Summary
An inguinal hernia is an abnormal protrusion of intra-abdominal contents (most commonly fat) through the inguinal canal. Inguinal hernias are the most common type of groin hernia, and can be further subdivided based on anatomic location: an indirect inguinal hernia protrudes lateral to the inferior epigastric vessels through the deep inguinal ring, whereas a direct inguinal hernia protrudes medial to the inferior epigastric vessels through a defect in the posterior wall of the inguinal canal. An uncomplicated inguinal hernia typically manifests as a mass in the groin with or without pain (inguinodynia). Incarceration, obstruction, and strangulation of hernial contents are collectively referred to as complicated inguinal hernia. Inguinal hernia is a clinical diagnosis. Imaging, preferably with ultrasound, is indicated if the clinical diagnosis is uncertain. Surgery is the only definitive management of inguinal hernia and can be performed as an open surgery or laparoscopically. A strangulated inguinal hernia is a surgical emergency. In patients with an incarcerated hernia with or without bowel obstruction, manual reduction of the hernia may be considered as a temporizing measure before surgery. Conservative management may be considered in selected adult patients with a small, uncomplicated inguinal hernia; timely surgical intervention is recommended in children due to the risk for complicated inguinal hernia.
Definitions
- Direct inguinal hernia: protrusion of abdominal and/or pelvic contents directly through the posterior wall of the inguinal canal
- Indirect inguinal hernia: protrusion of abdominal and/or pelvic contents into the inguinal canal through the deep inguinal ring
- Scrotal hernia: a large, indirect inguinal hernia that descends through the inguinal canal into the scrotum
- Uncomplicated inguinal hernia: an inguinal hernia that is completely reducible and not associated with signs of bowel obstruction or strangulation
- Complicated inguinal hernia: an inguinal hernia that is either irreducible (incarcerated) or associated with mechanical bowel obstruction and/or strangulation
- Occult inguinal hernia: an inguinal hernia that is not identifiable on physical examination



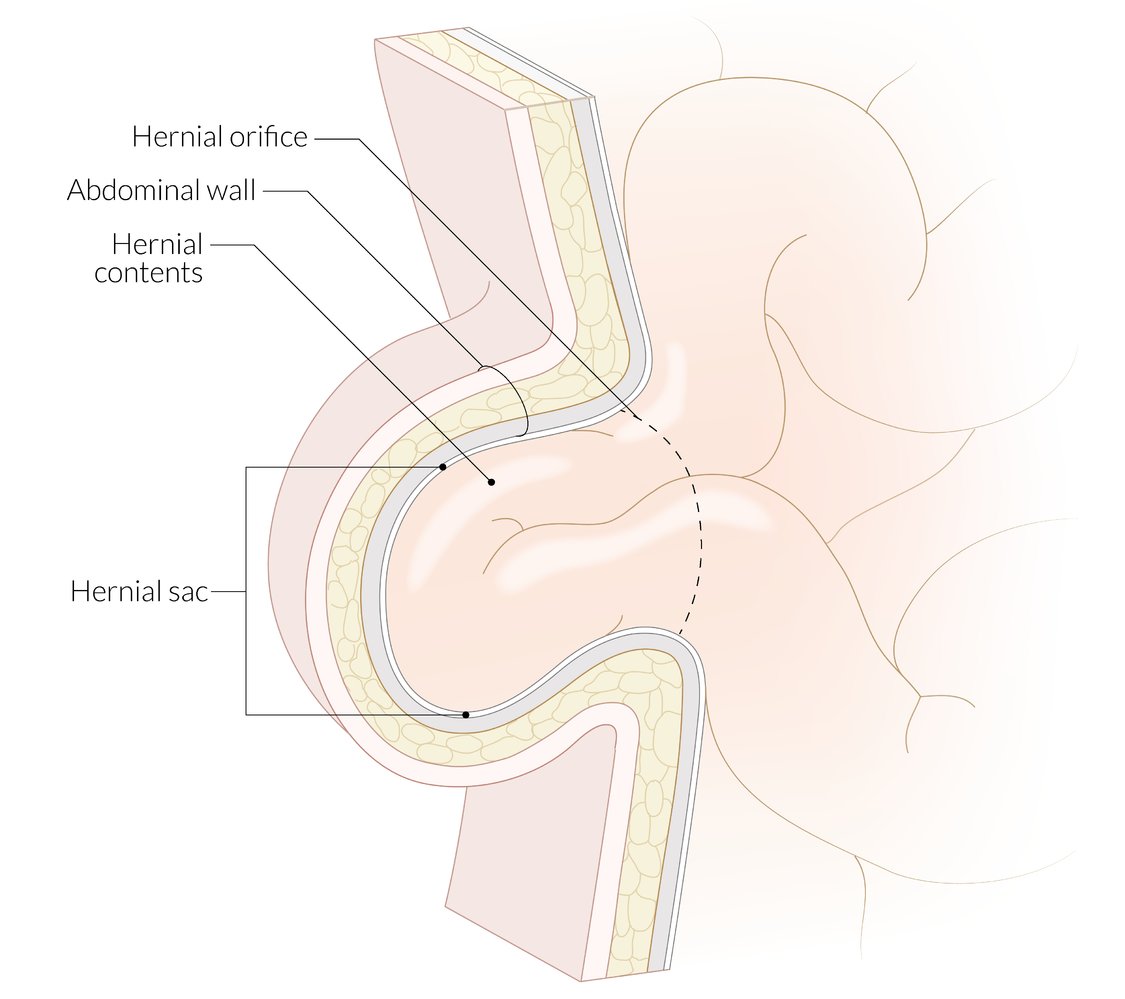
Abdominal and inguinal hernias have three components:
– Hernial sac: parietal peritoneum surrounding the hernial contents
– Hernial contents: typically the omentum and/or loops of small intestine; uncommonly, the large intestine, appendix, bladder, fallopian tubes
– Hernial coverings: layers of the abdominal wall
The hernial orifice is a hiatus (e.g., the umbilicus, deep inguinal ring, posterior wall of the inguinal canal) through which hernial contents herniate. The hernial contents are constricted at the hernial orifice; this constricted area is known as the neck of a hernia.
© AMBOSS
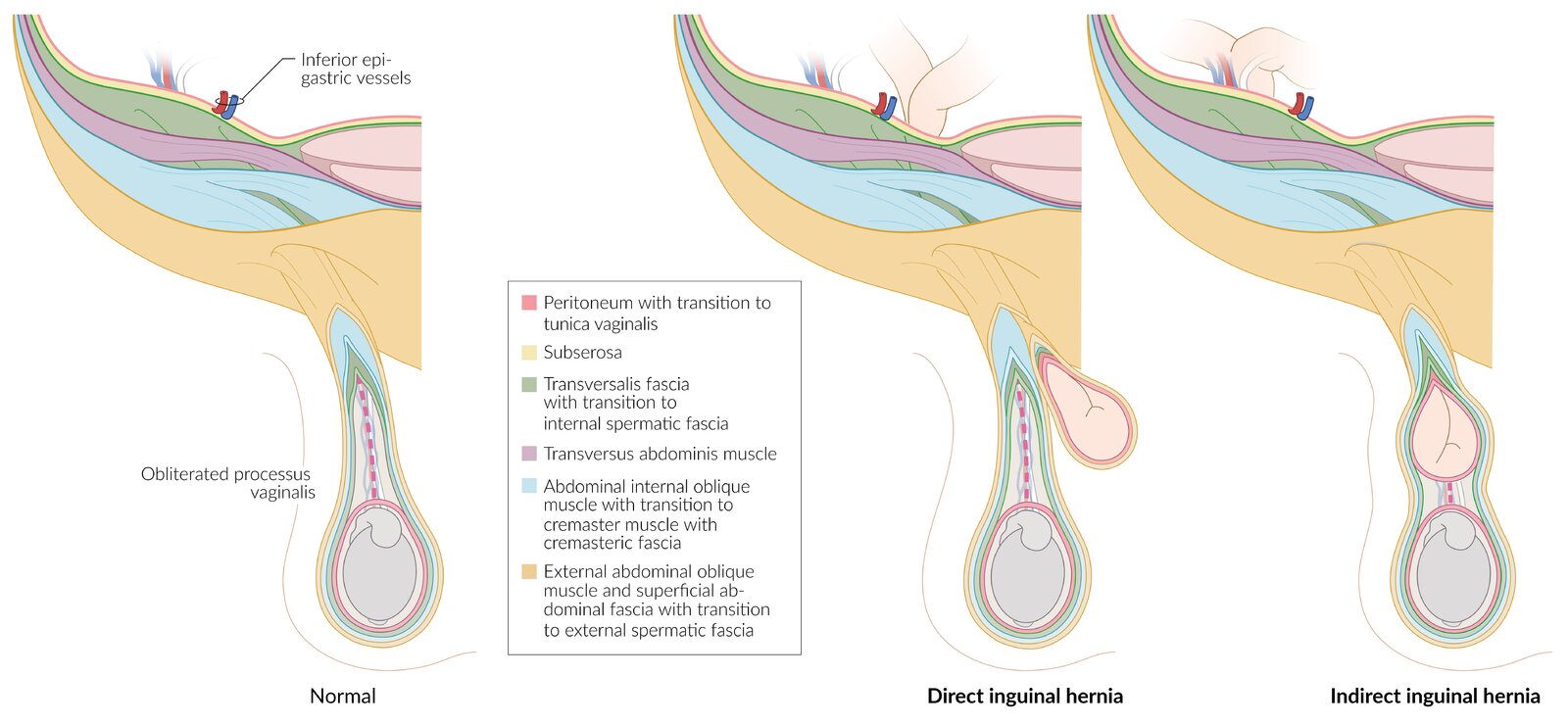
Normally, the only contents of the inguinal canal are the spermatic cord (or round ligament in females) and the ilioinguinal nerve.
Direct inguinal hernia: herniation of intraabdominal contents through the posterior wall of the inguinal canal, medial to the inferior epigastric vessels. The hernial sac lies posteromedial to and outside the spermatic cord
Indirect inguinal hernia: herniation of intraabdominal contents through the deep inguinal ring into the inguinal canal, and, in the case of large inguinal hernia, also through the superficial inguinal ring. The hernial sac lies within the spermatic cord and is therefore covered by the same tissue layers as the spermatic cord.
© AMBOSS
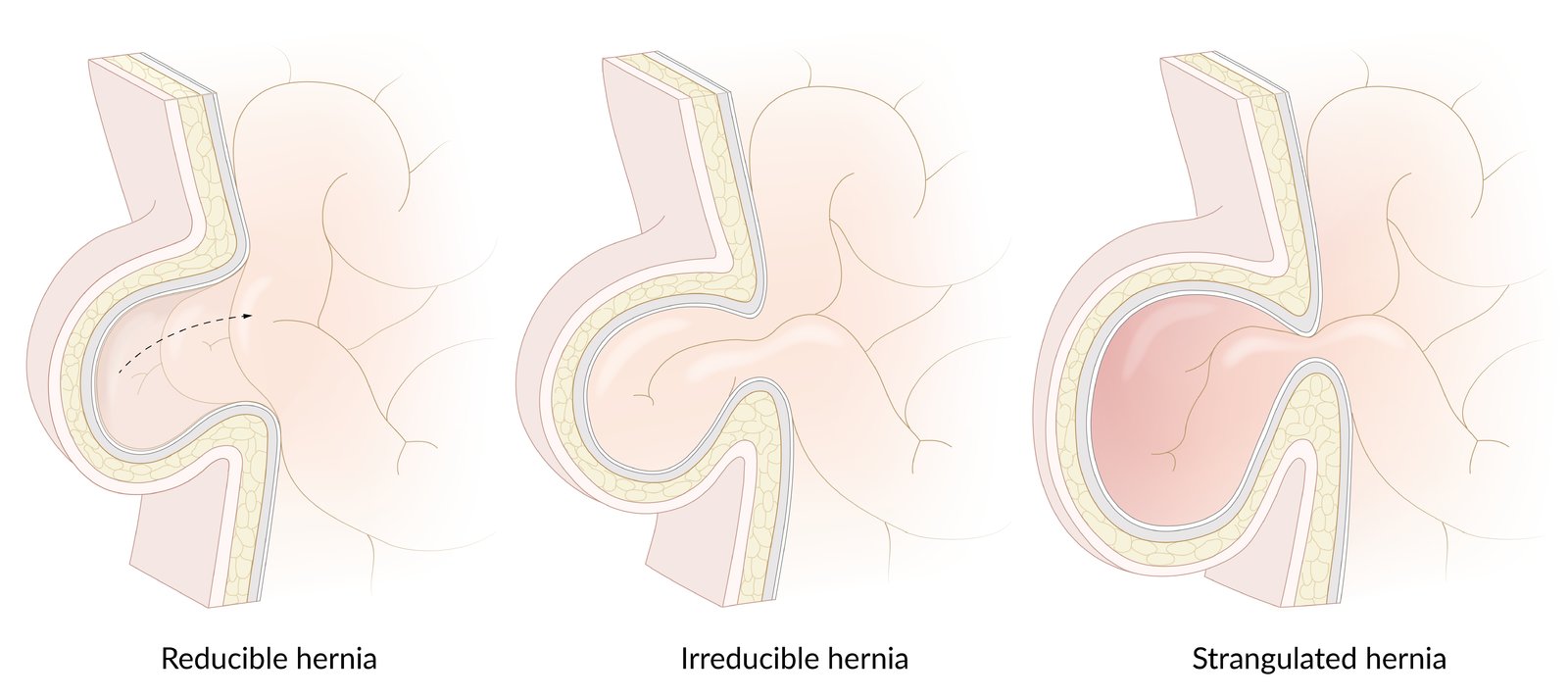
– Reducible hernia: The hernia is easily reducible.
– Irreducible hernia: The hernia is not easily reducible because its contents adhere to the hernial sac.
– Strangulated hernia: ischemia of hernial contents resulting from a tight abdominal wall defect compromising the vascular supply of the hernial contents
© AMBOSS
Overview
| Overview of hernias | |||
|---|---|---|---|
| Inguinal hernia | Femoral hernia | ||
| Indirect | Direct | ||
| Epidemiology |
|
|
|
|
|
||
| Etiology |
|
|
|
| Location |
|
|
|
| Clinical features |
|
|
|
| Diagnostics |
|
||
| Treatment |
|
||
See “Femoral hernia” for further information.



Normally, the only contents of the inguinal canal are the spermatic cord (or round ligament in females) and the ilioinguinal nerve.
Direct inguinal hernia: herniation of intraabdominal contents through the posterior wall of the inguinal canal, medial to the inferior epigastric vessels. The hernial sac lies posteromedial to and outside the spermatic cord
Indirect inguinal hernia: herniation of intraabdominal contents through the deep inguinal ring into the inguinal canal, and, in the case of large inguinal hernia, also through the superficial inguinal ring. The hernial sac lies within the spermatic cord and is therefore covered by the same tissue layers as the spermatic cord.
© AMBOSS
Sagittal view of the male inguinal region at the level of the superior pubic ramus, medial to the epigastric vessels
There is a protruding hernial sac (comprised of the transversalis fascia and parietal peritoneum) below the inguinal ligament but above the pubic bone, which, in the example shown, contains intestine.
© AMBOSS
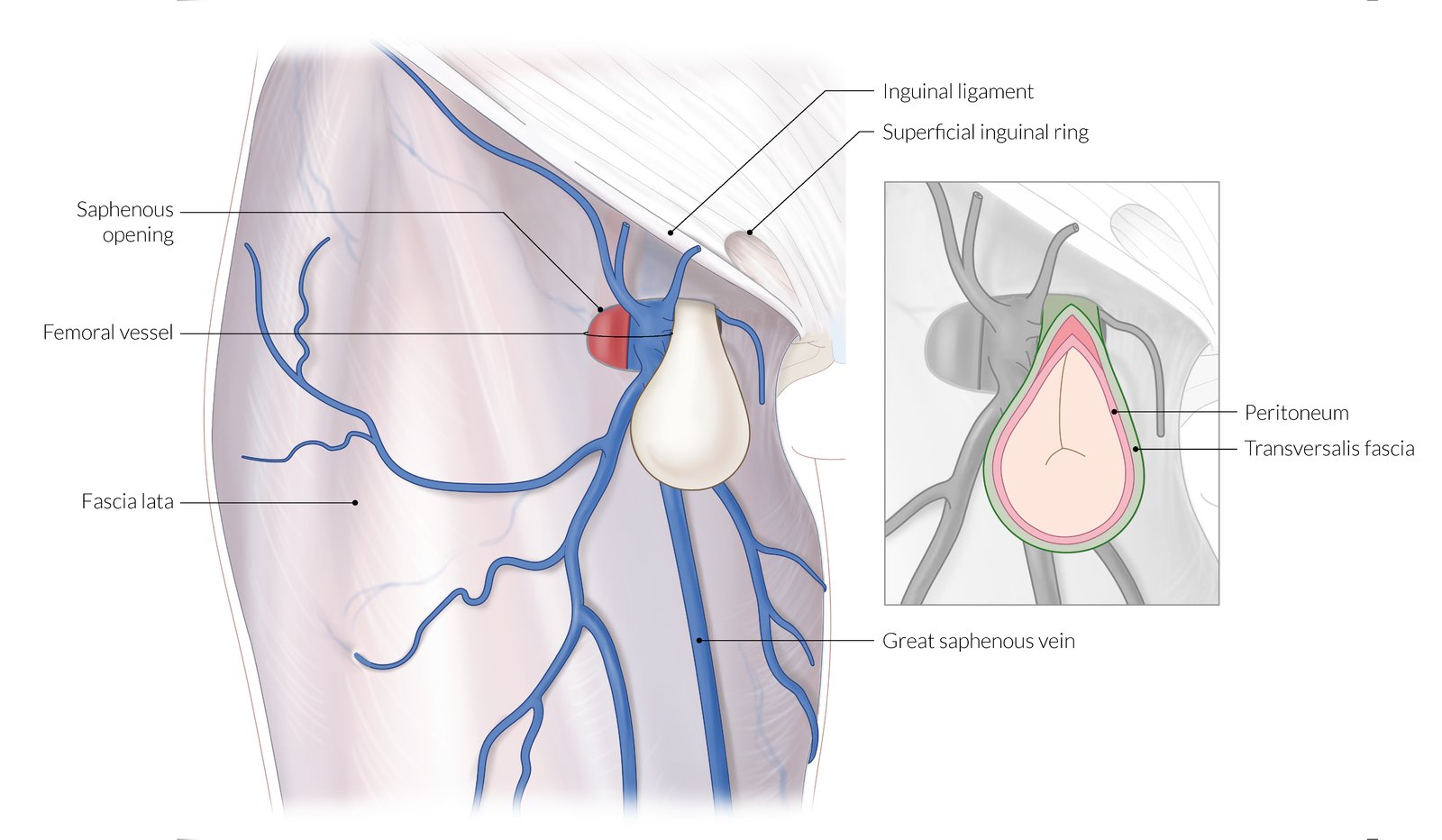
Femoral hernia passes through the vascular lacuna (internal hernial orifice), below the inguinal ligament and usually medial to the femoral vein and runs through the femoral canal until it reaches the saphenous opening (external hernial orifice; approx. 2cm caudal).
The saphenous opening typically contains loose connective and fatty tissue as well as inguinal lymph nodes.
Due to the increased width of the female pelvis, and therefore larger vascular lacuna, femoral hernia occurs predominantly in women.
© AMBOSS

Pelvic and inguinal region
There is a pronounced protrusion on the right side (circled). Inguinal hernia can be confirmed with palpation and a cough test.
Source: “Hernia” by James Heilman, MD, Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}
Epidemiology
-
Prevalence
- 5–10% In the US [2]
- Inguinal hernias are the most common type of hernias (∼ 75% of all cases). [3]
- Indirect inguinal hernia > direct inguinal hernia
- Responsible for one of the most common general surgical procedures in the United States [2]
- Sex: ♂ > ♀
-
Age
- Indirect inguinal hernia: most commonly seen in male infants and older men
- Direct inguinal hernia: most commonly seen in older men
Epidemiological data refers to the US, unless otherwise specified.
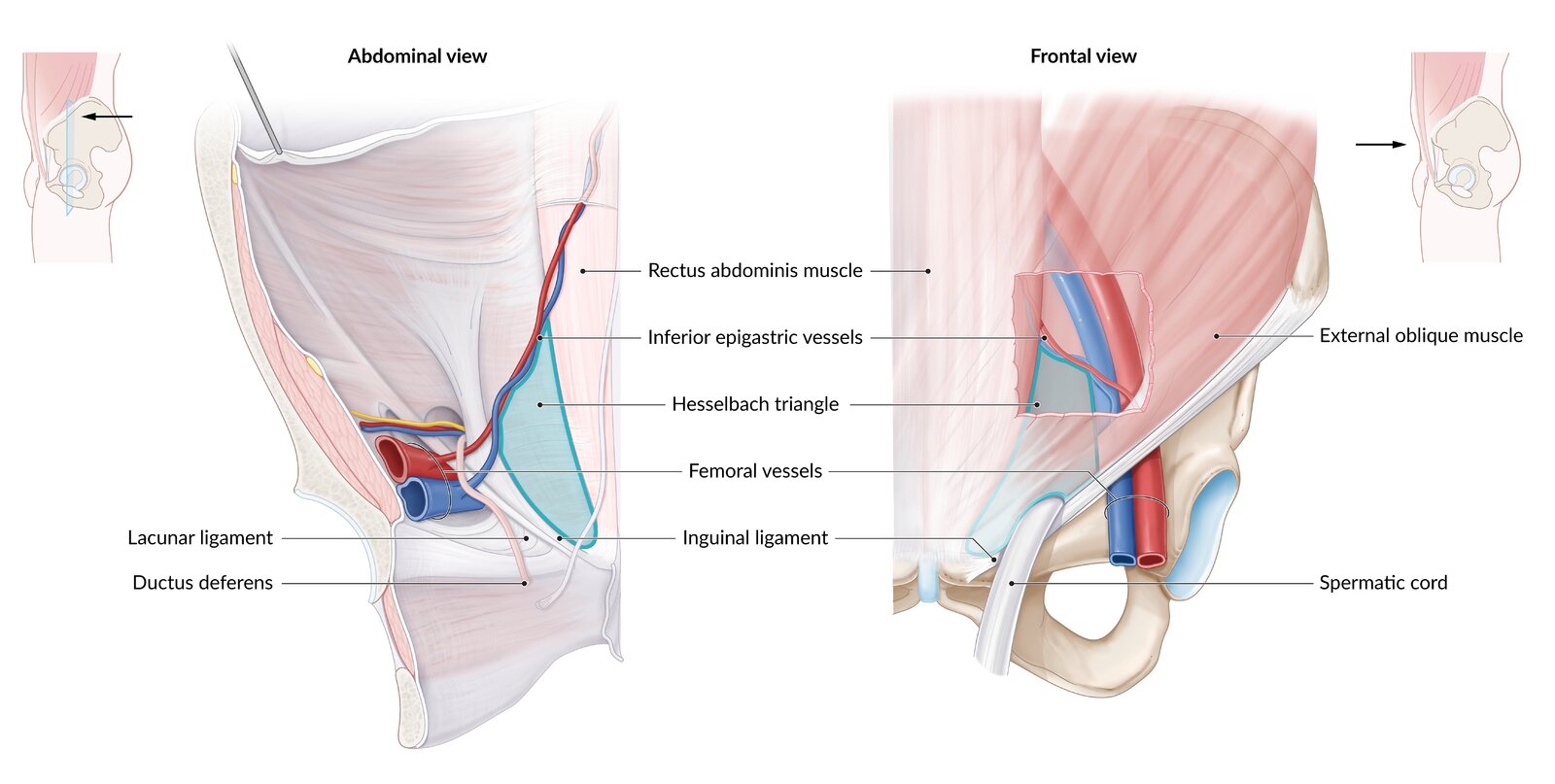
Anatomy
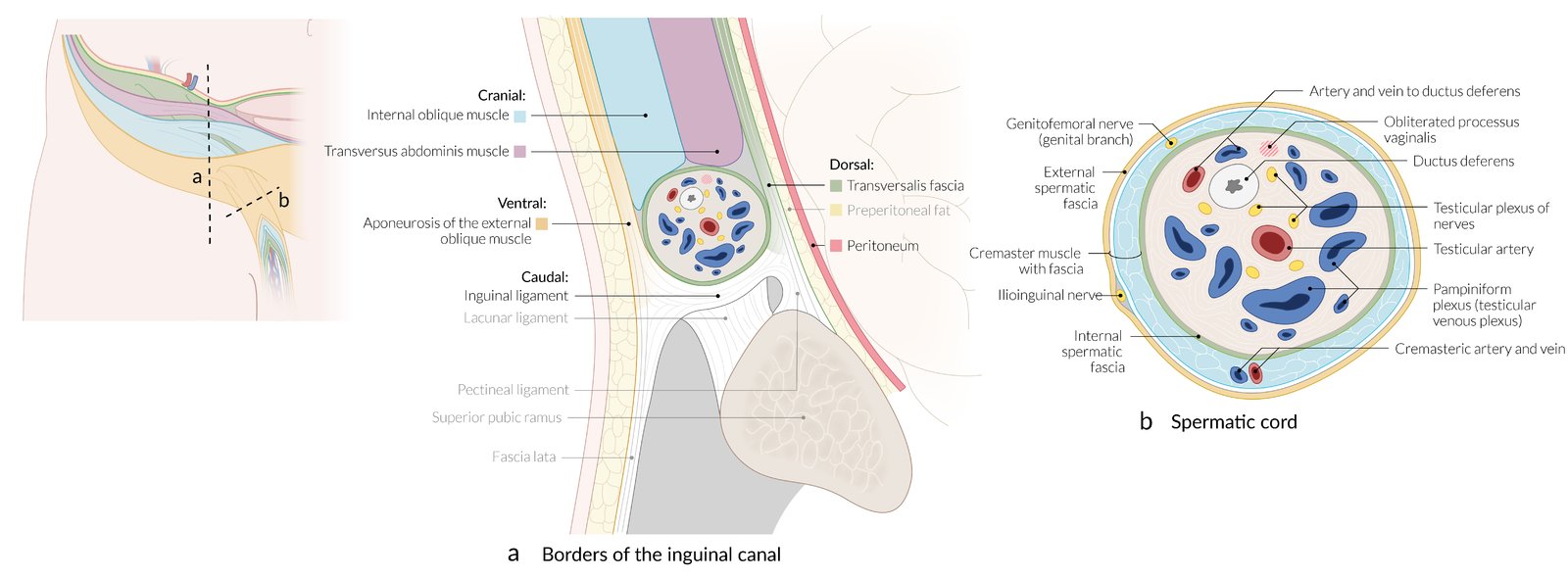
Inguinal canal
- Extends between the deep (internal) and superficial (external) ring
- Roof (superior): internal oblique and transversus abdominis muscles
- Floor (inferior): inguinal ligament (shelving edge of external oblique) and lacunar ligament (medially)
- Posterior wall: transversalis fascia laterally; conjoint tendon medially
- Anterior wall: external oblique aponeurosis and internal oblique muscle laterally

Hesselbach triangle borders
- Medially: rectus abdominis muscle
- Laterally: inferior epigastric vessels
- Inferiorly: inguinal ligament



References:[4]
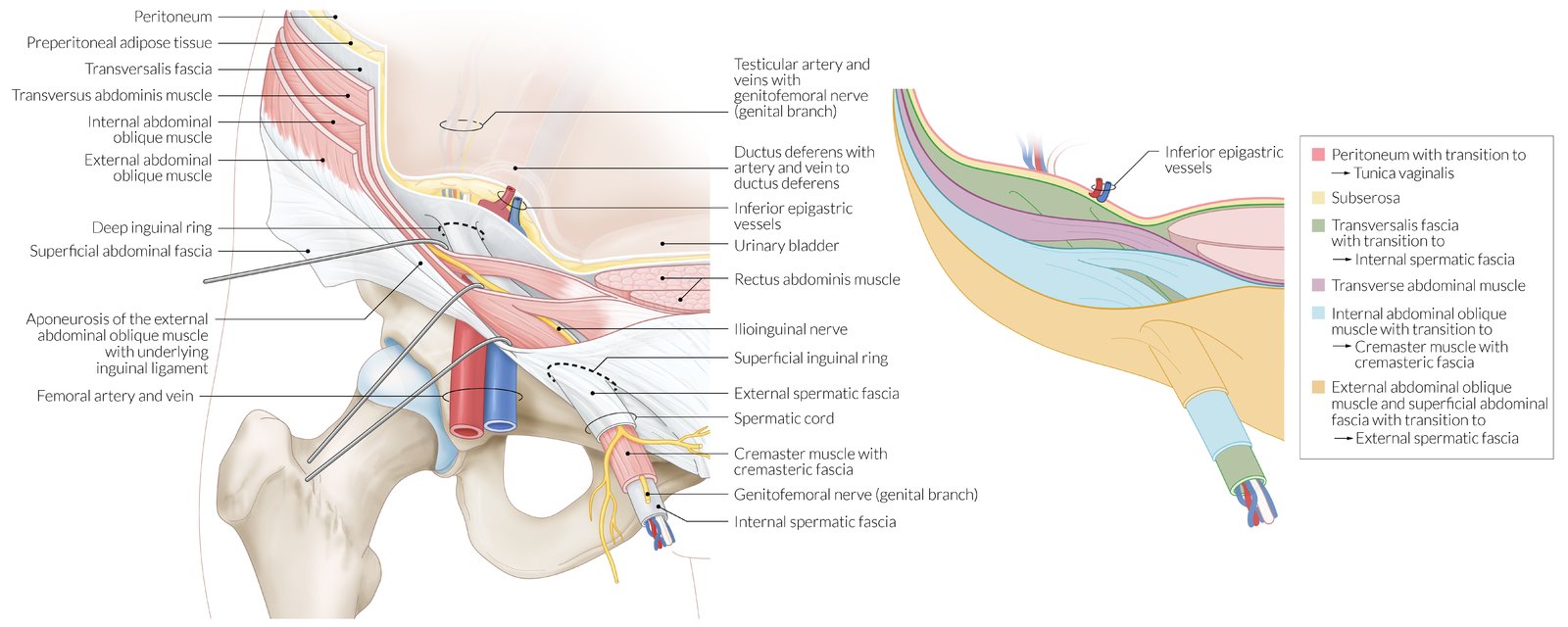
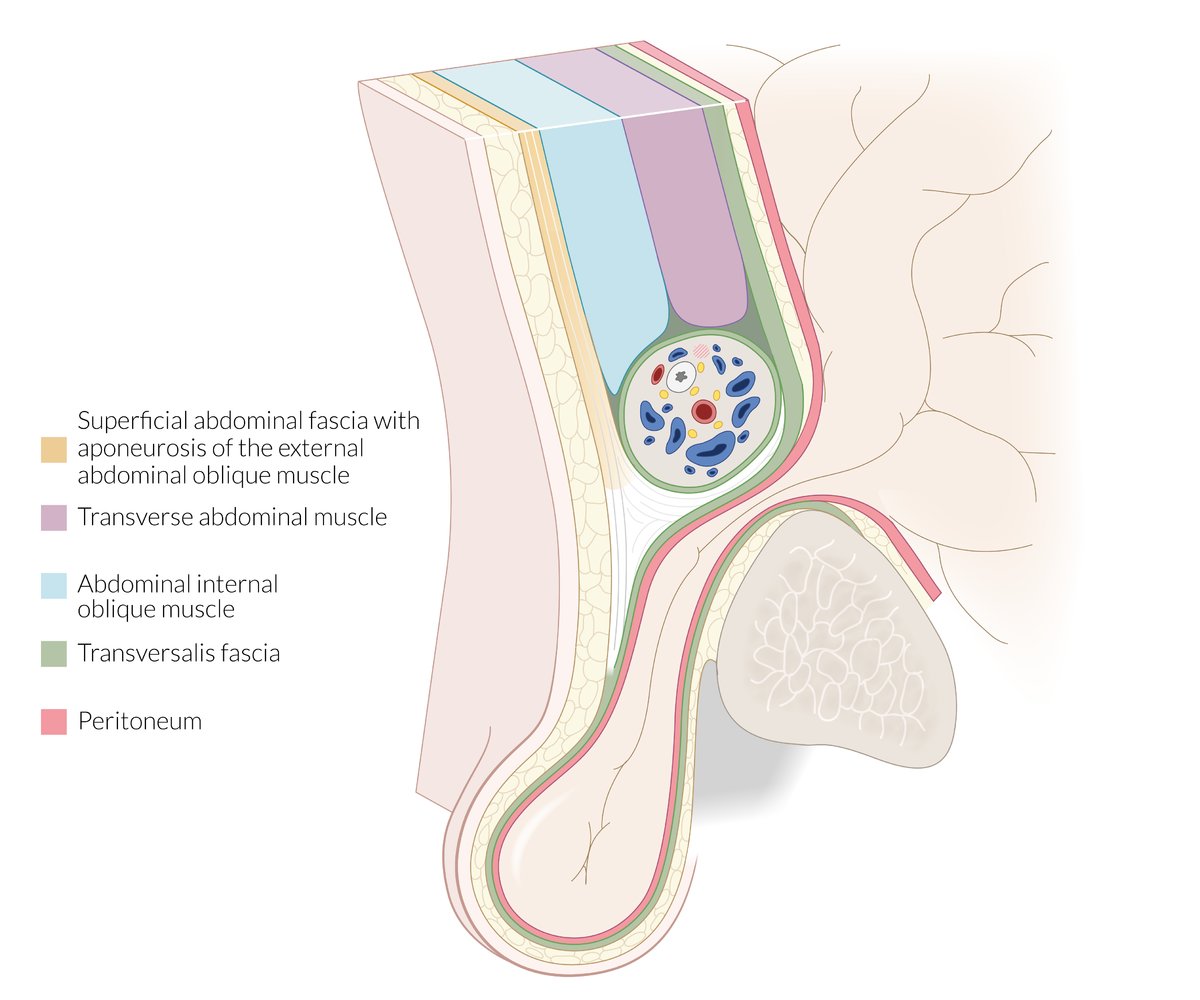
Left illustration: anatomy of the inguinal canal and spermatic cord
The inguinal canal extends from the deep inguinal ring to the superficial ring.
– Anterior wall: aponeurosis of the external abdominal oblique muscle
– Posterior wall: the transversalis fascia
– Roof: the transversalis fascia, transversus abdominis muscles, and the internal oblique muscle
– Floor: inguinal ligament
– Content: in men, the ilioinguinal nerve, genitofemoral nerve, and spermatic cord; in women, the round ligament of the uterus
The spermatic cord contains the vas deferens, three arteries (testicular artery, artery to the ductus deferens, and cremasteric artery), the pampiniform plexus, and the genital branch of the genitofemoral nerve.
Right illustration: the three coverings of the spermatic cord
From superficial to deep, the coverings are the external spermatic fascia (orange), cremasteric fascia (blue), and internal spermatic fascia (green).
© AMBOSS
© AMBOSS
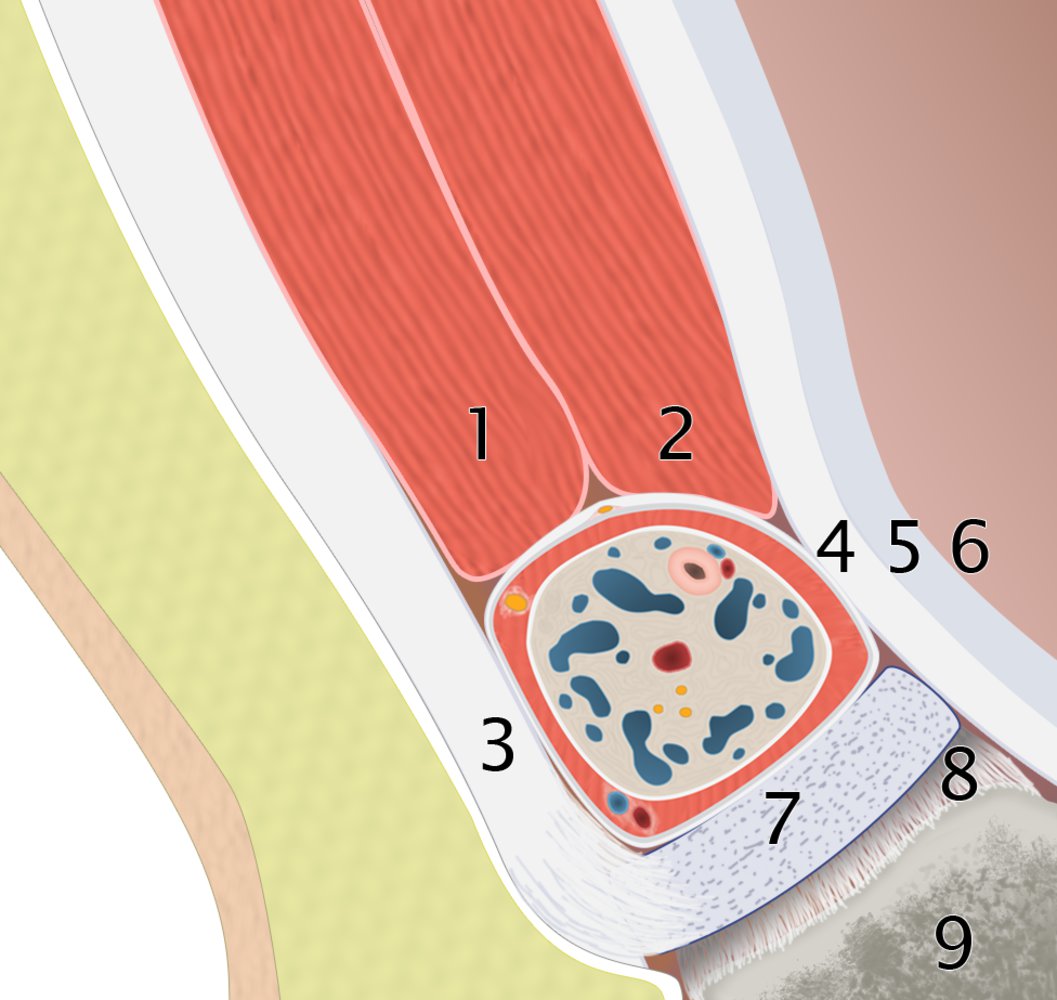
Sagittal plane of the male inguinal area showing the walls of the inguinal canal:
Roof (superior): internal oblique (1) and transversus abdominis (2) muscles;
Anterior wall: external oblique aponeurosis (3) and internal oblique muscle laterally (not shown)
Posterior wall: transversalis fascia (4), conjoint tendon medially (not shown), parietal peritoneum (5), and peritoneal cavity (6);
Floor (inferior): inguinal ligament (7), lacunar ligament (8), and superior pubic ramus (9).
© AMBOSS
© AMBOSS
Pathophysiology
Direct inguinal hernia
- Acquired condition
-
Caused by weakening of the transversalis fascia
- Commonly secondary to conditions resulting in increased intraabdominal pressure (e.g., chronic obstructive pulmonary disease with chronic coughing, constipation)
- May be associated with long-term glucocorticoid use
- Medial to the inferior epigastric blood vessels (within Hesselbach triangle) and lateral to the rectus abdominis
- Hernial sac protrudes directly through the posterior wall of the inguinal canal (without involvement of the spermatic cord or round ligament of the uterus)
- Only herniates through the superficial (external) ring
- Only surrounded by the external spermatic fascia
Indirect inguinal hernia
- Most commonly results from incomplete obliteration of processus vaginalis; during fetal development (but can also be acquired)
- May not become apparent until adulthood despite being present since birth.
- Lateral to the inferior epigastric blood vessels (outside Hesselbach triangle)
- Runs from the deep inguinal ring through the inguinal canal to the superficial (external) inguinal ring (in men, along with the spermatic cord)
- Surrounded by the external spermatic fascia, cremasteric muscle fibers, and internal spermatic fascia
- Indirect inguinal hernia may be associated with a communicating hydrocele.
"The DIRECT path leads through the MiDdle, the INDIRECT path goes beLow." (DIRECT hernias lie MeDial and INDIRECT hernias lie Lateral to the inferior epigastric vessels)
References:[2][3][4][5]
Normally, the only contents of the inguinal canal are the spermatic cord (or round ligament in females) and the ilioinguinal nerve.
Direct inguinal hernia: herniation of intraabdominal contents through the posterior wall of the inguinal canal, medial to the inferior epigastric vessels. The hernial sac lies posteromedial to and outside the spermatic cord
Indirect inguinal hernia: herniation of intraabdominal contents through the deep inguinal ring into the inguinal canal, and, in the case of large inguinal hernia, also through the superficial inguinal ring. The hernial sac lies within the spermatic cord and is therefore covered by the same tissue layers as the spermatic cord.
© AMBOSS
Abdominal and inguinal hernias have three components:
– Hernial sac: parietal peritoneum surrounding the hernial contents
– Hernial contents: typically the omentum and/or loops of small intestine; uncommonly, the large intestine, appendix, bladder, fallopian tubes
– Hernial coverings: layers of the abdominal wall
The hernial orifice is a hiatus (e.g., the umbilicus, deep inguinal ring, posterior wall of the inguinal canal) through which hernial contents herniate. The hernial contents are constricted at the hernial orifice; this constricted area is known as the neck of a hernia.
© AMBOSS
Clinical features
Uncomplicated inguinal hernia [6][7][8]
- Typically manifests as an ill-defined mass in the inguinal region with the following features:
- Increases in size when coughing or straining
- Decreases in size on lying supine
- Inguinal pain; (inguinodynia) or vague inguinal discomfort that increases with physical activity; can also be painless
- Inguinodynia with no palpable groin mass is typically the only manifestation of an occult inguinal hernia. [9]
-
Physical examination
- Ask the patient to perform the Valsalva maneuver and observe for an expansile cough impulse in the inguinal region.
-
Palpate the inguinal canal.
- Male patients: Invaginate the scrotal skin toward the superficial inguinal ring with the index or little finger.
- Female patients: Palpate the area over the inguinal ligament.
- Ask the patient to perform the Valsalva maneuver.
- A palpable bulge confirms the diagnosis of an inguinal hernia.
- The hernia is completely reducible and soft.
Female patients rarely present with visible bulges but often report a sensation of heaviness or dull discomfort in the groin or pelvis that is worsened by lifting, straining, or prolonged standing. [10]

Complicated inguinal hernia [7][8][11]
-
Incarcerated hernia
- The hernia is irreducible.
- Skin overlying the hernia: normal
- Obstructed hernia: : symptoms of mechanical bowel obstruction (sudden onset of pain, nausea, vomiting, abdominal distention, constipation or obstipation)
-
Strangulated hernia
- Sudden, severe groin pain caused by constriction and ischemia (or necrosis) of hernial contents
- Signs of sepsis or signs of shock
- Features of bowel obstruction if the hernia contains intestinal loops
- Skin overlying the hernia: warm, erythematous, tender, and may appear exfoliated or blistered
Manual reduction of an inguinal hernia should not be attempted if there are any signs of strangulated hernia!
Pelvic and inguinal region
There is a pronounced protrusion on the right side (circled). Inguinal hernia can be confirmed with palpation and a cough test.
Source: “Hernia” by James Heilman, MD, Wikimedia Commons, licensed under CC BY-SA 3.0.
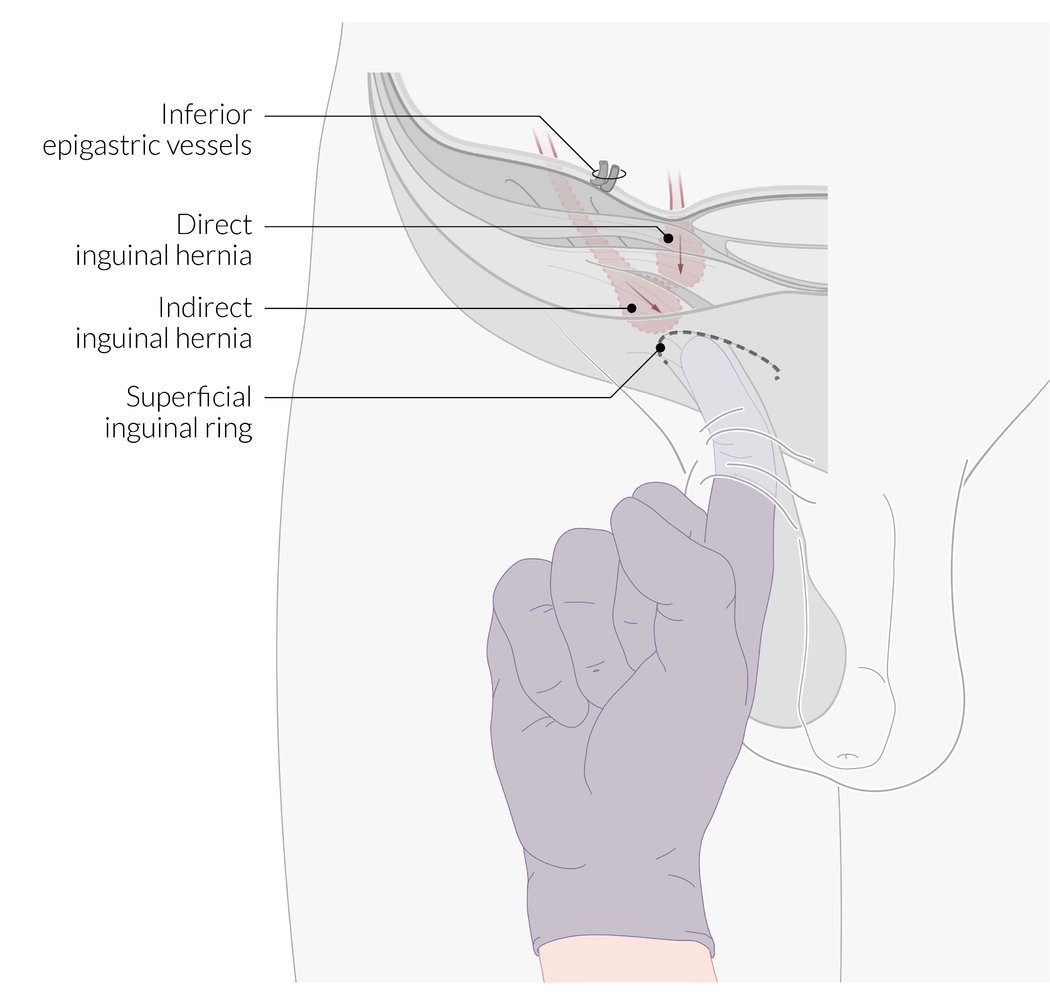
1. Ask the patient to stand up.
2. Palpate from the scrotal skin towards the superficial external inguinal ring.
3. Ask the patient to cough or strain and bear down.
The increase in intraabdominal pressure leads to bulging of an existing inguinal hernia, which can then be felt with the tip of the finger. An indirect inguinal hernia can be palpated from the lateral direction, while a direct inguinal hernia can be palpated cranially.
© AMBOSS
– Reducible hernia: The hernia is easily reducible.
– Irreducible hernia: The hernia is not easily reducible because its contents adhere to the hernial sac.
– Strangulated hernia: ischemia of hernial contents resulting from a tight abdominal wall defect compromising the vascular supply of the hernial contents
© AMBOSS
Diagnosis
Inguinal hernia is typically a clinical diagnosis; however, imaging may be useful if the clinical diagnosis is unclear or to investigate an underlying cause.
Clinical evaluation
-
Medical history should include:
- Identification of typical clinical features (e.g., of uncomplicated inguinal hernia)
- Onset and duration of symptoms [12]
- Evaluation of risk factors for an acquired inguinal hernia.
-
Physical examination should include:
- Palpation of the inguinal canal
- Evaluation for signs of complicated inguinal hernia
- Identification of signs of underlying etiologies, e.g., ascites, BPH
To avoid missing inguinal hernias, routinely examine the inguinal canal in patients with unexplained acute abdominal pain and/or clinical features of bowel obstruction, especially in those with verbal impairment.
Imaging for inguinal hernia [6][13]
Indications
- Uncertain clinical diagnosis
- Suspected recurrent or occult inguinal hernia
- Consider preoperative imaging for complicated inguinal hernia.
Modalities [6]
- First line: ultrasound of the groin [7][13]
- Inconclusive ultrasound findings: CT or MRI abdomen and pelvis
- Complicated inguinal hernia: Consider CT abdomen and pelvis with IV contrast. [11][14]
- Suspected occult inguinal hernia or recurrent inguinal hernia; consider any of the following modalities: [9]
- MRI groin [15]
- Dynamic CT or dynamic MRI, if available
- Herniography [15][16][17]
Supportive findings
- Visualization of the hernial sac with its contents (e.g., bowel, omentum)
-
Uncomplicated inguinal hernia
- Visible expansile cough impulse
- Direct inguinal hernia: fascial defect in the posterior wall of the inguinal canal
- Indirect inguinal hernia: widening of the deep inguinal ring
-
Obstructed hernia [18]
- Free fluid and thickening of bowel wall within the hernial sac
- Dilated bowel loops within the abdomen (see “Radiological signs of mechanical bowel obstruction” for details)
-
Strangulated inguinal hernia [19][20]
- Absence of blood flow to the hernial contents
- Absence of peristalsis in bowel loops within the hernial sac
Do not delay emergency surgery for imaging in unstable patients with signs of strangulated hernia or obstructed hernia. [6]
Laboratory studies [19]
The following tests should be obtained in patients with strangulated inguinal hernia or incarcerated inguinal hernia with bowel obstruction for supportive diagnostic evidence and to assess for complications. [21]
- CBC
- Blood glucose
- Serum electrolytes
- BMP
- Serum lactate
- Urinalysis
Maintain a high index of suspicion for strangulation in patients with an incarcerated hernia and leukocytosis. [12]
Differential diagnoses
Groin or scrotal mass [7][8]
| Overview of inguinal masses | |||||
|---|---|---|---|---|---|
| Etiology | Clinical features | Diagnosis | Treatment | ||
| Inguinal hernia | Direct |
|
|
|
|
| Indirect |
|
||||
| Femoral hernia |
|
|
|||
| Femoral lymphadenopathy |
|
|
|
|
|
| Femoral arteriovenous fistula |
|
|
|
|
|
| Psoas abscess |
|
|
|
|
|
| Femoral artery aneurysm |
|
|
|
|
|
- Hydrocele
- Varicocele
- Spermatocele
- Round ligament varicosities
- Large cutaneous or subcutaneous masses in the inguinal region
- Lipoma
- Sebaceous cyst
- Hematoma
- See also “Overview of scrotal abnormalities.”
A groin bulge with an expansile cough impulse above the inguinal ligament is diagnostic of an inguinal hernia. A femoral hernia typically manifests as a groin bulge below the inguinal ligament and lateral to the pubic tubercle. [8]
Groin pain [7]
If these diagnoses are chronic or recurrent, they may cause inguinodynia.
- Sports hernia: chronic groin pain due to an injury or weakness of the posterior wall of the inguinal canal; an actual hernia may or may not be present [22]
- Muscular strain or injury
- Pathology of the hip joint
- Lumbar disk herniation
- Osteitis pubis
- Neuropathy
- See also: “Causes of pelvic pain”
The differential diagnoses listed here are not exhaustive.
Management
Overview [6][7]
Critically ill patients with complicated inguinal hernias need to be stabilized and evaluated concurrently. Well-appearing patients with easily reducible hernias typically do not need further workup in the emergency department.
-
Complicated inguinal hernias
- Strangulated hernia and/or signs of mechanical bowel obstruction: emergency surgery (within hours)
-
Incarcerated hernia without strangulation: Consider manual reduction of the inguinal hernia.
- Successful manual reduction: Close monitoring is required; consider surgery during the same hospital admission.
- Unsuccessful manual reduction: urgent surgery
- Uncomplicated inguinal hernia: Recommend elective surgery; consider watchful waiting in selected patients.
Strangulated inguinal hernias and obstructed hernias are surgical emergencies.
Initial management and disposition [19][23]
-
All patients
- Assess hernia reducibility.
- Consider ultrasound if the diagnosis is unclear.
- Provide analgesia as needed.
- Reducible hernia: Refer for outpatient surgical management (watchful waiting or elective hernia repair).
-
Incarcerated hernia
- Provide resuscitation as needed; see “ABCDE survey.”
- Assess for signs of obstruction and strangulation.
- Establish NPO status and provide supportive care as needed (e.g., antiemetics, parenteral analgesics, fluid resuscitation, and electrolyte repletion).
- No signs of strangulated hernia: Consider manual reduction of the inguinal hernia as a temporizing measure. [23][24]
- Attempt to reduce the hernia 1–2 times.
- Consider admission or discharge after observation in the emergency department if reduction is successful.
- Consult surgery urgently for operative management if reduction is unsuccessful.
- Signs of strangulated hernia
- Consider broad-spectrum IV antibiotics (see “Empiric antibiotic therapy for intraabdominal infection”). [25][26]
- Consider NG tube insertion for obstructed hernias.
- Consult surgery urgently for operative management; do not attempt manual reduction.
Intestinal infarction can occur within 6 hours of strangulation. [12]
Risk factors associated with poor outcomes in incarcerated and strangulated hernias include older age, obesity (BMI > 30 kg/m2), prolonged duration of symptoms, female sex, and a delayed diagnosis. [6]
Manual reduction of an inguinal hernia
Manual reduction of an inguinal hernia is a bedside procedure where hernia contents are manually guided back into the abdominal cavity through the fascial inguinal defect. [19][23][27]
- Indication: Consider as a temporizing measure before surgery in patients with an incarcerated hernia with or without bowel obstruction.
- Contraindication: strangulated inguinal hernia
-
Preparation
- Informed consent
- NPO, parenteral analgesia, consider procedural sedation
-
Procedure
- Place the patient in the Trendelenburg position.
- Apply an ice pack to the affected area to reduce the swelling.
- Manually guide the hernia through the fascial defect with slow, steady pressure.
-
Successful hernia reduction: Observe the patient for 12–24 hours with serial abdominal examination. [23]
- Symptoms improve: Schedule an elective hernia repair as soon as possible.
- Symptoms worsen: immediate surgical consult to evaluate for recurrence or reduction en masse [28]
- Unsuccessful hernia reduction: urgent surgery (see “Surgeries for inguinal hernia”)
Manual reduction of hernial contents is contraindicated in patients with signs of a strangulated hernia, as necrotic bowel or omentum may be pushed into the abdominal cavity, which can lead to serious complications including peritonitis. [23]
Manual reduction can be performed in patients with an incarcerated inguinal hernia causing bowel obstruction provided there is no evidence of strangulation. [27]
Surgeries for inguinal hernia
- Surgical repair of the hernial defect is the only definitive treatment for inguinal hernia.
- The management of direct inguinal hernia and indirect inguinal hernia does not differ.
- Once the hernial contents are reduced (i.e., returned to the abdominal cavity), the goal of hernia surgery is to reinforce the posterior wall of the inguinal canal with a synthetic mesh or through primary tissue approximation.
- Emergency surgery is associated with an increased risk of complications; elective surgery is preferred when it is an option.
Indications
-
Elective surgery
- Significant inguinodynia limiting daily activities.
- Female patients
- Worsening of symptoms during watchful waiting.
- Patient prefers surgery to watchful waiting.
- Emergency surgery: complicated inguinal hernia
Hernioplasty (mesh repair)
- Definition: repair of a hernial defect using a synthetic mesh
- Indication: gold standard for inguinal hernia repair [6]
-
Open surgery
- Preferred in patients with complicated inguinal hernia or contraindications for laparoscopic repair [8]
- Procedures include Lichtenstein repair, in which a synthetic mesh is placed between the transversalis fascia and the external oblique aponeurosis to reinforce the posterior wall of the inguinal canal. [11]
-
Laparoscopic surgery: preferred in patients with bilateral or recurrent inguinal hernia [8]
- Transabdominal preperitoneal repair (TAPP): laparoscopic, preperitoneal mesh implementation between the parietal peritoneum and transverse fascia
- Total extraperitoneal repair (TEP): laparoscopic, extraperitoneal mesh implementation between parietal peritoneum and transverse fascia

")
")

Herniorrhaphy (non-mesh repair)
- Definition: open surgical repair of a hernial defect using autologous tissue
- Indication: Consider in patients at high risk of surgical site infection. [8][25]
-
Options: Shouldice repair
- A pure tissue repair that involves a multilayer imbricated repair of the posterior wall of the inguinal canal with a continuous running suture technique. [8]
- Preferred procedure when hernioplasty is not feasible
- Has a lower recurrence rate than other non-mesh repairs
- Important consideration: Herniorrhaphy is associated with a greater risk of recurrence than hernioplasty. [29]

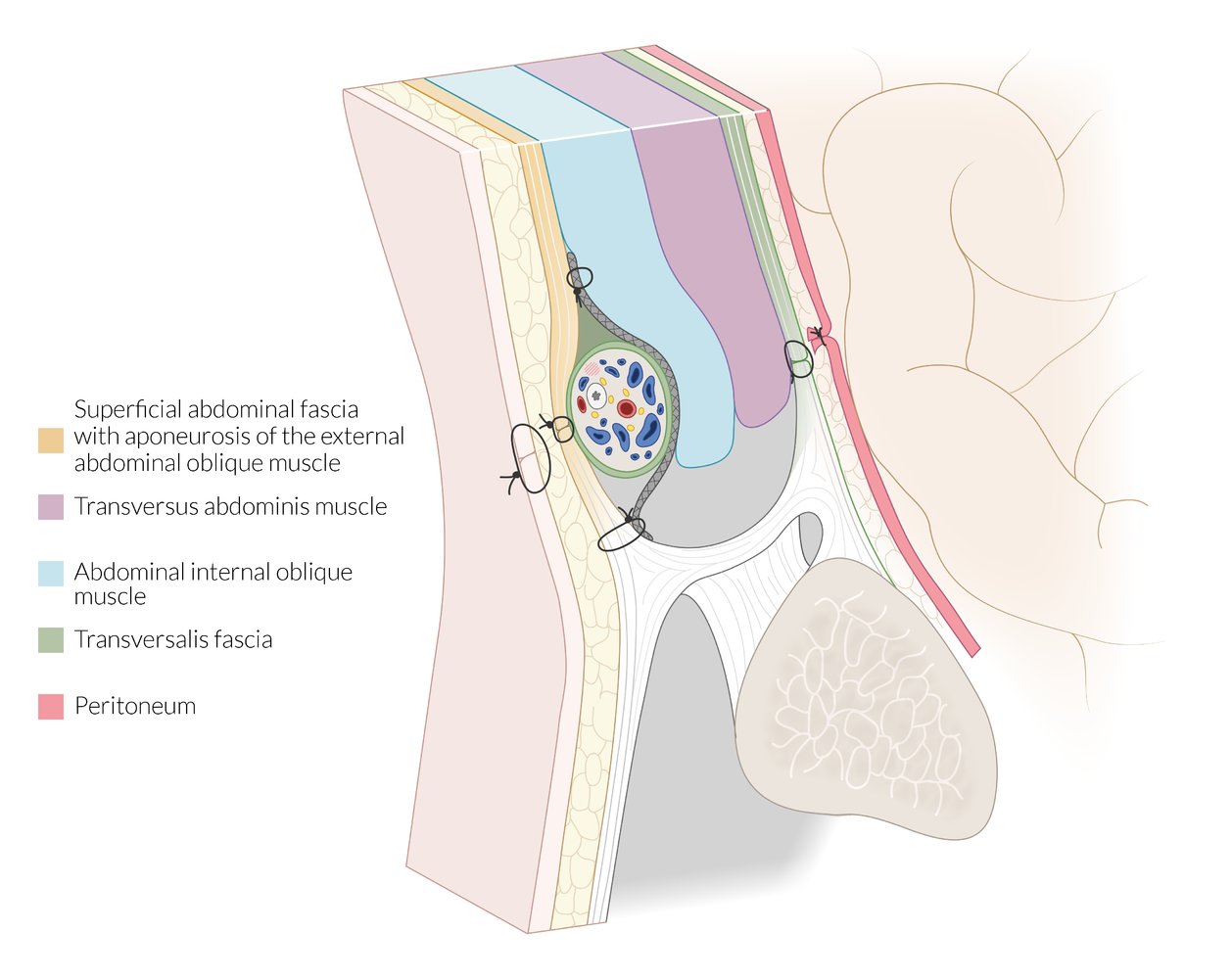
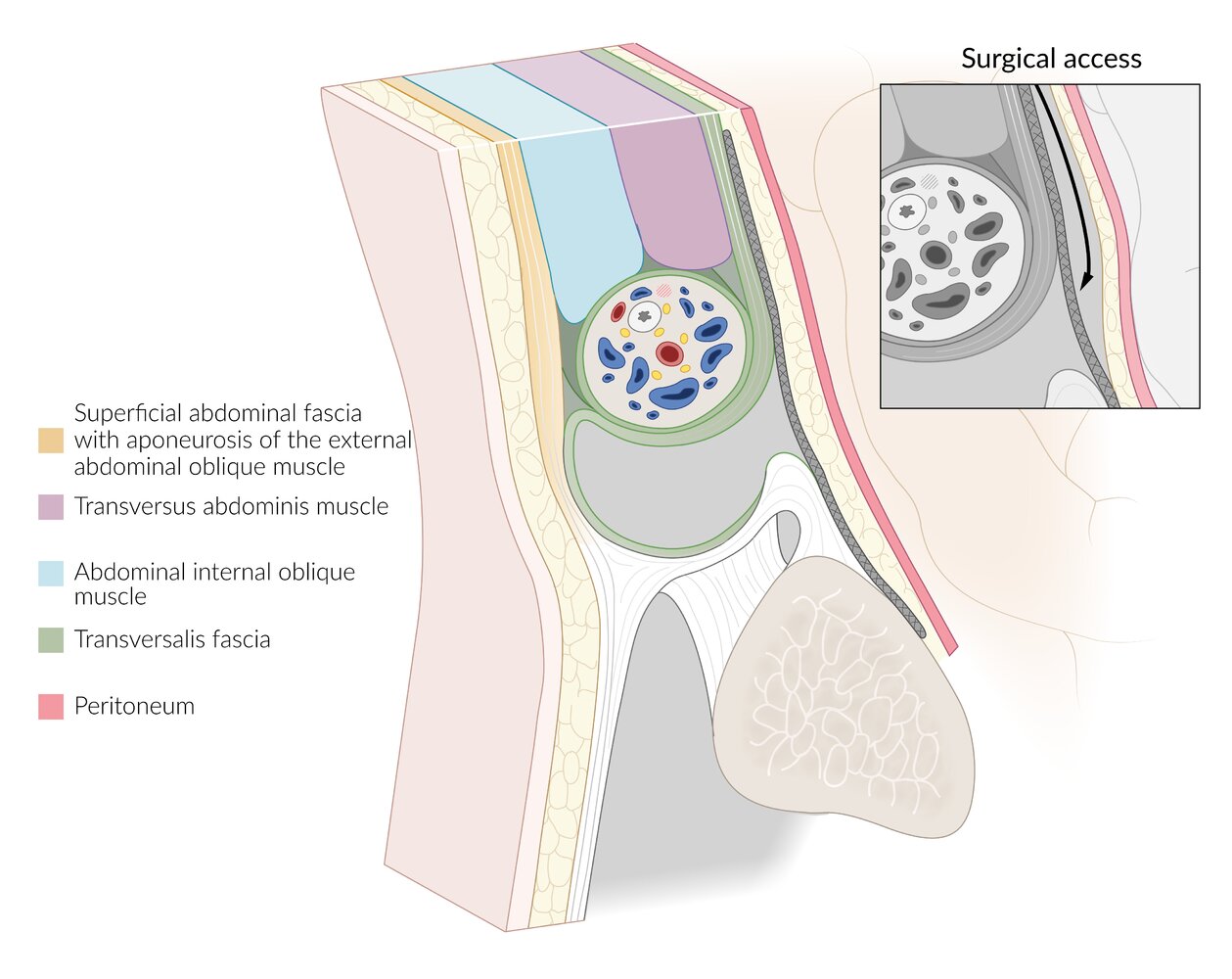
Illustration depicting the inguinal area in a male patient (sagittal view, medial to the epigastric blood vessels)
The Lichtenstein technique is a procedure for tension-free open inguinal hernia repair by implanting a synthetic mesh. After resecting or repositioning the hernial sac, the surgeon closes the parietal peritoneum. A synthetic mesh (gray) is then placed in between the abdominal internal oblique muscle and the external oblique aponeurosis and sutured to both. Closure of the aponeurosis of the external abdominal oblique muscle positions the spermatic cord between this aponeurosis and the mesh.
© AMBOSS
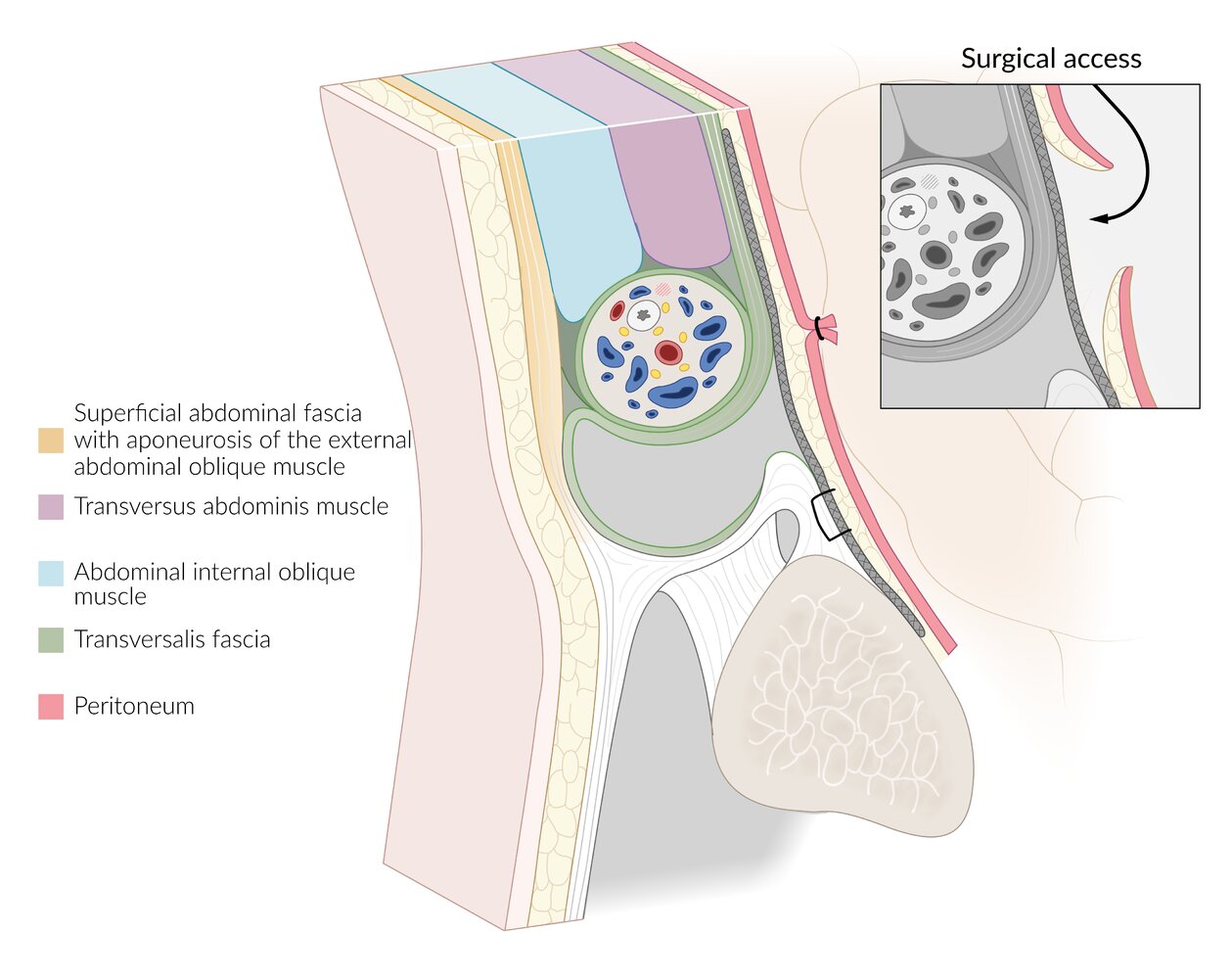
Schematic representation of male inguinal area in sagittal plane, medial to the epigastric blood vessels
The TAPP technique allows for the laparoscopic repair of inguinal hernia. The hernial sac is repositioned into the peritoneal cavity. Next, the parietal peritoneum is opened from the abdominal cavity (arrow). The surgeon then places a synthetic mesh (gray) between the parietal peritoneum and the transverse fascia and closes the parietal peritoneum again, e.g., using suture. The intraabdominal pressure and the counter-pressure of the abdominal muscles stabilize the mesh, which may also be anchored using absorbable clips or fibrin glue.
© AMBOSS
Schematic representation of a male inguinal area in sagittal plane, medial to epigastric blood vessels
The TEP technique allows for laparoscopic, extraperitoneal repair of inguinal hernia using a synthetic mesh.
Following the repositioning of the hernial sac in the peritoneal cavity, the mesh (gray) is placed between the parietal peritoneum and the transverse fascia. Access is minimally invasive and remains preperitoneal, between the parietal peritoneum and transverse fascia (arrow). The intraabdominal pressure and the counter-pressure of the abdominal muscles stabilize the mesh, which may also be anchored using absorbable clips or fibrin glue.
© AMBOSS
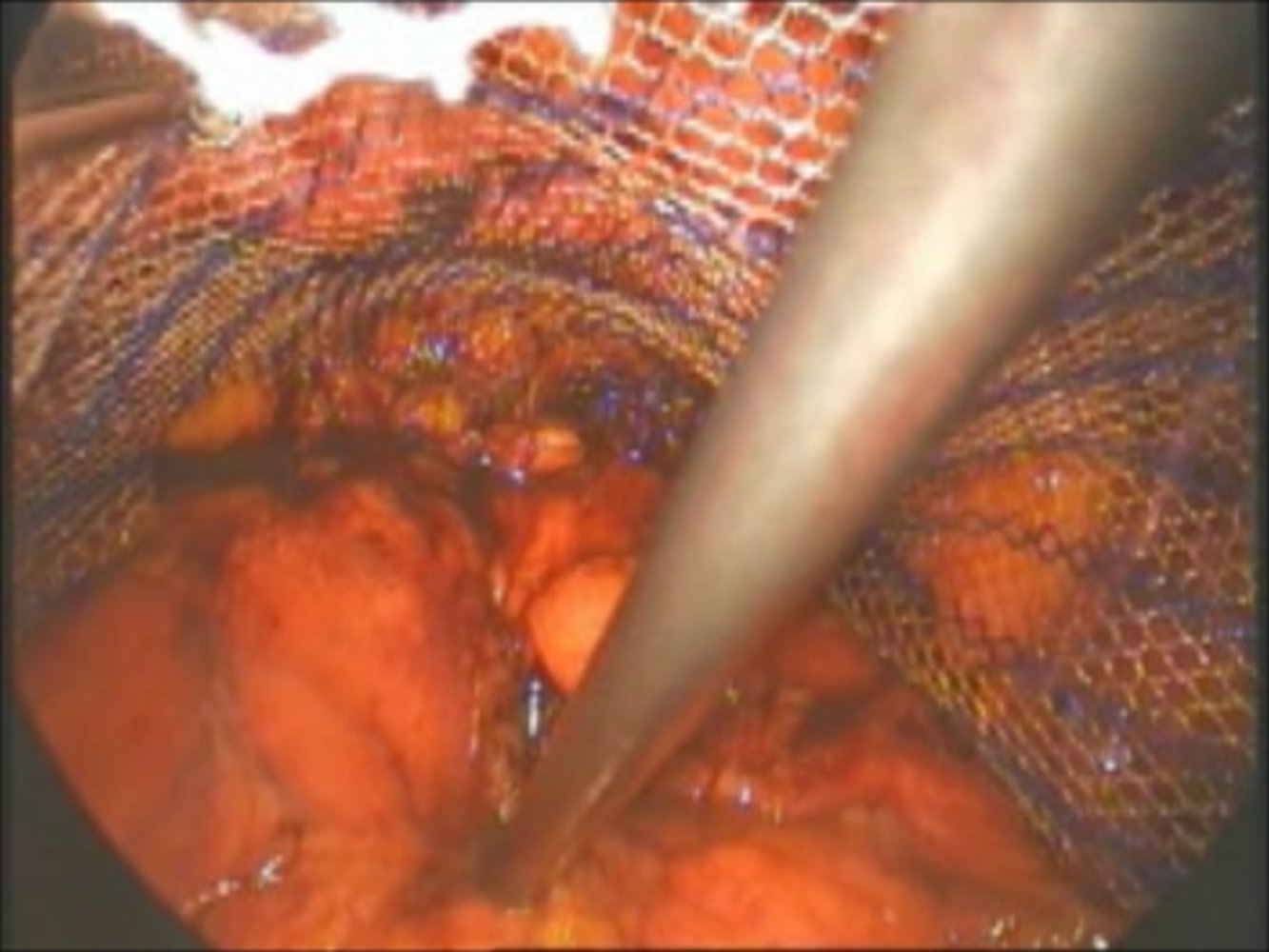
Intraoperative photo taken during a total extraperitoneal repair (TEP) of an inguinal hernia (dorsal view)
The inguinal canal is located ventral to the placed mesh. The right instrument holds back the parietal peritoneum and the bladder, which is located underneath.
Created by: Andreas Plamper, St. Franziskus-Hospital, Köln.
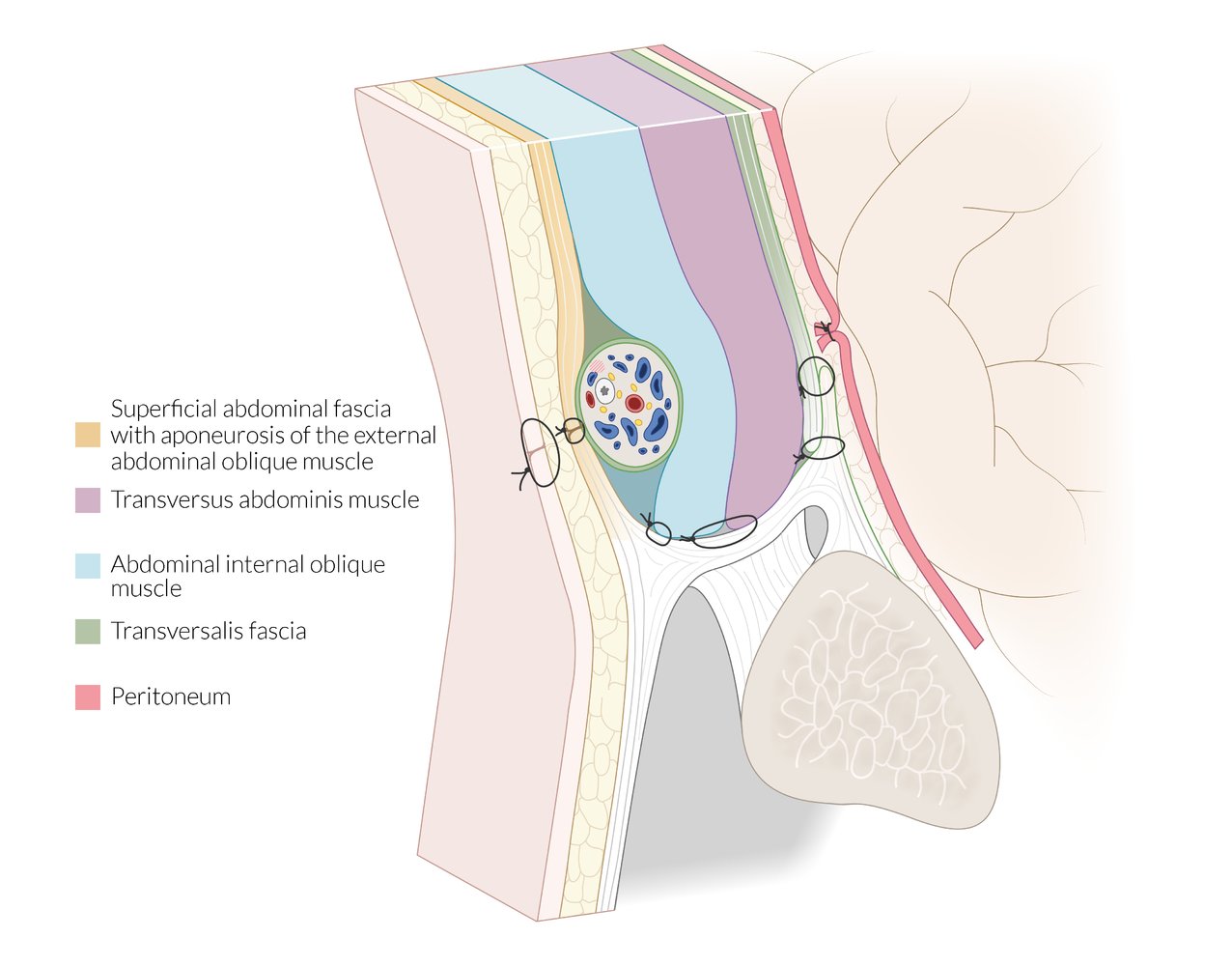
Illustration of the inguinal area in a male patient (sagittal view, medial to the epigastric blood vessels)
The Shouldice technique is a procedure for a tension-free open inguinal hernia repair without placement of a synthetic mesh. After resecting or repositioning the hernial sac in the peritoneal cavity, the surgeon closes the parietal peritoneum. The incised transversalis fascia is positioned so that the upper and lower flap overlap each other, and the flaps are sutured together cranially and anchored to the inguinal ligament caudally. For ventral stabilization, both the abdominal internal oblique muscle and transverse muscle are sutured to the inguinal ligament. Closure of the aponeurosis of the external abdominal oblique muscle positions the spermatic cord between this aponeurosis and abdominal internal oblique muscle.
© AMBOSS
Conservative management
Most patients who are managed conservatively will eventually require surgical repair. [6][19]
-
Indications [30]
- Asymptomatic or minimally symptomatic, completely reducible hernia in a male patient
- Uncomplicated inguinal hernia in patients unfit for surgery or anesthesia
-
Contraindications [6]
- Symptoms significant enough to limit daily activities [30]
- Complicated inguinal hernia
- Female patients
-
General recommendations [6]
- Consider the use of a truss.
- Advise against lifting heavy weights.
- Advise returning to seek care if symptoms worsen. [6]
- Evaluate and treat potential risk factors of hernia.
Management checklist
All patients with inguinal hernia
- Examine the inguinal canal, assessing for hernia reducibility and signs of obstruction and strangulation.
- If signs of strangulated hernia are present, see “Acute management of strangulated inguinal hernia.”
- Order abdominopelvic imaging (e.g., pelvic ultrasound) if the diagnosis is unclear.
- Refer easily reducible uncomplicated inguinal hernias for outpatient elective surgical management.
- Attempt manual reduction of the inguinal hernia if for incarcerated hernias without signs of strangulated hernia (maximum 2 attempts).
- Observe patients with successful manual reduction with serial abdominal examinations (e.g., for 12–24 hours).
- Consult surgery urgently if manual reduction is unsuccessful.
Acute management of strangulated inguinal hernia
- Perform ABCDE assessment.
- Consult surgery immediately and do not attempt manual reduction.
- Establish NPO status.
- Establish IV access and obtain CBC, BMP, lactate, and other studies required for emergency preoperative assessment.
- Administer IV fluids, analgesics, and antiemetics.
- Start empiric antibiotic therapy for intraabdominal infection.
- Consider CT abdomen and pelvis with IV contrast once stable.
- Consider NG tube placement for obstructed hernia.
- Consider Foley catheter placement
Complications
Preoperative complications [6]
- Incarcerated hernia: progression to mechanical bowel obstruction or strangulation of hernia sac contents
-
Strangulated hernia
- Necrosis of bowel or other hernia sac contents
- Gastrointestinal perforation and/or peritonitis
- Systemic inflammatory response syndrome (SIRS)
Postoperative complications [6]
-
Early
- Surgical site infection
- Urinary retention
- Hematoma
- Seroma
- Visceral and vascular injuries (rare)
-
Delayed
- Inguinodynia; paresthesia or anesthesia over the surgical site [31]
- Paresthesia or anesthesia over the surgical site
- Sexual dysfunction
- Recurrence
We list the most important complications. The selection is not exhaustive.
Inguinal hernia in children
Epidemiology
- Incidence: up to 5% in term infants and up to 20% in preterm infants [32][33][34]
- ♂ > ♀ (4–5:1) [33][34]
Etiology [32][33]
-
Anatomical causes
- Indirect (most common): due to a patent processus vaginalis
- Direct (rare in children): due to weakening of the transversalis fascia
-
Risk factors
- Male sex
- Premature birth
- Low birth weight
- Increased intra-abdominal pressure (e.g., from ventriculoperitoneal shunt, ascites)
- Family history
- Connective tissue disease
Clinical features [33]
-
Groin mass
- More common on the right side (in ∼ 60% of patients) [32]
- Increases in size with coughing or crying
- Can extend to the scrotum or labia majora
- May be reducible or incarcerated [32][34]
- Typically painless; large hernias can cause discomfort [32][34]
-
Features of associated conditions may be present, e.g.:
- Nonpalpable testes in cryptorchidism [35]
- Joint hypermobility, skin hyperextensibility in connective tissue disorders (e.g., Ehlers-Danlos syndrome) [33]
- Ambiguous genitalia or palpable testes in phenotypic female individuals with differences of sex development (e.g., androgen insensitivity syndrome) [34]
-
Features suggestive of incarcerated or strangulated hernias [36]
- Similar to those in adults; see "Complicated inguinal hernia."
- Inconsolable crying and fussiness suggests complicated hernia in nonverbal children.
In children, the risk of inguinal hernia incarceration is highest in infancy. [32][34]
Diagnosis [33][34]
- Inguinal hernia is a clinical diagnosis.
- A reducible hernia may be detectable only during crying or coughing.
- Use caregiver reports of intermittent mass in the groin as supportive evidence.
- Laboratory studies and imaging are not routinely indicated.
- Ultrasound may be used in case of diagnostic uncertainty. [33][37]
Management [32][33][34]
Surgery is recommended for all patients as hernia in children is associated with a significant risk of incarceration and, consequently, strangulation.
-
Reducible hernia [34]
- Refer to a specialist (e.g., pediatric surgery, pediatric urology) for elective surgery.
- Timing of surgery [32][33]
- Premature neonates: Surgery performed after discharge from neonatal ICU may be associated with optimal outcomes. [33][38]
- Older infants and children: Timing depends on patient factors such as risk of incarceration. [32]
-
Incarcerated hernia [33][34][36]
- Perform manual reduction of the inguinal hernia; sedation or analgesia may be required.
- Consult a specialist for urgent surgery.
- Timing of surgery
- Irreducible hernia: emergency surgery [36]
- Successful manual reduction: typically during the same admission (within 24 hours to 5 days) to minimize risk of recurrent incarceration [39][40]
-
Strangulated hernia
- Immediate referral for surgery.
- Initiate management for pain and associated complications (e.g., bowel obstruction, shock).
- Manual reduction is contraindicated.
Hernia surgery in children [33][36]
- Herniorrhaphy is typically performed; mesh repair (hernioplasty) may be considered in selected patients.
- Surgery can be performed using an open or laparoscopic approach. [32][41]
- Evaluation for contralateral hernia during surgery is controversial. [32][33][34]
- Counsel patients and/or caregivers on the small risk of recurrence. [32][36]
External Resources
- 2023 Assessment and Management of Inguinal Hernias in Children url::
- 2018 HerniaSurge Guidelines for Groin Hernia Management
- 2015 IEHS Update of Guidelines on TAPP and TEP Treatment of Inguinal Hernias
- 2013 EAES Consensus on Endoscopic Repair of Groin Hernias
- 2009 EHS Guidelines on Inguinal Hernia Treatment
References
- Brooks DC, Hawn M. "Classification, clinical features and diagnosis of inguinal and femoral hernias in adults". UpToDate. UpToDate. https://www.uptodate.com/contents/classification-clinical-features-and-diagnosis-of-inguinal-and-femoral-hernias-in-adults. [2016-02-04]
- Rather AA. "Abdominal Hernias". WebMD. http://emedicine.medscape.com/article/189563. [2015-12-01]
- HerniaSurge Group. "International guidelines for groin hernia management". Hernia. 22(1). :1-165. (2018)
- LeBlanc KE, LeBlanc LL, LeBlanc KA. "Inguinal hernias: diagnosis and management". Am Fam Physician. 87(12). :844-8. (2013)
- Townsend CM Jr, Beauchamp RD, Evers BM, Mattox KL. "Sabiston Textbook of Surgery: The Biological Basis of Modern Surgical Practice". Elsevier. (2016). ISBN: 9780323299879
- Miller J, Cho J, Michael MJ, Saouaf R, Towfigh S. "Role of imaging in the diagnosis of occult hernias.". JAMA surgery. 149(10). :1077-80. (2014)
- Towfigh S. "Obscure Groin Pain in Women". Springer Milan. :181-186. (2017). ISBN: 9788847039469
- Towfigh S, Shafik Y. "Textbook of Hernia". Springer. (2017)
- Shirin Towfigh. "Emergency General Surgery". Springer International Publishing. :377-385. (2019). ISBN: 9783319962856
- Piga E, Zetner D, Andresen K, Rosenberg J. "Imaging modalities for inguinal hernia diagnosis: a systematic review". Hernia. (2020)
- Jacobson JA, Khoury V, Brandon CJ. "Ultrasound of the Groin: Techniques, Pathology, and Pitfalls". American Journal of Roentgenology. 205(3). :513-523. (2015)
- Murphy KP, O’Connor OJ, Maher MM. "Adult Abdominal Hernias". American Journal of Roentgenology. 202(6). :W506-W511. (2014)
- Ng TT, Hamlin JA, Kahn AM. "Herniography: analysis of its role and limitations.". Hernia. 13(1). :7-11. (2009)
- Heise CP, Sproat IA, Starling JR. "Peritoneography (herniography) for detecting occult inguinal hernia in patients with inguinodynia.". Ann Surg. 235(1). :140-4. (2002)
- Rettenbacher T, Hollerweger A, Macheiner P, et al. "Abdominal wall hernias: cross-sectional imaging signs of incarceration determined with sonography.". AJR Am J Roentgenol. 177(5). :1061-6. (2001)
- Tintinalli JE, Stapczynski JS, Ma OJ, et al. "Tintinalli's Emergency Medicine: A Comprehensive Study Guide, 9th edition". McGraw Hill Professional. (2019). ISBN: 9781260019940
- Stavros AT, Rapp C. "Dynamic ultrasound of hernias of the groin and anterior abdominal wall.". Ultrasound Q. 26(3). :135-69. (2010)
- Montagnana M, Danese E, Lippi G. "Biochemical markers of acute intestinal ischemia: possibilities and limitations.". Annals of translational medicine. 6(17). :341. (2018)
- Sheen AJ, Stephenson BM, Lloyd DM, et al. "‘Treatment of the Sportsman's groin’: British Hernia Society's 2014 position statement based on the Manchester Consensus Conference". Br J Sports Med. 48(14). :1079-1087. (2013)
- Birindelli A, Sartelli M, Di Saverio S, et al. "2017 update of the WSES guidelines for emergency repair of complicated abdominal wall hernias". World Journal of Emergency Surgery. 12(1). (2017)
- Niebuhr H, Köckerling F. "Surgical risk factors for recurrence in inguinal hernia repair - a review of the literature". Innovative surgical sciences. 2(2). :53-59. (2017)
- Hakeem A, Shanmugam V. "Current trends in the diagnosis and management of post-herniorraphy chronic groin pain". World journal of gastrointestinal surgery. 3(6). :73-81. (2011)
- Khan F, Jancelewicz T, Kieran K, et al. "Assessment and Management of Inguinal Hernias in Children". Pediatrics. 152(1). (2023)
- Rosenberg J, Baig S, Chen D, Derikx J. "Groin hernia". Nat Rev Dis Primers. 11(1). (2025)
- Grant A, Carpenter C. "Advances in Pediatric Inguinal Hernia and Hydrocele Repair: A Comprehensive Review". Curr Treat Options Pediatr. 10(4). :203-212. (2024)
- Kolon TF, Herndon CDA, Baker LA, et al. "Evaluation and Treatment of Cryptorchidism: AUA Guideline". J Urol. 192(2). :337-345. (2014)
- Abdulhai S, Glenn I, Ponsky T. "Incarcerated Pediatric Hernias". Surg Clin North Am. 97(1). :129-145. (2017)
- Basta A, Courtier J, Phelps A, Copp H, MacKenzie J. "Scrotal Swelling in the Neonate". J Ultrasound Med. 34(3). :495-505. (2015)
- HIP Trial Investigators, Blakely M, Krzyzaniak A, et al. "Effect of Early vs Late Inguinal Hernia Repair on Serious Adverse Event Rates in Preterm Infants". JAMA. 331(12). :1035. (2024)
- Ramsey W, Huerta C, O’Neil C, et al. "Timing of Pediatric Incarcerated Inguinal Hernia Repair: A Review of Nationwide Readmissions Data". J Surg Res. 295. :641-646. (2024)
- Abdulhai S, Glenn I, Ponsky T. "Inguinal Hernia". Clin Perinatol. 44(4). :865-877. (2017)
- Davies D, Rideout D, Clarke S. "The International Pediatric Endosurgery Group Evidence-Based Guideline on Minimal Access Approaches to the Operative Management of Inguinal Hernia in Children". J Laparoendosc Adv Surg Tech A. 30(2). :221-227. (2020)
- Le T, Bhushan V, Sochat M, et al. "First Aid for the USMLE Step 1 2014". McGraw-Hill Medical. (2014). ISBN: 9780071831420
- Jiang ZP, Yang B, Wen LQ, et al. "The etiology of indirect inguinal hernia in adults: congenital or acquired?". Hernia. 19(5). ::697-701. (2015)
- Townsend CM, Beauchamp RD, Evers BM, Mattox KL. "Sabiston Textbook of Surgery: The Biological Basis of Modern Surgical Practice". Elsevier. (2021). ISBN: 9780323640626
- Yeh DD, Alam HB. "Hernia emergencies". Surg Clin North Am. 94(1). :97-130. (2014)
- Pawlak M, East B, de Beaux AC. "Algorithm for management of an incarcerated inguinal hernia in the emergency settings with manual reduction. Taxis, the technique and its safety". Hernia. 25(5). :1253-1258. (2021)
- Wong PF, Gilliam AD, Kumar S, et al. "Antibiotic regimens for secondary peritonitis of gastrointestinal origin in adults". Cochrane Database of Systematic Reviews. (2005)
- East B, Pawlak M, de Beaux AC. "A manual reduction of hernia under analgesia/sedation (Taxis) in the acute inguinal hernia: a useful technique in COVID-19 times to reduce the need for emergency surgery-a literature review". Hernia. 24(5). :937-941. (2020)
- Yatawatta A. "Reduction en masse of inguinal hernia: a review of a rare and potential fatal complication following reduction of inguinal hernia". BMJ case reports. 2017. (2017)
- Montgomery J, Dimick JB, Telem DA. "Management of Groin Hernias in Adults-2018.". JAMA. 320(10). :1029-1030. (2018)
- Kim B, Robinson P, Modi H, et al. "Evaluation of the usage and influence of groin ultrasound in primary and secondary healthcare settings.". Hernia. 19(3). :367-71. (2015)
- Köckerling F, Schug-Pass C. "Diagnostic Laparoscopy as Decision Tool for Re-recurrent Inguinal Hernia Treatment Following Open Anterior and Laparo-Endoscopic Posterior Repair.". Frontiers in surgery. 4. :22. (2017)
- Miller J, Tregarthen A, Saouaf R, Towfigh S. "Radiologic Reporting and Interpretation of Occult Inguinal Hernia.". J Am Coll Surg. 227(5). :489-495. (2018)
- Miserez M, Alexandre JH, Campanelli G, et al. "The European hernia society groin hernia classification: simple and easy to remember.". Hernia. 11(2). :113-6. (2007)
- Ekberg O. "Inguinal herniography in adults: technique, normal anatomy, and diagnostic criteria for hernias.". Radiology. 138(1). :31-6. (1981)
- Burkhardt JH, Arshanskiy Y, Munson JL, Scholz FJ. "Diagnosis of inguinal region hernias with axial CT: the lateral crescent sign and other key findings.". Radiographics. 31(2). :E1-12
- Revzin MV, Ersahin D, Israel GM, et al. "US of the Inguinal Canal: Comprehensive Review of Pathologic Processes with CT and MR Imaging Correlation.". Radiographics. 36(7). :2028-2048. (2016)
- Ijpma FFA, Boddeus KM, de Haan HH, van Geldere D. "Bilateral round ligament varicosities mimicking inguinal hernia during pregnancy". Hernia. 13(1). :85-88. (2008)