Summary
Infant nutrition includes the use of breast milk, infant formula, infant vitamin supplementation, and complementary feeding. Breast milk (i.e., from breastfeeding, self-expression, or donors) is the preferred source of infant nutrition for the first 6 months of life. Contraindications to breastfeeding are rare and include infant metabolic conditions (e.g., galactosemia) and, in lactating individuals, certain untreated infections and the use of toxic substances (e.g., recreational drug use, chemotherapy agents, radioactive agents). Iron-fortified infant formula is an appropriate alternative or supplement to breast milk if indications for formula are present. Exclusively or partially breastfed infants require vitamin D and iron supplementation. Complementary feeding is introduced at 6 months of age, while continuing to provide breast milk or infant formula until 12 months of age. Due to the many benefits of breastfeeding, prolonged breastfeeding is encouraged for ≥ 2 years if desired. To prevent early cessation of breastfeeding, provide regular assessment of breastfeeding and promptly manage any breastfeeding issues or complications. A risk-benefit analysis is recommended before prescribing medications to lactating individuals; most medications are not contraindicated during breastfeeding.
For children ≥ 1 year of age, see “Pediatric well-child anticipatory guidance” for nutritional guidance.
Infant nutrition
General principles [1][2][3][4]
- Counseling on infant nutrition should begin during prenatal care and continue during well-child visits. [5]
- While breast milk is preferred, formula is an acceptable alternative.
- Provide education and support for the caregiver's preferred feeding choice. [3]
Age < 6 months [1][2][3][4]
- Encourage exclusive breast milk for the first 6 months of life. [2][3][4][6]
- Iron-fortified infant formula may be used as an alternative or supplement.
Age 6–11 months [1][2][3][4]
- Continue breast milk (preferred) and/or iron-fortified infant formula until 12 months of age.
- Introduce complementary foods.
- Water is optional; limit most infants to ≤ 4 oz per day [7]
- Introduce a sippy cup.
At 12 months [1][2][3][4]
- Recommended beverages: breast milk, whole milk, and/or water
- Encourage continued breast milk ≥ 2 years of age, if desired. [3][8]
- Infant formulas or toddler formulas are not recommended. [9]
- See “Pediatric well-child anticipatory guidance” for further recommendations.
Discourage parents from offering foods and beverages that are not recommended for infants.
Infant feeding schedule [5][10][11]
- Infant feeding should be on demand and guided by infant hunger cues rather than at set times.
- Stop feeding when the infant shows signs of satiety.
- Infants who consume breast milk typically drink smaller amounts and more frequently than formula-fed infants. [11]
| Typical feeding frequency and amounts for infants [7][11][12] | |
|---|---|
| Age | Feeding amount and frequency |
| First month [1] |
|
| 1–5 months |
|
| 6–11 months[13] |
|
| 12 months |
|
Do not wake infants for feeds once they are ≥ 1 month of age with good weight gain. [12]
Assessment of milk intake [1][14]
The following clinical signs apply to both formula-fed and breastfed infants.
Adequate milk intake in newborns
- 8–12 feeds per day
- Signs of infant satiety after feeds
- 6–8 wet diapers per day after the first 2 days
- Stools transition from black to green by day 3 and to a bright, seedy yellow by day 5
- Normal weight patterns [1]
- An initial weight loss < 8% of birth weight
- After days 3–4, gains 15–30 g/day
Inadequate milk intake in newborns
- No audible swallowing during feeds
- Infant hunger cues persist after feeds
- Lethargy
- Insufficient wet diapers for age (uric acid crystals may be in diaper) [15][16]
- Persistent black-green stools after days 3–5.
- Excessive weight loss in breastfed infants
Infant vitamin supplementation
-
Vitamin D [3][17]
- Exclusively or partially breastfed infants; : oral vitamin D from birth until meeting the recommended daily intake of vitamin D through diet [17][3]
- See “Prevention of vitamin D deficiency” for additional information.
-
Iron [18][19]
- Exclusively or partially breastfed infants: oral iron from 4 months of age until consuming the recommended daily intake of iron through diet [5][10][19]
- Premature infants: oral iron from birth until consuming the recommended daily intake of iron through diet [19]
- See “Prevention of iron deficiency in children” for additional information.
- Fluoride for infants ≥ 6 months of age if water supply is not fluoridated [10][20]
Exclusively or partially breastfed infants require vitamin D and iron supplementation until they can meet their daily requirements through their diet. [10]
In exclusively formula-fed infants, vitamin D and iron supplementation are generally not required unless there are underlying medical conditions (e.g., malabsorption, prematurity). [17][18][19]
Breast milk
Breast milk composition
Breast milk contains all the required nutrients (except vitamin D and vitamin K) for infants up to 6 months of age.
- Colostrum: the first milk produced during late pregnancy until 3–4 days postpartum; rich in proteins and immunoglobulins
- Mature milk is composed of:
- Proteins, lactose and oligosaccharides, fats, minerals, trace elements, and vitamins
-
Proteins and cells that provide passive immunity in neonates
- Immunoglobulins (secretory IgA), lactoferrin, lysozymes
- Lymphocytes, macrophages
- Bifidobacteria that contribute to the neonate's gastrointestinal flora
Refer breastfeeding parents who follow a vegan or vegetarian diet to a dietitian to evaluate for additional nutritional needs (e.g., vitamin B12 supplementation). [10][21]
Storage and preparation of breast milk [10][22]
- Freshly expressed breast milk: Discard after ≥ 4 hours at room temperature or ≥ 4 days of refrigeration. [22]
-
Frozen breast milk [22]
- Discard after ≥ 2 hours at room temperature, ≥ 24 hours of refrigeration, or > 12 months in the freezer.
- Use breast milk that has been frozen the longest first.
- Thaw breast milk in the refrigerator overnight or with lukewarm water.
- Never refreeze breast milk.
- Freshly expressed or frozen breast milk: Discard any remaining breast milk offered as a feed within 2 hours after the infant stops feeding.
Donor breast milk, which may be used for very low birth weight infants, should be pasteurized and come from a qualified milk bank. [3]
Avoid storing breast milk in the door of the refrigerator or freezer due to temperature fluctuations. [22]
Infant formula
Indications for infant formula [3][14]
- Parental desire
- Contraindications to breastfeeding
-
Need for supplementation, e.g., [16]
- Inadequate breast milk production
- Signs of inadequate breast milk intake
- Excessive weight loss in breastfed infants
- Complications in the infant
Infant formula options [7][10][23]
- Iron-fortified infant formulas are an acceptable alternative to breast milk until 12 months of age.
- Cow's milk infant formula is the standard initial formula for healthy, term infants.
- Medical indications for specialized formulas include
- Allergies (e.g., cow milk protein allergy): hypoallergenic formulas
- Prematurity: premature formulas
- Galactosemia, lactose intolerance: soy-based formulas
- During formula shortages, see “Tips and Links” for recommendations from trusted societies.
Generic and brand commercial infant formulas are nutritionally equivalent.
Avoid homemade infant formulas due to the risk of nutritional deficiencies. [10]
Storage and preparation of infant formula [10][24][25]
- Use clean bottles and nipples; sterilization is not necessary for healthy, term infants. [26]
- Ensure water is safe to use for consumption.
- Follow package instructions for recommended measurements and preparation.
- Offer prepared formula immediately or keep refrigerated until the infant is ready to feed.
- If warming is desired, use lukewarm water and check the temperature before feeding.
- Discard prepared formula after
- ≥ 1 hour after being offered as a feed
- ≥ 2 hours at room temperature
- ≥ 24 hours of refrigeration
Compared to breastfed infants, the stools of formula-fed infants are usually firmer, browner, and have a stronger odor due to differences in digestion and the composition of formula. The stool frequency of formula-fed infants varies greatly from several stools per day to one stool every 3 to 4 days.
Complementary feeding
Introducing complementary feeding [3][5][10]
- In addition to breast milk or formula, start offering foods at 6 months if the infant shows signs of complementary feeding readiness. [10][27]
- Recommend the following:
- Foods rich in protein, iron, and zinc; iron-fortified infant cereal and pureed meats are good first sources of iron
- A variety of foods that includes fruits, vegetables, and potentially allergenic foods (see “Food allergy prevention”) [27][28]
- Avoidance of foods and beverages that are not recommended for infants
-
Start with 0.5–1 oz (1–2 tbsp) of a single food once a day. [10]
- Consider waiting 3–5 days before introducing another food to monitor for allergic reactions. [5][10]
- Gradually increase the amount, variety, and texture of foods as tolerated.
- Avoid overfeeding.
- Stop feeding when the infant shows signs of satiety.
- As solid food intake increases, breast milk and/or formula intake will decrease.
- See “Infant feeding schedule” for recommendations by age.
Delaying the introduction of allergenic foods (e.g., peanut products, eggs, wheat) is no longer recommended and may increase the risk of food allergies. [27][28]
Signs of complementary feeding readiness [10]
- Interest when food is presented, e.g., smiling, mouth opening, reaching for food.
- Developmental readiness
- Good head and neck control
- Sitting upright with minimal support
- Exploring objects with the mouth
- Reaching for desired objects
- Resolution of the tongue thrust reflex
Infants with developmental delay may not be ready for solid foods at 6 months of age. [10]
Foods and beverages to avoid in infants [10][29]
-
Foods
- Honey
- Unpasteurized dairy products, e.g., yogurt, cheese, milk
- Uncooked meat
- Sweetened products, e.g., syrups, chocolate
- Salt, e.g., canned foods, processed meats
- Fish high in mercury
-
Beverages
- Water: no water if < 6 months of age and generally limit to 4 oz/day between 6–11 months
- Teas
- Cow's milk (excluding infant formula) or alternative milk, e.g., goat's milk [7]
- Drinks that are carbonated or sweetened (including artificial sweeteners)
Do not give honey to infants < 12 months of age due to the risk of infant botulism. [10][25]
Storage and preparation of complementary food [10][30]
Home-prepared food and commercially prepared infant food are acceptable. For commercially prepared food, follow the instructions on the container. For home-prepared food: [30]
- Cook foods according to FDA food safety standards. [31]
- Do not add sugar, salt, or excess fat.
- Ensure food is served safely to prevent choking hazards.
- Mash or puree foods to the right consistency.
- Remove bones from fish and meat before cooking.
- Cut finger foods, especially round firm foods (e.g., grapes), into small cubes or thin slices. [30]
- Remove seeds and pits.
- Discard food after:
- Offering it as a feed (due to the risk of contamination)
- 2 days of refrigeration
- 3 months in the freezer
Breastfeeding
General principles [1][14]
- Recommend exclusive breastfeeding for all infants 6 months of age.
- Encourage continued breastfeeding ≥ 2 years of age, if desired.
- Consider waiting to introduce nipples (e.g., pacifiers, bottles) until breastfeeding is well-established. [32]
- Breastfeeding infants require infant vitamin supplementation.
Physiology of lactation
- Lactogenesis: the process of mammary epithelial cell differentiation and milk production in the mammary gland that begins mid pregnancy as a result of increased estrogen and progesterone levels
- Lactation is initiated by the delivery of the placenta → abrupt ↓ progesterone levels → ↑ prolactin → stimulation of milk secretion
- Maintaining lactation requires suckling, which stimulates the secretion of:
- Prolactin; from the anterior pituitary: leads to stimulation of continued lactogenesis (milk production); and disruption of pulsatile GnRH secretion (causing lactational amenorrhea)
- Oxytocin; from the posterior pituitary: leads to stimulation of milk ejection (letdown); and uterine contractions

Benefits of breastfeeding [1][3][33]
In addition to promoting infant-parent bonding, breastfeeding offers a range of benefits for both individuals.
-
Benefits for the infant include reductions in
- Infant mortality (e.g., sudden infant death syndrome)
- Allergic conditions: asthma, atopic dermatitis
- Infections: AOM, respiratory, gastrointestinal (e.g., pediatric gastroenteritis, necrotizing enterocolitis)
- Inflammatory bowel disease
- Metabolic conditions: obesity, type 2 diabetes
-
Benefits for the lactating individual
- Faster postpartum uterine involution and weight loss [34]
- Spaced births for family planning (see “Lactational amenorrhea”)
- Reduced costs [10][35]
- Decreased risk of cancers (e.g., ovarian, endometrial, breast), hypertension, diabetes mellitus
Breast milk has antimicrobial, antiinflammatory, and immunoregulatory properties, which help the infant's immune system develop. [3][25]
Breast milk contains maternal immunoglobulins (especially IgA), which provide passive immunity to the infant. [10]
Contraindications to breastfeeding
| Contraindications to breastfeeding [3][25][33][36] | ||
|---|---|---|
| Absolute contraindications | Possible indications for breastfeeding modification | |
| Infant metabolic conditions |
|
|
| Infections in the lactating individual |
|
|
| Drug or medication use in the lactating individual |
|
|
Discourage the use of alcohol, marijuana, and tobacco while breastfeeding. [3]
Lactating individuals with opioid use disorder on stable treatment doses (i.e., methadone or buprenorphine) should be encouraged to breastfeed. [36]
LactMed (see “Tips and Links”) and FDA labels are good resources for evaluating medication safety while breastfeeding.
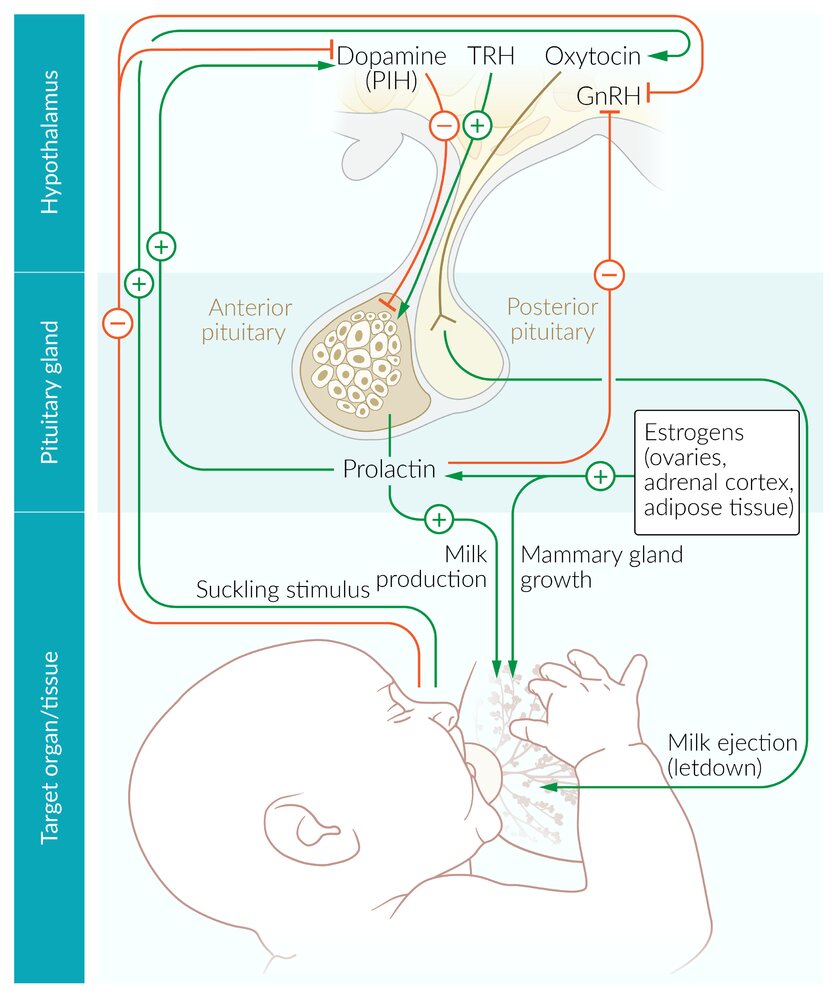
The suckling stimulus at the nipple triggers the secretion of oxytocin by the hypothalamus and inhibits the secretion of hypothalamic dopamine (prolactin-inhibiting hormone) and GnRH.
Normally, dopamine inhibits the secretion of prolactin (prolactin triggers milk production). The inhibition of dopamine by the suckling stimulus, therefore, promotes milk production. At the same time, the suckling stimulus promotes the production of oxytocin in the hypothalamus and its secretion in the posterior pituitary, leading to milk ejection.
The suckling stimulus also inhibits the secretion of GnRH by the hypothalamus, which, in turn, inhibits the secretion of LH and FSH in the anterior pituitary (→ lactational amenorrhea).
© AMBOSS
Assessment of breastfeeding
Approach [1][14]
- Provide anticipatory lactation counseling at hospital discharge.
- After delivery and at each postpartum and infant well-child visit, assess for:
- Signs of a good latch
- Signs of adequate milk intake in newborns
- Breastfeeding issues and complications
- Offer lactation services to any lactating parent, especially if issues are identified. [33][43]
Regular assessment and support for breastfeeding parents may prevent complications and early weaning. [14]
Consider using a validated scoring system, e.g., LATCH score, to assess breastfeeding. [1]
Signs of a good latch [14]
- Pain-free latch for the lactating individual
- Deep latch with most of the areola and nipple in the infant's mouth
- The infant's mouth is open and the lips everted, with the chin and nose resting on the breast.
- Rhythmic sucking and audible swallowing in the infant
- Signs of infant satiety after feeds
Breastfeeding complications
- Breastfeeding issues and complications are common reasons for early cessation of breastfeeding.
- Anticipatory lactation counseling, assessment of breastfeeding, and referral to a lactation consultant can prevent or quickly address identified issues.
| Common breastfeeding issues and complications [1][3][14] | ||
|---|---|---|
| Clinical findings | Initial management | |
| Breast engorgement [43][44] |
|
|
| Nipple injury |
|
|
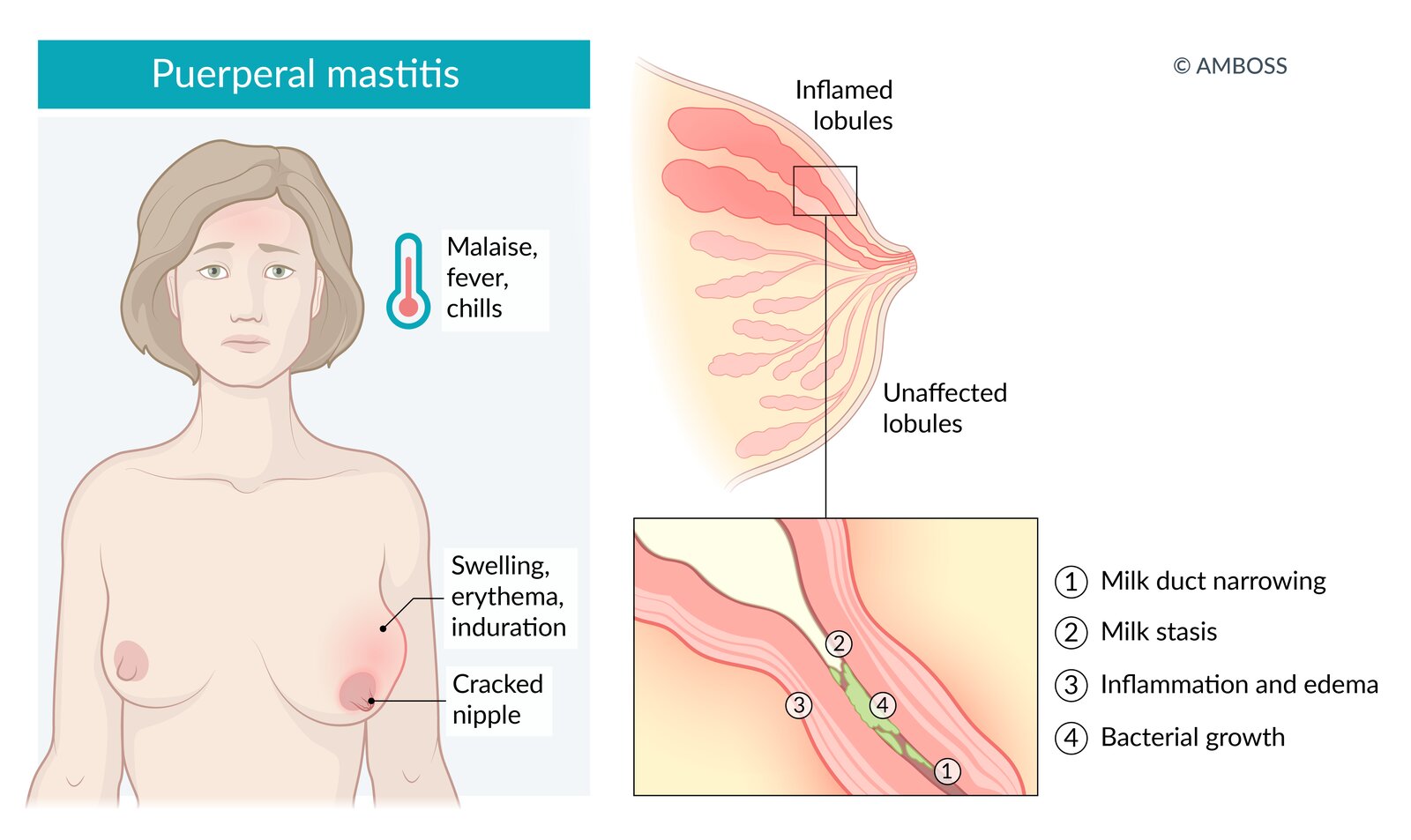
| Puerperal mastitis |
|
|
| Mammary candidiasis [46] |
|
|
| Galactocele |
|
|
| Inadequate breast milk production |
|
|
| Excessive weight loss in breastfed infants |
|
|
| Neonatal jaundice |
|
|
Encourage continued breastfeeding or breast milk expression while addressing breastfeeding issues or complications. [14]
Negative breastfeeding experiences increase the risk for postpartum depression and anxiety; screen and treat individuals accordingly. [14][47]



Nipple of a breastfeeding parent who reported pain during feeds
The surface of the nipple is injured and shows a small area of keratinized necrotic tissue.
These findings are characteristic of nipple injury.
Source: “Fig 1, In: A retrospective analysis of debridement in the treatment of chronic injury of lactating nipples” by Gao H, Wang J, Ding S et al., nature, licensed under CC BY 4.0. Modifications: image cropped.
© AMBOSS
External Resources
- 2022 AAP Policy Statement: Breastfeeding and the Use of Human Milk
- 2021 ACOG Committee Opinion Breastfeeding Challenges
- 2018 AFP Breastfeeding: Common Questions and Answers
- 2017 ABM Clinical Protocol #3:Supplementary Feedings in the Healthy Term Breastfed Neonate,Revised
- CDC Infant and Toddler Nutrition
- AAP Infant Food and Feeding website
- Drugs and Lactation Database (LactMed®)
- International Lactation Consultant Association IBCLC® Directory
- United States Lactation Consultant Association Find an IBCLC® Directory
- La Leche League USA
- CDC Information for Families During the Infant Formula Shortage, 2022
- AAP Baby Formula Shortages: What Parents Need to Know
- NASPGHAN Tools for Infants and Children Affected by Formula Shortages
- NASPGHAN Comparable Formulas That Are Safe to Interchange
References
- ACOG. "Breastfeeding Challenges". Obstet Gynecol. 137(2). :e42-e53. (2021)
- Westerfield KL, Koenig K, Oh R. "Breastfeeding: Common Questions and Answers". Am Fam Physician. 98(6). :368-373. (2018)
- Rouse C, Hanley L. "Barriers to Breastfeeding: Supporting Initiation and Continuation of Breastfeeding: ACOG Committee Opinion Summary, Number 821". Obstet Gynecol. 137(2). :396-397. (2021)
- Berens P, Brodribb W. "ABM Clinical Protocol #20: Engorgement, Revised 2016". Breastfeeding Medicine. 11(4). :159-163. (2016)
- Meek JY, Noble L. "Policy Statement: Breastfeeding and the Use of Human Milk". Pediatrics. 150(1). (2022)
- Zakarija-Grkovic I, Stewart F. "Treatments for breast engorgement during lactation". Cochrane Database Syst Rev. 9(9). :CD006946. (2020)
- Keister D, Roberts KT, Werner SL. "Strategies for breastfeeding success". Am Fam Physician. 78(2). :225-32. (2008)
- American College of Obstetricians and Gynecologists. "Pharmacologic Stepwise Multimodal Approach for Postpartum Pain Management". Obstetrics & Gynecology. 138(3). :507-517. (2021)
- Berens P, Eglash A, Malloy M, Steube AM. "ABM Clinical Protocol #26: Persistent Pain with Breastfeeding". Breastfeed Med. 11(2). :46-53. (2016)
- Pediatrics AAO. "Caring for Your Baby and Young Child, 7th Edition". Bantam. (2019). ISBN: 9781984817709
- Kellams A, Harrel C, Omage S, Gregory C, Rosen-Carole C. "ABM Clinical Protocol #3: Supplementary Feedings in the Healthy Term Breastfed Neonate, Revised 2017". Breastfeeding Medicine. 12(4). :188-198. (2017)
- Crowe S, Hanley L. "ACOG Committee Opinion No. 756: Optimizing Support for Breastfeeding as Part of Obstetric Practice". Obstet Gynecol. 132(4). :e187-e196. (2018)
- Schmitt B. "Bottle-Feeding (Formula) Questions". Pediatric Patient Education. (2022)
- "WIC Infant Nutrition and Feeding Guide". https://web.archive.org/web/20240208205330/https://wicworks.fns.usda.gov/resources/infant-nutrition-and-feeding-guide. [2019-04-01]
- Martinez JA, Ballew MP. "Infant Formulas". Pediatr Rev. 32(5). :179-189. (2011)
- "CDC: Infant Formula Preparation and Storage". https://web.archive.org/web/20240117101721/https://www.cdc.gov/nutrition/infantandtoddlernutrition/formula-feeding/infant-formula-preparation-and-storage.html
- AAP Committee on Infectious Diseases. "Red Book: 2021–2024 Report of the Committee on Infectious Diseases". American Academy of Pediatrics. (2021). ISBN: 9781610025218
- "CDC: How to Clean, Sanitize, and Store Infant Feeding Items". https://web.archive.org/web/20240201171555/https://www.cdc.gov/hygiene/childcare/clean-sanitize.html. [2021-02-23]
- Hagan JF, Shaw JS, Duncan PM. "Bright Futures: Guidelines for Health Supervision of Infants, Children and Adolescents, 4th Edition". American Association of Pediatrics. (2017). ISBN: 9781610020220
- Togias A, Cooper SF, Acebal ML, et al. "Addendum guidelines for the prevention of peanut allergy in the United States: Report of the National Institute of Allergy and Infectious Diseases–sponsored expert panel". J Allergy Clin Immunol. 139(1). :29-44. (2017)
- Soriano VX, Ciciulla D, Gell G, et al. "Complementary and Allergenic Food Introduction in Infants: An Umbrella Review". Pediatrics. 151(2). (2023)
- "Nutrition: Foods and Drinks to Avoid or Limit. Centers for Disease Control and Prevention (CDC)". https://web.archive.org/save/https://www.cdc.gov/nutrition/infantandtoddlernutrition/foods-and-drinks/foods-and-drinks-to-limit.html. [2023-06-08]
- "Once Baby Arrives - Food Safety for Moms to Be". https://web.archive.org/web/20240619233339/https://www.fda.gov/food/people-risk-foodborne-illness/once-baby-arrives-food-safety-moms-be. [2022-05-16]
- "Safe Food Handling". https://web.archive.org/web/20240619232018/https://www.fda.gov/food/buy-store-serve-safe-food/safe-food-handling. [2024-03-05]
- "Vitamin B12 Fact Sheet for Health Professionals". https://ods.od.nih.gov/factsheets/VitaminB12-HealthProfessional/. [2020-03-30]
- "Proper Storage and Preparation of Breast Milk". https://web.archive.org/web/20240228084154/https://www.cdc.gov/breastfeeding/recommendations/handling_breastmilk.htm. [2022-01-24]
- Sexton S, Natale R. "Risks and benefits of pacifiers". Am Fam Physician. 79(8). :681-5. (2009)
- Gunderson EP. "Impact of breastfeeding on maternal metabolism: implications for women with gestational diabetes". Curr Diab Rep. 14(2). :460. (2014)
- "Contraindications to Breastfeeding or Feeding Expressed Breast Milk to Infants". https://web.archive.org/web/20230920124855/https://www.cdc.gov/breastfeeding/breastfeeding-special-circumstances/contraindications-to-breastfeeding.html. [2023-05-23]
- Abuogi L, Noble L, Smith C, et al. "Infant Feeding for Persons Living With and at Risk for HIV in the United States: Clinical Report". Pediatrics. (2024)
- "Clinical Considerations for Mpox in People Who are Pregnant or Breastfeeding". https://web.archive.org/web/20240612172245/https://www.cdc.gov/poxvirus/mpox/clinicians/pregnancy.html. [2023-03-27]
- Committee on Infectious Disease, American Academy of Pediatrics. "Red Book: 2024-2027 Report of the Committee on Infectious Diseases, 33rd Edition". American Academy of Pediatrics. (2024). ISBN: 9781610027373
- "HCV Guidance: Recommendations for Testing, Managing, and Treating Hepatitis C". https://aasldhcvguidelines.kinsta.cloud/wp-content/uploads/legacy/full-guidance-pdf/AASLD-IDSA_HCVGuidance_December_19_2023.pdf. [2023-12-19]
- Datta P, Baker T, Hale TW. "Balancing the Use of Medications While Maintaining Breastfeeding". Clin Perinatol. 46(2). :367-382. (2019)
- Sachs HC, Frattarelli DAC, Galinkin JL, et al. "The Transfer of Drugs and Therapeutics Into Human Breast Milk: An Update on Selected Topics". Pediatrics. 132(3). :e796-e809. (2013)
- US Preventive Services Task Force, Bibbins-Domingo K, Grossman DC, et al. "Primary Care Interventions to Support Breastfeeding: US Preventive Services Task Force Recommendation Statement". JAMA. 316(16). :1688-1693. (2016)
- "Breastfeeding, Family Physicians Supporting (Position Paper)". https://web.archive.org/web/20240929024003/https://www.aafp.org/about/policies/all/breastfeeding-position-paper.html. [2022-01-01]
- "Breastfeeding (Policy Statement)". https://web.archive.org/web/20240616031602/https://www.aafp.org/about/policies/all/breastfeeding-policy-statement.html. [2023-10-01]
- "Practice Advisory to Update the Duration of Breastfeeding". https://www.acog.org/clinical/clinical-guidance/practice-advisory/articles/2023/02/duration-of-breastfeeding-update. [2023-02-01]
- Fuchs GJ, Abrams SA, Amevor AA, et al. "Older Infant-Young Child “Formulas”". Pediatrics. 152(5). (2023)
- Schmitt B. "Breastfeeding - Milk and Feeding Questions". Pediatric Patient Education. (2022)
- Schmitt B. "Solid Foods (Baby Foods)". Pediatric Patient Education. (2022)
- Joseph C, Gattineni J. "Proteinuria and hematuria in the neonate". Curr Opin Pediatr. 28(2). :202-208. (2016)
- Wagner CL, Greer FR. "Prevention of Rickets and Vitamin D Deficiency in Infants, Children, and Adolescents". Pediatrics. 122(5). :1142-1152. (2008)
- Riley LK, Rupert J, Boucher O. "Nutrition in Toddlers". Am Fam Physician. 98(4). :227-233. (2018)
- Baker RD, Greer FR. "Diagnosis and Prevention of Iron Deficiency and Iron-Deficiency Anemia in Infants and Young Children (0–3 Years of Age)". Pediatrics. 126(5). :1040-1050. (2010)
- Clark MB, et al. "Fluoride Use in Caries Prevention in the Primary Care Setting". Pediatrics. 146(6). (2020)