Summary
Infectious rashes are common in children and are caused by viruses, bacteria, fungi, or parasites. In acutely ill patients, perform initial management of rash to identify red flags for a life-threatening rash. A detailed history and skin examination are essential in all patients, as infectious rashes can often be diagnosed clinically. Diagnostic testing may be obtained to confirm certain diagnoses (e.g., measles, rubella, bacterial or fungal infections) and to exclude alternative diagnoses in case of diagnostic uncertainty. Management is based on the underlying cause. Most viral infections are managed with supportive care. Pharmacological treatment with antibiotics, antivirals, or ectoparasiticides may be indicated depending on the causative organism.
For information on rashes associated with congenital infections, see “Congenital TORCH infections.” For more information on each specific infection, see the respective articles.


© AMBOSS
Etiology
Viral [1][2][3]
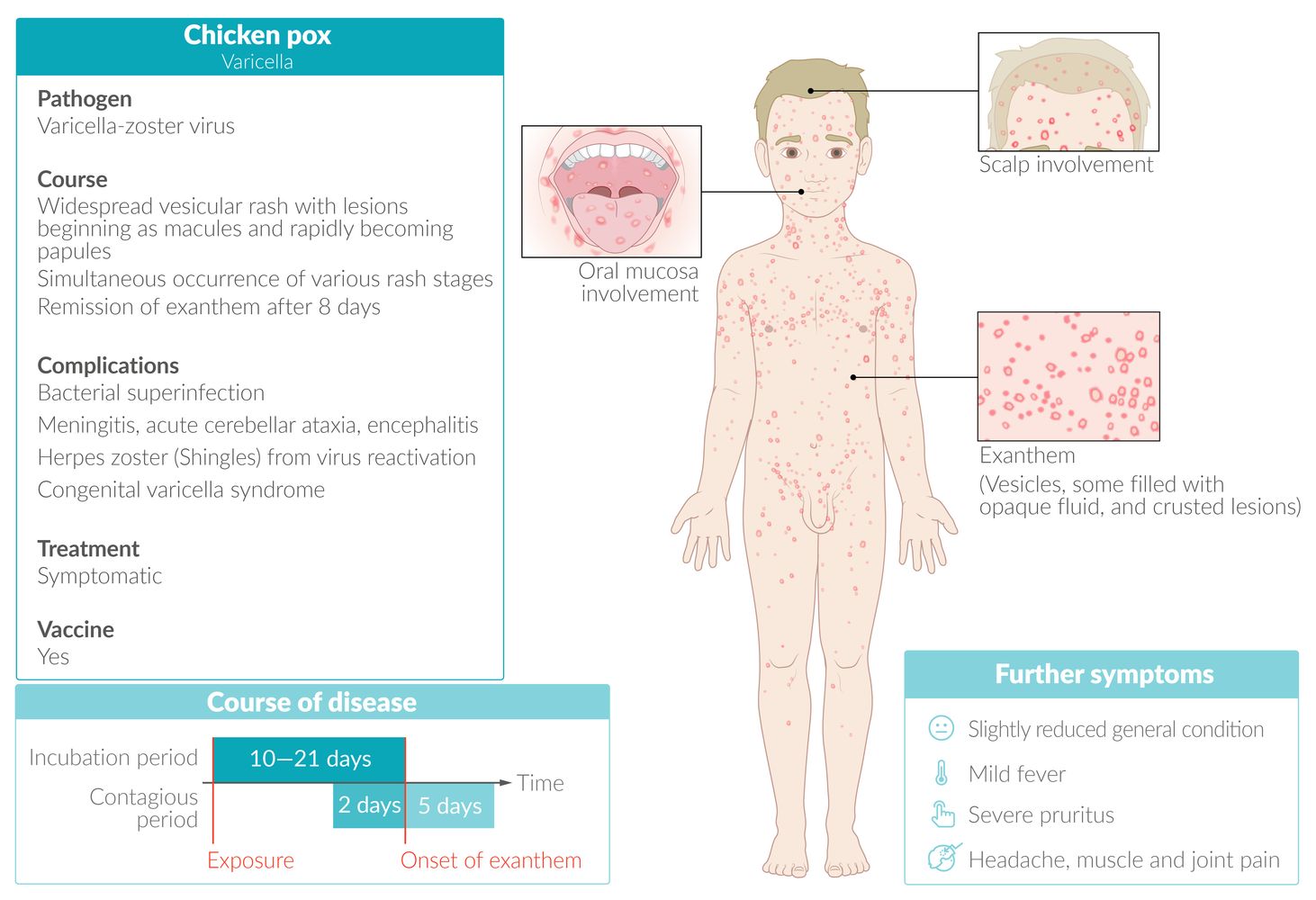
- Chickenpox
- Hand, foot, and mouth disease [4]
- Measles
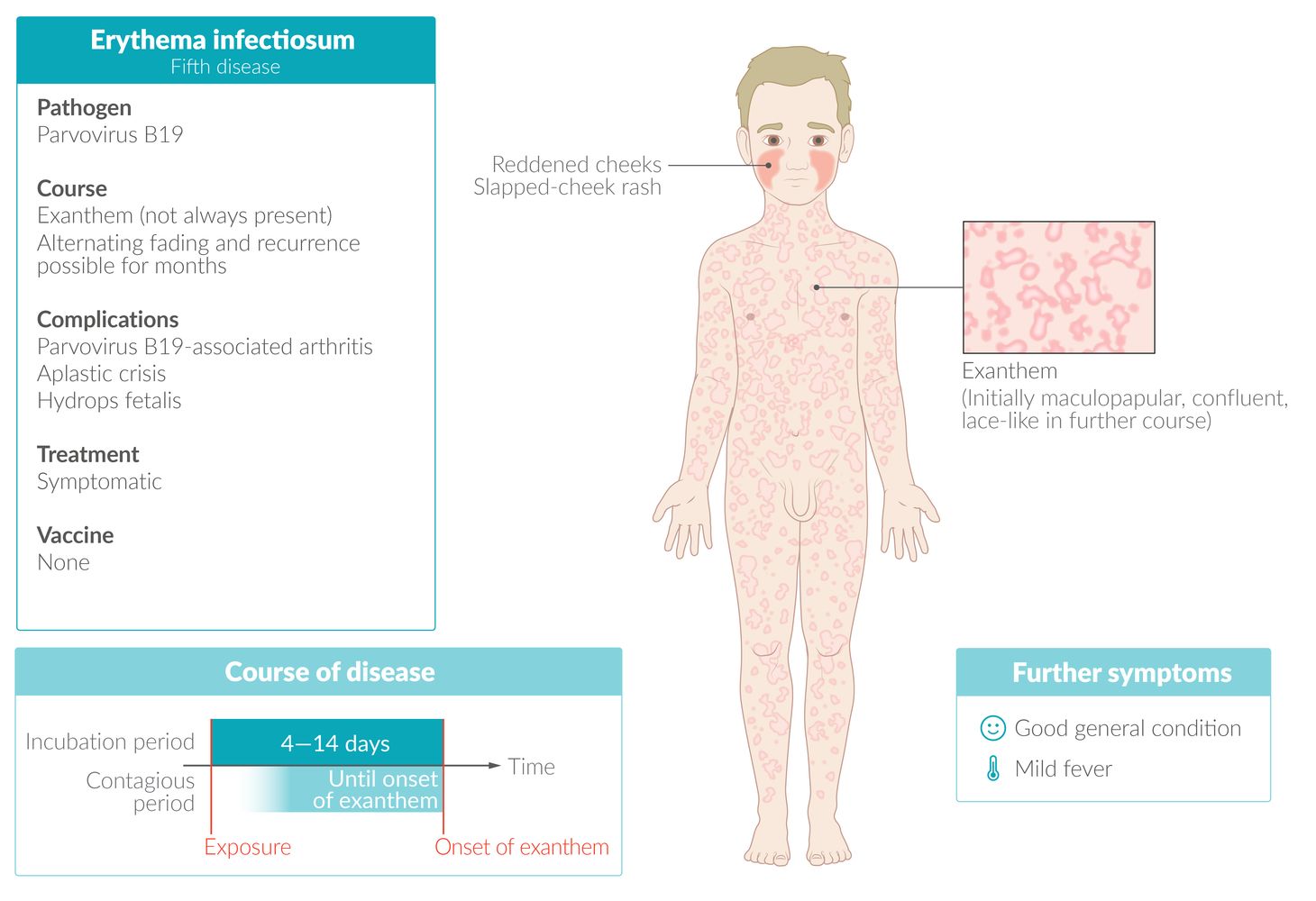
- Erythema infectiosum (Fifth disease)
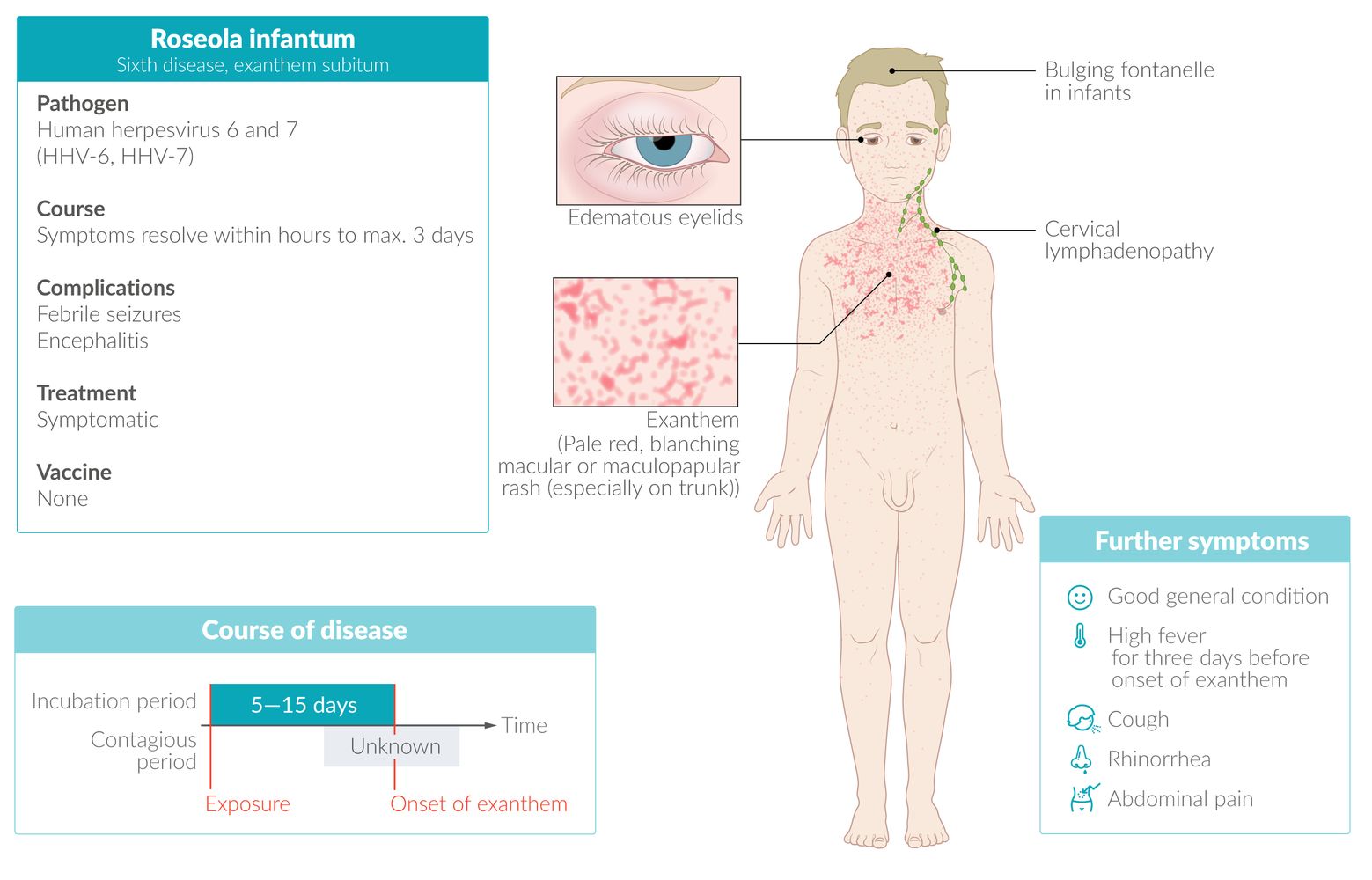
- Roseola infantum
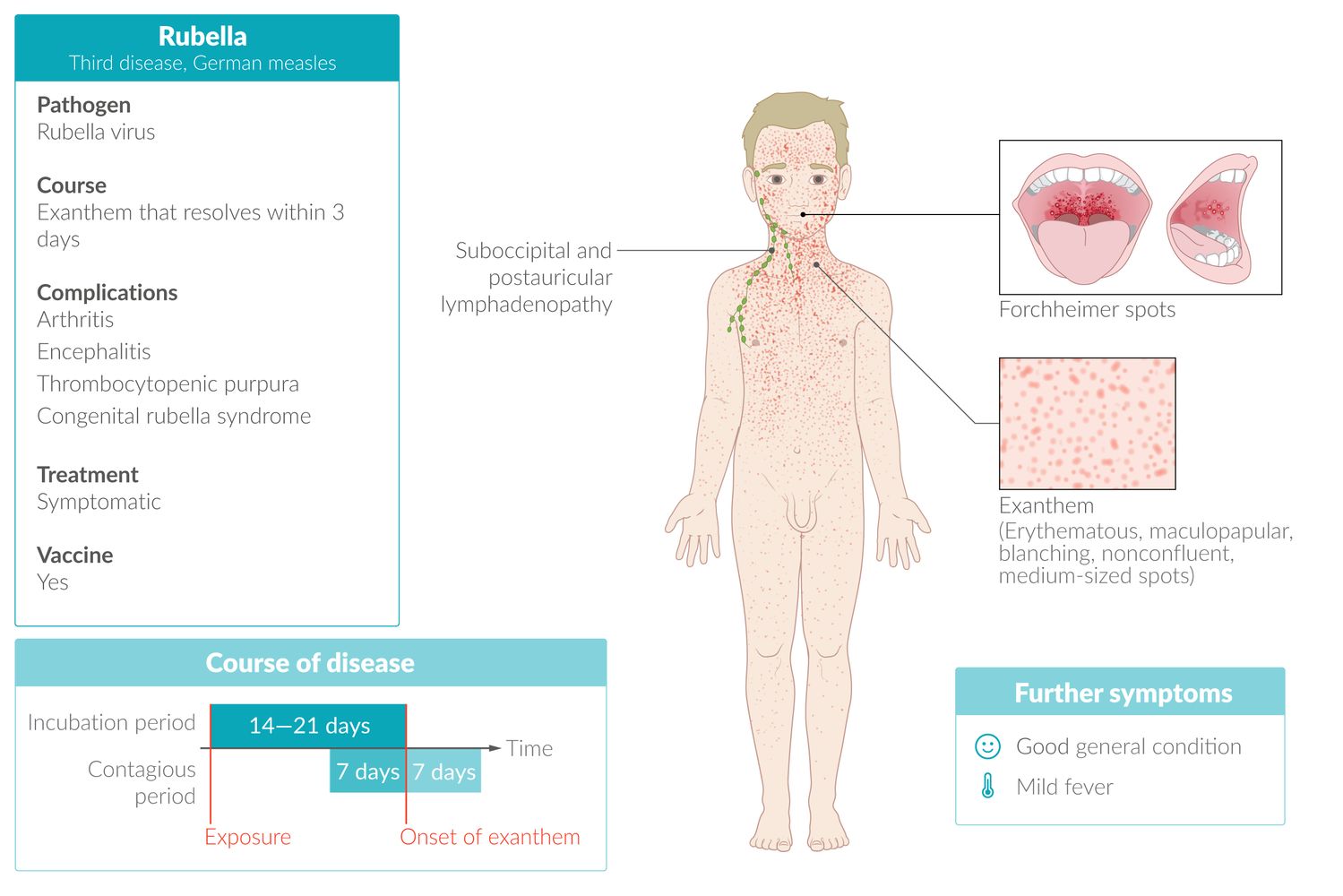
- Rubella
- Molluscum contagiosum
- Herpes simplex virus infections [5]
- Shingles
- Gianotti-Crosti syndrome
- Dengue
- Zika virus
- Chikungunya virus
- Acute HIV exanthem [6]
- Nonspecific viral exanthems [6]
Bacterial [1][6]
- Scarlet fever
-
Skin and soft tissue infections, e.g.:
- Impetigo [2]
- Staphylococcal scalded skin syndrome
- Folliculitis
- Meningococcal septicemia
- Lyme disease
- Rocky Mountain spotted fever (RMSF)
- Toxic shock syndrome
- Disseminated gonococcal infection [3]
Fungal [1]
- Dermatophyte infections
- Candidiasis
- Pityriasis versicolor
Parasitic [1]
- Scabies
- Lice
Clinical evaluation
Focused history [2][6]
-
Rash characteristics
- Onset, duration, progression
- Distribution
-
Associated symptoms
- Constitutional symptoms (e.g., fever)
- Pruritus
- Arthralgias
- Pharyngitis
-
Exposures
- New medications or products
- Recent travel
- Sick contacts
- Arthropod bites
Focused examination [2][6]
- Vital signs: to assess for fever
- General appearance: to assess for irritability or lethargy
- Lymph node examination
-
Skin examination: See “Primary skin lesions” and “Secondary skin lesions” for describing and documenting rashes.
- Determine lesion morphology (e.g., macules, papules, vesicles, pustules).
- Examine the entire skin and mucosa to determine rash distribution.
- Describe additional lesion characteristics (e.g., color, presence of scale or Nikolsky sign, blanchable).
Diagnostics
Approach [1][2][6]
- Acute illness: Perform initial management of rash, including identifying red flags for a life-threatening rash.
- Ensure appropriate isolation precautions (e.g., for suspected measles or meningococcal septicemia).
- In children, diagnosis is usually clinical.
- Obtain laboratory studies as needed to:
- Identify pathogen for diagnostic confirmation
- Exclude alternative diagnoses (see “Mimics”)
- Consider biopsy to rule out mimics in case of diagnostic uncertainty.
Laboratory studies [1][6]
- CBC: to identify leukocytosis, thrombocytopenia
-
Microbiological studies: to identify causative organism based on clinical suspicion
- Diagnostics for scarlet fever (e.g., rapid strep test, throat culture)
- Diagnostics for measles (e.g., measles-specific antibodies, RT-PCR)
- Diagnostics for rubella (e.g., rubella-specific antibodies, RT-PCR)
- Diagnostics for dermatophyte infections (e.g., KOH test, fungal culture)
- Diagnostics for HSV infections (e.g., PCR, viral culture)
- Diagnostics for RMSF (e.g., Rickettsia antibody panels)
- Diagnostics for Lyme disease (e.g., Lyme antibody testing)
- Diagnostics for meningitis in children (e.g., blood and CSF cultures)
Common causes
| Common causes of infectious rash in children [1][2][7][8] | |||
|---|---|---|---|
| Disease (pathogen) | Characteristic clinical features | Management | |
| Measles (Measles virus) |
|
|
|
| Scarlet fever (Streptococcus pyogenes) |
|
|
|
| Rubella (Rubella virus) |
|
|
|
| Fifth disease (erythema infectiosum) (Parvovirus B19) |
|
|
|
| Roseola infantum (exanthem subitum) (Human herpesvirus 6) |
|
|
|
| Chickenpox (varicella) (Varicella zoster virus) |
|
|
|
| Hand, foot, and mouth disease (Group A Coxsackievirus) |
|
|
|
| Impetigo [10] (Streptococcus pyogenes, Staphylococcus aureus) |
|
|
|
Measles and rubella are nationally notifiable diseases in the US. Notify the local health department of any suspected cases. [1]




 fact sheet")
 fact sheet")

© AMBOSS
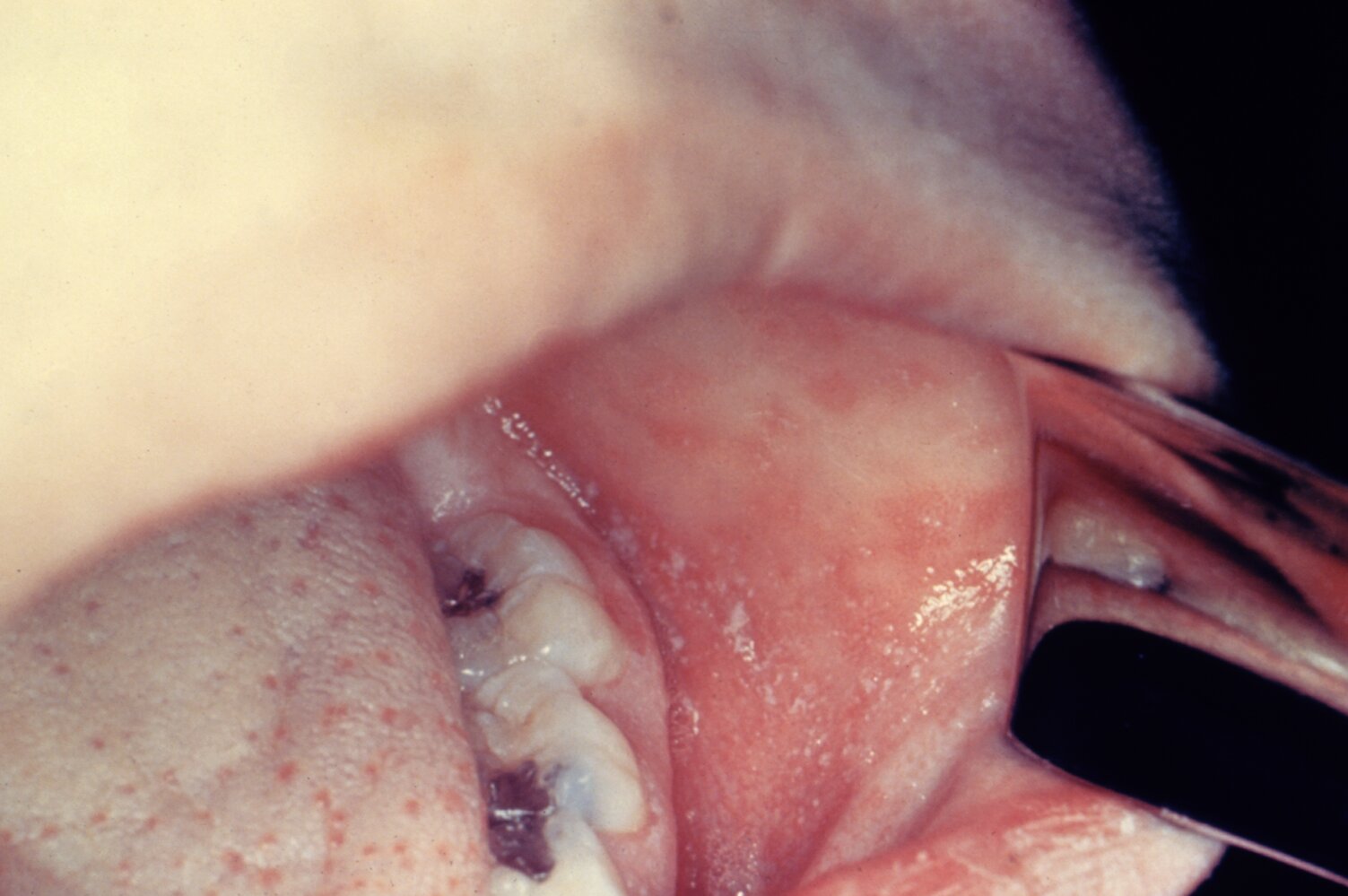
Numerous tiny white spots on an erythematous background (Koplik spots; examples indicated by arrowheads) are visible on the buccal mucosa.
Koplik spots are pathognomonic for measles infection.
This image is an adaptation. Source of original image: Centers for Disease Control and Prevention (CDC). Original title: “ID#4500”. Created by: CDC. Licensed under Public Domain. Modifications to original image: Image turned.

Photograph of a toddler
There is a generalized erythematous maculopapular exanthem. Some confluence is visible (e.g., on the upper thighs).
Source: "Measles rash PHIL", Centers for Disease Control and Prevention, Atlanta,USA, Centers for Disease Control and Prevention licensed under Public Domain
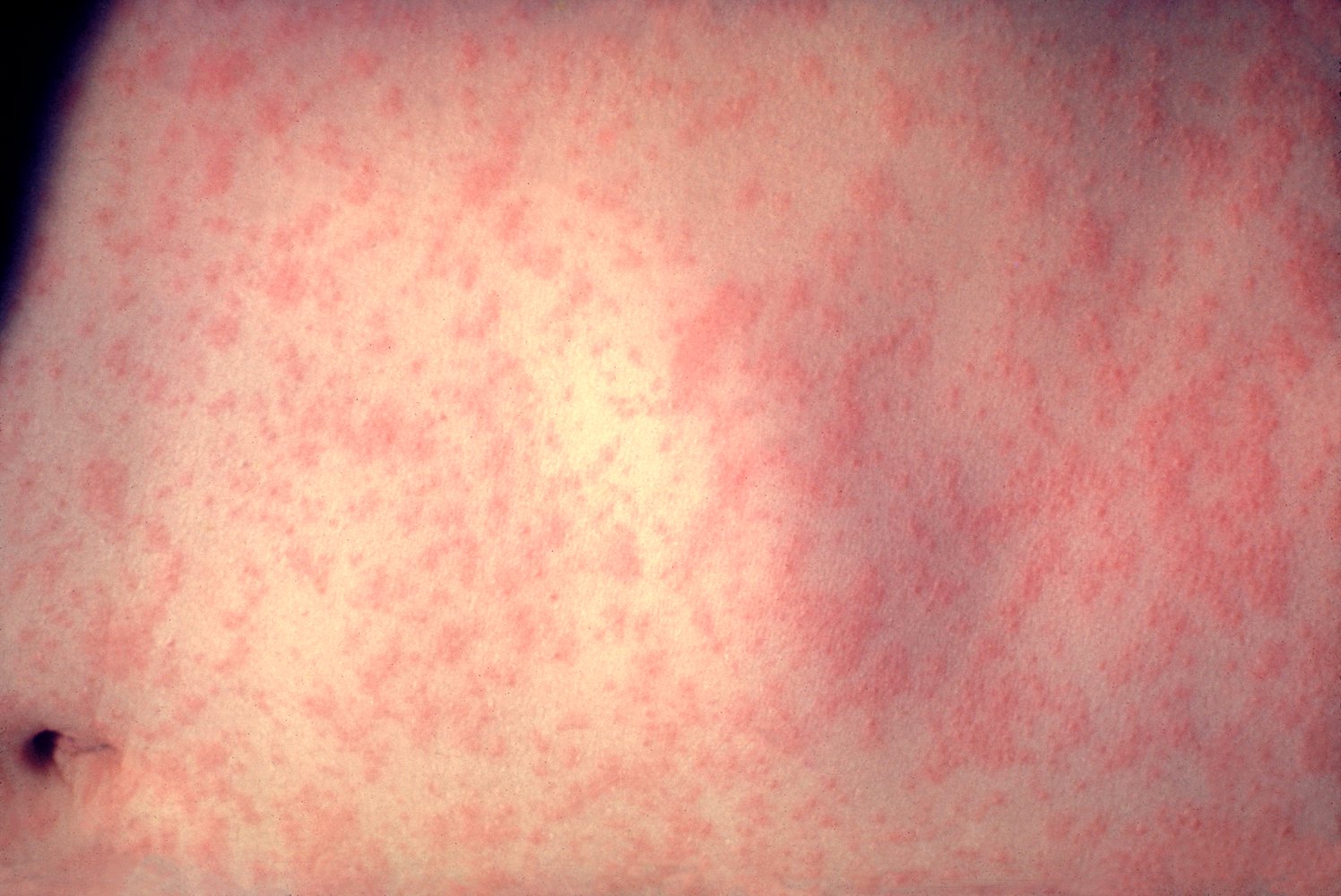
A widespread maculopapular rash is visible across the abdomen.
Source: "ID#: 3168", CDC/ Heinz F. Eichenwald, MD, Centers for Disease Control and Prevention (CDC) licensed under Public Domain

A partially confluent maculopapular exanthem is visible on the child's back.
In combination with the characteristic clinical features, these skin findings are suggestive of measles.
Source: "Measles in African Child 3", Mike Blyth, Wikimedia Commons licensed under Public Domain
{kind=link}

Multiple maculopapular blanching and partially confluent patches are disseminated over the head, neck, and back of this young patient.
These findings are consistent with a desquamating rash, which can occur after fading of the first erythematous exanthema, caused by an infection with the measles virus.
Source: “Figure 34, In: Atlas of Paediatric HIV Infection” by Regina E. Oladokun, Rannakoe J. Lehloenya, Carol Hlela et.al., Openbooks, licensed under CC BY-ND 4.0.
© AMBOSS

The typical scarlet-colored, fine, maculopapular exanthem of scarlet fever is seen on the right arm. Flushed cheeks and perioral pallor are also evident.
Source: “Scarlet Fever” by Badobadop, Wikimedia Commons, licensed under CC BY-SA 3.0. Modifications: Pixelated eyes.
{kind=link}

Palms showing lamellar desquamation of the skin ("skin glove"). Desquamation typically begins 7–10 days after rash resolves, and lasts up to 4–6 weeks. The face and trunk typically show pityriasiform scales.
Source: "Scharlach", YasminFeth, Wikimedia Commons licensed under Public Domain
{kind=link}

The tongue is bright red with prominent edematous papillae and a white coating. This finding is typically seen during the exanthematous phase of scarlet fever, but may also be seen in other conditions such as toxic shock syndrome or Kawasaki disease.
Source: “Scharlach” by Martin Kronawitter, Wikimedia Commons, licensed under CC BY-SA 2.5.
{kind=link}
© AMBOSS

A nonconfluent, pink, maculopapular rash is visible across this infant's trunk and extremities.
Source: "ID#: 4513", CDC, Centers for Disease Control and Prevention (CDC) licensed under Public Domain

Photograph of the posterior torso of a child
Coalescing red-pink macules with tiny papules are seen on the trunk.
These features are characteristic of a viral exanthem, in this case caused by rubella. In rubella, the rash typically starts in the face and neck region and spreads downwards.
Source: "ID#: 712", CDC, Centers for Disease Control and Prevention licensed under Public Domain
© AMBOSS

The cheeks are bright red (slapped-cheek rash) and a diffuse, red, confluent rash with macules and papules is visible over the body of this infant.
This is the characteristic cutaneous appearance of erythema infectiosum (fifth disease), which is caused by infection with parvovirus B19.
This image is an adaptation. Source of original image: Wikimedia Commons. Original title: “Fifth disease”. Created by: Andrew Kerr. Licensed under Public Domain. Modifications to original image: Pixelated eyes.
{kind=link}

Multiple erythematous, partially confluent macules and papules extend over the upper arm in a reticular pattern.
This is the typical appearance of the exanthem associated with erythema infectiosum (fifth disease).
Image source of original image: www.paediatrie-in-bildern.de. Created by: Dr. Thomas Rautenstrauch.

Diffuse erythema with perioral sparing is visible on both cheeks (slapped cheek rash).
This rash is characteristic of erythema infectiosum (fifth disease).
© Massachusetts Medical Society. All rights reserved. AMBOSS SE, exclusive licensee.
© AMBOSS

Photograph of a 1-year-old child with recent febrile illness
A patchy, nonpruritic, blanching, erythematous rash with macules and papules can be seen on the trunk and arms. Symptoms manifested one day after the fever resolved.
These features are consistent with roseola infantum.
Source: "Sestamalattia", Emiliano Burzagli, Wikimedia Commons licensed under Public Domain
{kind=link}

Photograph of a 9-month-old infant with recent high fever
A patchy, macular exanthem is visible on the trunk, neck, and behind the ears. Symptoms developed after the fever resolved.
These features are consistent with roseola infantum.
© AMBOSS
© AMBOSS

Upper body of a young boy with exanthem showing the simultaneous occurrence of various stages of rash; mainly vesicles and pustules, no crusted erosions. This clinical finding is also referred to as "starry sky" and is typical of chickenpox.
Source: "Varicela Aranzales", Camiloaranzales, Wikimedia Commons licensed under Public Domain
{kind=link}

The face of the girl shows macules, vesicles, and papules on an erythematous base, as well as erupted vesicles and crusted papules. The simultaneous occurrence of various stages of rash is sometimes described as "starry sky" and is typical of chickenpox.
Source: "ID#: 10486", CDC/ Dr. John Noble, Jr., Centers for Disease Control and Prevention (CDC) licensed under Public Domain

Multiple disseminated papules and vesicles on an erythematous base are visible on this patient's face. Numerous vesicles in the preauricular region appear umbilicated.
These lesions are caused by an infection with varicella zoster virus (VZV).
Source: “Varicelle importante chickenpox” by Grook da oger, Wikimedia Commons, licensed under CC BY-SA 4.0.
{kind=link}

Hands and feet of a 36-year-old male patient
Macular and papular lesions are visible on the inner surface of the hands and feet.
The localization in conjunction with the enanthem of the mucous membranes is typical of hand, foot, and mouth disease.
Source: “Hand Foot Mouth Disease Adult 36Years” by KlatschmohnAcker, Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}

12-month-old infant
Typical white-gray blisters with a diameter of approx. 3–5 mm surrounded by an erythematous halo are seen on the fingers (top images). Another common finding, as seen here, is a disseminated macular and papular rash on the upper and lower legs (bottom left). In addition, there is a partially crusted papulovesicular rash in the perioral region (bottom right). However, the eponymous involvement of the mouth refers to the typically painful aphthous enanthem of the oral mucosa, which is not shown here.
© AMBOSS

Confluent scabbed erosions and honey-colored crusts are visible in the perioral region. This appearance is typical of impetigo, which, in this patient, developed secondary to preexisting eczema and immunosuppression caused by HIV infection.
Source: “Figure 3, in: Atlas of Paediatric HIV Infection” by R. E. Oladokun, R. J. Lehloenya, C. Hlela et al., Open books - University of Cape Town, licensed under CC BY-ND 4.0.

Confluent erosions and honey-colored crusts with an erythematous base are visible on the face, forehead, temporal region, and part of the neck. As in this photo, vesicles may not always be present or noticeable.
Source: © IMPP
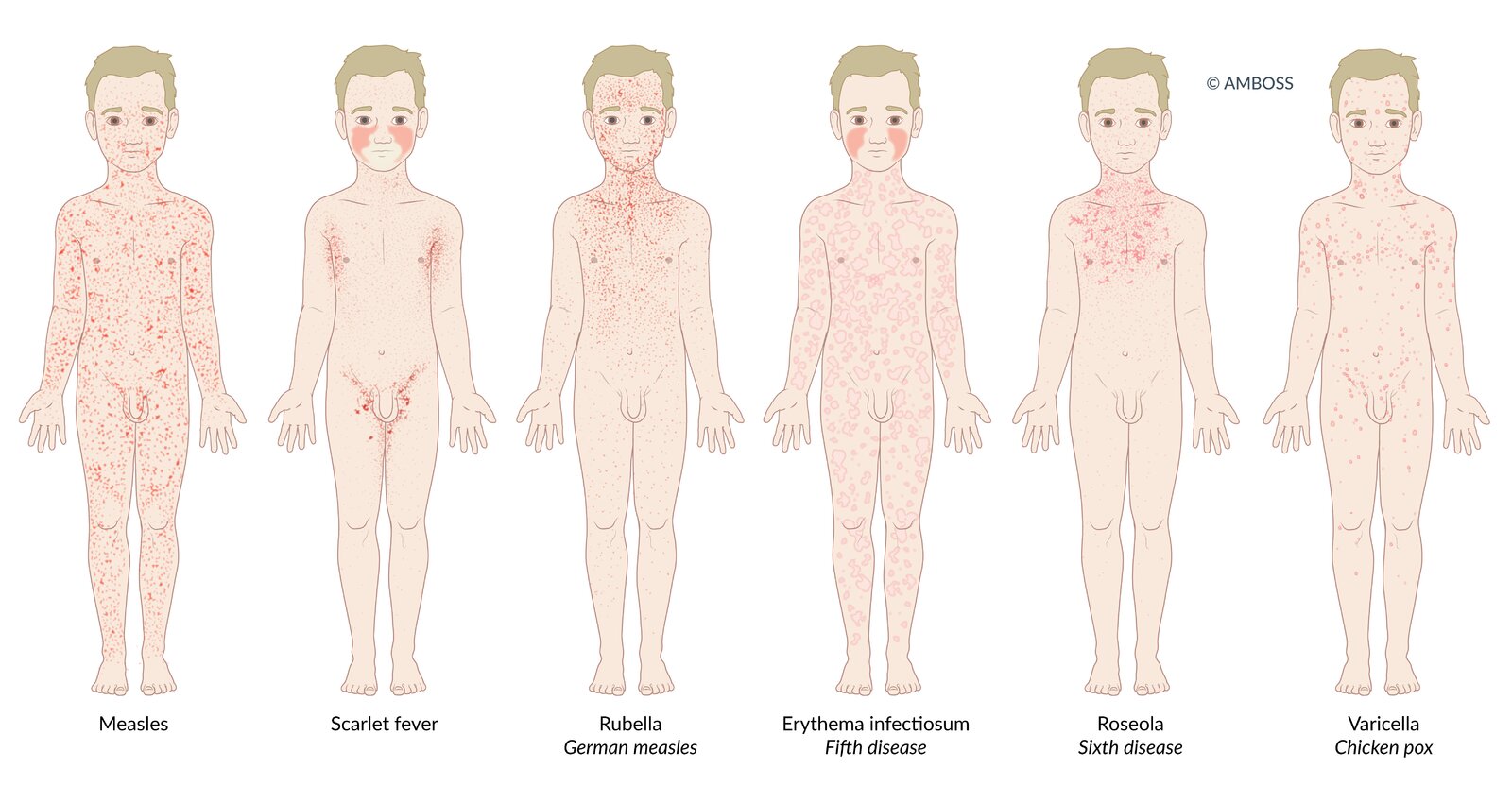
Many infectious diseases in children present with a rash (exanthem). The distribution and morphological characteristics of the exanthem allow the diseases to be differentiated from one another.
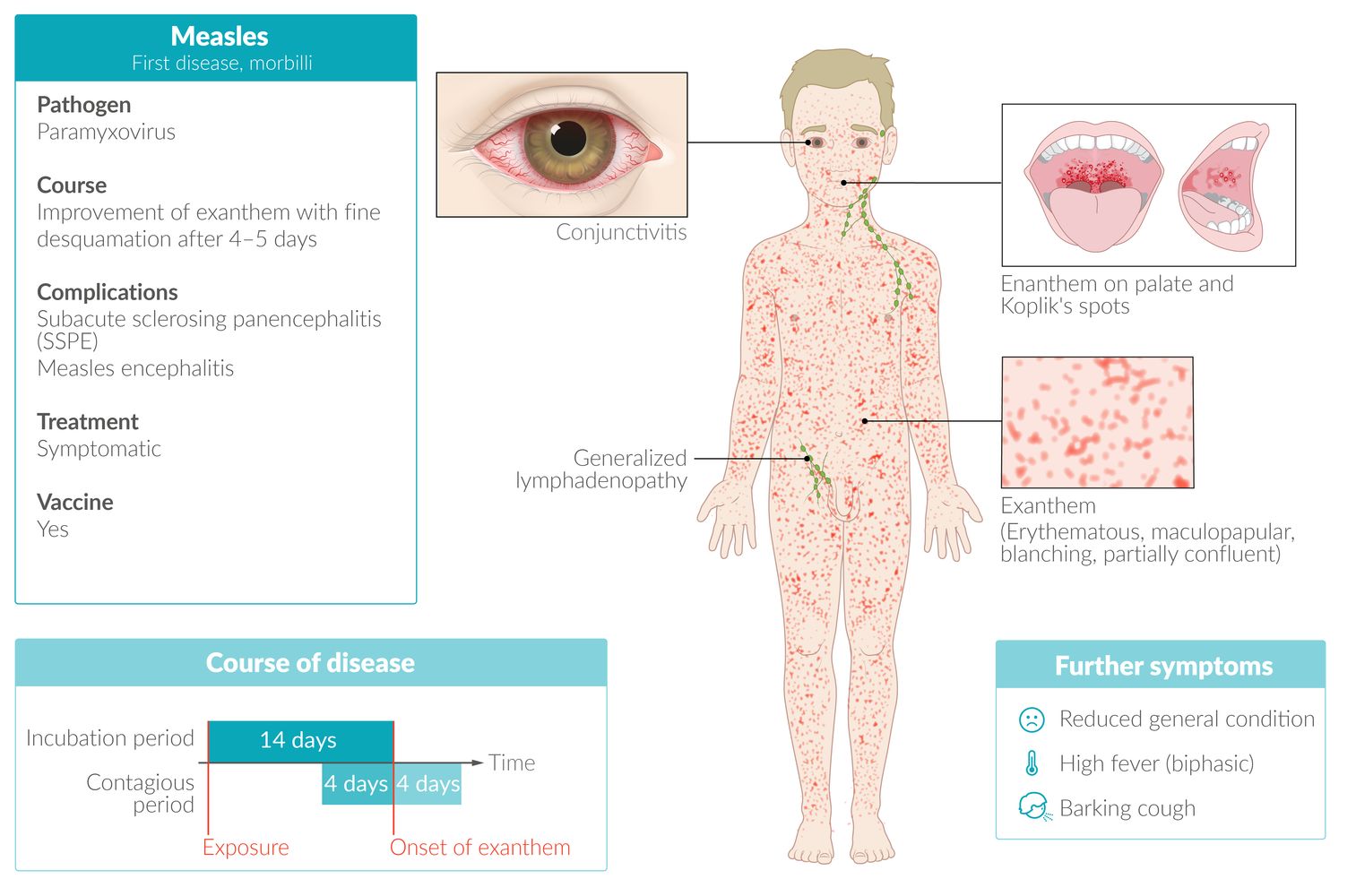
Measles: Patients present with a dark red, erythematous, maculopapular, partially confluent exanthem, which spreads from behind the ears to the rest of the body.
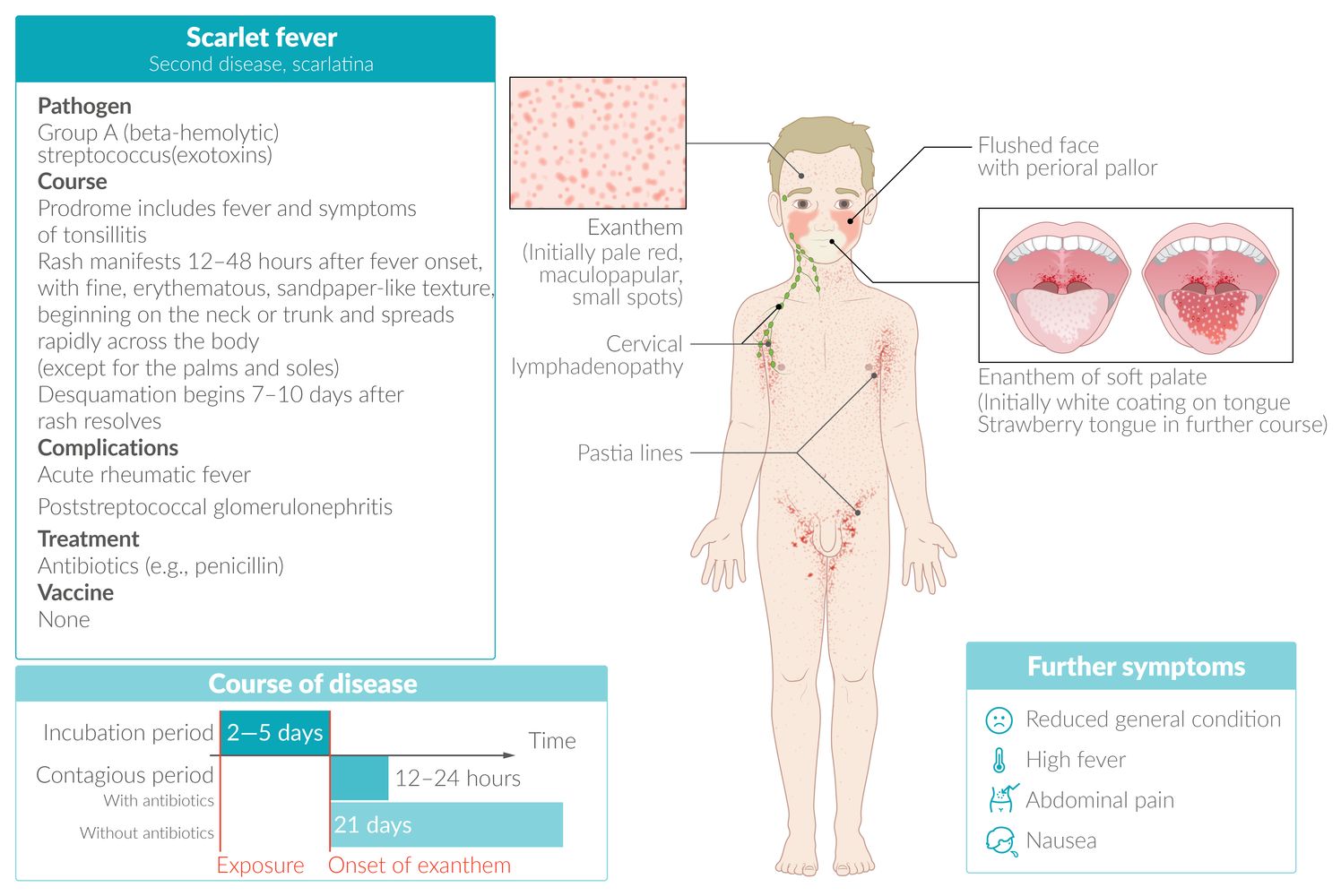
Scarlet fever: Patients present with a fine, light red rash with sandpaper-like texture. The exanthem begins on the neck or trunk and disseminates to the whole body. Cheeks may be flushed with perioral pallor. In flexural areas (e.g., axilla and groin), the rash may be more pronounced and linear petechiae (Pastia lines) may be present.
Rubella (German measles): Patients typically present with a nonconfluent, pink, maculopapular exanthem, which begins on the face and spreads to the trunk and extremities.
Erythema infectiosum (fifth disease): A confluent, maculopapular rash appears only in ¼ of patients. It may take on a lace-like, reticular appearance over time. Additionally, patients present with diffuse redness of the face with perioral sparing (slapped-cheek rash).
Roseola infantum (sixth disease): 3-7 days of high fever are followed by a sudden decrease in temperature and development of a patchy, blanching rose-pink maculopapular rash. The rash originates on the trunk, and may spread to the face and extremities.
Varicella (chickenpox): The exanthem affects the whole body, typically spreading to the scalp as well. Various stages of the rash occur simultaneously, which leads to the characteristic clinical finding known as “starry sky.”
© AMBOSS
Management
Management depends on the specific cause.
- Most viral infections are managed with supportive care.
- Pharmacological treatment (e.g., antibiotics, antivirals, ectoparasiticides) may be indicated depending on the causative organism.
Mimics
- Pityriasis rosea
- Dermatoses
- Atopic dermatitis
- Allergic contact dermatitis
- Irritant contact dermatitis
- Seborrheic dermatitis
-
Drug hypersensitivity reactions
- Exanthematous drug eruptions
- Drug reaction with eosinophilia and systemic symptoms (DRESS syndrome)
- Stevens-Johnson syndrome
- Toxic epidermal necrolysis
- Acute generalized exanthematous pustulosis
- Urticaria
- Rosacea
-
Vasculitides
- Kawasaki disease
- IgA vasculitis
- Multisystem inflammatory syndrome in children
- Systemic lupus erythematosus
Always consider drug reactions as a potential cause of rash.
References
- Committee on Infectious Disease, American Academy of Pediatrics. "Red Book: 2024-2027 Report of the Committee on Infectious Diseases, 33rd Edition". American Academy of Pediatrics. (2024). ISBN: 9781610027373
- Allmon A, Deane K, Martin KL. "Common Skin Rashes in Children". Am Fam Physician. 92(3). :211-6. (2015)
- Ely JW, Seabury Stone M. "The generalized rash: part I. Differential diagnosis". Am Fam Physician. 81(6). :726-34. (2010)
- Saavedra A, et al. "Fitzpatrick's Color Atlas and Synopsis of Clinical Dermatology, Ninth Edition". McGraw Hill Professional. (2023). ISBN: 9781264278022
- Weber R. "Pharyngitis". Prim Care. 41(1). :91-98. (2014)
- Hartman-Adams H, Banvard C, Juckett G. "Impetigo: diagnosis and treatment". Am Fam Physician. 90(4). :229-35. (2014)
- Gonzales Y Tucker RD, Addepalli A. "Fever and Rash". Emerg Med Clin North Am. 42(2). :303-334. (2024)
- "Hand, Foot & Mouth Disease". https://web.archive.org/web/20250214215011/https://wwwnc.cdc.gov/travel/yellowbook/2024/infections-diseases/hand-foot-and-mouth-disease
- Biesbroeck L, Sidbury R. "Viral exanthems: an update". Dermatol Ther. 26(6). :433-438. (2013)
- Ely JW, Seabury Stone M. "The generalized rash: part II. Diagnostic approach". Am Fam Physician. 81(6). :735-9. (2010)