Summary
Hepatitis B is a viral infection caused by the hepatitis B virus (HBV). It occurs worldwide and is transmitted sexually, parenterally, or vertically. After an incubation period of 1–6 months, most patients develop asymptomatic or mild inflammation of the liver, which usually resolves spontaneously within a few weeks or months. However, 5% of adult patients and 90% of infants infected perinatally develop chronic hepatitis B (CHB). Individuals with CHB may be asymptomatic carriers or develop ongoing hepatic inflammation with an increased risk of cirrhosis and hepatocellular carcinoma. Serologic testing initially includes measurement of hepatitis B surface antigen (HBsAg), hepatitis B surface antibody (anti-HBs), and hepatitis B core antibody (anti-HBc). A detectable serum anti‑HBs (indicating seroconversion) is a sign of recovery or successful immunization. CHB with persistent liver inflammation is characterized by detectable HBsAg and elevated HBV DNA and ALT. Treatment of acute hepatitis B consists of supportive measures. In patients with fulminant hepatitis, liver transplantation may be necessary. For chronic active hepatitis B, nucleoside or nucleotide analogs (e.g., tenofovir) are the preferred agents for reducing viral replication and infectivity. Prophylactic immunization with a recombinant vaccine is recommended for all age groups. Other preventive measures include postexposure prophylaxis for infants born to individuals with HBsAg positive or unknown status and for unvaccinated individuals with recent exposure to HBV.
See also “Acute liver failure.”

© AMBOSS
Epidemiology
-
Prevalence: Following the introduction of the hepatitis B vaccine in 1991, rates of acute hepatitis B in the US have declined by approx. 82%. [1]
- In 2016 there were an estimated 862,000 cases (∼ 0.3% of US population) in the US. [2][3]
- In 2015, there were > 257 million cases worldwide (3.5% of the global population). [4]
- The Western Pacific is the most affected region worldwide (6.2% of its population). [4]
Epidemiological data refers to the US, unless otherwise specified.
Etiology
Virus
-
Hepatitis B virus (HBV)
- Member of the Hepadnavirus family
- Circular, partially double-stranded DNA virus
- See “General virology” for more information on viral structure.
Transmission [4]
Frequency and patterns of transmission vary worldwide.
- Sexual: transmitted when bodily fluids come in contact with broken skin or mucous membranes (mouth, genitals, or rectum)
-
Parenteral
- Contaminated needles or instruments (including those for procedures like body piercings, tattoos, and acupuncture) that come into contact with the patient's blood
- Blood transfusions or organ transplants
- Vertical transmission (mother-to-child transmission) [4]
-
Common associations
- Hepatitis C virus (HCV) and HIV-positive individuals
- Travelers to regions where HBV is endemic [5]
Risk factors for HBV infection and groups at risk [6][7][8]
-
Vertical transmission
- Individuals born in countries with medium-to-high HBV prevalence (≥ 2%)
- Unvaccinated children born to parents from countries with high HBV prevalence (≥ 8%)
- Infants born to HBsAg-positive individuals
-
Parenteral or sexual transmission
- Injection drug use (current or previous)
- History of sexually transmitted infections or multiple sexual partners
- Sex workers
- Men who have sex with men
- Household, sexual, or needle-sharing contacts of individuals with HBV infection
- Current or previously incarcerated individuals
- Health care personnel (e.g., needlestick injury)
- HIV infection
- HCV infection (current or past)
- Chronic liver disease
- End-stage renal disease
- Dialysis
Pathophysiology
Replication cycle of HBV [9][10][11]
HBV carries a DNA polymerase with both DNA and RNA-dependent functions, also known as reverse transcriptase (RT).
- After entering the host cell's nucleus, reverse transcriptase completes the positive strand of the virus's partially double-stranded relaxed circular DNA (rcDNA).
- The rcDNA is converted to covalently closed circular DNA (cccDNA) primarily by host enzymes in a process that is not entirely understood.
- The cccDNA is then transcribed into viral mRNA by host RNA polymerase.
- The viral mRNA leaves the nucleus and is translated into HBV core proteins and new reverse transcriptase in the cytoplasm.
- Viral mRNA and reverse transcriptase are packaged into a capsid, where viral mRNA is then reverse-transcribed into viral rcDNA.
- New viral DNA genomes are enveloped and leave the cell as progeny virions.
Acute infection [12]
- In acute infection, the cellular immune response causes damage to hepatocytes.
- Hepatitis B-infected hepatocytes express viral peptides ; on their surfaces → detection of the HBV-derived peptides by lymphocytes and the subsequent activation of CD8+ T cells that attack the infected hepatocytes → hepatic inflammation with destruction of hepatocytes [13]
Chronic infection [14]
Caused by viral persistence due to failing immune clearance, which promotes:
- Persistent hepatic inflammation → necrosis, mitosis, and regeneration processes → cirrhosis and cellular dysplasia → hepatocellular carcinoma (HCC)
- Integration of HBV DNA into the host genome → altered expression of endogenous genes, chromosomal instability → HCC
- HBV proteins fulfill numerous immune-modulating functions that allow them to elude detection by the immune system and avoid clearance. [13]



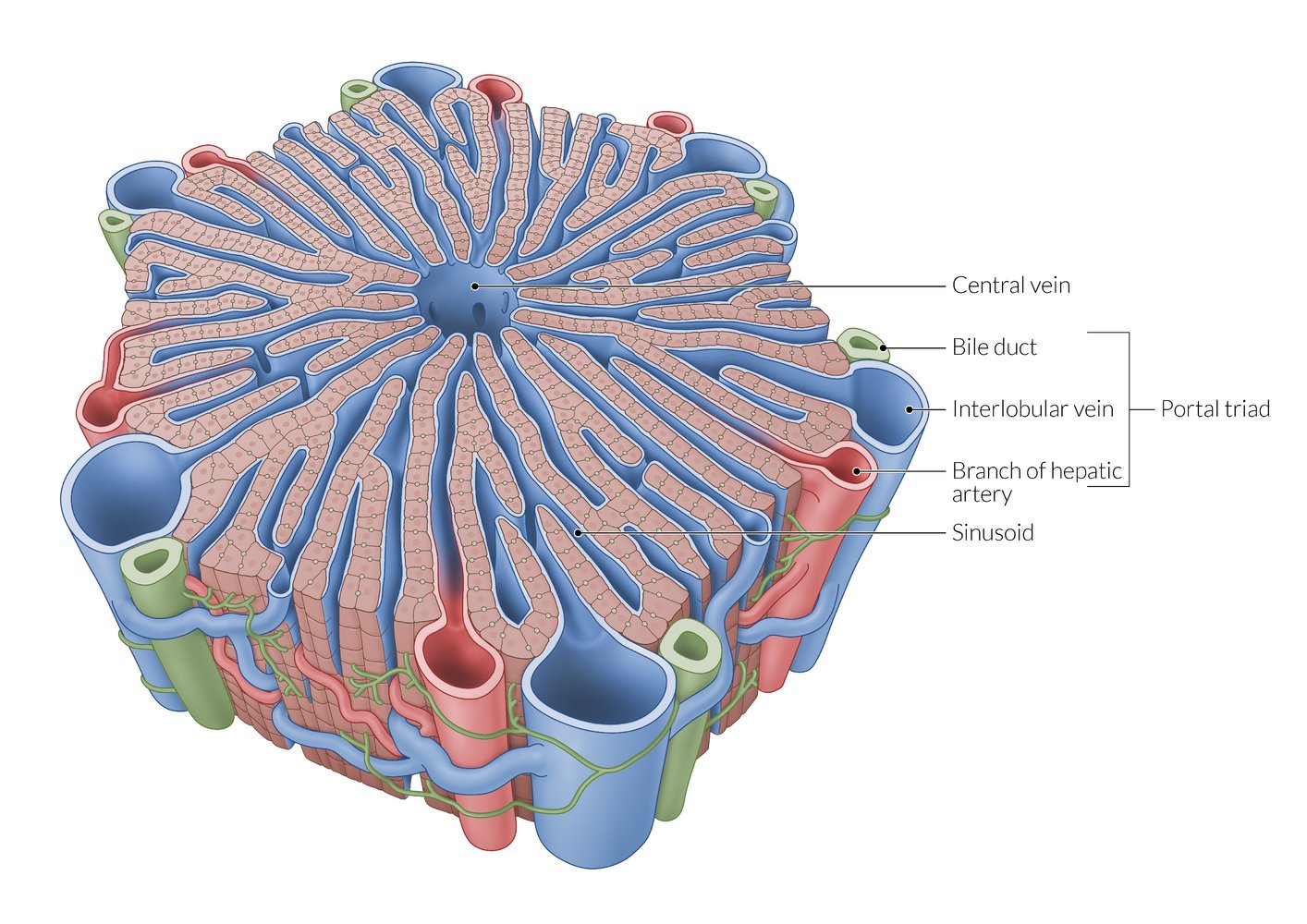
A lobule is a roughly hexagonal structural unit in the liver, separated from adjacent lobules by connective tissue. In each lobule, plates of hepatocytes are separated by hepatic sinusoids. At the vertices, branches of the hepatic artery and portal vein are arranged with bile ducts into portal triads. The flow of blood is from peripheral to central, as blood from the arteries and veins in the portal triads mixes in the sinusoids and drains via a central vein.
Note that sources differ regarding the distribution of portal triads, with some sources depicting them at every vertex of the hepatic lobules (as shown here) and others at only every second vertex.
© AMBOSS
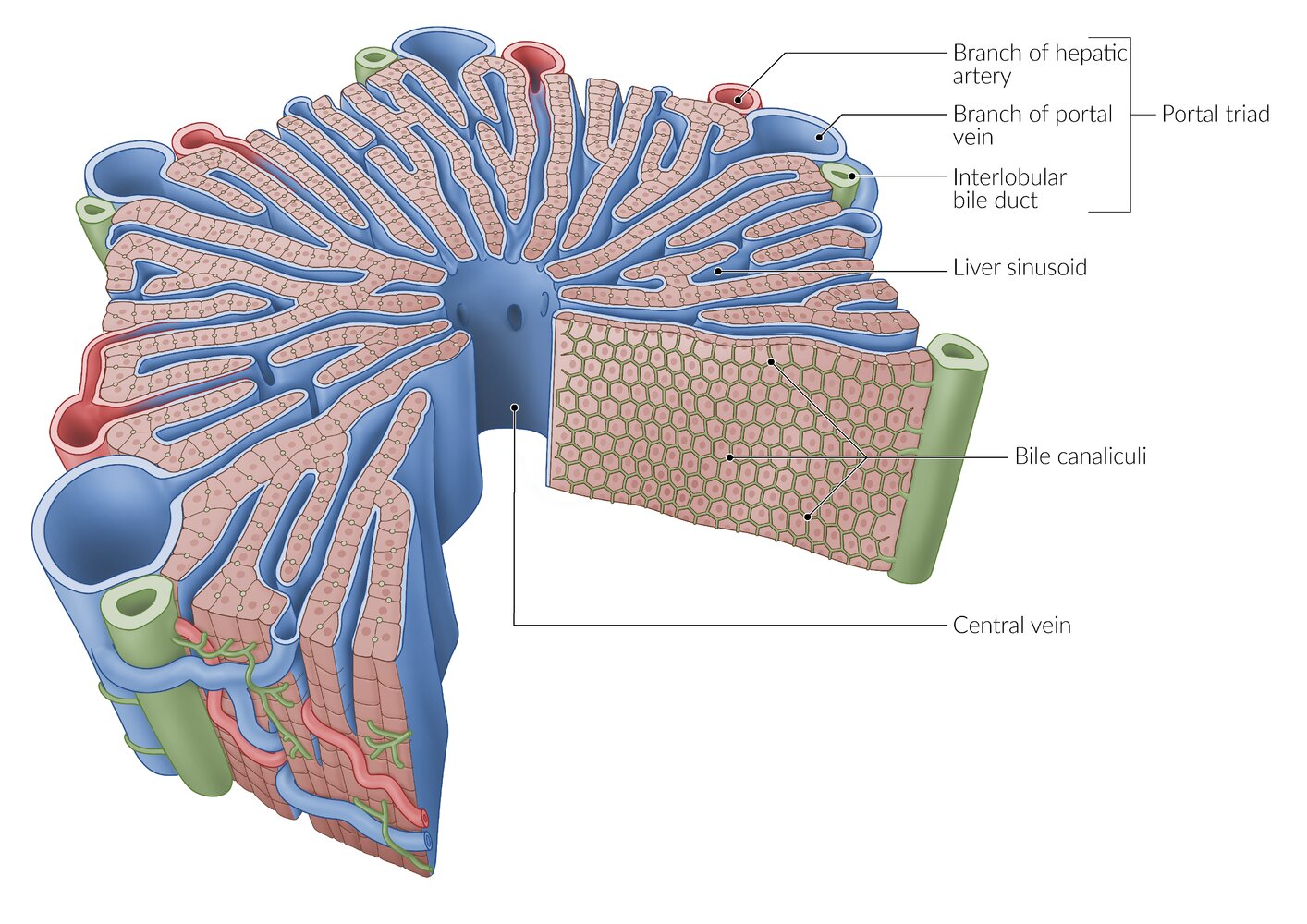
A lobule is a roughly hexagonal structural unit in the liver, separated from adjacent lobules by connective tissue. In each lobule, plates of hepatocytes are separated by hepatic sinusoids. At the vertices, branches of the hepatic artery and portal vein are arranged with bile ducts into portal triads. The flow of blood is from peripheral to central, as blood from the arteries and veins in the portal triads mixes in the sinusoids and drains via a central vein.
Between the hepatocytes is a network of bile canaliculi, which drains bile towards the interlobular bile ducts in the portal triads (the flow of bile is from central to peripheral, and thus opposite to the flow of blood).
© AMBOSS
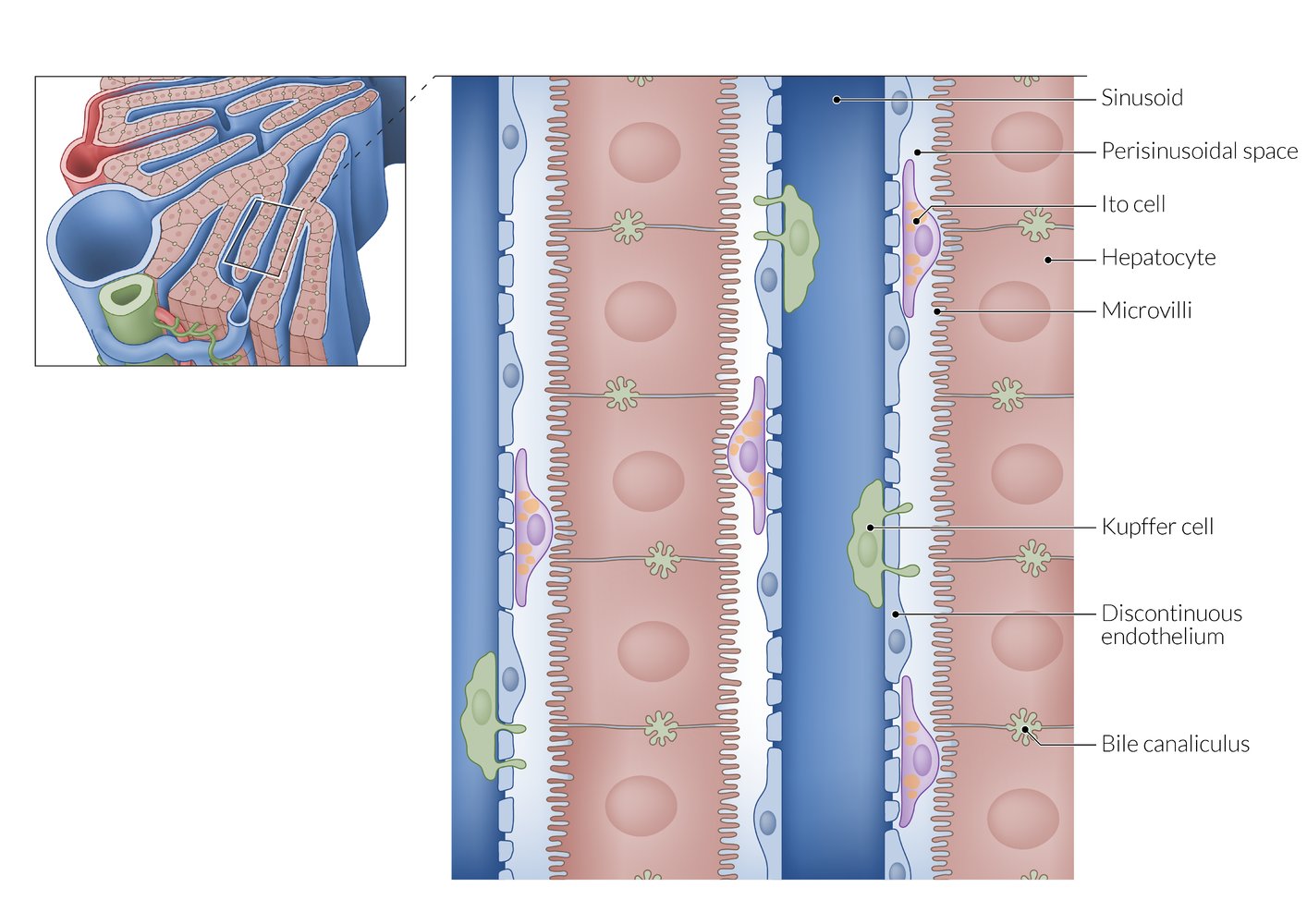
From the sinusoids, plasma can enter the perisinusoidal space through the highly fenestrated endothelium. Microvilli on the basolateral surface of the hepatocytes increase the surface area for efficient substance exchange. The apical surfaces of adjacent hepatocytes form the bile canaliculi, which drain into the peripherally located interlobular bile ducts.
© AMBOSS
Clinical features
Acute hepatitis B virus infection
Acute HBV infection is defined as infection acquired in the past 6 months.
- Incubation period: 1–6 months [4]
-
Clinical course: varies significantly [15][16]
- Serum sickness-like syndrome can develop during the prodromal (preicteric) period 1–2 weeks after infection: rash, arthralgias, myalgias, fever [17]
- Subclinical hepatitis (∼ 70% of cases) [2]
-
Symptomatic hepatitis (∼ 30% of cases; see also acute viral hepatitis)
- Fever, skin rash, arthralgias, myalgias, fatigue
- Nausea, anorexia
- Jaundice
- Right upper quadrant pain
- Symptoms usually resolve after a few weeks, but can last up to 6 months. [2]
- May develop into fulminant hepatitis (∼ 0.5% of cases)
Chronic hepatitis B virus infection [16]
Chronic HBV infection is defined as infection persisting for more than 6 months with detection of HBsAg and, possibly, signs and symptoms of liver damage.
- Most patients are inactive, noncontagious carriers. [18]
- Potential reactivation of chronic inactive hepatitis can manifest variably in the following ways:
- Asymptomatic
- Unspecific symptoms
- Fatigue, malaise
- Nausea, poor appetite
- Unspecific abdominal pain
- Similar to acute hepatitis
- Hepatic failure
-
The younger when infected, the more likely a patient develops chronic HBV [19]
- 90% of infants
- ∼ 50% of children between 1 and 5 years
- Only 5% of adults
Overview of HBV serology
| Overview of HBV antigens and their corresponding antibodies [5][20] | ||
|---|---|---|
| HBV antigen/DNA | Description | Corresponding antibodies |
| Hepatitis B surface antigen (HBsAg) |
|
|
| Hepatitis B core antigen (HBcAg) |
|
|
| Hepatitis B e antigen (HBeAg) [21] |
|
|



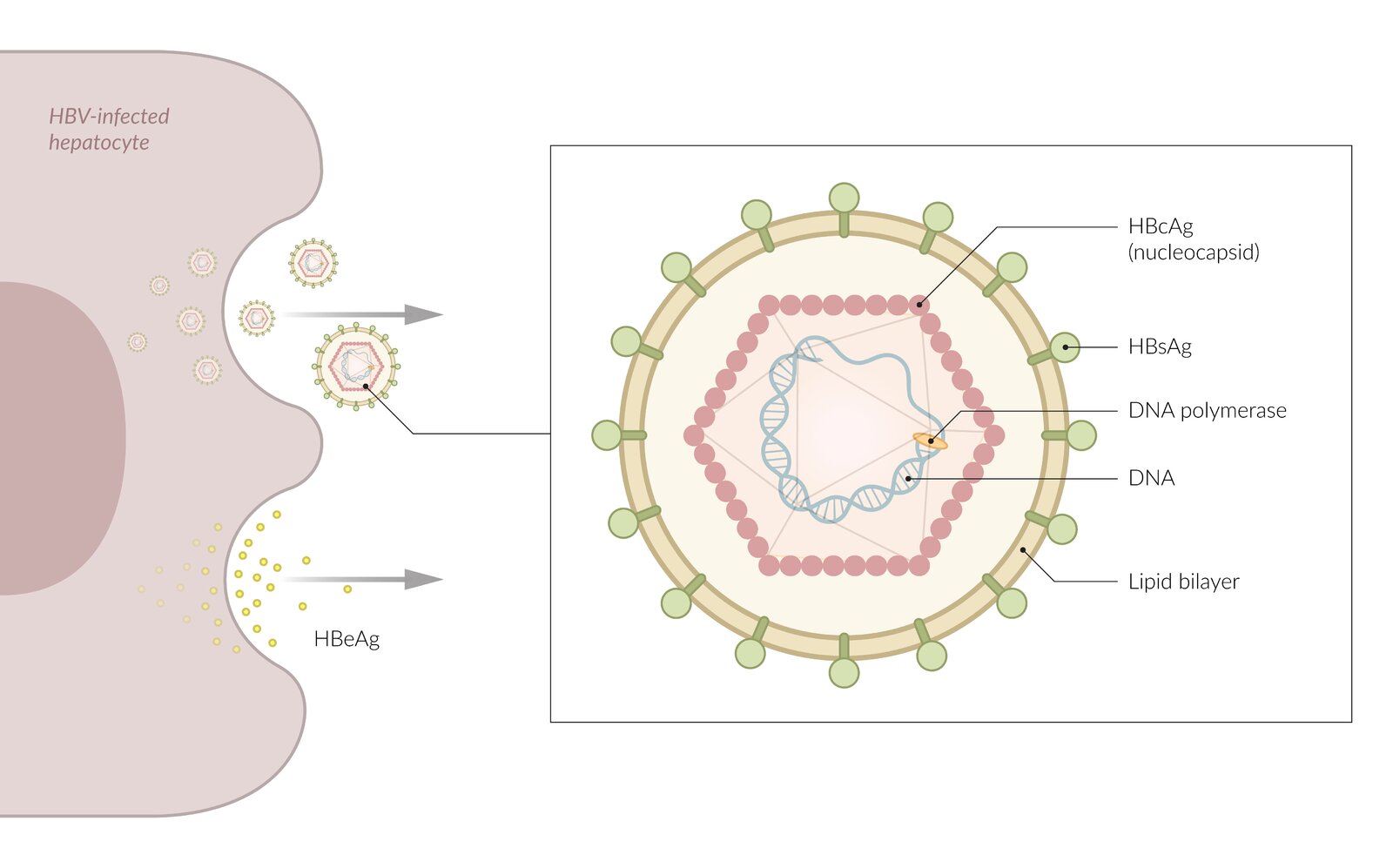
The hepatitis B surface antigen (HBsAg) is found on the outer wall of the virions lipid bilayer and confirms the presence of the virus in the blood. HBsAg is the first indicator of infection and can be detected as early as 1 week after infection. An infected hepatocyte may also release the hepatitis B envelope antigen (HBeAg), a protein produced by the virus that serves as an indicator of active viral replication.
© AMBOSS
© AMBOSS
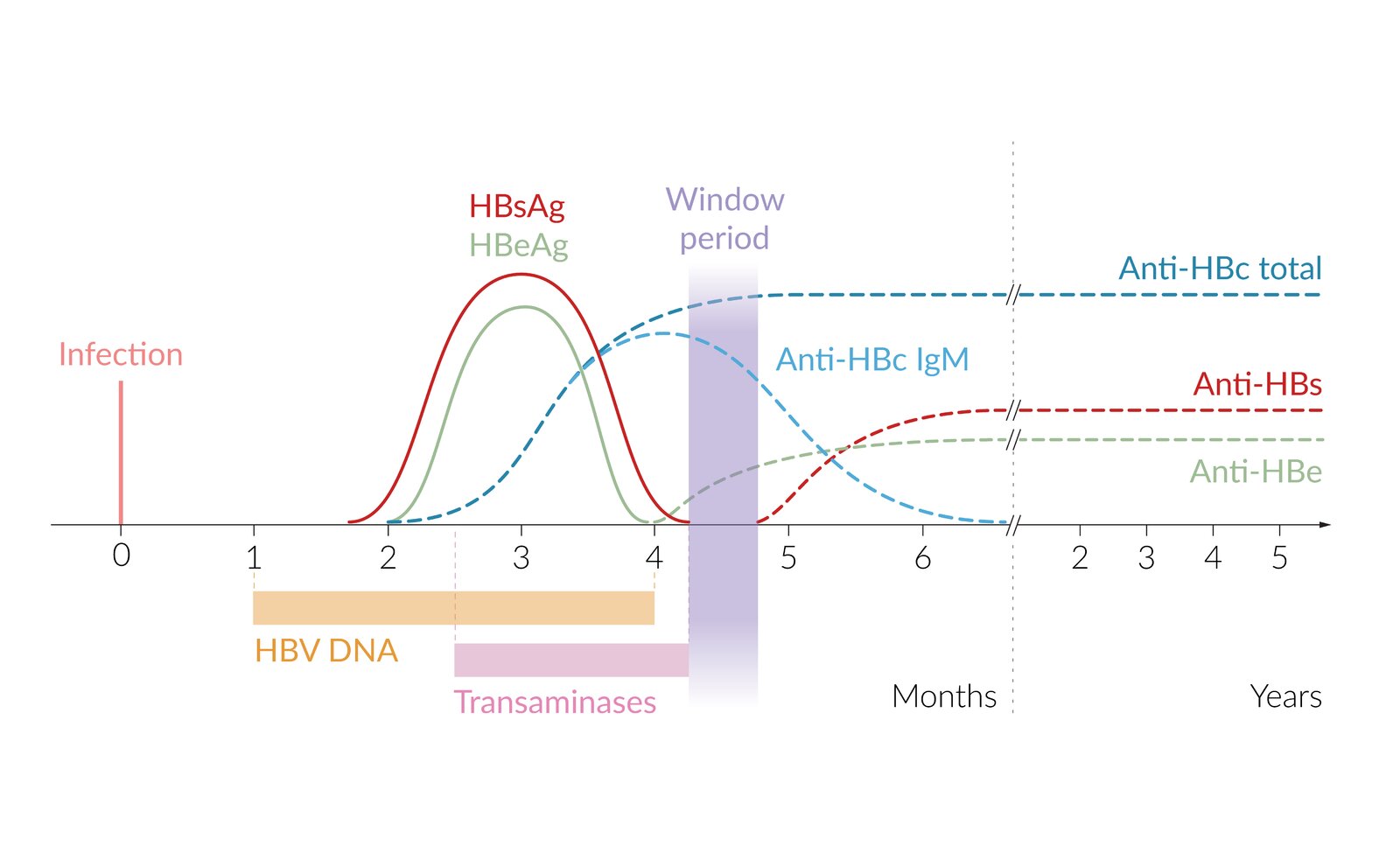
Schematic depiction of the time frames in which HBV DNA, antigens, and antibodies are measurable (and transaminases elevated) during acute HBV infection and resolution. Note that the timing can vary significantly between patients and that the pattern in chronic infection differs.
The window period is an interval in which HBsAg is no longer measurable, anti-HBs is not yet measurable, and only Anti-HBc and Anti-HBe can be detected.
HBV DNA: hepatitis B virus DNA; HBsAg: hepatitis B surface antigen; HBeAg: hepatitis B e antigen; Anti-HBc IgM: anti-hepatitis B core antigen IgM antibody; Anti-HBc total: anti-HBc IgM + anti-HBc IgG (conventionally measured together); Anti-HBs: anti-hepatitis B surface antigen antibody; Anti-HBe: anti-hepatitis Be antigen antibody
© AMBOSS
Screening
Indications for HBV screening [7][22][23]
Obtain initial HBV serology for the following individuals (see “Diagnostics” for interpretation of results):
- All individuals aged ≥ 18 years: at least once per lifetime
- Pregnant individuals: once per pregnancy, preferably in the first trimester (see “Perinatal hepatitis B”) [24]
- Individuals with risk factors for HBV infection [7][25]
- Patients with elevated transaminases of unknown etiology
- Blood and tissue donors [23]
- Individuals who require immunosuppression [23]
- Any individual who requests screening
Diagnosis
Approach [8][23][26]
Suspected acute HBV infection
- Obtain HBV serology to confirm the diagnosis.
- Consider routine laboratory studies to assess liver damage and function.
Chronic HBV infection
- Perform a clinical evaluation to assess for:
- Risk factors for comorbid liver disease, e.g., high-risk alcohol use, metabolic syndrome
- Family history of HCC
- Symptoms of cirrhosis
- Assess for liver fibrosis using, e.g.: [27]
- Liver elastography
- Noninvasive liver fibrosis scoring systems, e.g., APRI score or fibrosis-4 score
- Screen for other infections, including HCV, HDV, and HIV.
- Consider abdominal ultrasound and/or liver biopsy in certain patients.
Patients with chronic hepatitis B infection require further evaluation to identify and manage risk factors for liver-related morbidity and to identify patients eligible for antiviral therapy.
HBV serology [7][23][26]
-
Indications
- Screening for HBV infection
- Patients with symptoms of acute HBV infection or chronic HBV infection
-
Initial tests ; [7][8][23]
- HBsAg
- Anti-HBc
- Anti-HBs
-
Interpretation
- HBsAg or anti-HBc IgM is detected: positive for HBV
- Chronic HBV infection is confirmed if positive results persist for ≥ 6 months.
-
Further disease markers: indicated to assess disease activity if initial tests are positive
- HBeAg: marker of high HBV replication and transmissibility
- Anti-HBe: An undetectable HBeAg with development of anti-HBe indicates immune clearance or an inactive carrier state.
- HBV DNA: quantification of viral load
Interpretation of hepatitis B serology
| Interpretation of hepatitis B serology [20][23][28] | ||||||||
|---|---|---|---|---|---|---|---|---|
| HBsAg | Anti-HBs | Anti-HBc | HBeAg | Anti-HBe | HBV DNA | Transaminases | ||
| Acute infection | ↑ | Undetectable | ↑ IgM | ↑ | Undetectable | Undetectable or ↑ | ↑ (ALT > AST) | |
| Window period | Undetectable | Undetectable | ↑ IgM → ↑ IgG | Undetectable | Undetectable or ↑ | Undetectable or ↑ | ↑ (ALT > AST) | |
| Chronic infection | Active (high transmissibility) | ↑ | Undetectable | ↑ IgG | ↑ | Undetectable | HBV DNA > 2000 IU/mL | Normal or ↑ |
| Inactive (low transmissibility) | ↑ | Undetectable | ↑ IgG | Undetectable | ↑ | HBV DNA ≤ 2000 IU/mL | Normal | |
| Immunity | Resolved infection | Undetectable | ↑ | ↑ IgG | Undetectable | ↑ | Undetectable | Undetectable |
| HBV vaccination | Undetectable | Undetectable | ||||||
HBeAg: BEware! Extremely infEctious.
During the window period, anti-HBc IgM and anti-HBe may be the only markers available to diagnose an acute HBV infection.
Seroconversion of HBsAg to anti‑HBs indicates resolution of acute hepatitis.
Additional laboratory studies [26][27]
-
Liver chemistries: elevated in acute infection, normal or elevated in chronic infection
- Mixed hyperbilirubinemia
- Ferritin
- ALP
- GGT
-
ALT and AST
- AST:ALT ratio < 1 in acute infection
- AST:ALT ratio > 1 in chronic hepatitis may be a sign of cirrhosis.
-
Laboratory diagnostics for cirrhosis
- ↓ Albumin, ↑ INR
- ↑ Bilirubin
- ↓ Platelets
-
Evaluation of coinfection
- Hepatitis C serology (anti-HCV antibodies)
- Hepatitis D (anti-HDV antibodies)
- HIV testing
- Hepatitis A serology (anti-HAV IgG antibodies)
Laboratory findings in chronic HBV infection are highly variable; liver function tests may be normal or only mildly abnormal.
Abdominal ultrasound [26][27][29]
- Indication: to evaluate liver parenchyma and biliary tract and screen for fibrosis and/or HCC
-
Findings in acute hepatitis
- ↓ Liver echogenicity
- ↑ Echogenicity of portal vein radicle walls
-
Findings in chronic hepatitis
- ↑ Liver echogenicity
- ↓ Echogenicity, and number, of portal vein radicle walls
Liver biopsy [27]
-
Indications
- Diagnostic uncertainty when results will be used to guide treatment decisions
- Exclusion of other possible causes of liver damage in chronic disease or severely affected individuals
- Assessment of the severity of liver disease
- Findings: See “Pathology of viral hepatitis.”
Schematic depiction of the time frames in which HBV DNA, antigens, and antibodies are measurable (and transaminases elevated) during acute HBV infection and resolution. Note that the timing can vary significantly between patients and that the pattern in chronic infection differs.
The window period is an interval in which HBsAg is no longer measurable, anti-HBs is not yet measurable, and only Anti-HBc and Anti-HBe can be detected.
HBV DNA: hepatitis B virus DNA; HBsAg: hepatitis B surface antigen; HBeAg: hepatitis B e antigen; Anti-HBc IgM: anti-hepatitis B core antigen IgM antibody; Anti-HBc total: anti-HBc IgM + anti-HBc IgG (conventionally measured together); Anti-HBs: anti-hepatitis B surface antigen antibody; Anti-HBe: anti-hepatitis Be antigen antibody
© AMBOSS
Pathology
Active viral hepatitis [30][31]
- Eosinophilic single-cell necrosis (Councilman bodies)
- Bridging necrosis
- Kupffer cell proliferation

Chronic viral hepatitis [30][31]
- Formation of lymphoid follicles and mononuclear infiltrates
-
Interface hepatitis (piecemeal necrosis)
- Periportal liver cell necrosis with lymphocytic infiltration
- The cause of interface hepatitis is a CD8 T-cell‑induced hepatocyte apoptosis.
- Indicates chronic active hepatitis and poor prognosis
- Fibrous septa [32]
-
Ground glass hepatocytes ; [33]
- Hepatocytes with swollen transparent cytoplasm due to hyperplasia of the endoplasmic reticulum resulting in a ground glass appearance
- Pathognomonic for hepatitis B
- Result from increased production of viral membrane particles (HBsAg)
Ground glass hepatocytes are pathognomonic for HBV, whereas interface hepatitis, fibrous septa, and periportal infiltrates also occur in other types of chronic hepatitis.




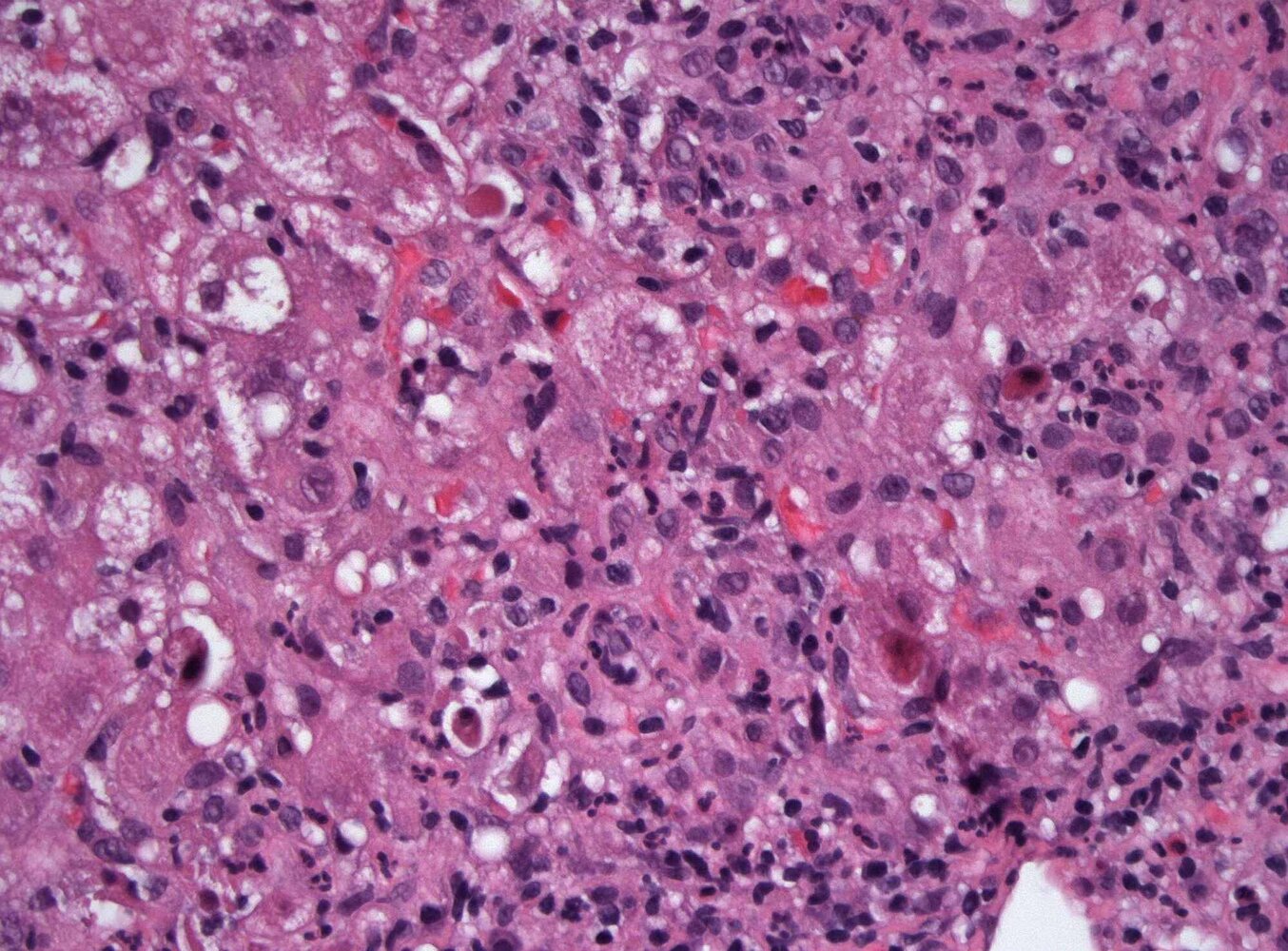
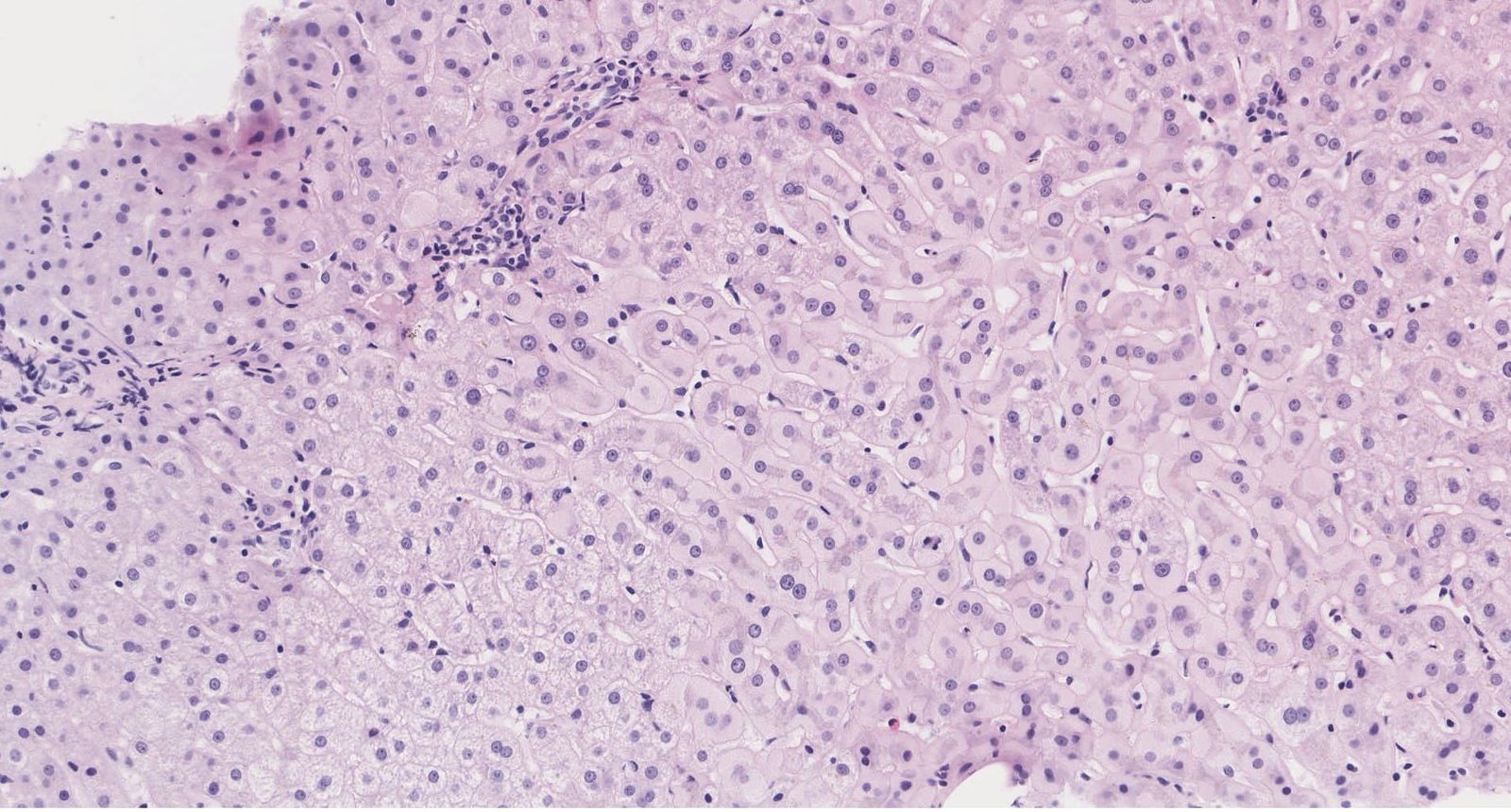
Photomicrograph of a hepatic tissue sample (H&E stain; 400x magnification)
There is heavy necroinflammatory activity in this hepatic lobule. The hepatocytes show reactive changes, including prominent swelling (exemplary green outline). Several apoptotic hepatocytes (also known as “acidophilic bodies” or “Councilman bodies;” examples indicated by yellow outlines) are visible.
These findings are typical of inflammatory changes consistent with an acute viral hepatitis (in this case hepatitis B exacerbated by hepatitis E coinfection).
Source: “Fig 1, In: Hepatitis E Virus Superinfection: an Underrecognized Trigger of Acute Hepatitis B Virus Flare” by Obeidat AE, Monti G, Sae-Ow W, Shinoda H, Lim H, Cureus, licensed under CC BY 4.0. Modifications: removal of the white arrow in the center of the image. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
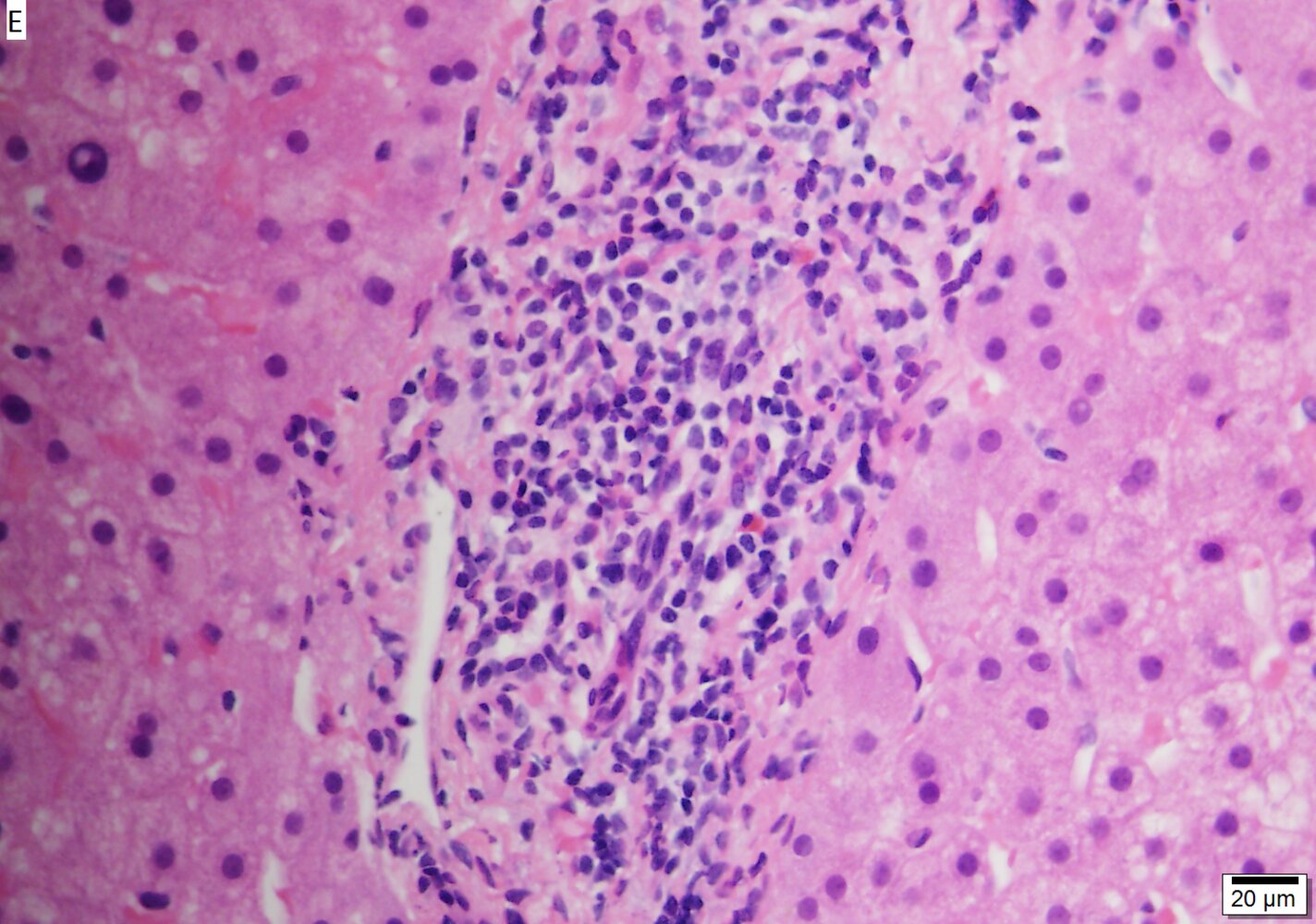
Photomicrograph of a liver biopsy specimen (H&E stain; high magnification)
A chronic inflammatory infiltrate (blue overlay) consisting of lymphocytes, plasma cells, and eosinophilic granulocytes can be seen in the center of the image. The infiltrate is located at the interface of the portal tract and hepatic lobules (yellow overlay), which is referred to as “interface hepatitis.”
These features are typical of chronic hepatitis, in this case, hepatitis B. Chronic inflammation of any tissue typically shows mononuclear cell infiltration (e.g., lymphocytes, plasma cells, macrophages) and fibrosis may be present simultaneously as well (not present here).
Source: “File:6 17281676469188 sl 5” by TexasPathologistMSW, Wikimedia Commons, licensed under CC BY-SA 4.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 4.0.
{kind=link}
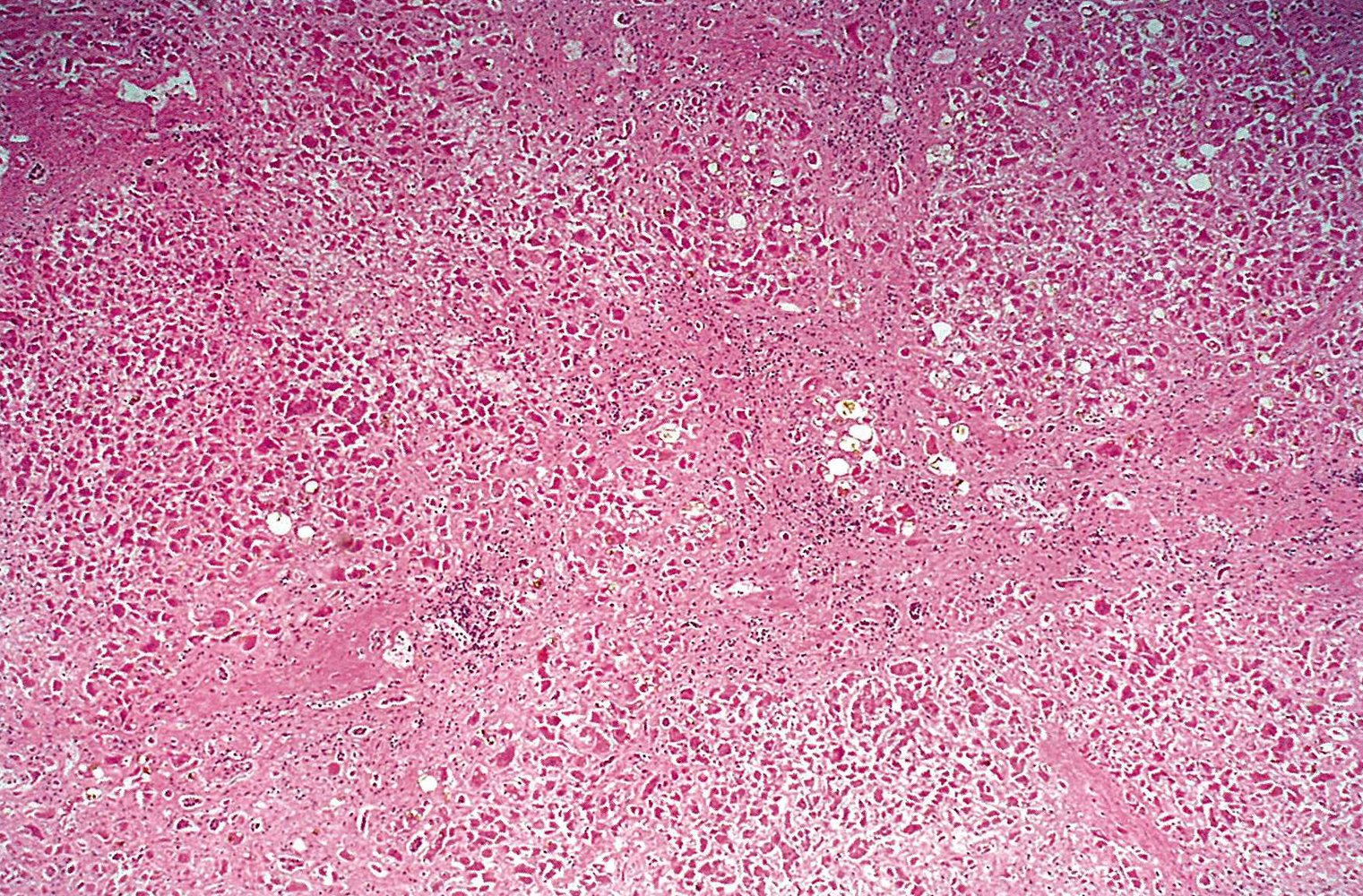
Photomicrograph of a liver tissue specimen from a patient with chronic hepatitis B (H&E stain; low magnification)
There is a total loss of liver tissue architecture (absence of defined hepatic lobules), and bridging fibrous septa (yellow overlay) can be seen.
These findings indicate liver cirrhosis following chronic viral hepatitis.
Source: © IMPP
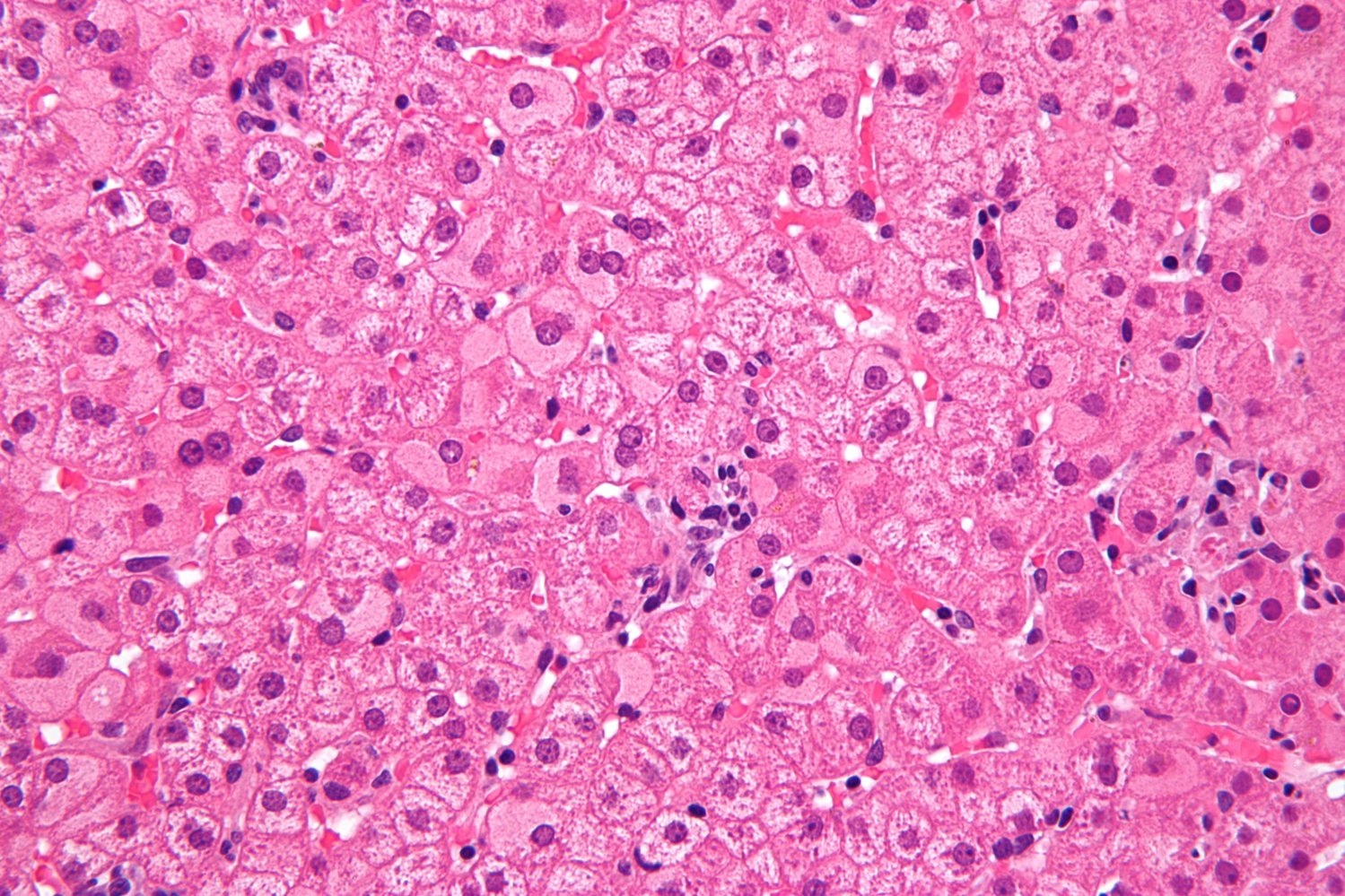
Photomicrograph of a liver biopsy specimen (H&E stain; high magnification)
Most of the hepatocytes have a pale, homogeneous cytoplasm (ground glass hepatocytes; examples marked by blue overlay).
Ground glass hepatocytes are often found in chronic hepatitis B infection.
Source: “Ground glass hepatocytes high mag 2” by Michael Bonert ("Nephron"), Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
Click on the Smartzoom button to view the entire specimen through a virtual microscope.
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: PD Dr. med. Alberto Perez Bouza, Facharzt für Pathologie
Differential diagnoses
For an overview comparing the different types of viral hepatitis see “Overview of viral hepatitides.”
The differential diagnoses listed here are not exhaustive.
Treatment
Approach [23][26][27][28]
-
All patients
- Provide supportive care; and patient education as needed.
-
Consider referral for liver transplantation in patients with:
- End-stage liver disease due to HBV
- Fulminant hepatic failure (emergency transplantation)
-
Acute hepatitis B
- Antiviral therapy is generally not indicated.
- In rare cases, patients may require management of acute liver failure.
-
Chronic hepatitis B
- Assess the need for antiviral therapy; refer to hepatology if indicated or uncertainty remains.
- Patients not on antiviral therapy should be monitored at fixed intervals based on disease activity.
- Consider indications for HCC screening.
Most acute hepatitis B infections in adults are self-limited. Antiviral therapy is not routinely indicated.
Antiviral therapy for chronic hepatitis B [23][26][27]
Treatment decisions should be made by a specialist and based on the risk of liver-related morbidity and mortality. The following information applies to nonpregnant individuals; for pregnant individuals, see “Management of hepatitis B in pregnancy.”
-
Indications for antiviral therapy for HBV infection include:
- Cirrhosis or advanced fibrosis
- Acute liver failure
- Immune active phase: ALT ≥ 2× ULN plus significantly elevated HBV DNA levels with or without HBeAg [23]
- HBV reactivation: an increase in HBV DNA or change from HBsAg negative to HBsAg positive in anti-HBc-positive patients
- Immunosuppression in HBV-positive patients
- Coinfection with HCV or HIV
- Family history of HCC
-
Agents: For details on mechanisms of action and adverse effects, see “Overview of antivirals against hepatitis B” and “Overview of antivirals against both hepatitis B and C.”
- Nucleotide reverse transcriptase inhibitors (NtRTIs), e.g., tenofovir disoproxil fumarate (TDF) or tenofovir alafenamide (TAF)
- Nucleoside reverse transcriptase inhibitors (NRTIs), e.g., entecavir (ETV)
- Pegylated interferon alfa (PEG-IFN-α)
-
Treatment regimens
- NtRTIs or NRTIs; are usually the preferred option; treatment duration varies but can be indefinite.
- PEG-IFN (e.g., for 48 weeks) is a treatment option for certain patient groups (e.g., younger patients with compensated liver disease, patients with HDV coinfection).
Treatment goals include immunologic cure (i.e., clearance of HBsAg and sustained HBV DNA suppression) and reduction of liver-related morbidity and mortality.
Pegylated interferon is a pregnancy category C drug, and is contraindicated in patients who have decompensated cirrhosis or uncontrolled psychiatric conditions.
Supportive care and patient education
- Avoid hepatotoxic medications.
- Advise alcohol cessation.
- Provide treatment of alcohol use disorder and/or management of substance use disorder as indicated.
- Provide counseling on weight and diet changes to encourage weight loss as indicated. [34]
- Educate patients on measures to prevent HBV transmission, including: [23]
- Vaccinating household and sexual contacts
- Abstaining from blood and tissue donation
- Practicing safer sex (e.g., using condoms)
- Covering open wounds
- Cleaning up blood spills with diluted bleach
- Avoiding IV drug use or practicing harm reduction strategies if injecting drugs
- Avoiding sharing of personal care items, such as razors, toothbrushes, glucometers, and injection equipment
HBV can survive outside the body (e.g., in dried blood on a surface) for at least 7 days, and remains infectious during that time. [5]
Complications
Acute liver failure
- Epidemiology: Affects ∼ 1% of acute HBV infections [35]
- Diagnosis: evidence of hepatic injury (e.g., ↑ transaminases, ↑ bilirubin), hepatic encephalopathy, and coagulopathy (INR > 1.5).
- Management: See “Acute liver failure.”
Long-term complications of hepatitis B [16]
- Liver cirrhosis
- Hepatocellular carcinoma (HCC) [36]
- Extrahepatic manifestations (10–20% of cases) [37]
- Polyarteritis nodosa (strong correlation: in 36% of cases, hepatitis B virus is the causative agent) [38]
-
Glomerulonephritis
- Membranous glomerulonephritis (more common)
- Membranoproliferative glomerulonephritis type 1 (less common)
- Aplastic anemia
- Reactivation of previous HBV infection due to immunosuppression
-
Post‑hepatitis syndrome
- Chronic fatigue, weakness
- Nausea, loss of appetite
- Possible upper quadrant pain
We list the most important complications. The selection is not exhaustive.
Prevention
Vaccination [5][39][40]
- The hepatitis B vaccine (HBV vaccine) is an inactivated recombinant vaccine that contains a subunit of the hepatitis B virus. [41]
- Single-antigen HBV vaccine
- Three-antigen HBV vaccine
- Combination HBV vaccines:
- DTaP-HepB-IPV vaccine
- DTaP-IPV-Hib-HepB vaccine
- HepA-HepB vaccine
-
The first dose of a 3-dose HBV vaccine series should be administered to all infants at birth
- Birth weight ≥ 2 kg: within 24 hours after birth
- Birth weight < 2 kg: at 1 month of age or hospital discharge (whichever occurs first)
-
Catch-up vaccination
- Unvaccinated children and adults aged < 59 years: Recommend for all; including during pregnancy. [40]
-
Unvaccinated adults aged ≥ 60 years
- With risk factors for HBV infection: Recommend vaccination.
- Without risk factors for HBV infection: Offer vaccination.
- Adults on dialysis or individuals ≥ 20 years with immunocompromise: Additional doses may be needed; see CDC for recommendations. [40]
- See “ACIP immunization schedule” for details.
Infants and children who did not receive a dose of vaccine at birth should receive the first dose as soon as possible.
Hepatitis B postvaccination serology [5][25]
Indications
- Individuals at risk of occupational exposure (e.g., health care workers)
- Immunocompromised individuals
- Patients receiving hemodialysis
- Sexual partners of HBsAg-positive persons
- Infants born to individuals with HBsAg positive or unknown status
Method
- Adults
- Test: anti-HBs titers
- Timing: 1–2 months after completion of vaccination
-
Infants [42]
- Tests: anti-HBs titers and HBsAg
- Timing: at ≤ 9 months of age and ≥ 1 month after the last dose of HBV vaccine
In infants, do not check postvaccination serology until they are least 9 months of age and their last HBV vaccine dose was at least 1 month ago. [43]
Follow up
- Anti-HBS ≥ 10 IU/mL: immune, and no further management is required
-
Anti-HBS < 10 IU/mL: non-immune
- Additional dose(s) and repeat postvaccination serology are required. Choose one of the following options:
- Administer 1 dose of HBV vaccine and repeat serology after 1–2 months. [5][25]
- Administer a second 3-dose HBV vaccine series and repeat serology after 1–2 months. [5][25]
- If repeat anti-HBs titers remain < 10 IU/mL after two complete series of HBV vaccine, the individual is considered an HBV vaccine nonresponder.
- Check HBsAg and anti-HBc levels to assess for HBV infection. [44]
- If HBsAg negative, counsel on measures to prevent HBV transmission.
- If exposed to HBV, see “Hepatitis B postexposure prophylaxis.”
- Additional dose(s) and repeat postvaccination serology are required. Choose one of the following options:
- HBsAg positive (in infants): Provide treatment for hepatitis B infection.
Hepatitis B postexposure prophylaxis [5]
For perinatal postexposure prophylaxis recommendations, see “Infants born to individuals with HBsAg positive or unknown status.”
- Exposure is defined as percutaneous or mucosal contact with blood or body fluids.
- Irrigate exposed tissue. [5]
- Mucous membranes: water
- Wounds and skin: soap and water
- HBV PEP recommendations differ for exposures in occupational and nonoccupational settings.
-
Depending on immunization status, affected individuals will receive one of the following:
- Active immunization (i.e., hepatitis B vaccination)
- Passive immunization (i.e., hepatitis B immune globulin)
- Combined active and passive immunization
- No intervention
Occupational exposure (i.e., health care providers)
- Verify vaccination status and immune response in the exposed health care provider (HCP).
- If series is complete and anti-HBs ≥ 10 mIU/mL is already documented, source patient HBsAg is not required.
- If series is complete and immune response is unknown, measure exposed HCP anti-HBs and source patient HBsAg.
- If unvaccinated or series is incomplete, measure source patient HBsAg only.
- See “Health care personnel exposures” for additional information, e.g., on needlestick injuries.
| HBV PEP for occupational exposure [5] | ||||
|---|---|---|---|---|
| HCP vaccination status | Source patient | |||
| HBsAg negative | HBsAg positive or unknown | |||
| Complete series | Anti-HBs ≥ 10 mIU/mL |
|
||
| Anti-HBs < 10 mIU/mL |
|
|
||
| Unvaccinated or incomplete series |
|
|||
Modification of work duties and sexual practices of HCPs following exposure to a patient with a positive or unknown HBsAg status is unnecessary during the 6-month follow-up period. Pregnancy and breastfeeding are safe during this time. [5]
HCPs exposed to a patient with a positive or unknown HBsAg status should not donate blood products, organs, tissue, and/or semen during the 6-month follow-up period. [5]
Nonoccupational exposure
- Exposure types include needle sharing and high-risk sexual contact.
- Obtain vaccination history and measure HBsAg, anti-HBs, and anti-HBc in unvaccinated exposed patients.
- Do not withhold or delay vaccination for prevaccination testing.
| HBV PEP following nonoccupational exposure [5][45] | |||
|---|---|---|---|
| Patient vaccination status | Source individual | ||
| HBsAg unknown | HBsAg positive | ||
| Complete series | Anti-HBs ≥ 10 mIU/mL |
|
|
| Anti-HBs < 10 mIU/mL or unknown |
|
|
|
| Unvaccinated or incomplete series |
|
|
|
Further notes: Materials developed and hosted by the CDC and available free of charge on the CDC website. Reference to specific commercial products, manufacturers, companies, or trademarks does not constitute its endorsement or recommendation by the U.S. Government, Department of Health and Human Services, or Centers for Disease Control and Prevention.
Perinatal hepatitis B
Approach [5][7][46]
- Perform universal screening for HBV in pregnancy, preferably in first trimester.
- If anti-HBs < 10 mIU/mL in a pregnant individual, initiate a 3-dose HBV vaccine series.
- If HBV serology indicates infection, manage HBV infection in pregnancy, including:
- Specialist referral
- Case reporting to relevant public health agencies
- Monitoring of HBV DNA and ALT
- Initiation of antiviral therapy in third trimester if HBV DNA > 200,000 IU/mL
- Provide appropriate immunoprophylaxis to infants born to individuals with HBsAg positive or unknown status.
- Administer first dose of HBV vaccine within 12 hours of birth.
- Infants born to HBsAg positive individuals: Additionally, administer 1 dose of HBIG within 12 hours of birth.
Hepatitis B vaccination is recommended for all pregnant individuals who have not been previously vaccinated. [46]
Hepatitis B in pregnancy [23][27][46]
The prevalence of HBV infection in pregnant individuals in the US is 0.9%. [47]
Screening for HBV infection in pregnancy [7][24][46]
Method
-
During each pregnancy, as part of initial prenatal screening for comorbidities during the first trimester
- All pregnant individuals: Test for HBsAg.
- Individuals with any of the following: Measure anti-HBs and anti-HBc titers.
- No documented completion of HBV vaccine series
- No documented initial HBV serology after 18 years of age
- Risk factors for HBV infection developed after documentation of initial HBV serology and/or are ongoing
-
When admitted for delivery, screen individuals if either:
- Screening was not done in prenatal period
- Or ongoing risk factors for HBV infection are present
Further management
- Anti-HBs < 10 mIU/mL: Administer a 3-dose hepatitis B vaccine series.
- HBV serology indicating infection: See “Management of hepatitis B in pregnancy.”
Management of HBV infection in pregnancy [48][49]
During pregnancy
-
For patients with newly positive HBsAg on prenatal screening, obtain additional HBV serology, including:
- Initial tests (i.e., anti-HBs, anti-HBc) if not already done
- Tests for additional disease markers (e.g., HBV DNA level, HBeAg, anti-HBe, and ALT level)
- Refer to infectious disease and/or hepatology specialists.
- Report case to state and local perinatal hepatitis B prevention programs (see “Tips and Links”). [45]
- Monitor HBV DNA and ALT every 3 months.
-
Evaluate the need for antiviral therapy with tenofovir disoproxil fumarate (preferred drug) ; [27][49]
- Standard indications for antiviral therapy for HBV infection (e.g., cirrhosis): A hepatologist may recommend therapy throughout pregnancy to prevent complications. [27][49]
- HBV DNA > 200,000 IU/mL: Initiate therapy during the third trimester to reduce the risk of vertical transmission.
Antiviral treatment is recommended in pregnant individuals with an HBV viral load > 200,000 IU/mL to reduce the risk of vertical transmission. [46]
Pegylated interferon alfa is a pregnancy category C drug and is therefore not recommended as first-line therapy for HBV infection in pregnant individuals. [49]
During delivery
- HBV infection is not an indication for cesarean delivery. [23][46]
- Follow standard precautions. [50]
After delivery
-
Breastfeeding may be started immediately if there are no contraindications (e.g., cracked or bleeding nipples), regardless of whether individuals:
- Have HBsAg positive or unknown status [5]
- Are receiving antiviral therapy [23][46]
- Continue close monitoring (e.g., of HBV DNA and ALT levels) for at least 6 months postpartum. [48]
Hepatitis B in infants [5][25][46]
Management of infants born to individuals with HBsAg positive or unknown status
These infants are at risk of acquiring perinatal HBV infection and developing complications.
- Administer the birth dose of HBV vaccine to all infants within 12 hours of life.
- If the birthing parent's HBsAg status is unknown, obtain test immediately.
- Determine the need for HBIG.
- This depends on the birthing parent's HBsAg status and infant's birth weight (see table).
- If HBIG and HBV vaccine are administered concurrently, they should be given in different limbs.
- Report case to state and local perinatal hepatitis B prevention programs (see “Tips and Links”).
| Management of infants born to HBsAg-positive and HBsAg-unknown individuals [5][25][46] | |||
|---|---|---|---|
| Status of birthing parent at delivery | HBIG [25] | HBV vaccine | |
| HBsAg-positive or other evidence of HBV infection |
|
|
|
| HBsAg-unknown | < 2,000 g birth weight |
|
|
| ≥ 2,000 g birth weight |
|
||
Infants born to HBsAg-positive individuals should receive 1 dose of HBIG and the first dose of HBV vaccine within 12 hours of birth. [5][25]
If birth weight is < 2,000 g, the dose of HBV vaccine given at birth does not count towards the vaccine series. [5]
Infants with HBV infection
- Transaminases are usually normal or only mildly elevated.
- Acute hepatitis B may develop in rare cases.
-
Chronic HBV infection [5]
- Develops in 80–90% of infants infected at birth
- 25% of those with chronic infection develop cirrhosis or liver cancer, leading to premature mortality.
Related One-Minute Telegram
- One-Minute Telegram 143-2026-3/3: Vax-ing and waning: the rise and fall of newborn HBV vaccination
Interested in the newest medical research, distilled down to just one minute? Sign up for the One-Minute Telegram in “Tips and links” below.
External Resources
- Sign up for the One-Minute Telegram
- 2023 CDC Recommendations on Screening and Testing for Hepatitis B Virus Infection
- 2020 USPSTF Hepatitis B Virus Infection in Adolescents and Adults: Screening
- 2018 CDC Recommendations on Prevention of Hepatitis B Virus Infection in the United States
- 2018 AASLD Update on Prevention, Diagnosis, and Treatment of Chronic Hepatitis B
- 2017 EASL Clinical Practice Guidelines on the Management of Hepatitis B Virus Infection
- 2015 AASLD Guidelines for Treatment of Chronic Hepatitis B
- CDC Hepatitis B
- CDC Perinatal Hepatitis B Prevention Program
References
- Daniels D, Grytdal S, Wasley A, Centers for Disease Control and Prevention (CDC).. "Surveillance for acute viral hepatitis - United States, 2007.". Morbidity and mortality weekly report. Surveillance summaries (Washington, D.C. : 2002). 58(3). :1-27. (2009)
- "Hepatitis B Questions and Answers for Health Professionals". https://web.archive.org/web/20200723170835/https://www.cdc.gov/hepatitis/hbv/hbvfaq.htm#overview. [2020-03-16]
- Hyun Kim B, Ray Kim W. "Epidemiology of Hepatitis B Virus Infection in the United States". Clinical Liver Disease. 12(1). :1-4. (2018)
- "Hepatitis B". http://www.who.int/mediacentre/factsheets/fs204/en/. [2016-07-01]
- Schillie S, Vellozzi C, Reingold A, et al. "Prevention of Hepatitis B Virus Infection in the United States: Recommendations of the Advisory Committee on Immunization Practices". MMWR Recomm Rep. 67(1). :1-31. (2018)
- Abara WE, Qaseem A, Schillie S, McMahon BJ, Harris AM. "Hepatitis B Vaccination, Screening, and Linkage to Care: Best Practice Advice From the American College of Physicians and the Centers for Disease Control and Prevention". Ann Intern Med. 167(11). :794. (2017)
- Conners EE, Panagiotakopoulos L, Hofmeister MG, et al. "Screening and Testing for Hepatitis B Virus Infection: CDC Recommendations — United States, 2023". MMWR Morb Mortal Wkly Rep. 72(1). :1-25. (2023)
- Krist AH, Davidson KW, et al. "Screening for Hepatitis B Virus Infection in Adolescents and Adults". JAMA. 324(23). :2415. (2020)
- Köck J, Schlicht HJ. "Analysis of the earliest steps of hepadnavirus replication: genome repair after infectious entry into hepatocytes does not depend on viral polymerase activity.". J Virol. 67(8). :4867-74. (1993)
- Datta S, Chatterjee S, Veer V, Chakravarty R. "Molecular Biology of the Hepatitis B Virus for Clinicians". Journal of Clinical and Experimental Hepatology. 2(4). :353-365. (2012)
- Urban S, Schulze A, Dandri M, Petersen J. "The replication cycle of hepatitis B virus". J Hepatol. 52(2). :282-284. (2009)
- Beck J, Nassal M. "Hepatitis B virus replication". World J Gastroenterol. 13(1). :48-64. (2007)
- Balmasova IP. "Immunopathogenesis of chronic hepatitis B". World Journal of Gastroenterology. 20(39). :14156. (2014)
- Hai H, Tamori A, Kawada N. "Role of hepatitis B virus DNA integration in human hepatocarcinogenesis". World J Gastroenterol. 20(20). :6236-43. (2014)
- Burns GS, Thompson AJ. "Viral Hepatitis B: Clinical and Epidemiological Characteristics". Cold Spring Harbor Perspectives in Medicine. 4(12). :a024935-a024935. (2014)
- Lok ASF. "Clinical Manifestations and Natural History of Hepatitis B Virus Infection". UpToDate. UpToDate. https://www.uptodate.com/contents/clinical-manifestations-and-natural-history-of-hepatitis-b-virus-infection. [2015-05-04]
- Wener MH. "Serum Sickness and Serum Sickness-Like Reactions". UpToDate. UpToDate. https://www.uptodate.com/contents/serum-sickness-and-serum-sickness-like-reactions. [2015-10-19]
- Sharma SK, Saini N, Chwla Y. "Hepatitis B virus: inactive carriers". Virol J. 2. :82. (2005)
- Fattovich G, Bortolotti F, Donato F. "Natural history of chronic hepatitis B: Special emphasis on disease progression and prognostic factors". J Hepatol. 48(2). :335-352. (2008)
- Terrault NA, Lok ASF, McMahon BJ, et al. "Update on prevention, diagnosis, and treatment of chronic hepatitis B: AASLD 2018 hepatitis B guidance". Hepatology. 67(4). :1560-1599. (2018)
- Wilkins T, Sams R, Carpenter M. "Hepatitis B: Screening, Prevention, Diagnosis, and Treatment.". Am Fam Physician. 99(5). :314-323. (2019)
- Terrault NA, Bzowej NH, Chang K-M, et al. "AASLD guidelines for treatment of chronic hepatitis B". Hepatology. 63(1). :261-283. (2016)
- Hall E., Wodi A.P., Hamborsky J. et al. "Hepatitis B". Centers for Disease Control and Prevention. (2021). ISBN: 0017066050
- Lampertico P, Agarwal K, Berg T, et al. "EASL 2017 Clinical Practice Guidelines on the management of hepatitis B virus infection". J Hepatol. 67(2). :370-398. (2017)
- Kurtz AB, Rubin CS, Cooper HS, et al. "Ultrasound findings in hepatitis". Radiology. 136(3). :717-723. (1980)
- Rubin E, Reisner HM. "Essentials of Rubin's Pathology". Lippincott Williams & Wilkins. (2009). ISBN: 9780781773249
- Ferrell L. "Liver pathology: cirrhosis, hepatitis, and primary liver tumors: Update and diagnostic problems". Mod Pathol. 13(6). :679-704. (2000)
- "Liver and Intrahepatic Bile Ducts - Nontumor - Hepatitis (Acute and Chronic) - Chronic Hepatitis - General". http://www.pathologyoutlines.com/topic/liverchronichepgeneral.html. [2017-10-31]
- Cohen C. ""Ground-glass" hepatocytes". S Afr Med J. 49(34). :1401-1403. (1975)
- El- Kader SMA, Al-Dahr MHS. "Impact of weight reduction program on serum alanine aminotransferase activity and immunologic response in obese hepatitis B patients". Afr Health Sci. 16(1). :128. (2016)
- Manka P, Verheyen J, Gerken G, Canbay A. "Liver Failure due to Acute Viral Hepatitis (A-E)". Visceral Medicine. 32(2). :80-85. (2016)
- Xie Y. "Hepatitis B virus-associated hepatocellular carcinoma". Springer Singapore. :11-21. (2017). ISBN: 9789811057649
- Cacoub P, Terrier B. "Hepatitis B-Related Autoimmune Manifestations". Rheumatic Disease Clinics of North America. 35(1). :125-137. (2009)
- Guillevin L, Mahr A, Callard P, et al. "Hepatitis B Virus-Associated Polyarteritis Nodosa". Medicine. 84(5). :313-322. (2005)
- Weng MK, Doshani M, Khan MA, et al. "Universal Hepatitis B Vaccination in Adults Aged 19–59 Years: Updated Recommendations of the Advisory Committee on Immunization Practices — United States, 2022". MMWR Morb Mortal Wkly Rep. 71(13). :477-483. (2022)
- "CDC/ACIP Vaccines & Immunizations: Immunization Schedules". https://web.archive.org/web/20250318202018/https://www.cdc.gov/vaccines/hcp/imz-schedules/index.html. [2024-11-21]
- "CDC Viral Hepatitis Hep B Information Frequently Asked Questions for Health Professionals". https://web.archive.org/web/20230711155352/https://www.cdc.gov/hepatitis/hbv/hbvfaq.htm. [2022-03-30]
- AAP Committee on Infectious Diseases. "Red Book: 2021–2024 Report of the Committee on Infectious Diseases". American Academy of Pediatrics. (2021). ISBN: 9781610025218
- Schillie S, Murphy TV, Fenlon N, Ko S, Ward JW. "Update: Shortened Interval for Postvaccination Serologic Testing of Infants Born to Hepatitis B-Infected Mothers". MMWR Morb Mortal Wkly Rep. 64(39). :1118-1120. (2015)
- "Management of Infants Born to Women with Hepatitis B Virus Infection for Pediatricians". https://www.cdc.gov/vaccines/programs/perinatal-hepb/downloads/HepB-Provider-tipsheet-508.pdf. [2018-01-12]
- "Pinkbook: epidemiology and Prevention of Vaccine-Preventable Diseases - Hepatitis B". https://web.archive.org/web/20240413140347/https://www.cdc.gov/vaccines/pubs/pinkbook/hepb.html. [2021-08-18]
- Workowski KA, Bachmann LH, Chan PA, et al. "CDC Sexually Transmitted Infections Treatment Guidelines 2021". MMWR Recomm Rep. 70(4). :1-187. (2021)
- Hwang JP, Lok AS. "USPSTF 2020 Hepatitis B Screening Recommendation". JAMA. 324(23). :2380. (2020)
- Owens DK, Davidson KW, et al. "Screening for Hepatitis B Virus Infection in Pregnant Women". JAMA. 322(4). :349. (2019)
- Gerlich WH, Glebe D, Kramvis A, Magnius LO. "Peculiarities in the designations of hepatitis B virus genes, their products, and their antigenic specificities: a potential source of misunderstandings". Virus Genes. 56(2). :109-119. (2020)
- Committee on Clinical Practice Guidelines–Obstetrics. "Viral Hepatitis in Pregnancy". Obstet Gynecol. 142(3). :745-759. (2023)
- USPSTF. "Screening for Hepatitis B Virus Infection in Pregnant Women: Recommendation Statement". Am Fam Physician. 101(2). :112-114. (2020)
- Aslam A, Campoverde Reyes KJ, Malladi VR, Ishtiaq R, Lau DTY. "Management of chronic hepatitis B during pregnancy". Gastroenterol Rep (Oxf). 6(4). :257-262. (2018)
- Ayoub WS, Cohen E. "Hepatitis B Management in the Pregnant Patient: An Update". J Clin Trans Hepatol. 4(3). :241-247. (2016)
- Siegel JD, Rhinehart E, Jackson M, Chiarello L. "2007 Guideline for Isolation Precautions: Preventing Transmission of Infectious Agents in Health Care Settings". Am J Infect Control. 35(10). :S65-S164. (2007)
- Franco E. "Hepatitis A: Epidemiology and prevention in developing countries". World Journal of Hepatology. 4(3). :68. (2012)
- MacLachlan JH, Cowie BC. "Hepatitis B Virus Epidemiology". Cold Spring Harbor Perspectives in Medicine. 5(5). :a021410-a021410. (2015)
- Mirazo S, Ramos N, Mainardi V, Arbiza J, Gerona S. "Transmission, diagnosis, and management of hepatitis E: an update". Hepatic Medicine: Evidence and Research. :45. (2014)
- Negro F. "Hepatitis D Virus Coinfection and Superinfection". Cold Spring Harbor Perspectives in Medicine. 4(11). :a021550-a021550. (2014)
- Kamar N, Izopet J, Dalton HR. "Chronic Hepatitis E Virus Infection and Treatment". Journal of Clinical and Experimental Hepatology. 3(2). :134-140. (2014)
- Matheny SC, Kingery JE. "Hepatitis A.". Am Fam Physician. 86(11). :1027-34; quiz 1010-2. (2012)
- "Epidemiological estimates of viral hepatitis". https://www.who.int/westernpacific/health-topics/hepatitis/regional-hepatitis-data. [2018-07-23]
- Jafri S, Gordon SC. "Epidemiology of Hepatitis C". Clinical Liver Disease. 12(5). :140-142. (2018)
- Farci P, Niro G. "Clinical Features of Hepatitis D". Semin Liver Dis. 32(03). :228-236. (2012)
- Wedemeyer H, Pischke S, Manns MP. "Pathogenesis and Treatment of Hepatitis E Virus Infection". Gastroenterology. 142(6). :1388-1397.e1. (2012)
- Choi M, Hofmann J, Köhler A, et al. "Prevalence and Clinical Correlates of Chronic Hepatitis E Infection in German Renal Transplant Recipients With Elevated Liver Enzymes". Transplantation Direct. 4(2). :e341. (2018)
- Guan R, Lui HF. "Treatment of Hepatitis B in Decompensated Liver Cirrhosis". International Journal of Hepatology. 2011. :1-11. (2011)
- Patel DM, Butler J, Feldman S, Graves GR, Rhodes PG. "Immunogenicity of hepatitis B vaccine in healthy very low birth weight infants". J Pediatr. 131(4). :641-643. (1997)
- Harris AM, Iqbal K, Schillie S, et al. "Increases in Acute Hepatitis B Virus Infections — Kentucky, Tennessee, and West Virginia, 2006–2013". MMWR Morb Mortal Wkly Rep. 65(3). :47-50. (2016)
- "Surveillance for Viral Hepatitis – United States, 2017". https://web.archive.org/web/20200804151623/https://www.cdc.gov/hepatitis/statistics/2017surveillance/index.htm. [2019-11-14]