Summary
Humerus fractures can result from direct or indirect trauma. They are classified by location into proximal humerus fracture, humeral shaft fracture, and distal humerus fracture. Proximal humerus fractures most commonly occur in older adults, while supracondylar fractures (a type of distal humerus fracture) are most common in children. Clinical features include pain, soft tissue swelling, and visible deformity. Nondisplaced, closed fractures are typically managed with a sling or splint. If there is evidence of neurovascular compromise or in the case of open fractures, operative management is usually required.
Epidemiology
- Proximal humerus fractures are the most common humerus fractures.
- Incidence increases with age.
- Sex: ♀ > ♂
Epidemiological data refers to the US, unless otherwise specified.
Etiology
-
Direct or indirect trauma
- Falls with axial loading on an outstretched hand (most common cause) [2]
- Motor vehicle accidents
- Violent seizures
- Direct blow to the back of the humerus
- Pathologic fractures: : e.g., Paget disease, metastatic bone disease (less common)
Classification
Proximal humerus fracture
- Proximal humerus fractures are common in older adults and typically occur between the major segments of the proximal humerus. [2]
- Neer classification: Fractures are classified as one- to four-part fractures, depending on the number of displaced fracture segments. [3]


Humeral shaft fracture
Humeral shaft fractures are further classified based on location. [2]
- Proximal humeral shaft fracture
- Middle humeral shaft fracture
- Distal humeral shaft fracture

Distal humerus fracture
Distal humerus fractures, of which there are many subtypes, are a type of elbow fracture. See “Forearm fractures” for other fractures with elbow involvement.
-
Supracondylar fracture
- A fracture of the distal humerus proximal to the epicondyles
- The most common pediatric elbow fracture [4]
- Transcondylar fracture
- Intercondylar fracture
- Condylar fracture
- Epicondylar fracture
- Capitellum fracture
- Trochlea fracture



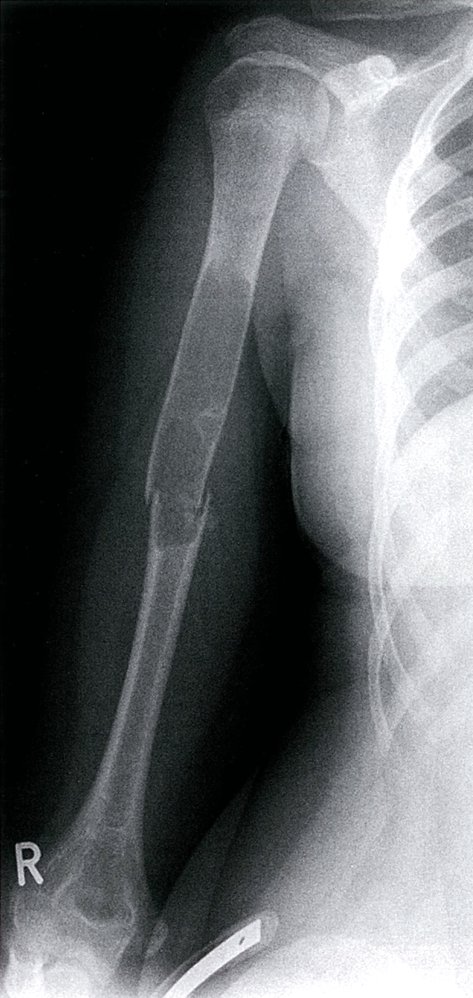
X-ray left shoulder (AP view)
A three-part fracture (Neer classification) of the surgical neck (white arrows) of the proximal humerus involves the greater tuberosity (black arrow). There is lateral angulation of the humeral shaft.
Source: “ProxHumeralFracture” by James Heilman, MD, Wikimedia Commons, licensed under CC BY-SA 4.0. Modifications: removal of the red arrow. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 4.0.
{kind=link}


X-ray (posteroanterior view) of the humerus
Fracture of the humerus into multiple fragments. The overlay highlights the points of fracture belonging together in green and red. White-filled overlay highlights the ulna. White outline highlights the humerus. White dashed outline highlights the radius.
Source: © IMPP

X-ray elbow (lateral view) of a child with a history of recent trauma
A comminuted supracondylar fracture of the distal humerus (H) shows posterior displacement of the distal fragment and growth plate involvement (white arrow). Joint effusion is present, with elevation of the lucent posterior fat pad (white arrowheads).
H: humerus; R: radius; U: ulna
Source: “Supracondylar09” by James Heilman, MD, Wikimedia Commons, licensed under CC BY-SA 3.0. Modifications: Removed black arrow. Removed the black letters.. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
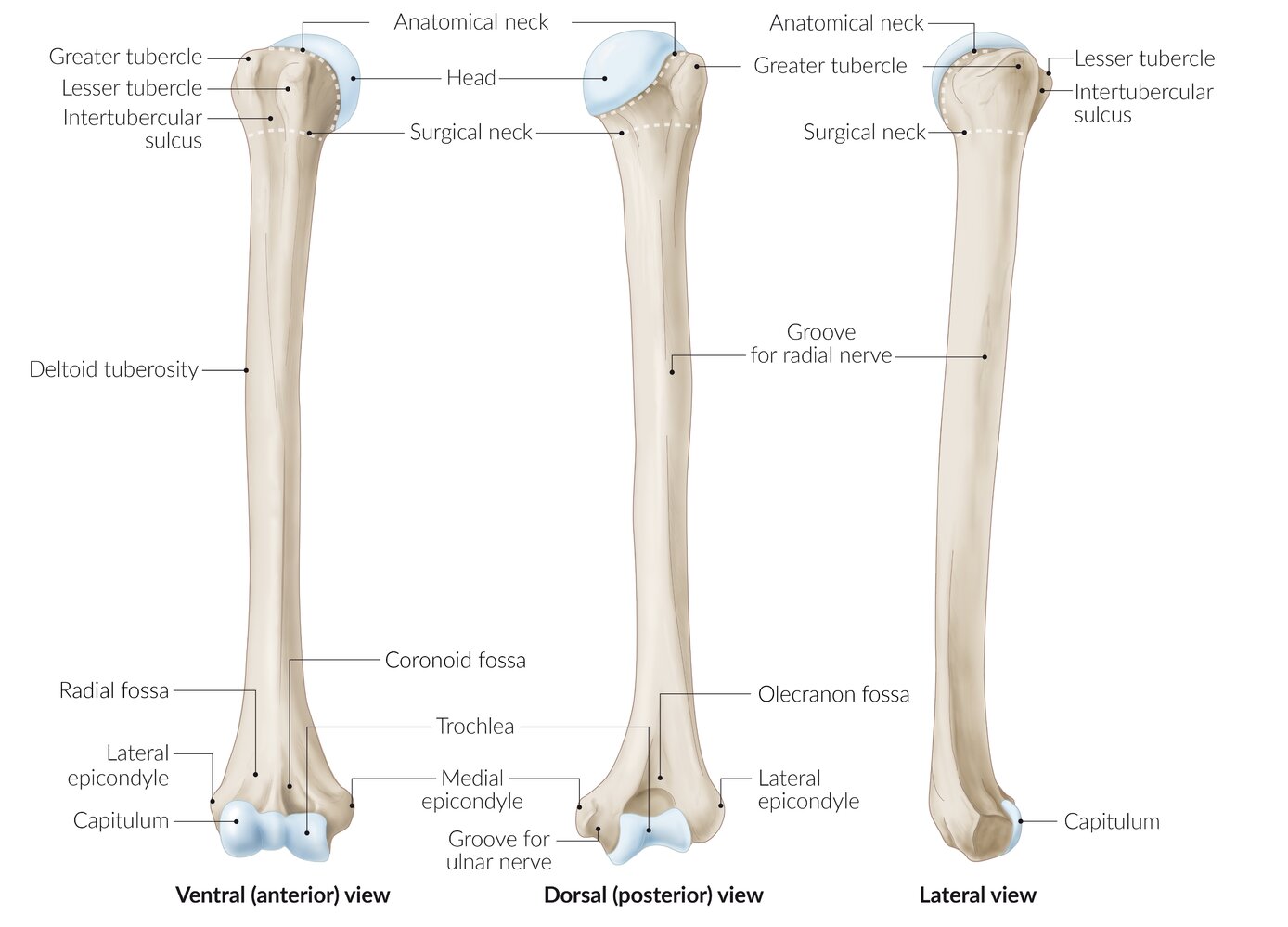
The humerus from a ventral (left), dorsal (center), and lateral (right) view.
The anatomical and surgical necks of the bone are marked with dashed lines.
© AMBOSS
Clinical features
- Severe local pain: exacerbated during palpation or movement at shoulder or elbow
- Local swelling (edema or bleeding), deformity, and/or crepitus
- Shortening of the arm (associated with displacement)
- Neurovascular complications such as radial nerve palsy (see “Complications” below)
- See “Signs of fracture.”
The radial nerve runs through the radial sulcus of the upper arm and is especially at risk in fractures of the middle third (midshaft) of the humerus!
Diagnosis
Clinical evaluation [2]
Any findings that suggest neurovascular injury or open fracture should prompt urgent orthopedic consultation.
-
Neurovascular exam
- Assess radial and ulnar artery pulses and capillary refill time.
- Evaluate for median nerve injury , radial nerve injury , and ulnar nerve injury.
- Skin exam: Evaluate for laceration, tearing, and tenting.
")



Imaging [2]
X-ray
Imaging for humerus fractures typically includes x-ray views of the humerus, shoulder, and elbow.
-
Views
- Shoulder: true anteroposterior, trans-scapular lateral (Y view), and axillary lateral
- Humerus: anteroposterior and lateral
- Elbow: anteroposterior and lateral, as well as oblique view as needed
-
Findings
- Radiographic fracture signs, fracture fragments, displacement, angulation, and/or dislocation
- Visible fat pads in elbow views suggest an intraarticular fracture.
- Posterior fat pad sign: a radiographic finding caused by an elbow joint effusion; results in the presence of a lucent crescent in the olecranon fossa on a lateral x-ray view of the elbow
- Anterior fat pad sign (sail sign): a radiographic finding caused by an elbow joint effusion; results in the presence of a convex lucent crescent in the coronoid fossa on a lateral x-ray view of the elbow
A visible anterior fat pad may be normal, but a visible posterior fat pad is always abnormal. [2]
 with pathological fracture")



Advanced imaging [2]
- CT: indicated in preoperative planning for complicated fractures, assessment of associated injuries, and inconclusive x-ray findings
- CT angiography: indicated for suspected vascular injury
- MRI: may be indicated for diagnosis of associated tendon/ligament injuries (e.g., rotator cuff injury)
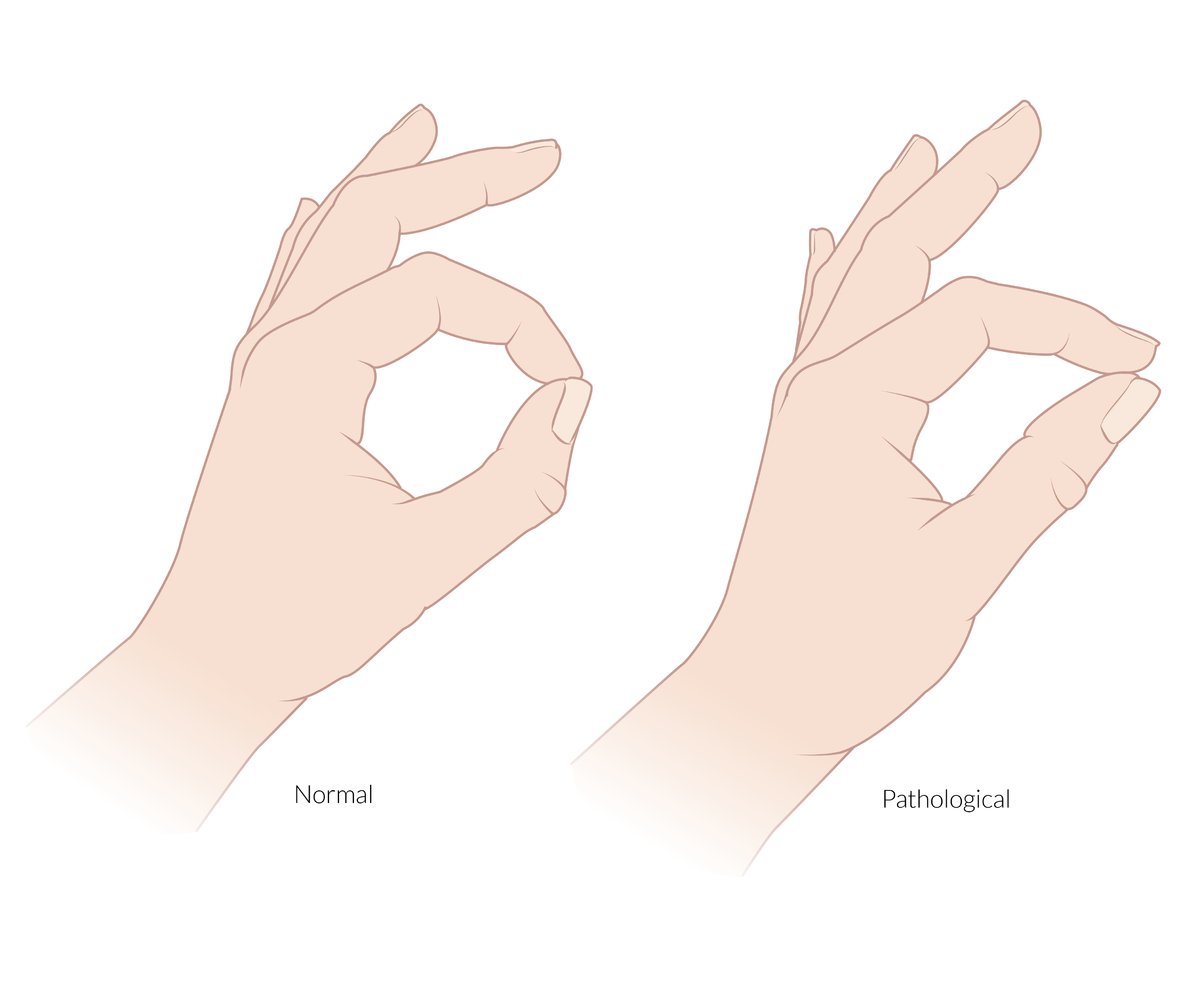
The anterior interosseous nerve is a pure motor branch of the median nerve. It supplies the flexor pollicis longus, the radial half of the flexor digitorum profundus (and the pronator quadratus).
Pinch sign: an inability to flex the DIP of the index finger and IP joint of the thumb when asked to make an “OK” sign that is caused by a lesion or entrapment of the anterior interosseous nerve
© AMBOSS

An inability to flex the index and middle fingers at the MCP and IP joints and an inability to oppose the thumb.
The hand of benediction is an active sign and is only seen when the patient is asked to make a fist. It indicates a paralysis of the thenar muscles (except the adductor pollicis), the flexor digitorum superficialis, and the radial half of the flexor digitorum profundus caused by a proximal lesion of the median nerve (above the elbow).
Also depicted is atrophy of the thenar muscles, which is seen in chronic median nerve palsy.
© AMBOSS
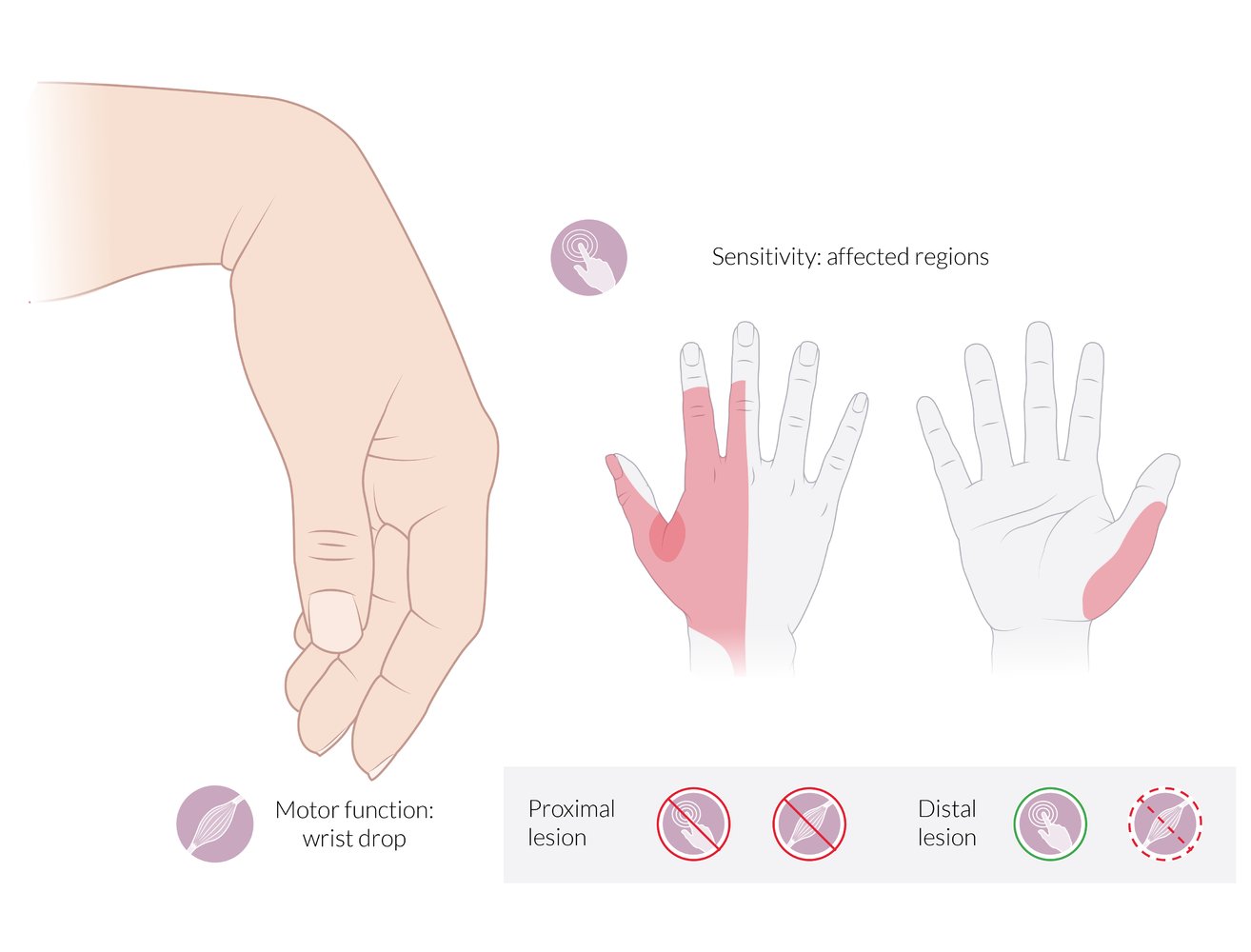
Motor deficits:
- Wrist drop: inability to extend (dorsiflex) the wrist
- Inability to extend the fingers at the MCP joints
Sensory deficits:
- Dorsal aspect: radial 2½ fingers (less commonly, 3½ fingers), excluding the tips of the 2nd and 3rd fingers. The 1st web space is the autonomous sensory zone of the radial nerve and is highlighted in red.
- Palmar aspect: the radial border of the thumb
Proximal lesion: complete loss of motor and sensory function
Distal lesion (radial tunnel syndrome): partial loss of motor function; preservation of sensory function
© AMBOSS
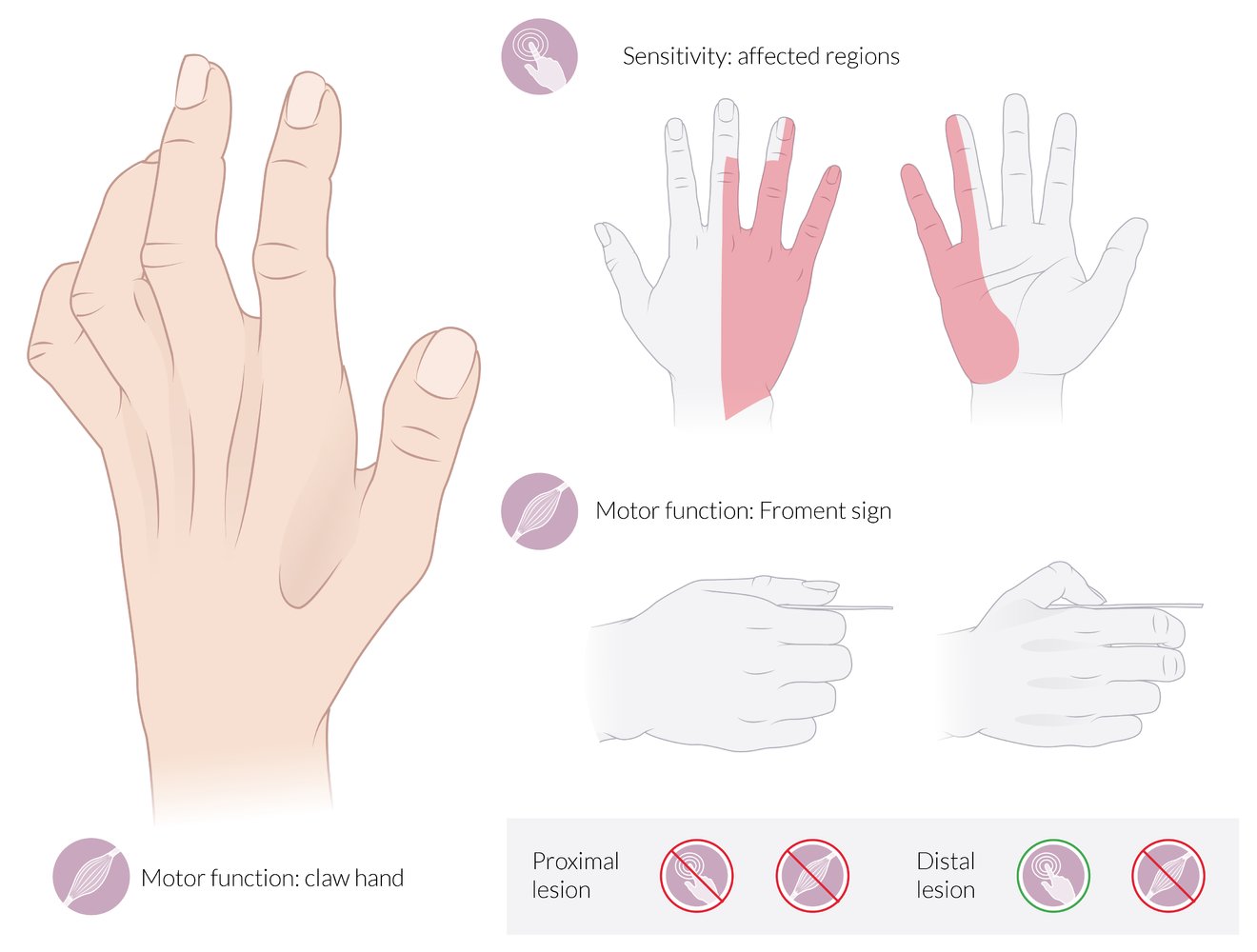
Motor deficits:
- Claw hand: The 4th and 5th joints are hyperextended at the MCP and flexed at the IP joints at rest (neutral position).
- Froment sign: The patient is asked to grasp a piece of paper between the thumb and the index finger. When the examiner tries to pull the paper away, the thumb flexes at the IP joint because the flexor pollicis longus (supplied by the median nerve) compensates for the paralyzed adductor pollicis (supplied by the ulnar nerve).
Also depicted here is hollowing of the intermetacarpal spaces and the 1st web space due to the atrophy of the interossei, which is seen in chronic ulnar nerve palsy.
Sensory deficits:
- Dorsal aspect: ulnar 2½ fingers (less commonly, 1½ fingers), excluding the tips of the 3rd and 4th fingers
- Palmar aspect: ulnar 1½ fingers
Proximal lesion: complete loss of motor and sensory functions
Distal lesion: complete loss of motor function; preservation of sensory function
© AMBOSS
X-ray left shoulder (AP view)
A three-part fracture (Neer classification) of the surgical neck (white arrows) of the proximal humerus involves the greater tuberosity (black arrow). There is lateral angulation of the humeral shaft.
Source: “ProxHumeralFracture” by James Heilman, MD, Wikimedia Commons, licensed under CC BY-SA 4.0. Modifications: removal of the red arrow. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 4.0.
X-ray (posteroanterior view) of the humerus
Fracture of the humerus into multiple fragments. The overlay highlights the points of fracture belonging together in green and red. White-filled overlay highlights the ulna. White outline highlights the humerus. White dashed outline highlights the radius.
Source: © IMPP
X-ray right humerus (AP view) of an adolescent patient with pain
An expansile lucent lesion in the humeral diaphysis (green overlay) has a geographic margin with a narrow zone of transition. The appearance is compatible with a unicameral bone cyst (simple bone cyst). A pathological fracture (red overlay) has occurred through the distal aspect of the cyst.
Unicameral bone cysts are common benign lucent bone lesions. They are typically discovered in childhood or adolescence either incidentally or in the course of diagnosing a pathological fracture.
Source: © IMPP
X-ray elbow (lateral view) of a child with a history of recent trauma
A comminuted supracondylar fracture of the distal humerus (H) shows posterior displacement of the distal fragment and growth plate involvement (white arrow). Joint effusion is present, with elevation of the lucent posterior fat pad (white arrowheads).
H: humerus; R: radius; U: ulna
Source: “Supracondylar09” by James Heilman, MD, Wikimedia Commons, licensed under CC BY-SA 3.0. Modifications: Removed black arrow. Removed the black letters.. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.

X-ray elbow (AP view)
A comminuted fracture of the distal humerus (H, green overlay) is accompanied by displacement and overriding of the main fragments, resulting in foreshortening of the humerus.
U: Ulna, R: Radius
Source: © IMPP

X-ray of the elbow joint, lateral view
13-year-old girl who fell on an outstretched hand. The bones show no fracture, but a fat pad sign can be seen ventral and dorsal to the humeral shaft. The fat pad sign indicates elbow joint effusion. It arises when the fatty tissue usually attached to the distal humerus is lifted off the bone because of the joint effusion; while the fatty tissue is usually visible as a lucency parallel to the humerus, it becomes crescent-shaped if there is an effusion.
Our great thanks to PD Dr. M. Jergas (Center for Diagnostic and Interventional Radiology, St. Elizabeth Hospital, Cologne) for kindly providing this image.
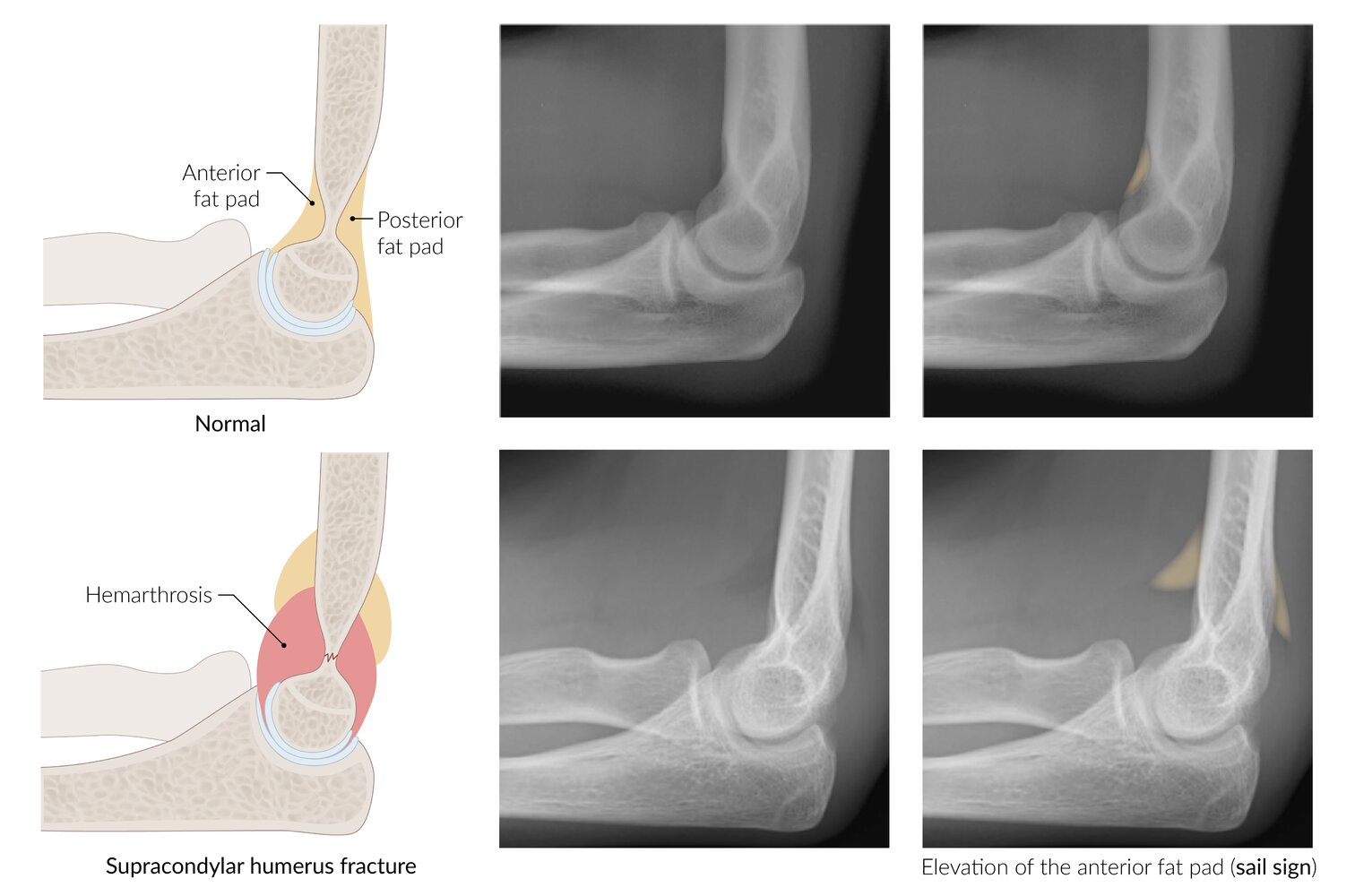
The top row shows lateral views of a normal elbow joint. The anterior fat pad (highlighted in yellow on the right radiograph) resides in the coronoid fossa and is normally visible. It is labeled on the illustration and seen on the left radiograph as a lucent stripe ventral to the distal humerus. The posterior fat pad resides in the olecranon fossa and is not normally visible.
The bottom row shows the result of a supracondylar fracture (not visible). Hemarthrosis has elevated the anterior and posterior fat pads. The posterior fat pad is now visible (posterior fat pad sign) and the anterior fat pad has the appearance of a spinnaker sail (anterior fat pad sign or sail sign).
The anterior and posterior fat pad signs are valuable in diagnosing fractures of the elbow, particularly in cases where a fracture line may not be visible (e.g., supracondylar humeral fracture, radial head fracture)
© AMBOSS
Differential diagnoses
Differential diagnosis of proximal humerus fractures [2]
- Shoulder dislocation
- Acromioclavicular joint separation
- Clavicle fracture
- Scapula fracture
- Rotator cuff injury
- Soft tissue injury
Differential diagnosis of distal humerus fractures [2]
- Olecranon fracture
- Radial head fracture
- Elbow dislocation
- Radial head subluxation
- Soft tissue injury
The differential diagnoses listed here are not exhaustive.
Treatment
Initial management by fracture type [2]
- All patients: Initiate general fracture care, including analgesia.
-
Proximal humerus fractures
- Immobilize in an arm sling.
- Consult orthopedics urgently for:
- Displaced fracture segments
- Fracture-dislocation
-
Humeral shaft fractures
- Immobilize in a coaptation splint.
- Consult orthopedics urgently for:
- Radial nerve injury
- Severely displaced fractures
- Comminuted fractures
-
Distal humerus fractures
- Immobilize in a long arm posterior splint.
- Consult orthopedics urgently for:
- Displaced supra- or epicondylar fractures
- All transcondylar, intercondylar, and condylar fractures
- Presence of intraarticular fragments
Nonoperative management
- Nonoperative management is generally possible for nondisplaced, closed fractures.
- Devices include hanging-arm casts, coaptation splints, and arm slings
- See also: “Conservative treatment of fractures”
Surgical treatment
-
Fractures that commonly require surgical treatment include:
- Open fractures
- Poor reduction of displaced fractures
- Neurovascular injury
- Pathologic fractures
- Simultaneous humerus and forearm fractures (floating elbow)
- Operative techniques depend on fracture location and type and include:
- Open reduction and internal fixation (ORIF)
- Closed reduction and internal fixation (CRIF)
- Intramedullary nailing (IMN)
- Arthroplasty

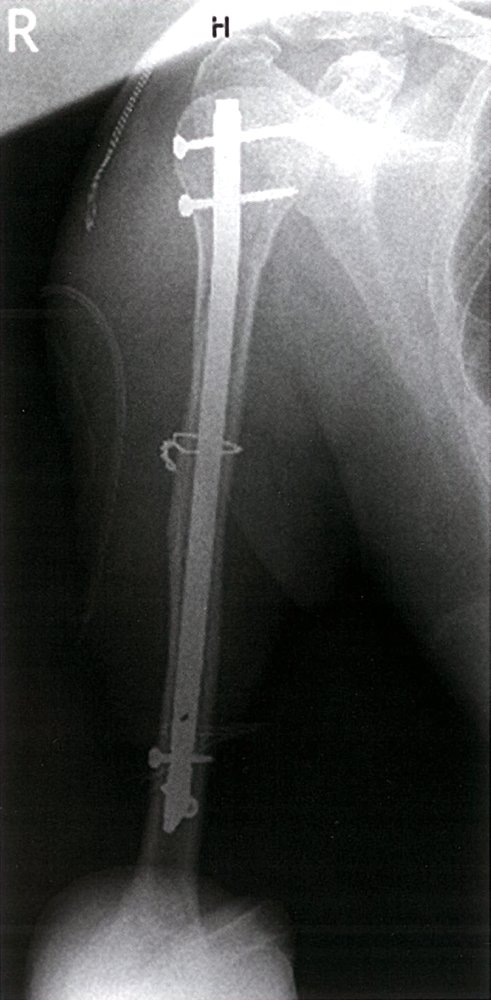
X-ray right humerus (AP view)
A comminuted humeral shaft fracture has been reduced to the correct anatomical position and surgically fixated using an intramedullary nail. There is good apposition of the fracture fragments.
Source: © IMPP
Complications
-
Proximal humerus fracture
- Avascular necrosis of humeral head (axillary artery injury)
- Adhesive capsulitis
- Heterotopic bone formation
-
Distal humerus fracture
-
Brachial artery injury (common)
- Absent or diminished radial pulse suggests brachial artery entrapment (especially following reduction) and compartment syndrome.
- May lead to Volkmann ischemic contracture (late complication)
- Malunion and varus deformity of the elbow
-
Brachial artery injury (common)
| Humerus fracture nerve palsies | |||
|---|---|---|---|
| Nerve | Motor function | Sensory function | Associated site of humerus fracture |
| Axillary |
|
|
|
| Radial |
|
|
|
| Ulnar |
|
|
|
| Median |
|
|
|
- See “Peripheral nerve injuries in the upper extremity“ and “Complications of fractures.”
“Broken ARM:“ Axillary, Radial, and Median nerves can be injured.
Injuries to the median nerve and brachial artery, which both cross the elbow, are common complications of supracondylar fractures.


We list the most important complications. The selection is not exhaustive.

Right forearm
There are multiple erythematous lesions on the fingers and there is a claw-like deformity of the hand. The sharp circular border on the forearm may indicate external compression of the area.
These findings suggest compression-related damage to the forearm muscles, resulting in the typical appearance of Volkmann ischemic contracture.
Source: “Fig 5, In: Management of Volkmann’s Ischemic Contracture: Case Series of 32 patients” by Benabdallah O, Shimi M, Benali HA et al., SICOT-J, licensed under CC BY 4.0.
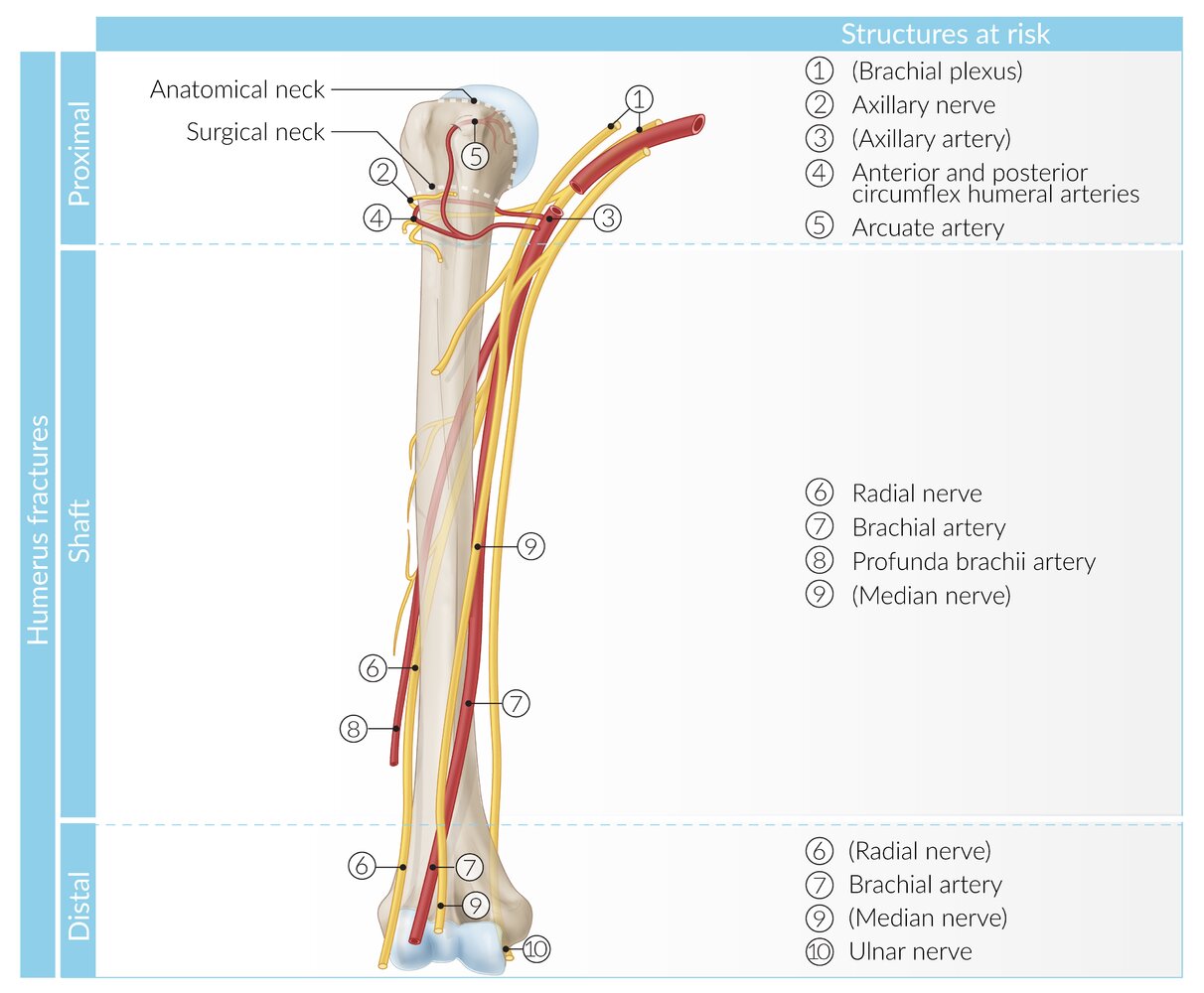
Depending on the location of humerus fractures, different anatomical structures are at risk.
Illustration indicates structures at lower risk of injury in parentheses.
© AMBOSS
References
- Walls R, Hockberger R, Gausche-Hill M, Erickson TB, Wilcox SR. "Rosen's Emergency Medicine 10th edition- Concepts and Clinical Practice E-Book". Elsevier Health Sciences. (2022). ISBN: 9780323757904
- Carofino BC, Leopold SS. "Classifications in brief: the Neer classification for proximal humerus fractures.". Clin Orthop Relat Res. 471(1). :39-43. (2013)
- Emery KH, Zingula SN, Anton CG, Salisbury SR, Tamai J. "Pediatric elbow fractures: a new angle on an old topic". Pediatr Radiol. 46(1). :61-66. (2015)
- Pencle FJ, Varacallo M. "Proximal Humerus Fracture". StatPearls. (2020)