Quick guide
Diagnostic approach
- Neurovascular exam
- Assess for associated injuries and acute complications (e.g., compartment syndrome).
- X-ray hip and pelvis
- MRI or CT hip if occult fracture is suspected
- CBC
- BMP
- Type and screen
- ECG if there is unexplained syncope
- Additional diagnostics in trauma as needed (e.g., FAST, CT head)
- Preoperative assessment
Red flag features
- Intracapsular fracture (e.g., femoral head and neck)
- Open fracture
- Neurovascular injury
- Compartment syndrome
- Fracture-dislocation
Management checklist
- ATLS algorithm for unstable patients or those with polytrauma
- Consult orthopedic surgery urgently.
- Peripheral nerve block and opioid-sparing acute pain management
- Treat acute comorbidities (e.g., anemia, AKI).
- Periprocedural management of oral anticoagulants as needed
- VTE prophylaxis if surgery is delayed
Summary
Hip fractures are classified as intracapsular (femoral head, femoral neck) or extracapsular (intertrochanteric, trochanteric, or subtrochanteric). Hip fractures in older adults are typically low-impact injuries and are often associated with osteoporosis. Hip fractures in younger patients are usually caused by a high-energy impact (e.g., motor vehicle collision). Clinical features include groin pain and deformity of the hip. X-rays are usually diagnostic, but an MRI may be required to diagnose occult fractures or pathologic fractures. Comorbid conditions (e.g., anemia, acute kidney injury, delirium) are common with hip fractures. Management typically includes multidisciplinary consultation, early pain management, IV fluid hydration, venous thromboembolism prophylaxis, and early surgical fixation. Nonoperative management may be considered for patients with severe comorbidities, although it is associated with a high mortality rate. Older adults are at the highest risk of morbidity and mortality; early involvement of geriatric care specialists is recommended for these patients. Thromboembolism and osteonecrosis of the femoral head are common severe complications. Hip fractures can be associated with hip dislocation. Posterior hip dislocations account for 90% of hip dislocations and typically follow a dashboard injury. Early reduction is vital to avoid vascular compromise and sciatic nerve injury.
Epidemiology
- Peak incidence: > 70 years [1]
- Sex: ♀ > ♂ [1]
Epidemiological data refers to the US, unless otherwise specified.
Etiology
-
Mechanism of injury [2]
-
Older adults
- Fall onto greater trochanter/lateral hip
- Forced lateral rotation (e.g., from tripping)
- Chronic overburdening can lead to insufficiency fractures, which can then completely fracture spontaneously.
- Pathological fracture due to metastases
- Children and young adults: high-speed trauma (e.g., motor vehicle accidents or falls from great heights) or underlying disease (e.g., fibrous dysplasia)
-
Older adults
-
Risk factors [2]
- Osteoporosis (especially postmenopausal women and older individuals)
- Muscle weakness
- Difficulty walking and impaired coordination
- Estrogen deficiency
- Low body weight
- Poor nutrition (vitamin D deficiency or calcium deficiency)
- Smoking, alcohol use
Initial management
Approach
-
All patients
- Identify associated injuries and complications that affect immediate management (e.g., open fracture, fracture-dislocation, neurovascular injury).
- Initiate multimodal pain management without delay (e.g., for confirmatory imaging).
- Obtain hip and pelvis x-rays and other hip fracture diagnostics as needed.
- Consult orthopedic surgery urgently.
- Manage comorbidities that affect short-term outcomes (see "Acute management of comorbidities”).
- Admit to hospital and begin multidisciplinary care.
- Provide definitive hip fracture treatment based on fracture type (see “Subtypes and variants”).
-
Unstable patients or those with polytrauma
- Follow the ATLS algorithm.
- Obtain bedside pelvis x-ray; defer other hip imaging until the patient is stabilized.
- Perform emergency preoperative assessment.
Pain management [3][4][5]
-
Preoperative peripheral nerve blocks [6]
- Recommended for all patients without contraindications. [3][5][6]
- Options: femoral block or fascia iliaca block by a trained specialist
-
Systemic analgesics [5][7]
- Use an opioid-sparing strategy (see “Acute pain management” for details).
- Use NSAIDs with caution; comorbid acute kidney injury (AKI) is common.
- Avoid anticholinergics, muscle relaxants, benzodiazepines, and gabapentinoids because they increase the risk of delirium.
A preoperative peripheral nerve block is recommended to improve pain control and reduce opioid consumption and the risk of perioperative delirium. [8]
Acute management of comorbidities
The following conditions are commonly associated with hip fractures and should be managed early as they can impact perioperative outcomes. See “Hip fracture in older adults” for age-related comorbidities.
- Anemia: Consider blood transfusion in symptomatic patients and/or those with hemoglobin < 8 g/dL. [3][9]:
-
AKI
- See “Management of AKI” for the approach to fluid replacement and hemodynamic monitoring.
- Withhold ACEIs and ARBs before surgery (see “Perioperative medication management” for details).
-
Venous thromboembolism (VTE) [10]
- Preoperative VTE prophylaxis: indicated if surgery is delayed [7]
- Administer LMWH (e.g., enoxaparin) up to 12 hours before surgery.
- See dosage for “Medical inpatients” in “Approach to VTE prophylaxis.”
- Postoperative VTE prophylaxis
- Resume LMWH after surgery and continue for 5 weeks.
- See dosage for “Surgical patients” in “Approach to VTE prophylaxis.”
- Preoperative VTE prophylaxis: indicated if surgery is delayed [7]
-
Acquired coagulopathy from antithrombotic agents [7]
- Aspirin for management of ASCVD is typically continued.
- Adjustment of dual antiplatelet therapy requires specialist consultation.
- VKA use may require anticoagulant reversal (e.g., with vitamin K).
- Surgery may need to be delayed for patients using DOACs.
- Further details
- See “Perioperative medication management.”
- See “Periprocedural management of oral anticoagulants.”
- See “Anticoagulant reversal.”
Disposition [11]
All individuals with hip fractures require hospital admission and multidisciplinary care.
- Consult orthopedics to determine if operative treatment is indicated.
- Consult medical specialists for the comanagement of medical comorbidities as required.
- Follow local protocols and admitting service agreements.
- Patients > 70 years of age are likely best treated in comprehensive geriatrics units (see “Hip fracture in older adults”). [11]
- Patients with hip fractures are often admitted to the hospitalist service or internal medicine.
- Consult other specialists as needed (e.g., physical therapist, occupational therapist, nutritionist, social worker).
Diagnosis
Clinical evaluation [12]
Perform the following prior to imaging of suspected hip fractures because they can impact acute management. See “Subtypes and variants” for clinical features by fracture type.
-
Neurovascular examination
-
Femoral artery injury
- Assess femoral, popliteal, dorsalis pedis, and posterior tibial artery pulses.
- Compare to the contralateral side if there is concern for arterial insufficiency.
- Sciatic nerve injury (The sciatic nerve branches into the tibial nerve and common peroneal nerve.)
-
Femoral artery injury
- Evaluation for severe complications (e.g., clinical features of acute compartment syndrome, skin laceration suggestive of open fracture)
Imaging [13]
-
X-ray hip and pelvis (first line) [14][15]
- Hip: AP view and lateral views
- Pelvis: AP view
- MRI hip and pelvis: preferred if an occult fracture is suspected [13]
- Other: CT hip or bone scan
Suspect occult fracture despite normal x-rays in patients with characteristic clinical features of hip fracture. [13]




Laboratory studies
- CBC: Evaluate for acute blood loss. [16]
- BMP: Evaluate for AKI. [17]
- Type and screen. [18]
- Additional preoperative testing for intermediate-risk surgery as indicated
Additional studies [12]
Consider the following based on clinical presentation:
- Concurrent trauma: e.g., CT head (See “Diagnostics in trauma.”)
- Unexplained syncope: e.g., ECG, cardiac monitoring (See “Syncope workup.”)
- See also “Hip fracture in older adults.”
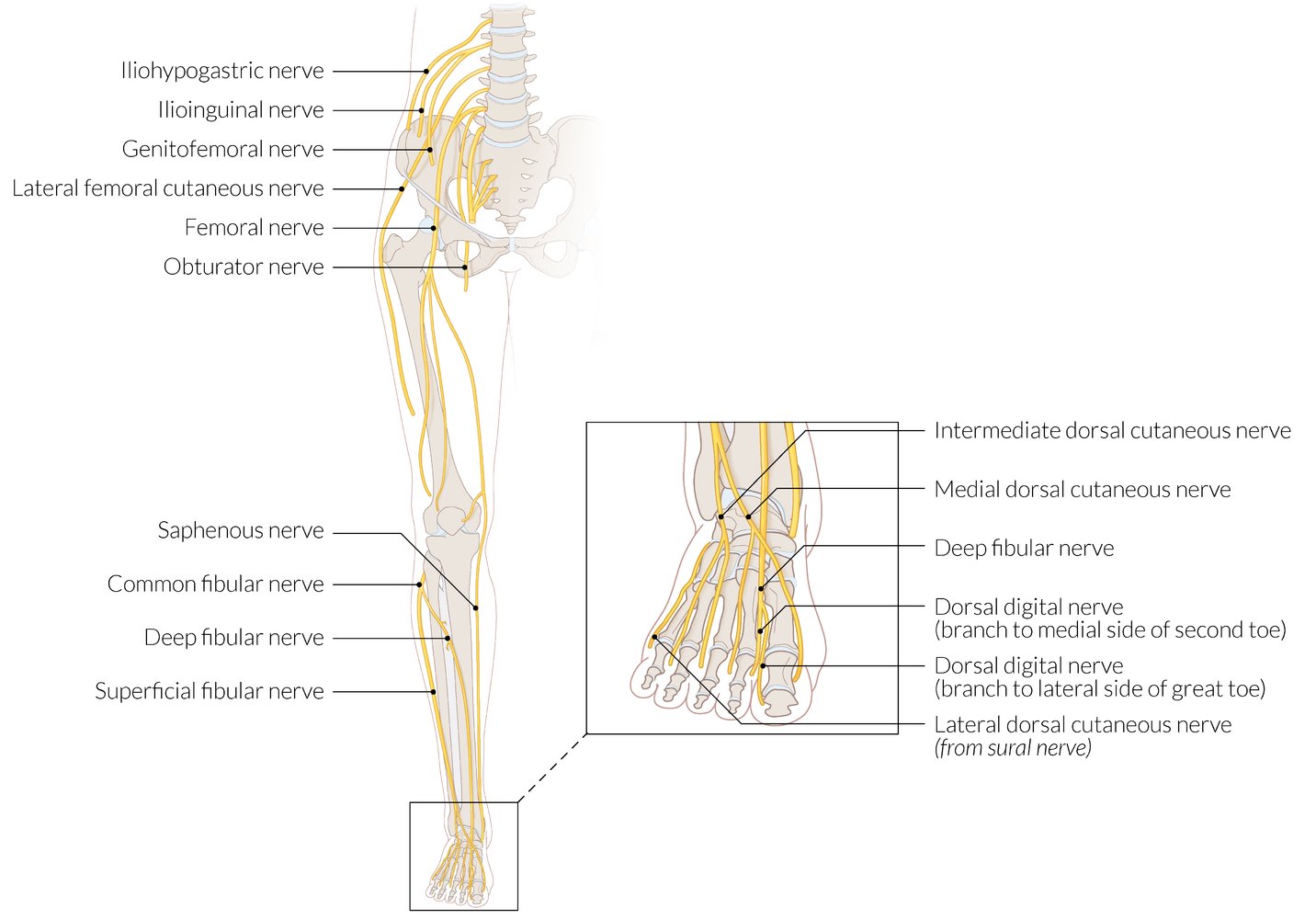
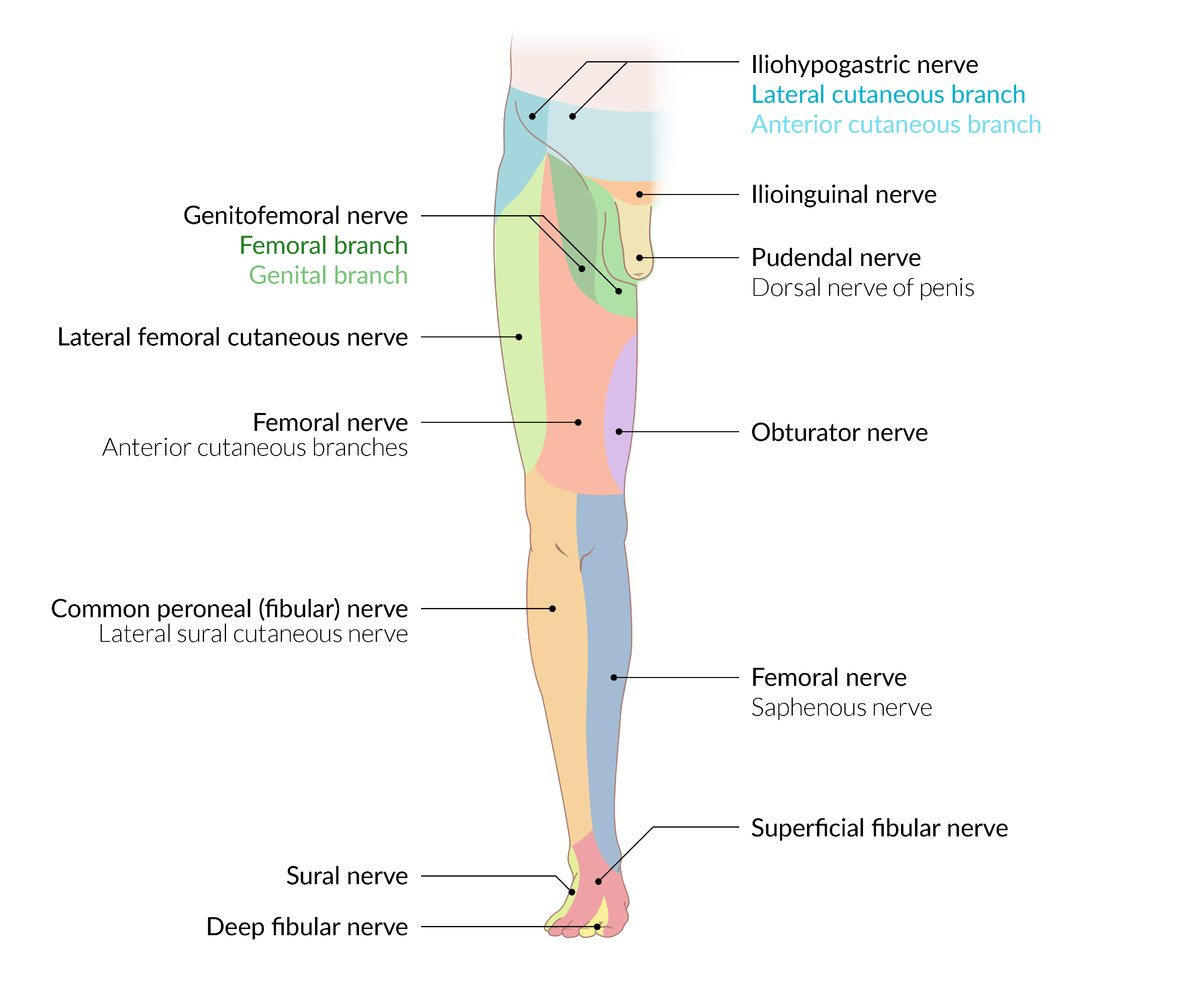
The femoral nerve is the main nerve of the anterior compartment of the thigh. The saphenous nerve and the medial and intermediate cutaneous nerves of the thigh originate from the femoral nerve.
The obturator nerve is the main nerve of the medial compartment of the thigh and exits the pelvis ventrally through the obturator foramen.
The iliohypogastric, ilioinguinal, genitofemoral, and lateral femoral cutaneous nerves are pure sensory nerves that arise directly from the lumbar plexus.
The common fibular nerve (a terminal branch of the sciatic nerve) branches into the superficial and deep peroneal nerves at or just below the neck of the fibula.
Cutaneous innervation of the foot is supplied by the saphenous nerve medially and the sural nerve laterally.
Cutaneous innervation of the dorsum of the foot is supplied by branches of the superficial fibular nerve, with the exception of the first interdigital space, which is supplied by a branch of the deep fibular nerve.
© AMBOSS
© AMBOSS
© AMBOSS

X-ray right hip (AP view)
A comminuted intertrochanteric fracture (fragments indicated by green, white, and yellow overlay) of the right femur is accompanied by superior displacement of the femoral shaft and distraction (indicated by red dashed lines and arrows) of the main fracture fragments.
Source: “Late Presentation of an Iatrogenic Pseudoaneurysm of the Profunda Femoris Artery following Intramedullary Nailing” by Kira Vande Voorde, Jan Dauwe, and Jan Van Oost, Hindawi, licensed under CC BY 4.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).

X-ray right hip (AP view)
The femoral neck is slightly deformed by a subtle irregular fracture (green overlay) that traverses the neck. The hip also shows degenerative osteophytes (dashed lines).
Source: “Fig. 1, in: Femoral neck fracture: the reliability of radiologic classifications” by Cazzato G., Oliva M.S., Masci G., et al., BMC Musculoskeletal Disorders, licensed under CC BY 4.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).

X-ray of the pelvis (AP view)
Partially displaced femoral neck fracture (Garden III).
Source: © IMPP

This CT reconstruction shows a dorsal view of the pelvis and femurs with a type C subtrochanteric fracture of the left femur.
Source: © IMPP
Treatment
General principles
- Treatment can vary depending on the fracture type and patient characteristics:
- See “Hip fractures in older adults.”
- See “Femoral head fracture” and “Femoral neck fracture.”
- See “Trochanteric fracture” and “Subtrochanteric fracture.”
- See “Hip fracture-dislocation.”
- Operative intervention is recommended for most patients.
Operative treatment
- Timing: Ideally within 24–48 hours of admission [3][19]
-
Surgical technique depends on fracture location and characteristics [19]
- Cancellous screws: nondisplaced femoral neck fracture
- Dynamic hip screw: nondisplaced base of femoral neck fracture
- Arthroplasty or hemiarthroplasty: displaced femoral neck fracture
-
Postoperative management:
- Initiate weight-bearing activity immediately after surgery to decrease complications. [20]
- Initiate an enhanced recovery after surgery program (ERAS) if available at the local institution. [7][21][22]
- ERAS programs decrease the time to surgery, length of stay, and complication rate. [22]
- Program components include peripheral nerve blocks, avoidance of prolonged fasting, early removal of drains, and early ambulation. [21]
Expedite medical evaluation and perioperative optimization to facilitate an operative repair within 48 hours of admission. [7]



")
Nonoperative treatment
Nonoperative management of hip fractures is uncommon as mortality rate is high. [19][23][24]
-
Indications [1][7]
- Extremely high perioperative risk (e.g., acute heart failure)
- Limited benefit of surgery (e.g., the patient has a terminal illness, severe dementia, and/or is nonambulatory)
- Some stable femoral neck fractures or simple avulsion fractures
- Treatment includes pain management, bed rest, and/or assisted mobilization. [25]
Weight-bearing status is determined by orthopedics. Clarify weight-bearing precautions and range of motion prior to consulting physical and occupational therapy.
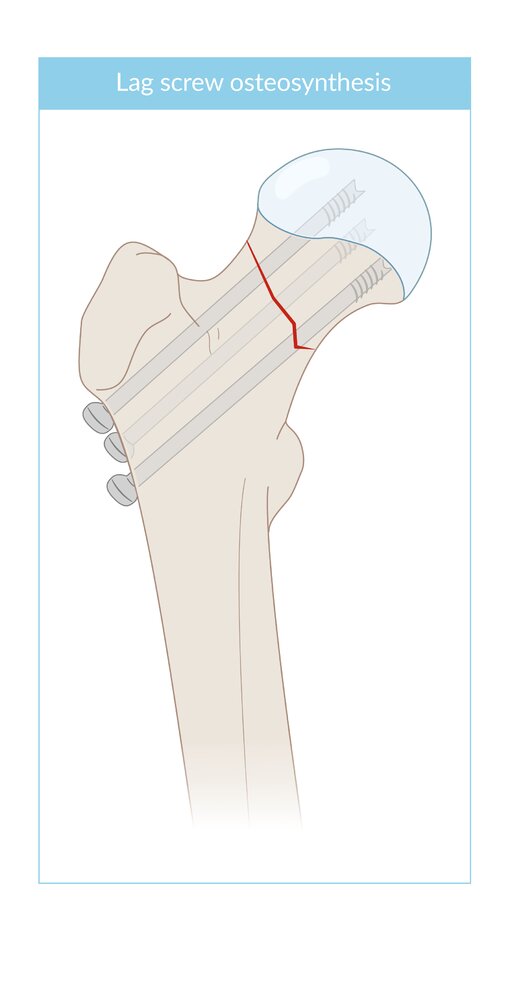
Three cancellous lag screws were used to stabilize a femoral neck fracture. They are positioned parallel to each other and parallel to the longitudinal axis of the femoral neck. These screws have a thread only at the terminal end, and the thread does not cross the fracture line. Tightening the screws, therefore, compresses the fracture fragments.
© AMBOSS
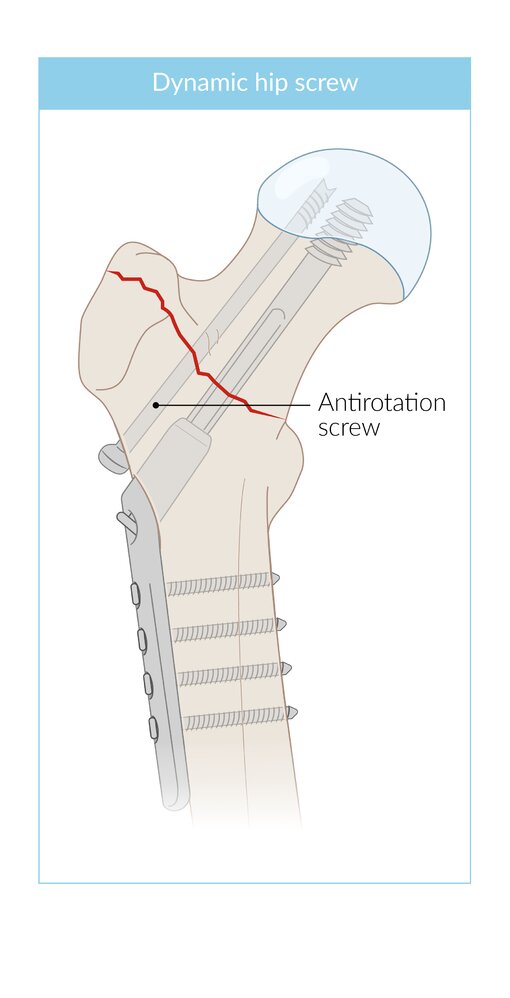
A dynamic hip screw (sliding hip screw) is an orthopedic implant used in the fixation of hip fractures of the intertrochanteric or lower femoral neck region.
The DHS consists of a sliding lag screw, a stabilizing side plate with a barrel (through which the lag screw is placed) and cortical screws for the fixation of the side plate. Movement of the lag screw along the barrel of the stabilizing plate allows for dynamic compression of the fracture as the patient bears weight (which aids bone healing). If there is rotational instability, an additional antirotation screw may be placed.
© AMBOSS
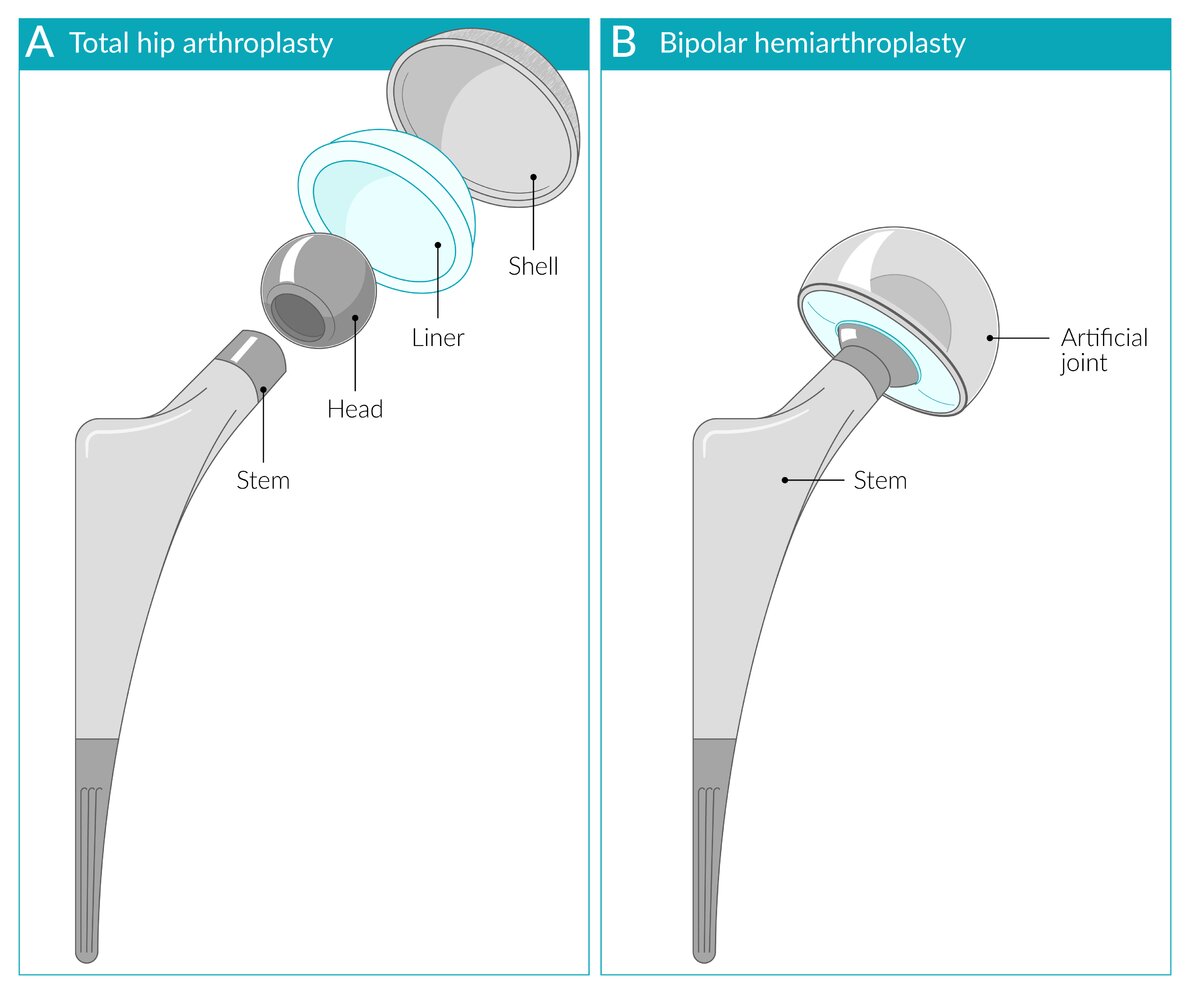
A total hip arthroplasty (A) consists of a shell (titanium), a liner (metal, ceramic, or polyethylene), a head (metal or ceramic), and a stem (titanium).
A bipolar hemiarthroplasty (B), as shown here, consists of a stem and a small head within a second head the size of the original femoral head. In hemiarthroplasty, the acetabulum remains the patient's own.
© AMBOSS
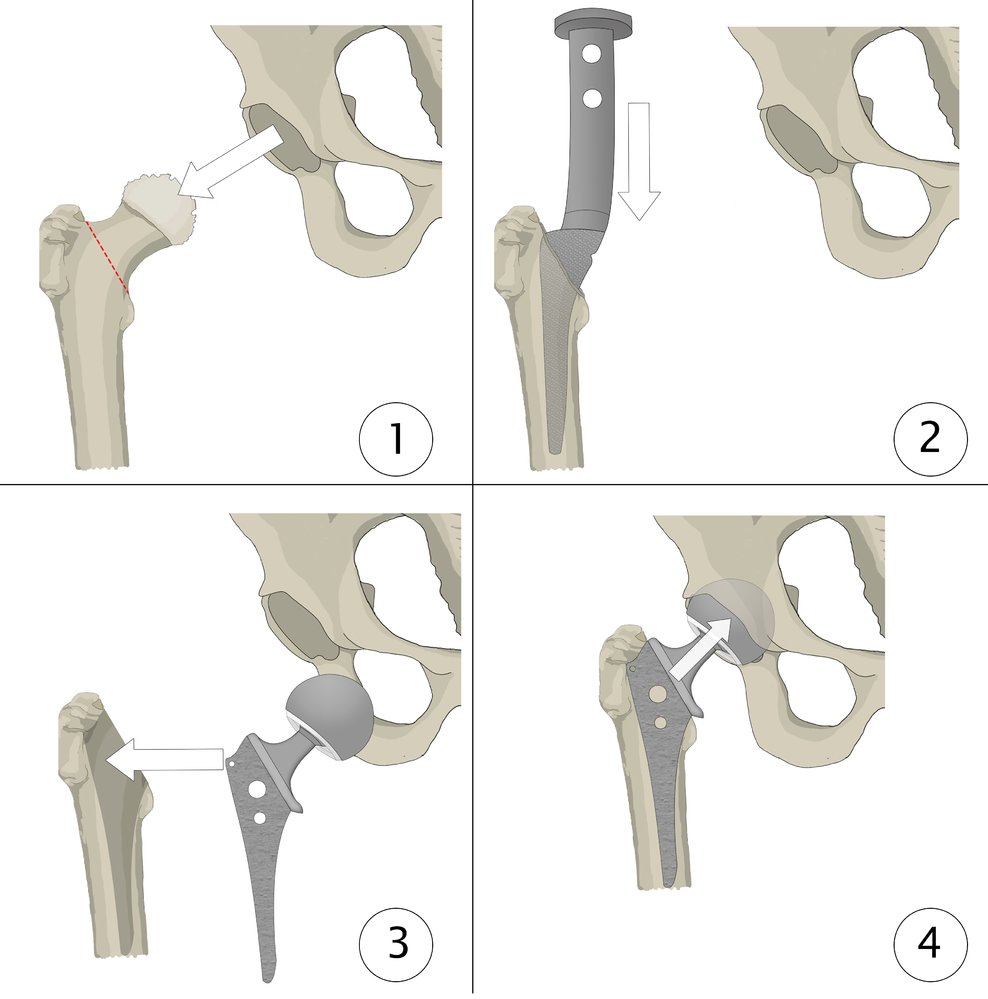
(1) Removal of the damaged femoral head from the acetabulum and resection of the femoral head and neck along the line between the greater and the lesser trochanter (red line)
(2) Enlargement of the medullary cavity of the femur; no changes to the acetabulum
(3) Insertion of the prosthesis stem into the femoral canal
(4) Reduction of the prosthetic head into the acetabulum
© AMBOSS
Special patient groups
Hip fractures in older adults
The following additional considerations apply to older adults with hip fractures (see also “Trauma in older adults”):
-
Diagnostics
- Diagnostics for osteoporosis (e.g., to establish a pretreatment baseline) [26]
- Syncope workup and/or fall risk assessment [27]
- Preoperative cardiac assessment (e.g., echocardiogram, ECG, cardiac biomarkers) based on individual risk [7]
-
Management
- Geriatric assessment
- Bone health optimization and pharmacotherapy for osteoporosis (e.g., bisphosphonates) [28]
- Delirium prevention or treatment of agitation in delirium
- Measures to minimize physical deconditioning
- Postoperative pulmonary rehabilitation (e.g., incentive spirometry) and aspiration precautions to prevent postoperative pneumonia [29]
- Disposition: admission to a comprehensive geriatric service or orthogeriatric service where available [11][19]
- Advance care planning: Consider early, especially in patients with a high frailty scale score.
-
Prognosis [19][30][31]
- 30-day mortality in patients with pulmonary complications (e.g., pneumonia, atelectasis, PE): up to 17% [29]
- 1-year mortality: ∼ 35%
- 50% of patients do not regain prefracture functionality.
Older adults have higher morbidity and mortality following a hip fracture because of coincident frailty and/or other complex medical problems. [19][30][31]
Subtypes and variants
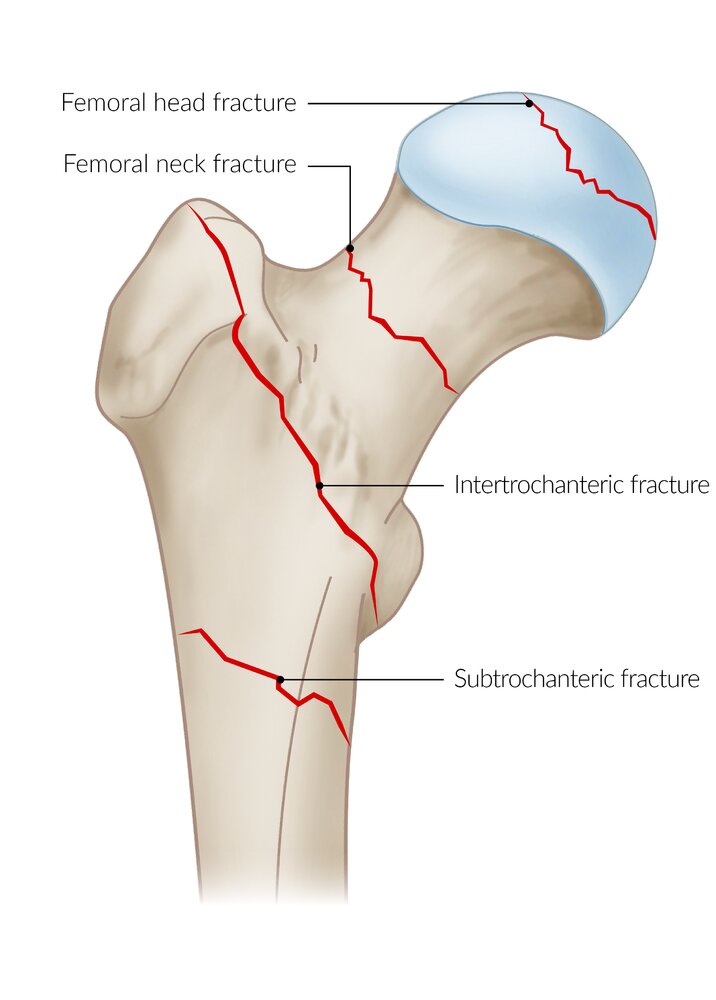
Hip fractures are classified as follows:
-
Intracapsular
- Femoral head
- Femoral neck
-
Extracapsular
- Trochanteric
- Intertrochanteric
- Subtrochanteric


© AMBOSS
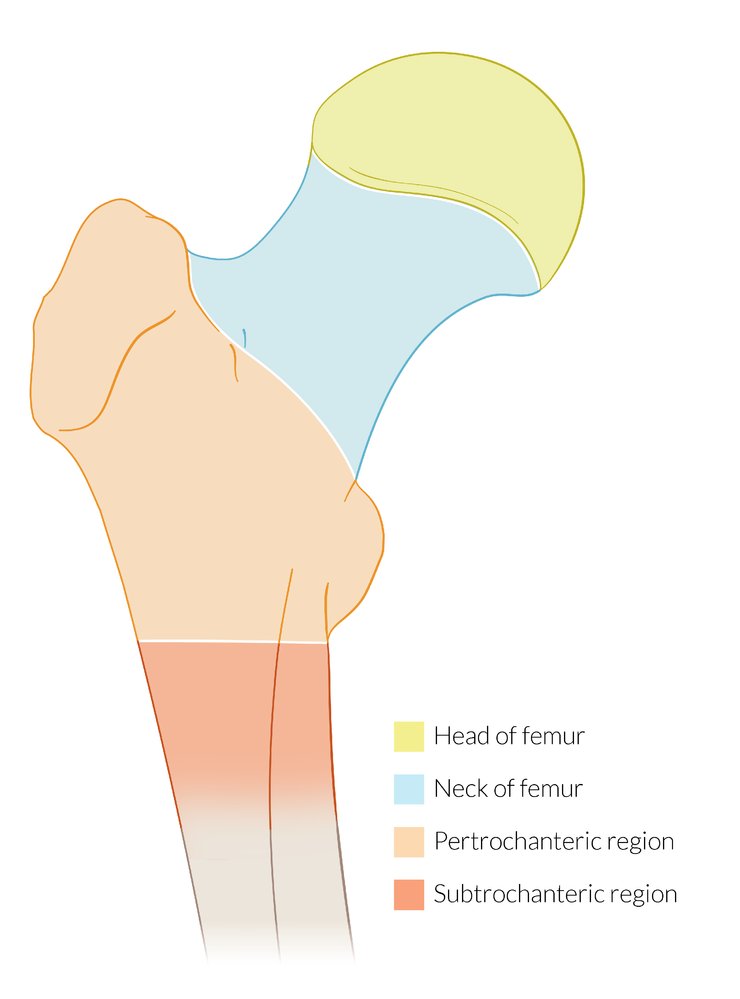
The head and neck of the femur are intracapsular while the pertrochanteric (or trochanteric) and subtrochanteric regions are extracapsular.
Lines: Delbet classification of pediatric prox. femur fractures
© AMBOSS
Femoral head fracture
- Occurrence: uncommon but often associated with a posterior hip dislocation following a dashboard injury
-
Clinical features
- Groin pain
- Local swelling and ecchymosis
-
Diagnostics
- Hip x-ray (AP with internal rotation and lateral view; should include the proximal thigh) : abnormal trabecular pattern, cortical defects, shortening and angulation of the femoral neck [32]
- MRI if findings are unclear or if an occult fracture is suspected
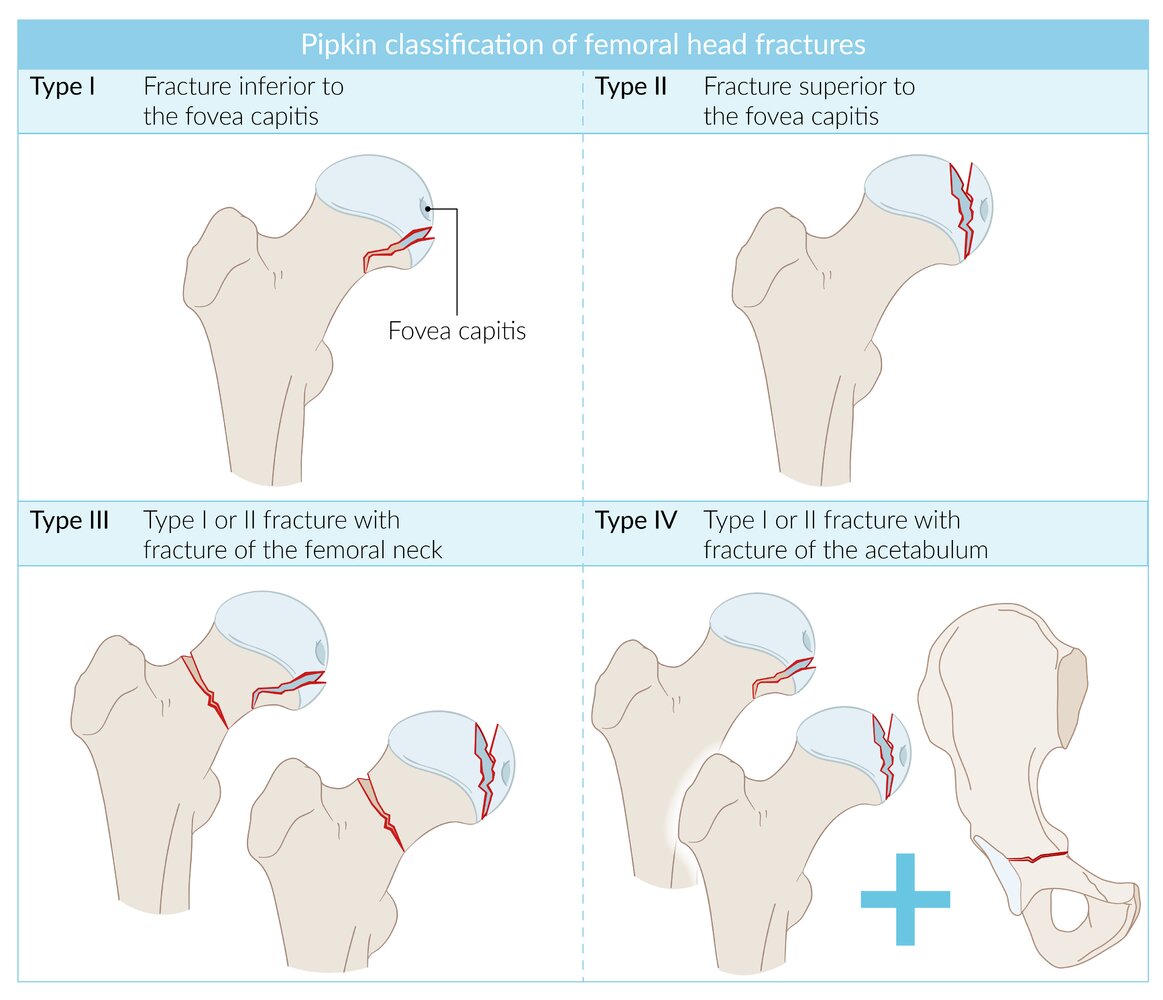
| Pipkin Classification | ||
|---|---|---|
| Description | Treatment after rapid repositioning | |
| Pipkin I |
|
|
| Pipkin II |
|
|
| Pipkin III |
|
|
| Pipkin IV |
|
|
A patient with an MVA dashboard injury may present with a femoral head fracture and hip dislocation.
Watch out for sciatic nerve injury in patients with femoral head fractures.




© AMBOSS
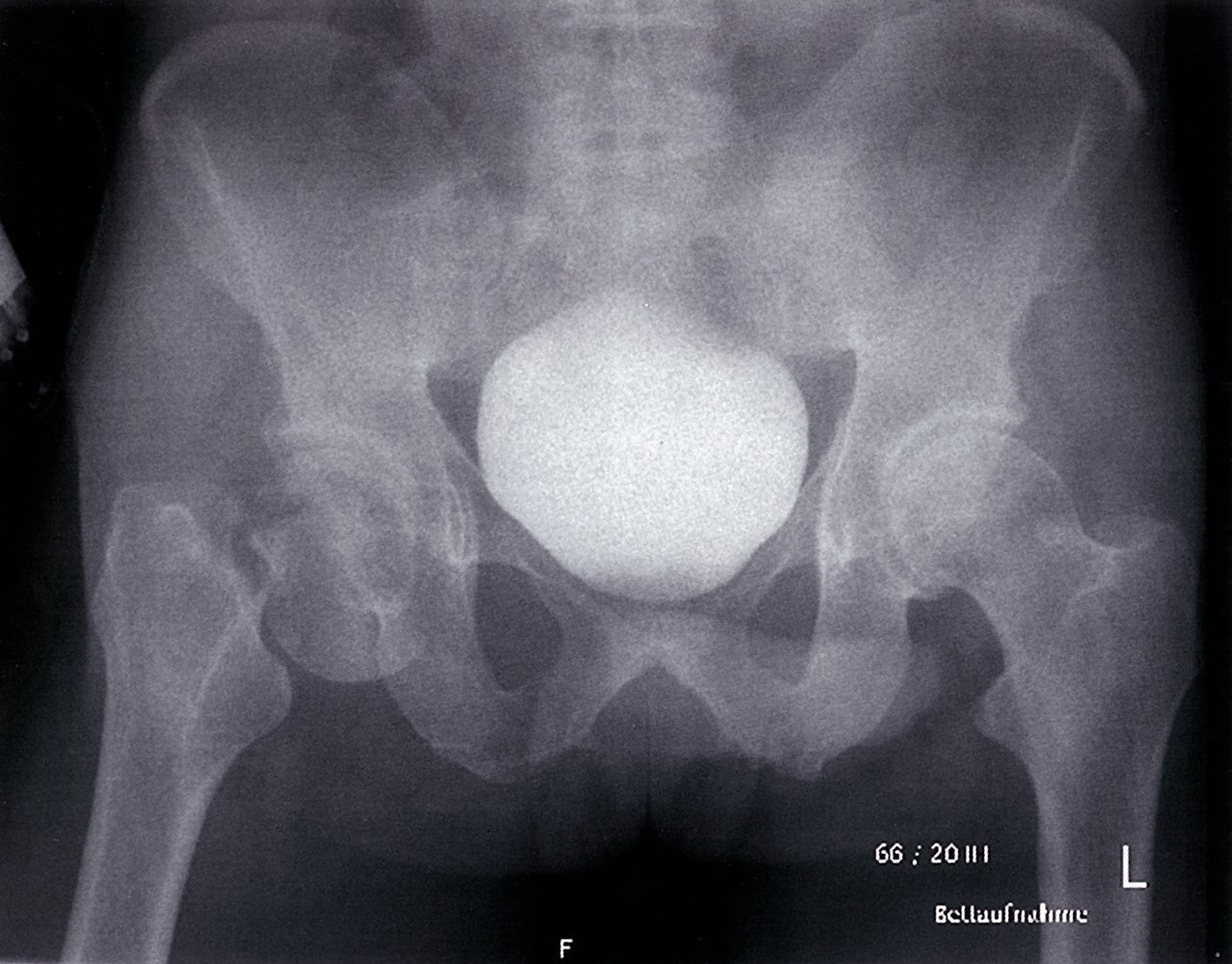
Anteroposterior x-ray of the pelvis: A femoral head fracture (green area and green line) in combination with a medial fracture of the femoral neck (angle 75°, Pauwels' classification) can be seen in this x-ray image. This fracture combination (femoral head fracture and medial fracture of the femoral neck) is categorized as Pipkin III according to the Pipkin classification.
Source: © IMPP
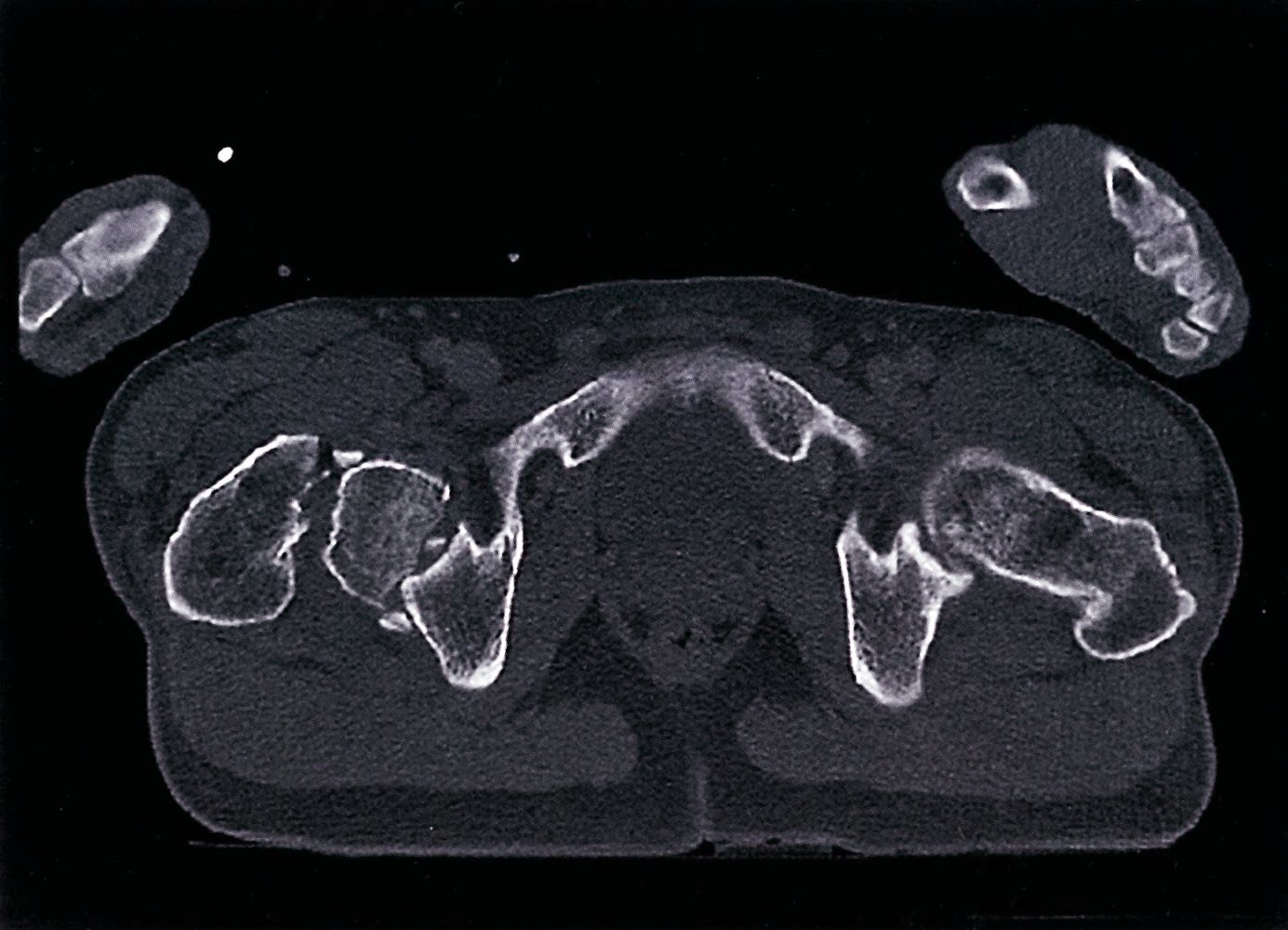
CT pelvis (axial section)
A: Fracture line at neck of femur
B: Fracture line at head of femur and dislocation of the femoral head from the acetabular notch (green overlay)
G: Greater trochanter
A fracture dislocation of the femoral head is classified as Pipkin III.
Source: © IMPP
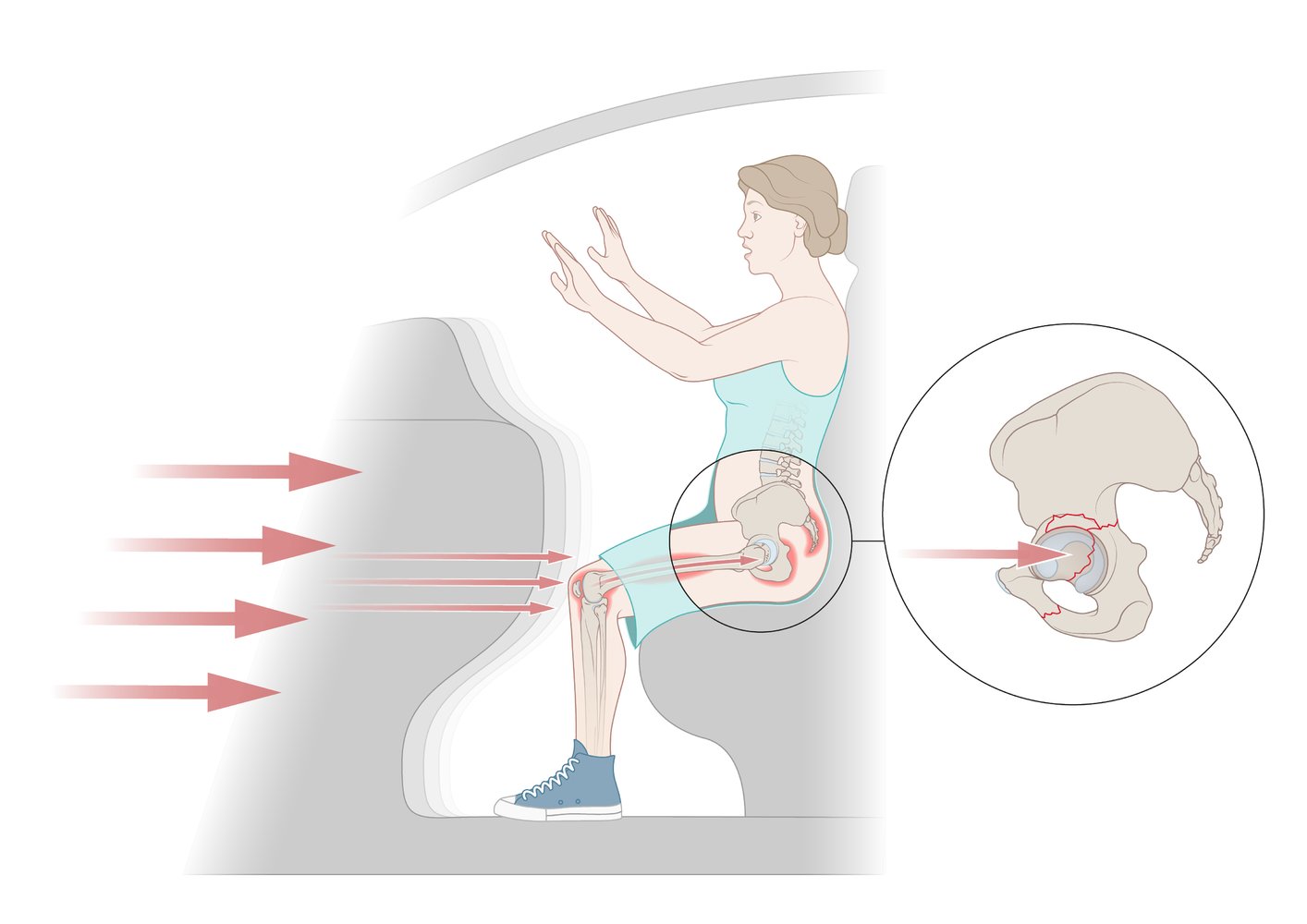
Dashboard injuries occur when a force is directed posteriorly towards an internally rotated, flexed, and adducted hip. Potentially resulting damage includes posterior dislocation of the hip; damage to the posterior cruciate ligament of the knee; fracture of the acetabulum, femoral head, or patella; and sciatic nerve injury.
© AMBOSS
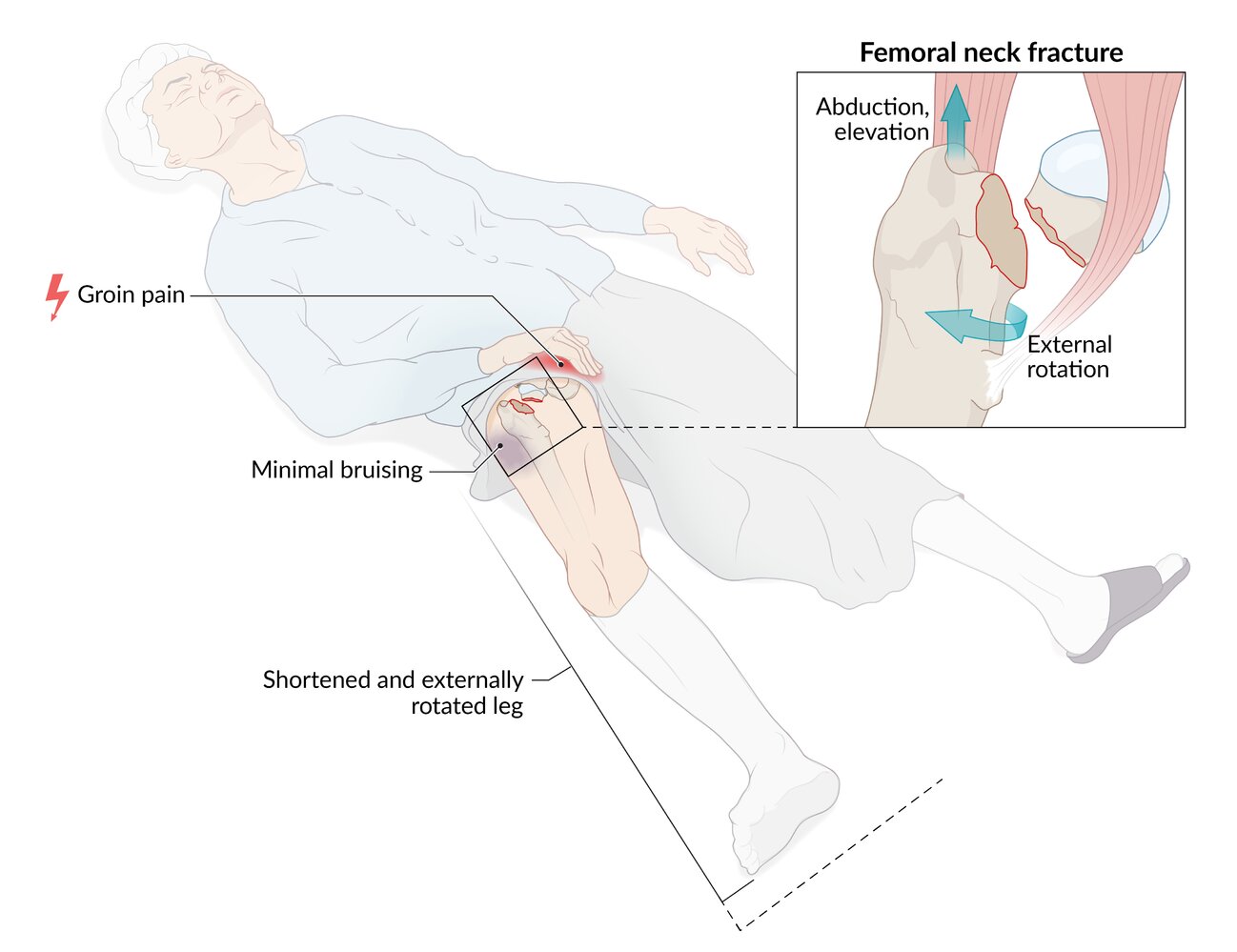
Femoral neck fracture
-
Clinical features
- Groin pain
- Shortened and externally rotated leg
- Minimal bruising
-
Diagnostics
- X-ray (AP and lateral view of the pelvis with internal rotation of the affected limb)
- MRI or bone scan if clinical suspicion is high despite absent findings on x-ray
| Garden Classification | |
|---|---|
| Garden I | Nondisplaced, incomplete, impaction fracture |
| Garden II | Complete, but nondisplaced fracture |
| Garden III | Partially displaced, complete fracture with medial contact of the fracture elements and varus displacement of the femoral head |
| Garden IV | Entirely displaced, complete fracture |
-
Treatment
-
Conservative management
- Indication: stable, nondisplaced fractures, especially abduction fractures , mostly in debilitated patients
- Methods
- Temporary bed rest; or use of crutches followed by mobilization with physical therapy
- Venous thromboembolism prophylaxis [33]
-
Surgery (usually within 72 hours ; ) is indicated for unstable fractures , typically adduction fractures, and fragment dislocation
- For children and young adults
- Attempt preservation of the femoral head
- Early open reduction internal fixation (ORIF) (within 6 hours)
- For older adults: total hip replacement (THR) or hip hemiarthroplasty
- For children and young adults
-
Conservative management



© AMBOSS
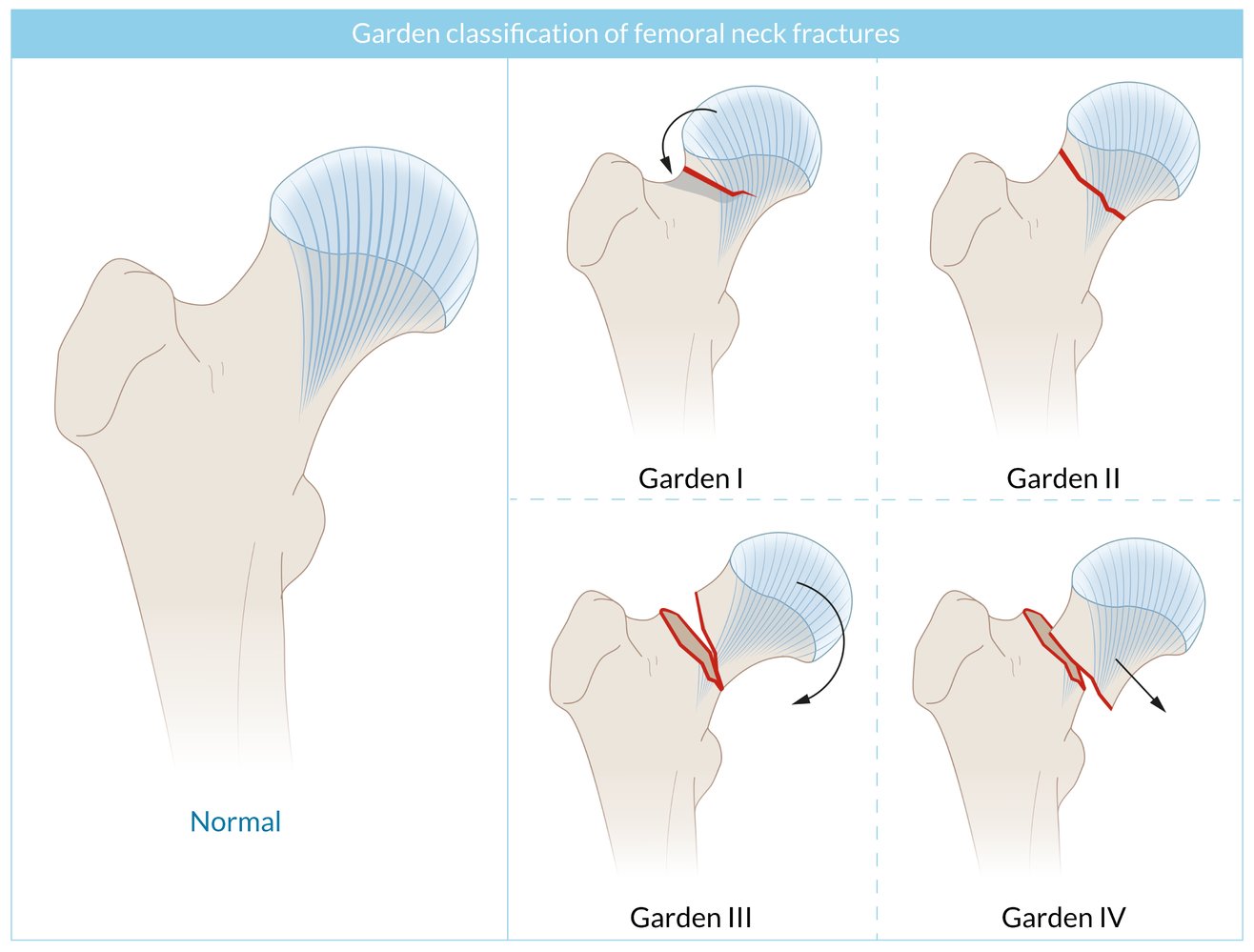
The degree of femoral neck displacement is determined by the course of the trabeculations in the femoral neck and head (depicted here as blue lines; grey area = impaction; red area = line of fracture).
Garden I: nondisplaced, incomplete, impaction fracture with valgus configuration (lateral distortion of the trabeculations)
Garden II: complete, but nondisplaced fracture (disruption of the trabeculations without distortion)
Garden III: complete and partially displaced fracture with medial contact of the fracture elements and varus displacement (medial distortion of the trabeculations)
Garden IV: complete, fully displaced fracture
© AMBOSS
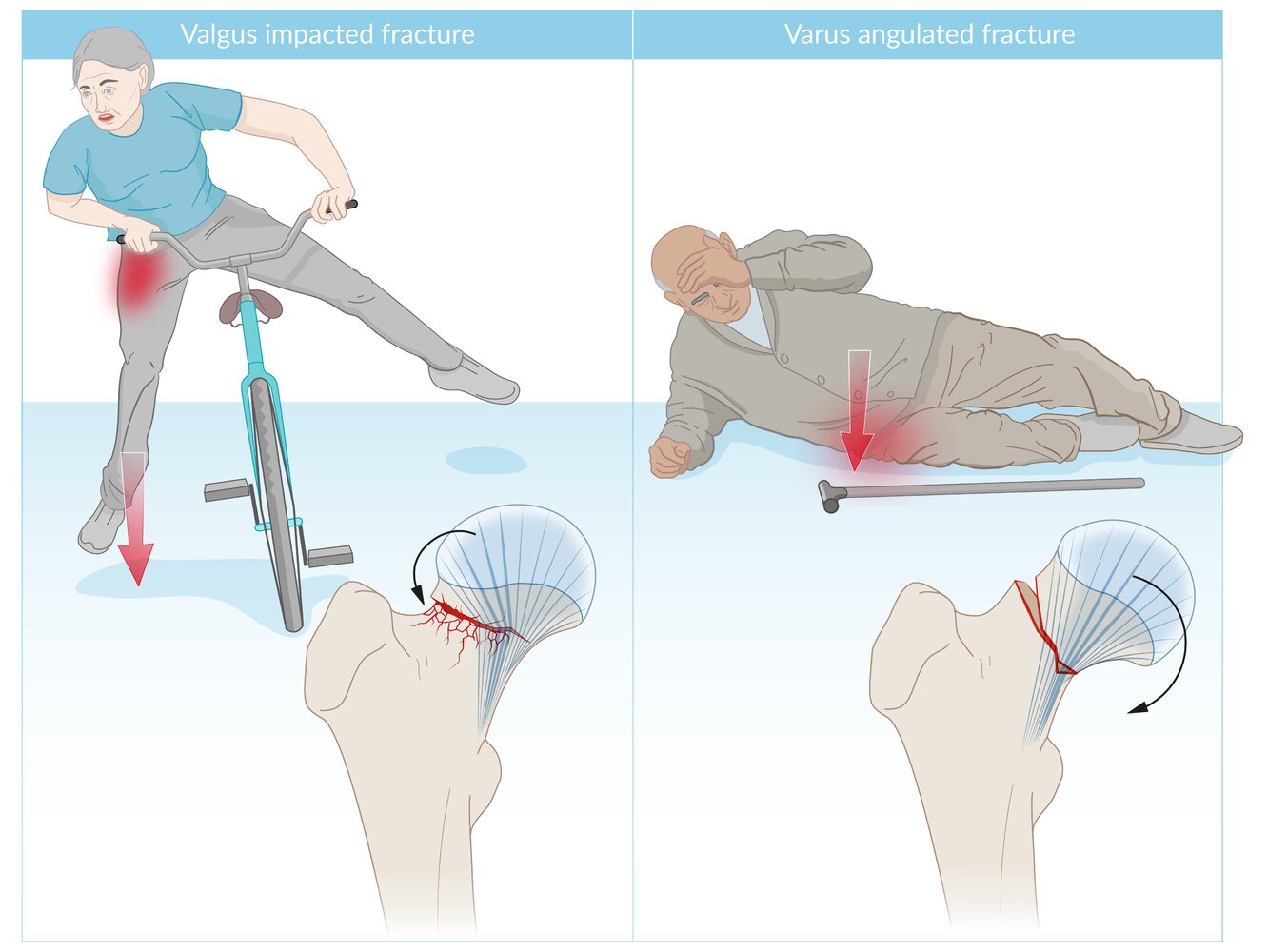
Left: A fall onto the abducted leg may result in an impaction fracture (red lines) with valgus angulation of the femoral head (black arrow) and lateral distortion of the trabeculations (blue lines). This fracture type, sometimes described as an “abduction fracture,” is uncommon and likely to be relatively stable.
Right: A fall sideways with a direct impact on the greater trochanter may result in a partially displaced fracture with varus angulation of the femoral head and medial distortion of the trabeculations. This fracture type, sometimes described as an “adduction fracture,” is more common and likely to be unstable.
© AMBOSS
Three cancellous lag screws were used to stabilize a femoral neck fracture. They are positioned parallel to each other and parallel to the longitudinal axis of the femoral neck. These screws have a thread only at the terminal end, and the thread does not cross the fracture line. Tightening the screws, therefore, compresses the fracture fragments.
© AMBOSS
Trochanteric fractures
-
Etiology
- Greater trochanteric fracture
- Avulsion of the greater trochanter apophysis due to forceful contraction of the gluteus medius and minimus muscles (typically during physical activity)
- Direct trauma to the greater trochanter (e.g., due to a fall onto the hip)
- Lesser trochanteric fracture
- Avulsion of the lesser trochanter apophysis due to forceful contraction of the iliopsoas muscle
- Most commonly seen in physically active young adults, particularly those who participate in high-impact sports such as wrestling
- Greater trochanteric fracture
-
Clinical features
- Greater trochanteric fracture: local pain exacerbated by abduction
- Lesser trochanteric fracture: groin pain, which radiates to the knee or posterior thigh and worsens with hip flexion and rotation
-
Diagnostics
- X-ray showing avulsion of the greater or lesser trochanter
- MRI if a pathological fracture is suspected or in individuals at risk of fracture extension (e.g., patients with osteoporosis)
-
Treatment [12]
- Typically self-limiting and conservative treatment suffices (e.g., no weight-bearing on the affected leg, ice, and physical therapy).
- Surgical repair in fractures with displacement > 1 cm



")
© AMBOSS

A photograph depicting a test for trochanteric pain
The patient is positioned supine and the examiner presses on the lateral hip joint in the region of the greater trochanter. Pain during this test would indicate a positive test.
A positive test may suggest pathology such as trochanteric bursitis or a fracture of the greater trochanter.
© AMBOSS

X-ray right femur (AP view) of an 86-year-old woman who fell from her bed
There is a displaced and angulated pertrochanteric fracture (green overlay) with avulsion of the right lesser trochanter (red overlay) and additional fragments (blue overlay).
Extensive atherosclerosis of the femoral artery is also seen (dotted lines).
Source: © IMPP

X-ray (AP view) of an adolescent athlete
An avulsion fracture of the lesser trochanter of the left femur is displaced superiorly (green overlay). The donor site of the left lesser trochanter shows an irregular contour (arrowheads) in contrast to the smooth contour of the right lesser trochanter.
The lesser trochanter is the insertion site for the iliopsoas muscle.
Source: “Figure 1, in: Conservative Treatment of Avulsion Injuries of the Lesser Trochanter in Adolescent Athletes” by Alexander Volpi,Chelsea Matzko,Daniel Feghhi,Travis Matheney,Srino Bharam, Cureus, licensed under CC BY 4.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).

© AMBOSS
Intertrochanteric fracture
-
Clinical features
- Hip pain and swelling
- Shortened and externally rotated leg
- Significant ecchymosis
- Often associated with other injuries (e.g. other extremity fractures)
-
Diagnostics
- X-ray (AP view with maximal internal rotation and lateral view): proximal femur fracture between the greater and lesser trochanters
- MRI if a pathological fracture is suspected
-
Treatment
- Nonsurgical approach for high risk patients
-
Surgery
- Dynamic hip screw (DHS) for stable fractures
- Intramedullary nail (Gamma nail) for stable or unstable fractures, fractures extending into the subtrochanteric region, or reverse oblique fractures
- Arthroplasty may be considered for comminuted fractures, pathological fractures, or if other surgical modalities fail.

")

X-ray right hip (AP view)
A comminuted intertrochanteric fracture (fragments indicated by green, white, and yellow overlay) of the right femur is accompanied by superior displacement of the femoral shaft and distraction (indicated by red dashed lines and arrows) of the main fracture fragments.
Source: “Late Presentation of an Iatrogenic Pseudoaneurysm of the Profunda Femoris Artery following Intramedullary Nailing” by Kira Vande Voorde, Jan Dauwe, and Jan Van Oost, Hindawi, licensed under CC BY 4.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).

AP radiograph of the right hip: Because of the low quality, the structure of the greater trochanter (T) is poorly defined; the dotted line shows a possible contour. A radiolucent fracture gap is located in between the greater and lesser trochanter and at the base of the lesser trochanter (t), possibly indicating an intertrochanteric femoral fracture.
Source: © IMPP Further notes: Pending reply from MST
A dynamic hip screw (sliding hip screw) is an orthopedic implant used in the fixation of hip fractures of the intertrochanteric or lower femoral neck region.
The DHS consists of a sliding lag screw, a stabilizing side plate with a barrel (through which the lag screw is placed) and cortical screws for the fixation of the side plate. Movement of the lag screw along the barrel of the stabilizing plate allows for dynamic compression of the fracture as the patient bears weight (which aids bone healing). If there is rotational instability, an additional antirotation screw may be placed.
© AMBOSS
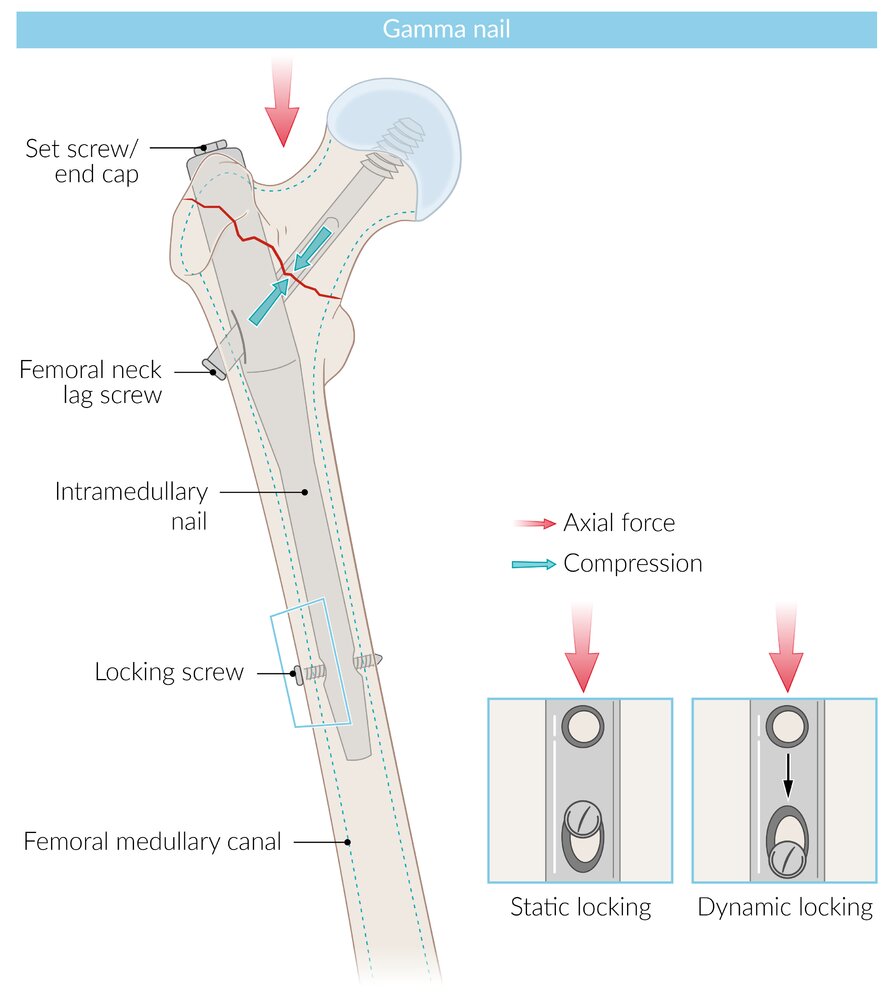
Osteosynthesis of an intertrochanteric fracture using a gamma locking nail: An intramedullary nail is placed directly into the bone marrow through the greater trochanter and held in position using a distal fixation screw. A lag screw is then placed through the nail, which enters the neck and head of the femur. This nail also allows for compression (weight-bearing) of the fracture site. The combination of intramedullary nail and lag screw resembles the Greek letter "γ" (gamma), which is why it is called a gamma locking nail.
© AMBOSS

X-ray of the right hip (AP view)
A bipolar hemiarthroplasty with a cemented femoral stem (green overlay) can be seen. There is no evidence of loosening, fracture, or bone resorption.
Source: © IMPP
Subtrochanteric fracture
-
Clinical features
- Hip pain with swelling
- Shortened and externally rotated leg
- Significant ecchymosis
-
Diagnostics [12]
- X-ray : fracture between the lesser trochanter up to 5cm below that (distally)
- MRI if a pathological fracture is suspected
-
Treatment
- Consider conservative approach (e.g., traction) in surgically unstable patients
-
Surgery is indicated in displaced/nondisplaced fractures in adults, especially if associated with multiple trauma, an open fracture, or pathological fractures
- Long intramedullary nail with a lag screw
- Locking plate may be considered for complicated fractures (e.g., pre-existing femoral deformity, associated femoral neck fracture)
This CT reconstruction shows a dorsal view of the pelvis and femurs with a type C subtrochanteric fracture of the left femur.
Source: © IMPP
Hip fracture-dislocation
General principles
- Hip fractures, especially fractures of the femoral head, can be associated with a hip dislocation.
- Hip fracture-dislocations require urgent orthopedic intervention; the decision to perform an urgent closed reduction or open reduction depends on fracture and dislocation characteristics.
Hip fracture-dislocations are associated with a high risk of osteonecrosis of the femoral head.
Overview of hip dislocation
Hip dislocation can occur in isolation or be associated with pelvic fractures (e.g., acetabular fractures) and/or hip fractures.
| Posterior vs. anterior hip dislocation | ||
|---|---|---|
| Posterior hip dislocation | Anterior hip dislocation | |
| Epidemiology |
|
|
| Etiology |
|
|
| Clinical features |
|
|
|
|
|
| Diagnostics |
|
|
| Treatment |
|
|
| Complications |
|
|
Complications
- Osteonecrosis of the femoral head
- Thromboembolism
- Infection
- Chronic pain and posttraumatic arthritis
- Nonunion
- Dislocation
- Nerve injury, e.g., sciatic nerve injury
Thrombolytic therapy reduces the risk of deep vein thrombosis in patients with hip fractures.


We list the most important complications. The selection is not exhaustive.
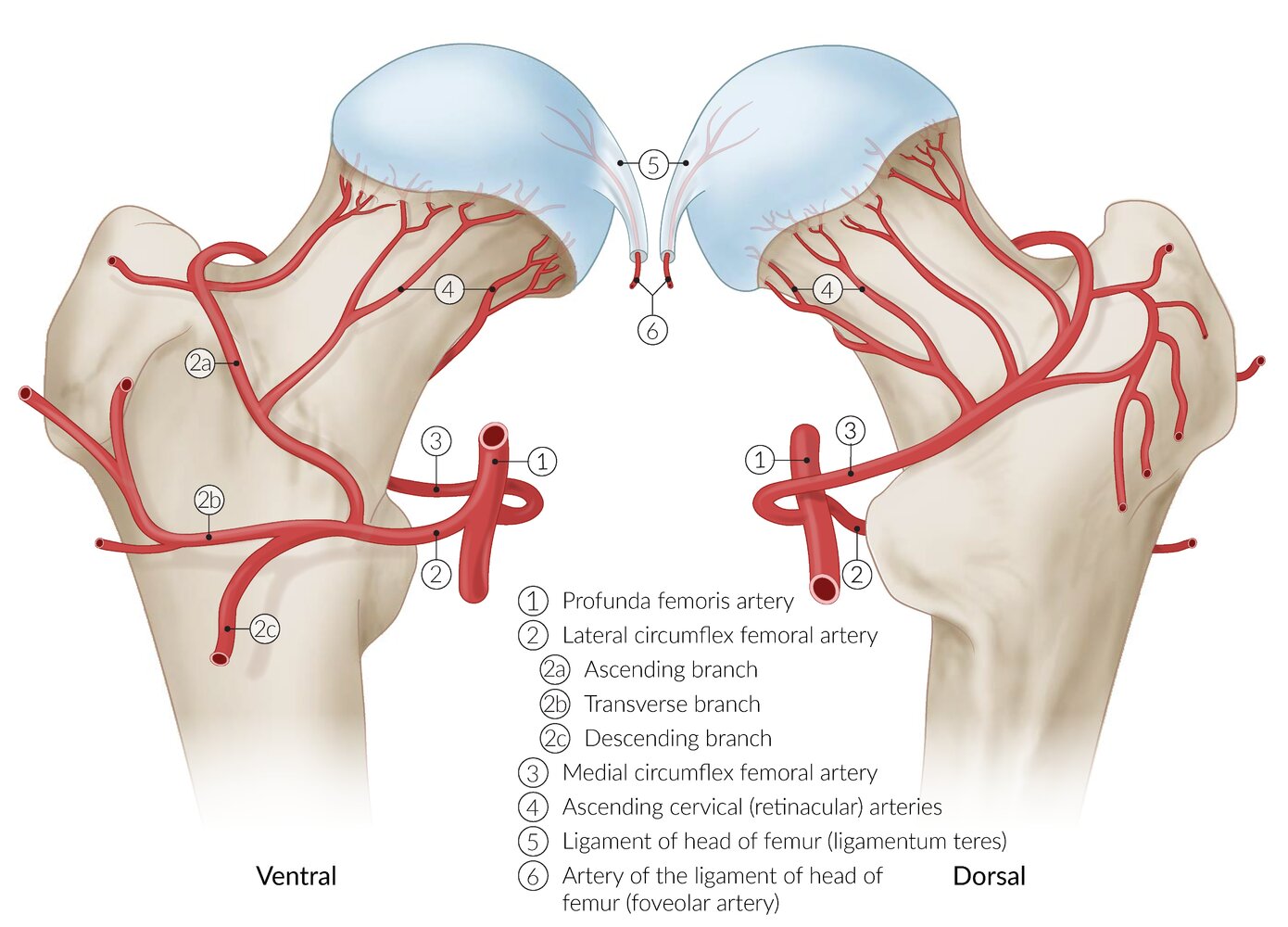
For arterial supply of the femoral head and neck, the profunda femoris artery gives off two vessels, as shown here: first, the medial circumflex femoral artery and, second, the lateral circumflex femoral artery.
Possible complication of a hip fractures: rupture of arteries → reduced arterial supply to the femoral head/neck → aseptic hip necrosis
© AMBOSS

X-ray pelvis (AP view)
Abnormal healing has occurred at the site of a fracture through the left femoral neck, with development of a pseudarthrosis. The fracture line (green overlay) remains visible, and sclerosis (red overlay) has developed along its margins. The femoral neck has widened. There are also degenerative changes, with medial joint space narrowing (indicated by arrowheads).
Source: © IMPP
Prognosis
- Intracapsular fractures (e.g., femoral head and neck fractures) have an increased rate of nonunion which leads to AVN
- Intertrochanteric fractures have a good prognosis following surgery
- Subtrochanteric fractures have a high rate of implant failure
Hip fractures have a high rate of associated morbidity and mortality in older adults.
Prevention
- Fall risk assessment, for example with the Tinetti-Test, which is used to evaluate a patient's gait and balance
- Implementation of fall prevention strategies
- Early preventative efforts such as fall training, physical therapy, removal of tripping hazards, and appropriate shoes
- Osteoporosis prophylaxis
External Resources
References
- LeBlanc KE, Muncie HL Jr, LeBlanc LL. "Hip fracture: diagnosis, treatment, and secondary prevention". Am Fam Physician. 89(12). :945-51. (2014)
- Lauritzen JB, McNair PA, Lund B. "Risk factors for hip fractures. A review.". Dan Med Bull. 40(4). :479-485. (1993)
- Walls R, Hockberger R, Gausche-Hill M, Erickson TB, Wilcox SR. "Rosen's Emergency Medicine 10th edition- Concepts and Clinical Practice E-Book". Elsevier Health Sciences. (2022). ISBN: 9780323757904
- Haj-Mirzaian A, Eng J, Khorasani R, et al. "Use of Advanced Imaging for Radiographically Occult Hip Fracture in Elderly Patients: A Systematic Review and Meta-Analysis". Radiology. 296(3). :521-531. (2020)
- Cannon J, Silvestri S, Munro M. "Imaging Choices in Occult Hip Fracture". J Emerg Med. 37(2). :144-152. (2009)
- Dominguez S, Liu P, Roberts C, Mandell M, Richman PB. "Prevalence of Traumatic Hip and Pelvic Fractures in Patients with Suspected Hip Fracture and Negative Initial Standard Radiographs-A Study of Emergency Department Patients". Acad Emerg Med. 12(4). :366-369. (2005)
- Smith GH, Tsang J, Molyneux SG, White TO. "The hidden blood loss after hip fracture". Injury. 42(2). :133-135. (2011)
- Porter CJ, Moppett IK, Juurlink I, et al. "Acute and chronic kidney disease in elderly patients with hip fracture: prevalence, risk factors and outcome with development and validation of a risk prediction model for acute kidney injury". BMC Nephrol. 18(1). (2017)
- Arshi A, Lai WC, Iglesias BC, et al. "Blood transfusion rates and predictors following geriatric hip fracture surgery". Hip Int. 31(2). :272-279. (2020)
- "American Academy of Orthopaedic Surgeons Management of Hip Fractures in Older Adults Evidence-Based Clinical Practice Guideline". https://www.aaos.org/hipfxcpg. [2021-12-03]
- Bhandari M, Swiontkowski M. "Management of Acute Hip Fracture". N Engl J Med. 377(21). :2053-2062. (2017)
- Ottesen TD, McLynn RP, Galivanche AR, et al. "Increased complications in geriatric patients with a fracture of the hip whose postoperative weight-bearing is restricted". Bone Joint J. 100-B(10). :1377-1384. (2018)
- Ackermann L, Schwenk ES, Lev Y, Weitz H. "Update on medical management of acute hip fracture". Cleve Clin J Med. 88(4). :237-247. (2021)
- Liu VX, Rosas E, Hwang J, et al. "Enhanced Recovery After Surgery Program Implementation in 2 Surgical Populations in an Integrated Health Care Delivery System". JAMA Surgery. 152(7). :e171032. (2017)
- Liu S yang, Li C, Zhang P xun. "Enhanced recovery after surgery for hip fractures: a systematic review and meta-analysis". Perioper Med. 10(1). (2021)
- van de Ree CLP, De Jongh MAC, Peeters CMM, et al. "Hip Fractures in Elderly People: Surgery or No Surgery? A Systematic Review and Meta-Analysis". Geriatr Orthop Surg Rehabili. 8(3). :173-180. (2017)
- Chlebeck JD, Birch CE, Blankstein M, et al. "Nonoperative Geriatric Hip Fracture Treatment Is Associated With Increased Mortality: A Matched Cohort Study". J Orthop Trauma. 33(7). :346-350. (2019)
- Jain R, Basinski A, Kreder HJ. "Nonoperative treatment of hip fractures". Int Orthop. 27(1). :11-17. (2003)
- Gilligan I, Chandraphak S, Mahakkanukrauh P. "Femoral neck-shaft angle in humans: variation relating to climate, clothing, lifestyle, sex, age and side". J Anat. 223(2). :133-151. (2013)
- "Management of hip fractures in the elderly". http://www.orthoguidelines.org/topic?id=1017. [2014-09-05]
- Sanzone AG. "Current Challenges in Pain Management in Hip Fracture Patients". J Orthop Trauma. 30(Supplement 1). :S1-S5. (2016)
- Cowan R, Lim JH, Ong T, Kumar A, Sahota O. "The Challenges of Anaesthesia and Pain Relief in Hip Fracture Care". Drugs Aging. 34(1). :1-11. (2016)
- Guay J, Parker MJ, Griffiths R, Kopp SL. "Peripheral Nerve Blocks for Hip Fractures". Anesth Analg. 126(5). :1695-1704. (2018)
- Ritcey B, Pageau P, Woo MY, Perry JJ. "Regional Nerve Blocks For Hip and Femoral Neck Fractures in the Emergency Department: A Systematic Review". CJEM. 18(1). :37-47. (2015)
- Carson JL, Terrin ML, Noveck H, et al. "Liberal or Restrictive Transfusion in High-Risk Patients after Hip Surgery". N Engl J Med. 365(26). :2453-2462. (2011)
- Falck-ytter Y, Francis CW, Johanson NA, et al. "Prevention of VTE in orthopedic surgery patients: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines". Chest. 141(Suppl 2). :e278S-325S. (2012)
- Prestmo A, Hagen G, Sletvold O, et al. "Comprehensive geriatric care for patients with hip fractures: a prospective, randomised, controlled trial". Lancet. 385(9978). :1623-1633. (2015)
- Rebolledo BJ, Unnanuntana A, Lane JM. "A Comprehensive Approach to Fragility Fractures". J Orthop Trauma. 25(9). :566-573. (2011)
- Parker M, Johansen A. "Hip fracture". BMJ. 333(7557). :27-30. (2006)
- Conley RB, Adib G, Adler RA, et al. "Secondary Fracture Prevention: Consensus Clinical Recommendations from a Multistakeholder Coalition". J Bone Miner Res. 35(1). :36-52. (2019)
- Chang SC, Lai JI, Lu MC, et al. "Reduction in the incidence of pneumonia in elderly patients after hip fracture surgery". Medicine. 97(33). :e11845. (2018)
- Tajeu GS, Delzell E, Smith W, et al. "Death, Debility, and Destitution Following Hip Fracture". J Gerontol A Biol Sci Med Sci. 69A(3). :346-353. (2013)
- Riemen AHK, Hutchison JD. "The multidisciplinary management of hip fractures in older patients". Orthop Trauma. 30(2). :117-122. (2016)