Summary
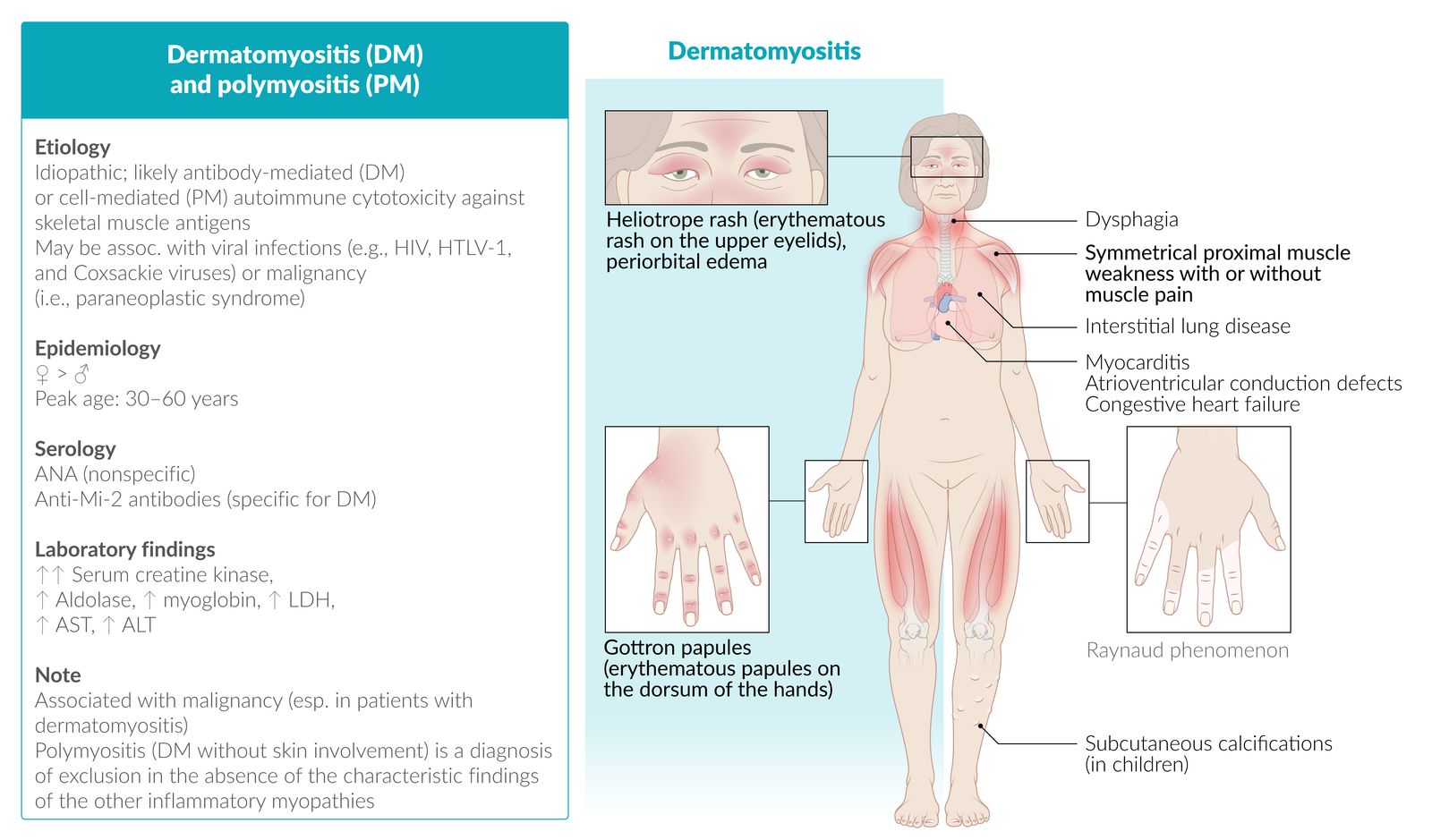
Idiopathic inflammatory myopathies (IIM) are a group of rare systemic diseases characterized by progressive weakness due to chronic skeletal muscle inflammation. They are classified based on clinicopathological findings into dermatomyositis (DM), overlap myositis (OM), immune-mediated necrotizing myopathy (IMNM), inclusion-body myositis (IBM), and polymyositis (PM). If onset occurs before the age of 18 years, it is called juvenile IIM, or JIIM. IIM typically manifests with proximal, symmetric weakness in appendicular muscles, which leads to difficulty reaching overhead, climbing the stairs, and/or standing up. The severity of muscle involvement can vary significantly between forms of IIM. In advanced disease, weakness may also affect oropharyngeal muscles (causing dysphagia and aspiration) and respiratory muscles (causing restrictive lung disease or even respiratory failure.) Patients may also have cutaneous features (including Gottron papules, heliotrope rash, and the shawl sign) and an increased risk of various malignancies (in DM, PM, and IMNM), and interstitial lung disease in some forms of DM, IMNM, and OM.
The diagnosis of suspected IIM is supported by laboratory tests, which show elevated muscle enzymes (e.g., creatine kinase, aldolase) as well as characteristic electromyogram (EMG) and biopsy findings. Management consists of supportive treatment (such as physical and occupational therapy) alongside immunosuppression with glucocorticoids and drugs such as methotrexate and azathioprine (except for IBM, for which treatment is supportive only).
Definitions
- Dermatomyositis (DM): : an inflammatory myopathy characterized by progressive symmetrical proximal muscle weakness and distinctive skin findings
- Overlap myositis (OM): any inflammatory myopathy that occurs in association with features of another autoimmune connective tissue disease. A classic form of OM is antisynthetase syndrome.
- Immune-mediated necrotizing myopathy (IMNM): an inflammatory myopathy affecting the proximal skeletal muscles that is particularly severe and associated with a markedly elevated CK level
- Inclusion body myositis (IBM): : an inflammatory myopathy affecting both the proximal and distal skeletal muscles
- Polymyositis (PM): : an inflammatory myopathy affecting the proximal skeletal muscles, with evidence of elevated CK and myositis on EMG and biopsy in the absence of any of the characteristic findings of the other IIM (a rare diagnosis of exclusion)
- Juvenile idiopathic inflammatory myopathy (JIIM): any inflammatory myopathy manifesting in an individual < 18 years old [1]
References:[2][3]
Epidemiology
-
Incidence
- PM and DM: 2/100,000 per year
- In the US, PM disproportionately affects the black population.
-
Sex
- PM and DM: ♀ > ♂ (2:1)
- IBM: ♂ > ♀ (2:1)
-
Peak incidence
- PM: 30–60 years
-
DM
- 5–15 years (juvenile dermatomyositis)
- 40–60 years (adult dermatomyositis)
- IBM: > 50 years
Epidemiological data refers to the US, unless otherwise specified.
Etiology
- The origin is unknown, but most forms of IM seem to involve an autoimmune reaction that leads to muscle inflammation, particularly in genetically susceptible individuals. Viral infections, malignancies, and connective tissue disorders may play a role.
- Polymyositis (PM): cell-mediated cytotoxicity: against unidentified skeletal muscle antigens, chiefly affecting the endomysium
- Dermatomyositis (DM): idiopathic or paraneoplastic antibody-mediated: vasculopathy, associated with malignancies (non-Hodgkin lymphoma; lung, stomach, colorectal, or ovarian cancer )
References:[4][5]
Clinical features
Clinical manifestations of IIM vary widely both between and within the subtypes. Symptoms can be grouped into three categories: muscle weakness, cutaneous features, and systemic manifestations. [2][6]
Muscle weakness
-
Limb weakness
- Symmetrical proximal muscle weakness and atrophy
- Commonly affects pelvic and shoulder girdle muscles, leading to difficulties combing hair, standing up from a sitting position, and climbing stairs
- Can also affect neck muscles (flexors more than extensors)
- May be accompanied by myalgia [7]
-
In inclusion body myositis, the weakness may be:
- Asymmetrical
- Additionally affecting distal muscle groups, making it hard to grip objects
-
Axial muscle weakness
- Oropharyngeal muscle weakness leading to dysphagia [8][9]
- Respiratory muscle weakness leading to restrictive lung disease
Cutaneous features [8]
Cutaneous features are characteristic of dermatomyositis but may be found in other subtypes.
-
Symmetric erythematous rash on the: ; [10]
- Extensor surfaces of the hand joints; , elbows, and knees (Gottron sign); scaly papules; may form (Gottron papules)
- Upper eyelids (heliotrope rash); often associated with periorbital edema
- Mid-face [11]
- Upper back, posterior neck, and shoulders; (shawl sign)
- Upper chest and anterior neck (V sign)
- Hips and lateral thighs (Holster sign)
- Poikiloderma may be seen in chronic disease. [12][13]
- Mechanic's hands: thickened and cracked skin on the sides of the fingers and palms (horizontal fissures may appear darkened or dirty, hence the name)
- Periungual telangiectasias
- Calcinosis cutis (in children)







Systemic manifestations
- Interstitial lung disease
- Cardiac involvement (primarily in dermatomyositis and polymyositis), including: [14]
- Myocarditis
- AV block
- Heart failure
- Constitutional symptoms
- Increased risk of malignancy (DM, PM, IMNM)
- Raynaud phenomenon
- Arthritis
- Gastrointestinal symptoms (e.g., abdominal pain, hematemesis, melena)
| Characteristic presentations of idiopathic inflammatory myopathies (IIM) [2][6][15][16] | |||
|---|---|---|---|
| Muscle weakness | Cutaneous features | Systemic features | |
| Dermatomyositis (DM) |
|
|
|
| Polymyositis (PM) |
|
||
| Antisynthetase syndrome |
|
|
|
| Immune-mediated necrotizing myopathy (IMNM) |
|
|
|
| Inclusion body myositis (IBM) |
|
|
|
| Juvenile IIM (JIIM) |
|
|
|
Think HAIR, CHAIRS, and STAIRS for the problems in activities of daily living caused by inflammatory myopathy: Muscle weakness causes difficulty raising the arms, getting up from a seated position, and climbing stairs.


Scaly, erythematous papules and periungual erythema are visible on the dorsal aspect of the interphalangeal and metacarpophalangeal joints.
Both localization and appearance are typical of Gottron papules, which are pathognomonic of dermatomyositis.
Source: “Gottron papules .dermatomyocitis” by Mohammad2018, Wikimedia commons, licensed under CC BY-SA 4.0.
{kind=link}

A confluent macular, erythematous rash is visible on both upper eyelids with concurrent periorbital edema.
This is a characteristic finding in dermatomyositis.
Source: “Figure 3, in: Lupus Erythematosus, Dermatomyositis and Systemic Sclerosis: Assessment and Differentials from A Dermatologic Point of View” by S. B. Fadhel, A. C. Diniz Silva, Enliven Archive, licensed under CC BY 3.0.

This photograph of the anterior chest and neck shows a large, irregular shaped area of erythema with petechiae on the right breast.
The shown features are termed “V sign” and is a characteristic cutaneous finding of dermatomyositis.
Source: “Figure 6, in: Paraneoplastic Dermatoses: A Brief General Review and an Extensive Analysis of Paraneoplastic Pemphigus and Paraneoplastic Dermatomyositis” by Didona D, Fania L, Didona B, Eming R, Hertl M, Di Zenzo G, International Journal of Molecular Sciences Online Journal; eScholarship, licensed under CC BY 4.0. Modifications: image has been cropped.

Photograph of the palmar aspect of the fingertips of a patient
A multinodular white lesion with superficial ulceration is visible at the fingertip of the index finger.
A yellowish-white plaque can be seen over the pulp of the middle finger.
These features are characteristic of calcinosis cutis, a subcutaneous calcium deposit seen in various connective tissue diseases (CREST, dermatomyositis, and SLE), hypercalcemic conditions (e.g., hyperparathyroidism, paraneoplastic syndromes), and secondary to trauma.
Source: Courtesy of Dr. Gary M. White, MD

Ellipsoid scaling papules are visible at the level of the proximal interphalangeal joints (white arrows).
These findings in a patient with dermatomyositis are consistent with Gottron papules.
Source: © IMPP

Erythematous papules are visible on the dorsal aspect of the interphalangeal and metacarpophalangeal joints. This is the typical localization of Gottron papules, which are pathognomonic of dermatomyositis.
Periungual erythema is also visible.
Source: © IMPP

A series of photographs of a 4-year-old with dermatomyositis
A: Edema with hyperpigmentation can be seen above the upper eyelids (heliotrope rash).
B: An ecthyma‐like ulcer can be seen on the left shoulder as well as nonscarring alopecia on the scalp.
C: A hyperpigmented rash can be seen on the neck.
D: Calcified papules and nodules appear around the knee, some of which are expelling calcified material (calcinosis cutis).
E: Small flat‐topped papules are located over the extensor aspects of the proximal and distal interphalangeal joints (possible early manifestation of Gottron papules).
These findings are typical of dermatomyositis.
Source: “Figure 1, in: Juvenile dermatomyositis in a 4‐year‐old Kenyan girl” by Marlous L. Grijsen, Deborah Mchaile, Inge Geut et al, Wiley Online Library, licensed under CC BY 4.0.
© AMBOSS
Diagnosis
General principles [2][18]
- There are different sets of diagnostic criteria for IIM; (e.g., the 2017 EULAR/ACR criteria) but none are universally accepted. [19]
-
Diagnosis is made based on the presence of characteristic clinical features and diagnostic studies. [6]
- Suspect IIM in patients with classic clinical features and elevated levels of muscle enzymes.
- Confirm the diagnosis with muscle biopsy.
- Patients with DM, PM, and IMNM: Arrange cancer screening at the time of diagnosis.
-
The Peter and Bohan criteria are still widely referenced but have significant limitations. The criteria are as follows: [20][21]
-
DM: characteristic skin findings and ≥ 3 additional features
- Symmetric proximal muscle weakness
- Elevated muscle enzymes
- Electromyogram (EMG) suggestive of inflammatory myopathy
- Evidence of myositis on muscle biopsy
- PM: all four of the above features in the absence of skin involvement
-
DM: characteristic skin findings and ≥ 3 additional features
Laboratory studies [3][22]
Routine
- CBC: may show leukocytosis [23]
- ESR and CRP: normal or mildly elevated
-
↑ Muscle enzymes [24]
-
↑ CK
- Typically elevated 2–100 times the normal value [9]
- May be normal in IBM and in 20–30% of DM cases
- Levels do not correlate with symptom severity.
- Liver chemistries: ↑ AST, ↑ ALT [6]
- ↑ LDH
- ↑ Aldolase
- ↑ Myoglobin
-
↑ CK
- Exclusion of differential diagnoses
- Serum electrolytes (BMP and magnesium): to rule out electrolyte disturbances causing muscle weakness
- TSH: to rule out myopathy secondary to hypothyroidism
Antibodies
The choice of antibody tests depends on the type of inflammatory myopathy under investigation and whether other connective tissue disorders are suspected. Consult rheumatology prior to ordering.
-
Antinuclear antibodies (ANAs)
- ANA: sensitive for autoimmune processes; but still negative in > ⅓ of IIM cases
- Depending on symptoms, consider specific ANAs to rule out myopathy due to other connective tissue disorders.
- Myositis-specific antibodies (MSAs): The choice of test depends on the suspected underlying condition. [2]
| Condition-specific antibody testing in IIM | |
|---|---|
| Dermatomyositis |
|
| Antisynthetase syndrome |
|
| Immune-mediated necrotizing myopathy (severe form) |
|
Other procedures [2][22]
-
Muscle biopsy: Gold standard for diagnosis of IIM ; [22]
- Perform on a muscle that is clinically affected but not wasted (MRI can be used to help select a site). [26]
-
Typical findings [6]
-
Muscle fiber damage
- Necrosis, degeneration, and regeneration
- IBM: rimmed vacuoles within muscle fibers
- Inflammatory cellular infiltrates (except in IMNM)
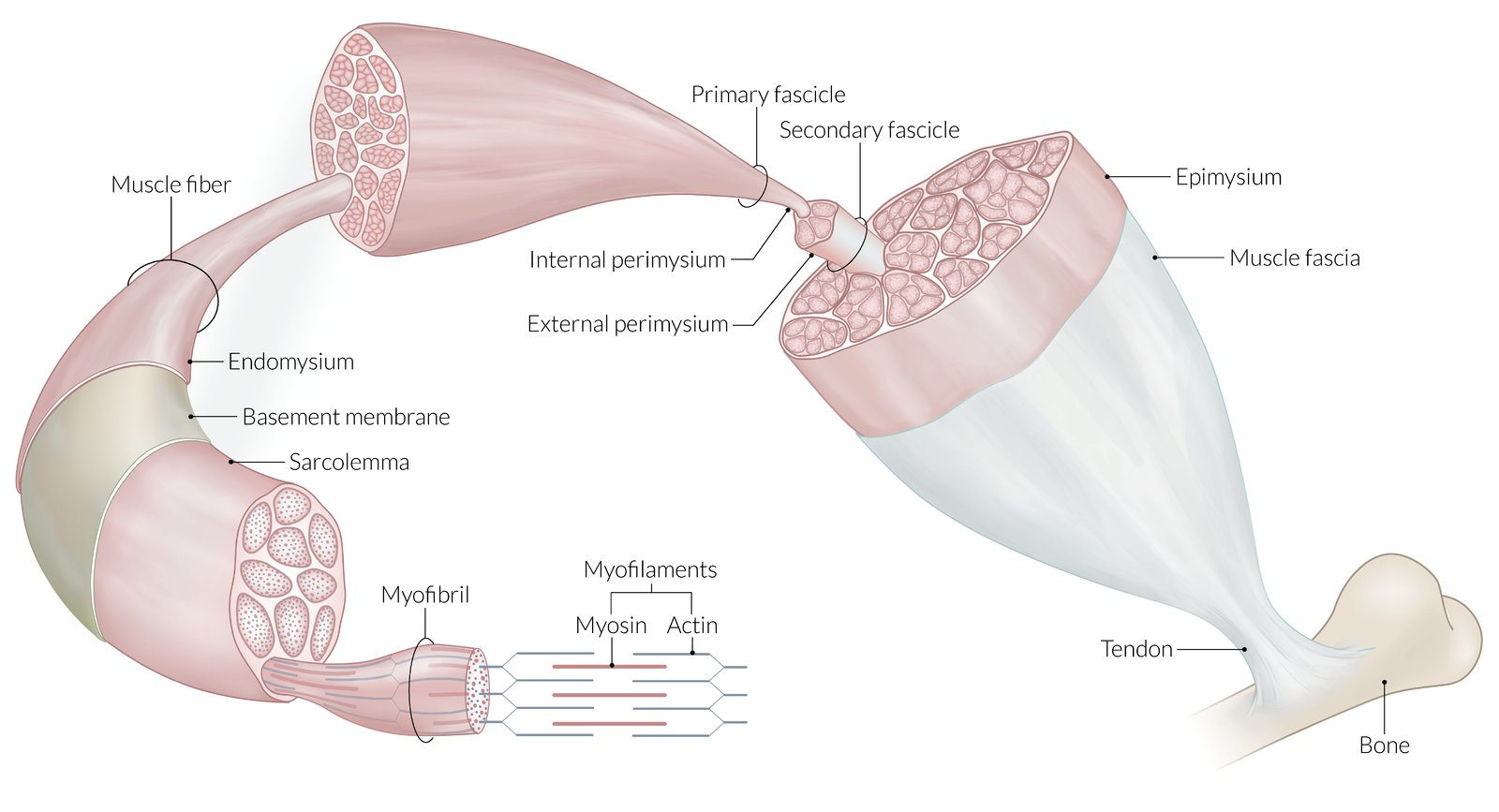
- DM: antibody-mediated inflammatory infiltrates that predominantly involve CD4+ T cells, plasmacytoid dendritic cells, and B lymphocytes in the perimysium (the connective tissue surrounding the fascicle); can lead to perifascicular atrophy
- IBM and PM: cell-mediated inflammatory infiltrates that predominantly involve cytotoxic CD8+ T cells in the endomysium (the connective tissue surrounding each muscle fiber)
- Immunohistochemistry in PM and IBM: overexpression of MHC-I on the sarcolemma
-
Muscle fiber damage
-
Electromyography: irritable myopathic pattern in all forms of IIM
- Characteristic of myopathy
- Can help distinguish between myopathic and neuropathic processes
- Include myopathic motor unit action potentials (polyphasic and of short duration and low amplitude), an increase in spontaneous activity (e.g., fibrillations, positive sharp waves), and early recruitment




Evaluation for extramuscular features [3][22]
- Evaluation for lung disease: baseline chest x-ray and pulmonary function tests
-
Malignancy workup in patients with DM, PM, and IMNM [22][27][28]
-
Standard age-appropriate cancer screenings, including: [3]
- Breast, pelvic, and prostate exams
- Mammography
- Colonoscopy
- Additional evaluation should be performed after consultation with rheumatology.
-
Standard age-appropriate cancer screenings, including: [3]
All patients diagnosed with DM, PM, and IMNM should be tested for malignancies.
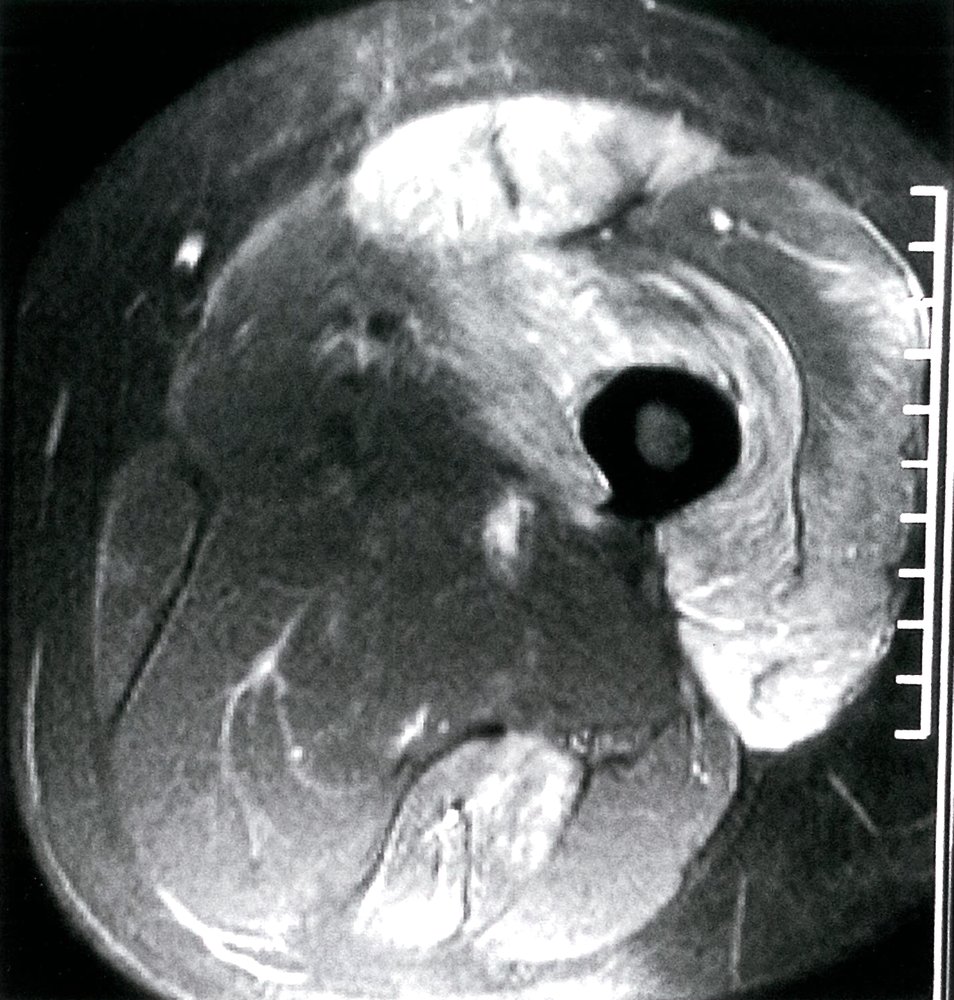
MRI thigh (T2-weighted with fat suppression, STIR sequence; axial plane)
A hyperintense signal, indicating inflammation (green overlay), is present in the quadriceps femoris group anteriorly and semitendinosus muscle posteriorly.
Source: © IMPP
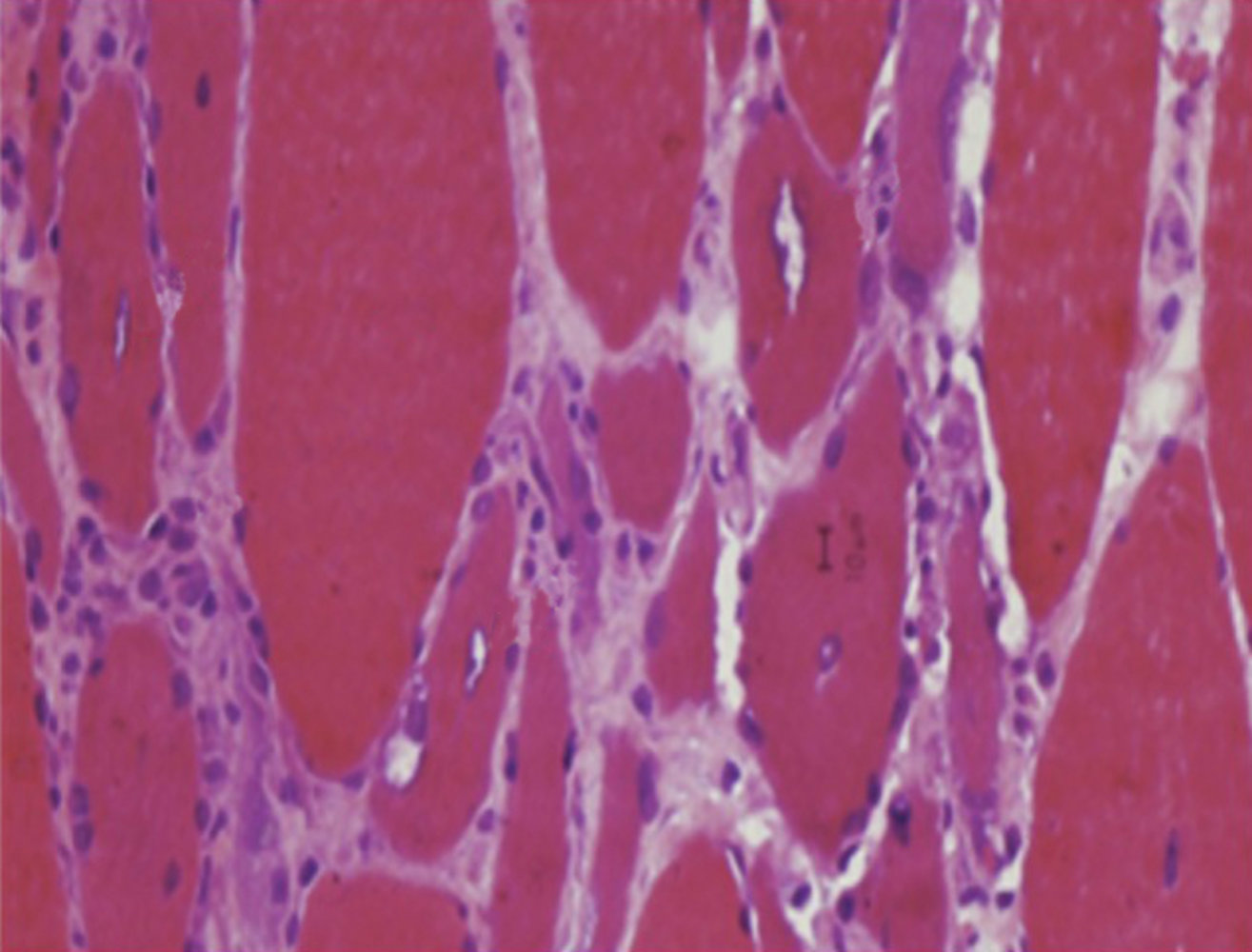
Photomicrograph of a biopsy sample of striated muscle tissue
Vacuoles (dotted white outlines) are present within the muscle fibers. The fibers vary in size, from smaller atrophic (green overlay) to larger hypertrophic (yellow overlay).
There is an abundance of inflammatory cells between the fibers.
These are typical histological findings in inclusion body myositis.
Source: “Figure 10, in: Idiopathic Inflammatory Myopathies: Clinical Approach and Management” by Asma Malik, Ghazala Hayat, Junaid S. Kalia, Miguel A. Guzman, Frontiers in Neurology, licensed under CC BY 4.0. Modifications: image cropped and labels removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
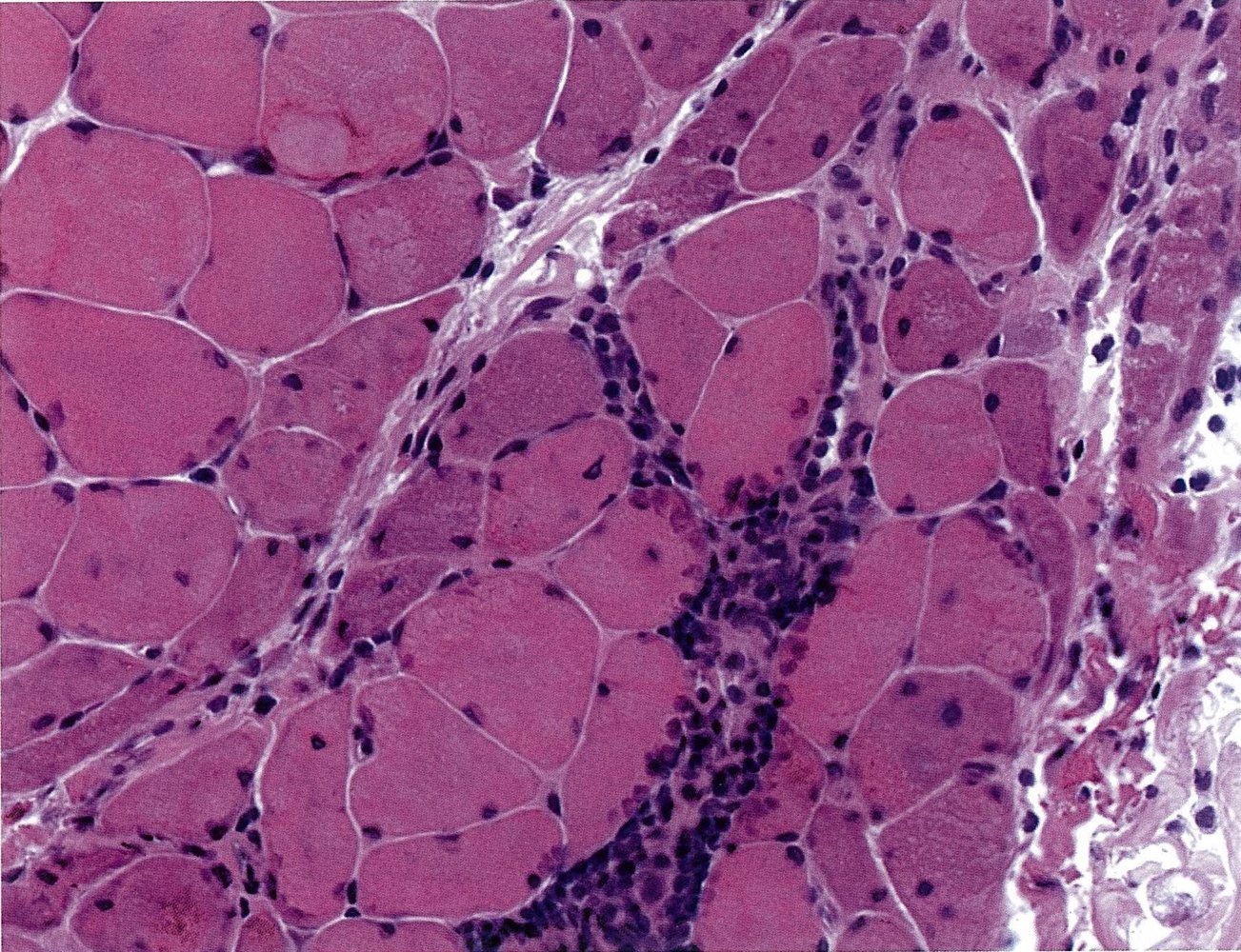
Histological section of muscle from the upper thigh (H&E stain)
In addition to the normal musculature, the following pathological findings are visible: pronounced interstitial (green overlay) and perivascular lymphocytic infiltration (V = vessel), muscle fiber necrosis and resorption (green arrow), and perifascicular atrophy (green hatched area), which is characteristic of dermatomyositis.
Source: © IMPP
© AMBOSS
Differential diagnoses
| Differential diagnosis of myopathy [29] | ||||||
|---|---|---|---|---|---|---|
| Features | ESR | CK | Muscle biopsy findings | |||
| Inflammatory myopathies | Dermatomyositis |
|
|
|
|
|
| Polymyositis |
|
|
|
|
||
| Inclusion body myositis |
|
|
|
|
||
| Polymyalgia rheumatica |
|
|
|
|
||
| Fibromyalgia |
|
|
|
|||
| Hypothyroid myopathy |
|
|
|
|
||
| Drug-induced myopathies | Corticosteroid-induced myopathy |
|
|
|
|
|
| Statin-induced myopathy [30] |
|
|
|
|
||
| Zidovudine-induced myopathy [31] |
|
|
|
|
||
| Alcohol-induced myopathy [32] |
|
|
|
|
||
|
|
|||||
| Cocaine-induced myopathy [33] |
|
|
|
|
||
-
Further differential diagnoses
- SLE
- Acute myopathy
- ALS
- Myasthenia gravis
- Muscular dystrophy
The differential diagnoses listed here are not exhaustive.
Treatment
Approach [2][3][22]
- Refer to a rheumatologist experienced in the management of IIM.
- All patients: Start supportive therapies (physical, occupational, and/or speech therapy, as appropriate) as soon as possible.
- Patients with any form of IIM except IBM: Start pharmacological therapy.
- Advise patients with cutaneous manifestations to use photoprotective measures.
- Educate patients on the possible increased risk of malignancy and the importance of attending screenings.
Pharmacologic therapy
Initial treatment [2][16]
-
First-line: glucocorticoids
- Prednisone [2][16]
- In severe disease or with multisystem involvement, consider an initial short course of pulsed IV methylprednisolone.
-
AND (usually) a steroid-sparing immunosuppressive agent, e.g.: ; [16]
- Methotrexate
- Azathioprine
Subsequent treatment [2][6]
Depending on the clinical presentation, additional medications may need to be added to the initial treatment regimen.
- Severe or refractory disease
- Intravenous immunoglobulins [34]
- AND/OR rituximab
- Dysphagia: intravenous immunoglobulins
- Rapidly progressive ILD: Consider plasmapheresis.
Complications
- Respiratory failure
- Myocarditis
- Esophageal disease
- Dystrophic calcinosis (common in juvenile dermatomyositis): Calcium deposits may be subcutaneous, intracutaneous, or intramuscular.
We list the most important complications. The selection is not exhaustive.
External Resources
References
- Huber AM. "Juvenile Idiopathic Inflammatory Myopathies". Pediatr Clin North Am. 65(4). :739-756. (2018)
- Selva-O’Callaghan A, Pinal-Fernandez I, Trallero-Araguás E, et al. "Classification and management of adult inflammatory myopathies". Lancet Neurol. 17(9). :816-828. (2018)
- Malik A, Hayat G, Kalia JS, Guzman MA. "Idiopathic Inflammatory Myopathies: Clinical Approach and Management". Front Neurol. 7. (2016)
- "Sporadic Inclusion Body Myositis". https://rarediseases.org/rare-diseases/sporadic-inclusion-body-myositis/. [2016-01-01]
- "Polymyositis and Dermatomyositis". http://www.msdmanuals.com/professional/musculoskeletal-and-connective-tissue-disorders/autoimmune-rheumatic-disorders/polymyositis-and-dermatomyositis. [2013-06-01]
- Dalakas MC. "Inflammatory Muscle Diseases". N Engl J Med. 372(18). :1734-1747. (2015)
- Dalakas MC, Hohlfeld R. "Polymyositis and dermatomyositis". Lancet. 362(9388). :971-982. (2003)
- Mainetti C, Terziroli Beretta-Piccoli B, Selmi C. "Cutaneous Manifestations of Dermatomyositis: a Comprehensive Review". Clin Rev Allergy Immunol. 53(3). :337-356. (2017)
- Christopher-Stine L, Plotz PH. "Adult inflammatory myopathies". Best Pract Res Clin Rheumatol. 18(3). :331-344. (2004)
- Mammen AL. "Dermatomyositis and polymyositis". Ann N Y Acad Sci. 1184(1). :134-153. (2010)
- Callen JP, Wortmann RL. "Dermatomyositis". Clin Dermatol. 24(5). :363-373. (2006)
- Koler RA, Montemarano A. "Dermatomyositis.". Am Fam Physician. 64(9). :1565-72. (2001)
- Dugan EM, Huber AM, Miller FW, Rider LG, International Myositis Assessment and Clinical Studies Group.. "Photoessay of the cutaneous manifestations of the idiopathic inflammatory myopathies.". Dermatol Online J. 15(2). :1. (2009)
- Lu Z, Guo-chun W, Li M, Ning Z. "Cardiac Involvement in Adult Polymyositis or Dermatomyositis: A Systematic Review". Clin Cardiol. 35(11). :685-691. (2012)
- Mammen AL. "Autoimmune Myopathies". Continuum (Minneap Minn). 22(6, Muscle and Neuromuscular Junction Disorders). :1852-1870. (2016)
- McGrath ER, Doughty CT, Amato AA. "Autoimmune Myopathies: Updates on Evaluation and Treatment". Neurotherapeutics. 15(4). :976-994. (2018)
- Mahler M, Miller FW, Fritzler MJ. "Idiopathic inflammatory myopathies and the anti-synthetase syndrome: A comprehensive review". Autoimmun Rev. 13(4-5). :367-371. (2014)
- Leclair V, Lundberg IE. "New Myositis Classification Criteria—What We Have Learned Since Bohan and Peter". Curr Rheumatol Rep. 20(4). :18. (2018)
- Lundberg IE, Tjärnlund A, Bottai M, et al. "2017 European League Against Rheumatism/American College of Rheumatology Classification Criteria for Adult and Juvenile Idiopathic Inflammatory Myopathies and Their Major Subgroups". Arthritis Rheumatol. 69(12). :2271-2282. (2017)
- Bohan A, Peter JB. "Polymyositis and Dermatomyositis – (First of Two Parts)". N Engl J Med. 292(7). :344-347. (1975)
- Bohan A, Peter JB. "Polymyositis and Dermatomyositis – (Second of Two Parts)". N Engl J Med. 292(8). :403-407. (1975)
- Ernste FC, Reed AM. "Idiopathic Inflammatory Myopathies: Current Trends in Pathogenesis, Clinical Features, and Up-to-Date Treatment Recommendations". Mayo Clin Proc. 88(1). :83-105. (2013)
- Peng J-M, Du B, Wang Q, et al. "Dermatomyositis and Polymyositis in the Intensive Care Unit: A Single-Center Retrospective Cohort Study of 102 Patients". PLoS ONE. 11(4). :e0154441. (2016)
- Amato AA, Barohn RJ. "Evaluation and treatment of inflammatory myopathies". J Neurol Neurosurg Psychiatry. 80(10). :1060-1068. (2009)
- Hengstman GJD, ter Laak HJ, Vree Egberts WTM, et al. "Anti-signal recognition particle autoantibodies: marker of a necrotising myopathy". Ann Rheum Dis. 65(12). :1635-1638. (2006)
- Jameson JL, Fauci AS, Kasper DL, et al. "Harrison's Principles of Internal Medicine, Twentieth Edition (Vol.1 & Vol.2)". McGraw-Hill Education / Medical. (2018). ISBN: 9781259644030
- Yang Z, Lin F, Qin B, Liang Y, Zhong R. "Polymyositis/dermatomyositis and Malignancy Risk: A Metaanalysis Study". J Rheumatol. 42(2). :282-291. (2014)
- Qiang JK, Kim WB, Baibergenova A, Alhusayen R. "Risk of Malignancy in Dermatomyositis and Polymyositis". J Cutan Med Surg. 21(2). :131-136. (2016)
- "Inflammatory Myopathies". http://neuropathology-web.org/chapter13/chapter13eInflammatory.html. [2013-10-01]
- Hansen KE, Hildebrand JP, Ferguson EE, Stein JH. "Outcomes in 45 patients with statin-associated myopathy". Arch Intern Med. 165(22). :2671-2676. (2005)
- Cupler EJ, Jay C, Dalakas MC, et al. "Early features of zidovudine-associated myopathy: histopathological findings and clinical correlations". Acta Neuropathol. 90(1). :1-6. (1995)
- Simon L, Jolley SE, Molina PE. "Alcoholic Myopathy: Pathophysiologic Mechanisms and Clinical Implications". Alcohol res. 38(2). :207-217. (2017)
- Selvaraj V, Gollamudi LR, Sharma A, Madabushi J. "A Case of Cocaine-Induced Myopathy". The Primary Care Companion For CNS Disorders. (2013)
- Lünemann JD, Quast I, Dalakas MC. "Efficacy of Intravenous Immunoglobulin in Neurological Diseases.". Neurotherapeutics. 13(1). :34-46. (2016)