Summary
Infertility is the inability to achieve pregnancy after 12 months of regular unprotected sexual intercourse in female individuals < 35 years of age and after 6 months in those ≥ 35 years of age, or the need for medically assisted reproduction to achieve pregnancy. Causes of female infertility include diminished ovarian reserve, ovulatory dysfunction, and tubal, pelvic, uterine, and cervical disorders. Causes of male infertility include male hypogonadism and sperm transport disorders. Diagnosis involves assessing both partners to determine the underlying causes and typically includes hormone tests to assess ovulatory function, imaging to evaluate for uterine abnormalities and tubal patency, and semen analysis. Management includes treatment of the underlying cause and often medically assisted reproduction, including ovulation induction, intrauterine insemination, and assisted reproductive technology (e.g., in vitro fertilization).
Definitions
-
Infertility is characterized by: [1]
-
An inability to achieve pregnancy despite regular unprotected sexual intercourse; based on factors such as age and medical, sexual, and reproductive history
- In female patients < 35 years of age: after 12 months
- In female patients ≥ 35 years of age: after 6 months
- The need for medically assisted reproduction to achieve pregnancy
-
An inability to achieve pregnancy despite regular unprotected sexual intercourse; based on factors such as age and medical, sexual, and reproductive history
- Primary infertility: infertility in individuals who have never achieved pregnancy [2]
- Secondary infertility: infertility in individuals who have previously achieved at least one pregnancy [2]
- Diminished ovarian reserve: : a decline in the number of functioning oocytes (either as a normal consequence of age or due to an underlying disorder such as endometriosis) that manifests as a reduced response to ovarian stimulation in reproductive-aged women with regular menstruation [3][4][5]
Epidemiology
Infertility affects approximately 1 in 6 people in their lifetime. [6]
Epidemiological data refers to the US, unless otherwise specified.
Etiology
Female infertility
- Diminished ovarian reserve
- Ovulatory dysfunction
- Tubal/pelvic causes
- Pelvic inflammatory disease
- Blocked or damaged fallopian tubes (e.g., pelvic adhesions, obstruction)
- Endometriosis
- Uterine causes
- Uterine leiomyoma
- Endometrial polyps
- Bicornuate uterus
- Septate uterus
- Asherman syndrome
- Mayer-Rokitansky-Kuster-Hauser syndrome
- Cervical causes
- Trauma (e.g., following cryotherapy, conization)
- Immune factors (e.g., antisperm antibodies in the cervical mucus)
- Diethylstilbestrol exposure in utero
- Cervical anomalies (e.g., insufficient cervical mucus production)
Male infertility
- Hypogonadism; see “Etiology of male hypogonadism.”
- Sperm transport disorders
Sperm transport disorders
-
Obstructive azoospermia
- Absence of spermatozoa in semen despite normal spermatogenesis due to structural or functional abnormalities (e.g., obstruction, absence, dysfunction) along the sperm transport system (epididymis, vas deferens, ejaculatory duct)
- Possible causes include infection (e.g., gonorrhea), iatrogeny (e.g., due to vasectomy), congenital (e.g., absent vas deferens in patients with cystic fibrosis), or genetic conditions (e.g., decreased sperm motility in primary ciliary dyskinesia).
-
Sexual dysfunction
- Anejaculation
- Premature ejaculation
The cause of infertility remains unexplained in up to a third of affected couples. [7][8]
Diagnosis
General principles [4][5][9]
-
Begin initial evaluation for infertility if pregnancy is not achieved after regular unprotected sexual intercourse for at least:
- 12 months in female individuals < 35 years of age
- 6 months in female individuals ≥ 35 years of age
-
Refer promptly to a reproductive endocrinologist for evaluation for the following indications: [10]
- Female individuals > 40 years of age [11]
- Known or suspected male infertility
- Known or suspected causes of infertility
- Assisted reproductive technology is required or desired (e.g., same-sex couples, individuals with anomalies of the female genital tract such as Mullerian agenesis)
- Evaluate both partners simultaneously to prevent unnecessary studies. [9]
-
Obtain a complete personal and family history of both partners, including:
- Comprehensive gynecologic and obstetric history for female individuals
- Reproductive history (e.g., coital frequency and timing)
- Medical history (e.g., chronic conditions, childhood illness, sexual dysfunction)
- Medication history (e.g., teratogens) and exposures (e.g., smoking, alcohol)
- In patients with amenorrhea: Perform diagnostics for amenorrhea (e.g., TSH and prolactin) before pursuing infertility workup. [4]
Female individuals
Initial assessment [2][4][5]
Approach
- Perform physical examination, including: [4]
- Skin examination (e.g., for hirsutism, acne, acanthosis nigricans)
- Thyroid examination
- Breast examination (e.g., for tenderness, mass, nipple discharge)
- Speculum examination
-
Evaluate for ovulatory dysfunction.
-
Patients with amenorrhea, AUB, and/or hirsutism: Perform ovulation testing.
- If no ovulation: Evaluate for underlying cause, i.e., with diagnostics for amenorrhea.
- If ovulation present: Proceed to imaging.
-
All other patients: Assume regular ovulation and evaluate for structural pathology with diagnostic imaging.
- Abnormal imaging: Refer to gynecology.
- Normal imaging: Refer to reproductive endocrinology for further assessment (e.g., ovarian reserve testing).
-
Patients with amenorrhea, AUB, and/or hirsutism: Perform ovulation testing.
Ovulation tests
Options include:
- Ovulation prediction test to identify pending ovulation
-
Mid-luteal phase serum progesterone level (∼ 1 week before expected menstrual period) [2][4][12]
- ≥ 3 ng/mL: suggests ovulation has recently occurred
- < 3 ng/mL: suggests anovulation
- Mid-luteal phase transvaginal ultrasound to evaluate quantity and size of developing follicles
Imaging
- Transvaginal ultrasound to evaluate cervix, adnexa, and uterus (e.g., for adnexal adhesions and endometriosis) [2][4]
-
Hysterosalpingography or sonohysterosalpingography to evaluate for: [4];
- Fallopian tube patency and morphology (e.g., tubal occlusion)
- Uterine abnormalities (e.g., septate uterus, submucosal fibroids, intrauterine adhesions)


Further assessment [2][3][4]
Further assessment is typically performed by reproductive endocrinology and may include the following.
-
Testing for diminished ovarian reserve, which may show: [3][4]
- ↓ Anti-Müllerian hormone level
- ↑ FSH and estradiol on days 2–4 of the menstrual cycle [4]
- ↓ Antral follicle count on transvaginal ultrasound
- Hysteroscopy: for definitive evaluation of intrauterine causes of infertility
- Additional diagnostic studies (e.g., laparoscopy with chromopertubation, MRI pelvis)
Although ovarian reserve testing can predict responsiveness to ovarian stimulation, it does not predict reproductive potential better than the patient's age and should not be performed to evaluate reproductive potential in female individuals without infertility. [3]
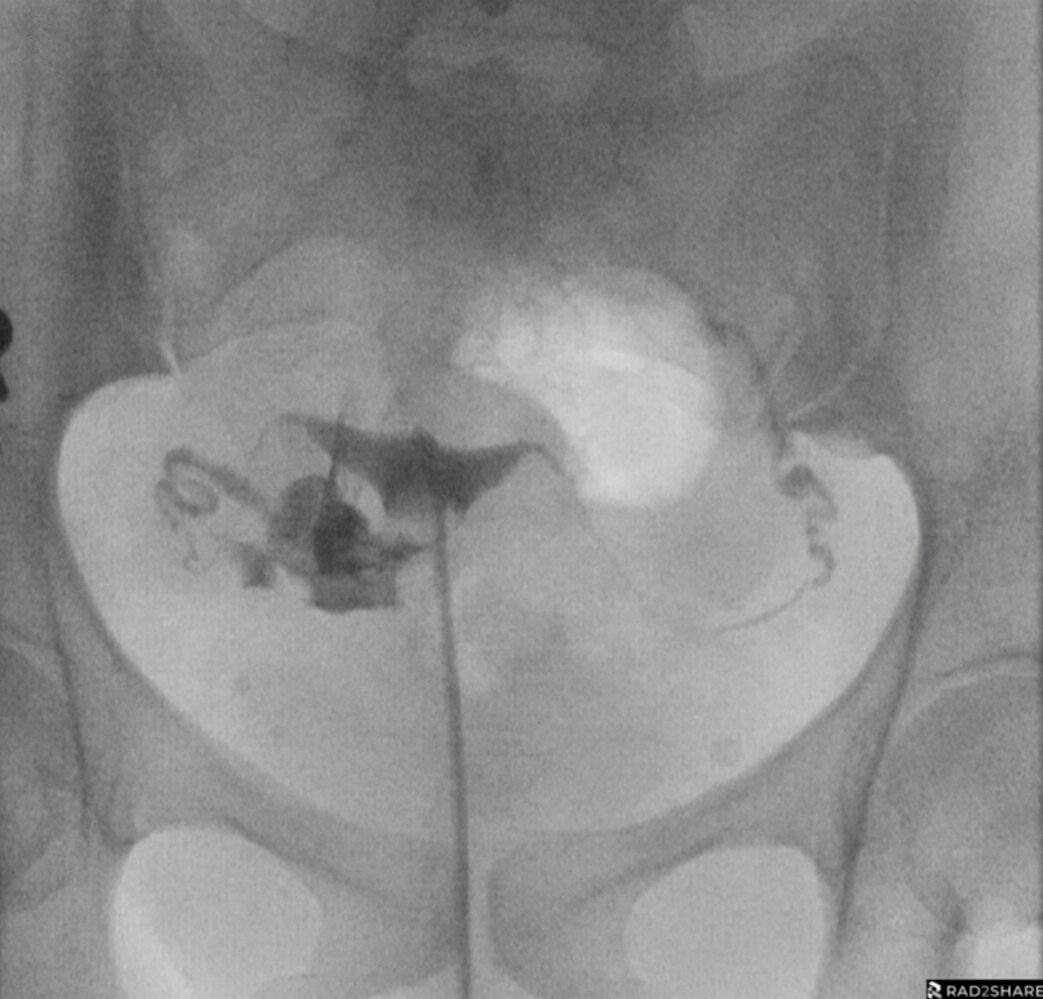
Hysterosalpingography (AP view)
The endometrial cavity (yellow overlay) is normal in size and contour, without distortion or filling defects. There is free flow of contrast into both fallopian tubes and free spill of contrast from each fallopian tube into the peritoneal cavity (blue overlay) indicating bilateral tubal patency. No loculated collections are identified in the pelvis to suggest peritubal adhesions
Black arrows: intramural portion; Black arrowheads: ampullary portion; Circle: catheter balloon; White arrow: HSG catheter; White arrowheads: isthmic portion
Source: “Fig 1A, In: Contrast media for hysterosalpingography: systematic search and review providing new guidelines by the Contrast Media Safety Committee of the European Society of Urogenital Radiology” by Geenen RWF, van der Molen AJ, Dekkers IA et al., SpringerNature Link, licensed under CC BY 4.0. Modifications: removal of letter A. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).

Hysterosalpingography (AP view) of 31-year-old woman
A catheter (dashed lines) is present in the uterus. The uterus is filled with contrast and is normal in size and shape. There is no evidence of a congenital anomaly. No intraluminal masses are seen. Contrast is present at the cornua (indicated by arrowheads), but the fallopian tubes have not filled.
Persistent nonfilling of a fallopian tube is consistent with tubal occlusion. Proximal tubal spasm can simulate occlusion, although the tube will often fill on a follow-up hysterosalpingogram (HSG).
Source: “Fig 1, In: Fertility Challenges: The Complexities of Retrograde Ejaculation and Cornual Block in Reproductive Health” by Kasbe MN, More A, Gajabe G et al., Cureus, licensed under CC BY 4.0. Modifications: removal of in-image text. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
Male individuals
Initial assessment [9][13][14][15]
- Perform:
- Physical examination, including penis and testes
- Semen analysis
- Refer to urology if there are abnormal findings on initial evaluation.
Further assessment [9][13][14][15]
Further assessment is typically performed by urology and may include the following.
- FSH and total testosterone, and possibly testicular biopsy: to assess for abnormal spermatogenesis (i.e., rule out obstructive azoospermia)
- Additional endocrine evaluation (e.g., LH, prolactin, TSH): to assess for underlying cause of low total testosterone
- Genetic testing (e.g., karyotyping, Y chromosome microdeletion, cystic fibrosis testing): to assess for genetic conditions associated with male infertility (e.g., Klinefelter syndrome) [9]
- Specialized semen testing (e.g., sperm antibody testing, sperm DNA fragmentation): to assess for other impairments of sperm function
- Post-ejaculatory urinalysis: to assess for retrograde ejaculation
- Imaging (e.g., transrectal ultrasonography): to assess for structural causes of obstructive azoospermia
Antisperm antibodies form when the blood testis barrier is disrupted, usually due to infections or trauma of the male genital tract, and can lead to immobilization and agglutination of sperm or have a spermatoxic effect. [13][16]
Management
Approach [2][5][9]
- All patients:
- Provide preconception care, including preconception counseling on diet and lifestyle.
- Consider referral to infertility counseling services.
- Patients with anovulation
- Manage underlying conditions, e.g., hyperprolactinemia (with bromocriptine), hypothyroidism (with levothyroxine), and insulin resistance in PCOS (with metformin).
- Patients with eugonadotropic eugonadism (e.g., PCOS): Provide oral ovulation induction.
-
Refer female patients to reproductive endocrinology for consideration of medically assisted reproduction if:
- A structural cause of infertility such as tubal disease or uterine lesions is identified (surgical management may also be considered for, e.g., removal of adhesions or leiomyomas)
- No cause for infertility is identified [8]
- Pregnancy is not achieved after 6 cycles of oral ovulation induction [2]
- Assisted reproductive technology is desired
- Refer male patients to urology.
Ovulation induction [2][17]
The goal of ovulation induction is to stimulate development of a single dominant follicle in patients with anovulation. [17]
-
Oral medications
- Indications
- Anovulation with eugonadotropic eugonadism (e.g., PCOS)
- Unexplained infertility [8]
- Options
- Letrozole (off-label): first-line in PCOS (see “Treatment of PCOS” for details) [18][19]
- Clomiphene citrate [20]
- Indications
- Pulsatile GnRH: may be used for functional hypothalamic amenorrhea [21]
-
Exogenous gonadotropins
-
Indications
- Anovulation due to hypogonadotropic hypogonadism
- Inadequate response to oral agents
- Options: recombinant FSH, LH, and/or hCG
-
Indications
Ovulation induction increases the risk of multiple pregnancy, and ovulation induction with exogenous gonadotropins increases the risk of ovarian hyperstimulation syndrome. [17]
Other forms of medically assisted reproduction [5][22]
- Intrauterine insemination: an infertility treatment in which washed and concentrated sperm are introduced directly into the uterine cavity at the time of ovulation [23]
- Assisted reproductive technology: infertility treatments involving the in vitro handling of human embryos, or of oocytes together with sperm
Assisted reproductive technology
In vitro fertilization may be combined with intracytoplasmic sperm injection and/or the use of donor gametes. [24]
-
In vitro fertilization [25]
- Multiple oocytes are obtained through ovarian stimulation with exogenous gonadotropins. [25]
- Transvaginal follicular puncture for oocyte retrieval is performed with ultrasound monitoring.
- Fertilization of gametes occurs extracorporeally.
- Embryos are transferred into the uterus.
- Intracytoplasmic sperm injection: Sperm is injected into an oocyte during in vitro fertilization. [22]
- Gamete donation [26]
Complications
Patients who start assisted reproductive technology are at risk of complications related to ovarian stimulation.
Ovarian hyperstimulation syndrome (OHSS) [27][28]
- Definition: a potentially life-threatening complication of ovulation induction or ovarian stimulation with exogenous human chorionic gonadotropin (hCG)
-
Pathophysiology
- Exogenous hCG is thought to be responsible for the massive luteinization of the ovarian granulosa cells.
- Formation of multiple ovarian follicles and corpus luteum cysts with rapid ovarian enlargement
- ↑ Release of vasoactive mediators (e.g., VEGF) that induce an increase in capillary permeability and consequent third spacing into the abdominal cavity
-
Clinical features: onset between 3 days (early onset) and ≥ 9 days (late onset) after hCG administration
- Abdominal pain and distention
- Nausea and/or vomiting
- Weight gain
- Ascites
- Oliguria or anuria
- Dyspnea
- Pleural effusion
- Syncope
- Venous thrombosis
-
Diagnostics
-
Laboratory analysis
- CBC (↑ Hct, leukocytosis)
- Serum electrolyte concentrations
- Renal function tests
- Liver function tests
- Transvaginal ultrasound: ascites and ovarian enlargement
-
Laboratory analysis
-
Management
- Mild to moderate OHSS (usually early onset): Manage on an outpatient basis.
- Limit physical activity.
- Pain management with acetaminophen
- Daily monitoring of body weight (should not increase by > 1 kg/day) and urine output
- Sufficient hydration (1–2 L/day)
- Paracentesis to relieve symptoms of ascites
- Severe OHSS (usually late onset)
- Hospitalization
- Multidisciplinary management approach: supportive care (e.g., cautious IV fluids), monitoring, and prevention of complications (e.g., prophylactic anticoagulation)
- Mild to moderate OHSS (usually early onset): Manage on an outpatient basis.
-
Complications
- Sepsis
- Thromboembolism
- Pericardial effusion
- Arrhythmias
- Acute respiratory distress syndrome
- Acute kidney injury
")
")
We list the most important complications. The selection is not exhaustive.
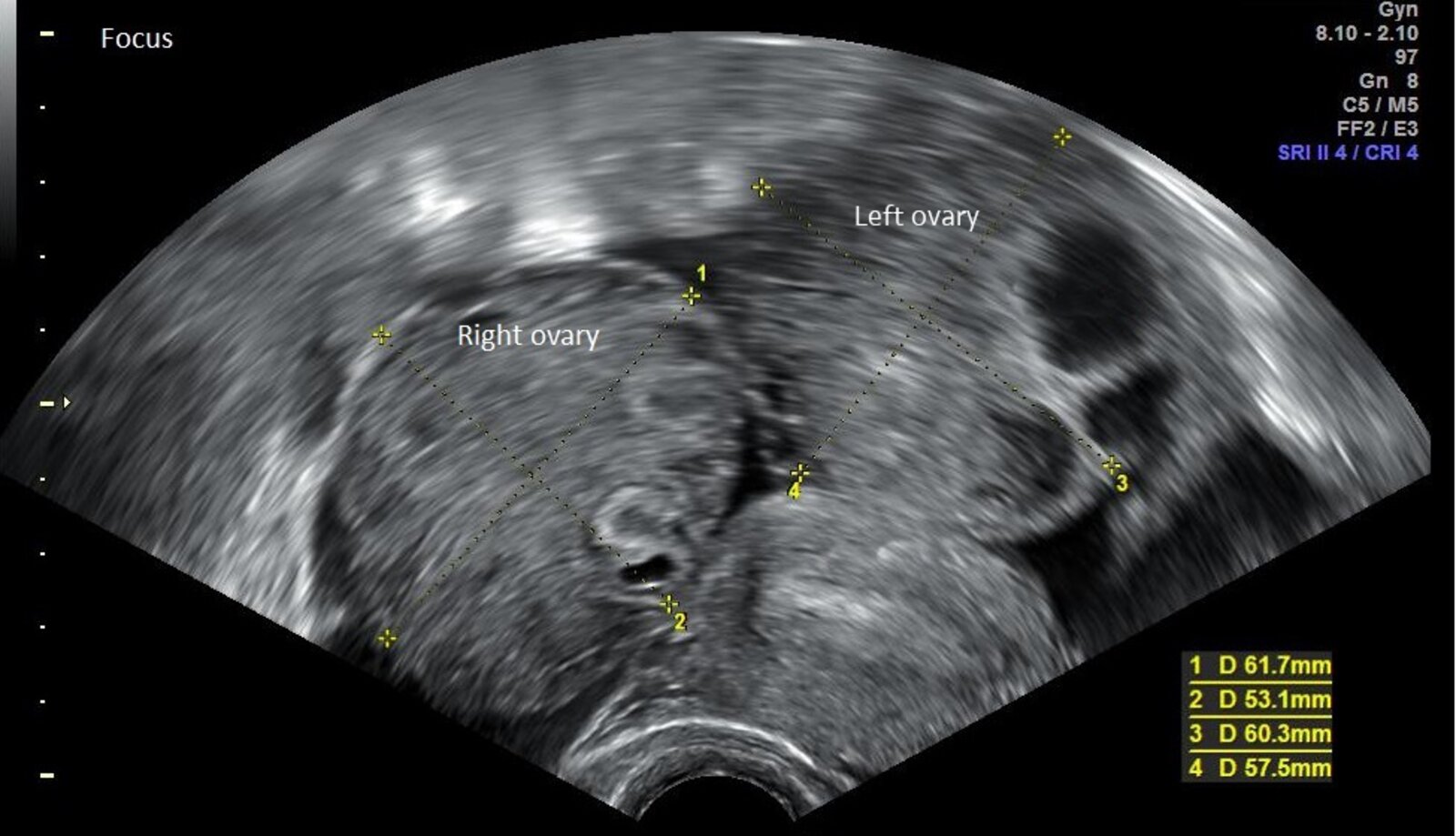
Ultrasound pelvis (transvaginal; coronal plane)
The ovaries are rounded and enlarged, with the right measuring 61.7 x 53.1 mm and the left measuring 60.3 x 57.5 mm. Small follicles are seen (examples indicated by green outline). There is adjacent anechoic free fluid (F).
Red outline: Uterus
This image is an adaptation. Source of original image: Wikimedia Commons. Original title: “Vaginal ultrasonography in mild ovarian hyperstimulation syndrome - coronal”. Created by: Mikael Häggström. Licensed under Public Domain. Modifications to original image: - text edits: removed "uterus"; shifted "left ovary". Further notes: Source of illustration: "Vaginal ultrasonography in OHSS - coronal", BruceBlaus, Wikimedia Commons licensed under CC BY 3.0 (https://commons.wikimedia.org/wiki/File:Vaginal_ultrasonography_in_OHSS_-_coronal.png) adapted from "Blausen 0602 Laparoscopy 02" (https://commons.wikimedia.org/wiki/File:Blausen_0602_Laparoscopy_02.png)
{kind=link}
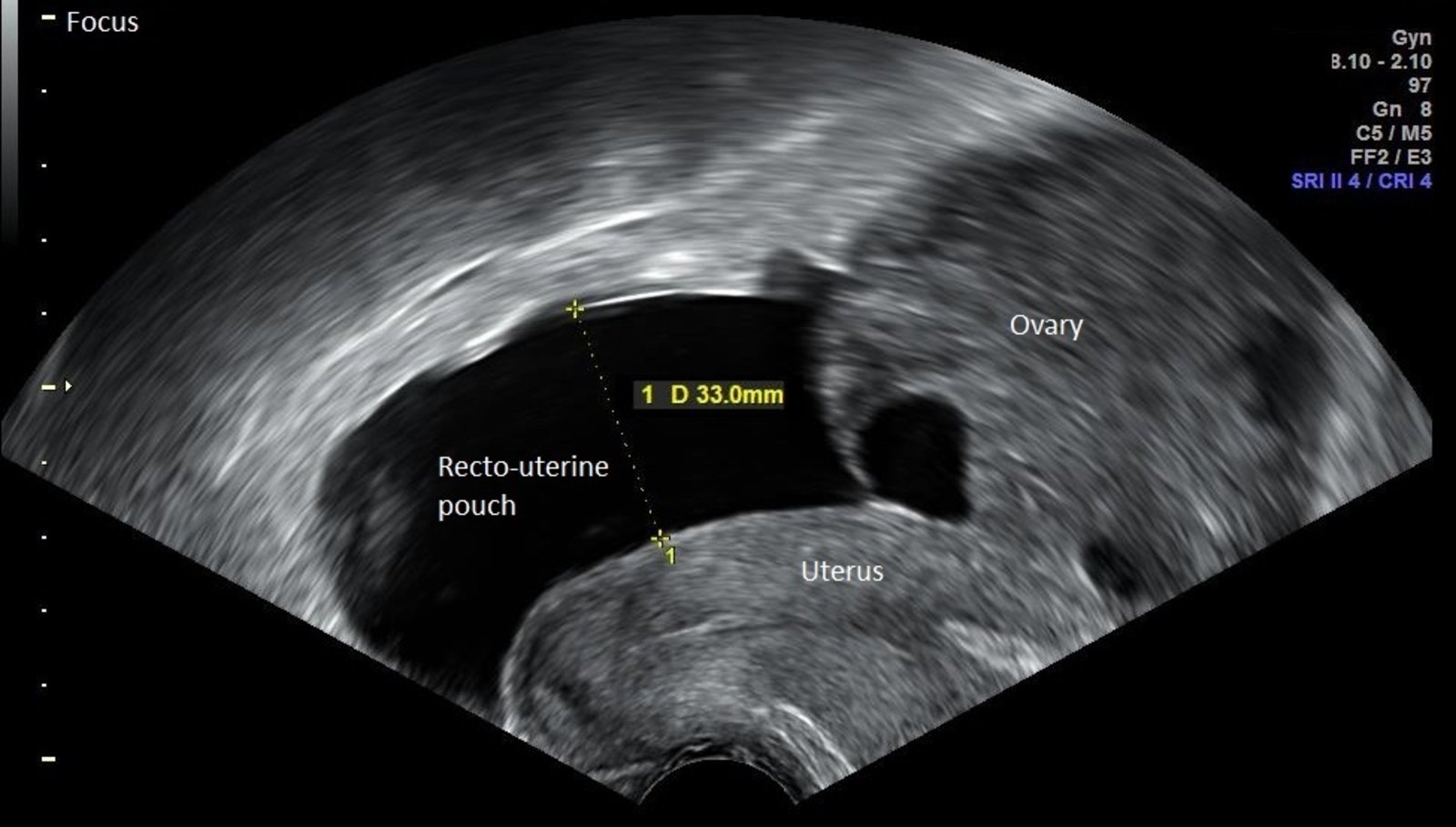
Ultrasound pelvis (transvaginal; sagittal plane)
Anechoic free fluid in the cul-de-sac (rectouterine pouch) measures 33 mm in depth. The visible left ovary is rounded and enlarged.
Source: "Vaginal ultrasonography in mild ovarian hyperstimulation syndrome - sagittal", Mikael Häggström, Wikimedia Commons licensed under Public Domain Further notes: Source of illustration: "Vaginal ultrasonography in OHSS - coronal", Mikael Häggström, from original by BruceBlaus, Wikimedia Commons licensed under CC BY 3.0 (https://commons.wikimedia.org/wiki/File:Vaginal_ultrasonography_in_OHSS_-_sagittal.png) adapted from "Blausen 0602 Laparoscopy 02" (https://commons.wikimedia.org/wiki/File:Blausen_0602_Laparoscopy_02.png)
{kind=link}
External Resources
- 2025 ACOG Committee Statement No. 14 on Infertility: Disparities and Access to Services
- 2024 AUA/ASRM Guideline on Updates to Male Infertility
- 2023 AUA/ASRM Guideline on Diagnosis and Treatment of Infertility in Men: Part I
- 2023 AUA/ASRM Guideline on Diagnosis and Treatment of Infertility in Men: Part II
- 2021 ASRM Committee Opinion on Fertility Evaluation of Infertile Women
- 2020 ASRM Committee Opinion on Testing and Interpreting Measures of Ovarian Reserve
- 2020 ASRM Committee Opinion on Use of Exogenous Gonadotropins for Ovulation Induction in Anovulatory Women
- 2015 ASRM Committee Opinion on Diagnostic Evaluation of the Infertile Male
References
- ASRM. "Definition of infertility: a committee opinion". Fertil Steril. 120(6). :1170. (2023)
- Phillips K, Olanrewaju RA, Omole F. "Infertility: Evaluation and Management". Am Fam Physician. 107(6). :623-630. (2023)
- Penzias A, Azziz R, Bendikson K, et al. "Testing and interpreting measures of ovarian reserve: a committee opinion". Fertil Steril. 114(6). :1151-1157. (2020)
- Practice Committee of the American Society for Reproductive Medicine. "Fertility evaluation of infertile women: a committee opinion". Fertil Steril. 116(5). :1255-1265. (2021)
- Santoro N, Polotsky AJ. "Infertility Evaluation and Treatment". N Engl J Med. 392(11). :1111-1119. (2025)
- "Infertility Definitions and Terminology". https://www.who.int/health-topics/infertility#tab=tab_1. [2017-06-28]
- Gelbaya TA, Potdar N, Jeve YB, Nardo LG. "Definition and Epidemiology of Unexplained Infertility". Obstet Gynecol Surv. 69(2). :109-115. (2014)
- Practice Committee of the American Society for Reproductive Medicine. "Evidence-based treatments for couples with unexplained infertility: a guideline". Fertil Steril. 113(2). :305-322. (2020)
- Brannigan RE, Hermanson L, Kaczmarek J, et al. "Updates to Male Infertility: AUA/ASRM Guideline (2024)". J Urol. :101097JU0000000000004180. (2024)
- ACOG. "Infertility: Disparities and Access to Services". Obstet Gynecol. 145(1). :e51-e57. (2025)
- ASRM and ACOG. "Female age-related fertility decline". Fertil Steril. 101(3). :633-634. (2014)
- Kumar P, Sait SF. "Ovarian hyperstimulation syndrome". J Hum Reprod Sci. (2011)
- Pfeifer S, Butts S, Dumesic D, et al. "Prevention and treatment of moderate and severe ovarian hyperstimulation syndrome: a guideline". Fertil Steril. 106(7). :1634-1647. (2016)
- American Society for Reproductive Medicine. "Diagnostic evaluation of the infertile male: a committee opinion". Fertility and Sterility. 103(3). :e18-e25. (2015)
- Schlegel PN, Sigman M, Collura B, et al. "Diagnosis and Treatment of Infertility in Men: AUA/ASRM Guideline Part I". J Urol. 205(1). :36-43. (2021)
- Schlegel PN, Sigman M, Collura B, et al. "Diagnosis and Treatment of Infertility in Men: AUA/ASRM Guideline PART II". J Urol. 205(1). :44-51. (2021)
- Gupta S, Sharma R, Agarwal A, et al. "Antisperm Antibody Testing: A Comprehensive Review of Its Role in the Management of Immunological Male Infertility and Results of a Global Survey of Clinical Practices". The World Journal of Men's Health. 40(3). :380. (2022)
- Garg A, Zielinska AP, Yeung AC, et al. "Luteal phase support in assisted reproductive technology". Nat Rev Endocrinol. 20(3). :149-167. (2023)
- ASRM. "Use of exogenous gonadotropins for ovulation induction in anovulatory women: a committee opinion". Fertil Steril. 113(1). :66-70. (2020)
- Teede HJ, Tay CT, Laven J, et al. "Recommendations from the 2023 International Evidence-based Guideline for the Assessment and Management of Polycystic Ovary Syndrome". Fertil Steril. 120(4). :767-793. (2023)
- American College of Obstetricians and Gynecologists' Committee on Practice Bulletins—Gynecology. "ACOG Practice Bulletin No. 194: Polycystic Ovary Syndrome (reaffirmed 2025)". Obstet Gynecol. 131(6). :e157-e171. (2018)
- The Practice Committee of the American Society for Reproductive Medicine. "Use of clomiphene citrate in infertile women: a committee opinion". Fertil Steril. 100(2). :341-348. (2013)
- Saadedine M, Kapoor E, Shufelt C. "Functional Hypothalamic Amenorrhea: Recognition and Management of a Challenging Diagnosis". Mayo Clin Proc. 98(9). :1376-1385. (2023)
- Zegers-Hochschild F, Adamson GD, Dyer S, et al. "The International Glossary on Infertility and Fertility Care, 2017". Fertil Steril. 108(3). :393-406. (2017)
- Ayeleke RO, Asseler JD, Cohlen BJ, Veltman-Verhulst SM. "Intra-uterine insemination for unexplained subfertility". Cochrane Database Syst Rev. 2020(3). (2020)
- ACOG. "Committee Opinion No 671: Perinatal Risks Associated With Assisted Reproductive Technology". Obstetrics & Gynecology. 128(3). :e61-e68. (2016)
- Ovarian Stimulation TEGGO, Bosch E, Broer S, et al. "ESHRE guideline: ovarian stimulation for IVF/ICSI". Human reproduction open. 2020(2). :hoaa009. (2020)
- Practice Committee of the American Society for Reproductive Medicine and the Practice Committee for the Society for Assisted Reproductive Technology. Electronic address: ASRM@asrm.org. "Guidance regarding gamete and embryo donation". Fertil Steril. 115(6). :1395-1410. (2021)