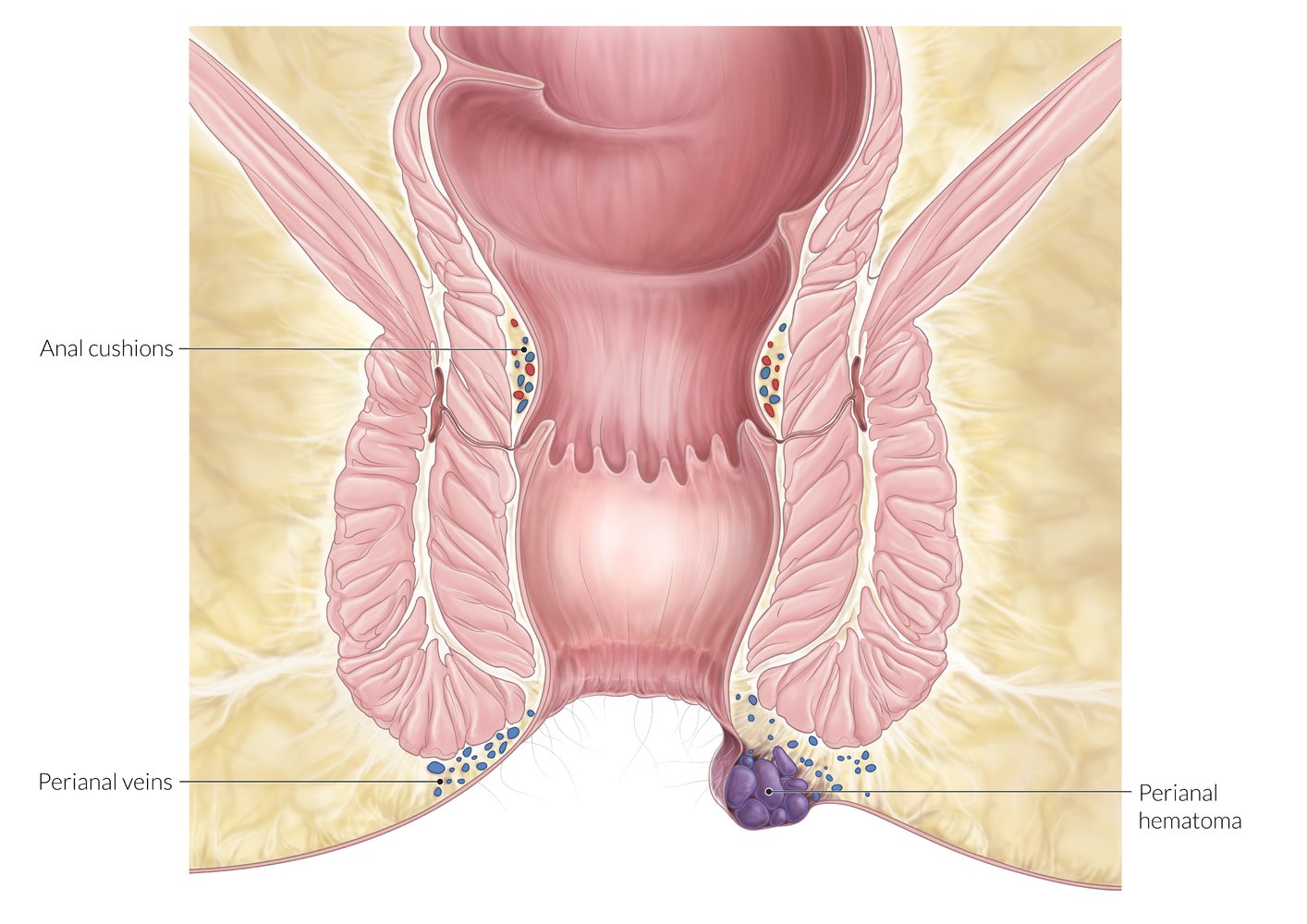
Longitudinal section of the anal canal
Thrombosis of external hemorrhoids results from the stasis of blood within the distended inferior hemorrhoid plexus and manifests as a tender congested (purple or blue) nodule at the anal verge.
© AMBOSS
Excision of thrombosed external hemorrhoids
Surgical excision may be considered for patients presenting with acute (< 3–4 days), severely painful thrombosed external hemorrhoids. [8]
Contraindications (relative) [17][18]
- Coagulopathy
- Serious systemic illnesses
- Hemodynamic instability
- Concurrent anorectal disease
Equipment checklist
- Wide adhesive tape
- Antiseptic solution
- Local anesthetic containing epinephrine (e.g., 1% lidocaine with epinephrine)
- Syringe with 25-gauge needle
- Scalpel (e.g., No. 15 blade, No. 11 blade)
- Small dissecting scissors
- Small grasping forceps
- 4 x 4 gauze squares
Procedure [17]
- Obtain informed consent.
- Position the patient in prone or lateral decubitus position.
- Retract the buttocks to expose the anal opening.
- Prep the skin with an antiseptic solution.
- Administer local anesthetic containing epinephrine.
- Use forceps to grasp the skin overlying the thrombus.
- Make an elliptical incision around the thrombus.
- Excise the skin island using the scalpel or dissecting scissors.
- Remove the entire thrombus.
- Confirm hemostasis.
- Apply a gauze dressing.
Use direct pressure, chemical cautery, electrocautery, or a figure-of-eight suture over the bleeding site to control localized bleeding.


Postprocedure checklist [18][19]
- Medical management of hemorrhoids reinforced to the patient
- Wound care discussed
- Return precautions discussed
- Colorectal surgery follow-up, 6 weeks postprocedure
Complications
- Bleeding
- Infection
- Recurrence [20]
Incision and drainage of a thrombosed external hemorrhoid is more likely to result in local recurrence; excision is the recommended surgical technique. [6][12]
This video demonstrates how to perform single-point local anesthesia infiltration used for localized painful procedures.
This video is part of a new AMBOSS format without voice/sound – optimized for quick clinical reference.
© AMBOSS
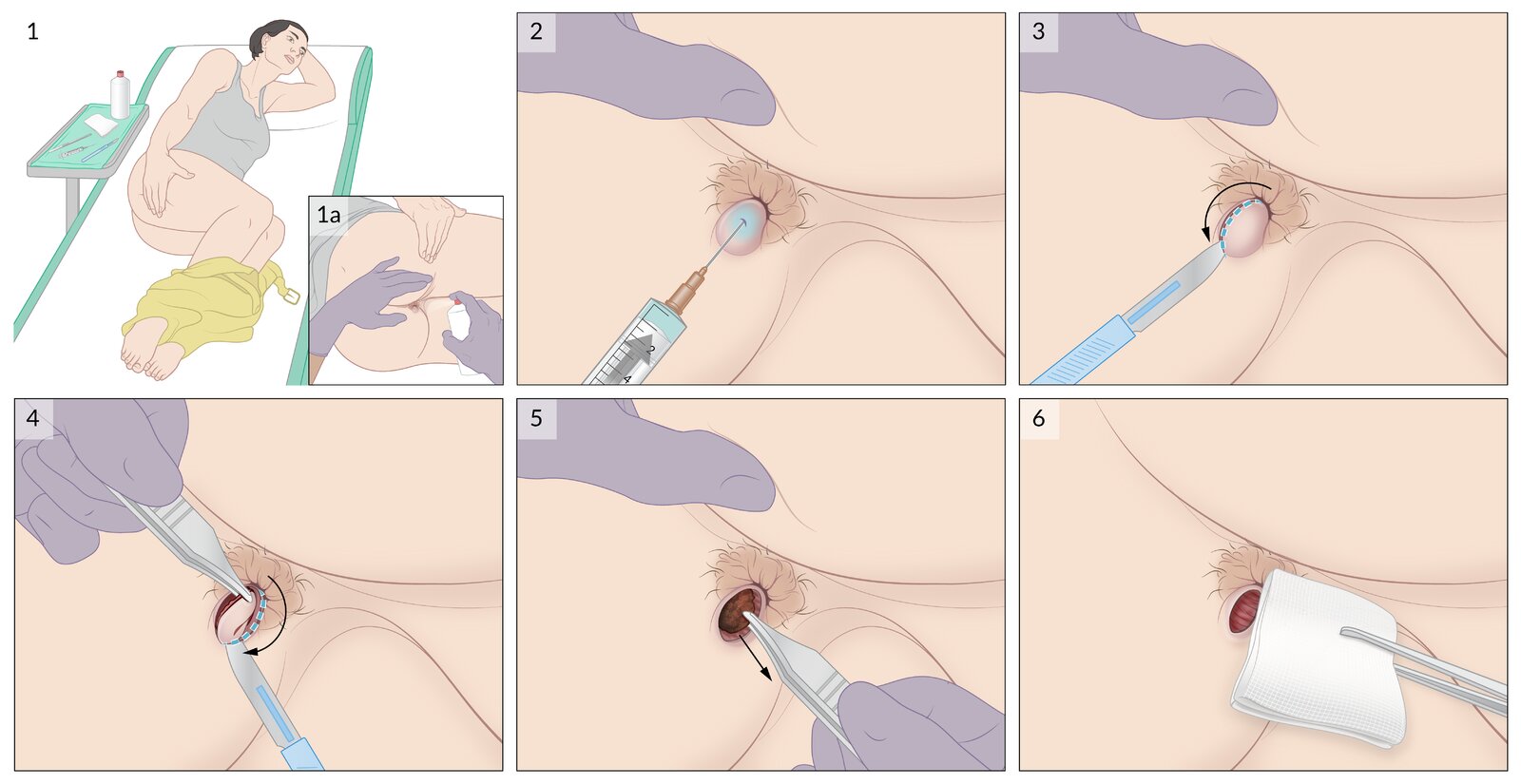
1. The patient is placed in the lateral decubitus position with the buttocks retracted, and the skin is prepped with antiseptic solution (1a).
2. Local anesthetic with epinephrine is injected into the subcutaneous tissue over the center of the hemorrhoid.
3. An elliptical incision is made into the skin over the hemorrhoid, cutting away from the anal opening.
4. A second incision is made away from the anal opening and the free skin is removed.
5. The entire thrombus is removed with forceps.
6. After hemostasis is confirmed, a loose dressing is applied over the wound.
© AMBOSS
Special patient groups
Hemorrhoids in pregnancy [15][21][22]
- Hemorrhoids are common in pregnant individuals.
- Management is typically conservative. [23]
Conservative management
- Provide medical management of hemorrhoids, including treatment of constipation. [23]
- Advise patients to:
- Perform Kegel exercises to improve muscle tone. [24]
- Lie on the left side to improve blood flow. [25]
Interventions
- When possible, defer office-based procedures for hemorrhoids and surgery for hemorrhoids until after the postpartum period. [26]
- Hemorrhoids frequently self-resolve after delivery.
-
Surgery during pregnancy is associated with:
- Induction of labor [15]
- Increased bleeding risk [26]
- Increased risk from sedation/anesthesia [21]
- Consider excision of thrombosed external hemorrhoids for acute thrombosis. [15][26]
External Resources
References
- Standring S. "Gray's Anatomy: The Anatomical Basis of Clinical Practice". Elsevier Health Sciences. (2016). ISBN: 9780702052309
- Garden OJ, Bradbury AW, Forsythe JLR, Parks RW. "Principles and Practice of Surgery". Elsevier Health Sciences. (2012). ISBN: 9780702043161
- Al Khalloufi K, Laiyemo AO. "Management of rectal varices in portal hypertension.". World journal of hepatology. 7(30). :2992-8. (2015)
- Robertson M, Thompson AI, Hayes PC. "The Management of Bleeding from Anorectal Varices". Current Hepatology Reports. 16(4). :406-415. (2017)
- Wald A, Bharucha AE, Limketkai B, et al. "ACG Clinical Guidelines: Management of Benign Anorectal Disorders". Am J Gastroenterol. 116(10). :1987-2008. (2021)
- Davis BR, Lee-Kong SA, Migaly J, Feingold DL, Steele SR. "The American Society of Colon and Rectal Surgeons Clinical Practice Guidelines for the Management of Hemorrhoids". Dis Colon Rectum. 61(3). :284-292. (2018)
- Mott T, Latimer K, Edwards C. "Hemorrhoids: Diagnosis and Treatment Options". Am Fam Physician. 97(3). :172-179. (2018)
- Jacobs D. "Hemorrhoids". N Engl J Med. 371(10). :944-951. (2014)
- Goroll AH, Mulley AG. "Primary Care Medicine". Lippincott Williams & Wilkins. (2009). ISBN: 9780781775137
- Clinical Practice Committee, American Gastroenterological Association. "American Gastroenterological Association medical position statement: Diagnosis and treatment of hemorrhoids". Gastroenterology. 126(5). :1461-1462. (2004)
- Modi RM, Hinton A, Pinkhas D, et al. "Implementation of a Defecation Posture Modification Device: Impact on Bowel Movement Patterns in Healthy Subjects". J Clin Gastroenterol. 53(3). :216-219. (2019)
- Migaly J, Sun Z. "Review of Hemorrhoid Disease: Presentation and Management". Clin Colon Rectal Surg. 29(01). :022-029. (2016)
- Hardy A, Chan CLH, Cohen CRG. "The Surgical Management of Haemorrhoids – A Review". Dig Surg. 22(1-2). :26-33. (2005)
- Lohsiriwat V. "Treatment of hemorrhoids: A coloproctologist’s view". World J Gastroenterol. 21(31). :9245-52. (2015)
- Mounsey AL, Halladay J, Sadiq TS. "Hemorrhoids". Am Fam Physician. 84(2). :204-210. (2011)
- Wald A, Bharucha AE, Cosman BC, Whitehead WE. "ACG clinical guideline: management of benign anorectal disorders". Am J Gastroenterol. 109(8). :1141-57; (Quiz) 1058. (2014)
- Shin GH, Toto EL, Schey R. "Pregnancy and Postpartum Bowel Changes: Constipation and Fecal Incontinence". Am J Gastroenterol. 110(4). :521-529. (2015)
- Tol RR, Kleijnen J, Watson AJM, et al. "European Society of ColoProctology: guideline for haemorrhoidal disease". Colorectal Disease. 22(6). :650-662. (2020)
- Story L, Rafique S, Samadi N, et al. "Lower gastrointestinal bleeding in pregnancy: Differential diagnosis, assessment and management". Obstet Med. 14(3). :129-134. (2021)
- Cengiz TB, Gorgun E. "Hemorrhoids: A range of treatments". Cleve Clin J Med. 86(9). :612-620. (2019)
- Ratcliffe SD. "Family Medicine Obstetrics E-Book". Elsevier Health Sciences. (2008). ISBN: 9780323070829
- Mirhaidari SJ, Porter JA, Slezak FA. "Thrombosed external hemorrhoids in pregnancy: a retrospective review of outcomes". Int J Colorectal Dis. 31(8). :1557-1559. (2016)
- Roberts JR. "Roberts and Hedges' Clinical Procedures in Emergency Medicine and Acute Care". Elsevier. (2018). ISBN: 9780323354783
- Reichman EF. "Emergency Medicine Procedures, Second Edition". McGraw-Hill Education / Medical. (2013). ISBN: 9780071613507
- Zuber TJ. "Hemorrhoidectomy for thrombosed external hemorrhoids". Am Fam Physician. 65(8). :1629-32, 1635-6, 1639. (2002)
- Walls R, Hockberger R, Gausche-Hill M, Erickson TB, Wilcox SR. "Rosen's Emergency Medicine 10th edition- Concepts and Clinical Practice E-Book". Elsevier Health Sciences. (2022). ISBN: 9780323757904