Summary
Infective endocarditis (IE) is an infection of the endocardium that typically affects one or more heart valves. The condition is usually due to bacteremia, which in adults is most commonly caused by dental procedures, surgery, distant primary infections, and nonsterile injections. Risk factors in children include congenital heart defects and invasive procedures. IE may be acute (developing over hours or days) or subacute (developing over weeks to months). Acute bacterial endocarditis is usually caused by Staphylococcus aureus and may cause rapid destruction of endocardial tissue. Subacute bacterial endocarditis is most commonly caused by viridans streptococci and usually affects individuals with preexisting damage to the heart valves, congenital heart defects, and/or prosthetic valves. Clinical features are similar in adults and children and include constitutional symptoms (e.g., fatigue, fever, chills, malaise) and signs of pathological cardiac changes (e.g., new or changed heart murmur, heart failure signs). Some patients develop symptoms of organ damage (e.g., glomerulonephritis, septic embolic stroke). Management is complex and early involvement of infectious diseases is recommended. The 2023 Duke-ISCVID criteria are used to assess the likelihood of IE, and the diagnosis is confirmed based on culture, histopathology, and/or imaging findings. Initial treatment consists of empiric IV antibiotics, which are adjusted based on blood culture results and continued for several weeks. Distinguishing between native and prosthetic valve IE allows for more tailored treatment. Surgery may be necessary in complex cases (e.g., valve perforation). IE prophylaxis is recommended in specific circumstances (e.g., in patients with congenital heart disease undergoing certain dental procedures). IE is typically fatal if left untreated.
Etiology
Typical pathogens in IE [1]
The identification of one of the following typical pathogens on blood culture may indicate IE.
All patients
-
Staphylococcus
- S. aureus
- S. lugdunensis
- Enterococcus faecalis
- All Streptococcus spp. (except S. pneumoniae and S. pyogenes)
- Granulicatella spp.
- Abiotrophia spp.
- Gemella spp.
-
HACEK group
- Haemophilus spp.
- Aggregatibacter actinomycetemcomitans
- Cardiobacterium hominis
- Eikenella corrodens
- Kingella kingae
Patients with intracardiac prostheses
- Coagulase-negative staphylococci
-
Corynebacterium
- C. striatum
- C. jeikeium
- Serratia marcescens
- Pseudomonas aeruginosa
- Cutibacterium acnes
- Nontuberculous mycobacteria (particularly Mycobacterium chimaerae)
- Candida spp.
Causes of blood culture-negative IE [2]
Blood culture-negative IE is most commonly caused by antibiotic use before blood sample collection but can be due to pathogens that are difficult to culture. Selected pathogens are listed below.
- Brucella spp.
- Bartonella spp.
- Coxiella burnetii
- Fungi (e.g., Aspergillus spp.)
- Legionella spp.
- Mycoplasma spp.
- Tropheryma whipplei
Specifics of selected pathogens
| Characteristics of selected causes of infective endocarditis | |
|---|---|
| Pathogen | Characteristics |
| Staphylococcus aureus |
|
| Viridans streptococci |
|
| Staphylococcus epidermidis |
|
| Enterococci (especially Enterococcus faecalis) |
|
| Streptococcus gallolyticus subsp. gallolyticus (Sgg) [7] |
|
| Gram-negative HACEK group |
|
| Fungal endocarditis (Candida, Aspergillus fumigatus) [9][10] |
|
| Coxiella burnetii Bartonella species |
|
Risk factors for infective endocarditis [3][6][12]
-
Demographics
- Male sex
- Age > 60 years
-
Cardiac conditions
- Acquired valvular disease (e.g., rheumatic heart disease, aortic stenosis, degenerative valvular disease)
- Prosthetic heart valves
- Congenital heart defects (e.g., VSD, bicuspid aortic valve)
- Previous IE
- Cardiac implantable electronic device (CIED) [6]
-
Noncardiac risk factors
- Poor dental status
- Dental procedures
- Nonsterile venous injections (e.g., in IV drug use)
- Intravascular devices
- Surgery
- Chronic hemodialysis
- Immunocompromise (e.g., HIV infection, diabetes)
- Other bacterial infections (e.g., UTIs, spondylodiscitis, periodontal infection)
- See also “Risk factors for IE in children.”
Pathophysiology
-
Pathogenesis [3]
- Damaged valvular endothelium → exposure of the subendothelial layer → adherence of platelets and fibrin → sterile vegetation (microthrombus)
- Localized infection or contamination → bacteremia → bacterial colonization of vegetation → formation of fibrin clots encasing the vegetation → valve destruction with loss of function (valve regurgitation) [13]
-
Valve involvement [12]
- Frequency of valve involvement: mitral valve > aortic valve > tricuspid valve > pulmonary valve
- The tricuspid valve is the most commonly affected valve in individuals who inject drugs (associated with Pseudomonas, S. aureus, and Candida).
-
Clinical consequences [3][13]
- Bacterial vegetation → bacterial thromboemboli → vessel occlusion → infarctions
- Emboli can lead to metastatic infections of other organs.
- Formation of immune complexes and antibodies against tissue antigens → glomerulonephritis, Osler nodes
“Don't tri drugs for the sake of your tricuspid valves.”


Coronal section of the heart; frontal view
There is bacterial colonization on the mitral valve.
© AMBOSS
Clinical features

Constitutional symptoms [3][14]
- Fever and chills (seen in ∼ 90% of patients) [3]
- Tachycardia
- General malaise, weakness, weight loss, night sweats
- Dyspnea, cough, pleuritic chest pain
- Arthralgias, myalgias
Patients with subacute IE often present with nonspecific flu-like symptoms, while patients with acute IE often present with signs of acute sepsis.
A high index of suspicion is required in patients with risk factors for IE, as classic extracardiac manifestations (e.g., splinter hemorrhages, Janeway lesions) are absent in the majority of patients. [8][15]
Cardiac manifestations [3][14]
-
Development of a new heart murmur or change in a preexisting murmur (seen in ∼ 75% of patients) [3];
-
Tricuspid valve regurgitation
- Holosystolic murmur that is loudest at the left sternal border
- Seen in individuals who inject drugs, immunocompromised individuals, patients with congenital heart disease, and patients with instrumentation in the right heart (e.g., central venous catheters) [4]
- Aortic valve regurgitation: early diastolic murmur that is loudest at ; the left 3rd and 4thintercostal spaces and along the left sternal border [6]
- Mitral valve regurgitation: holosystolic murmur that is loudest at the heart's apex and radiates to the left axilla
-
Tricuspid valve regurgitation
- Heart failure (e.g., dyspnea, lower limb edema) due to valve insufficiency
- Arrhythmias: Suspect a perivalvular abscess in patients with IE who develop a new conduction abnormality (e.g., heart block). [16]


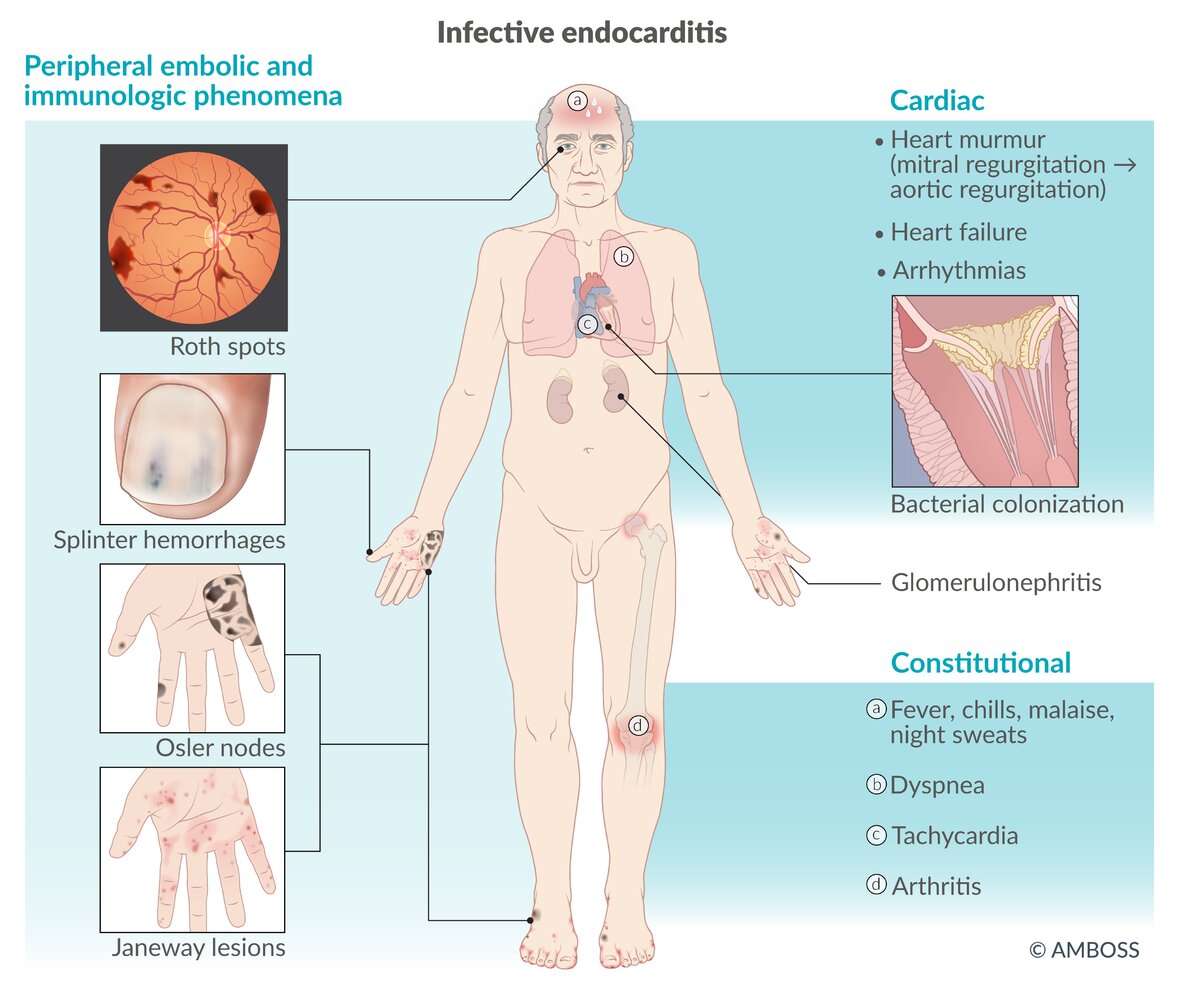
Extracardiac manifestations of IE [3][14]
Extracardiac manifestations are typically caused by septic microemboli and/or immune complex precipitation and are more commonly seen in left-sided IE, with the exception of pulmonary embolic manifestations, which are more common in right-sided IE. [3][17]
-
Peripheral embolic and immunologic phenomena of IE: seen in only 5–10% of patients. [3][17]
- Petechiae, especially splinter hemorrhages (hemorrhages underneath fingernails)
-
Janeway lesions
- Small, nontender, erythematous macules on palms and soles
- Microabscesses with neutrophilic capillary infiltration and areas of hemorrhage caused by septic microemboli from valve vegetations
- Osler nodes: painful nodules on pads of the fingers and toes caused by immune complex deposition
- Roth spots: round retinal hemorrhages with pale centers
-
Emboli to intraabdominal organs
-
Acute renal injury
- Including hematuria and anuria
- Due to renal artery occlusion or glomerulonephritis
-
Splenomegaly and possible LUQ pain
- Due to splenic artery occlusion or splenic abscess
- May lead to splenic rupture [18]
-
Acute renal injury
- Neurological manifestations: (e.g., seizures, paresis): due to septic embolic stroke, hemorrhage, meningitis, encephalitis, and/or abscess [19][20]
-
Pulmonary manifestations: caused by septic emboli resulting from tricuspid valve involvement
- Signs of pulmonary embolism (e.g., dyspnea)
- Signs of pulmonary infection, e.g., multifocal pneumonia, lung abscess, and/or empyema. [21]
- Others: Arthritis
Up to one-third of patients with left-sided IE present with symptoms of stroke. [20]
IE should always be considered as a cause of fever of unknown origin (FUO), especially in the presence of a new heart murmur.
“FROM JANE:” Features of IE include Fever, Roth spots, Osler nodes, Murmur, Janeway lesions, Anemia, Nail bed hemorrhage, and Emboli.




© AMBOSS
© AMBOSS
© AMBOSS

The vertical hemorrhages (arrowheads) underneath this patient's fingernails are most commonly caused by trauma but can also occur as a result of immune complex deposition or microthrombosis in subacute, infective endocarditis, SLE, or rheumatoid arthritis.
Source: "Splinter hemorrhage", Splarka, Wikimedia Commons licensed under Public Domain
{kind=link}

Multiple erythematous macules are visible on the thenar eminence and the base of the thumb.
These Janeway lesions are typically caused by septic microembolisms secondary to infective endocarditis.
Source: “Janeway lesion” by Warfieldian, Wikimedia Commons, licensed under CC BY-SA 4.0.
{kind=link}

There are multiple raised nodular lesions on the palm and palmar aspects of the first and second digits. The lesions appear dark brown, indicating subcutaneous hemorrhages.
This is the typical appearance of Osler nodes.
Source: “Osler Nodules Hand” by Roberto J. Galindo, Wikimedia Commons, licensed under CC BY-SA 4.0.
{kind=link}
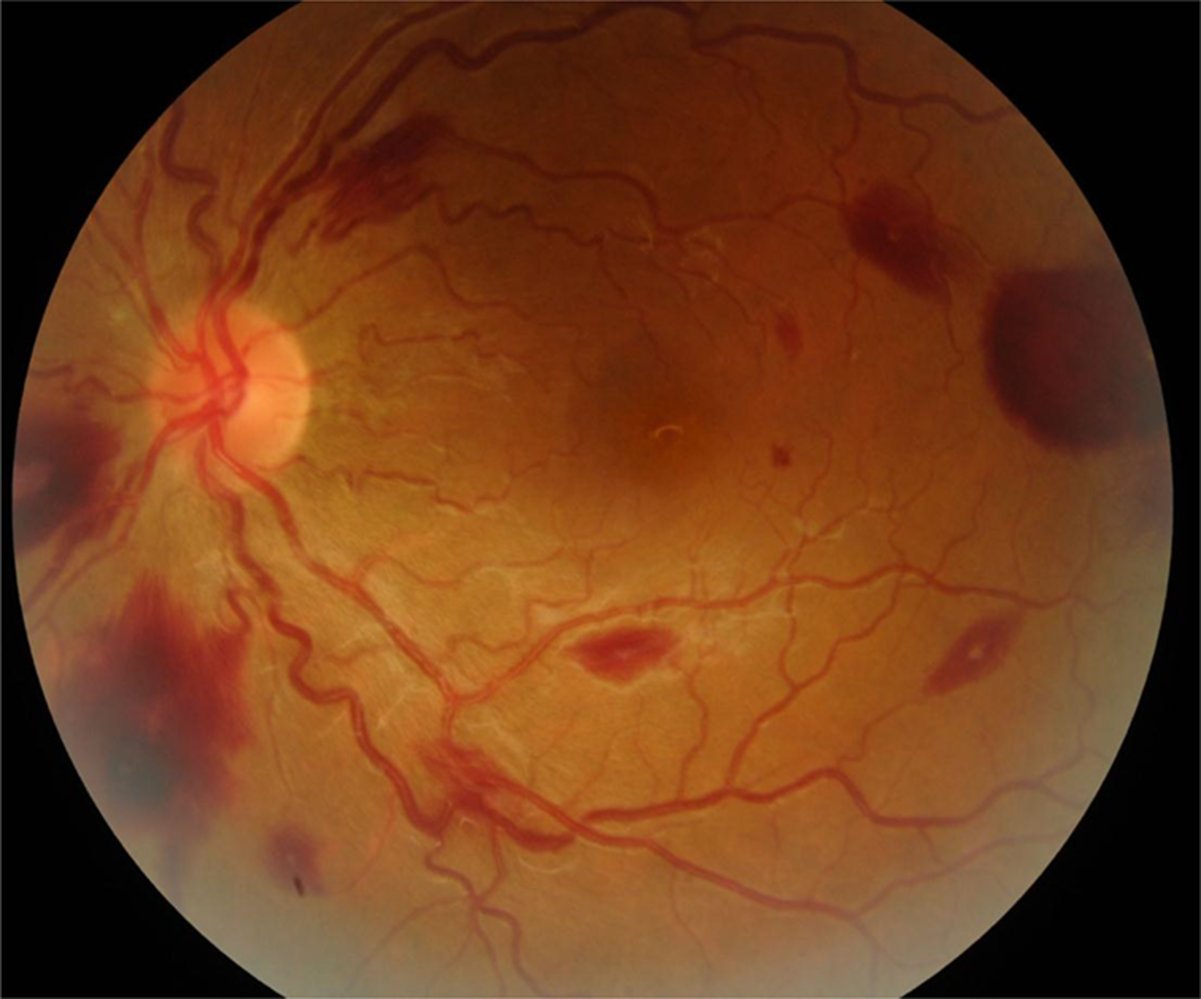
Fundus photography of a left eye
There are multiple red, white-centered lesions, which reflect small retinal hemorrhages with central accumulation of leukocytes or fibrin thrombocyte emboli (examples indicated by arrowheads).
Although these findings were formerly considered to be associated almost exclusively with infective endocarditis, they may actually occur in a variety of conditions, including hypertensive, diabetic, and HIV-related retinopathy; leukemia; and intracranial hemorrhage.
Circle: optic disc; M= macula
Source: “Figure 1. in: Ocular Manifestations of Endocarditis” by M.D. Cheima Wathek, InTechOpen, licensed under CC BY 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
Classification
- IE can be classified by:
- Type of affected valve (native vs. prosthetic)
- Acuity of the infection
- Location of the infection (left- vs. right-sided)
- Although this is not a definitive classification system, it can help in the approach to management and selection of empiric antibiotic regimens.
Classification by valve type and duration of infection
| Classified by type of valve involved and clinical course [17] | |||
|---|---|---|---|
| Native valve endocarditis | Prosthetic valve endocarditis | ||
| Acute bacterial endocarditis | Subacute bacterial endocarditis | ||
| Clinical features |
|
|
|
| Main pathogens |
|
|
|
| Affected valves |
|
|
|
Classification by location
| Classified by location of valves involved | ||
|---|---|---|
| Right-sided endocarditis [22] | Left-sided endocarditis [17] | |
| Distinguishing clinical features |
|
|
| Main pathogens |
|
|
| Affected valves |
|
|
Diagnosis
Approach [17][23]
- Suspect IE in patients with clinical features (e.g., fever of unclear etiology and a new heart murmur) and predisposing conditions.
-
Use the 2023 Duke-ISCVID criteria to determine the diagnostic likelihood of IE: definite, possible, or rejected. [8]
- Intended as a diagnostic guide and not a substitute for clinical judgment
- Incorporates clinical, microbiological, pathological, and imaging criteria
- Order echocardiography and multiple sets of blood cultures for all patients.
- Obtain ECG and additional imaging to investigate complications, new focal symptoms, and/or signs of metastatic infection.
- Consider serology to evaluate for blood culture-negative endocarditis.
- Consult infectious diseases if there is diagnostic uncertainty.
Draw three sets of blood cultures from different venipuncture sites as soon as IE is suspected, preferably before initiating antibiotic treatment.
Duke criteria
| 2023 Duke-ISCVID criteria [1] | ||
|---|---|---|
| Criteria | Findings | |
| Pathological |
|
|
| Clinical | Major |
|
| Minor |
|
|
| Interpretation |
|
|
The modified Duke criteria were revised in 2023 to improve diagnostic sensitivity for IE and have now been replaced by the 2023 Duke-ISCVID criteria.
Laboratory studies [17]
Routine studies [2]
Laboratory findings are nonspecific but may be used to assess disease severity.
- CBC: : leukocytosis (may show left shift), leukopenia, anemia, and/or thrombocytopenia
- Inflammatory markers: : ↑ CRP, ↑ ESR [23]
- CMP: Elevated creatinine and liver chemistries indicate end organ damage.
- Serum lactate: may be elevated
- Cardiac biomarkers: Troponin and BNP may be elevated. [24]
- Urinalysis: Hematuria and/or nephritic sediment may be present. [15][25]
Blood cultures [26]
-
Blood sample collection
- Before treatment: three sets of bacterial cultures from different venipuncture sites
- During treatment: two sets from separate venipuncture sites every 24–48 hours until bacteremia resolves
-
Interpretation
- Positive cultures are interpreted using the 2023 Duke-ISCVID criteria.
- Negative cultures cannot rule out IE as any of the following may produce a negative result: [8][26][27]
- Antibiotic therapy before blood culture sampling
- Fastidious bacteria (most commonly C. burnetii or Bartonella spp.) [15]
- Fungal infection
- Noninfective endocarditis
Negative blood cultures cannot rule out IE since some patients with IE have sterile cultures.
Echocardiography [1][2][17]
Transthoracic echocardiography (TTE) is the initial test of choice for all patients with suspected IE. TTE should ideally be performed within 12 hours of presentation and if new complications are suspected. Transesophageal echocardiography (TEE) is more invasive and should be considered in selected cases. [2]
-
Indications for TEE include:
- Presence of high-risk features
- TTE findings inconclusive or suggestive of IE [2]
- Patients due to undergo surgery
- Concern for intracardiac complications (e.g., abscess)
- Selected patients based on detected pathogens (e.g., S. aureus, E. faecalis, Streptococcus spp.)
-
Findings of IE on echocardiogram: 2023 Duke-ISCVID imaging major criteria have expanded on the modified Duke major criteria. ; [8][28][29]
- Valvular vegetations: hyperechoic mobile masses located on the valve, mural endocardium, or prosthetic material [30]
- Abscess (e.g., perivalvular abscess )
- New valvular regurgitation (especially in patients with valve prolapse, perforation, and/or destruction)
- New partial prosthetic valve dehiscence
- Valvular or leaflet aneurysm or perforation
- Pseudoaneurysm
- Intracardiac fistula
TEE is more sensitive (∼ 90%) than TTE (∼ 75%) and is more reliable for ruling out IE in patients with moderate to high pretest probability.
Additional studies for IE [17][26]
-
Serology
- To assess for culture-negative endocarditis, e.g.:
- C. burnetii anti-phase I IgG titer (> 1:800)
- B. henselae or B. quintana IgG titer (≥ 1:800)
- Limitations: cross-reactivity between different pathogens, confounding from prior infections
- To assess for culture-negative endocarditis, e.g.:
- Molecular testing (e.g., PCR, RNA sequencing): to assess for culture-negative endocarditis (e.g., due to C. burnetii, Bartonella spp., T. whipplei)
-
Tissue sampling (after surgery)
- Histopathology of resected valves (gold standard) [26][31]
- Gram stain and culture: to plan the duration of postoperative antimicrobial therapy [26]
- Molecular testing (e.g., T. whipplei PCR) [31]
- ECG: indicated in all patients to assess for complications (e.g., AV block or bundle branch blocks in paravalvular extension) [8][23]
- Dental assessment: in all patients receiving treatment for IE regardless of the initial source of bacteremia
- Colonoscopy: in patients with bacteremia due to S. gallolyticus to rule out colon cancer and mucosal lesions
Obtain an ECG in all patients with suspected IE to assess for new conduction abnormalities that indicate a perivalvular or myocardial abscess (e.g., AV block, bundle branch block). If present, consider urgent cardiac imaging (e.g., TEE, cardiac MRI). [8][23]
Imaging
Additional imaging may be performed if echocardiography is inconclusive and in selected patients to assess for complications.
-
Cardiac CTA [2]
- Consider in possible IE for diagnostic confirmation and/or assessment of valvular lesions.
- Consider in native or prosthetic valve IE to assess for paravalvular or periprosthetic complications if TTE and TEE are inconclusive.
- 18F-FDG PET/CT: Consider to evaluate for IE in patients with a prosthetic valve. [32][33][34]
- CXR: The presence of multiple pulmonary infiltrates may suggest right-sided IE. [15]
- Abdominal ultrasound: if splenic abscess or infarction is suspected
- MRI head: Consider to assess for intracranial septic emboli.

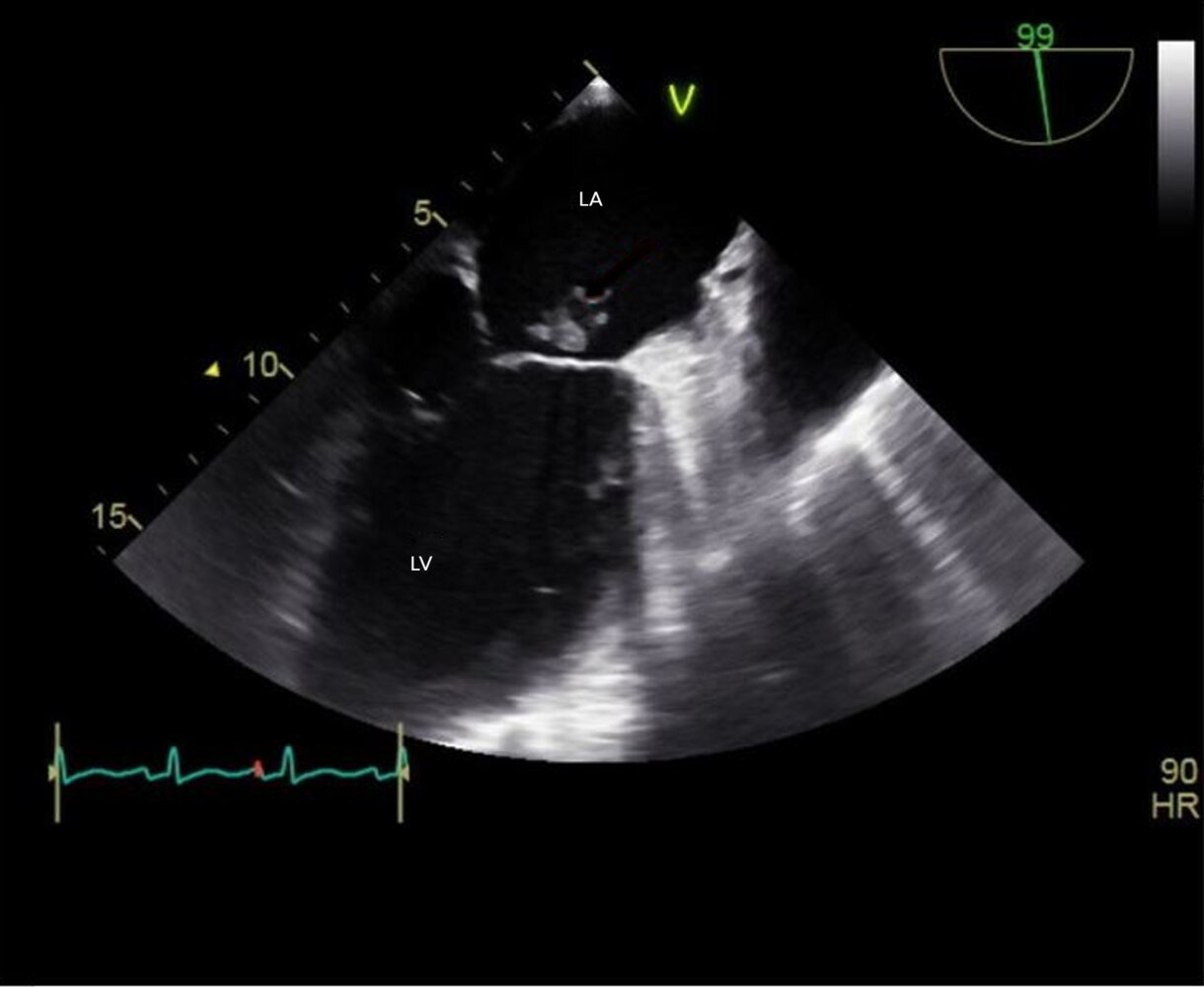
Echocardiography (transesophageal; mid esophageal two-chamber view)
An irregularly shaped vegetation (red overlay) is seen on the mitral valve (green overlay).
LA: left atrium; LV: left ventricle
Source: “Figure 1, in: Infective Endocarditis Manifesting as Severe Elevation in Serum Aminotransferases in the Absence of Severe Tricuspid Regurgitation, Heart Failure, or Shock: A Diagnostic Challenge” by Amaratunga E A, Hoggard J A, Kamau J, Ernst E B, Chalunkal M, Snyder R, Cureus, licensed under CC BY 4.0. Modifications: -Image was cropped, letter "A" in the top left corner was removed -FXV: Red arrow removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
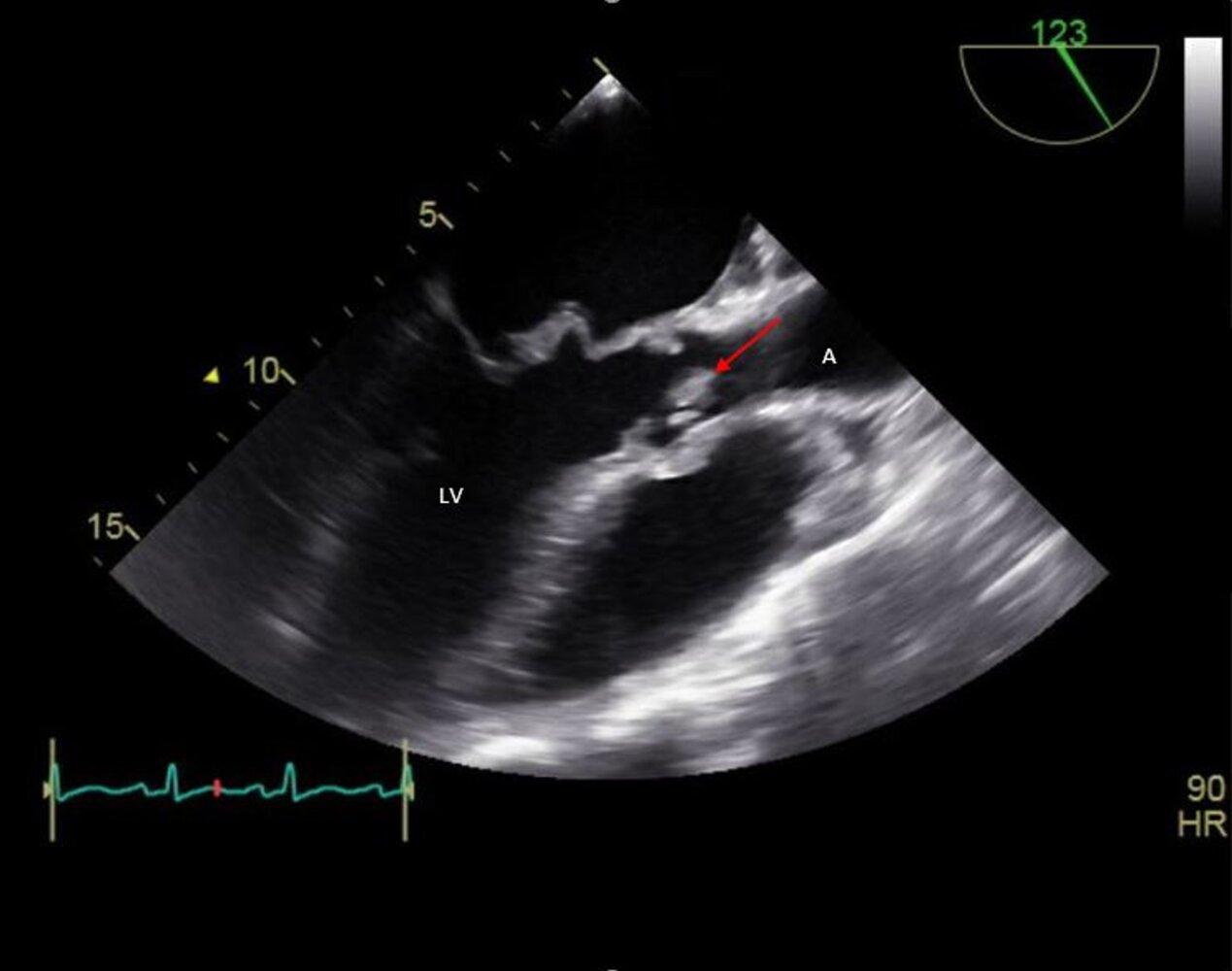
Echocardiography (transesophageal; mid esophageal long axis view)
A vegetation (red arrow) is seen as an echogenic structure on the right coronary cusp (green overlay) of the aortic valve.
A: aorta; LA: left atrium; LV: left ventricle; RV: right ventricle
Source: “Figure 1, in: Infective Endocarditis Manifesting as Severe Elevation in Serum Aminotransferases in the Absence of Severe Tricuspid Regurgitation, Heart Failure, or Shock: A Diagnostic Challenge” by Amaratunga E A, Hoggard J A, Kamau J, Ernst E B, Chalunkal M, Snyder R, Cureus, licensed under CC BY 4.0. Modifications: Image was cropped, letter "B" in the top left corner and letter "V" were removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
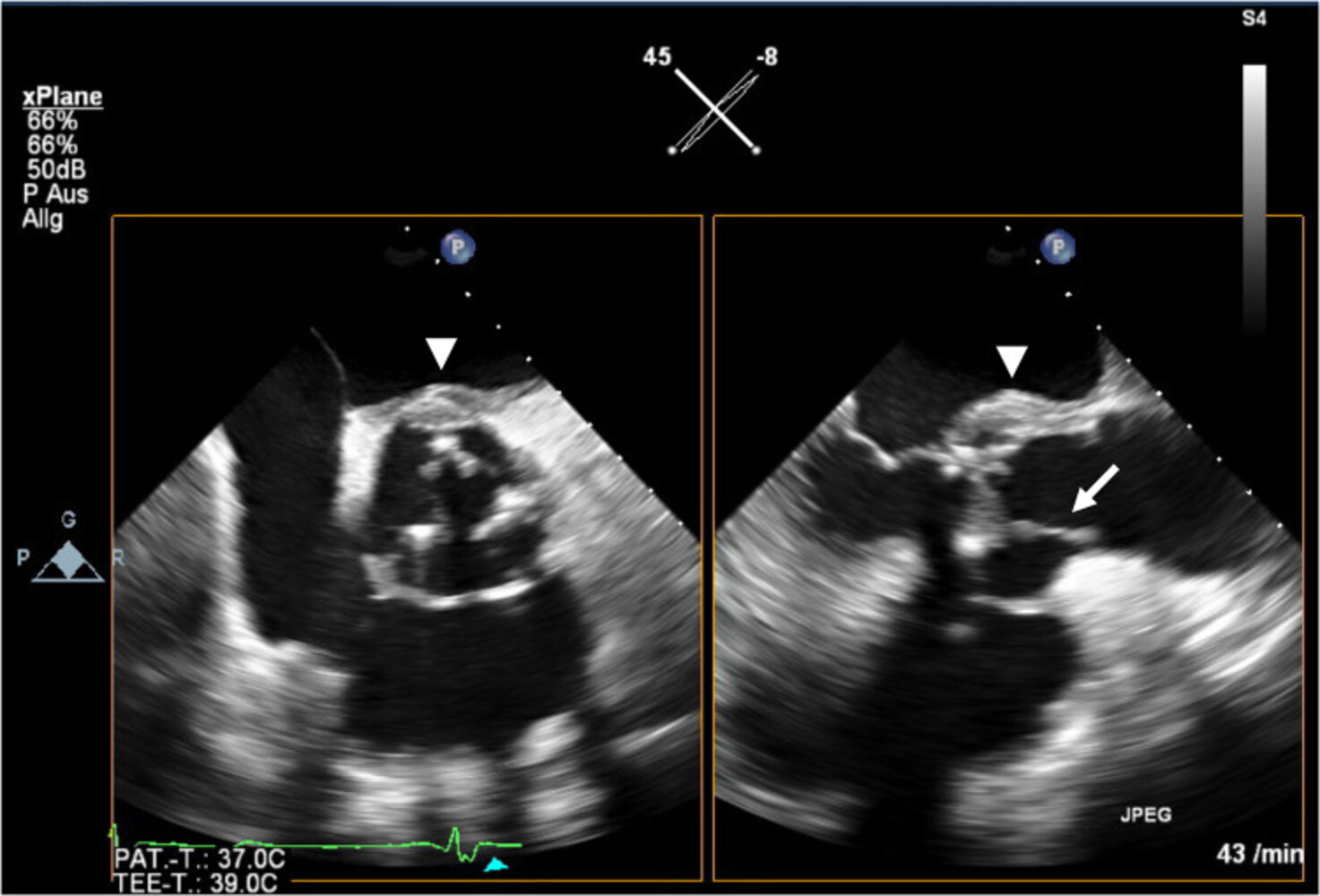
Echocardiography (transesophageal; biplane mid-esophageal) of patient with aortic valve bioprosthesis, fever, chest discomfort, and increasing shortness of breath
A mobile hyperechoic mass on the aortic valve (arrow) is suspicious for infectious endocarditis. Additional hyperechoic perivalvular thickening (arrowhead) suggests the presence of a valve ring abscess.
Ao: aorta; IAS: interatrial septum; LA: left atrium; LV: left ventricle; MV: mitral valve; RA: right atrium; RV: right ventricle; TV: tricuspid valve
Source: “Fig 2, In: Case report: takotsubo syndrome in infectious endocarditis” by Rattka M, Gundlach J, Rottbauer W, Keßler M, SpringerLink, licensed under CC BY 4.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
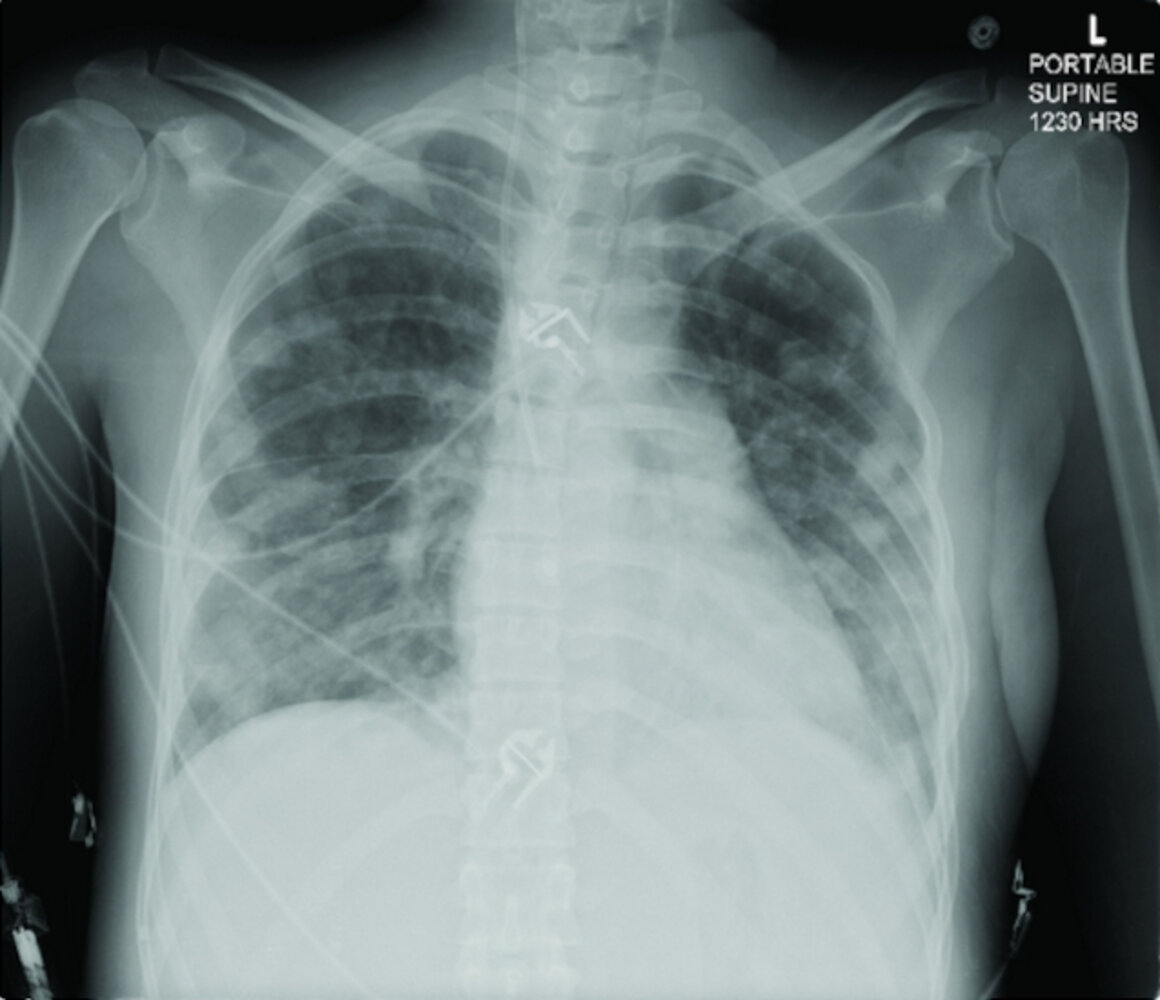
X-ray chest (supine) of a 24-year-old patient with history of intravenous drug use and septic emboli
Numerous pulmonary nodules are present in both lungs (examples indicated by green overlay). Some nodules have lucent centers indicating cavitation (examples indicated by red overlay). Air-space opacities, which were better appreciated on a subsequent CT scan (not shown), obscure the margins of some nodules.
The cardiac silhouette appears prominent as a result of rotation of the patient to the left.
The differential diagnosis of causes of multiple cavitary lung nodules includes bacterial, tuberculous, fungal, and parasitic infections as well as several noninfectious causes (e.g., rheumatic diseases and malignancies).
Arrowheads: thoracic spine spinous processes; dashed lines: medial clavicles; yellow overlay: right central line
Source: “Fig 2, In: Daptomycin Failure for Treatment of Pulmonary Septic Emboli in Native Tricuspid and Mitral Valve Methicillin-Resistant Staphylococcus aureus Endocarditis” by Zainah A, Zervos M, Stephane W et al., Hindawi, licensed under CC BY 3.0. Modifications: image cropped. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
Pathology
- Acute disease (leading to valve insufficiency, septic embolic infarcts, tendinous cord rupture) [35]
- Erosion → fibrin deposits on valves
- Ulceration
- Perforation
- Chronic disease (leading to valve insufficiency and valve stenosis) [35]
- Erosion → reorganization of fibrin layer
- Granulation tissue → valve scarring/fibrosis
- Calcification → thickened and/or shortened tendinous cords



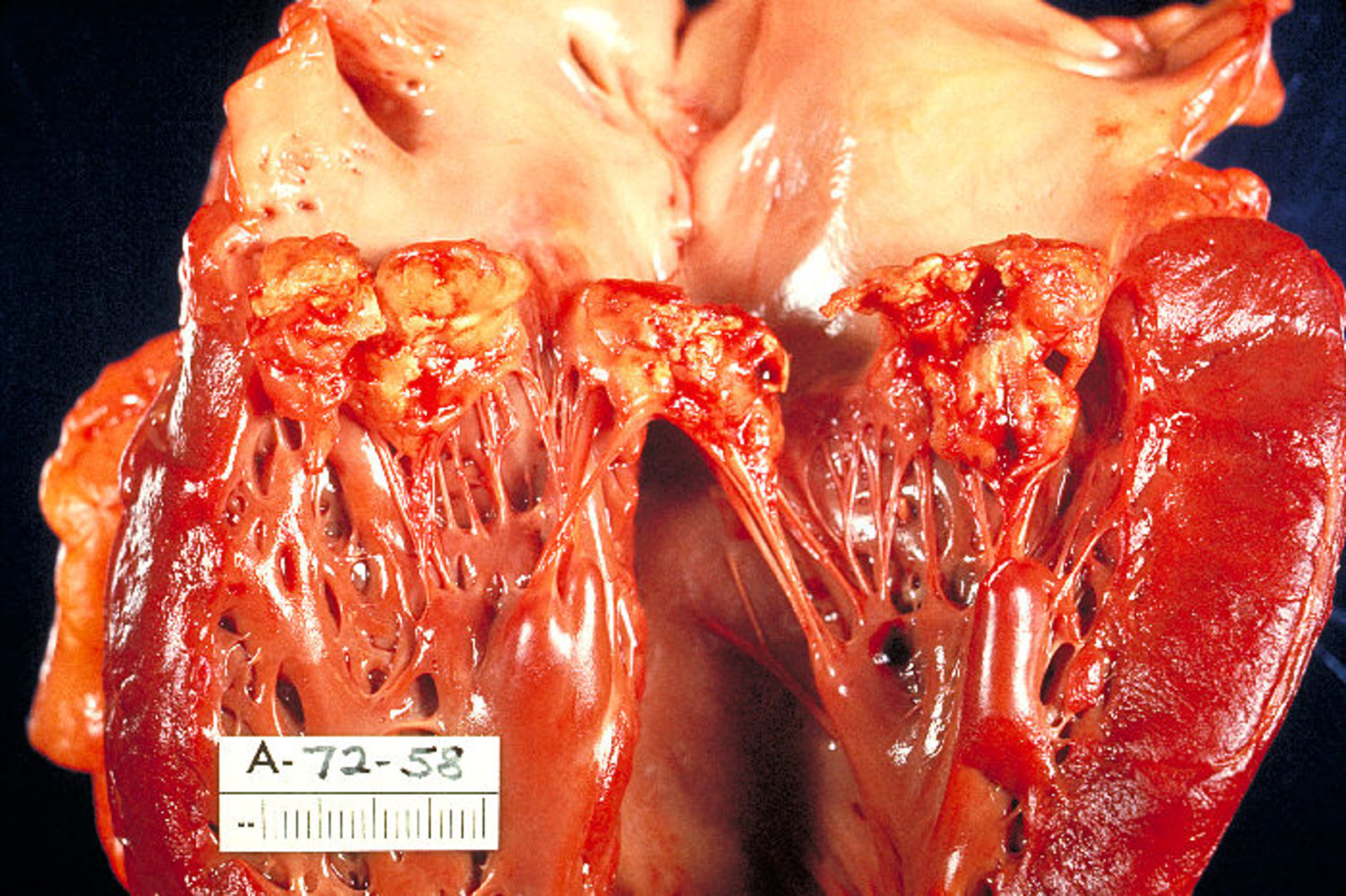
Photograph of a dissected heart specimen opened to show the endocardial aspect of left atrium and ventricle
The mitral valve is thickened (indicated by arrow) and shows numerous yellow vegetations on the atrial (superior) aspect of the valve (examples indicated by arrowheads).
This gross appearance is typical of infective endocarditis of the mitral valve.
Source: "ID#: 851", Centers for Disease Control and Prevention, Centers for Disease Control and Prevention licensed under Public Domain
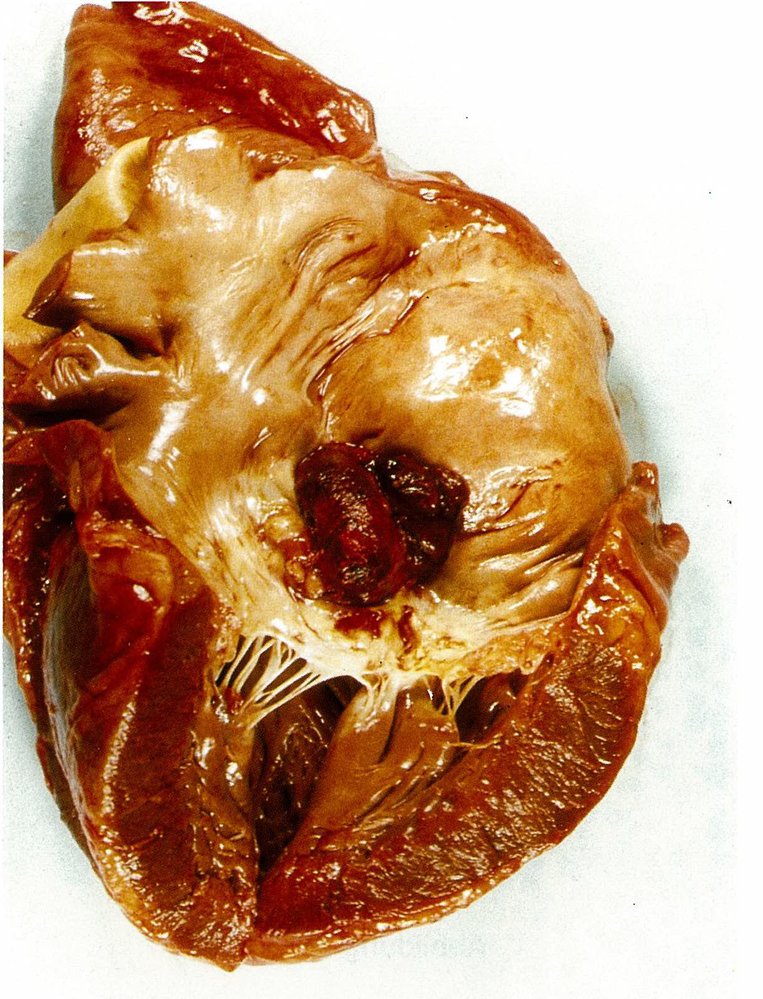
Left heart autopsy specimen (left ventricle opened longitudinally) from a patient who had a stroke
The mitral valve (blue overlay) shows ulcerations of valve leaflets (arrowheads) and two thrombi (dashed outline) protruding into the left atrium. The myocardium of the left ventricle (dimension line) appears normal with no signs of infarction.
Source: © IMPP
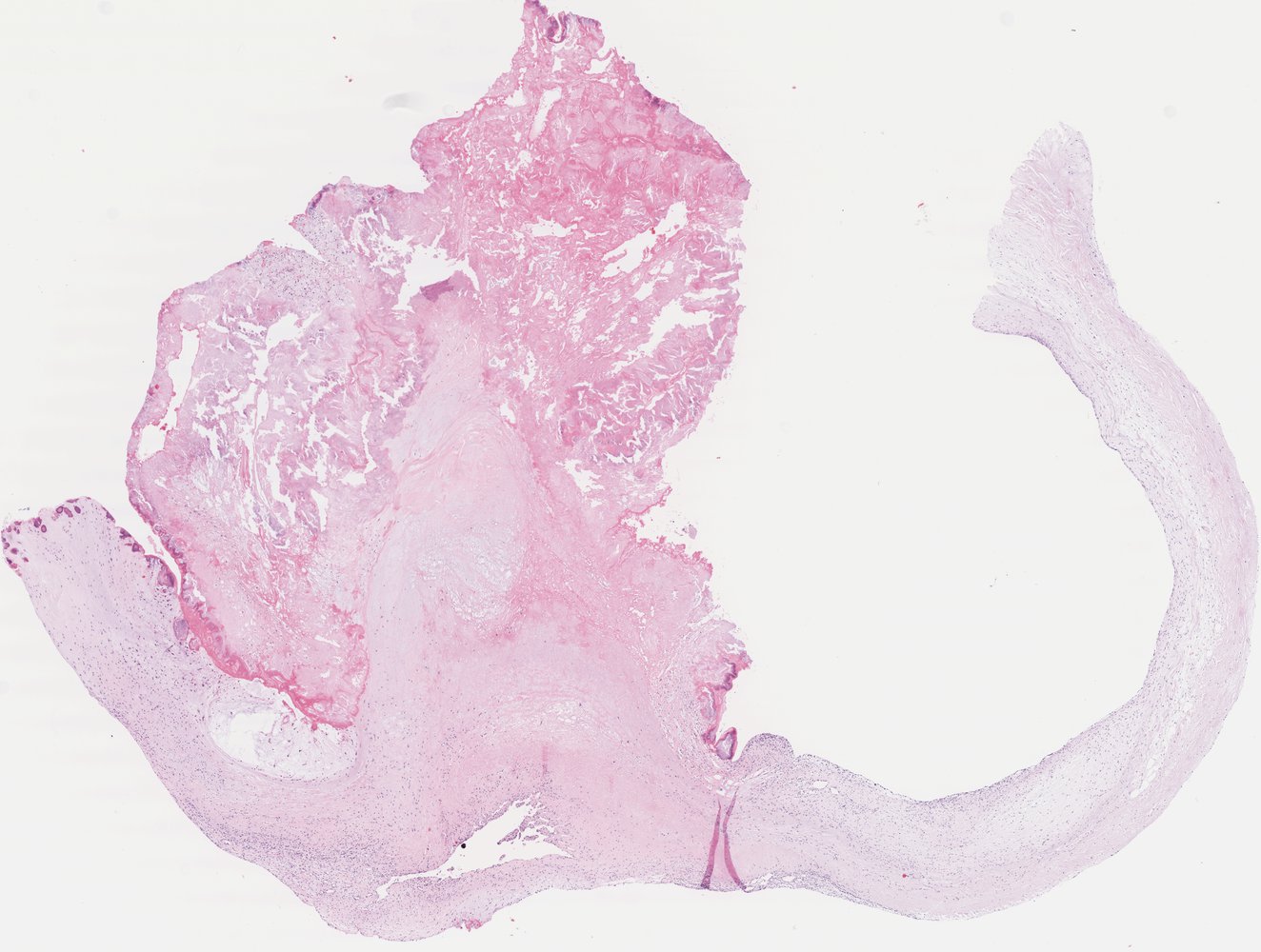
Click on the Smartzoom button to view the entire specimen through a virtual microscope.
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: PD Dr. Alberto Perez Bouza
Differential diagnoses
Noninfective endocarditis (nonbacterial thrombotic endocarditis) [36][37]
-
Description
- Rare, noninfective form of endocarditis due to sterile platelet thrombus formation on the heart valves (usually mitral and aortic valves)
- Libman-Sacks endocarditis: a type of noninfective endocarditis with verrucous vegetations in individuals with systemic lupus erythematosus or antiphospholipid syndrome [36]
-
Etiology
- Malignancy (e.g., pancreatic adenocarcinoma)
- Hypercoagulable states
- Underlying trauma (e.g., from indwelling vascular catheters)
- Previous rheumatic fever
- Autoimmune conditions (e.g., systemic lupus erythematosus, rheumatoid arthritis, antiphospholipid syndrome) [38]
- Chronic infections (e.g., TB, pneumonia, osteomyelitis)
-
Clinical features
- Valves and cardiac function are rarely impaired.
- Compared to IE, vegetations are easily dislodged and embolization is common, leading to hemorrhages under the nails, skin, and retina
- Most affected individuals are asymptomatic until embolization occurs.
-
Diagnostics
- Negative blood cultures
- Echocardiography: valve vegetations
-
Biopsy (definitive diagnosis)
- Sterile vegetations on either surface of the valve composed of immune complexes, mononuclear cells, and thrombi interwoven with fibrin strands
- Not always feasible, therefore diagnosis is mostly made based on clinical findings, negative blood cultures, echocardiography findings, and no response to antibiotic treatment
-
Treatment
- Anticoagulation with heparin
- Treatment of the underlying condition
Other
- Intravascular catheter infection
- Infection of prosthetic implants (e.g., prosthetic valves, joints, cardiac electronic devices)
- Prosthetic valve thrombosis
- Hematogenous osteomyelitis
- Septic thrombophlebitis
The differential diagnoses listed here are not exhaustive.
Treatment
Initial management [8][17][32][39]
- Unstable patients: Use the ABCDE approach and initiate management of sepsis as needed.
-
Consults [40]
- Consult infectious diseases (ID) early to plan treatment and consider empiric therapy.
- Identify patients with indications for surgery consult in IE.
-
Antibiotic therapy
- Start empiric antibiotic therapy for IE once blood cultures have been sampled. [8][39]
- Switch to targeted antibiotic therapy for IE once blood culture results are available. [8][39]
- Supportive care: Treat urgent complications (e.g., AHF, heart block) and the underlying cause (e.g., removal of infected central lines).
If IE is suspected, first obtain blood cultures, then consult ID to plan empiric antibiotic therapy. When culture results are available, adapt the therapy accordingly.
Antibiotics
Empiric antibiotic therapy for IE [17][41]
The goal of empiric antibiotic therapy is to provide broad-spectrum coverage for potential bacterial causes of IE (including multidrug-resistant organisms) until blood culture results are available.
- Choice of empiric agents: Consult infectious diseases and consider patient and disease factors as well as local and individual flora and resistance patterns (see “Risk factors for IE” and “Classification”).
-
Example regimen [41]
- Vancomycin (off-label) OR daptomycin (off-label) [17][41]
- PLUS a beta-lactam (e.g., ceftriaxone OR cefepime (off-label) ) [17]
- PLUS gentamicin and rifampin in selected cases (e.g., prosthetic valve IE) in consultation with infectious diseases
Targeted antibiotic therapy [17]
Targeted antibiotic therapy based on culture and sensitivity results is recommended for all patients with IE.
-
Common targeted antibiotic regimens
-
Staphylococci
- Methicillin-susceptible staphylococci (e.g., MSSA): antistaphylococcal beta-lactam (e.g., nafcillin, oxacillin)
- Methicillin-resistant staphylococci (e.g., MRSA): vancomycin
- Prosthetic valve IE (≤ 1 year after placement): Add gentamicin PLUS rifampin.
- Viridans group streptococci: beta-lactam (e.g., penicillin G, ampicillin)
- Enterococci: combination therapy (e.g., ampicillin PLUS gentamicin)
- HACEK: ceftriaxone (first line)
-
Staphylococci
- Oral step-down therapy: After initial IV antibiotics, the course may be completed with oral antibiotics in selected patients in consultation with infectious diseases. [2][41]
- Duration of therapy: depends on various factors (e.g., drug regimen, affected valve) and may be continued for more than 2–6 weeks after the first sterile blood culture
- Blood culture-negative endocarditis: targeted therapy based on additional studies (e.g., serology)
| Initial targeted antimicrobial therapy for infective endocarditis [17] | ||
|---|---|---|
| Organism | Native valve endocarditis (common regimens) | Prosthetic valveendocarditis (common regimens) |
| Methicillin-susceptible staphylococci (e.g., MSSA) |
|
|
| Methicillin-resistant staphylococci (e.g., MRSA) |
|
|
| Viridans group streptococci and S. gallolyticus |
|
|
| Enterococcus spp. (penicillin-sensitive) |
|
|
| Enterococcus spp. (penicillin-resistant) |
|
|
| HACEK |
|
|
Surgery [2][17][40]
The decision to perform surgery is typically made by a multidisciplinary team comprising cardiology, cardiothoracic surgery, and infectious diseases.
-
Indications for surgery consult in IE include:
- Prosthetic valve IE
- Valve dysfunction causing heart failure
- Uncontrolled infection (e.g., enlarging vegetation, persistent bacteremia)
- Perivalvular extension or complications (e.g., abscess, pseudoaneurysm, fistula, heart block)
- IE due to difficult to treat organisms (e.g., fungi, MDRO)
- High embolic risk (e.g., mobile vegetation ≥ 10 mm, recurrent embolism) [2]
- Surgical options: valve replacement or valve repair (see “Treatment” in “Valvular heart diseases”)
-
Complications
- Acute surgical complications (e.g., rebleeding from surgical sites, coagulopathy, acute kidney injury, pneumonia)
- Cardiac complications (e.g., CHF, myocarditis, pericarditis, new AV block)
- Systemic emboli (e.g., stroke)
Surgery is required in 50–60% of patients with IE. [40]
Supportive care
-
Antithrombotic agents [17][32]
- Consider holding existing anticoagulation if CNS emboli are present.
- Continue long-term antiplatelet therapy if there is no bleeding
- Initiation of antithrombotic therapy is not routinely recommended.
- Cardiovascular complications: See “Acute heart failure management” and “Management of heart block.” [42]
-
Others
- Remove infected central lines and CIEDs [43][44]
- Treat opioid use disorder if present, e.g., in IV drug use. [45][46]
- Inpatient dental evaluation
Acute management checklist for suspected acute IE
Unstable patients
- Perform ABCDE survey.
- Begin treatment of complications causing hemodynamic instability, e.g.:
- Sepsis management
- Management of acute heart failure
- Management of bradycardia (e.g., due to heart block)
All patients
- Perform a clinical evaluation, e.g., cardiac surgical history, screening for extracardiac manifestations of IE.
- Establish IV access
- Draw 3 sets of blood cultures from different sites,
- Obtain routine laboratory studies (e.g., CBC, BMP).
- Order echocardiogram.
- Use the 2023 Duke-ISCVID criteria to categorize the diagnostic likelihood of IE.
- Obtain ECG and screen for new conduction abnormalities.
- Consult infectious diseases.
- Start empiric antibiotics for IE after blood samples are obtained.
- Screen for metastatic infections and consider confirmatory imaging (e.g., CXR, CT abdomen and pelvis, CT head).
- Identify patients with indications for surgery consult in IE.
- Switch to targeted antibiotic therapy for IE once blood culture results are available.
- Treat underlying conditions (e.g., remove infected central lines and CIEDs, treat opioid use disorder)
- Admit to hospital.
- Screen and monitor for complications (e.g., valvulopathy, AHF, perivalvular abscess, AV block, stroke, PE).
Complications
-
Cardiac complications
- New or worsened valvular regurgitation
- Partial dehiscence of a prosthetic valve [17]
- Congestive heart failure (most common cause of death in patients with infective endocarditis)
- Perivalvular abscess and fistula
- Myocarditis
- Conduction abnormalities: e.g., AV blocks
-
Embolic complications
- Systemic embolism in left-sided endocarditis: e.g., stroke, renal infarct, splenic infarct
- Pulmonary embolism in right-sided endocarditis
- Septic emboli and mycotic aneurysms
-
Metastatic infections: due to septic emboli or bacteremia
- Multifocal pneumonia, lung abscess
- Spondylodiscitis
- Splenic abscess
- Meningitis, brain abscess
- Acute kidney injury: Often multifactorial [6]
We list the most important complications. The selection is not exhaustive.
Prevention
Endocarditis prophylaxis [2][47][48][49]
Prophylaxis is indicated prior to certain procedures with a high risk of bacteremia in patients with high-risk cardiac features. [47]
-
Cardiac risk factors requiring IE prophylaxis (for procedures that may cause bacteremia)
- Presence of prosthetic cardiac valve or material
- History of endocarditis
- Certain types of congenital heart disease (CHD), e.g., unrepaired cyanotic CHD, repaired CHD (within 6 months of repair), repaired CHD with residual post-operative shunt or regurgitation
- Valvulopathy in cardiac transplant recipients [32][49]
-
Procedures requiring IE prophylaxis in patients at risk for IE
- Some dental procedures including tooth extraction and routine dental cleaning
- Any invasive procedure involving respiratory tract or infected tissue (e.g., abscess drainage)
- Placement of a CIED [44][50]
- Surgical placement of prosthetic cardiac or intravascular material (e.g., heart valve, intravascular graft) [50]
-
Common regimens (usually administered 30–60 minutes prior to the procedure) [32]
-
Prior to dental procedures [47][51]
- No penicillin allergy: amoxicillin (off-label) OR ampicillin (off-label) OR cefazolin (off-label for children)
- Severe penicillin reaction: azithromycin; (off-label) OR doxycycline (off-label)
- Prior to CIED placement: cefazolin
- Pathogen-specific agents may be indicated depending on the site of the procedure. [32]
-
Prior to dental procedures [47][51]
IE prophylaxis is not routinely recommended prior to nondental procedures (including respiratory, skin, musculoskeletal, gastrointestinal, and genitourinary procedures) unless infected tissue is present. [32]
Special patient groups
Infective endocarditis in children [51][52]
Epidemiology [52]
- Incidence: approx. 0.05–0.12 cases per 1000 hospital admissions [52]
- 7.3% of pediatric IE occurs in neonates. [52]
Etiology [51][52]
-
Common pathogens in children [52]
- S. aureus
- Viridans streptococci [51]
- Enterococcus
- Coagulase-negative staphylococci
- Gram-negative bacteria
- Candida spp.
- Beta-hemolytic streptococci (e.g., S. pyogenes) [51]
-
Risk factors for IE in children [47][52]
- Congenital heart defects [52]
- Intravascular devices (e.g., central line)
- Previous cardiac surgery (e.g., prosthetic heart valves) [52]
- Rheumatic heart disease [52]
Dental procedures may cause transient bacteremia, but the risk for IE is very low. [52]
Clinical features [52]
-
Clinical features of IE are similar in adults and children, with the following exceptions:
- Older children: Arthritis is common.
- Infants: Septic emboli and neurological findings (e.g., seizures, hemiparesis) are common.
-
Neonates:
- Symptoms are nonspecific and similar to clinical features of neonatal bacterial infection
- Arthritis is uncommon.
- The classification of IE is the same in adults and children.
Peripheral embolic and immunologic phenomena of IE are uncommon in children. [52]
Diagnostics [52][53]
- Initial diagnostics for IE are similar in adults and children.
- The following studies are not routinely performed in children:
- Cardiac biomarkers
- Lactic acid
- Use the 2023 Duke-ISCVID criteria to help predict the likelihood of IE. [52]
- Obtain diagnostics for pediatric sepsis if signs of pediatric sepsis are present (obtain diagnostics for neonatal sepsis for all neonates with fever).
- If there is diagnostic uncertainty, consult a specialist (e.g., infectious diseases) for additional studies for IE.
Blood cultures are negative in up to 5% of children with IE. [52]
Treatment [51][52]
- Treatment of IE is similar to adults.
- Consult infectious diseases to direct antibiotic therapy; if not available, initiate empiric therapy, e.g.: [52]
- Ampicillin/sulbactam OR vancomycin
- PLUS gentamicin
- Nosocomial endocarditis : Add a cephalosporin (e.g., cefepime OR ceftazidime).
-
Prosthetic valve
- Add rifampicin.
- New valve (≤ 12 months): Also add a cephalosporin (e.g., cefepime OR ceftazidime).
- Transition to targeted antibiotic therapy based on culture and sensitivity results.
- Treatment typically lasts 4–6 weeks. [52]
- Clinically stable patients without complications : Consider continuing IV antibiotics on an outpatient basis in consultation with infectious diseases.
In well-appearing children whose blood cultures remain negative, continue monitoring for 48 hours before starting antibiotics, to allow for additional cultures to be obtained. [52]
Prevention [47][51]
- Prevention strategies are similar in adults and children; see “Endocarditis prophylaxis” for details.
- Encourage routine oral hygiene and dental care (see “Oral hygiene in children”). [52]
External Resources
- 2023 ISCVID Updating the Modified Duke Criteria
- 2023 ESC Guidelines for the Management of Endocarditis
- 2020 AHA/ACC Guideline for the Management of Patients With Valvular Heart Disease (AHA/ACC)
- 2015 AHA (endorsed by the IDSA) Guidelines on IE in Adults
- 2015 AHA Scientific Statement: Infective Endocarditis in Childhood
References
- Fowler VG, Durack DT, Selton-Suty C, et al. "The 2023 Duke-International Society for Cardiovascular Infectious Diseases Criteria for Infective Endocarditis: Updating the Modified Duke Criteria". Clin Infect Dis. 77(4). :518-526. (2023)
- Delgado V, Ajmone Marsan N, de Waha S, et al. "2023 ESC Guidelines for the management of endocarditis". Eur Heart J. 44(39). :3948-4042. (2023)
- Chambers HF, Bayer AS. "Native-Valve Infective Endocarditis.". N Engl J Med. 383(6). :567-576. (2020)
- Moss R, Munt B. "Injection drug use and right sided endocarditis". Heart. 89(5). :577–581. (2003)
- Murdoch DR. "Clinical Presentation, Etiology, and Outcome of Infective Endocarditis in the 21st Century". Arch Intern Med. 169(5). :463. (2009)
- Jameson JL, Fauci AS, Kasper DL, et al. "Harrison's Principles of Internal Medicine, Twentieth Edition (Vol.1 & Vol.2)". McGraw-Hill Education / Medical. (2018). ISBN: 9781259644030
- Abdulamir AS, Hafidh RR, Abu bakar F. "The association of Streptococcus bovis/gallolyticus with colorectal tumors: the nature and the underlying mechanisms of its etiological role". J Exp Clin Cancer Res. 30(1). :11. (2011)
- Cahill TJ, Prendergast BD. "Infective endocarditis". Lancet. 387(10021). :882-893. (2016)
- Arnold CJ, Johnson M, Bayer AS, et al. "Candida infective endocarditis: an observational cohort study with a focus on therapy". Antimicrob Agents Chemother. 59(4). :2365-2373. (2015)
- Tacke D, Koehler P, Cornely OA. "Fungal endocarditis". Curr Opin Infect Dis.. 26(6). :501-507. (2013)
- Kojic EM, Darouiche RO. "Candida infections of medical devices.". Clin Microbiol Rev. 17(2). :255-67. (2004)
- McDonald JR. "Acute infective endocarditis.". Infect Dis Clin North Am. 23(3). :643-64. (2009)
- Kasper DL, Fauci AS, Hauser SL, et al. "Harrison's Principles of Internal Medicine". McGraw-Hill Education. (2015). ISBN: 9780071802161
- Dhawan VK. "Infective Endocarditis in Elderly Patients". Clin Infect Dis. 34(6). :806-812. (2002)
- Long B, Koyfman A. "Infectious endocarditis: An update for emergency clinicians". Am J Emerg Med. 36(9). :1686-1692. (2018)
- Kang N, Wan S, Ng CS, Underwood MJ. "Periannular extension of infective endocarditis". Ann Thorac Cardiovasc Surg. 15(2). :74-81. (2009)
- Baddour LM, Wilson WR, Bayer AS, et al. "Infective Endocarditis in Adults: Diagnosis, Antimicrobial Therapy, and Management of Complications: A Scientific Statement for Healthcare Professionals From the American Heart Association". Circulation. 132(15). :1435-1486. (2015)
- Winearls JR, McGloughlin S, Fraser JF. "Splenic rupture as a presenting feature of endocarditis". European Journal of Cardio-Thoracic Surgery. 35(4). :737-739. (2009)
- Pruitt AA. "Neurologic Complications of Infective Endocarditis". Curr Treat Options Neurol. 15(4). :465-476. (2013)
- Bonaros N, Czerny M, Pfausler B, et al. "Infective endocarditis and neurologic events: indications and timing for surgical interventions". Eur Heart J Suppl. 22(Supplement_M). :M19-M25. (2020)
- Bui JT, Schranz AJ, Strassle PD, et al. "Pulmonary complications observed in patients with infective endocarditis with and without injection drug use: An analysis of the National Inpatient Sample". PLoS ONE. 16(9). :e0256757. (2021)
- Pierce D, Calkins BC, Thornton K. "Infectious endocarditis: diagnosis and treatment.". Am Fam Physician. 85(10). :981-6. (2012)
- Shiue AB, Stancoven AB, Purcell JB, et al. "Relation of Level of B-Type Natriuretic Peptide With Outcomes in Patients With Infective Endocarditis". Am J Cardiol. 106(7). :1011-1015. (2010)
- Majumdar A, Chowdhary S, Ferreira MAS, et al. "Renal pathological findings in infective endocarditis". Nephrol Dial Transplantation. 15(11). :1782-1787. (2000)
- Liesman RM, Pritt BS, Maleszewski JJ, Patel R. "Laboratory Diagnosis of Infective Endocarditis". J Clin Microbiol. 55(9). :2599-2608. (2017)
- Tattevin P, Watt G, Revest M, Arvieux C, Fournier P-E. "Update on blood culture-negative endocarditis". Med Mal Infect. 45(1-2). :1-8. (2015)
- Habib G, Badano L, Tribouilloy C, et al. "Recommendations for the practice of echocardiography in infective endocarditis". European Journal of Echocardiography. 11(2). :202-219. (2010)
- Bruun NE, Habib G, Thuny F, Sogaard P. "Cardiac imaging in infectious endocarditis". Eur Heart J. 35(10). :624-632. (2013)
- Evangelista A, Gonzalez-Alujas MT. "Echocardiography in infective endocarditis.". Heart. 90(6). :614-7. (2004)
- Subedi S, Jennings Z, Chen SC-A. "Laboratory Approach to the Diagnosis of Culture-Negative Infective Endocarditis". Heart Lung Circ. 26(8). :763-771. (2017)
- Habib G, Lancellotti P, Antunes MJ, et al. "2015 ESC Guidelines for the management of infective endocarditis". Eur Heart J. 36(44). :3075-3128. (2015)
- Pettersson GB, Coselli JS, Pettersson GB, et al. "2016 The American Association for Thoracic Surgery (AATS) consensus guidelines: Surgical treatment of infective endocarditis: Executive summary". J Thorac Cardiovasc Surg. 153(6). :1241-1258.e29. (2017)
- Hubers SA, DeSimone DC, Gersh BJ, Anavekar NS. "Infective Endocarditis: A Contemporary Review". Mayo Clin Proc. 95(5). :982-997. (2020)
- Thiene G, Basso C. "Pathology and pathogenesis of infective endocarditis in native heart valves.". Cardiovasc Pathol. 15(5). :256-263. (2006)
- Murtaza G, Iskandar J, Humphrey T, Adhikari S, Kuruvilla A. "Lupus-Negative Libman-Sacks Endocarditis Complicated by Catastrophic Antiphospholipid Syndrome.". Cardiol res. 8(2). :57-62. (2017)
- el-Shami K, Griffiths E, Streiff M. "Nonbacterial thrombotic endocarditis in cancer patients: pathogenesis, diagnosis, and treatment.". Oncologist. 12(5). :518-23. (2007)
- Asopa S, Patel A, Khan OA, Sharma R, Ohri SK. "Non-bacterial thrombotic endocarditis". European Journal of Cardio-Thoracic Surgery. 32(5). :696-701. (2007)
- Gould FK, Denning DW, Elliott TSJ, et al. "Guidelines for the diagnosis and antibiotic treatment of endocarditis in adults: a report of the Working Party of the British Society for Antimicrobial Chemotherapy". J Antimicrob Chemother. 67(2). :269-289. (2011)
- Cahill TJ, Baddour LM, Habib G, et al. "Challenges in Infective Endocarditis". J Am Coll Cardiol. 69(3). :325-344. (2017)
- McDonald EG, Aggrey G, Tarık Aslan A, et al. "Guidelines for Diagnosis and Management of Infective Endocarditis in Adults". JAMA Netw Open. 6(7). :e2326366. (2023)
- Brown RE, Chiaco JMC, Dillon JL, Catherwood E, Ornvold K. "Infective Endocarditis Presenting as Complete Heart Block With an Unexpected Finding of a Cardiac Abscess and Purulent Pericarditis". J Clin Med Res. 7(11). :890-895. (2015)
- Mermel LA, Allon M, Bouza E, et al. "Clinical practice guidelines for the diagnosis and management of intravascular catheter-related infection: 2009 Update by the Infectious Diseases Society of America". Clin Infect Dis. 49(1). :1-45. (2009)
- Baddour LM, Epstein AE, Erickson CC, et al. "Update on cardiovascular implantable electronic device infections and their management: a scientific statement from the American Heart Association.". Circulation. 121(3). :458-77. (2010)
- Jo Y, Nosal R, Vittori A, et al. "Effect of initiation of medications for opioid use disorder on hospitalization outcomes for endocarditis and osteomyelitis in a large private hospital system in the United States, 2014–18". Addiction. 116(8). :2127-2134. (2021)
- Kimmel SD, Walley AY, Li Y, et al. "Association of Treatment With Medications for Opioid Use Disorder With Mortality After Hospitalization for Injection Drug Use–Associated Infective Endocarditis". JAMA Netw Open. 3(10). :e2016228. (2020)
- Wilson WR, Gewitz M, Lockhart PB, et al. "Prevention of Viridans Group Streptococcal Infective Endocarditis: A Scientific Statement From the American Heart Association". Circulation. 143(20). (2021)
- Otto CM, Nishimura RA, Bonow RO, et al. "2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines". Circulation. 143(5). (2020)
- Wilson W, Taubert KA, Gewitz M, et al. "Prevention of Infective Endocarditis Guidelines From the American Heart Association". Circulation. (2007)
- Bratzler DW, Dellinger EP, Olsen KM, et al. "Clinical Practice Guidelines for Antimicrobial Prophylaxis in Surgery". Surg Infect (Larchmt). 14(1). :73-156. (2013)
- Committee on Infectious Disease, American Academy of Pediatrics. "Red Book: 2024-2027 Report of the Committee on Infectious Diseases, 33rd Edition". American Academy of Pediatrics. (2024). ISBN: 9781610027373
- Shmueli H, Thomas F, Flint N, et al. "Right‐Sided Infective Endocarditis 2020: Challenges and Updates in Diagnosis and Treatment". J Am Heart Assoc. 9(15). (2020)
- Baltimore RS, Gewitz M, Baddour LM, et al. "Infective Endocarditis in Childhood: 2015 Update: A Scientific Statement From the American Heart Association". Circulation. 132(15). :1487-515. (2015)
- Malik SB, Hsu JY, Hurwitz Koweek LM, et al. "ACR Appropriateness Criteria® Infective Endocarditis". J Am Coll Radiol. 18(5). :S52-S61. (2021)
- "Heart Valves and Infective Endocarditis". http://www.heart.org/HEARTORG/Conditions/More/HeartValveProblemsandDisease/Heart-Valves-and-Infective-Endocarditis_UCM_450448_Article.jsp#.WKGuAtIrLIW. [2016-05-01]
- Nishimura RA, Otto CM, Bonow RO, et al. "2014 AHA/ACC guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines". J Am Coll Cardiol. 63(22). :e57-185. (2014)
- Fournier PE, Casalta JP, Habib G, Messana T, Raoult D. "Modification of the diagnostic criteria proposed by the duke endocarditis service to permit improved diagnosis of q fever endocarditis". Am J Med. 100(6). :629-633. (1996)
- Habib G, Hoen B, Tornos P, et al. "Guidelines on the prevention, diagnosis, and treatment of infective endocarditis (new version 2009): the Task Force on the Prevention, Diagnosis, and Treatment of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) and the International Society of Chemotherapy (ISC) for Infection and Cancer.". Eur Heart J. 30(19). :2369-413. (2009)
- Lee A, Mirrett S, Reller LB, Weinstein MP. "Detection of Bloodstream Infections in Adults: How Many Blood Cultures Are Needed?". J Clin Microbiol. 45(11). :3546-3548. (2007)
- Werner M, Andersson R, Olaison L, Hogevik H. "A clinical study of culture-negative endocarditis.". Medicine. 82(4). :263-73. (2003)