Summary
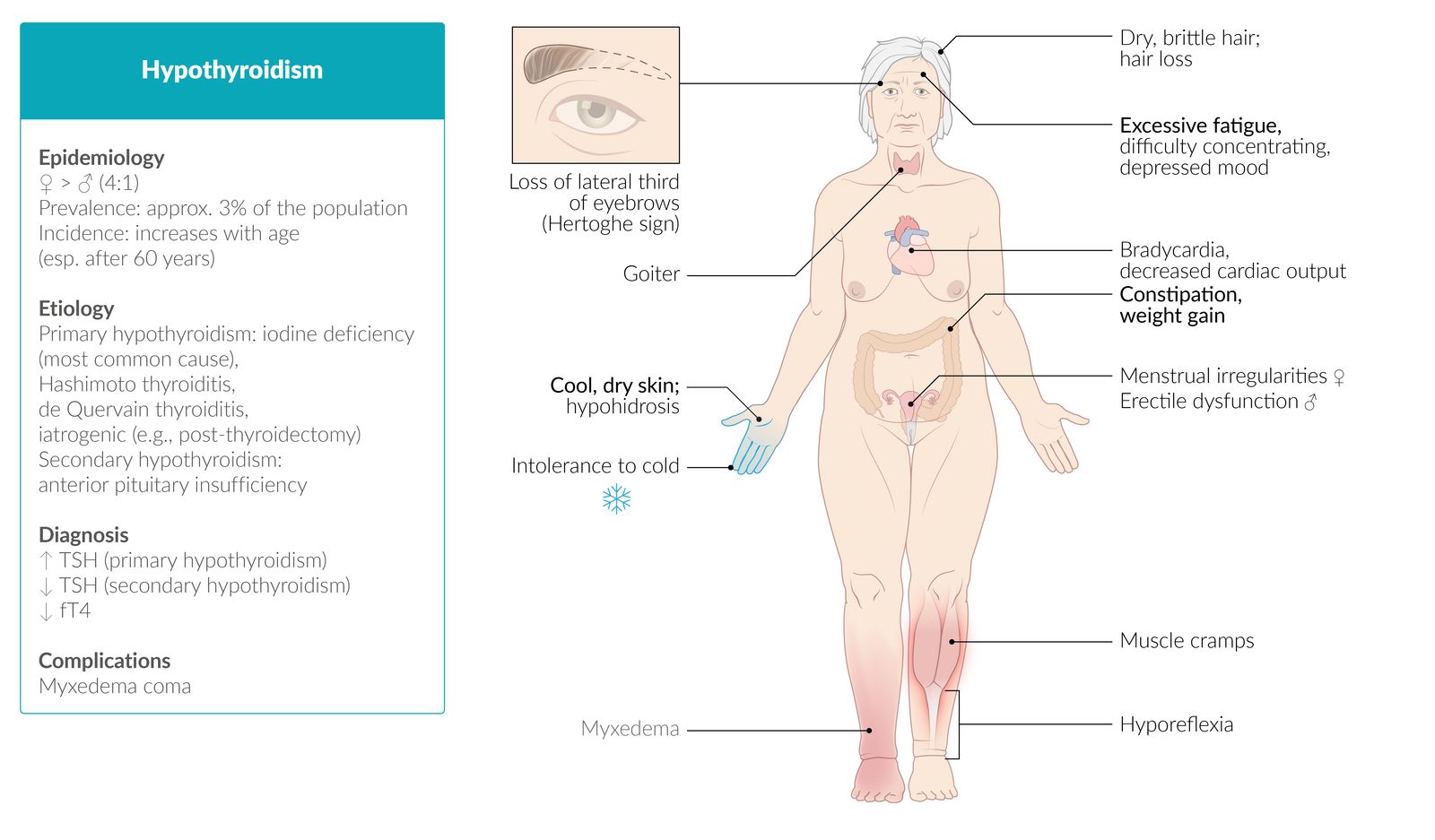
Hypothyroidism is a condition in which the thyroid gland is underactive, resulting in a deficiency of the thyroid hormones triiodothyronine (T3) and thyroxine (T4). Rarely, hormone production remains sufficient, but thyroid hormones may have insufficient peripheral effects. Hypothyroidism may be congenital or acquired. Congenital hypothyroidism is usually caused by thyroid dysplasia or aplasia. The most common cause of acquired hypothyroidism in both adults and children is Hashimoto thyroiditis; other causes include iatrogenic harm. The pathophysiology of hypothyroidism is characterized mainly by a reduction of the basal metabolic rate and generalized myxedema. Clinical features include fatigue, cold intolerance, dry skin, and constipation. More severe manifestations include myxedematous heart disease and myxedema coma, which may be fatal if untreated. In adults, diagnosis is established based on serum thyroid-stimulating hormone (TSH) and free T4 levels (FT4). Hypothyroidism in children may be acquired or congenital. Congenital hypothyroidism is usually detected during neonatal screening, but it may also manifest with distinct features (e.g., macroglossia, large posterior fontanelle, umbilical hernia, prolonged jaundice). If untreated, congenital hypothyroidism can lead to severe developmental delay.

© AMBOSS
Epidemiology
Prevalence: more common in women
- Women: up to 12:1,000
- Men: up to 4:1,000 [1]
Epidemiological data refers to the US, unless otherwise specified.
Etiology
-
Primary hypothyroidism: insufficient thyroid hormone production
-
Hashimoto thyroiditis
- The most common cause of hypothyroidism in iodine-sufficient regions [2]
- Associated with HLA-DR3 and other autoimmune diseases (e.g., vitiligo, pernicious anemia, type 1 diabetes, and systemic lupus erythematosus)
- Postpartum thyroiditis (subacute lymphocytic thyroiditis) [2]
- De Quervain thyroiditis (subacute granulomatous thyroiditis): often subsequent to a flu-like illness [2]
- Iatrogenic: e.g., post thyroidectomy, radioiodine therapy, antithyroid medication (e.g., amiodarone, lithium)
- Nutritional (insufficient intake of iodine): most common cause of hypothyroidism worldwide, particularly in iodine-deficient regions
- Riedel thyroiditis: occurs in IgG4-related systemic disease
- Wolff-Chaikoff effect
- Thyroid dysplasia: a disorder of embryologic development characterized by abnormal development and/or location of thyroid tissue (e.g., lingual thyroid)
-
Hashimoto thyroiditis
- Secondary hypothyroidism: pituitary disorders (e.g., pituitary adenoma) → TSH deficiency
- Tertiary hypothyroidism: hypothalamic disorders → TRH deficiency
| Overview of common causes of primary hypothyroidism | ||||||
|---|---|---|---|---|---|---|
| Hashimoto thyroiditis [2] | Postpartum thyroiditis [3] | Subacute granulomatous thyroiditis (De Quervain) [4] | Congenital hypothyroidism [5][6] | Riedel thyroiditis [7] | ||
| Epidemiology |
|
|
|
|
|
|
| Causes |
|
|
|
|
|
|
| Clinical course |
|
|
|
|
|
|
| Goiter | Structure |
|
|
|
|
|
| Pain |
|
|
|
|
||
| Antibodies |
|
|
|
|
|
|
| Iodine uptake on scintigraphy |
|
|
|
|
|
|
| Pathology findings |
|
|
|
|
|
|
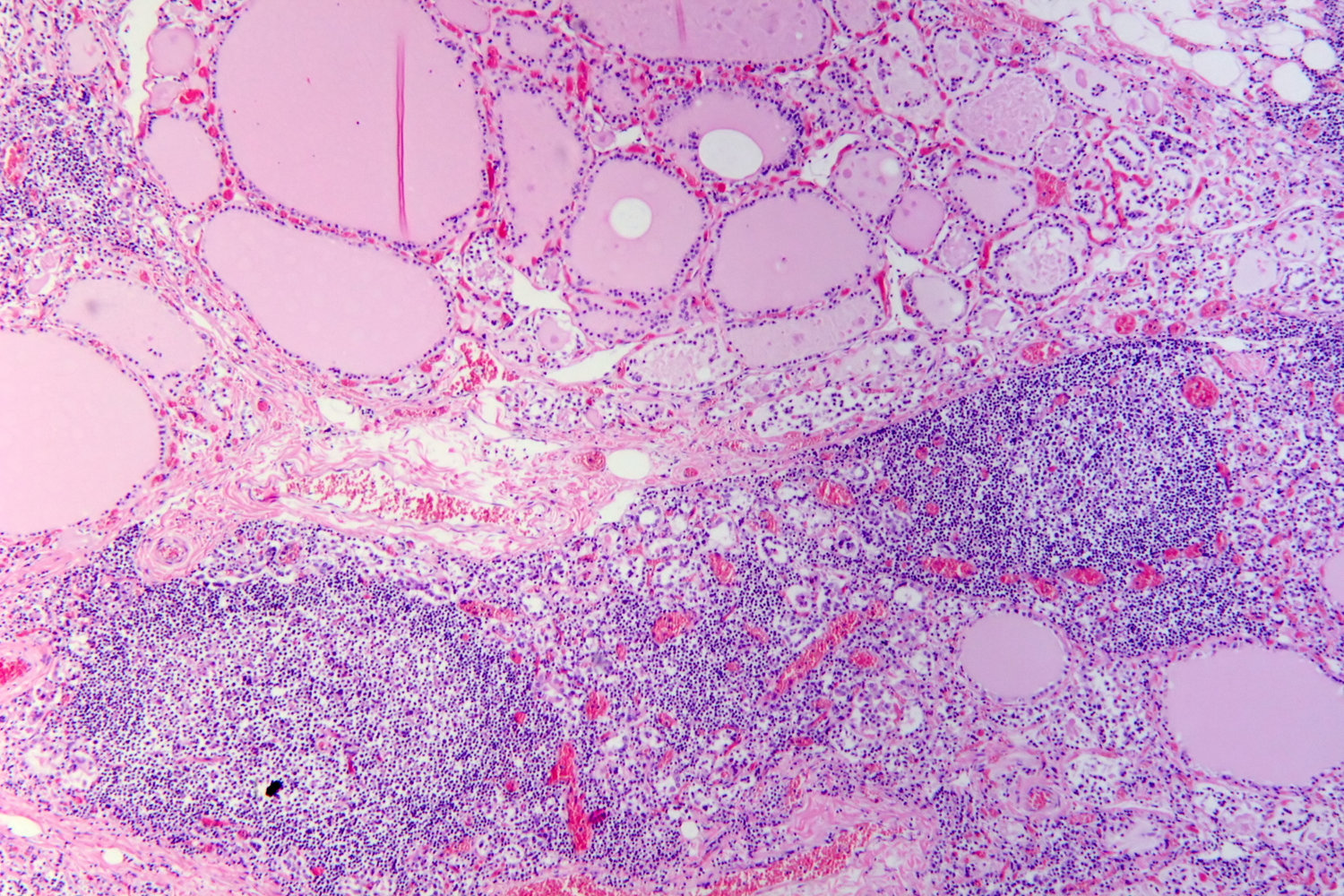
Photomicrograph of thyroid tissue (H&E stain)
The thyroid tissue in the lower half of the image is inflamed, as evidenced by the lymphocytic infiltrate (numerous purple dots) and dilated, congested blood vessels (examples indicated by arrows). Prominent lymphoid follicles with a germinal center (example indicated by orange overlay) surrounded by a hypercellular parafollicular region (example indicated by green overlay) are visible in the inflamed region. Normal thyroid follicles (example indicated by blue overlay) are visible in the top half of the image but are absent in the inflamed region.
Lymphocytic infiltration, lymphoid follicles with germinal centers, and destruction of thyroid follicles are characteristic features of Hashimoto thyroiditis.
Source: “Hashimoto's thyroiditis, HE 4” by Patho, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
Pathophysiology
Hypothalamic-pituitary-thyroid axis [8]
The hypothalamus, anterior pituitary gland, and thyroid gland, together with their respective hormones, comprise a self-regulatory circuit referred to as the “Hypothalamic-pituitary-thyroid axis.”
- Primary hypothyroidism: peripheral (thyroid) disorders → T3/T4 are not produced (↓ levels) → compensatory ↑ TSH
- Secondary hypothyroidism: pituitary disorders → ↓ TSH levels → ↓ T3/T4 levels
- Tertiary hypothyroidism: hypothalamic disorders → ↓ TRH levels → ↓ TSH levels → ↓ T3/T4 levels

Effects of hypothyroidism [8][9]
-
Generalized decrease in the basal metabolic rate → decreased oxygen and substrate consumption, leading to:
- CNS: apathy, slowed cognition
- Skin and appendages: skin dryness, alopecia
- Lipid profile: ↑ low-density lipoproteins, ↑ triglycerides
- Cold intolerance
-
Decreased sympathetic activity leads to:
- Decreased sweating
- Cold skin (due to decreased blood flow)
- Constipation (due to decreased gastrointestinal motility)
- Bradycardia
- Decreased transcription of sarcolemmal genes (e.g., calcium ATPases) → decreased cardiac output, myopathy
- Hyperprolactinemia: ↑ prolactin production is stimulated by TRH → suppression of LH, FSH, GnRH, and testosterone and stimulation of breast tissue growth
-
Myxedema: due to accumulation of glycosaminoglycans and hyaluronic acid within the reticular layer of the dermis
- Complex protein mucopolysaccharides bind water → nonpitting edema
- Initially, edema is pretibial, but as the condition progresses it can generalize, resulting in a range of symptoms (see “Clinical features” below).

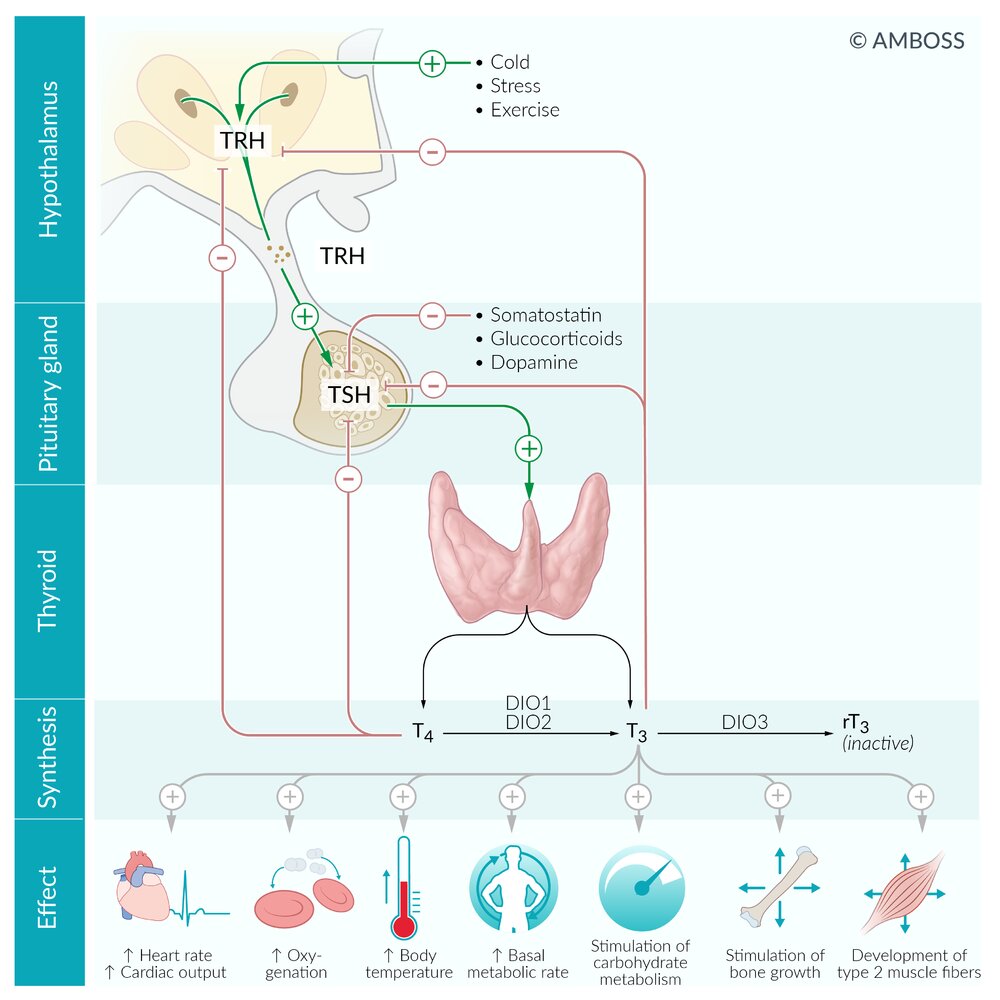
Energy-intensive processes (e.g., stress, physical activity, and cold) stimulate the release of thyrotropin-releasing hormone (TRH) from the hypothalamus. TRH reaches the adenohypophysis, simulating the release of thyroid-stimulating hormone (TSH), which, in turn, stimulates the synthesis and release of T4 and T3 in the thyroid gland.
T4 and T3 bind to the transport proteins thyroxin-binding globulin (TBG), thyroxin-binding pre-albumin (TBPA), and albumin, for transportation in the bloodstream.
T4 and T3 (as well as other hormones, including somatostatin, glucocorticoids, and dopamine) negatively feedback on TSH and TRH.
Deiodinases of type I and II (DIO1, DIO2), predominantly located in the liver, kidneys, muscle cells, and the thyroid gland, catalyze the conversion of (relatively) inactive T4 into biologically active T3. Deiodinase of type III (DIO3), present in the placenta and the CNS, catalyzes the conversion of T4 into biologically inactive reverse T3 (rT3).
Thyroid hormone receptors are transcription factors, which regulate gene expression of certain proteins, thereby mediating the effects of thyroid hormones on a cellular basis.
© AMBOSS
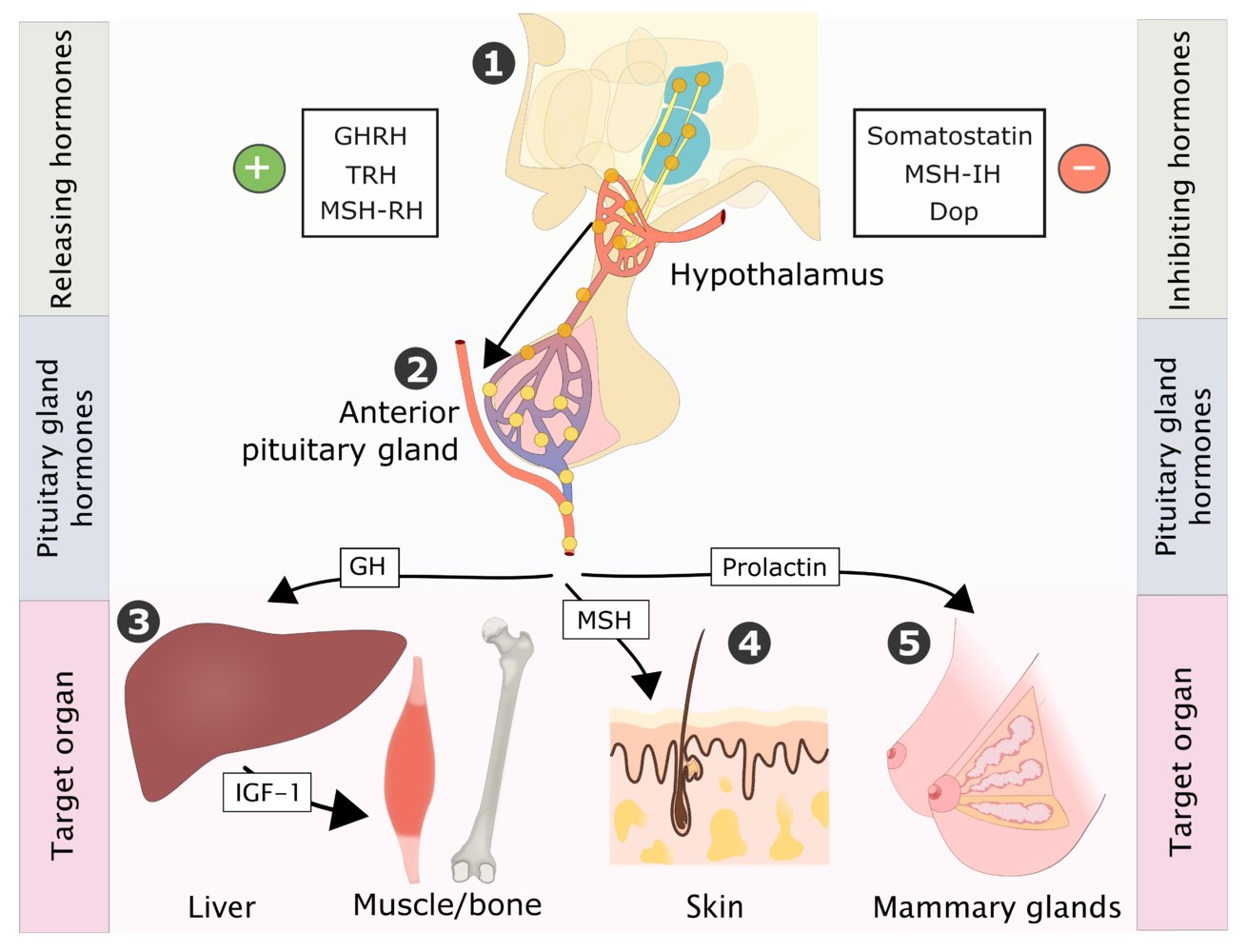
The nontropic releasing hormones are released in the hypothalamus (A) to the portal vascular system of the anterior pituitary gland (adenohypophysis , 2), where the nontropic hormones growth hormone (GH), melanocyte-stimulating hormone (MSH), and prolactin are released (2). These trigger the secretion of hormones in the target organs: GH leads to the secretion of insulin-like growth factor-1 (IGF-1) in the liver, which has an anabolic effect on the muscles and bones (3). In the skin, MSH stimulates the production of melanocytes (4). Prolactin triggers growth and lactation in the mammary glands (5). The inhibiting hormones are also released in the hypothalamus and subsequently reach the anterior pituitary gland, where they inhibit the release of nontropic hormones.
(GHRH = growth hormone-releasing hormone, TRH = thyrotropin-releasing hormone, MSH-RH = melanocyte-stimulating hormone-releasing hormone, MSH-IH = melanocyte-stimulating hormone-inhibiting hormone, Dop = dopamine)
© AMBOSS
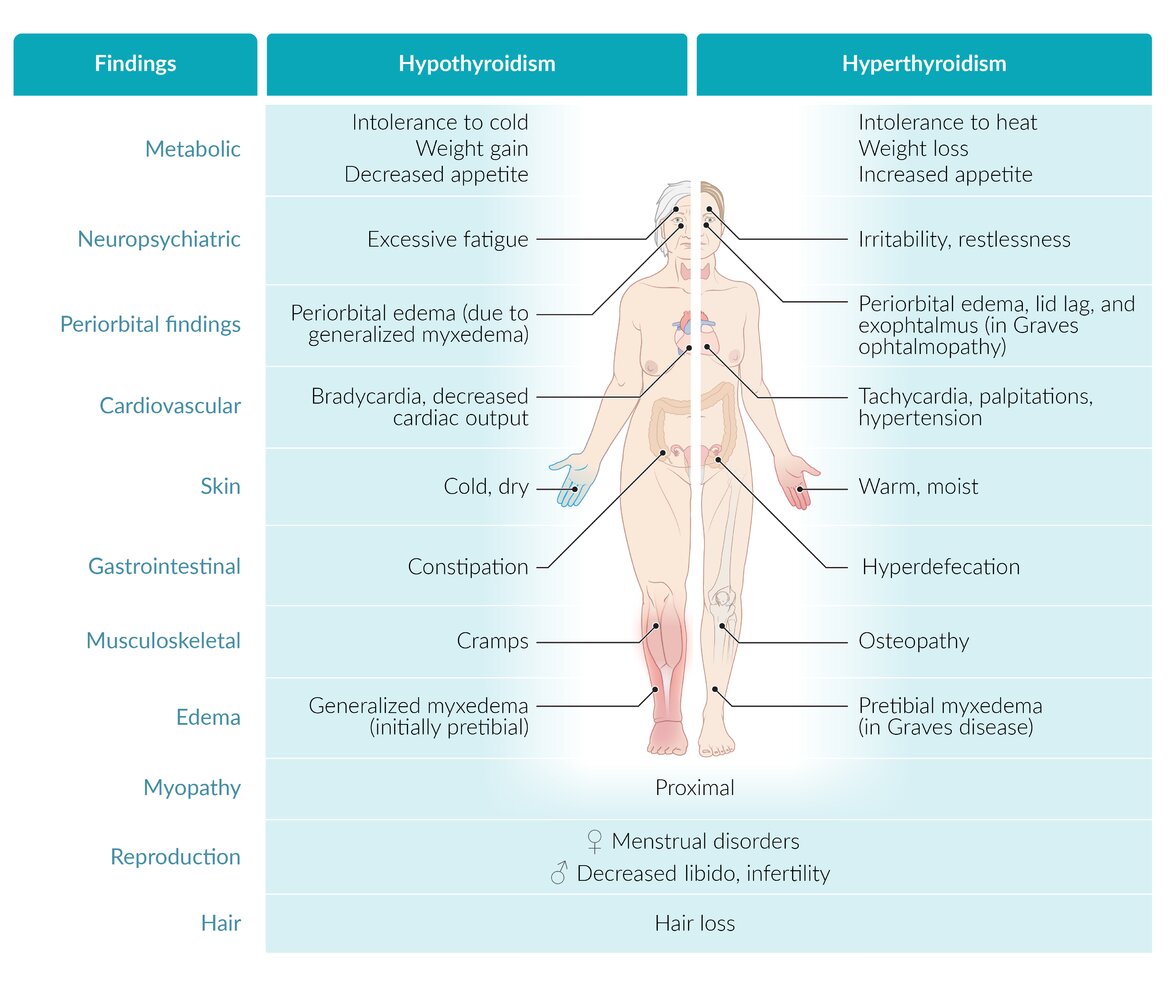
Clinical features
-
Symptoms related to decreased metabolic rate
- Fatigue, decreased physical activity
- Cold intolerance
- Decreased sweating
- Hair loss (Queen Anne sign), brittle nails, and cold, dry skin
- Weight gain (despite poor appetite)
- Constipation
- Bradycardia
- Hypothyroid myopathy, myalgia, stiffness, cramps
- Woltman sign: a delayed relaxation of the deep tendon reflexes, which is commonly seen in patients with hypothyroidism, but may also be associated with advanced age, pregnancy, and diabetes mellitus.
- Entrapment syndromes (e.g., carpal tunnel syndrome)
-
Symptoms related to generalized myxedema
- Doughy skin texture, puffy appearance
- Myxedematous heart disease (dilated cardiomyopathy, bradycardia, dyspnea)
- Hoarse voice, difficulty articulating words
- Pretibial and periorbital edema, generalized nonpitting edema
- Myxedema coma (see “Complications” below)
-
Symptoms of hyperprolactinemia
- Abnormal menstrual cycle; (esp. secondary amenorrhea; or menorrhagia)
- Galactorrhea
- Decreased libido, erectile dysfunction, delayed ejaculation, and infertility in men
-
Further symptoms
- Impaired cognition; (concentration, memory), somnolence, depression
- Hypertension [10]
- Goiter (in Hashimoto thyroiditis) or atrophic thyroid (in atrophic thyroiditis)
Older patients may not have typical symptoms of hypothyroidism. Instead, they may appear to have dementia or depression.
© AMBOSS
Hypothyroid myopathy
-
Epidemiology
- Occurs in 30–80% of individuals with hypothyroidism [11]
- Most common in patients with Hashimoto thyroiditis [12]
- ♂ = ♀
- Age of onset: < 40 years
-
Clinical features [12]
- Slowly progressive proximal muscle weakness
- Myalgia, muscle cramps, increased muscle tone
- Myoedema (highly specific sign): localized painless muscle contraction induced by light muscle percussion or pressure that manifests with palpable muscle swelling.
- Exercise intolerance (e.g., exertional pain)
- Sensorimotor polyneuropathy
- Slow DTRs and movement
- Dupuytren contracture, trigger digit, carpal tunnel syndrome
- Rare: rhabdomyolysis, compartment syndrome, Hoffmann syndrome, Kocher-Debre-Semelaigne syndrome
-
Diagnosis [12]
- ↑ Creatine kinase: 10–100× ULN
- LDH: may be elevated
- Thyroid autoantibodies: TgAB > TPOAb [13]
- Electromyography: may show EMG findings of myopathy (nonspecific finding)
- Muscle biopsy: indicated for the differential diagnosis of myopathy, usually normal
-
Treatment [12]
- Thyroid hormone replacement (see “Treatment of hypothyroidism”)
- Most patients recover within months of starting levothyroxine replacement. [14]
Hypothyroid myopathy is a clinical feature of hypothyroidism. Perform a diagnostic workup for hypothyroidism in undiagnosed patients with persistently elevated muscle enzymes (e.g., creatine kinase, LDH).
Diagnosis
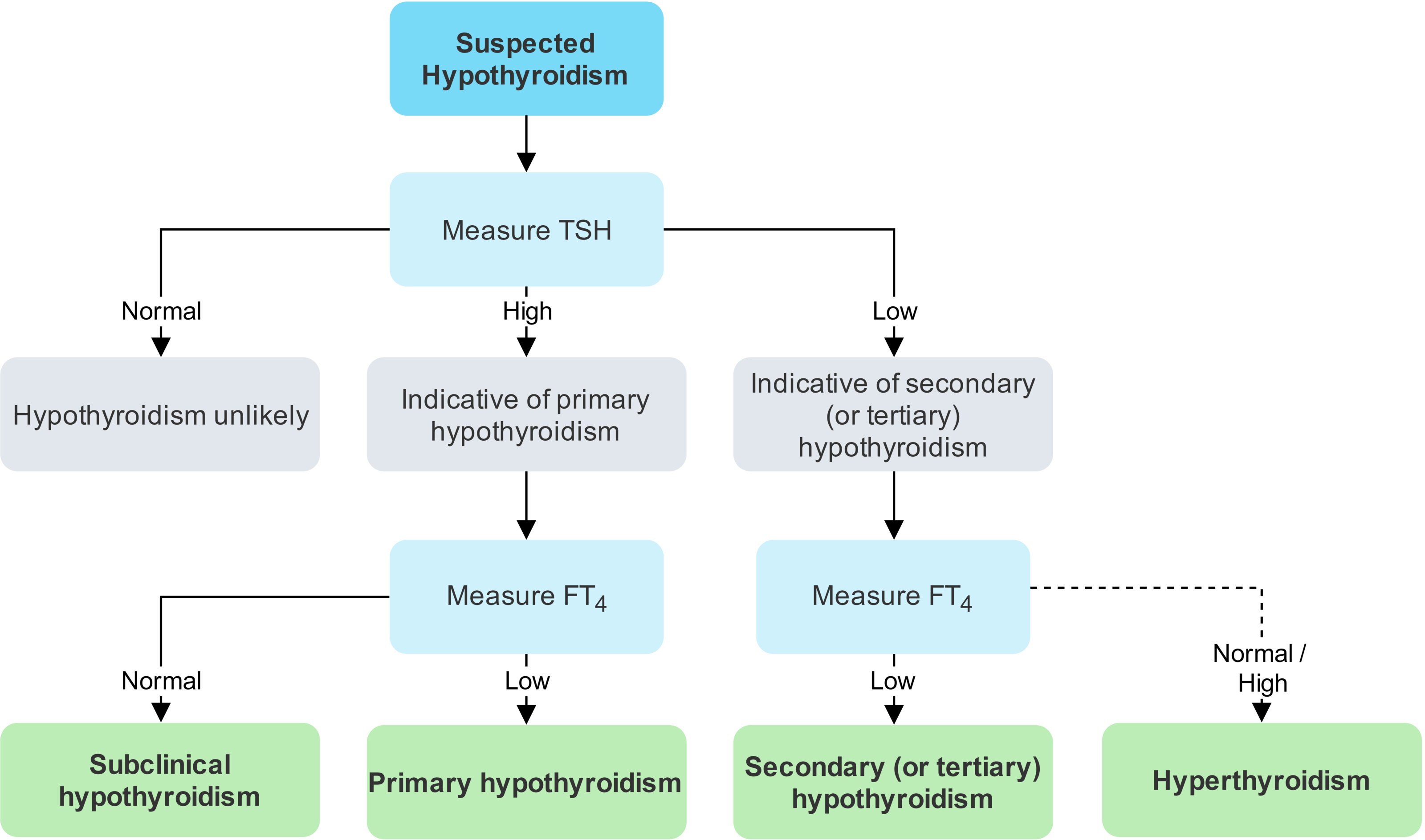
Approach [15][16]
-
Initial evaluation: thyroid function tests (TFTs)
- Obtain TSH level for all patients: ↑ TSH with classic clinical features is typically diagnostic for primary hypothyroidism.
- Abnormal TSH: Order FT4.
-
Further investigations: may be indicated to evaluate underlying etiology based on clinical suspicion (See also “Overview of common causes of primary hypothyroidism.”)
- Thyroid antibody testing: Consider if autoimmune thyroiditis is suspected (not routinely indicated). [15]
- Imaging: Consider if structural pathology (e.g., thyroid nodules, goiters, malignancy) is suspected. [17][18]
Normal TSH levels generally rule out primary hypothyroidism and hyperthyroidism and are therefore the decisive parameter in screening for both conditions. [19]


Laboratory studies
Thyroid function tests [15][16]
-
TSH
- Best initial screening test; also used to diagnose and monitor primary hypothyroidism
- Reference ranges vary between laboratories and differ in pregnancy and with increasing age. [15]
-
FT4
- Confirmatory test for primary hypothyroidism if TSH is elevated
- Primary test in suspected secondary or tertiary hypothyroidism and following treatment for hyperthyroidism
- Free or total T3: may be measured alongside FT4, but not used for the diagnosis of hypothyroidism
| Overview of TFT findings in the evaluation of suspected hypothyroidism [16][20] | |||||
|---|---|---|---|---|---|
| TSH | FT4 | FT3 | |||
| Subclinical hypothyroidism | Mildly ↑ | Normal | Normal | ||
| Overt hypothyroidism | Primary hypothyroidism | ↑ | ↓ | Normal or ↓ | |
| Secondary and tertiary hypothyroidism | ↓ | ||||
| Euthyroid sick syndrome [21] | Low T3 syndrome | Normal | Normal | ↓ Free T3 and ↑ reverse T3 | |
| Low T3 low T4 syndrome | ↓ | ↓ | |||
Avoid routine TSH screening in acutely ill patients unless a thyroid disturbance is the suspected cause (e.g., myxedema coma), since other non-thyroid illnesses can interfere with serum TSH and results may be unreliable. [15]
TSH can be abnormal in both hyperthyroidism and hypothyroidism. Peripheral hormones (FT4 and FT3) are elevated in hyperthyroidism as opposed to hypothyroidism, in which levels are reduced. [16]
Serum thyroid antibody testing [15][22]
Serum thyroid antibody testing can confirm suspected autoimmune thyroid disease. Thyroid peroxidase antibody measurements may also be considered in patients with subclinical hypothyroidism or recurring miscarriages.
- Thyroglobulin antibodies (TgAb) and thyroid peroxidase antibodies (TPOAb): detectable in the majority of patients with autoimmune hypothyroidism
- TSH receptor antibodies (TRAbs): detectable in up to 20% of cases of autoimmune hypothyroidism [23]
Associated laboratory findings [16]
Other routine blood tests are not required for the diagnosis but may show characteristic changes.
- CBC: mild anemia
- BMP: hyponatremia (in acute hypothyroidism) , hypoglycemia (rare) [24][25]
- Lipid profile: hypercholesterolemia (increased LDL), hyperlipidemia
- Creatine kinase: increased in hypothyroid myopathy [26]
Imaging [18]
Imaging has no role in the primary evaluation of hypothyroidism but may be indicated if structural abnormalities are present or suspected.
-
Thyroid ultrasound [17]
- Useful for the assessment of thyroid vascularity, goiters, and thyroid nodules
- Possible findings in hypothyroidism include signs of thyroiditis.
-
Nuclear medicine thyroid scan [27]
- May be indicated in the workup of thyroid nodules and goiters
- In hypothyroidism, radiotracer activity is decreased.
- MRI brain (including pituitary gland): for suspected central hypothyroidism[28][29]
© AMBOSS
© AMBOSS
Differential diagnoses
Nonthyroidal illness syndrome (NTIS) [21][30]
-
Description
- A change in thyroid hormone levels (typically decreased) that occurs in severe illness or severe physical stress
- Common in intensive care patients and associated with morbidity and mortality
- Also known as euthyroid sick syndrome (ESS)
-
Pathophysiology: multifactorial and not fully understood [31]
- Thyroid gland function typically remains normal.
- Cytokines (e.g., interleukin 6) are thought to cause various changes in levels of circulating TSH and thyroid hormones.
- Altered deiodinase enzyme activity leads to:
- ↓ Conversion of T4 to T3
- ↑ Conversion of T4 to reverse T3 (rT3) by thyroxine 5-monodeiodinase
- Various factors, e.g., protein loss due to nephrotic syndrome, may also lead to decreased levels of thyroid-binding globulin.
-
Clinical features
- Signs and symptoms of the underlying illness
- Typically no classic symptoms of hyper- or hypothyroidism
-
Diagnostics
- NTIS is typically diagnosed incidentally following TFT screening done in critically ill patients to rule out thyrotoxicosis or hypothyroidism as the underlying cause, e.g., patients with unexplained tachyarrhythmias or heart failure, suspected myxedema coma, or a strong family history of thyroid disease.
-
TSH is typically normal in both low T3 syndrome and low T3 low T4 syndrome.
- Low T3 syndrome: decrease in both total and FT3 levels, normal FT4 and TSH, and normal or increased rT3
- Low T3 low T4 syndrome: FT4 levels may be low in prolonged courses of illness, indicating a poor prognosis.
- Rarely, TSH may also be slightly low, but not enough to explain the low FT3 and/or FT4.
- Consult endocrinology as the interpretation of TFTs in critically ill patients is complex and can be misleading.
-
Treatment
- Continued treatment of underlying illness
- Thyroid hormone replacement is usually not recommended. [32]
Suspect NTIS in critically-ill patients who have a combination of the following: ↓ FT3, normal or ↓ FT4, normal or ↓ TSH, and absent typical clinical features of hypothyroidism. [21]
Other differential diagnoses [33]
The following conditions can mimic one or more manifestations of hypothyroidism:
- Adrenal insufficiency
- Hypopituitarism (can also be a cause of central hypothyroidism)
- CHF and other causes of pulmonary edema
- Other causes of shock
- Sepsis and other systemic infections
- Depression
- Major neurocognitive disorders
- Encephalopathy
- Environmental hypothermia
- Other differential diagnoses of constipation
The differential diagnoses listed here are not exhaustive.
Treatment
General principles [15][20][32]
-
Hypothyroidism is treated with lifelong hormone substitution.
-
Levothyroxine: synthetic form of T4
- First-line choice for the treatment of hypothyroidism
- Peripherally converted to T3 (biologically active metabolite) and rT3 (biologically inactive metabolite)
-
Liothyronine: synthetic form of T3
- Part of the treatment for myxedema coma
- Not recommended as monotherapy or in combination with levothyroxine for the long-term treatment of hypothyroidism [15][34][35]
-
Levothyroxine: synthetic form of T4
- Starting dose and monitoring requirements vary depending on factors such as age and comorbidities.
- Reassess treatment response regularly to avoid undertreatment and overtreatment.
Indications for treatment [15][32]
- Overt hypothyroidism: Initiate treatment.
-
Subclinical hypothyroidism: Treat select patients. [15][34]
- Repeat TSH measurement after 1–3 months to confirm the diagnosis. [36]
- Consider treatment in the following cases:
- TSH ≥ 10 mIU/L
- TSH < 10 mIU/L in addition to one of the following: positive TPOAb, cardiovascular risk factors, planned or current pregnancy
Ensure follow-up is in place for patients with subclinical hypothyroidism if treatment is not initiated.
Levothyroxine replacement [15][32]
- In primary hypothyroidism, levothyroxine is gradually titrated according to serial TSH measurements targeting a normal level; for example:
- ↑ TSH (suggests ↓ T4 activity): typically requires a dose increase
- ↓ TSH (suggests ↑ T4 activity): typically requires a dose decrease
- In secondary hypothyroidism, dosage is titrated according to FT4 levels.
| Dosage and administration of levothyroxine | |
|---|---|
| Dosage |
|
| Monitoring and dose adjustments |
|
| Administration |
|
Dosing in consultation with endocrinology is recommended for: [15]
| |
Titrate thyroid hormone substitution carefully for individuals with preexisting coronary artery disease. [32]
In patients with hypothyroidism who are pregnant, the levothyroxine dose must be increased in line with increased demand. Hypothyroidism adversely affects the development of the fetal nervous system. [16]
Long-term therapy considerations [15][32][39]
-
Side effects: Overtreatment can lead to symptoms of thyrotoxicosis.
- Sweating, heat intolerance, tremors
- Tachycardia; , palpitations, arrhythmias
- Weight loss, osteoporosis
- See also “Exogenous thyrotoxicosis.”
-
Drug interactions
- Drugs that reduce levothyroxine absorption include PPIs, calcium salts, ferrous sulfate, and bile acid sequestrants.
- Treatment with estrogens may necessitate a dose increase.
- Treatment with androgens may necessitate a dose reduction.
- Glucocorticoids interfere with thyroid hormone metabolism and the dose of levothyroxine may need to be reduced.
-
Reasons for treatment failure
- Nonadherence
- Malabsorption due to gastrointestinal conditions (e.g., gastritis, celiac disease)
Some individuals may misuse synthetic thyroid hormones for weight loss. [40]
Complications
Myxedema coma [41][42]
- Definition: : extremely rare, potentially life-threatening decompensation of preexisting thyroid hormone deficiency
-
Etiology
- Triggers include infections, severe illness or trauma, and certain drugs.
- Prior discontinuation of thyroid supplements is a frequent contributing factor in patients with known hypothyroidism.
-
Clinical presentation
- Cardinal symptoms: impaired mental status; , hypothermia; , and myxedema
- Hypoventilation with hypercapnia and hypoxemia
- Hypotension (possibly shock) and bradycardia
-
Diagnosis [43]
-
Laboratory studies
- TFTs: ↑ TSH and ↓ T4 and T3
- BMP: hypoglycemia and hyponatremia [24]
- ↓ Cortisol in patients with concomitant adrenal insufficiency
- Other possible findings: ↑ CK and LDH, abnormal clotting
- ECG: low-voltage QRS complexes, nonspecific T-wave changes [41]
- CSF analysis: slightly ↑ CSF protein [42]
-
Laboratory studies
-
Treatment [32][33][41]
- Immediate measures: airway management and fluid resuscitation (See “ABCDE approach.”)
- Intravenous hormone substitution: levothyroxine PLUS liothyronine PLUS hydrocortisone [32]
- Supportive treatment: passive rewarming, ventilatory support as indicated, management of precipitating factors, treatment of hypoglycemia
- Disposition: Admission to critical care is typically warranted for ventilatory support, invasive monitoring, and management of electrolytes and fluids. [33]
- Prognosis: Even with treatment, mortality rates of up to 60% have been described. [41]
Remember to evaluate precipitating factors, e.g., screening for infectious causes, or obtaining cardiac enzymes and an ECG to exclude myocardial infarction. [41]
Suspect myxedema coma in patients with typical symptoms and a history of hypothyroidism, and initiate treatment immediately without waiting for laboratory results! [41]
Further complications
-
Primary thyroid lymphoma
- Hashimoto thyroiditis is the most common cause of hypothyroidism and the only known risk factor for primary thyroid lymphoma. [44]
- Almost all primary thyroid lymphomas are non-Hodgkin large B-cell lymphomas.
- Increased cardiovascular risk
- Carpal tunnel syndrome [45]
We list the most important complications. The selection is not exhaustive.
Acute management checklist for myxedema coma
- Perform ABCDE survey.
- Secure airway and begin ventilatory support if there is respiratory failure.
- Establish IV access and send blood samples for thyroid function tests, cortisol, BMP, CK, LDH, and coagulation panel.
- Start fluid resuscitation and vasopressors as needed.
- Begin continuous cardiac and respiratory monitoring and consider invasive BP monitoring.
- Check core temperature and consider passive rewarming.
- Identify and treat hypoglycemia.
- Urgently consult endocrinology and critical care for admission.
- Administer IV hydrocortisone together with or prior to thyroid hormone replacement and continue until concomitant adrenal insufficiency is ruled out. [32]
- Start IV levothyroxine and IV liothyronine.
- Identify and treat precipitating factors.
- Admit to ICU.
Special patient groups
Hypothyroidism in children may be acquired or congenital. Tailor diagnosis and management approaches accordingly.
Congenital hypothyroidism
Epidemiology [5]
- US: affects ∼ 1:2300 newborns
- Worldwide: affects up to 1:2000 newborns
Etiology [6][46]
Permanent congenital hypothyroidism
-
Primary congenital hypothyroidism: defects in the thyroid gland or thyroid hormone synthesis
-
Thyroid dysgenesis (most common)
- Thyroid hypoplasia, dysplasia, or ectopy
- Thyroid aplasia (athyroidism)
- Hereditary dyshormonogenetic goiter: Defects in thyroid hormone synthesis (most commonly in thyroid peroxidase) lead to thyroid hyperplasia and goiter. [29]
-
Thyroid dysgenesis (most common)
- Central congenital hypothyroidism: rare; usually caused by pituitary disease [29]
Transient congenital hypothyroidism [47]
- Transplacental transmission of maternal antithyroid antibodies
- Fetal iodine deficiency syndrome: congenital hypothyroidism caused by iodine deficiency in utero (rare in iodine-sufficient areas) [47]
Congenital hypothyroidism may occur as part of another condition or genetic syndrome (e.g., Down syndrome). [6]
Clinical features of congenital hypothyroidism [6][29]
-
Onset
- Usually few or no features are present at birth, as maternal T4 can cross the placenta. [46]
- Features develop over weeks to months if hypothyroidism is untreated.
-
General features [6][29][48]
-
Signs and symptoms of hypothyroidism, e.g.:
- Hypothermia
- Bradycardia
- Constipation
- Growth faltering (length affected more than weight) [49]
-
Signs and symptoms of hypothyroidism, e.g.:
-
Neonatal features
- Umbilical hernia
- Prolonged neonatal jaundice
- Hypotonia
- Decreased activity and poor feeding
- Hoarse cry
- Coarse facial features, macroglossia
- Large posterior fontanelle
- Mottled skin
- Abdominal distension [50]
- Associated congenital anomalies (e.g. cardiac, renal, gastrointestinal, and skeletal anomalies) [29]
-
Features of severe untreated congenital hypothyroidism [6]
- Intellectual disability
- Short stature
- Hearing loss
Most children with congenital hypothyroidism are asymptomatic at birth because maternal thyroid hormone crosses the placenta. Newborn screening is essential to allow early treatment and prevent irreversible intellectual disability. [6][29]
The 7 Ps of congenital hypothyroidism are Pot-bellied, Pale, Puffy-faced, Protruding umbilicus, Protuberant tongue, Poor brain development, and Prolonged neonatal jaundice.
Newborn screening [6][51]
- Indication: all infants [6]
-
Methods [6]
- TSH and/or T4 measurements [6]
- Heel-stick blood specimen between 24 hours and 1 week of life (preferably between 48 and 72 hours)
-
Interpretation
-
Increased TSH levels and/or low T4
- Strongly suggest congenital hypothyroidism.
- Confirm diagnosis with thyroid function tests (see "Initial management").
- Normal TSH and T4 [6]
- Screen for high-risk features.
- Infants with high-risk features: Repeat screening for hypothyroidism at 2–4 weeks of age. [6]
-
Increased TSH levels and/or low T4
Congenital hypothyroidism is among the conditions mandated for newborn screening under federal law. [52]
Initial management [6]
The following outlines management of congenital hypothyrodism picked up on neonatal screening, however, a similar approach should be taken for children with normal neonatal screening or absent neonatal screening who later present with clinical features of hypothyroidism. [6]
Approach
- Consult with pediatric endocrinology to guide diagnosis and management.
- Determine if immediate treatment is required before performing confirmatory tests. [6][51]
- TSH screening result > 40 mIU/L: Start levothyroxine while awaiting confirmatory results.
- TSH screening result ≤ 40 mIU/L: Review full TFTs before initiating treatment.
- Obtain thyroid function tests (ideally within 24 hours) and begin management based on results. [6][51]
- Start levothyroxine if the patient has:
- Overt hypothyroidism
- Normal free T4 but TSH > 20 mIU/L
- Low or normal TSH and low T4 (suspected central hypothyroidism)
- If the patient has a normal free T4 but elevated TSH of ≤ 20 mIU/L:
- Monitor thyroid function every 1–2 weeks.
- Begin levothyroxine if TSH remains > 10 mIU/L after 4 weeks of age. [6][53]
- Start levothyroxine if the patient has:
- Consider imaging and additional diagnostic studies.
- Consider a formal hearing evaluation if there is concern about hearing [6]
Levothyroxine [6]
- Initiate oral levothyroxine as soon as possible after diagnosis.
-
Titrate the dose in consultation with endocrinology with the aim of normalizing: [6][29]
- T4 levels within 2 weeks
- TSH within 4 weeks
- Lifelong hormone replacement is necessary for children with permanent congenital hypothyroidism.
Adequate dosing and prompt initiation of levothyroxine treatment helps preserve normal long-term neurocognitive function. [6][29]
Imaging [6][53]
- Thyroid imaging is only performed if results will change management.
- Can identify thyroid dysgenesis
- Modalities include:
- Ultrasound: no radiation, but sensitivity is lower than scintigraphy
- Scintigraphy: radiation exposure; must be performed when TSH is elevated
Additional diagnostics based on risk factors [6][46]
- History of maternal autoimmune disease [6]
- Obtain TSH receptor antibody (TRAb) levels
- If levels are elevated, continue levothyroxine but advise caregivers that the hypothyroidism is likely transient.
- Features of central hypothyroidism (e.g., low or normal TSH and low T4)
- Obtain thyroxine-binding globulin concentration if TSH is low and free T4 is normal. [6]
- Assess for additional pituitary hormone deficits. [29]
- Consider:
- CNS imaging [29]
- Genetic testing in consultation with a geneticist [6]
- Clinical features of a recognizable syndrome or genetic condition: Obtain genetic testing. [6]
Follow-up
- Ensure regular follow-up throughout infancy and childhood to track growth and development and monitor treatment adherence. [6][6]
- Adjust levothyroxine dose to keep TSH and FT4 within the age-specific reference range. [6]
- Monitor thyroid function test results frequently after treatment adjustments. [6][29]
- Permanence of congenital hypothyroidism is confirmed by any of the following: [6]
- Serum TSH rise by > 10 mIU/L after the first year of life
- Thyroid dysgenesis on imaging
- Trial discontinuation of levothyroxine at 3 years of age; elevated TSH or low free T4 after 4 weeks
Acquired hypothyroidism in children
Etiology [32]
- The etiology of hypothyroidism is similar in adults and children with acquired hypothyroidism.
- Hashimoto thyroiditis is the most common cause in children in the US. [29]
-
Risk factors for autoimmune thyroid disease in children include: [29]
- Genetic syndromes (e.g., Down syndrome, Turner syndrome)
- Other autoimmune conditions (e.g., diabetes mellitus, celiac disease, vitiligo)
Iodine deficiency is rare in the US but is the most common cause of acquired hypothyroidism in children worldwide. [29]
Clinical features [32][46]
In addition to general signs and symptoms of hypothyroidism, children with acquired hypothyroidism may have:
- Linear growth failure [32]
- Delayed puberty [29]
Goiter is the most common sign of acquired hypothyroidism in children. [29]
Diagnosis [32][46]
- The diagnostic workup for hypothyroidism is similar in adults and children.
- Similar to in adults, thyroid ultrasonography is not part of the primary workup but may be used to identify the underlying cause. [46]
The presence of antithyroid antibodies (e.g., TPOAb) in patients with subclinical hypothyroidism is a predictor of conversion to overt hypothyroidism. [29][32]
Management [32][46]
Management of hypothyroidism in adults and children is similar; consult pediatric endocrinology for treatment guidance. [32]
-
Overt hypothyroidism
- Initiate levothyroxine replacement to reverse symptoms and restore normal growth and development. [32]
- Adjust levothyroxine dose as needed throughout childhood to maintain serum TSH and FT4 levels within desired age-adjusted reference ranges. [32][46]
- Perform regular developmental surveillance throughout childhood. [32]
-
Subclinical hypothyroidism
- TSH > 10 mIU/L: Consider levothyroxine if symptomatic or if risk factors for progression to overt hyperthyroidism are present (e.g., positive autoantibodies, goiter, other autoimmune diseases). [32][46]
- TSH ≤ 10 mIU/L: Levothyroxine is not typically recommended. [32]
External Resources
- 2022 AAP Clinical Report on Congenital Hypothyroidism: Screening and Management
- 2017 ATA Guidelines for the Diagnosis and Management of Thyroid Disease during Pregnancy and the Postpartum
- 2014 ATA Guidelines for the Treatment of Hypothyroidism
- 2012 AACE/ATE Clinical Practice Guidelines for Hypothyroidism in Adults
References
- Vanderpump MP. "The epidemiology of thyroid disease". Br Med Bull. 99(1). :39-51. (2011)
- Caturegli P, De Remigis A, Rose NR. "Hashimoto thyroiditis: Clinical and diagnostic criteria". Autoimmun Rev. 13(4-5). :391-397. (2014)
- Stagnaro-Green A. "Postpartum thyroiditis". Best Practice & Research Clinical Endocrinology & Metabolism. 18(2). :303-316. (2004)
- Alfadda AA et al. "Subacute Thyroiditis: Clinical Presentation and Long Term Outcome". International Journal of Endocrinology. 2014. :1-7. (2014)
- Rastogi MV, LaFranchi SH. "Congenital hypothyroidism". Orphanet J Rare Dis. 5(1). (2010)
- Rose SR, Wassner AJ, Wintergerst KA, et al. "Congenital Hypothyroidism: Screening and Management (Clinical Report)". Pediatrics. 151(1). (2022)
- James V. Hennessey. "Riedel's Thyroiditis: A Clinical Review". The Journal of Clinical Endocrinology & Metabolism. 96(10). :3031-3041. (2011)
- Yamada M, Mori M. "Mechanisms related to the pathophysiology and management of central hypothyroidism". Nat Clin Pract Endocrinol Metab. 4(12). :683-694. (2008)
- Kumar V, Abbas AK, Aster JC. "Robbins & Cotran Pathologic Basis of Disease". Elsevier Saunders. (2014). ISBN: 9781455726134
- Stabouli S, Papakatsika S, Kotsis V. "Hypothyroidism and hypertension". Expert Rev of Cardiovasc Ther. 8(11). :1559-1565. (2010)
- Garber JR, Cobin RH, Gharib H, et al. "Clinical practice guidelines for hypothyroidism in adults: cosponsored by the American Association of Clinical Endocrinologists and the American Thyroid Association". Endocr Pract. 18(6). :988-1028. (2012)
- Jameson JL, Fauci AS, Kasper DL, et al. "Harrison's Principles of Internal Medicine, Twentieth Edition (Vol.1 & Vol.2)". McGraw-Hill Education / Medical. (2018). ISBN: 9781259644030
- Hart JL, Lloyd C, Harvey CJ. "Ultrasound of the thyroid". British Journal of Hospital Medicine. 69(5). :68-71. (2008)
- Hoang JK, Oldan JD, Mandel SJ, et al. "ACR Appropriateness Criteria® Thyroid Disease". J Am Coll Radiol. 16(5). :S300-S314. (2019)
- Sheehan MT. "Biochemical Testing of the Thyroid: TSH is the Best and, Oftentimes, Only Test Needed – A Review for Primary Care". Clin Med Res. 14(2). :83-92. (2016)
- Gaitonde DY, Rowley KD, Sweeney LB. "Hypothyroidism: an update.". American Family Physician. 86(3). :244-51. (2012)
- Fliers E, Boelen A. "An update on non-thyroidal illness syndrome". J Endocrinol Invest. 44(8). :1597-1607. (2020)
- Froehlich E, Wahl R. "Thyroid autoimmunity: role of anti-thyroid antibodies in thyroid and extra-thyroidal diseases". Front Immunol. 8. (2017)
- Ajjan R, Weetman A. "Techniques to quantify TSH receptor antibodies". Nat Clin Pract Endocrinol Metab. 4(8). :461-468. (2008)
- Liamis G, Filippatos TD, Liontos A, Elisaf MS. "MANAGEMENT OF ENDOCRINE DISEASE: Hypothyroidism-associated hyponatremia: mechanisms, implications and treatment". Eur J Endocrinol. 176(1). :R15-R20. (2016)
- Bhutani J, Yadav T, Upadhyay M, Raghunandan S. "Recurrent hypoglycemia: An unusual finding of hypothyroidism". Thyroid Res Pract. 14(3). :127. (2017)
- Scott KR, Simmons Z, et al. "Hypothyroid myopathy with a strikingly elevated serum creatine kinase level". Muscle Nerve. 26(1). :141-144. (2002)
- Giovanella L, Avram AM, Iakovou I, et al. "EANM practice guideline/SNMMI procedure standard for RAIU and thyroid scintigraphy". Eur J Nucl Med Mol Imaging. 46(12). :2514-2525. (2019)
- Persani L, Brabant G, Dattani M, et al. "2018 European Thyroid Association (ETA) Guidelines on the Diagnosis and Management of Central Hypothyroidism". Eur Thyroid J. 7(5). :225-237
- Hanley P, Lord K, Bauer AJ. "Thyroid Disorders in Children and Adolescents: A Review". JAMA Pediatr. 170(10). :1008-1019. (2016)
- Iervasi G, Pingitore A, et al. "Low-T3 Syndrome". Circulation. 107(5). :708-713. (2003)
- Moura Neto A, Zantut-Wittmann DE. "Abnormalities of Thyroid Hormone Metabolism during Systemic Illness: The Low T3 Syndrome in Different Clinical Settings". Int J Endocrinol. 2016. :1-9. (2016)
- Jonklaas J, Bianco AC, Bauer AJ, et al. "Guidelines for the Treatment of Hypothyroidism: Prepared by the American Thyroid Association Task Force on Thyroid Hormone Replacement". Thyroid. 24(12). :1670-1751. (2014)
- Walls R, Hockberger R, Gausche-Hill M. "Rosen's Emergency Medicine". Elsevier Health Sciences. (2018). ISBN: 9780323354790
- Alexander EK, Pearce EN, Brent GA, et al. "2017 Guidelines of the American Thyroid Association for the diagnosis and management of thyroid disease during pregnancy and the postpartum". Thyroid. 27(3). :315-389. (2017)
- Hennessey JV, Espaillat R. "Current evidence for the treatment of hypothyroidism with levothyroxine/levotriiodothyronine combination therapy versus levothyroxine monotherapy". Int J Clin Pract. 72(2). :e13062. (2018)
- Biondi B, Cappola AR, Cooper DS. "Subclinical Hypothyroidism". Journal of the American Medical Association. 322(2). :153. (2019)
- "Global Tuberculosis Report 2019"
- Martinez Quintero B, Yazbeck C, Sweeney LB. "Thyroiditis: evaluation and treatment". Am Fam Physician. 104(6). :609-617. (2021)
- Colucci P, Yue CS, Ducharme M, Benvenga S. "A Review of the Pharmacokinetics of Levothyroxine for the Treatment of Hypothyroidism.". European endocrinology. 9(1). :40-47. (2013)
- Bernet VJ. "Thyroid hormone misuse and abuse". Endocrine. 66(1). :79-86. (2019)
- Mathew V, Misgar RA, et al. "Myxedema Coma: A New Look into an Old Crisis". J Thyroid Res. 2011. :1-7. (2011)
- Wall CR. "Myxedema coma: diagnosis and treatment". Am Fam Physician. 62(11). :2485-90. (2000)
- Markus Luster, Leonidas H. Duntas, Leonard Wartofsky. "The Thyroid and Its Diseases: A Comprehensive Guide for the Clinician". Springer. (2019). ISBN: 9783319721026
- R K Pedersen, N T Pedersen. "Primary non-Hodgkin's lymphoma of the thyroid gland: a population based study.". Histopathology. (1996)
- Shiri R. "Hypothyroidism and carpal tunnel syndrome: a meta-analysis". Muscle Nerve. 50(6). :879-883. (2014)
- Bauer AJ, Wassner AJ. "Thyroid hormone therapy in congenital hypothyroidism and pediatric hypothyroidism". Endocrine. 66(1). :51-62. (2019)
- Rose SR, Brown RS. "Update of Newborn Screening and Therapy for Congenital Hypothyroidism". Pediatrics. 117(6). :2290-2303. (2006)
- Léger J, Olivieri A, Donaldson M, et al. "European Society for Paediatric Endocrinology consensus guidelines on screening, diagnosis, and management of congenital hypothyroidism". J Clin Endocrinol Metab. 99(2). :363-84. (2014)
- Grüters A, Krude H. "Detection and treatment of congenital hypothyroidism". Nat Rev Endocrinol. 8(2). :104-113. (2011)
- Kliegman RM, III JWSG, pédiatre) JWSG. "Nelson Textbook of Pediatrics: 22nd edition". Elsevier. (2024). ISBN: 9780323883085
- "Newborn screening: Toward a uniform screening panel and system"
- "Screening for congenital hypothyroidism: US Preventive Services Task Force reaffirmation recommendation.". Ann Fam Med. 6(2). :166. (2008)
- Rose S, Wassner A, Wintergerst K, et al. "Congenital Hypothyroidism: Screening and Management (Technical Report)". Pediatrics. 151(1). (2022)
- Lin N, Wang J, Liao W, Wen Y. "Hypothyroid myopathy with periodic paralysis as the main symptom: a case report and literature review". Ann Palliat Med. 9(5). :3698-3704. (2020)
- Sindoni A, Rodolico C, Pappalardo MA, Portaro S, Benvenga S. "Hypothyroid myopathy: A peculiar clinical presentation of thyroid failure. Review of the literature". Rev Endocr Metab Disord. 17(4). :499-519. (2016)
- Rodolico C, Toscano A, Benvenga S, et al. "Myopathy as the Persistently Isolated Symptomatology of Primary Autoimmune Hypothyroidism". Thyroid. 8(11). :1033-1038. (1998)
- Jervis W, Shah N, Mongolu SK, Sathyapalan T. "Severe proximal myopathy secondary to Hashimoto's thyroiditis". BMJ Case Rep. 12(7). (2019)
- Kothari MJ. "Carpal tunnel syndrome: Etiology and epidemiology". UpToDate. UpToDate. http://www.uptodate.com/contents/carpal-tunnel-syndrome-etiology-and-epidemiology?source=search_result&search=carpal+tunnel+syndrome&selectedTitle=3~135#H8. [2016-02-09]
- Braun MM, Barstow CH, Pyzocha NJ. "Diagnosis and management of sodium disorders: hyponatremia and hypernatremia". Am Fam Physician. 91(5). :299-307. (2015)
- Sinclair D. "Clinical and laboratory aspects of thyroid autoantibodies". Annals of Clinical Biochemistry. 43(3). :173-183. (2006)
- Surks MI, Ortiz E, Daniels GH, et al. "Subclinical Thyroid Disease". Journal of the American Medical Association. 291(2). :228. (2004)
- Vaidya B, Pearce SHS. "Management of hypothyroidism in adults". BMJ. 337. :284-289. (2008)
- Kalra S, Sahay R, Unnikrishnan A. "The hypoglycemic side of hypothyroidism". Indian Journal of Endocrinology and Metabolism. 18(1). :1-3. (2014)
- Hennessey JV, Espaillat R. "Diagnosis and Management of Subclinical Hypothyroidism in Elderly Adults: A Review of the Literature". Journal of American Geriatrics Society. 63(8). :1663-1673. (2015)