Summary
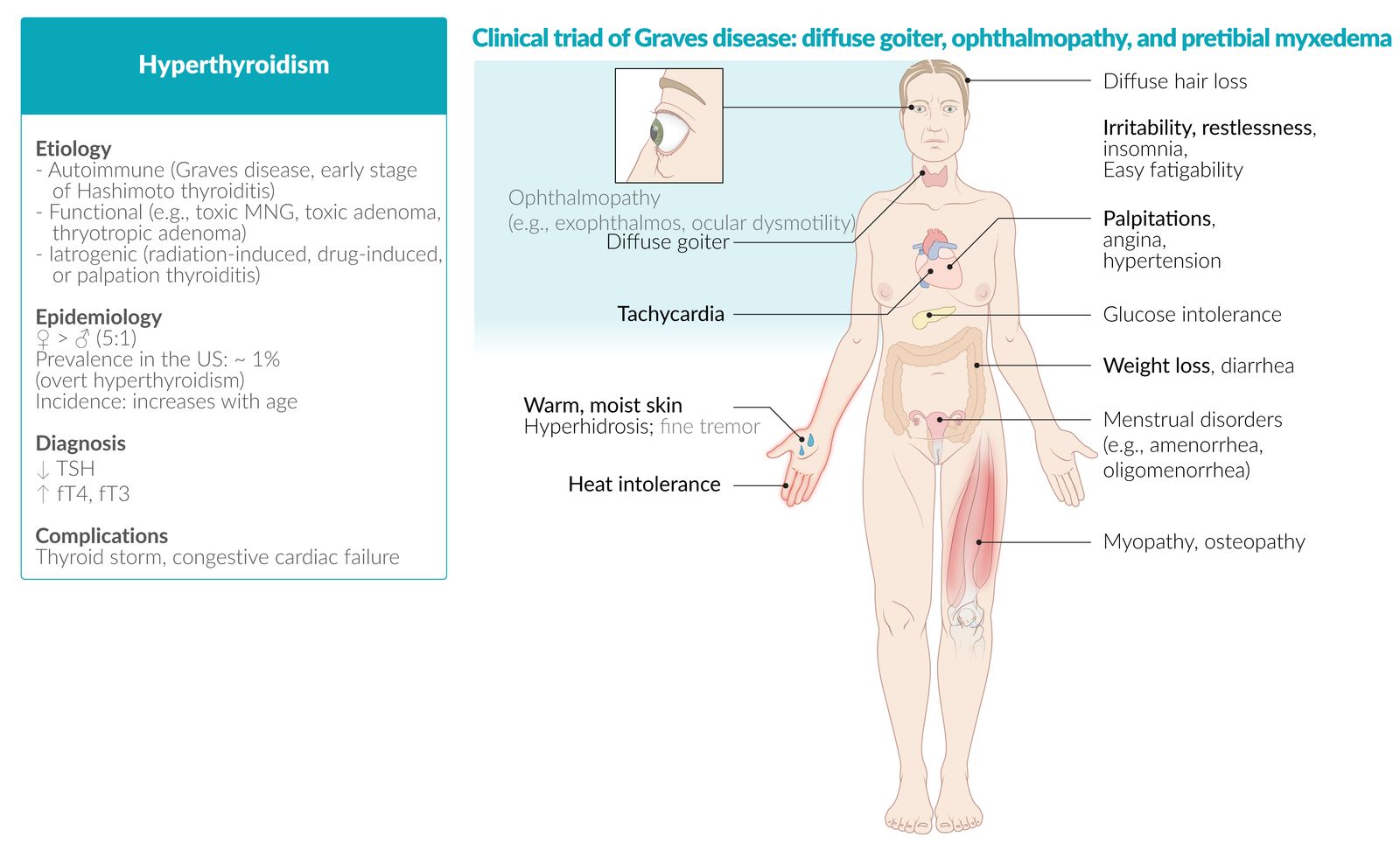
Thyrotoxicosis refers to the symptoms caused by the excessive circulation of thyroid hormones. It is typically caused by thyroid gland hyperactivity (i.e., hyperthyroidism), the most common causes of which are Graves disease (most common), toxic multinodular goiter (MNG), and toxic adenoma. It may also be caused by the inappropriate release of thyroid hormone from a damaged or inflamed thyroid gland (e.g., thyroiditis). In rare cases, thyrotoxicosis is caused by TSH-producing pituitary tumors (central hyperthyroidism), excessive production of hCG (e.g., in gestational trophoblastic disease), or oral intake of thyroid hormones (exogenous hyperthyroidism). The most common symptoms of thyrotoxicosis include fatigue, anxiety, heat intolerance, increased perspiration, palpitations, and significant weight loss despite increased appetite. Thyroid function tests (TFTs) confirm thyrotoxicosis, while TSH receptor antibodies, thyroid ultrasonography, and radioactive iodine uptake tests are used to identify the etiology. Management of any form of thyrotoxicosis involves the initial control of symptoms with beta blockers and antithyroid drugs, often followed by definitive therapy with either radioactive iodine ablation (RAIA) of the thyroid gland or thyroid surgery. An acute exacerbation of thyrotoxicosis can lead to a life-threatening hypermetabolic state known as thyroid storm, which is diagnosed clinically along with thyroid function tests. Patients with thyroid storm require urgent stabilization in critical care settings with fluids, beta blockers, antithyroid medications (propylthiouracil, potassium iodide, and parenteral glucocorticoids), active cooling, and management of tachyarrhythmias. Definitive therapy with RAIA or surgery is considered once they are stable.

© AMBOSS
Definitions
While thyrotoxicosis and hyperthyroidism are often used interchangeably, the two terms are not synonymous. [1]
- Thyrotoxicosis: a hypermetabolic condition caused by an inappropriately high level of circulating thyroid hormones irrespective of the source.
-
Hyperthyroidism: a condition characterized by the overproduction ; of thyroid hormones by the thyroid gland; can cause thyrotoxicosis
-
Overt hyperthyroidism
- ↓ Serum TSH levels with ↑ serum free T4 and/or T3 levels
- Patients typically experience symptoms of thyrotoxicosis.
-
Subclinical hyperthyroidism
- ↓ Serum TSH levels with normal serum free T4 and T3 levels
- Patients are normally asymptomatic or mildly symptomatic.
- May progress to overt hyperthyroidism
-
Overt hyperthyroidism
Overview
| Overview of common etiologies in hyperthyroidism and thyrotoxicosis [2][3][4][5][6][7][8] | ||||||
|---|---|---|---|---|---|---|
| Graves disease | Toxic MNG | Subacute granulomatous thyroiditis (de Quervain thyroiditis) | Subacute lymphocytic thyroiditis (silent thyroiditis) | Iodine-induced hyperthyroidism | ||
| Thyroid status |
|
|
|
|
||
| Epidemiology |
|
|
|
|
||
| Causes |
|
|
|
|
|
|
| Goiter | Consistency |
|
|
|
|
|
| Pain |
|
|
|
|
|
|
| Other findings |
|
|
|
|
||
| Thyroid function tests |
|
|
|
|
||
| Antibodies |
|
|
|
|
||
| Iodine uptake on scintigraphy |
|
|
|
|
||
| Histopathological findings |
|
|
|
|
|
|
Epidemiology
-
Prevalence [9]
- Overt hyperthyroidism: ∼ 1%
- Subclinical hyperthyroidism: 2–3%
- Sex: ♀ > ♂ (5:1)
- Age range at presentation [10]
- Graves disease: 20–30 years of age
- Toxic adenoma: 30–50 years of age
- Toxic MNG: peak incidence > 50 years of age
References:[11][12]
Epidemiological data refers to the US, unless otherwise specified.
Etiology
-
Hyperfunctioning thyroid gland
- Graves disease (∼ 60–80% of cases)
- Toxic MNG (∼ 15–20% of cases)
- Toxic adenoma (3–5% of cases)
- TSH-producing pituitary adenoma (thyrotropic adenoma)
- hCG-mediated hyperthyroidism: e.g., gestational transient thyrotoxicosis (GTT), gestational trophoblastic disease (GTD)
-
Destruction of the thyroid gland (destructive thyroiditis)
- Thyroiditis (see “Subacute thyroiditis”)
- Subacute granulomatous thyroiditis (de Quervain thyroiditis)
- Subacute lymphocytic thyroiditis (e.g., postpartum thyroiditis)
- Drug-induced thyroiditis (e.g., amiodarone, lithium)
- Contrast-induced thyroiditis (Jod-Basedow phenomenon)
- Hashitoxicosis (see “Hashimoto thyroiditis”)
- Radiation thyroiditis
- Palpation thyroiditis: due to thyroid gland manipulation during parathyroid surgery.
- Riedel thyroiditis
- Thyroiditis (see “Subacute thyroiditis”)
- Exogenous thyrotoxicosis
-
Ectopic (extrathyroidal) hormone production
- Struma ovarii
- Metastatic follicular thyroid carcinoma
References:[2][13][14]
Pathophysiology
Hypothalamic-pituitary-thyroid axis
The hypothalamus, anterior pituitary gland, and thyroid gland, together with their respective hormones, make up a self-regulating circuit known as the hypothalamic-pituitary-thyroid axis.
- Physiological regulation: See “Thyroid gland” in “General endocrinology.”
-
Hyperthyroidism
- Disorders of the thyroid gland → excess production of T3/T4 → compensatory decrease of TSH
- Thyrotropic adenoma → ↑ TSH levels → ↑ T3/T4 levels
- Other causes of thyrotoxicosis
- Excess intake/ectopic production of thyroid hormone → ↑ levels of circulating T3/T4 → compensatory decrease of TSH
- Trigger ; → inflammation of the thyroid gland → cellular damage and destruction → inappropriate release of T3/T4
Effects of thyrotoxicosis
-
Generalized hypermetabolism (increased substrate consumption)
- ↑ Number of Na+/K+-ATPase → elevation of basal metabolism → promoted thermogenesis
- Upregulation of β-adrenergic receptors → hyperstimulation of the sympathetic nervous system
-
Cardiac effects (increased cardiac output) [15]
- ↑ Numbers of ATPase on cardiac myocytes; ↓ amount of phospholamban (PLB) → ↑ transsarcolemmal Ca2+ movement → enhanced myocardial contractility
- ↓ Peripheral vascular resistance
Clinical features
-
General
- Heat intolerance
- Excessive sweating because of increased cutaneous blood flow
- Weight loss despite increased appetite
- Frequent bowel movements (because of intestinal hypermotility)
- Weakness, fatigue
-
Skin
- Infiltrative dermopathy, especially in the pretibial area (pretibial myxedema)
-
Onycholysis
- An early cutaneous manifestation of hyperthyroidism
- Thickened nails with distal white discoloration and separation of the nail plate
- Initially develops in the fourth fingers, but can involve all nails, including the toenails
- Thyroid acropachy: nail clubbing seen in late stages of Graves disease
-
Eyes
- Lid lag: caused by adrenergic overactivity, which results in spasming of the smooth muscle of the levator palpebrae superioris
- Lid retraction: “staring look”
- Graves ophthalmopathy (exophthalmos, edema of the periorbital tissue)
-
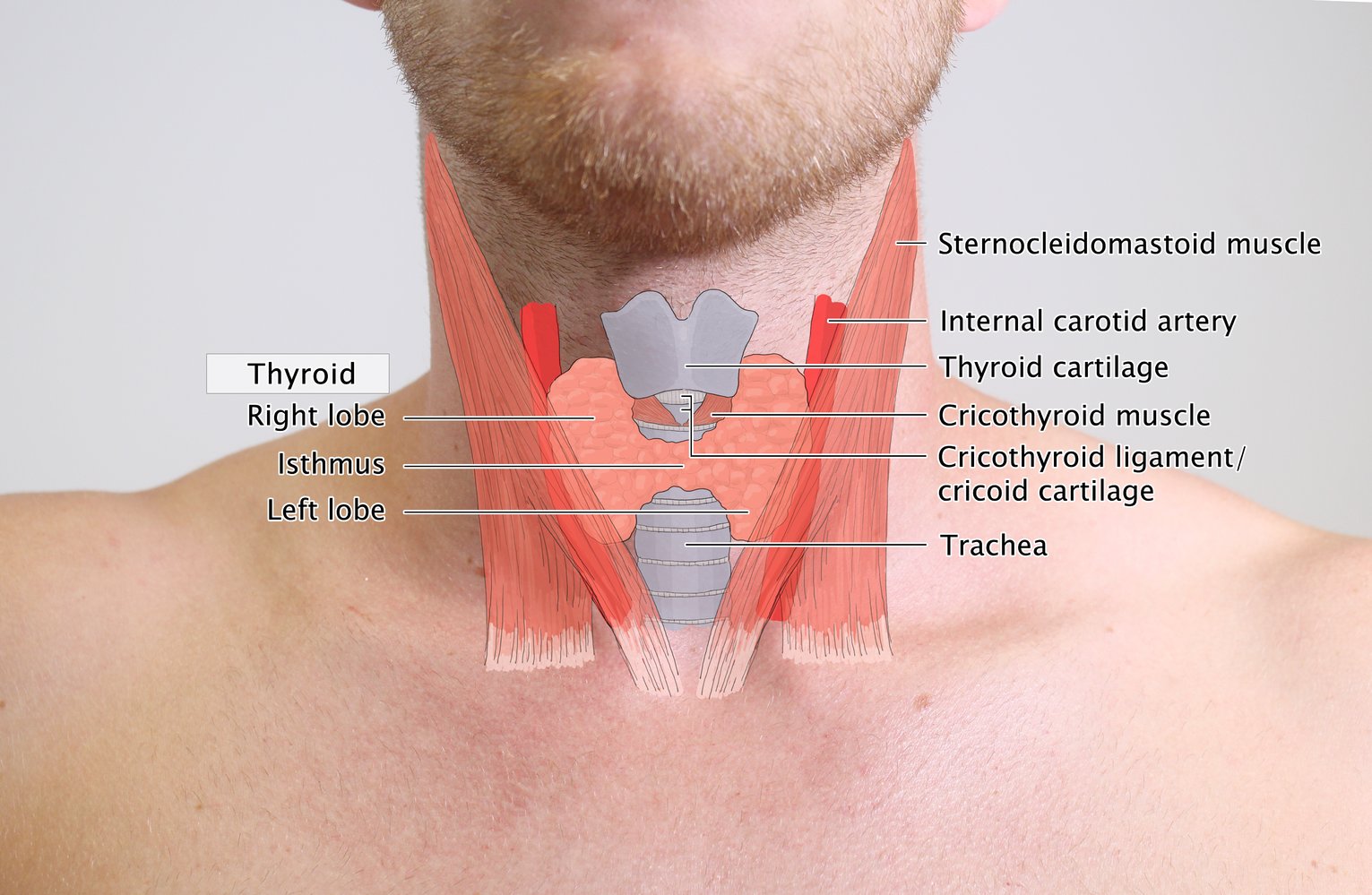
Goiter
- Diffuse, smooth, nontender goiter
- Often with an audible bruit at the superior poles
- Also seen in subacute thyroiditis, toxic adenoma, and toxic MNG
-
Cardiovascular
- Tachycardia
- Palpitations, irregular pulse (due to atrial fibrillation/ectopic beats)
-
Hypertension with widened pulse pressure
- Systolic pressure is increased due to increased heart rate and cardiac output.
- Diastolic pressure is decreased due to decreased peripheral vascular resistance.
- Thyrotoxicosis-induced cardiac failure; : elderly patients often present with features of cardiac failure (e.g., pedal edema, exertional dyspnea).
- Abnormal heart rhythms, including atrial fibrillation
- Chest pain
-
Musculoskeletal
- Fine tremor of the outstretched fingers
-
Hyperthyroid myopathy: a condition of muscle weakness, pain, and atrophy associated with hyperthyroidism (e.g., from Graves disease, thyroiditis)
- Predominantly affects individuals > 40 years of age
- Can develop acutely or several weeks to months after the onset of hyperthyroidism.
- Typically affects proximal muscles (e.g., hip flexors, quadriceps) more than distal muscles
- Serum creatine kinase levels are most often normal
- Treatment of hyperthyroidism often reverses myopathy
- Osteopathy: osteoporosis due to the direct effect of T3 on osteoclastic bone resorption , fractures (in the elderly)
-
Endocrinological
- Female: oligomenorrhea, amenorrhea, anovulatory infertility, dysfunctional uterine bleeding
- Male: gynecomastia, decreased libido, infertility, erectile dysfunction
-
Glucose intolerance [16]
- ↓ Insulin sensitivity of peripheral tissue
- Impaired insulin secretion
-
Neuropsychiatric system
- Anxiety
- Emotional instability
- Depression
- Restlessness
- Insomnia
- Tremoulousness (results from the hyperadrenergic state)
- Hyperreflexia




© AMBOSS
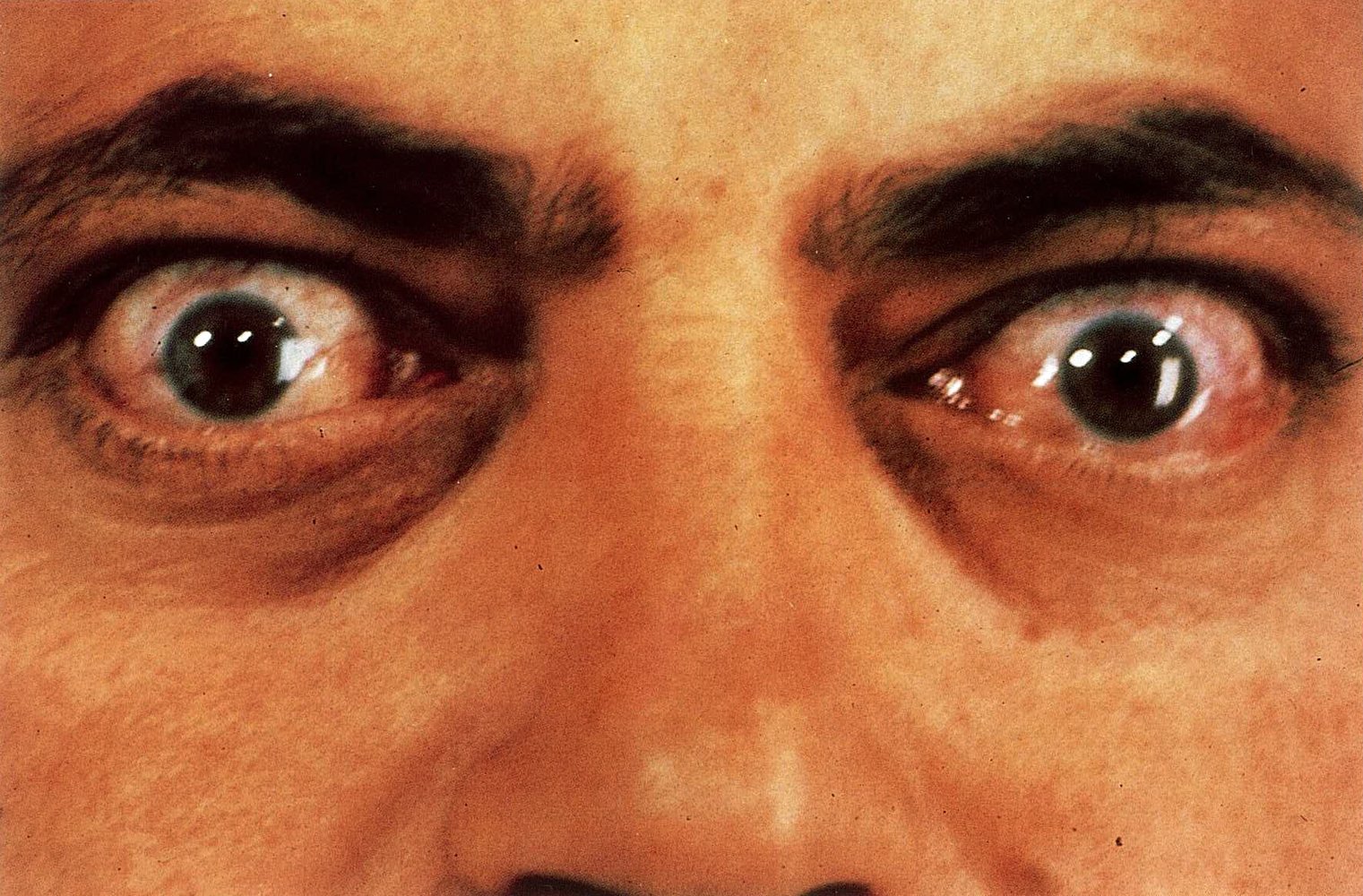
The patient's sclerae are visible at the upper margin of the cornea (Dalrymple sign) due a widening of the palpebral fissure caused by upper eye lid retraction. In addition, chemosis and conjunctival injection are evident.
This combination of these signs is classical for Graves ophthalmopathy.
Source: © IMPP

The neck is asymmetrical and the thyroid gland is enlarged. The green hatched overlay represents the normal size of a thyroid; the light green overlay is the estimated size of this patient's thyroid.
© AMBOSS
© AMBOSS

© AMBOSS
Subtypes and variants
Exogenous thyrotoxicosis
Etiology [17][18]
Exogenous thyrotoxicosis is caused by excessive intake of thyroid hormone.
- Intentional
- Therapeutic: suppressive doses of thyroid hormones for thyroid cancer treatment
- Related to psychiatric illness (e.g., eating disorders, body dysmorphia, or factitious disorders) [19]
- Attempting weight loss
-
Unintentional
- Iatrogenic
- Accidental ingestion (primarily in children) [17]
- Dietary supplements
Clinical features [17][20]
- Symptoms of thyrotoxicosis
- Goiter is absent. [21]
Diagnostics [17][20]
- Low/undetectable TSH
- High levels of T4 and/or T3; T3:T4 ratio < 20 ng/mcg [17]
- Low Tg levels
- Low RAI uptake on scintigraphy [22]
Treatment [17]
- Taper and stop the exogenous thyroid hormone. [19]
- Consider symptomatic therapy for thyrotoxicosis with beta blockers if symptoms are severe.
- Consider psychiatric consultation, depending on the reason for ingestion. [19]
- For severe thyrotoxicosis, consider: [17]
- Cholestyramine (which binds to T3 and T4 in the intestine and interrupts the enterohepatic circulation) [17]
- Charcoal hemoperfusion [17]
Diagnosis
For neonates or pregnant individuals, see “Special patient groups” for additional information.
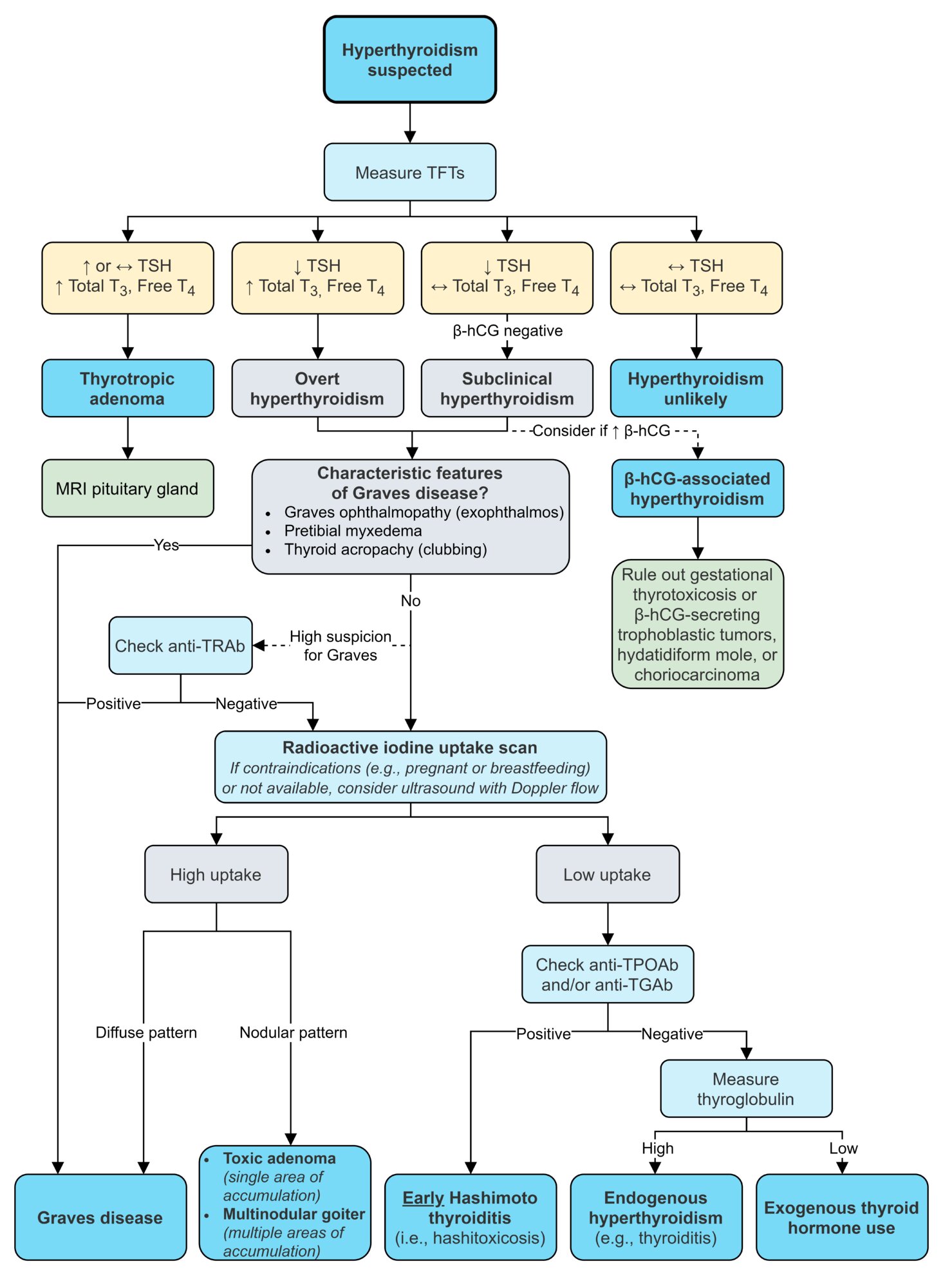
Approach
-
Initial evaluation: perform clinical assessment and screen thyroid function tests (TFTs) alongside routine laboratory studies.
- Consider alternate diagnoses if TFTs are normal.
- If characteristic features of Graves disease are present: can stop investigations and begin management of Graves disease.
- Identify any tachyarrhythmia requiring treatment (see also “Atrial fibrillation” and “Acute management of tachycardia”).
-
Subsequent evaluation depends on the clinical picture . Options include:
- Thyroid scintigraphy: first-line for most patients with uncertain diagnoses, e.g., suspected thyroid adenoma or toxic MNG
- TSH receptor antibody (TRAb): for suspected Graves disease without characteristic features
- Thyroid ultrasound: first-line for pregnant/lactating patients, palpable nodules or suspected thyroiditis
-
Further evaluation: based on initial results
- Normal imaging and negative TRAb: consider serum thyroglobulin to identify exogenous thyrotoxicosis
- Inconclusive imaging and negative TRAb: consider thyroid peroxidase antibodies to identify thyroiditis
- Suspicious nodules visible on imaging: refer for FNAC (see also “Thyroid nodules”)

Initial evaluation [17][23]
-
Thyroid function tests
- Thyroid-stimulating hormone (TSH) level (initial screening test): Typically low/undetectable; a normal TSH level usually rules out hyperthyroidism.
- Free T4 (FT4) and total T3 levels: Typically both elevated; indicated when thyrotoxicosis is strongly suspected or TSH is abnormal
| Interpretation of elevated thyroid hormones [17][23] | |||
|---|---|---|---|
| Condition | TSH level | Free T4 | Total T3 |
| Overt hyperthyroidism and thyrotoxic-phase thyroiditis | ↓ | ↑ In 90% of cases | ↑ |
| Subclinical hyperthyroidism | ↓ | Normal | Normal |
| Early pregnancy | ↓ | Normal | Normal |
| Exogenous thyrotoxicosis or hyperthyroidism in older adults/comorbid illness | ↓ | ↑ | Normal or ↑ |
| Thyrotropic adenoma | Normal or ↑ | ↑ | ↑ |
-
Routine laboratory studies
- CBC: leukocytosis and/or mild anemia
-
BMP
- Hyperglycemia
- Mild hypercalcemia
- Liver chemistries: mildly elevated AST, ALT, ALP, and bilirubin
- Serum cholesterol: decreased total cholesterol, LDL, and HDL
- ESR: typically elevated (> 100 mm/hour) in subacute thyroiditis
-
ECG findings
- Tachycardia
- Atrial fibrillation
- LBBB and ECG signs of LVH in patients with dilated cardiomyopathy
Subsequent evaluation
Indicated if the diagnosis remains uncertain after clinical assessment and initial evaluation. The choice and priority of studies depends on the clinical picture, patient characteristics and test availability.
TSH receptor antibody (TRAb)
- Indication: if Graves disease is suspected but classic clinical features are absent [17]
-
Interpretation
- Positive: Diagnosis of Graves disease is established.
- Negative: Further investigation is necessary. [17]
Nuclear medicine thyroid scan and radioactive iodine uptake measurement[24]
-
Definitions
- Nuclear medicine thyroid scan: a nuclear medicine imaging technique that visualizes the distribution of thyroid function; using an oral or IV radiotracer (most commonly Tc-99m pertechnetate or iodine-123)
- Radioactive iodine uptake measurement (RAIU test): a test that quantifies the percentage of the administered amount of radioactive iodine taken up by the thyroid gland [25]
-
Indications [17]
- First-line test for most patients with uncertain etiology of thyrotoxicosis after initial evaluation
- Assessment of functional status of thyroid nodules [25]
- Thyroid malignancy
- Identification of ectopic thyroid tissue (e.g., lingual thyroid, struma ovarii)
- Evaluation of retrosternal goiters
- Evaluation of thyroglossal cysts
- Contraindications: pregnant or breastfeeding women [17]
-
Findings
- Hot nodule: Hyperfunctioning tissue takes up large amounts of radioactive iodine
- Cold nodule: Non-functioning nodules do not take up any radioactive iodine and appear "cold”, but the surrounding normal thyroid tissue takes up radioactive iodine and appears "warm"
- See also “Diagnostics” in “Thyroid cancer” and “Diagnostic steps for thyroid nodules”
| Characteristic findings of nuclear medicine thyroid scan and RAIU measurement [24] | ||
|---|---|---|
| Appearance of thyroid | RAIU measurement | |
| Normal thyroid tissue |
|
|
| Graves disease |
|
|
| Toxic MNG |
|
|
| Toxic adenoma |
|
|
| Destructive thyroiditis |
|
|
| Exogenous thyrotoxicosis |
|
|
| Thyrotropic adenoma |
|
|



Thyroid ultrasound with Doppler
-
Indications [22]
- Palpable abnormality, e.g., goiter or nodules
- Additional study following nuclear medicine thyroid scan or second-line initial imaging study
- Preferred imaging technique in pregnant or breastfeeding women
-
Typical findings [22]
- Changes to morphology: diffuse enlargement or nodules
- Increased perfusion: either diffuse (Graves disease, toxic adenoma) or nodular (toxic MNG)
- Decreased perfusion: destructive thyroiditis
- Hypoechoic areas in acute thyroiditis and malignancy





Further evaluation
These additional tests are not routinely required but may be performed depending on the suspected underlying etiology.
-
Ultrasound-guided FNAC
- Consider for suspicious nodules (see “Diagnostic steps for thyroid nodules” and “Indications for FNAC in thyroid nodules”).
- Can help confirm etiology if diagnosis remains uncertain (see “Pathological findings” in “Common causes of thyrotoxicosis”)
-
Other thyroid antibodies [17]
-
Thyroid peroxidase antibodies (TPOAb)
- Indication: suspected subacute lymphocytic thyroiditis, including postpartum thyroiditis
- Elevated levels may also be seen in Graves disease.
- Thyroglobulin antibodies (TgAb): not routinely indicated but can be elevated in Graves disease, autoimmune conditions, and thyroid cancer
- See also “Thyroid antibodies.”
-
Thyroid peroxidase antibodies (TPOAb)
-
Serum thyroglobulin (Tg): indicated for suspected exogenous hyperthyroidism with unclear history
- Serum Tg should be assessed alongside TgAb because a TgAb-positive result indicates an unreliable serum Tg finding. [17]
- Findings
- Exogenous hyperthyroidism: ↓ Tg due to production that is suppressed by the administered thyroid hormones
- Endogenous hyperthyroidism: normal or ↑ Tg
© AMBOSS
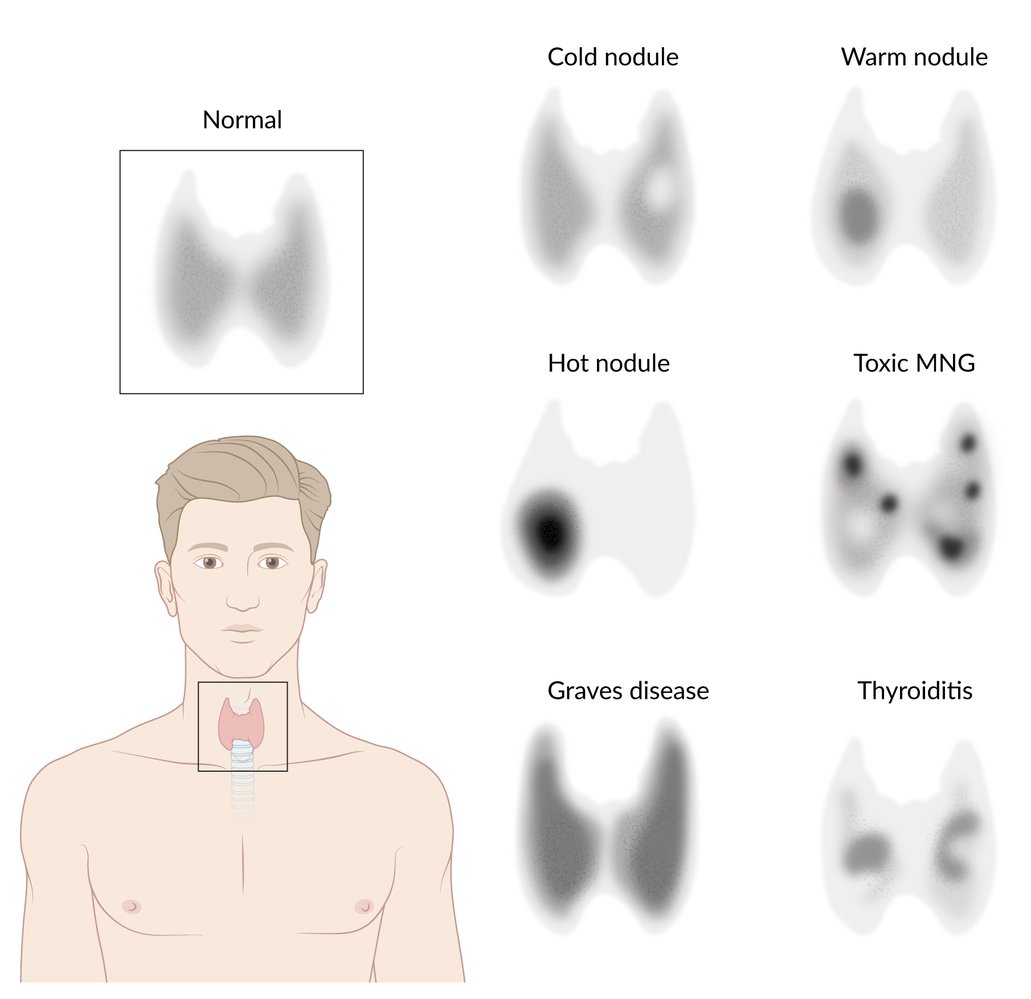
Overview of radioactive iodine uptake patterns in hyperthyroidism
Toxic MNG: Toxic multinodular goiter
© AMBOSS

Thyroid scintigraphy (99mTc pertechnetate)
The thyroid appears significantly enlarged, with a 99mTc uptake of 25% (normal values: 0.5–2%).
This finding is consistent with Graves disease.
Source: © IMPP
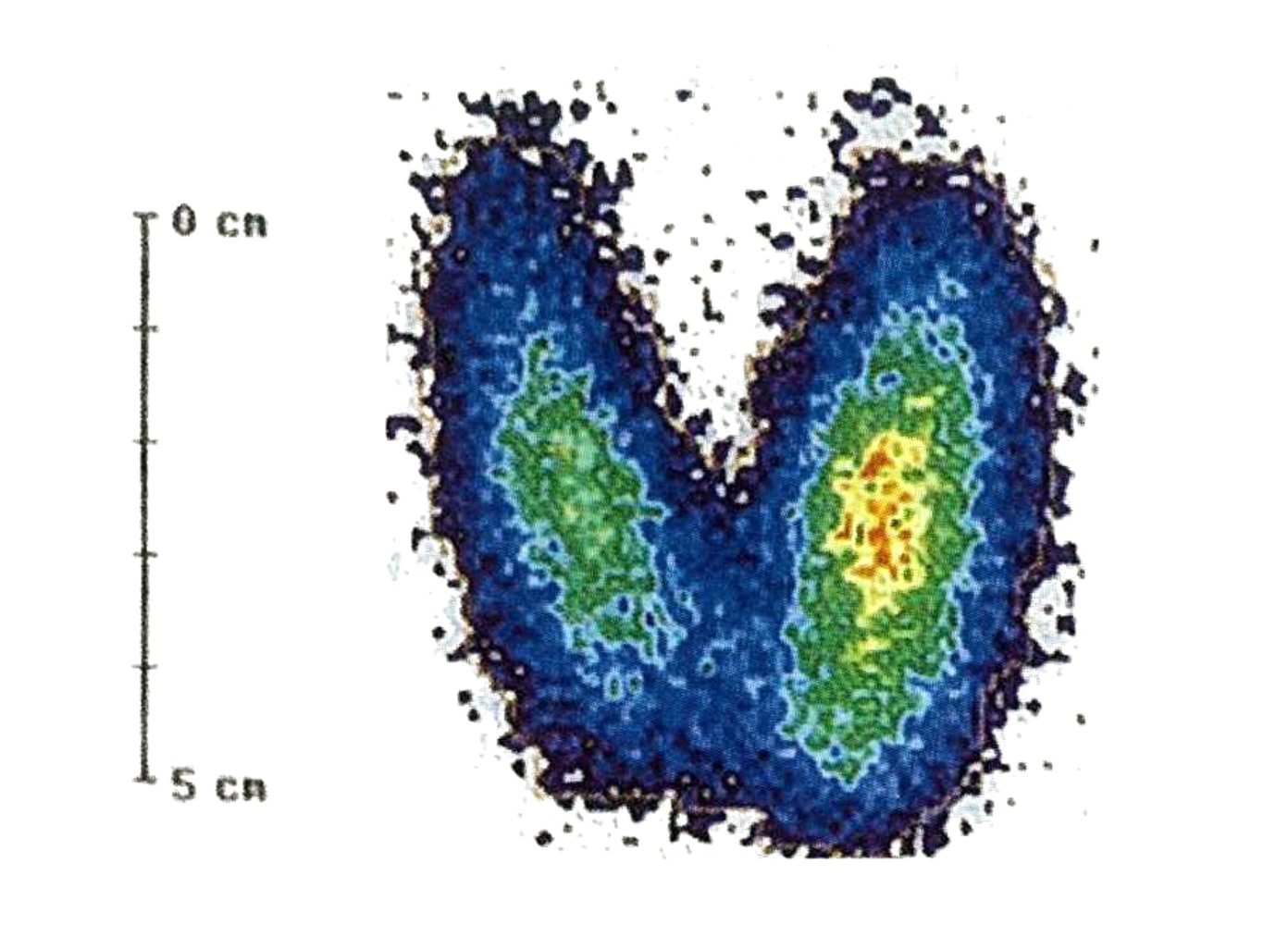
Thyroid scintigraphy
The thyroid appears enlarged. There is also homogeneous radionuclide uptake. Blue indicates poor uptake, with increasing uptake indicated by green, then yellow, then red.
These findings are typical of Graves disease.
Source: © IMPP
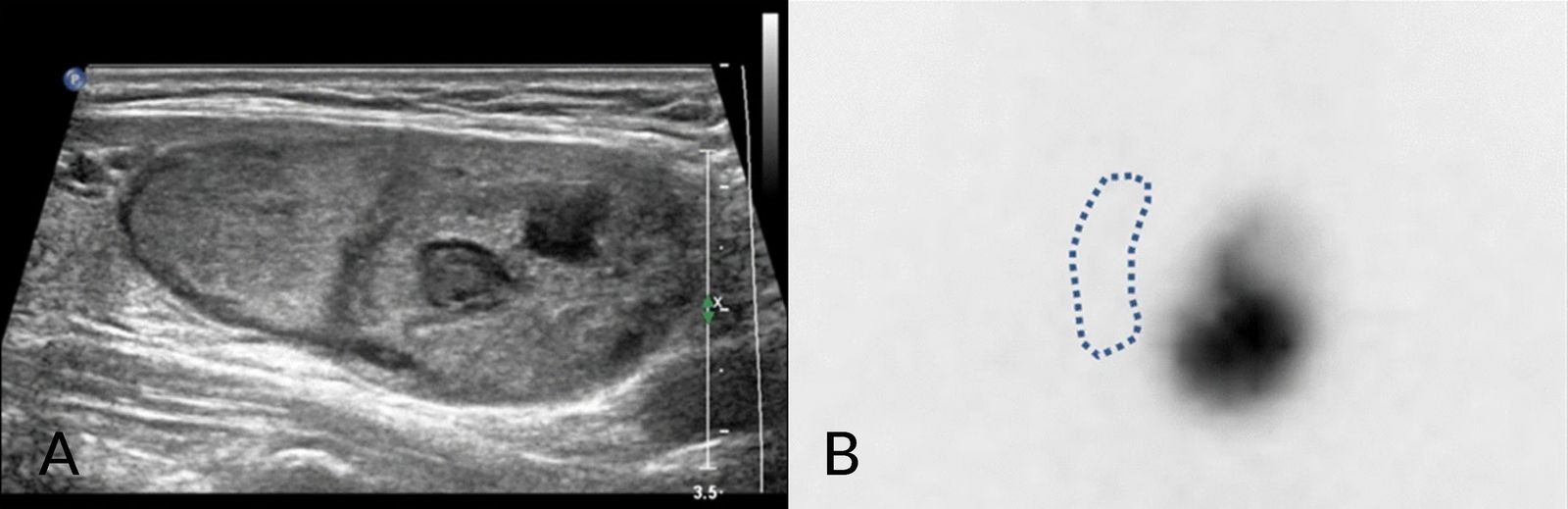
A. Ultrasound thyroid (left lobe); B. Nuclear medicine thyroid scan (technetium-99m pertechnetate; anterior view) of patient with T3 thyrotoxicosis
A complex solid nodule (blue overlay) in the left thyroid lobe is slightly hypoechoic relative to surrounding normal thyroid parenchyma (T). The nodule (N) shows markedly increased tracer uptake while right thyroid lobe uptake is suppressed (dashed line).
Source: “Fig. 1, in: Quantitative Iodine-123 single-photon emission computed tomography/computed tomography for Iodine-131 therapy of an autonomously functioning thyroid nodule” by Lee WW, Song YS, So Y, European Journal of Hybrid Imaging , licensed under CC BY 4.0. Modifications: Image is a combination of figure 1b and 1c, added letters A and B . The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
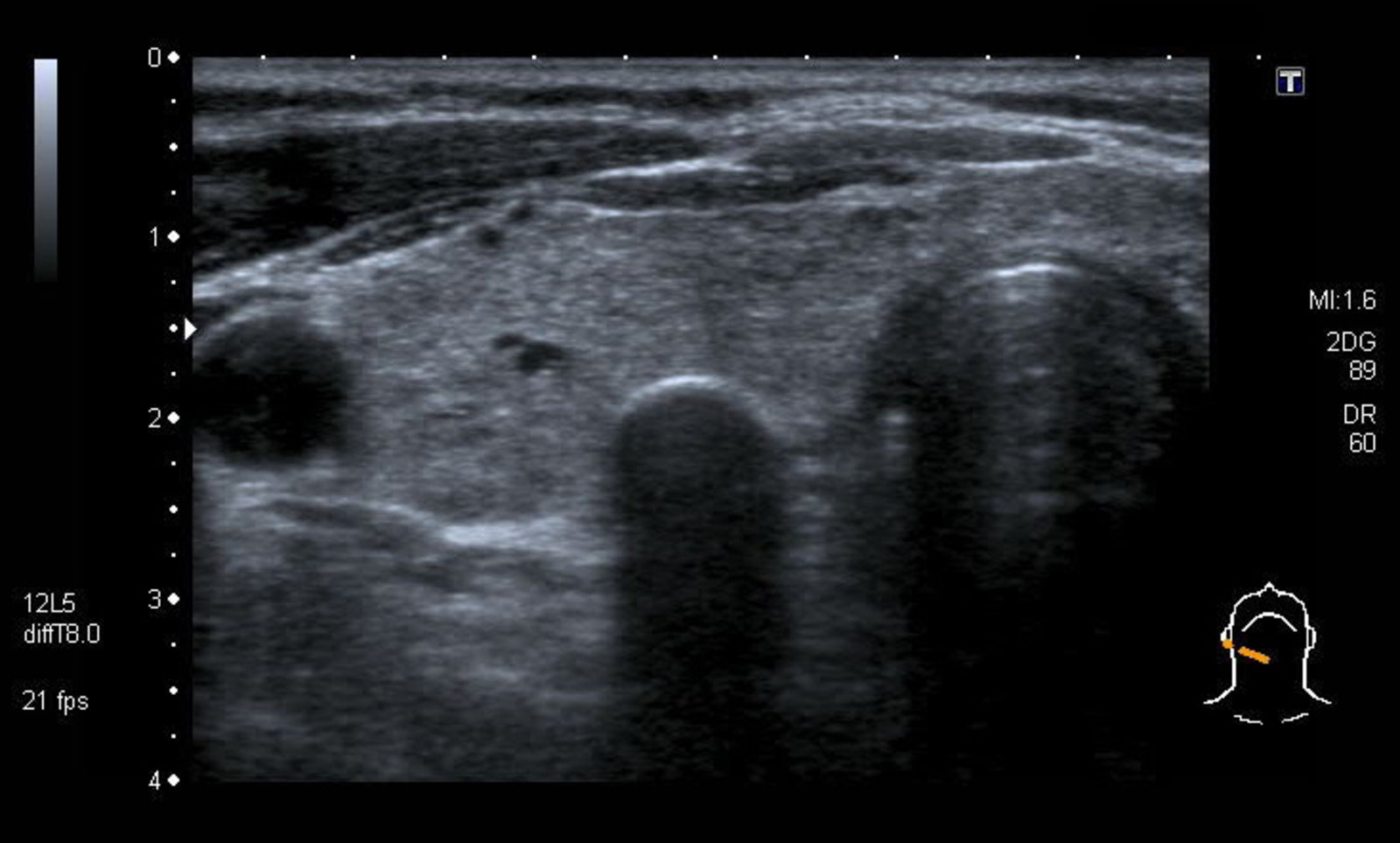
Ultrasound thyroid (transverse plane)
A crescent-shaped, hyperechoic structure (yellow overlay) in the right thyroid lobe (blue overlay) producing marked posterior acoustic shadowing (indicated by white overlay and lines) corresponds to rim calcification along the anterior margin of a thyroid nodule. The internal components of the nodule are completely obscured and cannot be assessed. The nodule scores as moderately suspicious using the Thyroid Imaging Reporting and Data System (TI-RADS) risk stratification system.
CA: carotid artery; T: trachea
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.
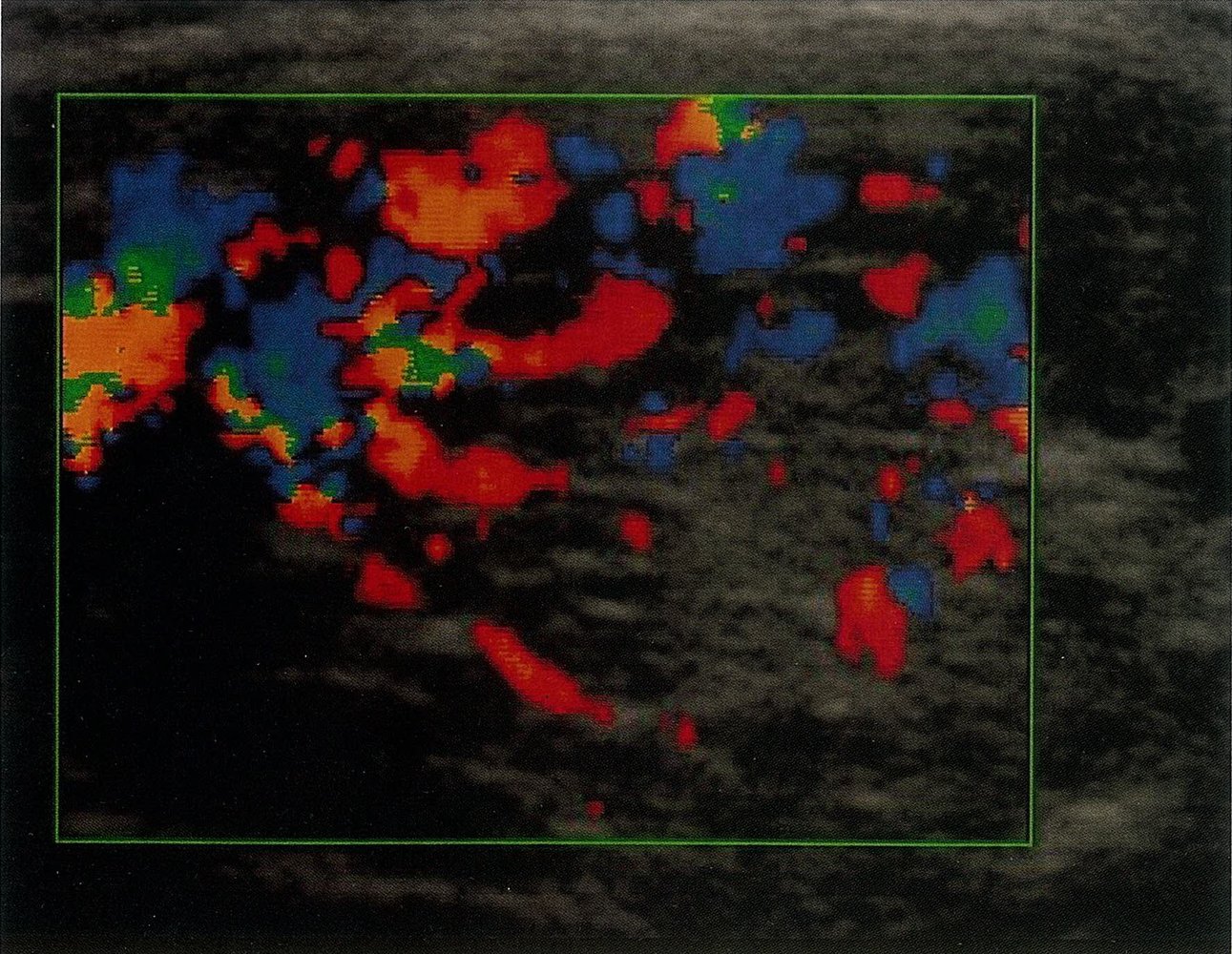
Ultrasound left thyroid lobe (with color Doppler; longitudinal plane)
On B-mode, the thyroid lobe (dotted line) appears heterogeneous with hyperechoic and hypoechoic areas. Color Doppler image window (green rectangle) shows increased vascularity.
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.
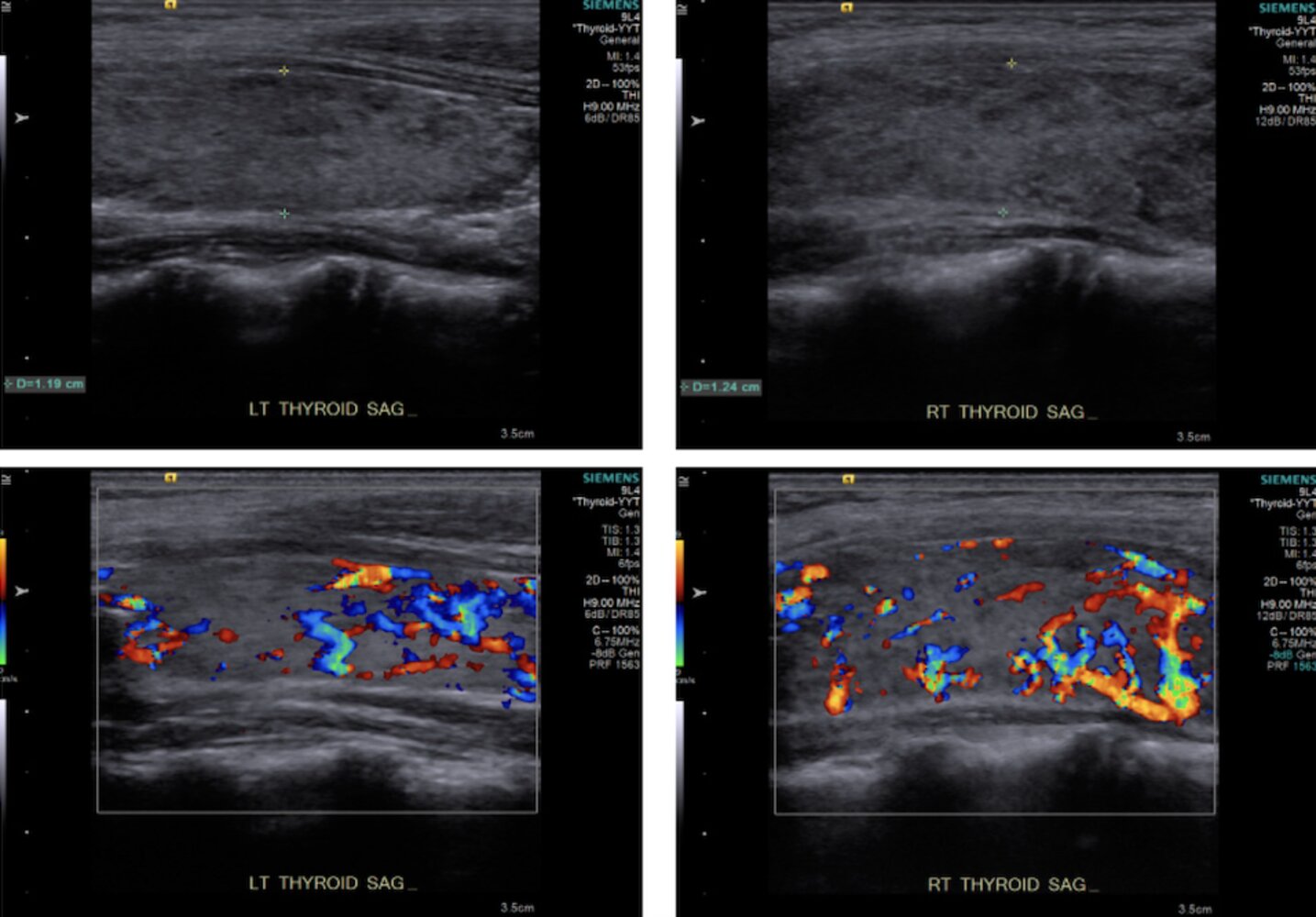
Ultrasound thyroid (color Doppler) of patient with history of Graves disease
The thyroid gland (outline) shows increased color Doppler signal indicating hypervascularity. Visible portions of the gland are heterogeneous and hypoechoic (examples indicated by arrows).
Thyroid gland assessment in Graves disease should be multifactorial, taking into consideration B-mode, spectral, and color Doppler features. Hypervascularity is common in Graves disease but can also be caused by other conditions (e.g., vasculitis, hypothyroidism). The thyroid gland in Graves disease is typically enlarged, hypoechoic, and heterogeneous, with increased color Doppler signal. Peak systolic velocity in the inferior thyroid artery on Doppler spectral analysis is classically higher than in thyroiditis.
Source: © IMPP
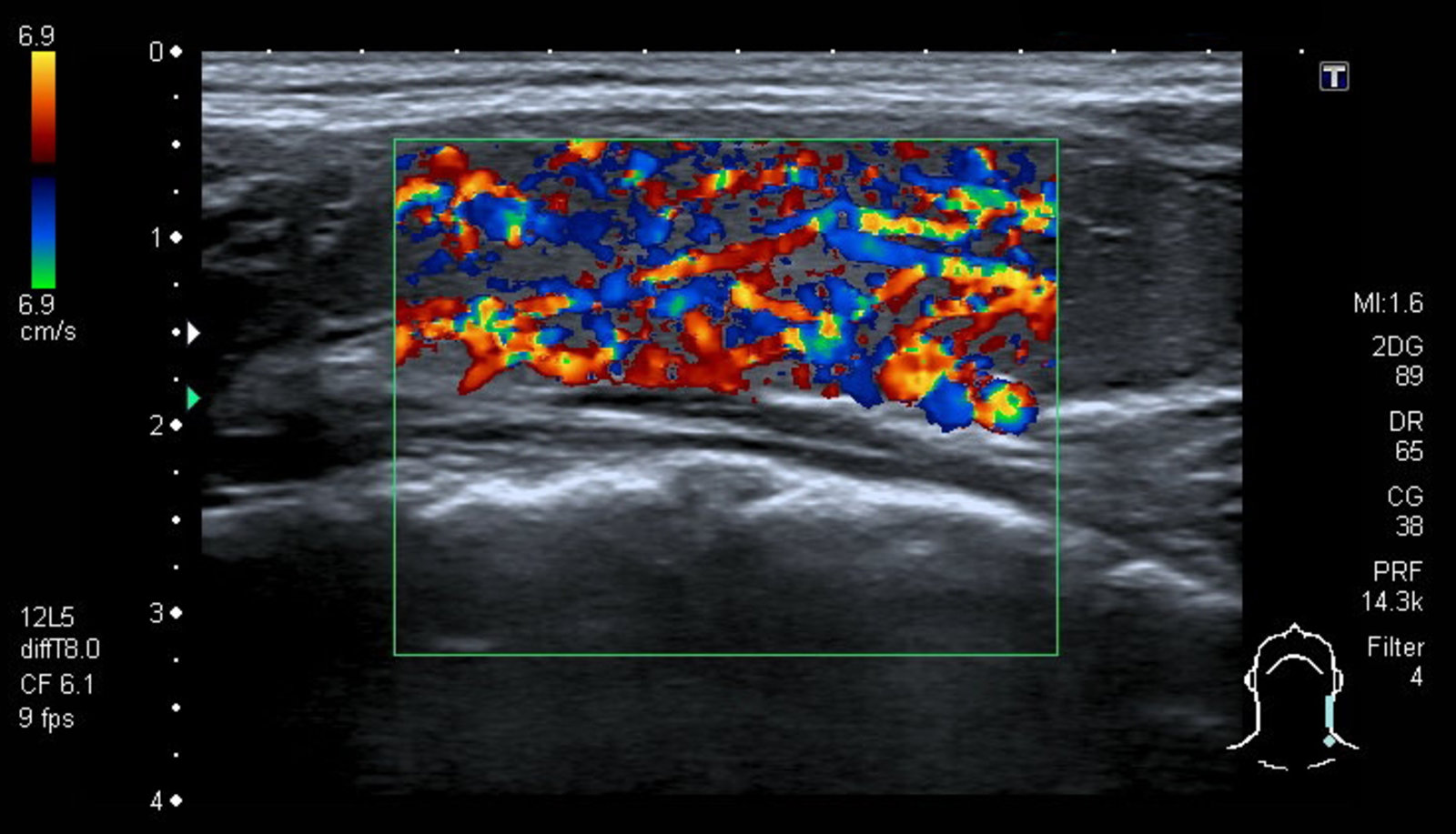
Ultrasound thyroid (longitudinal plane; bottom: with color Doppler) of a patient with Graves disease
The echotexture of the thyroid gland is diffusely heterogenous, and the gland is hypervascular on color Doppler. A normal thyroid gland is homogeneous and shows less blood flow on color Doppler than seen in this patient. The color red indicates blood flow directed toward the ultrasound probe, while the color blue indicates blood flow directed away from the probe.
Hypoechogenicity and increased blood flow are characteristic features of Graves disease. Although not shown in this patient, the thyroid gland is also often enlarged in Graves disease.
There is overlap of the appearance of this gland with some ultrasound presentations in patients with thyroiditis.
Source: “Fig 3, In: Evolution of Graves’ Disease during Immune Reconstitution following Nonmyeloablative Haploidentical Peripheral Blood Stem Cell Transplantation in a Boy Carrying Germline SAMD9L and FLT3 Variants” by Ip PP, Fang L-H, Shen Y-L et al., MDPI, licensed under CC BY 4.0. Modifications: image cropped.
Differential diagnoses
The symptoms of thyrotoxicosis are nonspecific and overlap significantly with other common conditions. If there is any clinical uncertainty, TSH should be assessed.
- Neuropsychiatric symptoms: anxiety/panic disorders
- Hyperadrenergic symptoms: intoxication with anticholinergics; cocaine/amphetamine misuse; withdrawal syndromes
- Weight loss: diabetes mellitus, malignancy
- Cardiac symptoms: congestive cardiac failure
References:[2][4][5][6][7][8][14]
The differential diagnoses listed here are not exhaustive.
Treatment
Overview [17][23]
- For severe symptoms, screen for thyroid storm (e.g., with BWPS) and start immediate treatment of thyroid storm if present.
- For hyperadrenergic symptoms, initiate symptomatic therapy for thyrotoxicosis (e.g., beta blockers).
- Symptomatic patients and asymptomatic individuals with risk factors : Management depends on the individual clinical situation and patient preferences.
- Graves disease: Antithyroid drugs, RAIA, and thyroid surgery are all effective options (see “Management of Graves disease”).
- Toxic MNG and toxic adenoma: Definitive therapy for hyperthyroidism (i.e., RAIA or thyroid surgery) is preferable to antithyroid drugs.
- Asymptomatic younger adults without risk factors: Consider either observation or treatment. [17]
- Identify and treat reversible causes (e.g., discontinuing offending medications , starting NSAIDs or corticosteroids for thyroiditis).
- Avoid triggers, e.g., contrast medium, amiodarone, and aspirin.
Symptomatic therapy for thyrotoxicosis [17]
The treatment of hyperadrenergic symptoms is important for decreasing the risk of cardiac complications in thyrotoxicosis, such as atrial fibrillation and heart failure.
- Indication: all symptomatic patients
-
Treatment of hyperadrenergic symptoms: beta blockers (first line) [17];
- Provide immediate control of symptoms, e.g., neuropsychiatric and/or hyperadrenergic symptoms
- Treatment options
- First line: propranolol
- Alternatives: atenolol OR metoprolol
- Severe thyrotoxicosis or thyroid storm treated in ICU: esmolol
- If there are contraindications to beta blockers, e.g., severe asthma, Raynaud phenomenon ; , consider CCBs: verapamil OR diltiazem . [26]
-
Treatment of cardiac complications [23]
- Heart failure: patients should receive the same treatment as euthyroid patients with heart failure (see “Treatment” in “Acute heart failure”).
-
Atrial fibrillation
- May be refractory to treatment until antithyroid therapy has been initiated
- Amiodarone should be avoided.
- See “Treatment” in “Atrial fibrillation” for details on further management.
Antithyroid drugs
Antithyroid drugs can effectively render a patient euthyroid. 20–75% of patients with Graves disease achieve permanent remission after 1–2 years of treatment; however, some patient groups have a higher likelihood of remission than others.
-
Indications
- Thyroid storm: initial management ; as well as prevention in at-risk patients prior to surgery or RAIA
- Graves disease: Patients with high remission likelihood , and/or moderate to severe active Graves ophthalmopathy [27]
- Contraindications to both RAIA and surgery
- Other: hyperthyroidism in pregnancy, limited life expectancy, patient preference
- Contraindication: destructive thyroiditis [17]
-
Medication for hyperthyroidism
- The choice of medication depends on the severity of symptoms and patient factors.
- Most patients: methimazole
- Thyroid storm or first trimester of pregnancy: propylthiouracil
- The choice of medication depends on the severity of symptoms and patient factors.
-
Monitoring [17]
-
CBC, liver chemistries, and bilirubin
- Obtain baseline prior to therapy.
- Repeat if febrile illness or symptoms of liver injury, e.g., jaundice.
- TFTs: measure free T4 and T3 2–6 weeks after initiation of therapy and adjust dosage accordingly.
- See also “Adverse effects” in “Antithyroid drugs”.
-
CBC, liver chemistries, and bilirubin
-
Duration of therapy
- Primary therapy for Graves disease: typically 12–18 months
- Preparation for surgery: given until TFTs normalize, after which surgery may be performed [28]
- Preparation for RAIA: given until TFTs normalize and stopped 2–3 days before ablation
Obtain a CBC and liver chemistries immediately if patients develop fever or signs of hepatotoxicity while taking ATD. [17]
ATDs are ineffective in the management of destructive thyroiditis-induced thyrotoxicosis, which is caused by a release of preformed thyroid hormones by the damaged follicles [17]

Definitive therapy for hyperthyroidism and thyrotoxicosis [17][29]
Radioactive iodine ablation (RAIA) [30]
- Definition: destruction of thyroid tissue via radioactive iodine (iodine-131) through a sodium/iodine symporter
-
Technical background: Radioactive iodine-131 emits both gamma and beta rays.
- Gamma rays: diagnostic effect
- Beta rays: therapeutic effect
-
Indications
- Toxic MNG and toxic adenoma with high nodular radioactive iodine uptake
- Failure to achieve euthyroidism with antithyroid drugs (ATDs) in Graves disease, due to:
- Refractory disease
- Contraindications to ATDs, e.g., liver disease
- Major adverse reactions to ATDs
- High surgical risk due to comorbidities or previous surgery or radiation of the neck
- Limited life-expectancy
- Other: thyrotoxic periodic paralysis, post-surgical treatment of certain thyroid cancers, large/compressive nontoxic goiters [31]
-
Contraindications
- Pregnant/breastfeeding women
- Children < 5 years of age
- Initial treatment for confirmed or suspected thyroid malignancy
- Moderate to severe Graves ophthalmopathy
- Inability to follow radiation safety regulations
-
Preparation for RAIA
- RAIA can cause a transient worsening of hyperthyroidism.
-
Prophylactic treatment can reduce the risk of complications in high-risk patient groups, e.g., severe hyperthyroidism, older patients, and those with comorbid conditions.
- Consider beta blockers even in asymptomatic patients (see “Symptomatic therapy for thyrotoxicosis” for dosages).
- Administer methimazole to rapidly achieve a euthyroid state; must be discontinued 2–3 days before RAIA is started.
- Avoid excess iodine for 7 days prior to RAIA.
- In women of childbearing potential, a negative pregnancy test must be confirmed within 48 hours before RAIA.
- Procedure: Single oral dose of iodine-131 → isotope uptake by thyroid gland → emission of beta radiation that slowly destroys the thyroid tissue
-
Complications [32][33]
- Early
- Most patients with Graves disease become hypothyroid after RAIA and require life-long thyroid hormone replacement with L-thyroxine
- Gastritis: nausea and vomiting
- Sialadenitis
- Other: transient loss of taste or smell, stomatitis, transient bone marrow suppression
- Late
-
Radiation-induced thyroiditis: a form of acute thyroiditis that occurs a few days after the thyroid gland is exposed to radiation
- It is most commonly seen following radioiodine therapy in patients with Graves disease, or following external beam radiotherapy for head and neck cancers.
- Patients present with pain in the thyroid region and thyrotoxicosis (due to the release of T3 and T4 following rapid destruction of thyroid tissue).
- Secondary malignancy or leukemia
- Dry mouth (xerostomia)
-
Radiation-induced thyroiditis: a form of acute thyroiditis that occurs a few days after the thyroid gland is exposed to radiation
- Early

Thyroid surgery for hyperthyroidism [34]
The efficacy of antithyroid drugs and RAIA has reduced the need for thyroid surgery.
-
Indications
- Large goiters (≥ 80 g) or obstructive symptoms
- Confirmed or suspected thyroid malignancy
-
Graves disease with: [35]
- Concomitant primary hyperparathyroidism or periodic paralysis
- Moderate to severe active Graves ophthalmopathy [27]
- Toxic MNG or toxic adenoma with: concomitant primary hyperparathyroidism, insufficient RAIA, or retrosternal extension
- Other: large thyroid nodules , refractory amiodarone-induced thyrotoxicosis , planned pregnancy within next 6 months , or patient preference
-
Contraindications
- Severe comorbidities that influence surgical risk
- Pregnancy
-
Preparation for thyroid surgery
- Achieving euthyroidism prior to surgery: preoperative application of antithyroid drugs (and beta blockers if necessary) for at least 4–8 weeks if possible (see “Symptomatic therapy for thyrotoxicosis” and “Antithyroid drugs for thyrotoxicosis” for doses).
- Patients with Graves disease: potassium iodide solution for 10 days preoperatively (harnesses the Wolff-Chaikoff effect)
- Assess for hypocalcemia: Replete calcium and 25-hydroxy vitamin D as needed
- Urgent surgery or antithyroid drug allergy/intolerance: Consider adding corticosteroids and cholestyramine in consultation with a specialist. [26][36]
-
Procedure
- Graves disease or toxic MNG: near-total or total thyroidectomy
- Isolated toxic adenoma: lobectomy
- See also “Procedure/application” in “Thyroid surgery.”
-
Postprocedural care for thyroid surgery
- Measure serum calcium and PTH levels at 6 and 12 hours post-operatively and start calcium and calcitriol. [17]
- Wean beta blockers.
- Stop ATDs.
- Start levothyroxine replacement. . [34]
Ongoing management for patients treated for hyperthyroidism [17]
- Ongoing management is usually provided by endocrinology and/or surgery.
- Thyroid function is measured at set intervals depending on the treatment given. [17]
- Patients who have undergone surgery are given calcium and vitamin D and monitored for postoperative hypoparathyroidism.
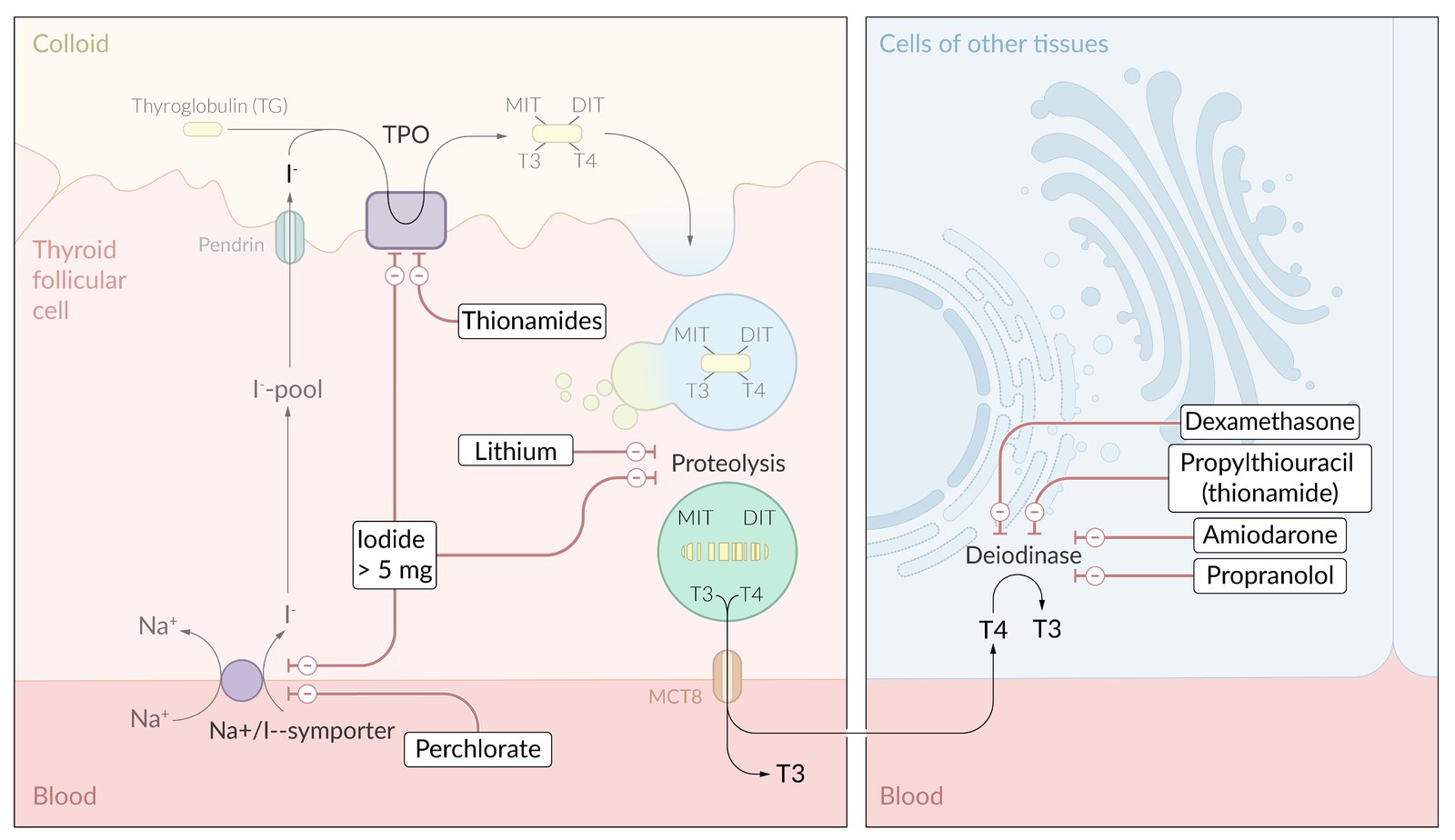
Left side: effect of drugs on the thyroid gland.
- Thionamides inhibit thyroid peroxidase (TPO), which blocks thyroid hormone synthesis.
- Lithium inhibits the release of thyroid hormones and may be used off-label in a thyroid storm.
- Perchlorate inhibits the sodium-iodine cotransporter in the membrane, which blocks iodide uptake in the thyroid gland.
Right side: drug effects in the periphery. A number of drugs inhibit the enzyme deiodinase, which blocks the peripheral conversion of T4 to the active form T3.
© AMBOSS
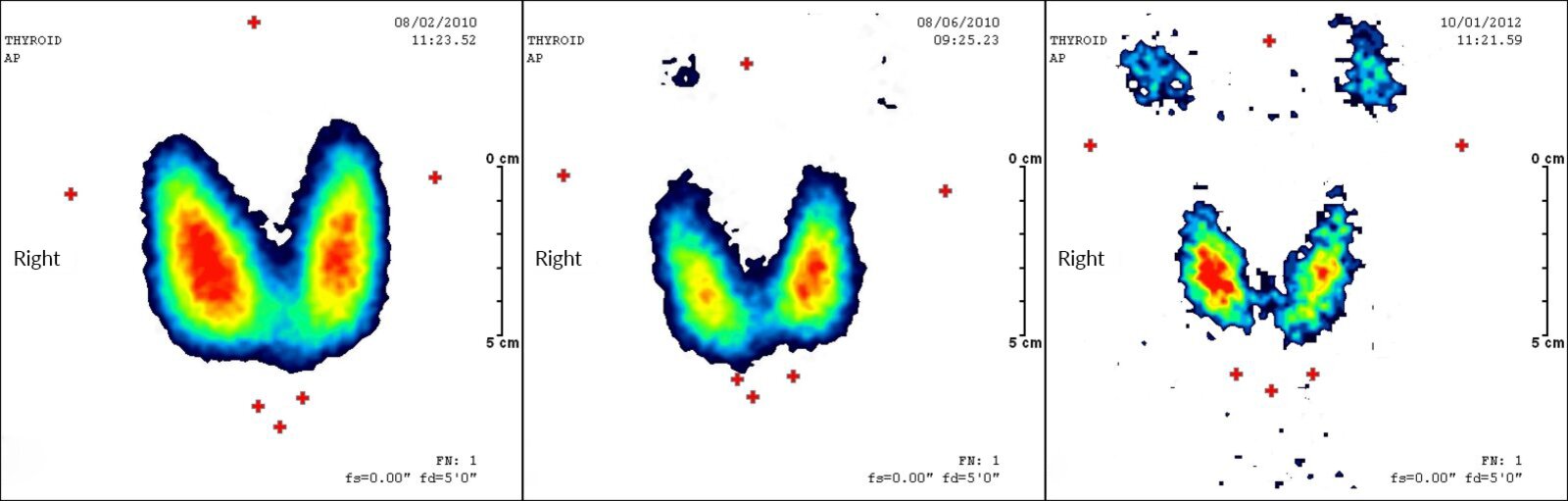
Nuclear medicine thyroid scan (99mTc pertechnetate; left: before radioiodine therapy; middle: three months after therapy; right: 10 months after therapy) of a patient with Graves disease
A decline in thyroid gland size and radioactivity over time is seen after radiotherapy.
Iodine uptake is represented by a color scale (blue > green > yellow > red)
Source: “Serie Radiojodtherapie Basedow” by Drahreg01, Wikimedia Commons, licensed under CC BY-SA 3.0. Modifications: Changed German "Rechts" to "Right", deleted in-image text.
{kind=link}
Special patient groups
Management of hyperthyroidism differs slightly in select patient groups (e.g., individuals who are pregnant or planning pregnancy, newborns). For more information on management of Graves disease, the most common cause of hyperthyroidism, see “Special patient groups” in “Graves disease.”
Thyroid storm
Definition [17]
- An acute exacerbation of hyperthyroidism that results in a life-threatening hypermetabolic state.
- Also known as thyrotoxic crisis
Etiology [17]
-
Iatrogenic
- Thyroid surgery
- RAIA
- Exogenous iodine from contrast media or amiodarone
- Discontinuation of antithyroid medication
-
Stress-related catecholamine surge
- Nonthyroidal surgery
- Anesthesia induction
- Labor
- Intercurrent illness, e.g., sepsis, myocardial infarction, diabetic ketoacidosis
Clinical features [17]
- Hyperpyrexia with profuse sweating
- Tachycardia (> 140/minute) and (possibly severe) arrhythmia (e.g., atrial fibrillation), hypertension with wide pulse pressure, congestive cardiac failure
- Hypotension/shock secondary to high output heart failure or hypovolemia as a result of GI and insensible losses
- Symptoms of thyrotoxicosis
- Abdominal pain
- Severe nausea, vomiting, diarrhea, possibly jaundice
- Severe agitation and anxiety, delirium and psychoses, seizures, coma
Diagnostics [17]
- A thyroid storm is diagnosed on the basis of classic clinical features and supporting TFT abnormalities, e.g., low/undetectable TSH, elevated free T3/T4.
- Further tests should be performed to identify any underlying precipitants and to assess for complications, e.g.:
- ECG to assess for atrial fibrillation
- Liver chemistries to assess for evidence of jaundice
- The Burch-Wartofsky Point Scale (BWPS) can be considered to assess disease severity and guide treatment.
| Burch-Wartofsky Point Scale for the diagnosis of thyroid storm (BWPS) [17] | ||
|---|---|---|
| Criteria | Points | |
| Temperature | 37.2–37.7°C (99.0–99.9°F) | 5 |
| 37.8–38.2°C (100–100.9°F) | 10 | |
| 38.3–38.8°C (101–101.9°F) | 15 | |
| 38.9–39.4°C (102–102.9°F) | 20 | |
| 39.4–39.9°C (103–103.9°F) | 25 | |
| ≥ 40°C (≥ 104°F) | 30 | |
| Tachycardia | 100–109/minute | 5 |
| 110–119/minute | 10 | |
| 120–129/minute | 15 | |
| 130–139/minute | 20 | |
| ≥ 140/minute | 25 | |
| Atrial fibrillation | Absent | 0 |
| Present | 10 | |
| Congestive heart failure | Absent | 0 |
| Mild | 5 | |
| Moderate | 10 | |
| Severe | 20 | |
| Gastrointestinal-hepatic dysfunction | Absent | 0 |
| Moderate (e.g., diarrhea, abdominal pain, nausea/vomiting) | 10 | |
| Severe (jaundice) | 20 | |
| Central nervous system disturbance | Absent | 0 |
| Mild (agitation) | 10 | |
| Moderate (e.g., delirium, psychosis, extreme lethargy) | 20 | |
| Severe (e.g., seizure, coma) | 30 | |
| Identified precipitant | Yes | 10 |
| No | 0 | |
Interpretation
| ||
 for Thyrotoxicosis")
Treatment of thyroid storm [17][37]
Thyroid storm has a high mortality rate and patients should receive aggressive treatment to manage complications and restore normal thyroid function.
Approach
- Consult critical care for ICU admission and monitoring.
- Start symptomatic treatment to manage hypotension, hyperpyrexia, and tachycardia.
- Administer medication to reduce thyroid hormone synthesis and release, and inhibit their peripheral action.
- Identify and treat any precipitating cause.
- Once the patient is stable, initiate definitive therapy for hyperthyroidism and thyrotoxicosis.
- Consider plasmapheresis or emergency surgery as life-saving treatment for rare refractory cases
Symptomatic treatment
-
Hyperadrenergic symptoms: beta blockers are first-line
- Preferred: Propranolol , due to combined beta-blockade and antithyroid effects
- Alternatives
- Preexisting heart failure: esmolol [23][38]
- Mild obstructive airway disease/stable asthma: atenolol or metoprolol
- Beta blocker contraindications: consider CCBs, e.g., diltiazem
-
Hyperthermia
- External cooling techniques (e.g., ice packs, cooling blankets, alcohol washes)
- Antipyretics, e.g., consider IV acetaminophen
- Avoid aspirin.
-
Hypotension and hypovolemia: fluid resuscitation to treat insensible and GI losses [37]
- Fluids containing 5–10% dextrose are preferred to meet the high metabolic demand.
- Fluid requirement is often high (3–5 L/day).
- Electrolyte disturbances: (see “Electrolyte repletion” for specific repletion regimens)
- Agitation: benzodiazepines, e.g., lorazepam
- Concurrent conditions: e.g., CHF and/or Atrial fibrillation (See “Management” in “Acute heart failure” and “Management of Afib with RVR”)
If thyroid storm has led to congestive heart failure, esmolol is the preferred beta blocker. All patients receiving beta blockers should be monitored carefully for signs of heart failure.
Antithyroid drugs in thyroid storm [17][23][26]
-
Inhibition of thyroid hormone synthesis
- First line: propylthiouracil
- Alternative: methimazole
-
Inhibition of thyroid hormone release (through the Wolff-Chaikoff effect)
- First line: iodine solutions given at least 1 hour after antithyroid drugs
- Potassium iodide solution
- Lugol solution
- In patients with iodine allergy or iodine-induced thyrotoxicosis, lithium can be used .
- First line: iodine solutions given at least 1 hour after antithyroid drugs
-
Inhibition of peripheral conversion of T4 to T3
- Propranolol
-
Glucocorticoids: can also treat concurrent adrenal insufficiency
- First line: hydrocortisone
- Alternative: dexamethasone
Treat thyroid storm with PROverbial PROficiency and POetic GLUttony: PROpranolol, PROpylthiouracil, POtassium iodide, and GLUcocorticoids.
Acute management checklist for thyroid storm
- Conduct ABCDE survey and draw initial laboratory studies (e.g., TFTs, BMP, liver chemistries)
- Begin IV fluid resuscitation
- Identify and treat tachyarrhythmias or acute heart failure
- Treat hyperadrenergic symptoms with beta blockers (first-line: propranolol).
- Treat hyperthermia: external cooling and acetaminophen.
- Consider BWPS if uncertain diagnosis or for assessing severity and need for aggressive therapy.
- Consult critical care for ICU admission.
- Initiate antithyroid drugs:
- PTU
- KI
- IV glucocorticoids
- Identify and treat reversible triggers.
- Electrolyte repletion as needed
- Administer benzodiazepines as needed for agitation.
- Consider plasmapheresis for life-threatening refractory cases.
- Ensure definitive therapy for hyperthyroidism and thyrotoxicosis when stabilized.
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
External Resources
- 2020 AAES Guidelines for the Definitive Surgical Management of Thyroid Disease in Adults
- 2019 EANM Practice Guideline/SNMMI Procedure Standard for RAIU and Thyroid Scintigraphy
- 2016 ATA Guidelines for Diagnosis and Management of Hyperthyroidism and Other Causes of Thyrotoxicosis
- 2016 JTA/JES Guidelines for the Management of Thyroid Storm
References
- Kim YA, Park YJ. "Prevalence and Risk Factors of Subclinical Thyroid Disease". Endocrinology and Metabolism. 29(1). :20. (2014)
- Ahsan I. "Textbook of Surgery". Harwood Academic Publishers. (1997). ISBN: 9057021390
- Vanderpump MP. "The epidemiology of thyroid disease". Br Med Bull. 99(1). :39-51. (2011)
- "Hyperthyroidism". http://endocrinefacts.org/health-conditions/thyroid/4-hyperthyroidism/. [2017-02-09]
- Ross DS. "Disorders that cause hyperthyroidism". UpToDate. UpToDate. https://www.uptodate.com/contents/disorders-that-cause-hyperthyroidism. [2015-11-03]
- Fisher JN. "Management of thyrotoxicosis". South Med J. 95(5). :493-505. (2002)
- Schraga ED. "Hyperthyroidism, Thyroid Storm, and Graves Disease". WebMD. http://emedicine.medscape.com/article/767130-overview. [2016-08-05]
- Bachman ES, Hampton TG, Dhillon H, et al. "The Metabolic and Cardiovascular Effects of Hyperthyroidism Are Largely Independent of β-Adrenergic Stimulation". Endocrinology. 145(6). :2767-2774. (2004)
- Roubsanthisuk W, Watanakejorn P, Tunlakit M, Sriussadaporn S. "Hyperthyroidism induces glucose intolerance by lowering both insulin secretion and peripheral insulin sensitivity.". Journal of the Medical Association of Thailand. 89 Suppl 5. :S133-40. (2006)
- Ross DS, Burch HB, Cooper DS, et al. "2016 American Thyroid Association Guidelines for Diagnosis and Management of Hyperthyroidism and Other Causes of Thyrotoxicosis". Thyroid. 26(10). :1343-1421. (2016)
- Walls R, Hockberger R, Gausche-Hill M. "Rosen's Emergency Medicine". Elsevier Health Sciences. (2018). ISBN: 9780323354790
- Intenzo CM, Depapp AE, Jabbour S, et al. "Scintigraphic manifestations of thyrotoxicosis". Radiographics. 23(4). :857-869. (2003)
- Giovanella L, Avram AM, Iakovou I, et al. "EANM practice guideline/SNMMI procedure standard for RAIU and thyroid scintigraphy". Eur J Nucl Med Mol Imaging. 46(12). :2514-2525. (2019)
- Hoang JK, Oldan JD, Mandel SJ, et al. "ACR Appropriateness Criteria® Thyroid Disease". J Am Coll Radiol. 16(5). :S300-S314. (2019)
- Smith TJ, Hegedüs L. "Graves’ Disease". N Engl J Med. 375(16). :1552-1565. (2016)
- Knobel M. "Etiopathology, clinical features, and treatment of diffuse and multinodular nontoxic goiters". J Endocrinol Invest. 39(4). :357-373. (2015)
- Alfadda AA et al. "Subacute Thyroiditis: Clinical Presentation and Long Term Outcome". International Journal of Endocrinology. 2014. :1-7. (2014)
- Samuels MH. "Subacute, Silent, and Postpartum Thyroiditis". Med Clin North Am. 96(2). :223-233. (2012)
- Leung AM, Braverman LE. "Iodine-induced thyroid dysfunction". Current Opinion in Endocrinology & Diabetes and Obesity. 19(5). :414-419. (2012)
- Carroll R, Matfin G. "Review: Endocrine and metabolic emergencies: thyroid storm". Ther Adv Endocrinol Metab. 1(3). :139-145. (2010)
- Douglas RS et al. "Teprotumumab for the Treatment of Active Thyroid Eye Disease". N Engl J Med. 382(4). :341-352. (2020)
- Piantanida E. "Preoperative management in patients with Graves' disease.". Gland Surg. 6(5). :476-481. (2017)
- Papaleontiou M, Haymart MR. "Approach to and Treatment of Thyroid Disorders in the Elderly". Medical Clinics of North America. 96(2). :297-310. (2012)
- Sisson JC, Freitas J, Mcdougall IR, et al. "Radiation safety in the treatment of patients with thyroid diseases by radioiodine 131I : practice recommendations of the American Thyroid Association". Thyroid. 21(4). :335-346. (2011)
- Graf H. "THERAPY OF ENDOCRINE DISEASE: Recombinant human TSH and radioactive iodine therapy in the management of benign multinodular goiter". Eur J Endocrinol. 172(2). :R47-R52. (2015)
- Lee SL. "Complications of Radioactive Iodine Treatment of Thyroid Carcinoma". J Natl Compr Canc Netw. 8(11). :1277-1287. (2010)
- Fard-Esfahani A, Emami-Ardekani A, Fallahi B, et al. "Adverse effects of radioactive iodine-131 treatment for differentiated thyroid carcinoma". Nucl Med Commun. 35(8). :808-817. (2014)
- Patel KN et al. "The American Association of Endocrine Surgeons Guidelines for the Definitive Surgical Management of Thyroid Disease in Adults". Ann Surg. 271(3). :e21-e93. (2020)
- Mohan V, Lind R. "A review of treatment options for Graves' disease: why total thyroidectomy is a viable option in selected patients". J Community Hosp Intern Med Perspect.. 6(4). (2016)
- Yang Y et al. "Refractory Graves' Disease Successfully Cured by Adjunctive Cholestyramine and Subsequent Total Thyroidectomy". Endocrinology and Metabolism. 30(4). :620. (2015)
- Burman KD. "Overview of thyroiditis". UpToDate. UpToDate. https://www.uptodate.com/contents/overview-of-thyroiditis. [2015-07-08]
- Biondi B, Cooper DS. "Subclinical Hyperthyroidism". N Engl J Med. 378(25). :2411-2419. (2018)
- Jonklaas J, Bianco AC, Bauer AJ, et al. "Guidelines for the Treatment of Hypothyroidism: Prepared by the American Thyroid Association Task Force on Thyroid Hormone Replacement". Thyroid. 24(12). :1670-1751. (2014)
- Mooij CF, Cheetham TD, Verburg FA, et al. "2022 European Thyroid Association Guideline for the management of pediatric Graves’ disease". Eur Thyroid J. 11(1). (2022)
- Asa SL, Erickson LA, Rindi G. "The Spectrum of Endocrine Pathology". Endocr Pathol. :1-14. (2023)
- Matfin G. "Endocrine and Metabolic Medical Emergencies". John Wiley & Sons. (2018)
- Satoh T, Isozaki O, Suzuki A, et al. "2016 Guidelines for the management of thyroid storm from The Japan Thyroid Association and Japan Endocrine Society (First edition)". Endocr J. 63(12). :1025-1064. (2016)
- Sharma A, Stan MN. "Thyrotoxicosis: Diagnosis and Management". Mayo Clin Proc. 94(6). :1048-1064. (2019)
- "NCCN Clinical Practice Guidelines in Oncology: Thyroid Cancer, Version 2.2017". https://www.nccn.org/professionals/physician_gls/pdf/thyroid.pdf. [2017-05-01]
- Tessler FN, Middleton WD, Grant EG, et al. "ACR Thyroid Imaging, Reporting and Data System (TI-RADS): White Paper of the ACR TI-RADS Committee". J Am Coll Radiol. 14(5). :587-595. (2017)
- Cooper DS. "Long-Term Antithyroid Drug Treatment of Patients With Graves’ Disease". Clin Thyroidol. 31(6). :230-233. (2019)