Quick guide
Diagnostic approach
- ABCDE approach
- Targeted clinical evaluation (e.g., mental status, volume status)
- POC glucose
- Serum glucose to confirm hyperglycemia
- Serum osmolality
- Urinalysis for ketones
- Serum β-hydroxybutyrate
- Blood gas analysis
- BMP
- CBC with diff
- Serum lipase
- HbA1c
- Urine tox screen
- Urine pregnancy test in individuals who can become pregnant
- 12-lead ECG
- Chest x-ray
BG < 200 mg/dL does not rule out DKA, especially in patients on SGLT2i therapy or pregnant patients. Check ketones if acidosis is present.
Diagnostic criteria
- DKA: glucose ≥ 200 mg/dL, pH < 7.3, HCO3 < 18 mEq/L, ketones (β-hydroxybutyrate ≥ 3 mmol/L or urine strip ≥ 2+)
- Severe DKA: pH < 7.0, HCO3-< 10 mEq/L, β-OHB > 6 mmol/L, AMS
- HHS: glucose ≥ 600 mg/dL, calculated osmolality > 300 mOsm/kg (or total > 320 mOsm/kg), pH ≥ 7.3, HCO3- ≥ 15 mEq/L, minimal or no ketones
Red flag features
- AMS, lethargy, and/or coma
- Hyperventilation
- Signs of significant dehydration
- Signs of cerebral edema
- Severe abdominal pain
- Nausea and/or vomiting in patients with diabetes
Management checklist
- IV access
- Identify and treat life-threatening causes (e.g., MI, sepsis).
- IV fluid resuscitation with 0.9% NaCl or LR 500–1000 mL/hour
- Replete K+ and maintain levels at 4–5 mEq/L.
- Replete other electrolytes as indicated.
- Start continuous insulin infusion once serum K+ is > 3.5 mEq/L.
- Hourly POC glucose checks
- Consider IV sodium bicarbonate if pH remains < 7.0 despite adequate fluid therapy.
- Add dextrose to IV fluids once POC glucose is < 250 mg/dL.
- Monitor BMP, serum osmolality, and blood gas every 2–4 hours.
- Consider endocrine consult.
- Hospital admission; consider ICU admission (e.g., for severe DKA or HHS, AMS, hemodynamic instability).
Administering insulin when serum K+< 3.5 mEq/L can cause life-threatening hypokalemia due to intracellular shift.
Fluid resuscitation alone lowers glucose; avoid overly rapid correction of glucose and osmolality.
Summary
Hyperglycemic crisis is a condition characterized by severe hyperglycemia and metabolic disturbances and may be the initial manifestation of diabetes mellitus or a complication of diabetes or another condition. Inadequate insulin replacement (e.g., due to poor adherence) or increased insulin demand (e.g., due to acute illness, surgery, or stress) may lead to acute hyperglycemia. In diabetic ketoacidosis (DKA), which is more common in patients with type 1 diabetes (T1DM), no insulin is available to suppress lipolysis, causing ketone formation and acidosis. In a hyperglycemic hyperosmolar state (HHS), which is more common in patients with type 2 diabetes (T2DM), there is still some insulin available and therefore minimal or no ketone formation. Clinical features of both DKA and HHS include polyuria, polydipsia, nausea and vomiting, volume depletion (e.g., dry oral mucosa, decreased skin turgor), and eventually mental status changes and/or coma. Features unique to DKA include breath with a fruity odor, hyperventilation, and abdominal pain. DKA typically has an acute onset (e.g., within hours), while HHS usually develops insidiously (e.g., within days) and manifests with more extreme volume depletion. The mainstay of treatment for both DKA and HHS consists of IV fluid resuscitation, electrolyte repletion, and insulin therapy.
For management of hyperglycemic crises in children, see "Diabetic ketoacidosis in children." For patients with hyperglycemia without DKA or HHS, see also “Diabetes mellitus” and “Inpatient management of hyperglycemia.”


Link to the video version without molecular structures: https://www.youtube.com/watch?v=8nDCV4b1vXA
© AMBOSS
Link to the video version with molecular structures: https://www.youtube.com/watch?v=aAU54OtAVO8
© AMBOSS
© AMBOSS
Overview
| Comparison of DKA and HHS | ||
|---|---|---|
| Diabetic ketoacidosis [1] | Hyperglycemic hyperosmolar state [1] | |
| Insulin |
|
|
| Ketones |
|
|
| Pathogenesis |
|
|
| Signs/symptoms |
|
|
| Labs |
|
|
| Complications |
|
|
| Treatment |
|
|
The most important findings of diabetic ketoacidosis (DKA) are: Delirium/psychosis, Dehydration, Kussmaul respirations, Abdominal pain/nausea/vomiting, fruity (Acetone) breath odor.
© AMBOSS
Link to the video version without molecular structures: https://www.youtube.com/watch?v=8nDCV4b1vXA
© AMBOSS
Link to the video version with molecular structures: https://www.youtube.com/watch?v=aAU54OtAVO8
© AMBOSS
Etiology
-
Lack of or insufficient insulin replacement therapy
- Undiagnosed, untreated diabetes mellitus
-
Treatment failure in known diabetics:
- Insulin pump failure
- Forgotten insulin injection
- Poor adherence to insulin therapy
- Inability to afford treatment
- Use of expired insulin
-
Increased insulin demand
- Stress: infections, surgery, trauma, myocardial infarction, burns, heatstroke
- Drugs: glucocorticoid therapy, cocaine use, alcohol abuse
DKA, often precipitated by infection (e.g., pneumonia, urinary tract infection), is a common initial manifestation of type 1 diabetes mellitus (∼ 30% of cases).
Pathophysiology
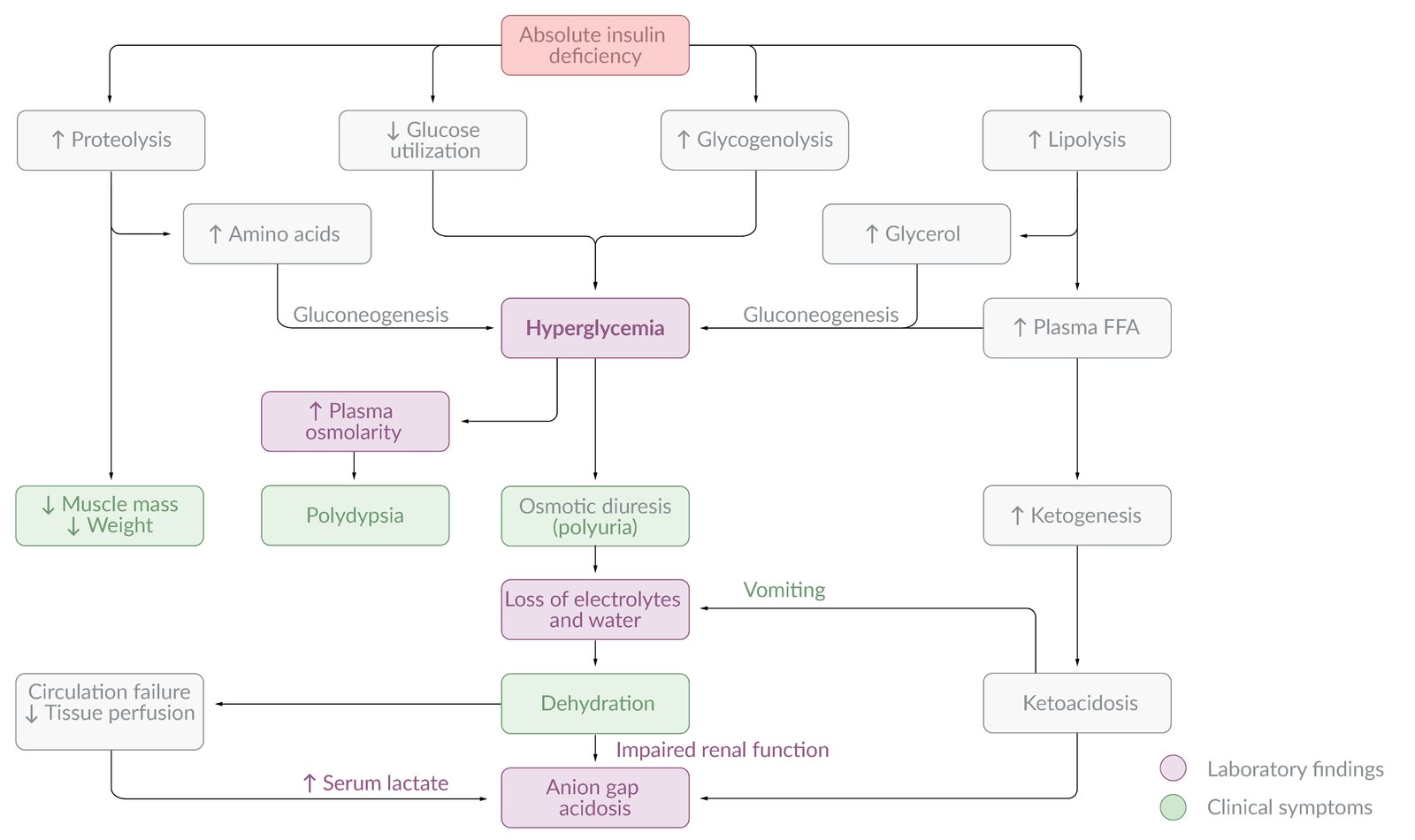
Pathophysiology of diabetic ketoacidosis (DKA)
DKA primarily affects patients with type 1 diabetes.
Osmotic diuresis and hypovolemia
- Insulin normally elevates cellular uptake of glucose from the blood.
- In the insulin-deficient state of DKA, hyperglycemia occurs.
- Hyperglycemia, in turn, leads to progressive volume depletion via osmotic diuresis.
- Insulin deficiency → hyperglycemia → hyperosmolality → osmotic diuresis and loss of electrolytes → hypovolemia
Hypovolemia resulting from DKA can lead to acute kidney injury (AKI) due to decreased renal blood flow! Hypovolemic shock may also develop.
Metabolic acidosis with increased anion gap
- Insulin deficiency increases fat breakdown (lipolysis) through increased activity of hormone-sensitive lipase.
- Metabolic acidosis develops as the free fatty acids generated by lipolysis become ketones, two of which are acidic (acetoacetic acid and beta-hydroxybutyric acid).
- Serum bicarbonate is consumed as a buffer for the acidic ketones. Metabolic acidosis with an elevated anion gap is therefore characteristic of DKA.
- Insulin deficiency → ↑ lipolysis → ↑ free fatty acids → hepatic ketone production (ketogenesis) → ketosis → bicarbonate consumption (as a buffer) → anion gap metabolic acidosis
DKA is an important cause of anion gap metabolic acidosis with respiratory compensation.
Intracellular potassium deficit
- As a result of hyperglycemic hyperosmolality, potassium shifts along with water from inside cells to the extracellular space and is lost in the urine.
- Insulin normally promotes cellular potassium uptake but is absent in DKA, compounding the problem.
- A total body potassium deficit develops in the body, although serum potassium may be normal or even paradoxically elevated.
- Insulin deficiency → hyperosmolality → K+ shift out of cells + lack of insulin to promote K+ uptake → intracellular K+depleted → total body K+ deficit despite normal or even elevated serum K+
There is a total body potassium deficit in DKA. This becomes important during treatment, when insulin replacement leads to rapid potassium uptake by depleted cells and patients may require potassium replacement.

Pathophysiology of hyperglycemic hyperosmolar state (HHS)
- Primarily affects patients with type 2 diabetes
- The pathophysiology of HHS is similar to that of DKA.
- However, in HHS, there are still small amounts of insulin being secreted by the pancreas, and this is sufficient to prevent DKA by suppressing lipolysis and, in turn, ketogenesis.
- HHS is characterized by symptoms of marked dehydration (and loss of electrolytes) due to the predominating hyperglycemia and osmotic diuresis.
© AMBOSS
Clinical features
Signs and symptoms of both DKA and HHS
- Polyuria
- Polydipsia
- Recent weight loss
- Nausea and vomiting
- Signs of significant dehydration
-
Neurological abnormalities
- Altered mental status
- Lethargy
- Coma
- Other neurological examination abnormalities, e.g., blurred vision and weakness
Patients with known diabetes who present with nausea and/or vomiting should be immediately assessed for DKA/HHS.
Specific findings in DKA [2]
- Rapid onset (< 24 h) in contrast to HHS
- Abdominal pain
- Fruity odor on the breath (from exhaled acetone)
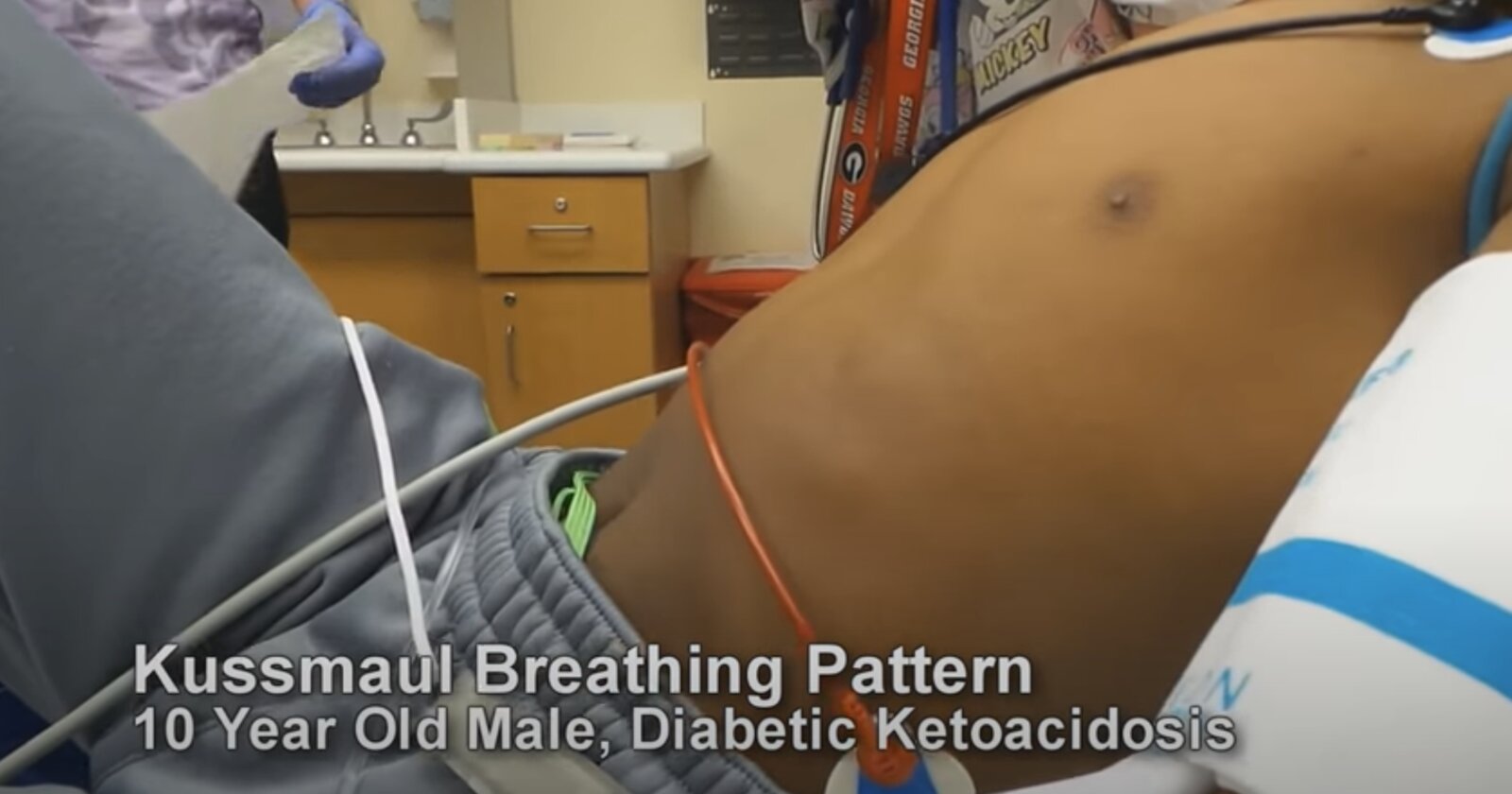
- Hyperventilation: rapid and/or deep breaths (Kussmaul respirations)

Comparison: DKA vs. HHS [1]
| Clinical findings of DKA versus HHS | ||
|---|---|---|
| DKA | HHS | |
| Diabetes | Typically type 1 | Typically type 2 |
| History of severe stress, illness, hospitalization | + | + |
| Polyuria, polydipsia | + | + |
| Nausea, vomiting | + | +/- |
| Dehydration | + | ++ (Profound) |
| Mental status | Usually alert | Usually altered |
| Hyperventilation or Kussmaul breathing | + | - |
| Fruity breath | + | - |
| Severe abdominal pain | + | - |
| Onset | Rapid (< 24 h) | Insidious (days) |
In DKA, absolute insulin deficiency leads to the rapid development of symptomatic acidosis and an early presentation (within hours) with only moderate hyperglycemia (≥ 200 mg/dL). [1]
In HHS, residual insulin production prevents significant ketoacidosis leading to insidious progression (days to weeks) and profound hypovolemia and hyperglycemia (≥ 600 mg/dL). [1]
Diagnosis
Approach [1][3]
- Check serum glucose to confirm hyperglycemia.
- Check BMP for serum bicarbonate, anion gap, electrolytes, and renal function.
- Check for ketones.
- Urine ketones: Standard urine dipstick assays detect acetoacetate and acetone but not β-hydroxybutyrate.
- Serum β-hydroxybutyrate
- Check blood gas analysis for pH. [4]
- Diagnostic workup to evaluate the underlying cause: HbA1c, CBC, ECG, infectious workup
DKA is the diagnosis in patients who have hyperglycemia or a history of diabetes along with elevated ketones (in blood and/or urine) and metabolic acidosis.
HHS is the diagnosis in patients who have hyperglycemia and hyperosmolality.
Diagnostic criteria and severity
Diagnostic criteria of HHS [1][5]
- Hyperglycemia (blood glucose ≥ 600 mg/dL)
- Hyperosmolality (calculated effective serum osmolality > 300 mOsm/kg or total serum osmolality > 320 mOsm/kg)
- Absence of ketonemia and acidosis
Diagnostic criteria and severity of DKA [1][5]
- Hyperglycemia (blood glucose ≥ 200 mg/dL) and/or history of diabetes
- Ketosis (serum β-hydroxybutyrate ≥ 3 mmol/L and/or ≥ 2+ on urine strip)
- Metabolic acidosis (pH < 7.3 and/or bicarbonate < 18 mEq/L)
| Severity of DKA [1] | ||||
|---|---|---|---|---|
| Arterial pH | Serum bicarbonate | Serum β-hydroxybutyrate | Mental status | |
| Mild | 7.26–7.29 | 15–18 mEq/L | 3–6 mmol/L | Alert |
| Moderate | 7.0–7.25 | 10–14 mEq/L | 3–6 mmol/L | Alert or drowsy |
| Severe | < 7.0 | < 10 mEq/L | > 6 mmol/L | Stuporous or comatose |
Laboratory findings in hyperglycemic crises [1]
| Laboratory findings in DKA and HHS [1] | |||
|---|---|---|---|
| Laboratory test | DKA | HHS | |
| BMP | Glucose |
|
|
| Bicarbonate |
|
|
|
| Anion gap |
|
|
|
| Urinalysis |
|
|
|
| Serum β-hydroxybutyrate |
|
|
|
| Blood gas |
|
|
|
| Serum osmolality |
|
|
|

Normal serum osmolality in a stuporous patient rules out HHS; assess for other causes of altered mental status.
Euglycemia does not rule out DKA. Assess ketone levels in all patients with high anion gap metabolic acidosis to evaluate for euglycemic DKA.
Electrolytes and renal function [3][7]
-
Sodium
- Hyponatremia is common in both DKA and HHS due to hypovolemic hyponatremia ; and hypertonic hyponatremia
- Always check corrected sodium for hyperglycemia.
- Potassium in DKA: normal or elevated (despite a total body deficit)
- Magnesium levels are typically low.
- Phosphorus levels may be elevated despite a total body deficit.
- BUN and creatinine are often elevated. [8]
For anion gap calculation, use the measured serum sodium concentration rather than the corrected serum sodium concentration. [9]
Additional diagnostic workup [1][3][10]
Additional diagnostics are indicated depending on suspected precipitating causes and differential diagnoses.
- HbA1c
- Urine pregnancy test [11]
-
Diagnostics for AMS, e.g.:
- CT head
- Toxicology screen
-
Diagnostics for sepsis, e.g.:
- CBC with differential
- Serum lactate
- Diagnostics for myocardial infarction (e.g., 12-lead ECG)
-
Diagnostics for acute abdomen, e.g.:
- Abdominal imaging
- Serum lipase [12]
- Serum transaminases
Rule out infection, myocardial infarction, and pancreatitis in all patients presenting with a hyperglycemic crisis.
Pregnancy and SGLT2-inhibitors can cause euglycemic DKA (i.e., high anion gap metabolic acidosis with normal or near-normal glucose). [11][13]
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
Management
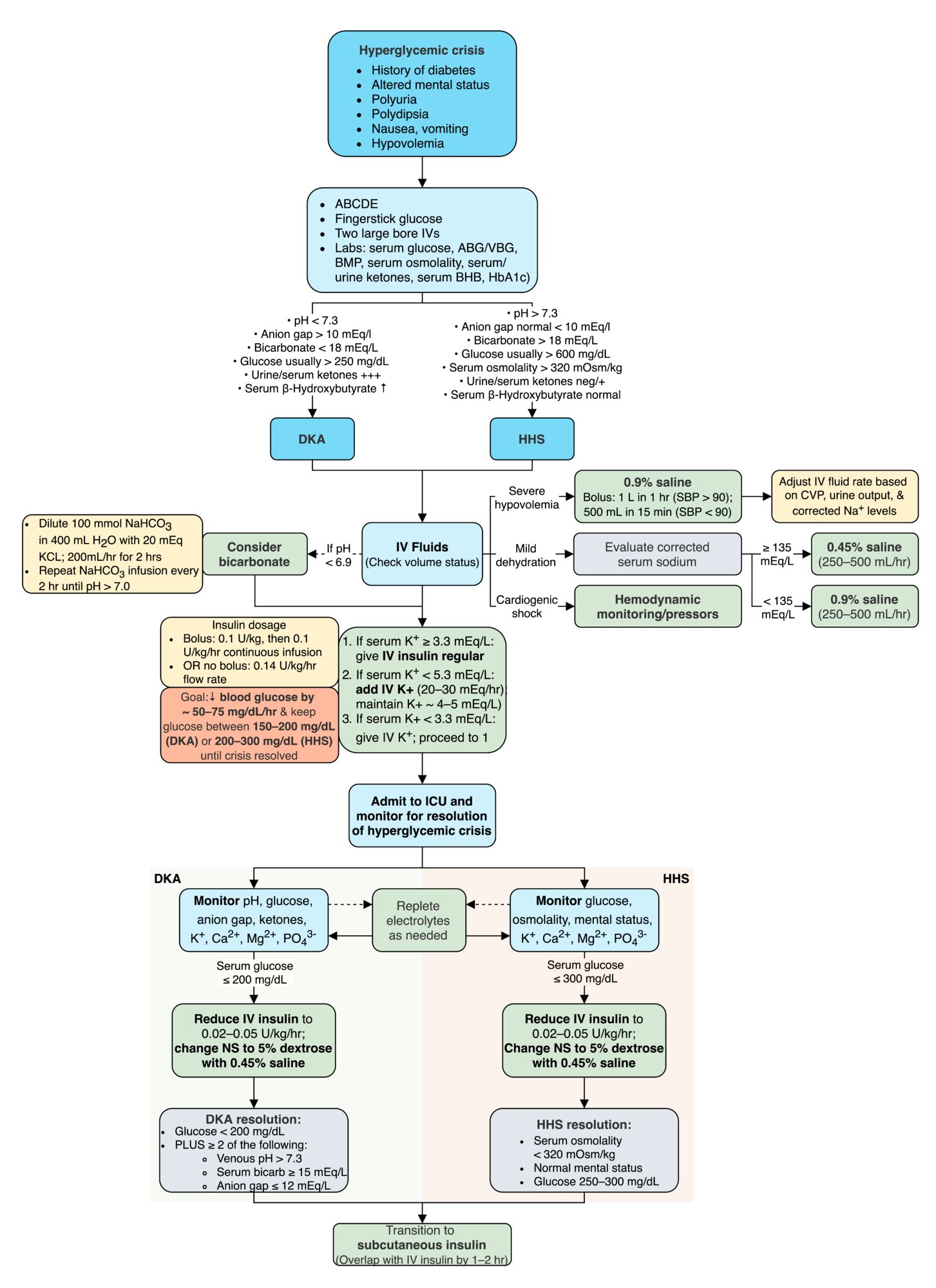
Approach [1][10][14]
-
Initial steps
- ABCDE approach
- Urgent diagnostics (e.g., POC glucose, BMP, blood gas analysis)
- Volume status assessment
-
Principal interventions
- Fluid resuscitation: initially with normal saline (0.9% NaCl) or lactated Ringer's solution
- Potassium repletion: for baseline potassium level ≤ 5 mEq/L
- Insulin therapy: Initiate short-acting insulin as soon as possible once potassium level is > 3.5 mEq/L.
- IV sodium bicarbonate: consider only for severe refractory metabolic acidosis (e.g., pH < 7.0) [1][15]
- Identify and treat precipitating causes (e.g., sepsis).
- Avoid overly rapid correction of serum sodium and osmolality.
- Consider endocrine consult and admission to the ICU.
-
Noninsulin diabetes medications
- Avoid noninsulin agents in patients with T1DM.
- Stop SGLT2 inhibitors.
- Consider use of other noninsulin agents for patients with T2DM in consultation with endocrinology.
The goal of therapy is to resolve hyperglycemia, ketonemia, and acidosis in DKA and hyperglycemia and hyperosmolarity in HHS.
Pregnant patients with DKA should be assessed by an endocrinologist and obstetrician due to the potential for a high-risk pregnancy.

Monitoring [1][16][17]
- All patients
- Hourly vital signs, mental status assessment, and hydration status
- POC glucose every 1–2 hours until hyperglycemic crisis resolves.
- Blood gas and BMP with electrolytes every 2–4 hours ≤ 0.5 mEq/L≤ 10 mEq/L
- HHS: serum osmolality every 2–4 hours until hyperglycemic crisis resolves
- DKA: serum β-hydroxybutyrate every 4 hours until hyperglycemic crisis resolves
Regularly monitor volume status, serum glucose, serum electrolytes, and acid-base status.
Consider cerebral edema (due to overly rapid correction of serum osmolality) in patients with headache, mental status deterioration, seizures, and pupillary changes.
Disposition [1][14][18]
-
Admission
- Indicated for all patients with HHS and most patients with DKA [19]
- Consider ICU admission for patients with any of the following:
- Persistently altered mental status or hemodynamic instability
- Severe DKA or HHS
- Underlying critical illness (e.g., sepsis, MI)
-
Discharge may be considered for patients with mild DKA and all of the following:
- Resolved acidosis
- No concerning precipitating cause
- Toleration of oral hydration and nutrition
- Adequate basal-bolus insulin regimen
- Ability to adhere to discharge instructions, including outpatient follow-up
© AMBOSS
Fluid and electrolyte management
Fluid resuscitation [1][10][16]
- First 2–4 hours: 0.9% NaCl or balanced crystalloid solutions (e.g., lactated Ringer's solution) at 500–1000 mL/hour [1]
- Next 8–12 hours: 0.9% NaCl or crystalloid solution to replace 50% of remaining fluid deficit [1]
-
Within the first 24–48 hours: Adjust IV fluid rate and composition according to CVP, urine output, blood glucose, and corrected sodium levels.
-
Check corrected sodium for hyperglycemia.
- If corrected serum sodium ≥ 135 mmol/L: 0.45% NaCl
- If corrected serum sodium < 135 mmol/L: 0.9% NaCl
-
Check corrected sodium for hyperglycemia.
- Switch to a solution containing dextrose (e.g., D5NS) once glucose falls to < 250 mg/dL. [1]
Carefully monitor for signs of fluid overload during fluid resuscitation, especially in patients with comorbidities (e.g., congestive heart failure, chronic kidney disease). [14]
IV fluids alone can decrease blood glucose concentrations by 50 mg/dL/hour. [1]
To reduce the risk of complications in HHS, ensure that serum sodium levels decline by ≤ 10 mmol/L/day and osmolality decreases by less than 3–8 mOsm/kg/hour. [1]
Electrolyte repletion [1]
-
Potassium
- Potassium levels must be > 3.5 mEq/L before insulin therapy is initiated.
- Initiate potassium replacement if levels are ≤ 5 mEq/L.
- Maintain serum potassium between 4–5 mEq/L.
- Use extreme caution with potassium repletion in anuric patients.
- Monitor potassium levels 2 hours after starting insulin and every 2–4 hours thereafter until hyperglycemic crisis resolves.
- See also “Repletion regimens for hypokalemia.”
| Potassium repletion in hyperglycemic crises [1] | |
|---|---|
| Serum postassium | Recommended dose [1] |
| < 3.5 mEq/L |
|
| 3.5–5.0 mEq/L |
|
| > 5.0 mEq/L |
|
- Phosphorus: Replete only if symptomatic (e.g., muscle weakness, cardiac or respiratory compromise) and phosphorous < 1 mmol/L (see “Repletion regimens for hypophosphatemia”). [1]
- Magnesium: See “Repletion regimens for hypomagnesemia.”
Potassium levels must be > 3.5 mEq/L before administering insulin, as insulin will lower serum potassium and potentially cause severe hypokalemia.
Acid-base status [1]
- Acidosis usually resolves with fluids and insulin therapy; IV sodium bicarbonate is usually unnecessary.
- If pH < 7.0 despite adequate IV fluid resuscitation, administer IV sodium bicarbonate.
Insulin therapy
General principles [1][16][20]
- Insulin is essential to halting lipolysis and ketoacidosis in patients with DKA.
- Recommended regimens
- Initial insulin bolus in DKA if there is a delay in initiating infusion [1]
- Short-acting insulin by continuous IV infusion (e.g., regular insulin in DKA or HHS ) [1]
- Consider treatment with subcutaneous rapid-acting insulin analogues for uncomplicated mild-moderate DKA.
- Consider coadministration of low-dose basal insulin.
- In HHS, ensure blood glucose levels decline by less than 90–120 mg/dL/hour in order to prevent cerebral edema. [1]
- Check glucose level every 1–2 hours and adjust insulin infusion rate as needed.
- In patients requiring ongoing insulin infusion:
- Switch IV fluids to D5NS or D10NS infusion once serum glucose falls to < 250 mg/dL. [1]
- Titrate insulin to a glycemic target of 150–200 mg/dL (in DKA) or 200–250 mg/dL (in HHS). [1]
Resolution of hyperglycemic crises [1]
| Criteria for the resolution of hyperglycemic crises [1][3] | |
|---|---|
| DKA | HHS |
|
|
Transition to subcutaneous insulin [1]
-
Criteria for transitioning to subcutaneous insulin
- Resolution of hyperglycemic crisis
- Precipitating factor identified and treated
- Patient tolerating oral nutrition and eating consistently
-
Procedure for transitioning to subcutaneous insulin
- Stop dextrose infusion.
- Administer a basal-bolus insulin regimen (∼ 50% basal insulin and 50% prandial insulin).
- Estimate total daily dose (TDD) based on: [1]
- Prior outpatient regimen in patients previously on insulin (adjust as needed)
- Weight-based estimates in insulin-naive patients (e.g., 0.3–0.6 units/kg/day) [1]
- IV insulin hourly requirement (e.g., quantity used in the preceding 6 hours)
- Continue IV insulin for 1–2 hours after initiating subcutaneous insulin.
Differential diagnoses
- Other causes of anion gap metabolic acidosis, e.g.:
- Alcoholic ketoacidosis
- Lactic acidosis
- Starvation ketoacidosis
- Toxin ingestion
- Other causes of hyperglycemia and hypovolemia (e.g., sepsis, acute pancreatitis)
- Other causes of AMS, e.g., hypoglycemia
All other causes of altered mental status must be considered in the differential diagnosis of DKA/HHS. Intoxication and other endocrine disorders, as well as gastroenteritis, myocardial infarction, pancreatitis, and other causes of high anion gap metabolic acidosis, should all be excluded.
The differential diagnoses listed here are not exhaustive.
Complications
- Cerebral edema
- Cardiac arrhythmias
- Heart failure, respiratory failure
- Mucormycosis (Mucor and Rhizopus species)
- Hypoglycemia
- Hypokalemia
We list the most important complications. The selection is not exhaustive.
External Resources
References
- Westerberg DP. "Diabetic Ketoacidosis: Evaluation and Treatment". Am Fam Physician. 87(5). :337-346. (2013)
- Umpierrez GE, Davis GM, ElSayed NA, et al. "Hyperglycemic Crises in Adults With Diabetes: A Consensus Report". Diabetes Care. 47(8). :1257-1275. (2024)
- Veauthier B, Levy-Grau B. "Diabetic Ketoacidosis: Evaluation and Treatment". Am Fam Physician. 110(5). :476-486. (2024)
- Kelly A-M. "The case for venous rather than arterial blood gases in diabetic ketoacidosis". Emergency Medicine Australasia. 18(1). :64-67. (2006)
- ElSayed NA, McCoy RG, et al. "6. Glycemic Goals and Hypoglycemia: Standards of Care in Diabetes—2025". Diabetes Care. 48(Supplement_1). :S128-S145. (2024)
- ElSayed NA, McCoy RG, et al. "16. Diabetes Care in the Hospital: Standards of Care in Diabetes—2025". Diabetes Care. 48(Supplement_1). :S321-S334. (2024)
- Kitabchi AE, Umpierrez GE, Miles JM, Fisher JN. "Hyperglycemic Crises in Adult Patients With Diabetes". Diabetes Care. 32(7). :1335-1343. (2009)
- Orban JC, Maizière EM, Ghaddab A, Van Obberghen E, Ichai C. "Incidence and characteristics of acute kidney injury in severe diabetic ketoacidosis.". PLoS ONE. 9(10). :e110925. (2014)
- Beck LH. "Should the actual or the corrected serum sodium be used to calculate the anion gap in diabetic ketoacidosis?". Cleve Clin J Med. 68(8). :673-674. (2001)
- Gosmanov AR, Gosmanova EO, Kitabchi AE, et al. "Hyperglycemic Crises: Diabetic Ketoacidosis (DKA), And Hyperglycemic Hyperosmolar State (HHS)". endotext.org. (2018)
- Kamalakannan D. "Diabetic ketoacidosis in pregnancy". Postgrad Med J. 79(934). :454-457. (2003)
- Yadav D, Nair S, Norkus EP, Pitchumoni CS. "Nonspecific hyperamylasemia and hyperlipasemia in diabetic ketoacidosis: incidence and correlation with biochemical abnormalities". Am J Gastroenterol. 95(11). :3123-3128. (2000)
- Handelsman Y, Henry RR, Bloomgarden ZT, et al. "American Association of Clinical Endocrinologists and American College of Endocrinology Position Statement on the Association of Sglt-2 Inhibitors and Diabetic Ketoacidosis". Endocr Pract. 22(6). :753-762. (2016)
- Walls R, Hockberger R, Gausche-Hill M, Erickson TB, Wilcox SR. "Rosen's Emergency Medicine 10th edition- Concepts and Clinical Practice E-Book". Elsevier Health Sciences. (2022). ISBN: 9780323757904
- Chua HR, Schneider A, Bellomo R. "Bicarbonate in diabetic ketoacidosis - a systematic review". Ann. Intensive Care. 1(1). (2011)
- Van Ness-Otunnu R, Hack JB. "Hyperglycemic Crisis". J Emerg Med. 45(5). :797-805. (2013)
- Savage MW, Dhatariya KK, Kilvert A, et al. "Joint British Diabetes Societies guideline for the management of diabetic ketoacidosis". Diabetic Medicine. 28(5). :508-515. (2011)
- Tintinalli JE, Stapczynski JS, Ma OJ, et al. "Tintinalli's Emergency Medicine: A Comprehensive Study Guide, 9th edition". McGraw Hill Professional. (2019). ISBN: 9781260019940
- Fayfman M, Pasquel FJ, Umpierrez GE. "Management of Hyperglycemic Crises: Diabetic Ketoacidosis and Hyperglycemic Hyperosmolar State". Med Clin North Am. 101(3). :587-606. (2017)
- Kitabchi AE, Umpierrez GE, Fisher JN, Murphy MB, Stentz FB. "Thirty Years of Personal Experience in Hyperglycemic Crises: Diabetic Ketoacidosis and Hyperglycemic Hyperosmolar State". J Clin Endocrinol Metab. 93(5). :1541-1552. (2008)