Summary
Hodgkin lymphoma (HL) is a malignant lymphoma of B-cell origin. Incidence follows a bimodal age distribution, with peaks in the third, and sixth to eighth decades of life. The WHO classifies HL as either classical HL (CHL) or nodular lymphocyte predominant HL (NLPHL). Most patients (95%) with HL have CHL, which includes four histological subtypes: nodular sclerosing CHL (most common), mixed cellularity CHL, lymphocyte-rich CHL, and lymphocyte-depleted CHL. Risk factors for HL include Epstein-Barr virus (EBV) infection and immunodeficiency (e.g., due to HIV infection). Clinical features of HL include painless lymphadenopathy, hepatosplenomegaly, and B symptoms. Pel-Ebstein fevers and alcohol-induced pain in affected lymph nodes are rare but specific features of HL. Excisional biopsy of an affected lymph node or extranodal site is required to confirm the diagnosis; Hodgkin cells and Reed-Sternberg cells are present in CHL and popcorn cells are present in NLPHL. Staging is performed using the Lugano classification, which incorporates histopathology results, the presence of B symptoms, and PET-CT scan findings. Additional prognostic factors are used for risk stratification to guide treatment. Typically, limited-stage HL is treated with chemotherapy and radiation therapy, while advanced-stage HL is treated with chemotherapy alone. Overall, the prognosis is good with treatment. Patients require ongoing management for HL to monitor for disease recurrence and treatment-related complications (e.g., second cancers, cardiovascular disorders).
Epidemiology
-
Incidence
- 2–3/100 000 per year [1]
- Subtype variance with age (see “Pathology” below)
- Young adults: nodular sclerosing HL
- Elderly adults: mixed-cellularity HL
-
Age: bimodal distribution [2]
- 1st peak: 25–30 years
- 2nd peak: 50–70 years
-
Sex: ♂ > ♀ [2]
- Male predominance, especially in pediatric cases
- Exception: ♀ = ♂ in nodular sclerosing HL (most common type)
Epidemiological data refers to the US, unless otherwise specified.
Etiology
The exact causes are unknown, but several risk factors have been associated with HL. [3][4]
- Strong association with Epstein-Barr virus (EBV)
- Immunodeficiency: e.g., organ or cell transplantation, immunosuppressants, HIV infection , chemotherapy
- Autoimmune diseases (e.g., rheumatoid arthritis, sarcoidosis)
Clinical features
-
Painless lymphadenopathy:
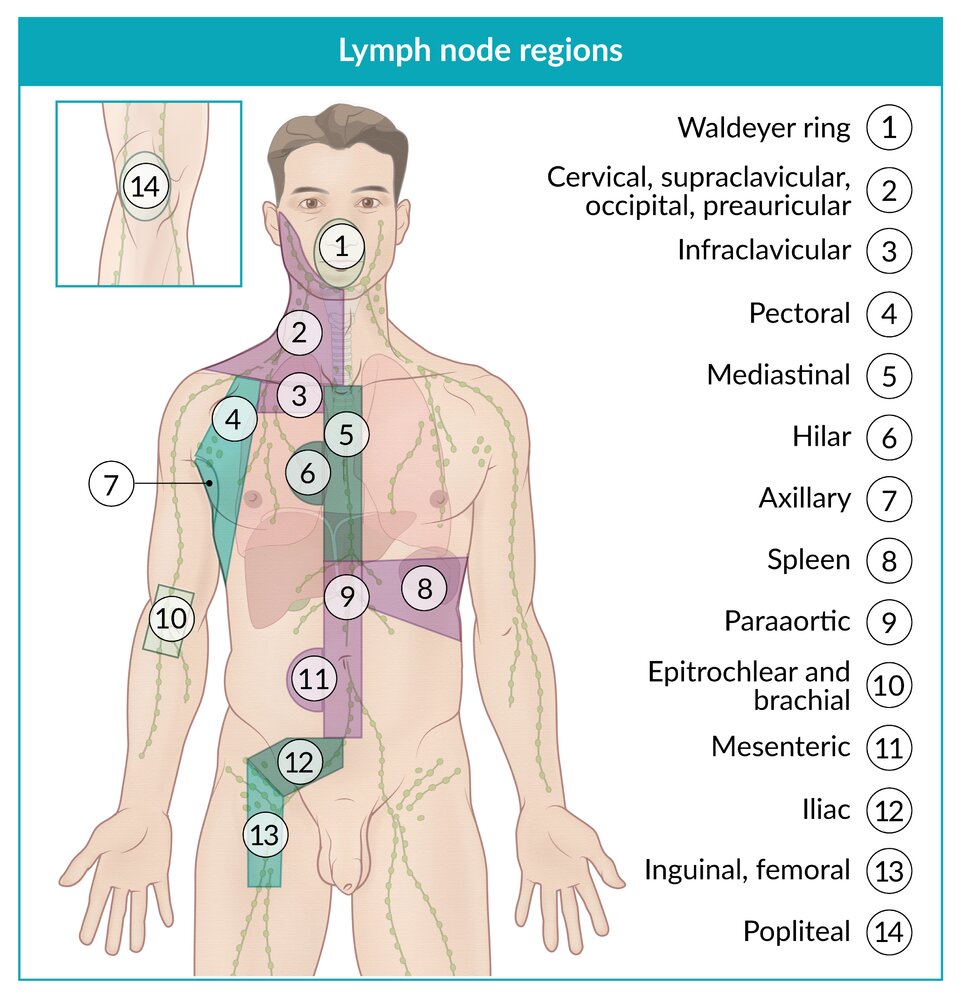
- First develops in a single group of lymph nodes; : typically cervical; , supraclavicular, or mediastinal lymph nodes [5][6][7]
- Spreads contiguously through the lymphatic system: cervical nodes → supraclavicular lymph nodes → axillary nodes → inguinal nodes [8]
- Splenomegaly or hepatomegaly [9]
-
B symptoms [10]
- Night sweats, weight loss > 10% in the past 6 months, fever > 38.0°C (> 100.4°F)
- Can occur in a variety of diseases (see “Differential diagnosis of B symptoms” below)
- In the case of confirmed HL, the presence of a single B symptom suffices for a positive diagnosis of B symptoms.
- Pel-Ebstein fever: intermittent fever with periods of high temperature for 1–2 weeks, followed by afebrile periods for 1–2 weeks; relatively rare but very specific for HL
- Alcohol-induced pain: pain in involved lymph nodes after ingestion of alcohol; relatively rare but highly specific for HL
- Pruritus: focal or generalized


© AMBOSS
© AMBOSS
Diagnosis
- Biopsy is required to confirm the diagnosis of HL in patients with unexplained lymphadenopathy with or without B symptoms.
- Once the diagnosis is confirmed, further studies, including PET-CT, are required for staging of HL.
Initial studies
Laboratory studies and imaging are not required for diagnosis but are commonly performed for the evaluation of lymphadenopathy and B symptoms.
Laboratory studies
-
CBC with differential [6]
- Elevated or decreased WBC count [11]
- Anemia
- Eosinophilia
- Thrombocytosis or thrombocytopenia
-
CMP
- Elevated transaminases and/or hyperbilirubinemia [12][13]
- Elevated alkaline phosphatase [12]
- Hypoalbuminemia [11]
- Hypercalcemia (uncommon) due to paraneoplastic production of 1,25-dihydroxyvitamin D [12][14]
- ESR: elevated [6][12]
- LDH: elevated [12]
Imaging
- Ultrasound or CT scan: Consider in individuals with palpable lymphadenopathy and/or hepatosplenomegaly.
- CXR: Consider in individuals with generalized lymphadenopathy to evaluate for mediastinal lymphadenopathy.
Anemia, leukocytosis, leukopenia, elevated ESR, elevated LDH, and hypoalbuminemia are all poor prognostic factors.
Confirmatory biopsy [6][8][15]
-
Modalities
- Gold standard: excisional biopsy of an involved lymph node or extranodal site
- Alternative: core needle biopsy
-
Findings
- Hodgkin cells and Reed-Sternberg cells: CHL
- Popcorn cells: NLPHL
Excisional biopsy is the gold standard for diagnosing HL. [8]
Fine-needle aspiration is not recommended for suspected HL, as it cannot obtain sufficient tissue. [6][12]




CT chest (with contrast; axial plane) of a patient with Hodgkin lymphoma
A large anterior mediastinal soft tissue mass (green overlay) with surface lobulation and mild contrast enhancement is visible. It is bounded anteriorly by the thoracic wall and posteriorly by the ascending aorta (AA) and superior vena cava (SVC). The left brachiocephalic vein (LBCV) is encased. A cluster of lymph nodes (included in green overlay) can be seen between the aorta and the carina.
The broad histopathological spectrum of mediastinal masses includes both benign and malignant conditions. Most masses (e.g., thymoma, teratoma, thyroid disease, lymphoma) involve the anterior compartment.
AV: azygos vein; DA: descending aorta; LMB: left main bronchus; LPA: left pulmonary artery; RMB: right main bronchus
Source: © IMPP
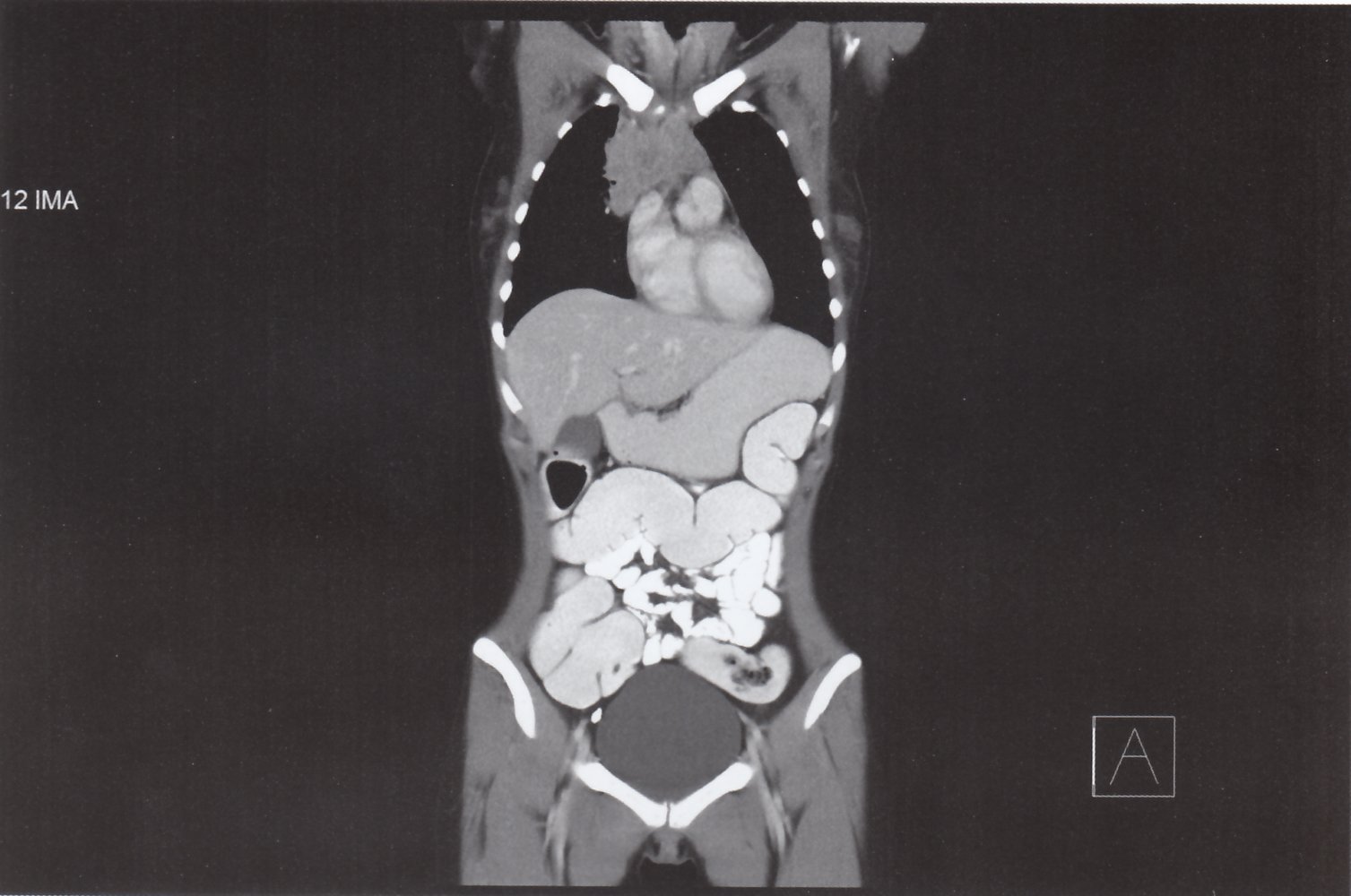
CT scan chest, abdomen, and pelvis (with contrast; coronal plane) of a patient with Hodgkin lymphoma
A large anterior mediastinal soft tissue mass (green overlay) with surface lobulation and mild contrast enhancement is visible.
LV: left ventricle; PT: pulmonary trunk; RA: right atrium; RV: right ventricle
Source: © IMPP
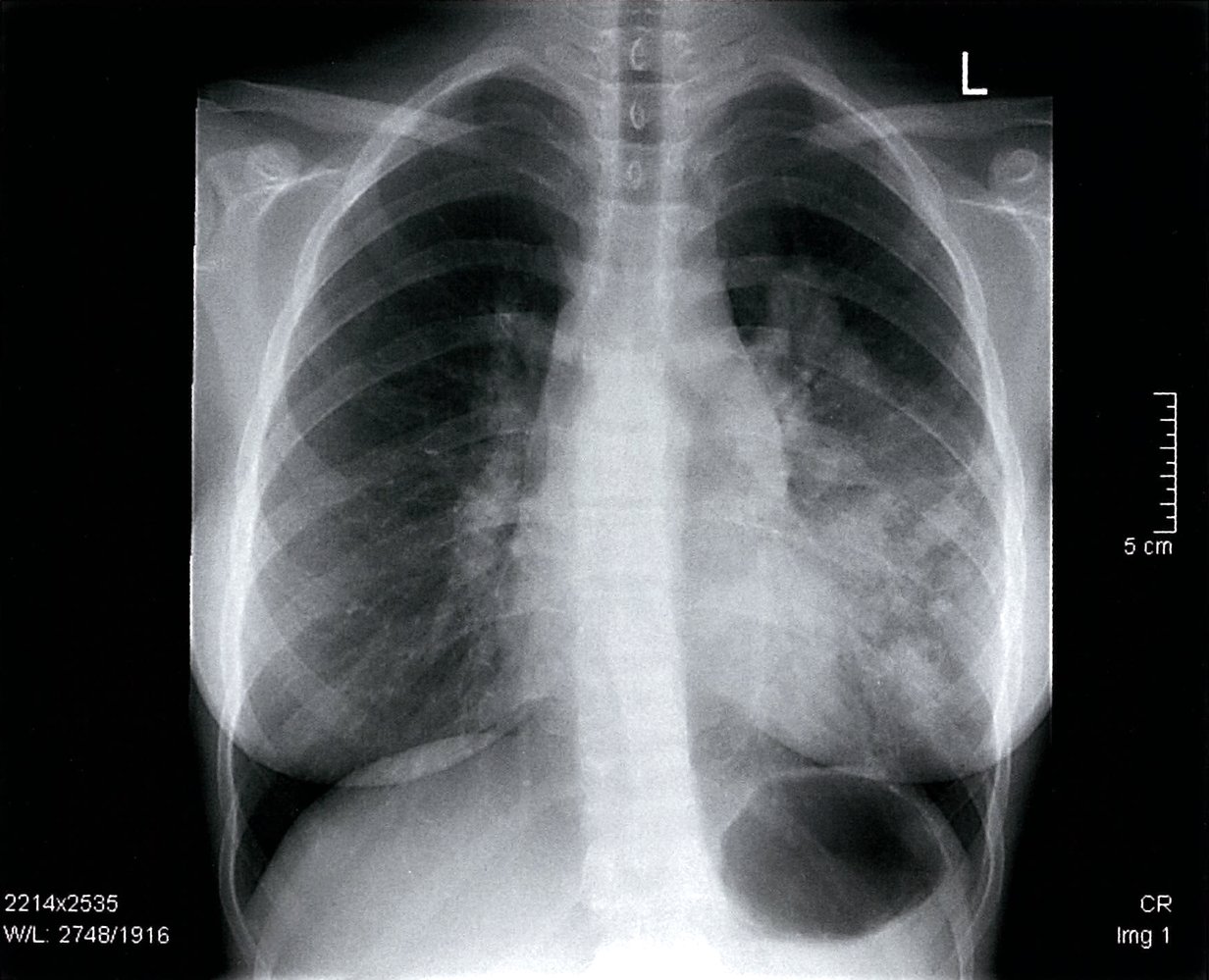
Chest x-ray (AP view)
Hilar and left pulmonary nodular shadows are visible (green overlay). There is a discrete widening of the superior mediastinum with a masked aortic arch (hatched green overlay).
These findings are consistent with malignant lymphoma with mediastinal, hilar, and pulmonary involvement.
Source: © IMPP
Differential diagnoses
Differential diagnoses of B symptoms
- Non-Hodgkin lymphomas, Hodgkin lymphomas
- Other hematopoietic malignancies (e.g., CML, ALL)
- Solid tumors
- Tuberculosis
- HIV
Hodgkin vs. non-Hodgkin lymphoma
| Hodgkin lymphoma vs. non-Hodgkin lymphoma | ||
|---|---|---|
| Feature | Hodgkin lymphoma | Non-Hodgkin lymphoma |
| Age distribution |
|
|
| Etiology |
|
|
| Lymph node involvement |
|
|
| Histology |
|
|
| Five-year survival rate |
|
|
Other differential diagnoses
- “Differential diagnoses of lymphadenopathy”
- “Differential diagnoses of granulomatous disease”
The differential diagnoses listed here are not exhaustive.
Pathology
-
Reed-Sternberg cells (RSCs)
- Tumor cells that are pathognomonic of HL
- Originate from B cells
- Large cells with binuclear/bilobed nuclei with dark centers of chromatin and pale halos, which result in an owl-eye appearance on histopathologic examination.
- CD15/CD30-positive
- Hodgkin cells: mononuclear, malignant B lymphocytes
- Inflammatory background containing the following cell types in varying numbers: lymphocytes, neutrophils, eosinophils, macrophages/histiocytes, plasma cells, and fibroblasts
- Granuloma formation






Reed-Sternberg cells are bi(2)nucleate with CD15/CD30 positivity. To recall the cell markers, remember that 2 x 15 = 30.
| Histological classification of Hodgkin lymphoma (WHO) | ||||
|---|---|---|---|---|
| Classification | Subtype | Characteristics | Prognosis | Pathology |
| Classical Hodgkin lymphoma (95%) | Nodular sclerosing classical HL (NSHL) |
|
|
|
| Mixed-cellularity classical HL (MCHL) |
|
|
|
|
| Lymphocyte-rich classical HL (LRHL) |
|
|
|
|
| Lymphocyte-depleted classical HL (LDHL) |
|
|
|
|
| Lymphocyte predominant Hodgkin lymphoma (5%) | Nodular lymphocyte predominant HL (NLPHL) |
|
|
|


")
")
")
Microscopic image of the right supraclavicular lymph node
Enlarged lymph nodes with disrupted architecture and partially diffuse, partially interfollicular infiltration with Reed-Sternberg cells. There are multinucleated Reed-Sternberg cell (green overlay) and mononucleated Hodgkin cells (arrows).
Source: © IMPP
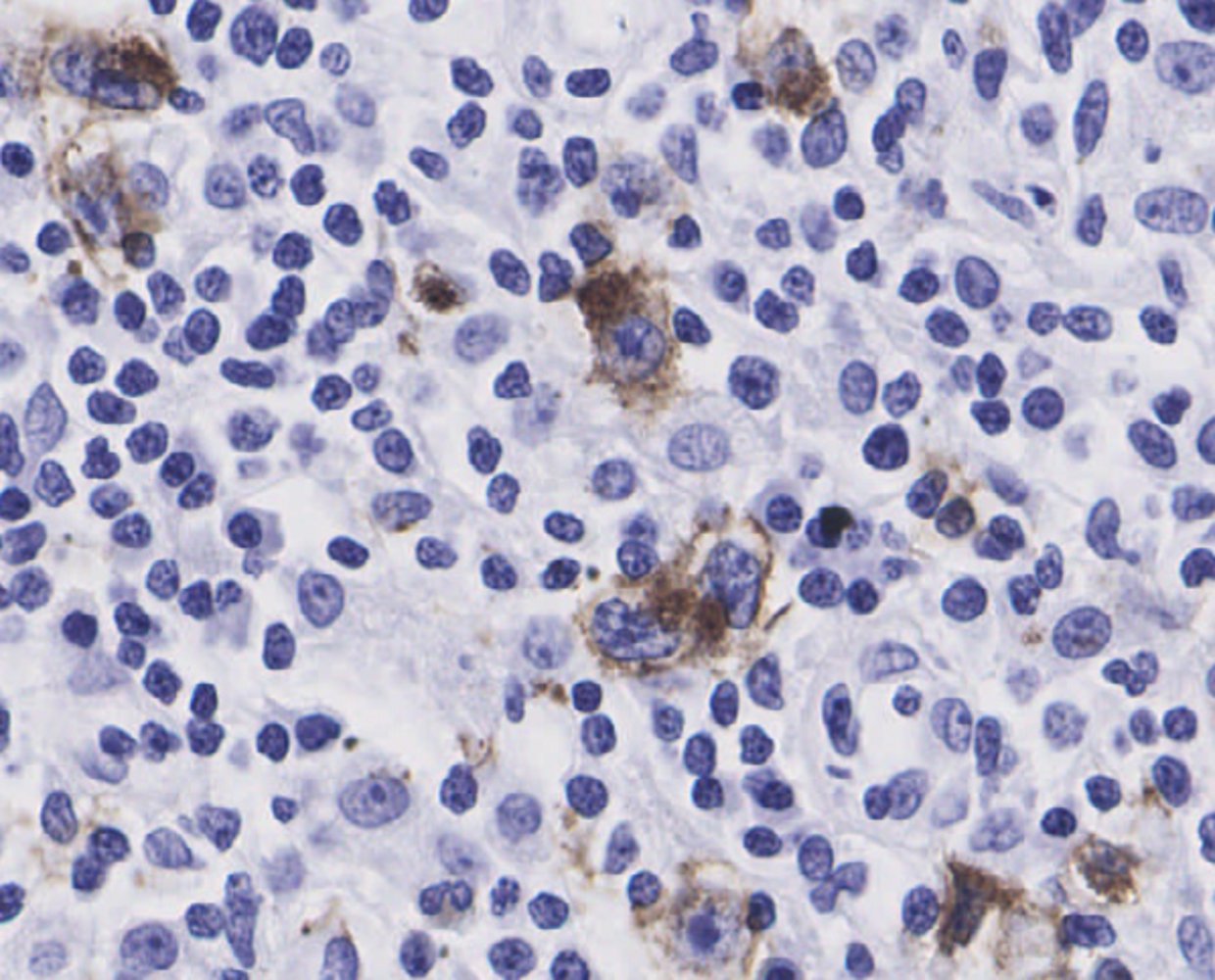
Microscopic image of the lymph node (anti-CD3 antibody) showing CD3+ T cells (dark red) surrounding a CD30+ Reed-Sternberg cell (whitish-blue) in the middle of the image.
Source: © IMPP
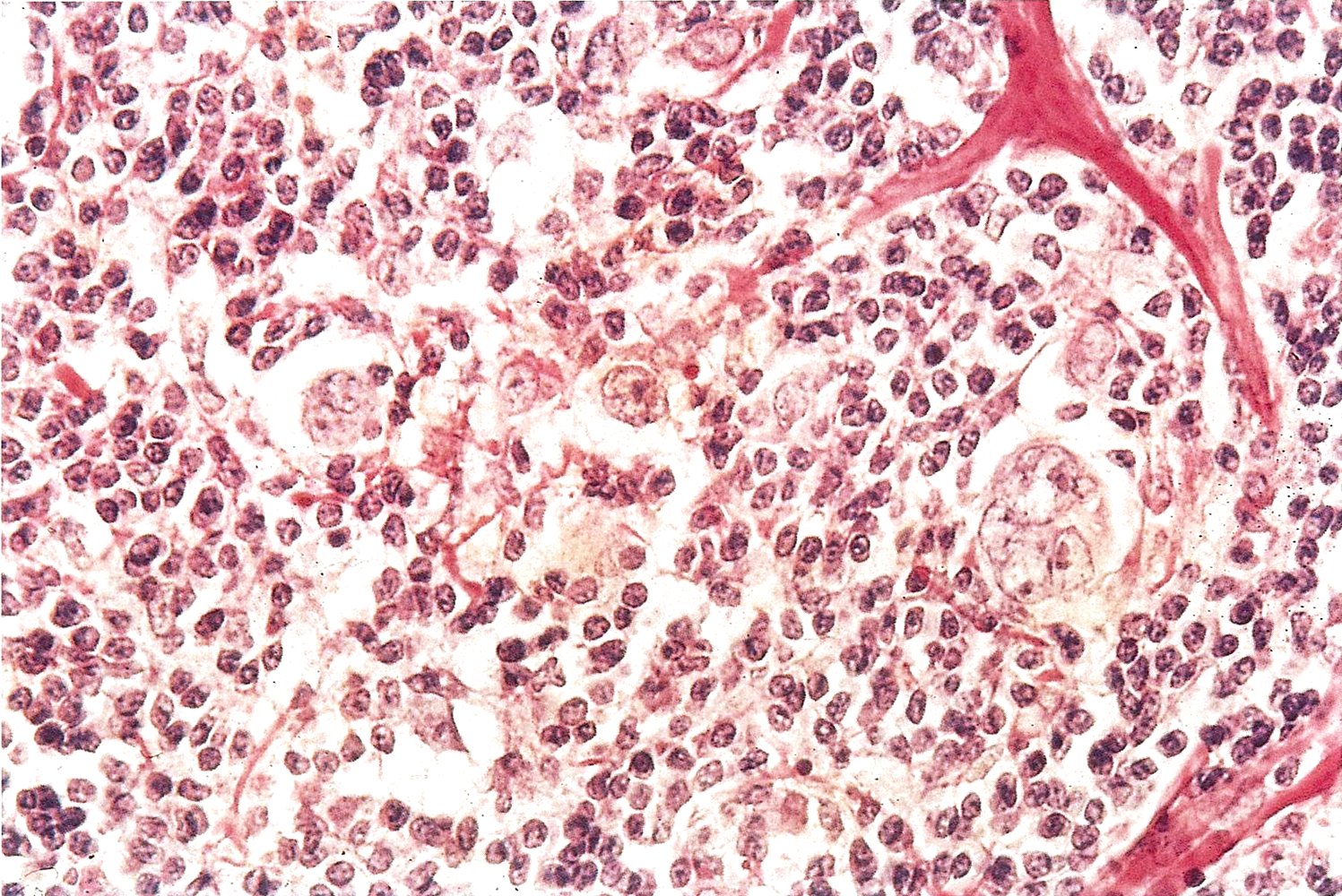
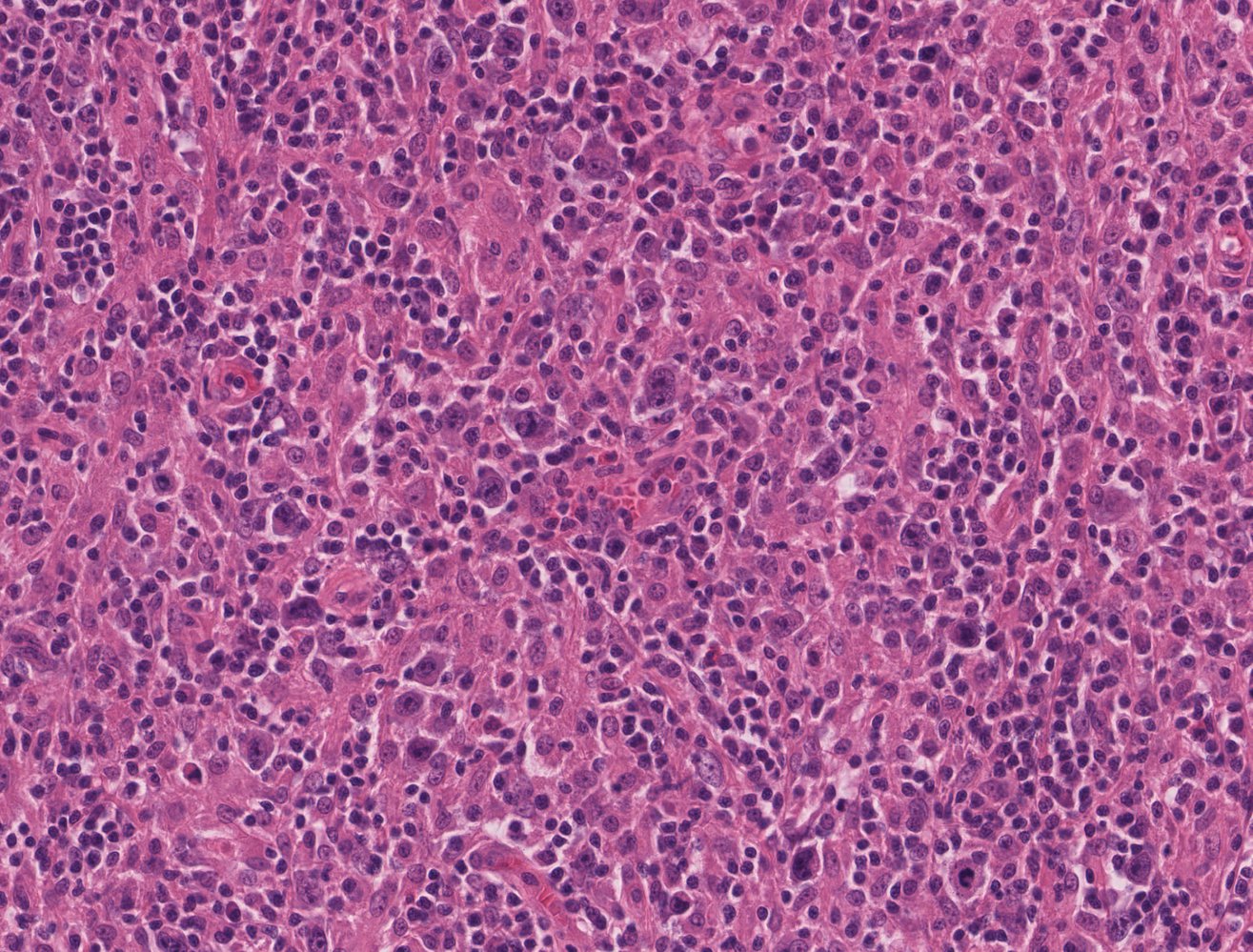
Photomicrograph of a lymph node biopsy specimen (H&E stain, high magnification)
A Reed–Sternberg cell (green overlay) can be seen in the center of the image. It is surrounded by numerous lymphocytes (examples indicated by arrowheads).
This histopathological appearance is characteristic of Hodgkin lymphoma.
Source: © IMPP
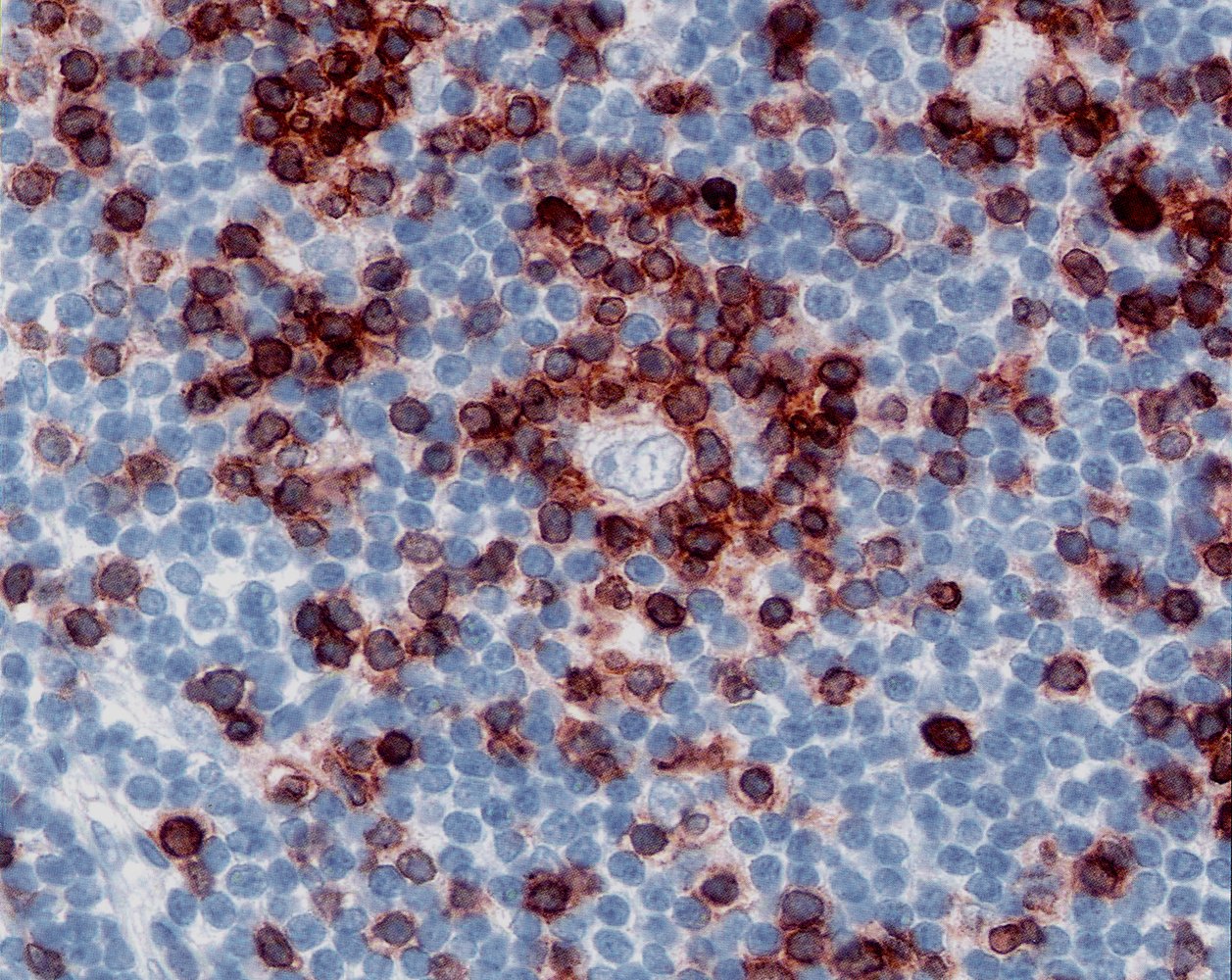
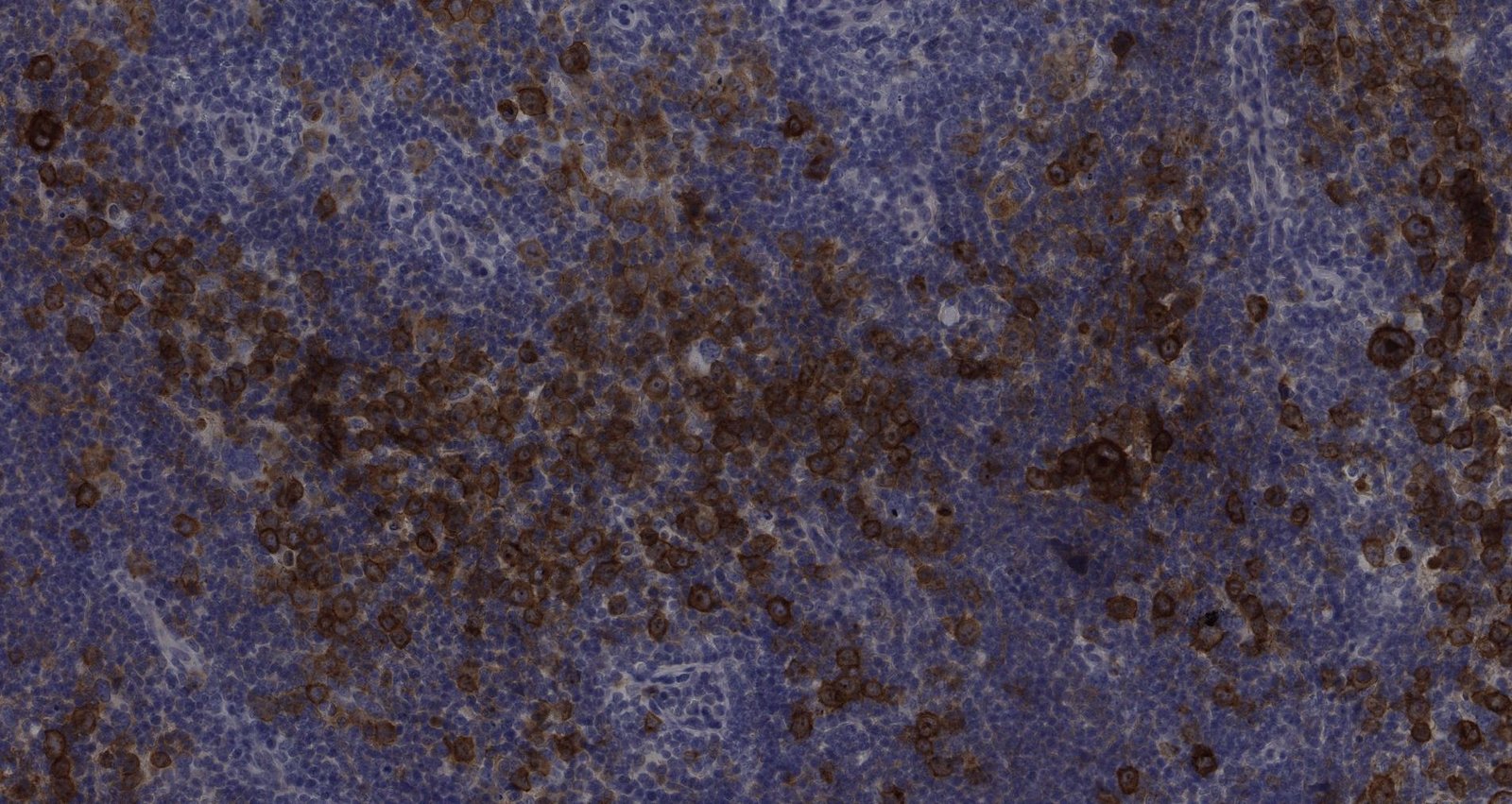
Histopathologic image of Hodgkin lymphoma (CD30 immunostain)
Reed-Sternberg cells (middle of the image). CD30 is a surface marker expressed on Reed-Sternberg cells and stains red.
Source: © IMPP
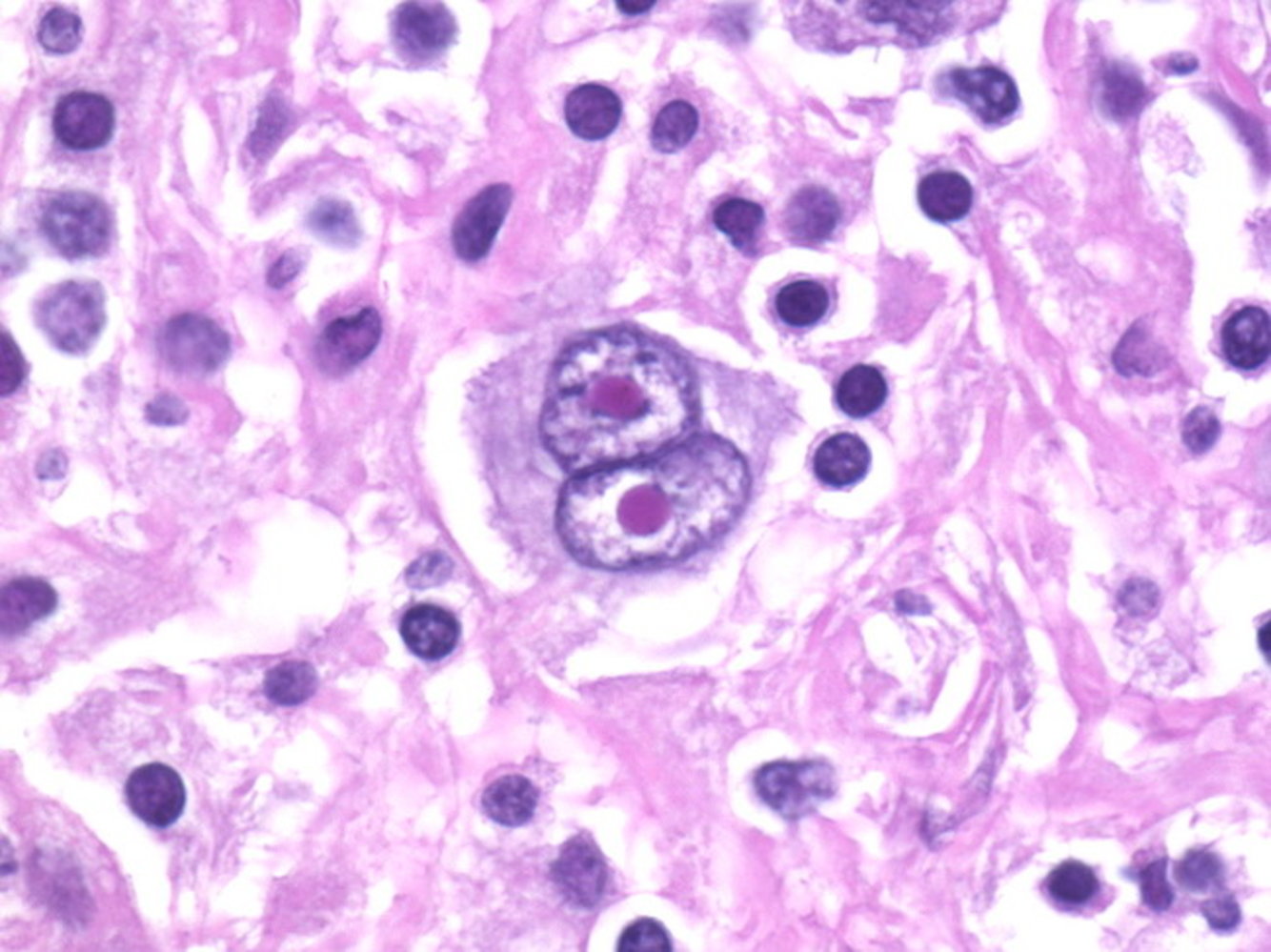
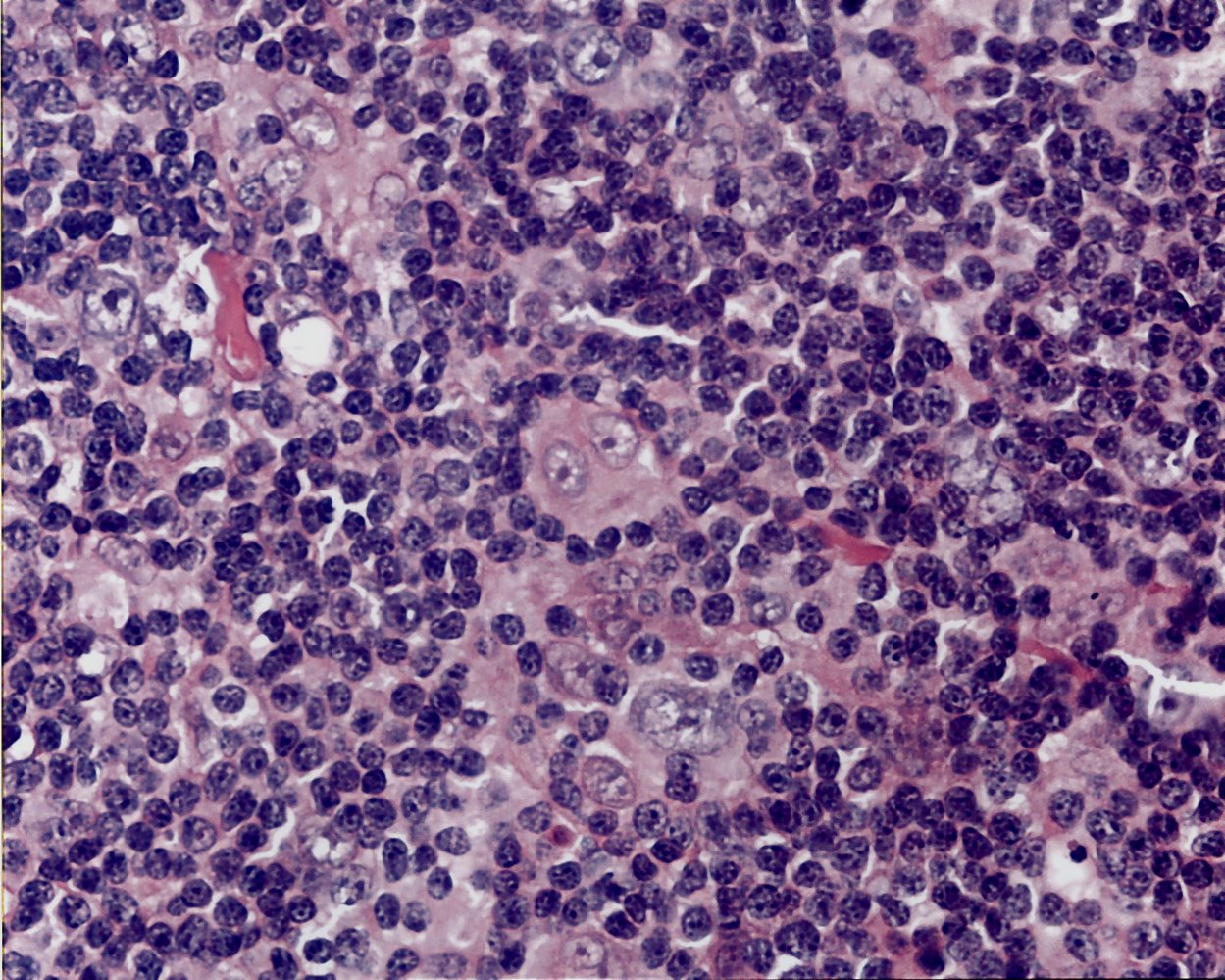
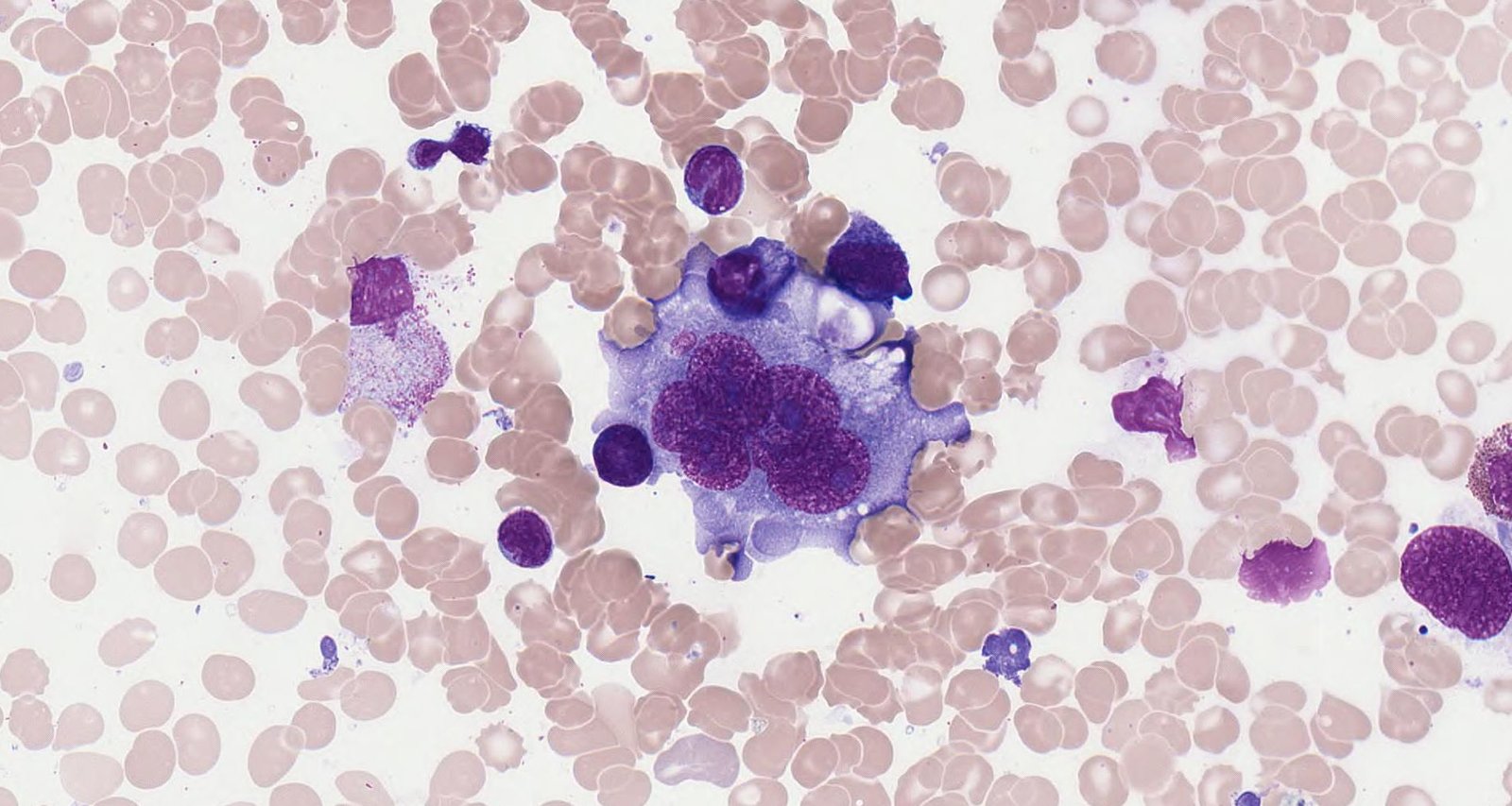
Photomicrograph of a lymphatic tissue specimen (H&E stain, high magnification)
In the center of the image is a typical Reed-Sternberg cell (yellow outline) with two nuclei (blue overlay), each with a prominent cherry-red nucleolus (black arrowheads). This creates the characteristic owl's-eye appearance of Reed-Sternberg cells. Additionally, numerous lymphocytes with basophilic nuclei (arrows) are visible.
Reed-Sternberg cells are pathognomonic for Hodgkin lymphoma.
Source: “Te bao RS” by Nva1991, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
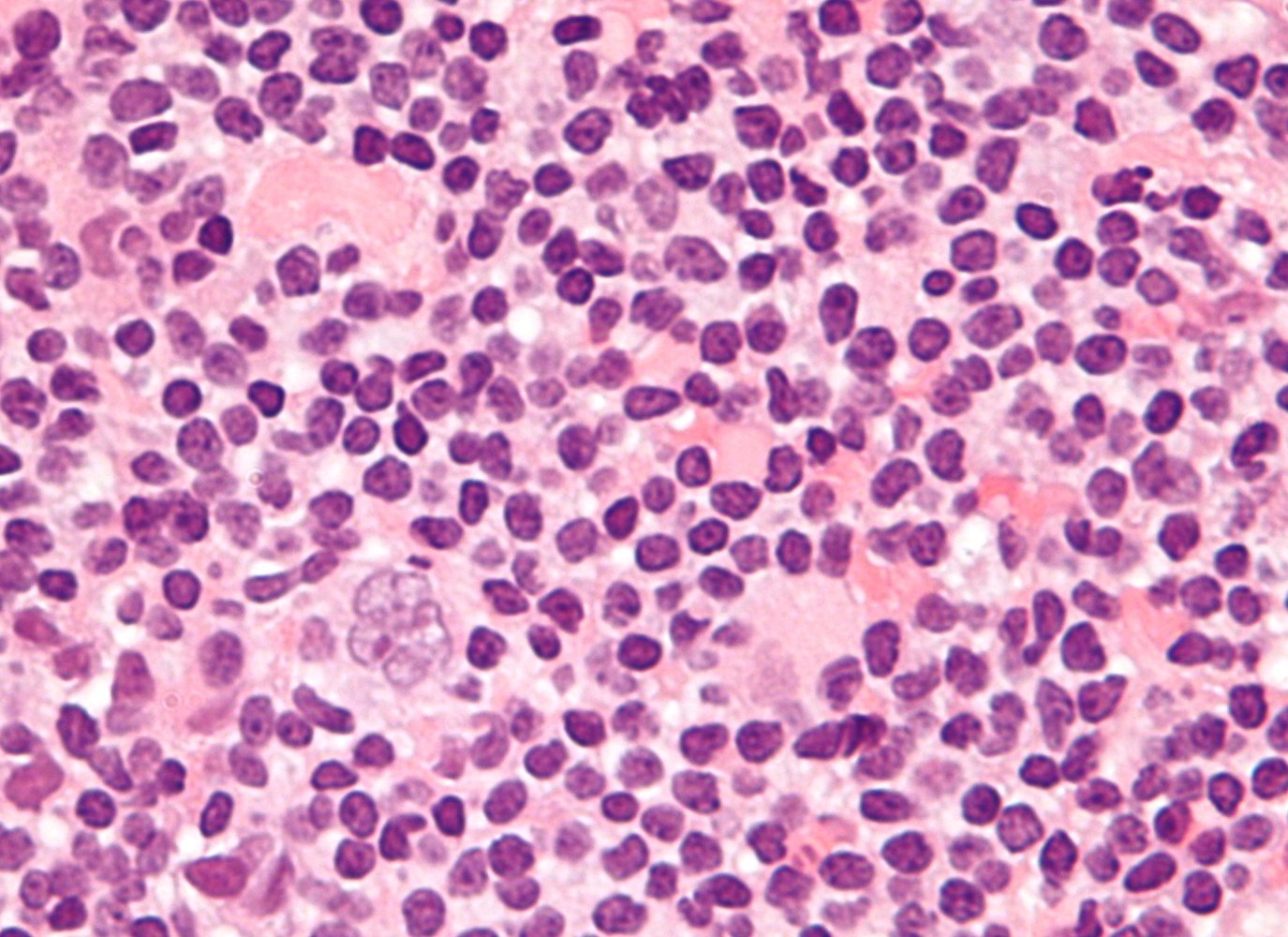
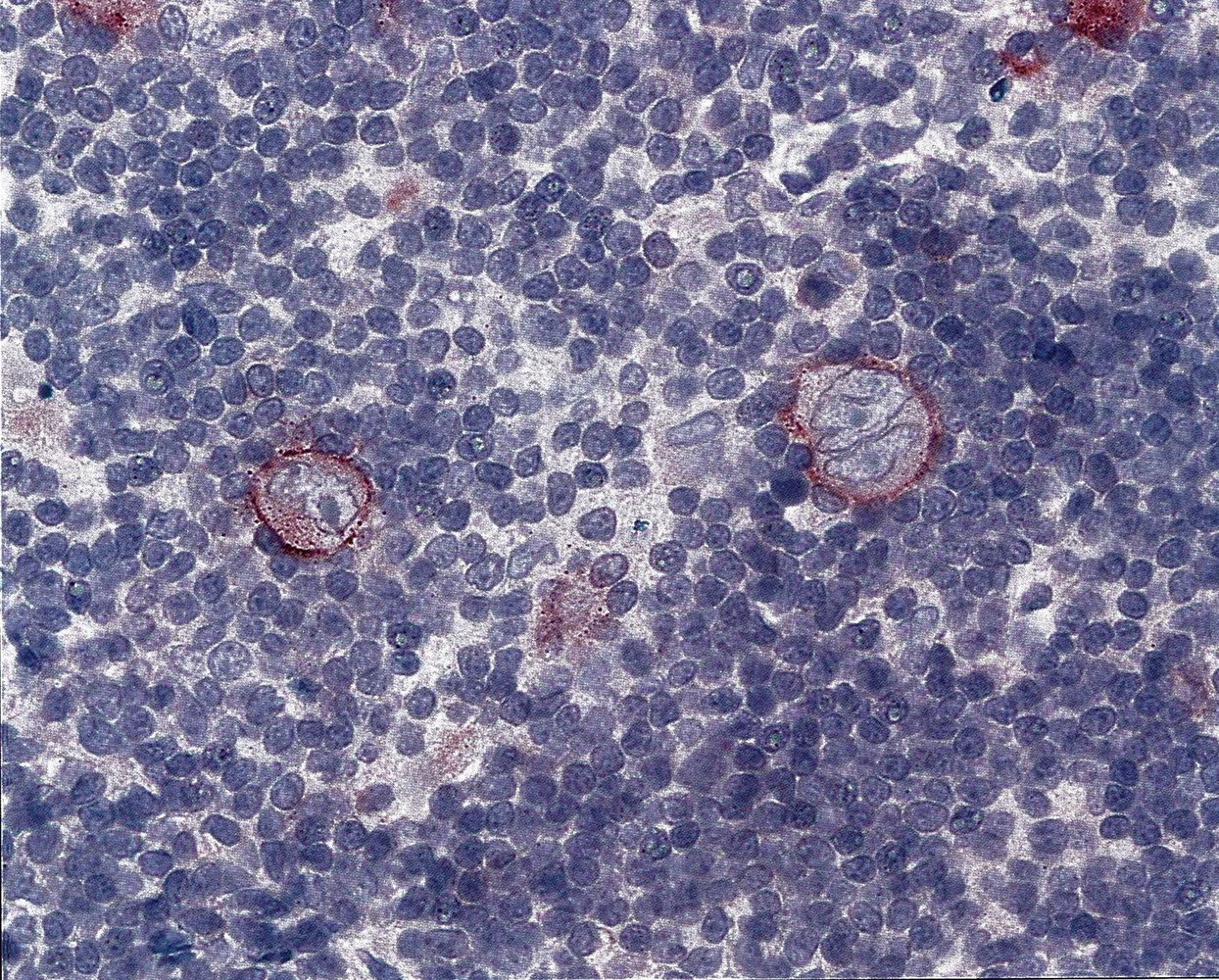
Photomicrograph of lymph node tissue (H&E stain; very high magnification)
A popcorn cell is identifiable as a large lymphocyte with a pale multilobular nucleus (green overlay). Numerous small lymphocytes are visible throughout the image.
Popcorn cells are typically seen in nodular lymphocyte predominant Hodgkin lymphoma.
Source: “Popcorn cell in nodular lymphocyte predominant Hodgkin lymphoma - very high mag cropped” by Nephron, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
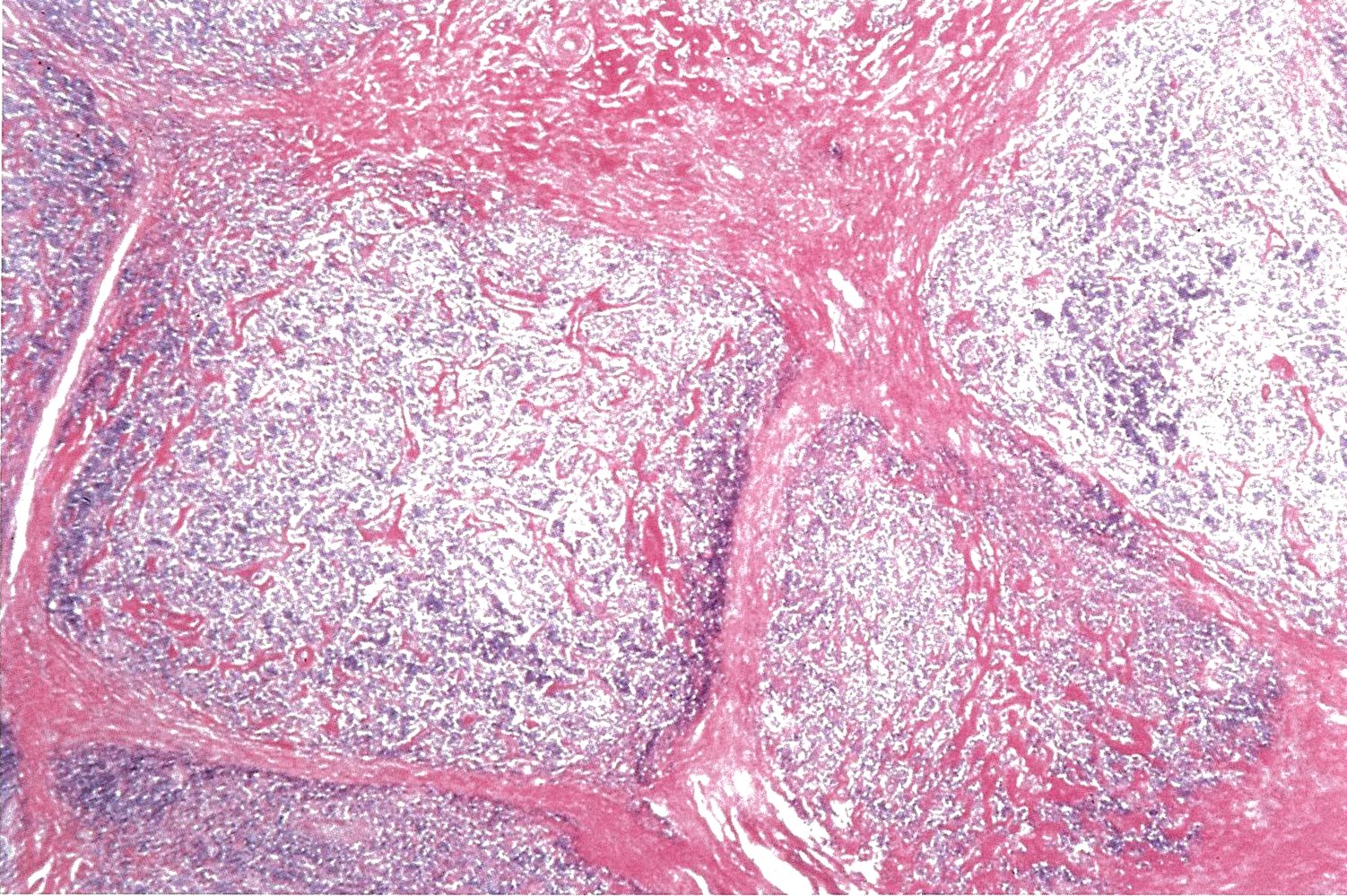
Photomicrograph of lymph tissue (H&E stain)
Lymphocyte-rich nodules can be seen surrounded by collagen fibers. There is diffuse, partially interfollicular infiltration of large tumor cells (Reed-Sternberg cells).
Diagnosis: nodular sclerosing Hodgkin lymphoma
Source: © IMPP
Click on the Smartzoom button to view the entire specimen through a virtual microscope.
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: PD Dr. Alberto Perez Bouza
Click on the Smartzoom button to view the entire specimen through a virtual microscope.
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: PD Dr. Alberto Perez Bouza
Click on the Smartzoom button to view the entire specimen through a virtual microscope.
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: PD Dr. Alberto Perez Bouza
Click on the Smartzoom button to view the entire specimen through a virtual microscope.
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: Prof. Dr. Karl-Anton Kreuzer, Facharzt für Innere Medizin, Hämatologie und Onkologie
Staging
Lugano classification of lymphomas [9]
- The Lugano classification is used for staging of HL and staging of NHL.
- Imaging with PET-CT or CT scan is required. [9][18][19]
| Lugano classification of primarily nodal lymphomas [9] | ||
|---|---|---|
| Stage | Features | |
| Limited-stage lymphoma | I |
|
| II |
|
|
| II bulky |
|
|
| Advanced-stage lymphoma | III |
|
| IV |
|
|
| A and B modifiers are only used for HL [9] A: absence of B symptoms B: B symptoms present | ||
Staging of HL is based on the number of affected nodes, the presence or absence of B symptoms, and whether or not the disease is present on both sides of the diaphragm.


Individuals who have undergone PET-CT do not routinely require bone marrow biopsy. [6][15][20]
Bone marrow biopsy is only indicated for staging if PET-CT scan imaging is unavailable or if there is evidence of bone marrow infiltration, e.g., CBC with pancytopenia, and the PET-CT scan does not demonstrate bone marrow involvement. [8][9]
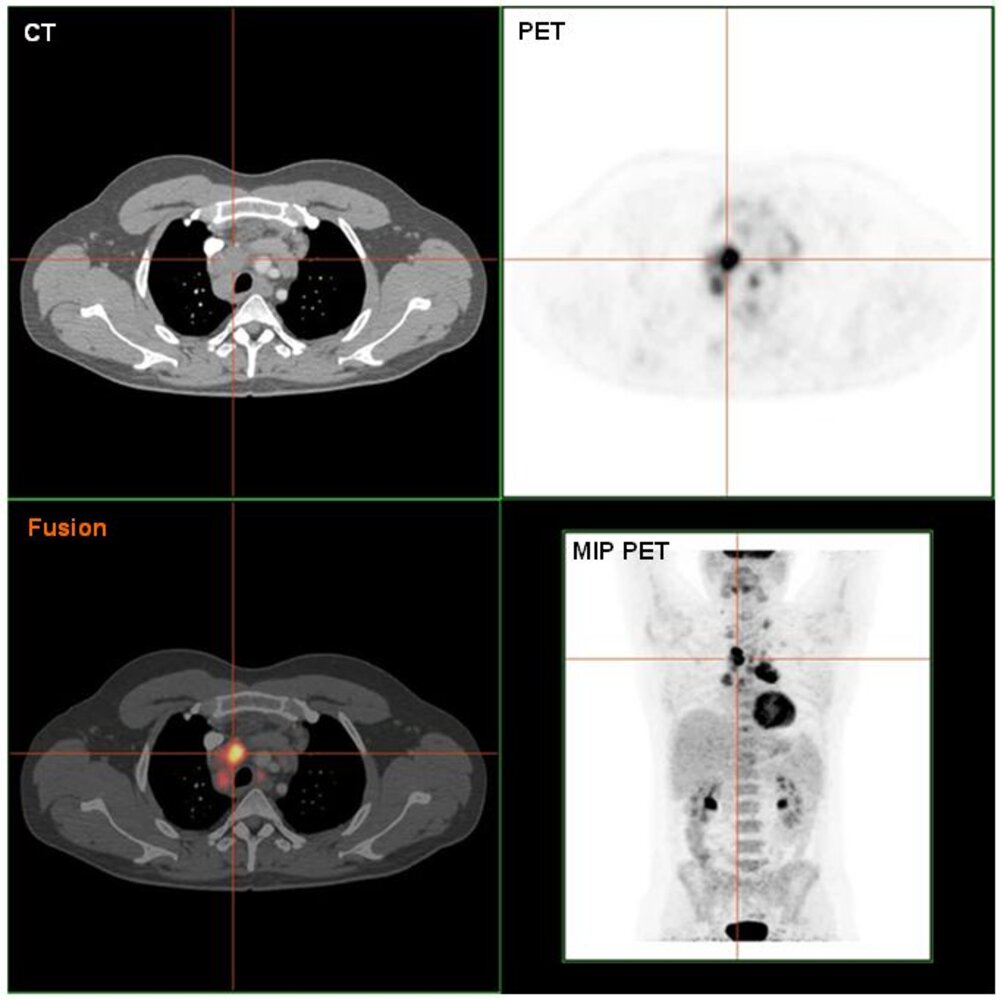
PET-CT (upper left: CT chest, axial plane; upper right: PET image, axial plane; lower left: fusion image, axial plane; lower right: PET image, maximum intensity projection) of a patient with a history of Hodgkin lymphoma
Enlarged mediastinal lymph nodes seen on the chest CT image are shown to be metabolically active on the PET and fusion images performed after F-18 fluorodeoxyglucose (FDG) administration. The whole-body PET image shows abnormal intense radiotracer uptake in several additional nodes in the neck, chest, and abdomen, as well as normal physiological uptake in the brain, heart, kidneys, and bladder.
Crosshairs (orange) show the location of one of the enlarged right upper paratracheal lymph nodes (green overlay) on all images.
Bl: Bladder; Br: Brain, H: Heart, IA: Innominate Artery; K: Kidneys; LBCV: Left brachiocephalic vein; LCA: Left common carotid artery; LSA: Left subclavian artery; SVC: Superior vena cava
Source: "HodgkinLymphomPETCT", Hg6996, Wikimedia Commons licensed under Public Domain
{kind=link}
CT chest (with contrast; axial plane) of a patient with Hodgkin lymphoma
A large anterior mediastinal soft tissue mass (green overlay) with surface lobulation and mild contrast enhancement is visible. It is bounded anteriorly by the thoracic wall and posteriorly by the ascending aorta (AA) and superior vena cava (SVC). The left brachiocephalic vein (LBCV) is encased. A cluster of lymph nodes (included in green overlay) can be seen between the aorta and the carina.
The broad histopathological spectrum of mediastinal masses includes both benign and malignant conditions. Most masses (e.g., thymoma, teratoma, thyroid disease, lymphoma) involve the anterior compartment.
AV: azygos vein; DA: descending aorta; LMB: left main bronchus; LPA: left pulmonary artery; RMB: right main bronchus
Source: © IMPP
CT scan chest, abdomen, and pelvis (with contrast; coronal plane) of a patient with Hodgkin lymphoma
A large anterior mediastinal soft tissue mass (green overlay) with surface lobulation and mild contrast enhancement is visible.
LV: left ventricle; PT: pulmonary trunk; RA: right atrium; RV: right ventricle
Source: © IMPP
© AMBOSS
Risk stratification
Following Lugano classification, patients are assessed for the presence or absence of prognostic factors to make risk-based treatment decisions. [8][15][21]
Unfavorable prognostic factors for limited-stage HL [6][20][21]
All patients with limited-stage HL are assessed for unfavorable prognostic factors. [8][15]
-
Risk factors
- High ESR [8][12]
- High LDH [22]
- B symptoms
- Involvement of > 3 lymph node areas
- ≥ 1 extranodal site
- Bulky disease
- Age ≥ 50 years
-
Interpretation
- Limited-stage favorable HL: Limited-stage HL without unfavorable prognostic factors
- Limited-stage unfavorable HL: Limited-stage HL with unfavorable prognostic factors
International prognostic score (IPS) for advanced-stage HL
All patients with advanced-stage HL (i.e., Lugano classification III or IV) are assessed with the international prognostic score to guide treatment. [11][15][21]
-
Risk factors: One point is given for each risk factor.
- Hypoalbuminemia (< 4 g/dL)
- Hemoglobin < 10.5 g/dL
- Male sex
- Age ≥ 45 years
- Lugano classification stage IV
- WBC ≥ 15,000/mm3
- Lymphopenia: lymphocyte count < 8% or absolute lymphocyte count < 600/mm3
-
Interpretation: Scores are used to estimate the freedom from progression (FFP) and overall survival (OS) at 5 years. [23][21]
- IPS score 0–1: FFP ≥ 77%, OS ≥ 89%
- IPS score 2–3: FFP ∼60–67%, OS ∼ 78-81%
- IPS score 4–7: FFP < 51%, OS ≤ 61%
Newer prediction models, e.g., the Advanced-stage cHL International Prognostication Index (A-HIPI), may be more accurate than the IPS due to improvements in treatment options. [23][24]
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
Treatment
Approach [15][18]
The following is performed by, or in coordination with, the patient's oncology team.
-
Select a risk-based treatment option. Treatment for CHL includes: [25]
- Limited-stage favorable HL: short courses of chemotherapy plus radiation therapy [15]
- Limited-stage unfavorable HL: may be treated with longer courses of chemotherapy ± radiation therapy [15][26]
- Advanced-stage HL: longer courses of chemotherapy without radiation therapy [15][21]
-
Perform a pretreatment evaluation.
- All patients: routine preparation for cancer treatment, including screening studies for pregnancy and underlying comorbidities
- Doxorubicin candidates: ECHO [15]
- Bleomycin candidates: pulmonary function testing with DLCO [27]
- Splenic radiation candidates: additional vaccinations as part of infection prevention for asplenia [28][29]
-
Provide ongoing supportive care.
- After treatment, provide long-term management for HL.
- See “Principles of cancer care” for information on multidisciplinary care, common cancer-related symptoms, and treatment-related complications.
HL treatment has high cure rates. For all stages of HL, the initial goal of treatment is remission. [8]
Chemotherapy [15][18][20]
- First-line treatment for all patients is typically ABVD: Adriamycin® (doxorubicin), bleomycin, vinblastine, and dacarbazine. [6][12][15]
- Alternative treatments (e.g., in advanced-stage or refractory HL)
- Stanford V: doxorubicin, vinblastine, mechlorethamine, vincristine, bleomycin, etoposide, and prednisone
- BEACOPP: bleomycin, etoposide, Adriamycin (doxorubicin), cyclophosphamide, Oncovin® (vincristine), procarbazine, and prednisone
Radiation therapy [20][25]
- Indication: patients with limited-stage HL, after chemotherapy [6][25]
- Radiation should target involved lymph nodes and/or extranodal sites. [6]
Other treatments [15][20][25]
- Autologous stem cell transplantation: may be used after high-dose chemotherapy in patients with relapsed or refractory disease
- Immunotherapy (e.g., brentuximab, nivolumab, or pembrolizumab) may be used for:
- Initial treatment of advanced HL
- Prevention of relapse after autologous stem cell transplantation
- Management of relapsed or refractory disease
Long-term management
Survivors of HL are at risk of disease recurrence (especially in the first 5 years after treatment) and long-term treatment-related complications. Counseling and screening are required to prevent and identify complications. [18]
Follow-up schedule [18]
- Oncology follow-up
- Years 1–2: every 3–6 months
- Year 3: every 6–12 months
- Years ≥ 4: annually
- If cancer-free after 5 years, the primary care provider may take over annual follow-up care.
Screening [18][30]
| Recommended screening after HL treatment [18][20][31] | ||
|---|---|---|
| Testing, intervals, and indications | ||
| Disease recurrence |
|
|
| Second cancers |
|
|
| Cardiovascular disorders [6] |
|
|
| Endocrine disorders | Hypothyroidism |
|
| Diabetes |
|
|
| Reproductive disorders |
|
|
| Mental health and neurological disorders |
|
|
Preventative health considerations
- Immunizations [18][35]
- During treatment: Vaccinations are typically not recommended; inactivated seasonal vaccinations may be given if indicated.
- After completion of treatment: Resume routine immunizations (3 months after chemotherapy, 6 months after immunotherapy).
- Individuals with HSCT or functional asplenia: Evaluate the need for additional vaccines and boosters.
- Counsel on smoking cessation. [12]
Prognosis
- Overall, HL has a good prognosis with a 5-year survival rate of ∼ 80–90% (in children, > 95%). [18][20][36]
- Lymphocyte-rich classical HL (LRHL) and nodular lymphocyte predominant HL (NLPHL) have the best prognoses among HL subtypes. [37][38]
- Prognosis is largely determined by disease stage.
- There is an increased risk for treatment-related second malignancies (e.g., breast, lung, colorectal). [39]
External Resources
References
- Ansell SM. "Hodgkin lymphoma: 2016 update on diagnosis, risk-stratification, and management". Am J Hematol. 91(4). :434-442. (2016)
- Asif S, Raza S. "Long-term time trends in incidence, survival and mortality of Hodgkin lymphoma in the United States: A surveillance, epidemiology, and end results (SEER) database study 1975-2015.". Journal of Clinical Oncology. 37(15_suppl). :e19014-e19014. (2019)
- "Hodgkin lymphoma risk factors". http://www.cancerresearchuk.org/health-professional/cancer-statistics/statistics-by-cancer-type/hodgkin-lymphoma/risk-factors. [2017-02-08]
- Ansell SM. "Hodgkin lymphoma: 2018 update on diagnosis, risk-stratification, and management". Am J Hematol. 93(5). :704-715. (2018)
- Gobbi PG, Ferreri AJM, Ponzoni M, Levis A. "Hodgkin lymphoma". Crit Rev Oncol Hematol. 85(2). :216-237. (2013)
- Shanbhag S, Ambinder RF. "Hodgkin lymphoma: A review and update on recent progress". CA Cancer J Clin. 68(2). :116-132. (2017)
- Piña-Oviedo S, Moran CA. "Primary Mediastinal Classical Hodgkin Lymphoma". Adv Anat Pathol. 23(5). :285-309. (2016)
- Connors JM, Cozen W, Steidl C, et al. "Hodgkin lymphoma". Nat Rev Dis Primers. 6(1). (2020)
- Cheson BD, Fisher RI, Barrington SF, et al. "Recommendations for Initial Evaluation, Staging, and Response Assessment of Hodgkin and Non-Hodgkin Lymphoma: The Lugano Classification". J Clin Oncol. (2014)
- Mauch PM, Kalish LA, Kadin M, et al. "Patterns of presentation of Hodgkin disease. Implications for etiology and pathogenesis". Cancer. 71(6). :2062-2071. (1993)
- Dirk Hasenclever, Volker Diehl, James O. Armitage, et al. "A Prognostic Score for Advanced Hodgkin's Disease". N Engl J Med. 339(21). :1506-1514. (1998)
- Caligiuri M, Levi MM, Kaushansky K, et al. "Williams Hematology, 9E". McGraw-Hill Education / Medical. (2015). ISBN: 9780071833004
- Oliver Tavabie, Abid R. Suddle. "Lymphoma and hematological conditions: I. Lymphoma and liver complications of bone marrow transplant". Clinical Liver Disease. 8(1). :1-5. (2016)
- JF Seymour, RF Gagel. "Calcitriol: the major humoral mediator of hypercalcemia in Hodgkin's disease and non-Hodgkin's lymphomas". Blood. 82(5). :1383-1394. (1993)
- Hoppe RT, Advani RH, Ai WZ, et al. "Hodgkin Lymphoma, Version 2.2020, NCCN Clinical Practice Guidelines in Oncology". J Natl Compr Canc Netw. 18(6). :755-781. (2020)
- Porwit A, McCullough JJ, Erber WN. "Blood and Bone Marrow Pathology". Churchill Livingstone. (2011). ISBN: 9780702031472
- Friedman DL. "Hodgkin Lymphoma". Elsevier. :429-441. (2016). ISBN: 9780128013687
- Lewis WD, Lilly S, Jones KL. "Lymphoma: Diagnosis and Treatment". Am Fam Physician. 101(1). :34-41. (2020)
- Ansell SM. "Hodgkin lymphoma: A 2020 update on diagnosis, risk‐stratification, and management". Am J Hematol. 95(8). :978-989. (2020)
- Blank O, von Tresckow B, Monsef I, et al. "Chemotherapy alone versus chemotherapy plus radiotherapy for adults with early stage Hodgkin lymphoma". Cochrane Database Syst Rev. (2017)
- Allen PB, Gordon LI. "Frontline Therapy for Classical Hodgkin Lymphoma by Stage and Prognostic Factors". Clin Med Insights Oncol. 11. :117955491773107. (2017)
- Shippee BM, Bates JS, Richards KL. "The role of screening and monitoring for bleomycin pulmonary toxicity". J Oncol Pharm Pract. 22(2). :308-312. (2015)
- Ariza-Heredia EJ, Chemaly RF. "Practical review of immunizations in adult patients with cancer". Hum Vaccin Immunother. 11(11). :2606-2614. (2015)
- Brigden ML. "Detection, education and management of the asplenic or hyposplenic patient". Am Fam Physician. 63(3). :499-506, 508. (2001)
- Eichenauer DA, Aleman BMP, André M, et al. "Hodgkin lymphoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up". Ann Oncol. 29. :iv19-iv29. (2018)
- Ehrhardt MJ, Flerlage JE, Armenian SH, et al. "Integration of Pediatric Hodgkin Lymphoma Treatment and Late Effects Guidelines: Seeing the Forest Beyond the Trees". J Natl Compr Canc Netw. 19(6). :755-764. (2021)
- Volker Diehl, Michael Sextro, Jeremy Franklin, et al. "Clinical Presentation, Course, and Prognostic Factors in Lymphocyte-Predominant Hodgkin's Disease and Lymphocyte-Rich Classical Hodgkin's Disease: Report From the European Task Force on Lymphoma Project on Lymphocyte-Predominant Hodgkin's Disease". J Clin Oncol. 17(3). :776-776. (1999)
- Allemani C, Sant M, De Angelis R, Marcos-Gragera R, Coebergh JW. "Hodgkin disease survival in Europe and the U.S.". Cancer. 107(2). :352-360. (2006)
- Schaapveld M, Aleman BMP, van Eggermond AM, et al. "Second Cancer Risk Up to 40 Years after Treatment for Hodgkin’s Lymphoma". N Engl J Med. 373(26). :2499-2511. (2015)
- Ha CS, Hodgson DC, Advani R, et al. "ACR Appropriateness Criteria Follow-up of Hodgkin Lymphoma". J Am Coll Radiol. 11(11). :1026-1033.e3. (2014)
- Ng AK. "Current survivorship recommendations for patients with Hodgkin lymphoma: focus on late effects". Blood. 124(23). :3373-3379. (2014)
- "Long-Term Follow-Up Guidelines for Survivors of Childhood, Adolescent and Young Adult Cancers, Version 5.0". https://web.archive.org/save/http://www.survivorshipguidelines.org/pdf/2018/COG_LTFU_Guidelines_v5.pdf. [2018-10-01]
- Gebauer J, Higham C, Langer T, Denzer C, Brabant G. "Long-Term Endocrine and Metabolic Consequences of Cancer Treatment: A Systematic Review". Endocr Rev. 40(3). :711-767. (2018)
- Bhasin S, Brito JP, Cunningham GR, et al. "Testosterone Therapy in Men With Hypogonadism: An Endocrine Society* Clinical Practice Guideline". J Clin Endocrinol Metab. 103(5). :1715-1744. (2018)
- "Altered Immunocompetence. General Best Practice Guidelines for Immunization". https://web.archive.org/web/20240118195954/https://www.cdc.gov/vaccines/hcp/acip-recs/general-recs/immunocompetence.html. [2023-08-01]
- Meignan M, Hutchings M, Schwartz LH. "Imaging in Lymphoma: The Key Role of Fluorodeoxyglucose-Positron Emission Tomography". Oncologist. 20(8). :890-895. (2015)
- Qi J, Gu C, Wang W, et al. "Elevated Lactate Dehydrogenase Levels Display a Poor Prognostic Factor for Non-Hodgkin’s Lymphoma in Intensive Care Unit: An Analysis of the MIMIC-III Database Combined With External Validation". Front Oncol. 11. (2021)
- Moccia AA, Donaldson J, Chhanabhai M, et al. "International Prognostic Score in Advanced-Stage Hodgkin's Lymphoma: Altered Utility in the Modern Era". Journal of Clinical Oncology. 30(27). :3383-3388. (2012)
- Rodday AM, Parsons SK, Upshaw JN, et al. "The Advanced-Stage Hodgkin Lymphoma International Prognostic Index: Development and Validation of a Clinical Prediction Model From the HoLISTIC Consortium". J Clin Oncol. 41(11). :2076-2086. (2023)