Quick guide
Diagnostic approach
- ABCDE survey
- Targeted clinical evaluation
- Assess for clinical features of dehydration and hypovolemia.
- Consider diagnostics for infectious gastroenteritis.
Gastroenteritis is a clinical diagnosis. Diagnostic studies are usually reserved for patients with severe gastroenteritis or other red flag features.
Red flag features
- Bloody stools
- Severe abdominal cramping and/or tenderness
- Fever and/or sepsis
- Severe dehydration
- End-organ dysfunction
- Immunocompromise
- Duration > 1 week
Management checklist
- Oral rehydration therapy or IV fluid therapy
- Electrolyte repletion as needed
- Oral or parenteral antiemetics (e.g., promethazine )
- Consider empiric antibiotics for bacterial gastroenteritis.
- Counsel on prevention of infectious gastroenteritis.
Avoid antimotility drugs (e.g., loperamide) in patients with fever or inflammatory diarrhea.
Summary
Infectious gastroenteritis is an inflammation of the gastrointestinal tract that is most commonly caused by viruses (e.g., norovirus, rotavirus, enteric adenovirus). However, it can also be caused by bacteria (e.g., Campylobacter, Salmonella, Shigella, Yersinia, Vibrio cholerae, diarrheagenic Escherichia coli, Clostridioides difficile), fungi, or parasites, such as protozoans (e.g., giardiasis, or cryptosporidiosis) or helminths (e.g., nematodes, or cestodes). Transmission is commonly fecal-oral, foodborne, or waterborne and therefore education on food and water hygiene is crucial for preventing disease. Clinical features can be mild, manifesting as abdominal pain and diarrhea, nausea, and/or vomiting, or severe, e.g., sepsis, intense abdominal pain, and/or significant dehydration from severe diarrhea and/or vomiting. For mild disease courses, diagnostic studies are not usually required, and since the disease is usually self-limiting, patients often only require supportive therapy (e.g., oral rehydration and antiemetics). Stool cultures followed by empiric antibiotic therapy may be considered in patients with severe gastroenteritis and/or risk factors for complicated disease (e.g., those who are immunocompromised).
Infectious gastroenteritis in children and Clostridioides difficile infection are covered separately in their respective articles.
Overview
Definitions
- Gastroenteritis: inflammation of the gastrointestinal tract that usually manifests with acute diarrhea, vomiting, and/or abdominal pain
- Infectious gastroenteritis: gastroenteritis caused by pathogens; most commonly viruses, but can also be caused by bacteria, parasites, and fungi
Clinical features of infectious gastroenteritis [1][2][3][4]
-
Mild-to-moderate gastroenteritis
- Abdominal pain with normal abdominal examination
- Mild diarrhea, nausea, and/or vomiting
-
Severe gastroenteritis includes: [2]
-
Gastrointestinal features
- Bloody stools
- Severe diarrhea, nausea, and/or vomiting
- Severe abdominal cramping and/or tenderness
- Systemic features
- Fever (≥ 38.3°C) or sepsis
- Clinical signs of significant dehydration
- End-organ damage
- Duration > 1 week
-
Gastrointestinal features
Diagnostics for infectious gastroenteritis [1][5][6]
Approach
-
Clinical diagnosis
- Perform a thorough history and physical examination.
- Evaluate for risk factors for specific pathogens.
- Evaluate for clinical features of dehydration and hypovolemia.
-
Diagnostic studies are only recommended for the following: [1][2][3]
- Patients with severe gastroenteritis or risk factors for severe illness
- And/or if the results may alter management
Suspect Shiga toxin-producing E. coli (STEC) gastroenteritis in patients with abdominal pain or tenderness and bloody diarrhea in the absence of fever. [2]
Viral gastroenteritis may be asymptomatic or manifest with nonbloody watery diarrhea and vomiting, which is sometimes accompanied by abdominal pain or cramps, and fever. [3]
Laboratory studies [1][4]
- BMP and serum electrolytes: may show AKI or electrolyte abnormalities (see “Laboratory findings in dehydration and hypovolemia”)
-
CBC
- Leukocytosis with left shift: may indicate an inflammatory bacterial infection
- Eosinophilia: may indicate a parasitic infection caused by invasive helminths
- Stool analysis: (for inflammatory markers): may show leukocytes, occult blood, and/or lactoferrin [1][4]
Testing for leukocytes and/or lactoferrin in the stool in patients with suspected infectious gastroenteritis is controversial and 2017 IDSA guidelines recommend against these studies in patients with acute infectious diarrhea. [1]
Diagnostic confirmation
-
Indications include:
- Severe gastroenteritis or persistent diarrhea
- Patients with risk factors for severe illness
- Consider for patients with leukocytes and/or lactoferrin in the stool.
-
Recommended studies [3]
- Obtain a stool culture to look for Shigella, Salmonella, Campylobacter, Yersinia, and STEC.
- Alternatively, obtain non-culture-based studies.
-
Further studies (in select cases)
- Clostridioides difficile toxin: Obtain for patients with risk factors for C. difficile infection (CDI), e.g., recent history of antibiotic use.
- Blood cultures
- Stool microscopy (e.g., to identify ova and parasites)
- Endoscopy (colonoscopy or sigmoidoscopy) : may show signs of inflammation (e.g., in infectious colitis)
Microbiological studies should be reserved for patients with fever, mucoid or bloody stools, signs of sepsis, immunosuppression, or severe abdominal cramping, and cases in which the identification of a causative pathogen would modify management.

Differential diagnosis
See “Overview of bacterial gastroenteritis,”; “Overview of viral gastroenteritis,” “Diagnostic workup of diarrhea,” and “Food poisoning.”
Treatment of infectious gastroenteritis [1]
Supportive therapy for gastroenteritis
Infectious gastroenteritis is usually self-limiting. Supportive therapy may suffice for most patients.
-
Diet and fluids
- Bland diet: e.g., broths, saltine crackers, boiled vegetables
- Oral rehydration therapy or intravenous fluid therapy: i.e., fluid replacement or fluid resuscitation
- Oral or parenteral electrolyte repletion
-
Pharmacotherapy (not routinely recommended)
- Oral or parenteral antiemetics as needed: e.g., ondansetron (off label) or promethazine )
- Consider antimotility drugs (e.g., loperamide ) for immunocompetent adult patients with acute watery diarrhea.
Antimotility drugs (e.g., loperamide) should be avoided in patients with fever or inflammatory diarrhea because of the risk of developing toxic megacolon.
Antibiotic therapy [1]
Antibiotic therapy is not routinely indicated in bacterial gastroenteritis. When indications for empiric antibiotics exist, they should be started after appropriate cultures have been collected.
-
Empiric antibiotics for bacterial gastroenteritis
-
Indications include:
- Suspected Shigella infection
- Suspected enteric fever
- High-grade fever or sepsis
- High-risk groups
- Recommended regimens (adult patients) [2]
- Azithromycin (off label) [2]
- Ciprofloxacin [2]
- Trimethoprim/sulfamethoxazole is not recommended because of high resistance rates.
-
Indications include:
-
Targeted therapy: Once a pathogen has been identified, modify therapy accordingly.
- E.g., treatment for C. difficile infection
- Consider discontinuing or adjusting therapy for other pathogens (see relevant sections below for details).
Antibiotic therapy is contraindicated for enterohemorrhagic E. coli. It may increase the risk of or worsen HUS.
Complications
- Dehydration (most common; especially severe in shigellosis and cholera)
- Malnutrition
- Permanent carrier status (chronic Salmonella carrier)
- Reactive arthritis
- Postinfectious irritable bowel syndrome
Prevention of infectious gastroenteritis [1][7][8]
General measures
- Food and water hygiene
- Educate patients and caregivers on preventing onward community transmission of infectious gastroenteritis. [1][9][10]
- Regular hand hygiene with soap and water including after changing diapers.
- Clean bathrooms, high-touch, and contaminated areas with bleach-based cleaners.
- Use gloves to handle soiled items and wash them at the highest heat.
- Avoid sharing towels and linens.
- Avoid food preparation for others until symptoms have resolved. [11]
- Isolate at home until symptoms are resolved.
- For prevention of nosocomial transmission, see “Infection prevention and control.”
- Prophylaxis against select infections (e.g., cystoisosporiasis) is recommended for patients with advanced HIV; see “Primary prevention of opportunistic infections in HIV.”
Reporting suspected outbreaks [12][13]
- Nationally notifiable diseases in the US include: [12][13]
- Salmonellosis
- Shigellosis
- STEC colitis
- Vibrio (cholera and noncholera species) infections
- Other suspected outbreaks should be reported to local health departments. [9]
Vaccination [1][5]
- Infants: rotavirus vaccination
- Specific vaccines (e.g., typhoid vaccine, cholera vaccine) may be recommended for international travelers depending on the destination.
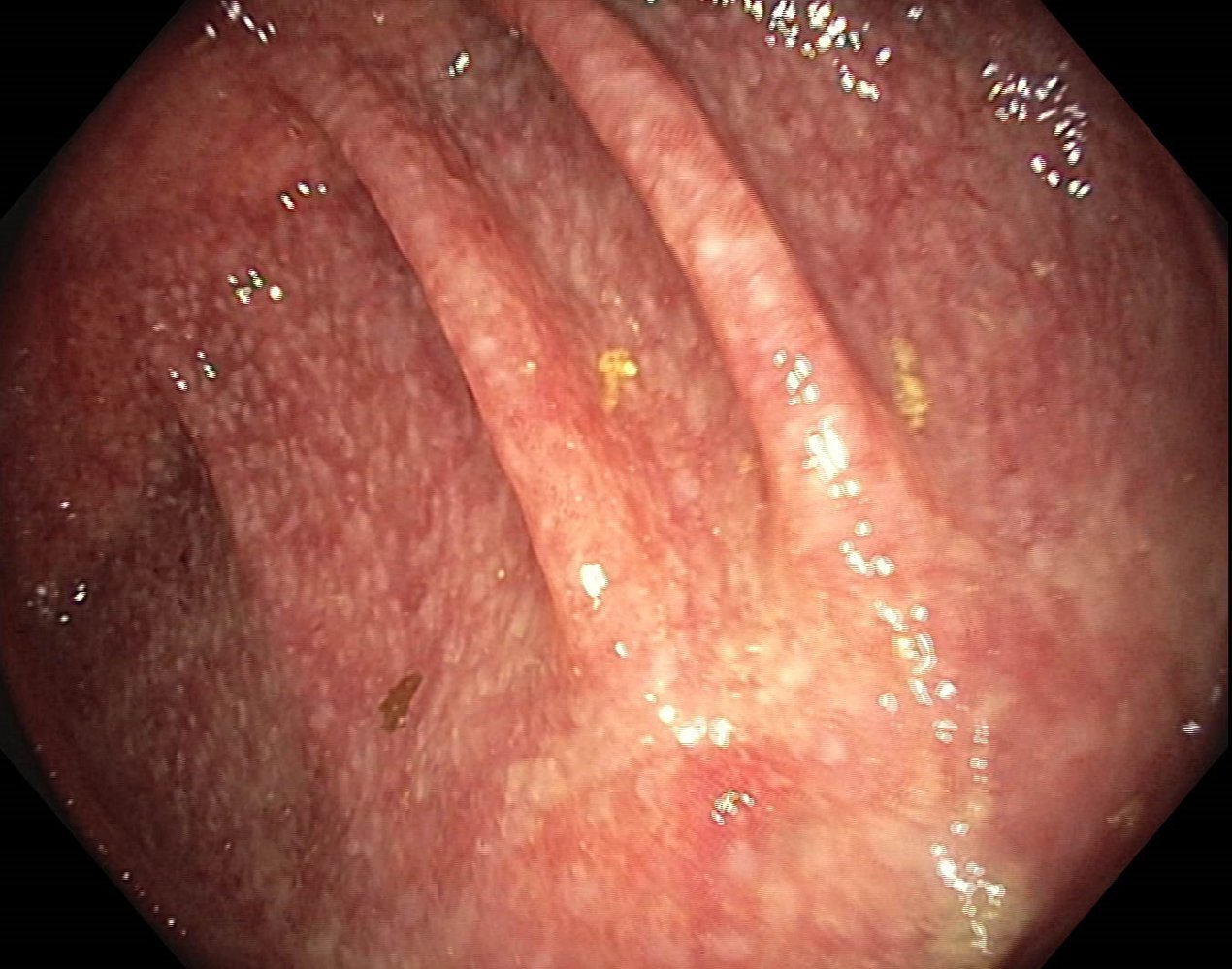
Endoscopic view of the colon
Erythematous mucosa with multiple small fibrinous spots can be seen. The semilunar folds and haustra are normal and the vascular pattern remains recognizable. The brown and yellow deposits are residual bowel contents.
These findings are consistent with infectious colitis.
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.
Viral gastroenteritis
- Infection with enteric viruses is the leading cause of gastroenteritis worldwide and may contribute to local outbreaks.
- Patients often present with acute onset of vomiting and diarrhea but the illness is generally self-limiting.
- Routine testing is often not required but may be helpful in severe cases.
| Overview of viral gastroenteritis | |||
|---|---|---|---|
| Pathogen | Incubation period [14] | Transmission | Key features |
| Norovirus [15][16] |
|
|
|
| Rotavirus [10][17] |
|
|
|
| Enteric adenovirus [18][19] |
|
|
|
| Astrovirus [20] |
|
|
|
| Cytomegalovirus (CMV) [21] |
|
|
|
Bacterial gastroenteritis
| Overview of bacterial gastroenteritis [6] | |||
|---|---|---|---|
| Pathogen | Pathophysiology | Associations | Stool findings |
| Secretory diarrhea | |||
| Bacillus cereus |
|
|
|
| Enterotoxigenic E. coli (ETEC) |
|
||
| Clostridium perfringens |
|
||
| Staphylococcus aureus |
|
||
| Vibrio cholerae |
|
||
| Invasive diarrhea | |||
| Yersinia |
|
|
|
| Salmonella enterica serotype Typhi or Salmonella enterica serotype Paratyphi |
|
||
| Inflammatory diarrhea | |||
| Campylobacter |
|
|
|
| Enterohemorrhagic E. coli (EHEC) |
|
||
| Clostridioides difficile |
|
||
| Shigella |
|
||
| Noncholera Vibrio species |
|
||
| Salmonella (nontyphoidal) |
|
||
Campylobacter enteritis (campylobacteriosis)
Overview
-
Pathogen
- Campylobacter jejuni, Campylobacter coli
- Curved, gram-negative, oxidase-positive rods with polar flagella
- Optimal growth temperature: 37–42°C [23]
- Most common pathogen responsible for foodborne gastroenteritis in the US [24]
- Highly contagious: low infective dose required (> 500 organisms)
-
Transmission
- Fecal-oral
- Foodborne (undercooked meat; and unpasteurized milk; ), contaminated water
- Direct contact with infected animals (i.e., cats, dogs, pigs) or animal products
- Incubation period: 2–4 days
“There's no camping without a campfire:” Campylobacter jejuni grows best at hot temperatures.

Clinical features
- Duration: up to a week
- High fever, aches, dizziness
- Inflammatory (bloody) diarrhea, especially in children
- Severe abdominal pain may present as pseudoappendicitis or colitis.
Treatment
- Supportive therapy for gastroenteritis: e.g., bland diet, oral rehydration therapy
- Antibiotic therapy: : macrolides, e.g., erythromycin (off label) or azithromycin (off label) in severe cases [4][25][26]
Complications
Complications are more common and severe in patients with HIV (see “HIV-associated conditions” for details).
- Guillain-Barré syndrome
- Reactive arthritis
- Acute abdomen: cholecystitis, pancreatitis
- Bacteremia
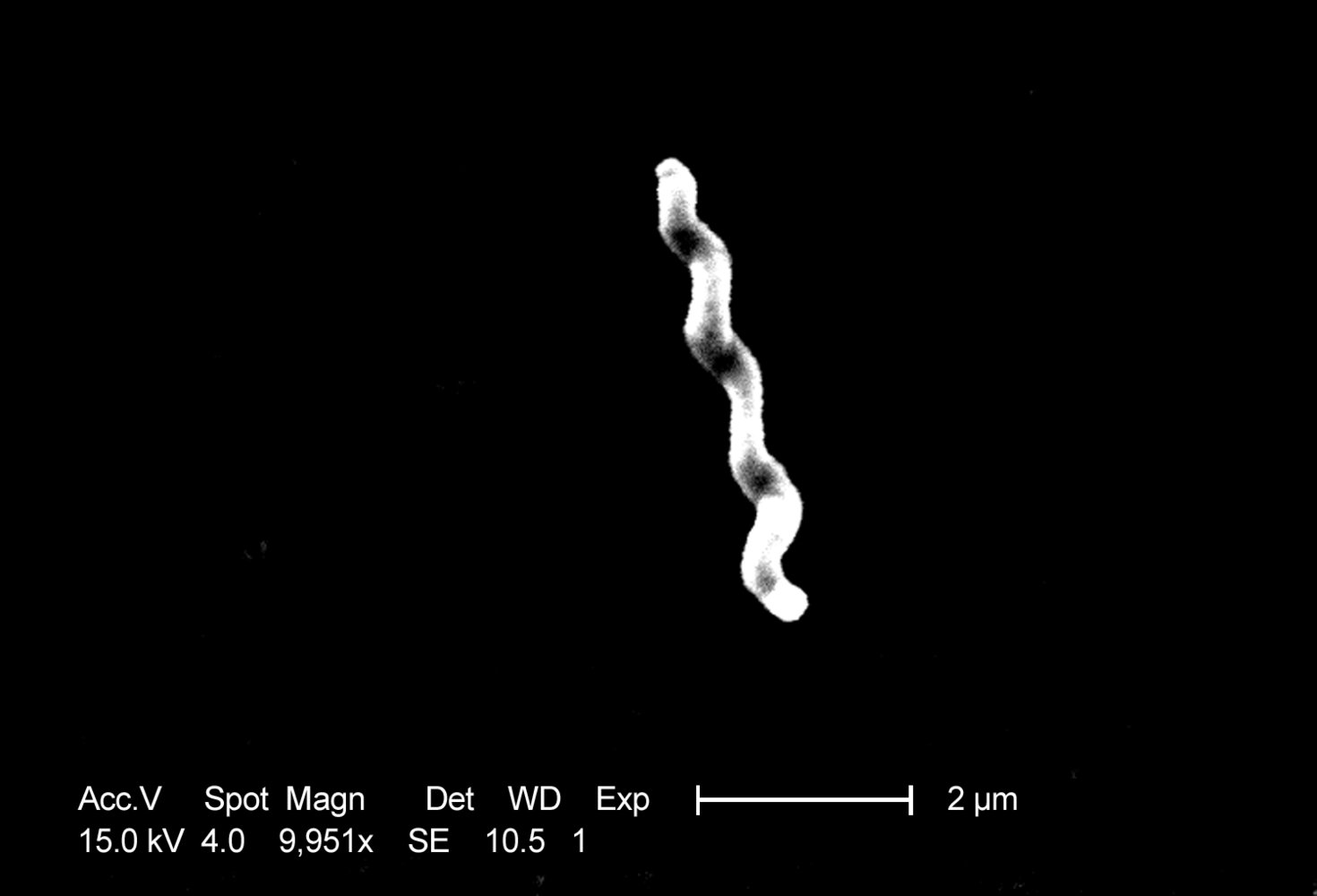
Scanning electron micrograph
C. jejuni is a spirillum bacteria. Contamination with even very small quantities of C. jejuni causes inflammatory gastroenteritis.
Source: "ID#: 5781", CDC/ Dr. Patricia Fields, Dr. Collette Fitzgerald, Janice Carr, Centers for Disease Control and Prevention (CDC) licensed under Public Domain
Salmonellosis (salmonella gastroenteritis)
This section covers nontyphoidal Salmonella. For S. enterica serotype Typhi and S. enterica serotype Paratyphi enteric fever, see “Typhoid fever.”
Overview
-
Pathogens: Salmonella enterica serotype Enteritidis, Salmonella enterica serotype Typhimurium, Salmonella enterica serotype Heidelberg
- Gram-negative bacteria, obligate pathogens
- Produce hydrogen sulfide
- Do not ferment lactose
- 2nd most common group of pathogens responsible for bacterial foodborne gastroenteritis
- High infectious dose required (104–106 pathogens), depending on the strength of an individual's immune system
- Transmission: foodborne (poultry, raw eggs, and milk), reptiles (e.g., pet turtles or snakes) [27]
- Incubation period: : 0–3 days
- Prevention: no vaccine available
Clinical features
- Duration: 3–7 days
- Fever (usually resolves within 2 days), chills, headaches, myalgia
- Severe vomiting, abdominal pain, and inflammatory (watery-bloody) diarrhea
Treatment [1][4][28]
- Supportive therapy for gastroenteritis: e.g., bland diet, oral rehydration therapy
-
Antibiotic therapy
- Not routinely indicated (usually not indicated in immunocompetent individuals)
- Indications: severe cases of nontyphoidal Salmonella (consider also for high-risk patients ) [1]
- Preferred regimens (usually given for 7–10 days ) [4]
- Fluoroquinolones: e.g., ciprofloxacin (off label)
- OR cephalosporins. e.g., ceftriaxone (off label)
- Alternatives
- Trimethoprim/sulfamethoxazole (off label) [28]
- OR azithromycin (off label) [28]
Antibiotic treatment for salmonellosis prolongs fecal excretion of the pathogen. Therefore, it is only indicated for severe nontyphoidal Salmonella infections (e.g., in patients with systemic manifestations or ≥ 9 episodes of diarrhea per day, and those who require hospitalization).
Complications
Complications are more frequent in immunocompromised patients, e.g., those with HIV; treatment for complicated salmonellosis (e.g., antibiotic therapy) in patients with HIV should be given in consultation with a specialist.
- Bacteremia
- Chronic Salmonella carriage
- Systemic disease: e.g., osteomyelitis, meningitis, myocarditis, aortitis
- Reactive arthritis
Shigellosis (bacillary dysentery)
Overview [29]
-
Pathogens: Shigella dysenteriae, Shigella flexneri, Shigella sonnei
- Gram-negative rods
- Produce Shiga toxin (enterotoxin) and endotoxin
- Invade M cells via pinocytosis and travel from cell to cell via actin filaments (no hematogenous spread)
-
Transmission
- Fecal-oral (especially a concern in areas with poor sanitation)
- Oral-anal sexual contact
- Foodborne (unpasteurized milk products and raw unwashed vegetables)
- Contaminated water
- Incubation period: 0–2 days
- Infectivity: highly contagious; very low infective dose required (≥ 10 bacteria)
- Prevention: no vaccine available
Clinical features
- Duration: 2–7 days
- High fever
- Tenesmus, abdominal cramps
- Profuse inflammatory, mucoid-bloody diarrhea
Treatment [1][4][28]
- Supportive therapy for gastroenteritis: e.g., bland diet, oral rehydration therapy
-
Antibiotic therapy
- Preferred regimens [1][28]
- Ciprofloxacin [28]
- OR azithromycin (off label) [28]
- OR ceftriaxone (off label) [28]
- Alternative: trimethoprim/sulfamethoxazole [28]
- Preferred regimens [1][28]
Complications
- HUS
- Febrile seizures
- Reactive arthritis
- Intestinal complications (e.g., toxic megacolon, colonic perforation, intestinal obstruction, proctitis, rectal prolapse)
Cholera
Overview
-
Pathogen: Vibrio cholerae
- Most common in developing countries
- Gram-negative, oxidase positive, curved bacterium with a single polar flagellum → production of cholera toxin
- Cholera toxin stimulates adenylate cyclase via activation of Gs → increased cyclic AMP → increased ion (mainly chloride) and water secretion into the intestinal lumen → profuse liquid stools
-
Transmission
- Fecal-oral
- Undercooked seafood or contaminated water (e.g., unseparated drinking water and sewage systems)
- Incubation period: 0–2 days
-
Infectivity
- Acid-labile (grows well in an alkaline medium)
- High infective dose required (over 108 pathogens)
- Gastric acid provides a natural barrier against V. cholerae infection; therefore, the infective dose in individuals with reduced gastric acidity is lower.


Clinical features
- Low-grade fever, vomiting
- Profuse “rice-water” stools
Diagnosis
- Dipstick (rapid test; initial test)
- Stool culture (confirmatory)
Treatment [1][28][30]
- Supportive therapy for gastroenteritis: Urgent initial fluids for dehydration and hypovolemia (e.g., oral rehydration solution, IV fluids) [31]
-
Antibiotic therapy: Treatment should be based on culture susceptibility testing. [1][28]
- Indications: severe cases
- Preferred regimen: doxycycline [30]
- Alternative regimens [1][28]
- Azithromycin (off label) [28]
- OR tetracycline [28]
- OR trimethoprim/sulfamethoxazole (off label) [28]
- OR ciprofloxacin (off label) [30]
Complications
- Severe dehydration
- Pneumonia may occur in children.
- Cholera sicca (rare): intestinal paralysis and accumulation of liquid in the intestinal lumen → circulatory collapse and high mortality rate
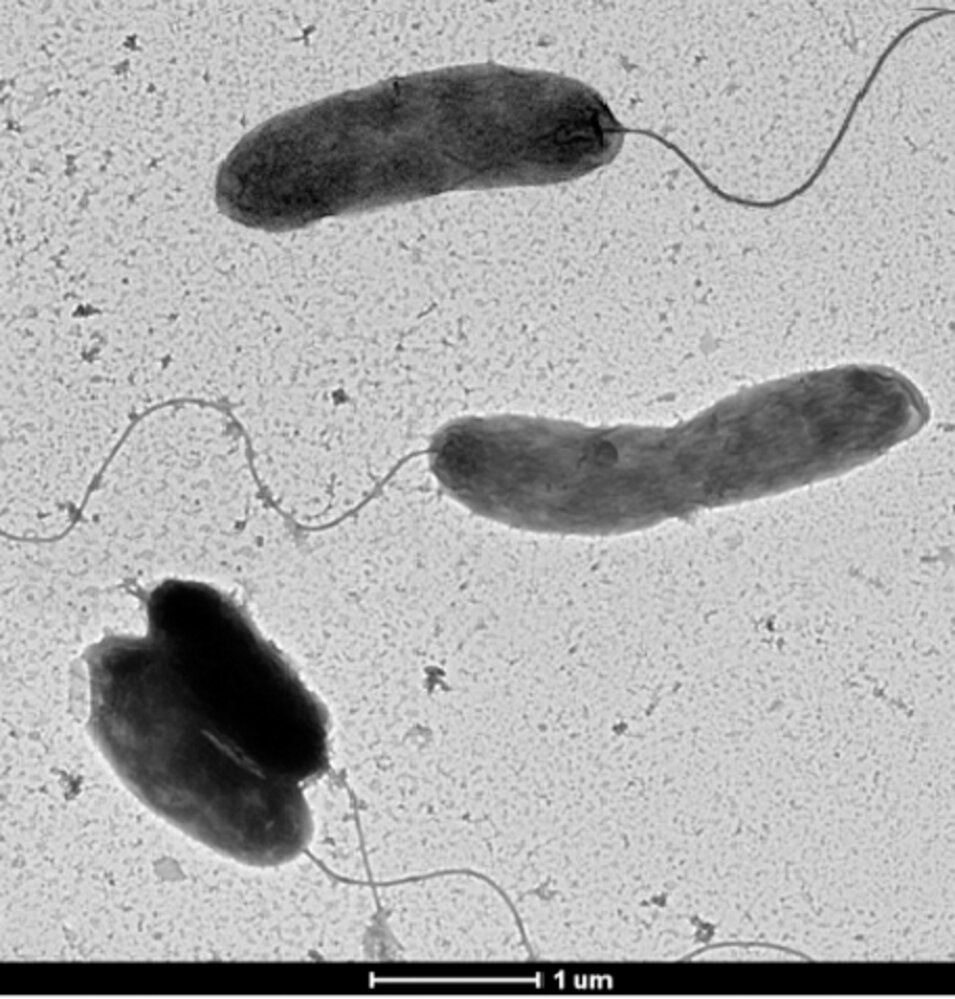
Electron micrograph
Comma-shaped bacteria with flagellae used for motility are visible.
Source: “Figure 6, in: Isolation and Characterization of the New Mosaic Filamentous Phage VFJ Φ of Vibrio cholerae” by Wang Q, Kan B, Wang R, Plos one, licensed under CC BY 4.0. Modifications: Image cropped.
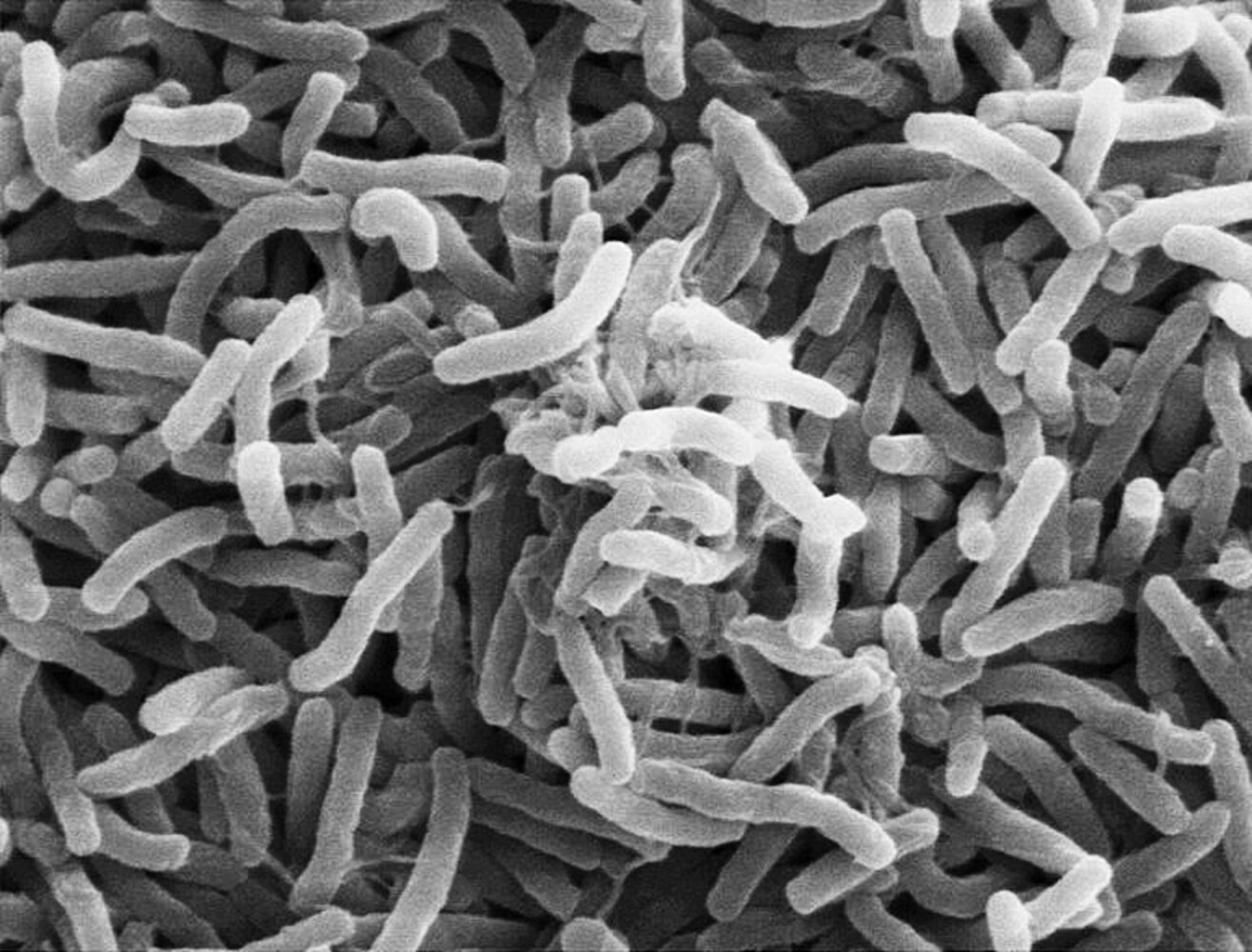
Scanning electron micrograph
Numerous curved (comma-shaped) vibrio cholerae bacteria can be seen.
Source: “Scanning electron micrograph of Vibrio cholerae, in: Adjusting Cholera Models to Recent Experimental Data” by Synopsis, PloS Medicine, licensed under CC BY 4.0.
Yersiniosis
Overview
-
Pathogens: Yersinia enterocolitica, Yersinia pseudotuberculosis [32]
- Gram-negative, rod-shaped, pleomorphic bacteria; obligate pathogens
- High infective dose required (109 pathogens)
-
Transmission
- Foodborne (e.g., raw/undercooked pork, unpasteurized milk products)
- Contaminated water
- Direct/indirect contact with infected animal (e.g., dogs, pigs, rodents) and/or their feces [32]
- Incubation period: 4–6 days [32]
Clinical features
- Duration: 12–22 days
- Low-grade fever, vomiting
- Invasive diarrhea (may be bloody in severe cases) [6]
- Pseudoappendicitis: mesenteric lymphadenitis, particularly in the ileum, with typical signs of appendicitis
Diagnosis
- Direct pathogen detection in culture or cold enrichment
Treatment [1][32]
- Supportive therapy for gastroenteritis: e.g., bland diet, oral rehydration therapy
-
Antibiotic therapy: Treatment should be based on culture susceptibility testing.
- Indications: severe cases
- Recommended regimens
- Trimethoprim/sulfamethoxazole (off label) [28]
- OR fluoroquinolones: e.g., ciprofloxacin (off label) [28]
- OR third-generation cephalosporins: e.g., cefotaxime (off label)
Complications
Particularly common in patients with HLA-B27
- Reactive arthritis
- Erythema nodosum
- Acute abdomen: appendicitis, bowel perforation, toxic megacolon, cholangitis
- Bacteremia
Clostridium perfringens enterocolitis
Overview
-
Pathogen: Clostridium perfringens
- Gram-positive, anaerobic
- Spore-forming rod-shaped bacterium → produce exotoxins [33]
- Transmission: foodborne (undercooked or poorly refrigerated meat, legumes)
- Incubation period: 6–24 hours
Clinical features
- Duration: < 24 hours
- Severe abdominal cramping
- Watery diarrhea
Diagnosis
- Toxin detection in stool cultures
Treatment
- Supportive therapy for gastroenteritis: e.g., bland diet, oral rehydration therapy
Complications
- Clostridial necrotizing enteritis
- Requires antibiotic therapy: penicillin, metronidazole
- Surgery may be required for complicated and/or refractory disease (e.g., perforation)
Noncholera Vibrio infection
Overview
-
Pathogen
- Vibrio parahaemolyticus; : non-lactose fermenter, gram-negative bacilli
- Vibrio vulnificus: lactose fermenter, gram-negative bacilli
-
Transmission
- Foodborne (raw or undercooked shellfish)
- Wounds infected by contaminated sea water
- Incubation period: : 12–52 hours
Clinical features
- Inflammatory diarrhea
- Low-grade fever, vomiting, abdominal pain
- Cellulitis, bullous skin lesions
Treatment [4][35][36]
- Supportive therapy for gastroenteritis: e.g., bland diet, oral rehydration therapy
- Surgical debridement: may be needed in patients with severe wound infections
-
Antibiotic therapy
- Indications
- Severe gastroenteritis due to V. parahaemolyticus
- Gastroenteritis due to V. vulnificus
- Wound infections due to Vibrio species
- Suggested regimen: give for 7–14 days
- Doxycycline (off label)
- OR fluoroquinolone: e.g., ciprofloxacin (off label) [4]
- For patients with V. vulnificus and/or wound infections, add a third-generation cephalosporin: e.g., ceftazidime (off label) . [36]
- Indications
Infections caused by Vibrio species are often self-limiting and may only require supportive care.
Complications
- Complications of noncholera Vibrio infection are common in patients with high levels of free iron (e.g., liver disease, hemochromatosis), diabetes, or immunocompromise.
- Septic shock and necrotizing fasciitis associated with Vibrio vulnificus infection (rare)
Protozoal gastroenteritis
| Overview of protozoal gastroenteritis | |||
|---|---|---|---|
| Pathogen | Transmission | Key features | Treatment |
| Giardia duodenalis [8][37] |
|
|
|
| Entamoeba histolytica [38][39] |
|
|
|
| Cystoisospora belli [40][41] |
|
|
|
| Cryptosporidium species [42] |
|
|
|
Cystoisosporiasis (isosporiasis)
Overview [40][41]
-
Pathogen: Cystoisospora belli; formerly known as Isospora belli
- Worldwide distribution, but commonly found in tropical and subtropical areas (e.g., Central and South America, Southeast Asia, the Caribbean, India, Africa)
- High risk of chronic illness in immunocompromised individuals (e.g., those with HIV)
- Transmission: contaminated food and/or water
- Infectivity: Oocytes shed in feces and become infective after maturing in the environment for 1–2 days
- Prevention: See "Primary prevention of opportunistic infections in HIV."
Clinical features [40][41]
- Usually self-limited in immunocompetent individuals
-
Watery, nonbloody diarrhea
- Most common manifestation
- May last for > 1 month; typically in patients with CD4 counts < 200 cells/mm3 [41]
- Abdominal pain and cramping
- Anorexia
- Nausea and vomiting
- Low-grade fever
- Severe disease is associated with:
- Severe dehydration
- Weight loss
- Malabsorption
Chronic cystoisosporiasis infection lasting > 1 month is an AIDS-defining condition in individuals with HIV. [43]
Diagnostics [40][41]
Oocyst shedding is intermittent; repeat stool examinations and stool sample concentration procedures may be necessary.
-
Stool microscopy: large, ellipsoidal oocysts, 25–30 μm in diameter [44]
- UV fluorescence microscopy: Oocyst walls autofluoresce.
- Modified acid-fast stain: Oocysts stain bright red.
- Gastrointestinal pathogen panel: ↑ sensitivity compared with microscopy
- Upper GI sampling: Consider if there is high clinical suspicion but negative stool studies.
- Duodenal aspirate: detection of oocysts
- Small-bowel biopsy or string test: direct parasite identification
Management [41]
The following treatment recommendations are based on guidelines for people living with HIV. [41]
Acute infection
-
Supportive care
- Fluid and electrolyte supplementation for individuals with dehydration
- Nutritional support for patients with malnutrition
-
First-line antibiotics: trimethoprim/sulfamethoxazole (off-label) [41]
- Consider IV administration for patients with malabsorption.
- Increase daily dose and/or extend treatment duration in patients with worsening or persistent symptoms.
-
Alternative treatments: for sulfa-intolerant patients
- Pyrimethamine (off-label) PLUS leucovorin (off-label) [41]
- Ciprofloxacin (off-label) [41]
Prophylaxis
- Indication: HIV and CD4 count < 200 cells/mm³
- First-line antibiotics: trimethoprim/sulfamethoxazole (off-label) [41]
-
Alternative treatments
- Sulfa-tolerant patients: trimethoprim/sulfamethoxazole (off-label) [41]
- Sulfa–intolerant patients
- First line: pyrimethamine (off-label) PLUS leucovorin (off-label) [41]
- Second line: ciprofloxacin (off-label) [41]
-
Discontinuation: Consider for patients on ART who meet the following criteria [41]
- Sustained CD4 count > 200 cells/mm³ for > 6 months
- No evidence of active infection
Complications [41]
- Electrolyte derangements (e.g., hypokalemia)
- Acalculous cholecystitis
- AIDS cholangiopathy
- Reactive arthritis
- Extraintestinal dissemination (e.g., to the biliary tract, lymph nodes, liver, and/or spleen)
Cryptosporidiosis
Overview [42]
-
Pathogen
- Cryptosporidium species, most commonly C. hominis, C. parvum, or C. meleagridis
- Highest risk of chronic infection in immunocompromised individuals, e.g., those with HIV (typically at CD4 counts < 100 cells/mm³)
-
Transmission
- Fecal-oral
- Contaminated water
- Person-to-person (e.g., through sexual contact)
Clinical features [42]
- Chronic, watery diarrhea (lasting > 1 month; in immunocompromised patients, e.g., those with HIV)
- Nausea
- Abdominal pain
Diagnostics [42]
Oocyst shedding is intermittent; repeat stool examinations and stool sample concentration procedures may be necessary.
- Stool microscopy; : spherical, homogeneously-stained acid-fast oocysts, 4–5 μm in diameter [44]
- Gastrointestinal pathogen panel
Treatment [42]
- Symptomatic care (e.g., oral rehydration solution and antimotility agents)
- Consider antiparasitic therapy (e.g., nitazoxanide ).
External Resources
References
- "Campylobacter (Campylobacteriosis)". https://web.archive.org/web/20201017012508/https://www.cdc.gov/campylobacter/technical.html. [2019-12-23]
- "Campylobacter Fact sheet". http://www.who.int/mediacentre/factsheets/fs255/en/. [2016-12-01]
- Switaj T, Winter K, Christensen S. "Diagnosis and Management of Foodborne Illness". Am Fam Physician
- Riddle MS, DuPont HL, Connor BA. "ACG Clinical Guideline: Diagnosis, Treatment, and Prevention of Acute Diarrheal Infections in Adults". Am J Gastroenterol. 111(5). :602-622. (2016)
- DuPont HL. "Acute Infectious Diarrhea in Immunocompetent Adults". N Engl J Med. 370(16). :1532-1540. (2014)
- "Shigella – Shigellosis - General Information". https://web.archive.org/web/20170416130145/https://www.cdc.gov/shigella/general-information.html. [2016-08-03]
- Shane AL, Mody RK, Crump JA, et al. "2017 Infectious Diseases Society of America Clinical Practice Guidelines for the Diagnosis and Management of Infectious Diarrhea". Clin Infect Dis. 65(12). :e45-e80. (2017)
- Barr W, Smith A. "Acute Diarrhea in Adults". Am Fam Physician. (2014)
- "Reptiles and Amphibians". https://www.cdc.gov/features/salmonellafrogturtle/index.html. [2019-10-28]
- "Cholera - Vibrio cholerae infection - Antibiotic Treatment". https://web.archive.org/web/20170610025706/https://www.cdc.gov/cholera/treatment/antibiotic-treatment.html. [2015-01-20]
- LaRocque R, Harris JB. "Cholera: Clinical Features, Diagnosis, Treatment, and Prevention". UpToDate. UpToDate. https://www.uptodate.com/contents/cholera-clinical-features-diagnosis-treatment-and-prevention. [2018-02-08]
- "Yersinia enterocolitica (Yersiniosis)". https://web.archive.org/web/20180627055926/https://www.cdc.gov/yersinia/healthcare.html. [2016-10-24]
- Humphries RM, Linscott AJ. "Laboratory Diagnosis of Bacterial Gastroenteritis". Clin Microbiol Rev. 28(1). :3-31. (2015)
- "Travelers' Health - Travelers' Diarrhea". https://web.archive.org/web/20170322081537/https://wwwnc.cdc.gov/travel/yellowbook/2016/the-pre-travel-consultation/travelers-diarrhea. [2015-07-10]
- "Food safety - Clostridium perfringens". https://web.archive.org/web/20170502095138/https://www.cdc.gov/foodsafety/diseases/clostridium-perfringens.html. [2017-01-10]
- Sobel J, Mixter CG, Kolhe P, et al. "Necrotizing enterocolitis associated with Clostridium perfringens type A in previously healthy North American adults". J Am Coll Surg. 201(1). :48-56. (2005)
- Baker-Austin C, Oliver JD, Alam M, et al. "Vibrio spp. infections". Nat Rev Dis Primers. 4(1). :1-19. (2018)
- Bross MH, Soch K, Morales R, Mitchell RB. "Vibrio vulnificus infection: diagnosis and treatment.". Am Fam Physician. 76(4). :539-44. (2007)
- Zollner-Schwetz I, Krause R. "Therapy of acute gastroenteritis: role of antibiotics". Clin Microbiol Infect. 21(8). :744-749. (2015)
- Bányai K, Estes MK, Martella V, Parashar UD. "Viral gastroenteritis". The Lancet. 392(10142). :175-186. (2018)
- Hartman S, Brown E, Loomis E, Russell HA. "Gastroenteritis in Children". Am Fam Physician. 99(3). :159-165. (2019)
- AAP Committee on Infectious Diseases. "Red Book: 2021–2024 Report of the Committee on Infectious Diseases". American Academy of Pediatrics. (2021). ISBN: 9781610025218
- Hall AJ, Vinjé J, Lopman B et al. "Updated Norovirus Outbreak Management and Disease Prevention Guidelines". Morbidity and Mortality Weekly Report. 60(3). :1-15. (2011)
- Crawford SE, Ramani S, Tate JE, et al. "Rotavirus infection". Nat Rev Dis Primers. 3(1). (2017)
- Barclay L, Park GW, Vega E, et al. "Infection control for norovirus". Clin Microbiol and Infect. 20(8). :731-740. (2014)
- "Nationally Notifiable Diseases". https://web.archive.org/web/20210927031918/https://www.cdc.gov/healthywater/statistics/surveillance/notifiable.html
- "Division of Foodborne, Waterborne, and Environmental Diseases (DFWED) - Surveillance & Data Systems". https://web.archive.org/web/20170130163741/https://www.cdc.gov/ncezid/dfwed/keyprograms/surveillance.html. [2016-09-29]
- Lee RM, Lessler J, Lee RA, et al. "Incubation periods of viral gastroenteritis: a systematic review". BMC Infect Dis. 13(1). (2013)
- Glass RI, Parashar UD, Estes MK. "Norovirus Gastroenteritis". N Engl J Med. 361(18). :1776-1785. (2009)
- Robilotti E, Deresinski S, Pinsky BA. "Norovirus". Clin Microbiol Rev. 28(1). :134-164. (2015)
- Anderson EJ, Weber SG. "Rotavirus infection in adults". Lancet Infect Dis. 4(2). :91-99. (2004)
- Sanaei Dashti A, Ghahremani P, Hashempoor T, Karimi A. "Molecular Epidemiology of Enteric Adenovirus Gastroenteritis in under-Five-Year-Old Children in Iran". Gastroenterol Res Pract. 2016. :1-5. (2016)
- Albert MJ. "Enteric adenoviruses". Arch Virol. 88(1-2). :1-17. (1986)
- Bosch A, Pintó RM, Guix S. "Human Astroviruses". Clin Microbiol Rev. 27(4). :1048-1074. (2014)
- Fakhreddine AY, Frenette CT, Konijeti GG. "A Practical Review of Cytomegalovirus in Gastroenterology and Hepatology". Gastroenterol Res Pract. 2019. :1-11. (2019)
- "About Cytomegalovirus (CMV)". https://web.archive.org/web/20200925152731/https://www.cdc.gov/cmv/overview.html. [2020-08-18]
- CDC. "DPDx - Laboratory Identification of Parasites of Public Health Concern: Cystoisosporiasis". (2024)
- "Guidelines for the Prevention and Treatment of Opportunistic Infections in Adults and Adolescents with HIV". https://web.archive.org/web/20260126024001/https://clinicalinfo.hiv.gov/sites/default/files/guidelines/documents/adult-adolescent-oi/guidelines-adult-adolescent-oi.pdf. [2025-07-14]
- Selik RM, Mokotoff ED, Branson B, et al. "Revised Surveillance Case Definition for HIV Infection — United States, 2014". MMWR Recomm Rep. :1-10. (2014)
- Koneman EW. "Koneman's Color Atlas and Textbook of Diagnostic Microbiology". Lippincott Williams & Wilkins. (2006). ISBN: 9780781730143
- "Parasites - Giardia - Sources of Infection & Risk Factors". https://web.archive.org/web/20170505090647/https://www.cdc.gov/parasites/giardia/infection-sources.html. [2015-07-21]
- Shirley DAT, Farr L, Watanabe K, Moonah S. "A Review of the Global Burden, New Diagnostics, and Current Therapeutics for Amebiasis". Open Forum Infect Dis. 5(7). (2018)
- "Amebiasis". https://web.archive.org/web/20170123233339/https://www.cdc.gov/dpdx/amebiasis/index.html. [2013-11-29]
- "Guidelines for the Prevention and Treatment of Opportunistic Infections in Adults and Adolescents with HIV". https://web.archive.org/web/20240520230552/https://clinicalinfo.hiv.gov/en/guidelines/hiv-clinical-guidelines-adult-and-adolescent-opportunistic-infections/whats-new?view=full. [2024-05-02]