Summary
Inhalational anesthetics are used for the induction and maintenance of general anesthesia as well as sedation. The exact mechanisms by which they act are still unknown. The most common inhalational anesthetics are sevoflurane, desflurane, and nitrous oxide. Of these, sevoflurane is the most common because of its rapid onset of action and the fact that patients recover quickly from it. Inhalational anesthetics cause respiratory depression, a decrease in arterial blood pressure and cerebral metabolic demand, and an increase in cerebral blood flow. While side effects differ based on the substance (e.g., halothane can cause hepatotoxicity), the most common side effect is nausea.
Overview
| Overview of inhalational anesthetics | |||||
|---|---|---|---|---|---|
| Agents | Indications | Mechanism of action | Adverse effects | ||
| Nitrous oxide |
|
|
|
|
|
| Desflurane |
|
||||
| Sevoflurane |
|
||||
| Isoflurane |
|
||||
| Enflurane |
|
||||
| Halothane |
|
||||
| Methoxyflurane |
|
||||
Pharmacokinetics and pharmacodynamics
Pharmacokinetic principles
-
Uptake into the blood: inhalational anesthetics are taken up passively via diffusion, which depends on:
- Blood solubility of the anesthetic
- Blood-gas partition coefficient: the ratio of anesthetic concentrations in the blood and alveolar space when partial pressures in the two compartments are equal
- The higher the blood-gas partition coefficient of an inhalational anesthetic, the higher the solubility of that substance in the blood.
- Lung ventilation, volumes, and perfusion
- Blood solubility of the anesthetic
-
Distribution and uptake into the brain: Transport to and uptake into the brain depend on cerebral perfusion and the fat solubility of the inhalational anesthetic.
- Brain-blood partition coefficient: the ratio of anesthetic concentrations between brain tissue and blood when partial pressures are equal. The higher the brain-blood partition coefficient, the higher the solubility of the anesthetic in brain tissue
- Onset of effect: : The lower the blood-gas partition coefficient of an inhalational anesthetic, the faster the substance takes effect (less induction time)
-
Elimination
- Inhalational anesthetics are eliminated by the lungs
- The lower the blood-gas partition coefficient of an inhalational anesthetic, the faster the effect ceases (less recovery time)
- Inhalational anesthetics are metabolized only to a small degree
- Exception: halothane is metabolized in the liver
- With prolonged duration of anesthesia in obese patients, inhalational anesthetics with a high fat solubility can accumulate in adipose tissue and slow down recovery from anesthesia (increased context-sensitive half-life).
- Inhalational anesthetics are eliminated by the lungs


Pharmacodynamic principles
-
Measure of potency of inhalational anesthetics: minimum alveolar concentration (MAC)
- MAC is the fraction of volume of the anesthetic present in the inspired air that provides sufficient analgesia in 50% of patients, meaning that patients will not respond to an extremely painful stimulus such as surgical skin incision.
- MAC is inversely related to anesthetic potency (potency = 1/MAC) and represents the ED50 value.
-
The lower the MAC value, the more fat soluble the anesthetic. For example:
- Halothane has a slow induction and high potency because of its high lipid and blood solubility.
- Nitrous oxide (N2O), in contrast, has a fast induction and low potency due to low lipid and blood solubility.
Pharmacokinetics and pharmacodynamics of common inhalational anesthetics
| Blood-gas partition coefficient | Brain-blood partition coefficient | Minimum alveolar concentration (MAC) | |
|---|---|---|---|
| Nitrous oxide |
|
|
|
| Desflurane |
|
|
|
| Sevoflurane |
|
|
|
| Isoflurane |
|
|
|
| Enflurane |
|
|
|
| Halothane |
|
|
|
References:[3][4][5][6]
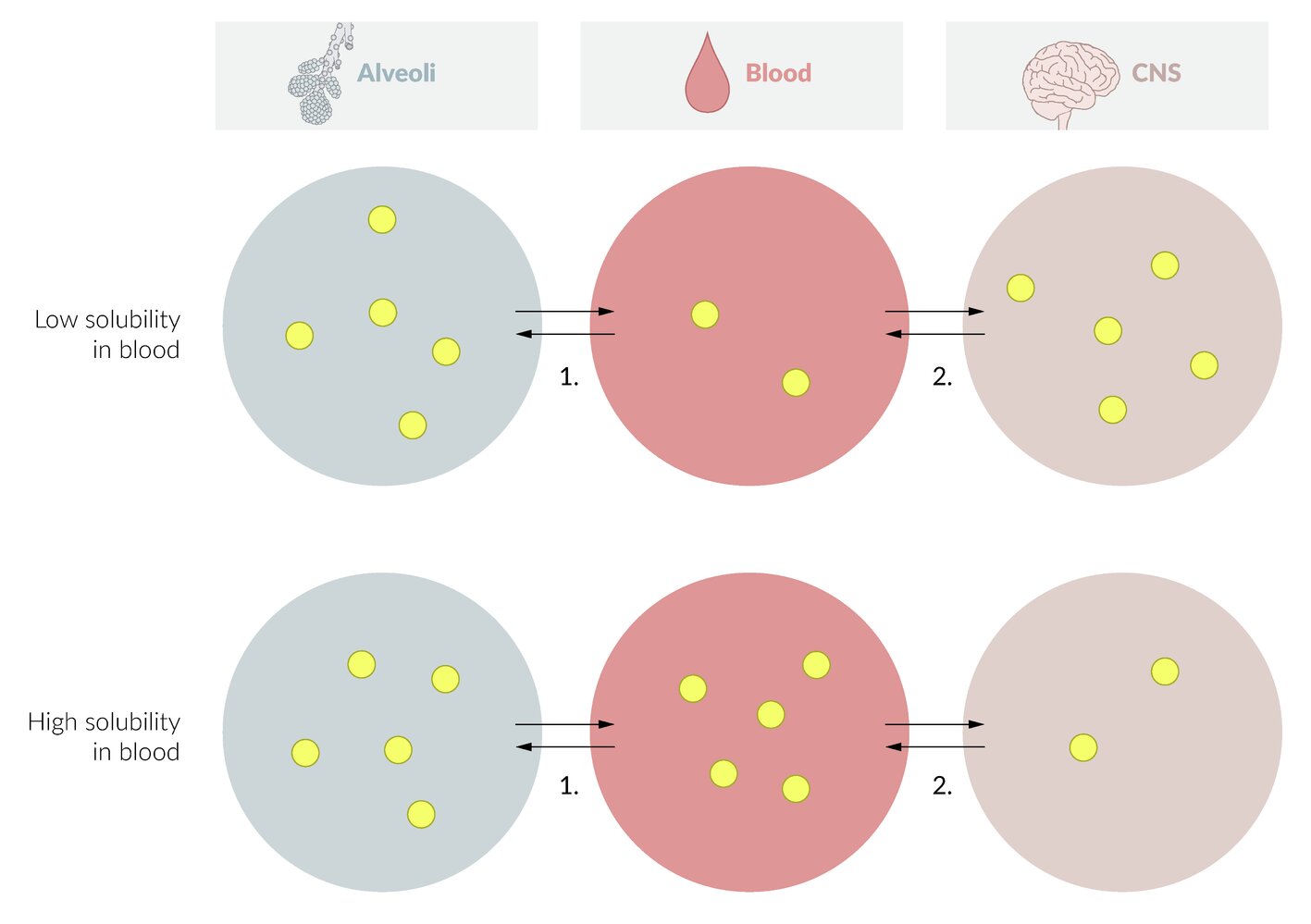
The relationship between blood solubility and rate of onset can be illustrated using the three-compartment model which considers the distribution of the inhalation anesthetic in the lung, blood, and central nervous system (CNS). Yellow circles represent the concentration of the inhalation anesthetic in the respective compartment.
Top: When blood solubility is low, the substance dissolves poorly in the blood. Accordingly, this compartment is quickly saturated and the inhalation anesthetic can thus pass to the next compartment (CNS).
Bottom: When blood solubility is high, the substance dissolves easily in the blood. Accordingly, it takes longer for this compartment to be saturated and for the anesthetic to transfer to the next compartment (CNS). The onset of effect is thus delayed.
This figure is highly simplified and does not include other factors influencing the onset of effect, e.g.
- factors influencing the transition from the alveolar air to blood: partial pressure of the inhalation anesthetic in the inspiratory gas, fresh gas flow, alveolar ventilation, blood-gas partition coefficient, and cardiac output.
- factors influencing the transition from blood to brain: brain-blood partition coefficient and perfusion of the brain.
© AMBOSS
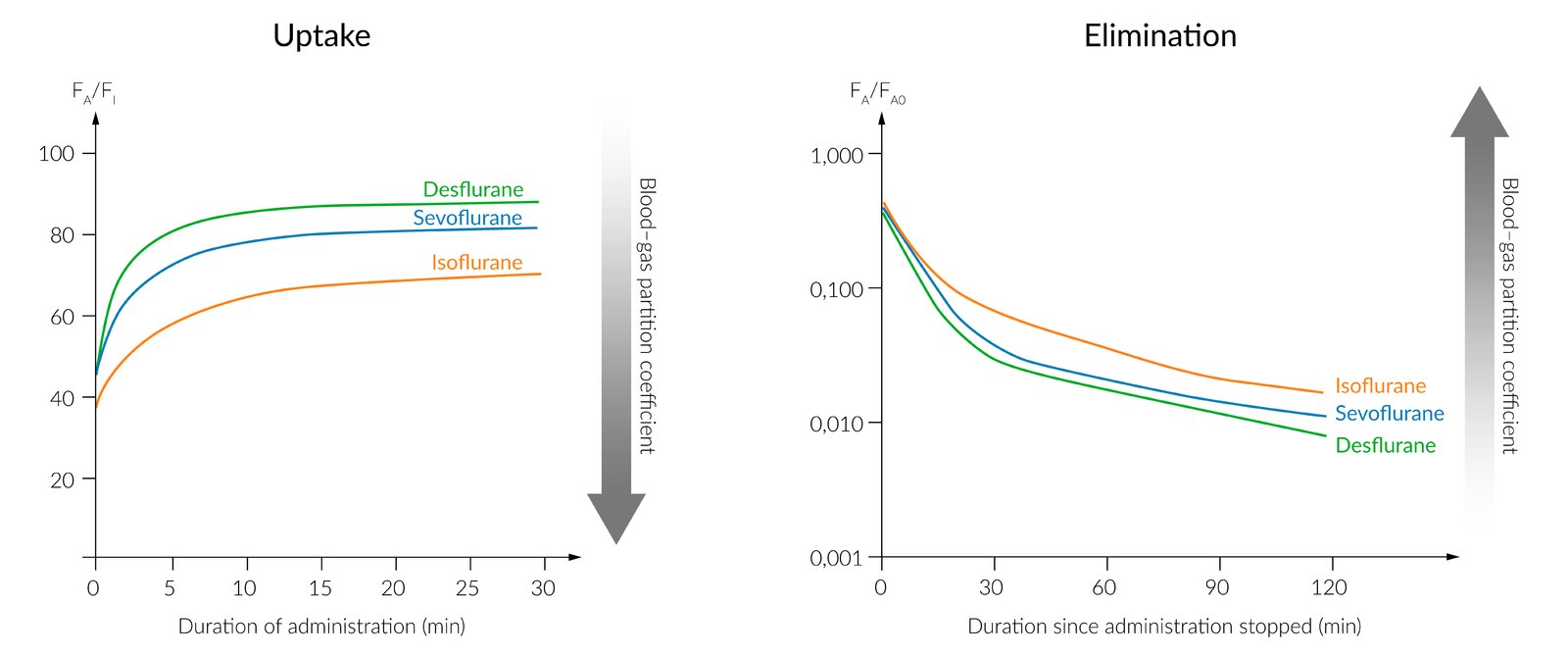
The figure shows the uptake (left) and elimination (right) of the clinically most relevant inhalational anesthetics, relating it to the blood-gas partition coefficients. With regard to the depth of anesthesia, inhalational anesthetics with rapid uptake and elimination are more controllable.
Left: The x-axis represents the duration of the administration of inhalational anesthetics. The y-axis represents the ratio of the alveolar concentration (FA) to inspiratory concentration (FI) which increases more or less rapidly, depending on the type of anesthetic. The speed of uptake increases with decreasing blood-gas partition coefficients.
Right: The x-axis represents the time since the termination of anesthetic administration. The y-axis represents the ratio of the alveolar concentration (FA) to the alveolar concentration immediately prior to the termination of its application (FA0). The speed of elimination increases with decreasing blood-gas partition coefficients.
© AMBOSS
Pharmacodynamics
General effects
- Anesthesia
- Sedation/narcosis
- ↓ Respiration
- ↓ Arterial blood pressure
- Myocardial depression
- ↓ Cerebral metabolic demand
- ↑ Cerebral blood flow
- ↑ ICP
- Postoperative: nausea and vomiting
Specific characteristics of common inhalational anesthetics
| Specific characteristics | |
|---|---|
| Nitrous oxide |
|
| Desflurane |
|
| Sevoflurane |
|
| Isoflurane |
|
| Methoxyflurane |
|
| Enflurane |
|
| Halothane |
|
References:[4]
Adverse effects
General side effects
- Postoperative nausea and vomiting [7]
- Risk of malignant hyperthermia (except nitrous oxide)
- Postoperative shivering
Side effects of specific substances
-
Nitrous oxide
- Can diffuse into gas-filled body compartments and cause expansion of the gas present there → potential damage to organs/tissues
- Causes mild myocardial depression and increases pulmonary vessel resistance
-
Desflurane [8]
- ↓ Systemic vascular resistance → hypotension
- Cardiac output is well-preserved.
- High concentrations → transient stimulation of the sympathetic nervous system → possible tachycardia, hypertension, and dysrhythmias
-
Sevoflurane
- Interacts with soda lime → nephrotoxic breakdown products (known as compounds A–E)
- ↓ Minute ventilation [8]
-
Isoflurane
- ↑ Intracranial pressure
- Nausea and vomiting (postoperatively)
- Malignant hyperthermia
- Methoxyflurane: nephrotoxic
- Enflurane: proconvulsive
-
Halothane: hepatotoxic → halothane hepatitis [9]
- Pathophysiology: underlying mechanism not fully understood
- Clinical features
- Occurs 2 days to 3 weeks after halothane exposure
- Signs of acute hepatitis (e.g., jaundice, fever, vomiting, hepatomegaly)
- Rash, arthralgias
- Diagnostics: diagnosis of exclusion
- Possible laboratory findings: ↑ eosinophils, ↑ serum transaminases ; , ↑ bilirubin, ↑ alkaline phosphatase
- Biopsy shows massive centrilobular hepatic necrosis
- Treatment: depending on the severity of liver damage, ranges from supportive treatment to liver transplantation [10]
References:[4][7][9][11]
We list the most important adverse effects. The selection is not exhaustive.
References
- "ULTANE® (sevoflurane) volatile liquid for inhalation"
- "FORANE (isoflurane, USP) Liquid For Inhalation"
- Katzung B, Trevor A. "Basic and Clinical Pharmacology". McGraw-Hill Education. (2014). ISBN: 9780071825054
- ASA. "Practice guidelines for preoperative fasting and the use of pharmacologic agents to reduce the risk of pulmonary aspiration: Application to healthy patients undergoing elective procedures". Anesthesiology. 114(3). :495-511. (2011)
- Brunton L. "Goodman and Gilman's The Pharmacological Basis of Therapeutics, 13th Edition". McGraw-Hill Education / Medical. (2017). ISBN: 9781259584732
- "Drug record - Halothane". https://livertox.nih.gov/Halothane.htm
- "Halothane Hepatotoxicity". http://emedicine.medscape.com/article/166232-overview. [2016-10-17]
- Eger EI II. "Characteristics of anesthetic agents used for induction and maintenance of general anesthesia". Am J Health Syst Pharm. 61(20). (2004)
- Le T, Bhushan V. "First Aid for the USMLE Step 1 2015". McGraw-Hill Education. (2014). ISBN: 9780071840071
- King A, Weavind LM, Joshi GP, Nussmeier NA. "General Anesthesia: Induction". UpToDate. UpToDate. https://www.uptodate.com/contents/general-anesthesia-induction. [2017-09-07]
- Wenker OC. "Review of Currently Used Inhalation Anesthetics; Part I". The Internet Journal of Anesthesiology. 2(3). (1999)