Quick guide
Diagnostic approach
- ABCDE survey
- GCS
- Neurological exam
- CT head without contrast
- CBC
- Coagulation studies
- POC glucose
")
Red flag features
- GCS score ≤ 8
- Signs of brain herniation
- Altered mental status
- Severe headache
- Symptoms of increased ICP
- Focal neurological deficit
- CT findings (e.g., midline shift, intraventricular extension)
Management checklist
- Continuous monitoring of heart rate, BP, and SpO2
- Airway management
- If SBP > 220 mm Hg, lower to 140–180 mm Hg with nicardipine and/or labetalol.
- Stop anticoagulants and antiplatelet agents.
- Administer anticoagulant reversal agents if INR > 1.4.
- Initiate neuroprotective measures.
- ICP management as needed
- Consult neurosurgery and neurology.
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
Summary
Intracerebral hemorrhage (ICH) refers to bleeding within the brain parenchyma. The term should not be confused with intracranial hemorrhage, which is a broader term that encompasses bleeding within any part of the skull, i.e., extradural, subdural, subarachnoid, or intracerebral bleeding. The most significant risk factor for spontaneous ICH is arterial hypertension. Symptoms are often nonspecific (e.g., headache); however, depending on the affected vessel and cerebral region, focal neurological deficits (e.g., hemiparesis) may occur. Compared with ischemic stroke, patients with ICH are more likely to present with severe headache and have rapidly progressing symptoms. The initial imaging investigation of choice is CT head without contrast, which typically shows a hyperdense mass lesion. Treatment involves management of the underlying and associated conditions (e.g., controlling hypertension, reversing coagulopathy) in order to limit hematoma expansion and prevent secondary brain injury. In severe cases, neurosurgical intervention may be required. Approximately half of patients with spontaneous ICH die within 30 days of symptom onset. Traumatic ICH may result from traumatic brain injury (TBI) and is managed similarly to spontaneous ICH.
See also “Overview of intracranial hemorrhage” and “Overview of stroke” for more information.
Definitions
- Intracerebral hemorrhage (ICH): bleeding within the brain parenchyma
- Intracranial hemorrhage: a broad term used to describe any bleeding within the skull (including intracerebral hemorrhage, subarachnoid hemorrhage, subdural hemorrhage, and epidural hemorrhage) due to traumatic brain injury or nontraumatic causes (e.g., hemorrhagic stroke, ruptured aneurysm, hypertensive vasculopathy)
-
Hemorrhagic stroke
- Rupture of a blood vessel within the brain or the cerebrospinal fluid
- Subtypes
- Intracerebral hemorrhage (intraparenchymal hemorrhage): bleeding within the brain parenchyma
- Subarachnoid hemorrhage: bleeding into the subarachnoid space
- Intraventricular hemorrhage: bleeding within the ventricles
Epidemiology
- ICH is responsible for approx. 10% of all strokes. [1]
- Most commonly affects the deep structures of the brain [2]
- Intraventricular extension occurs in approx. 30% of patients with ICH.
Epidemiological data refers to the US, unless otherwise specified.
Etiology
-
Nontraumatic (spontaneous)
- Hypertension: most common cause of spontaneous ICH
- Cerebral amyloid angiopathy: most common cause of spontaneous ICH in individuals > 60 years of age
- Arteriovenous malformations: most common cause of spontaneous intracerebral hemorrhage in children
- Vasculitis (e.g., giant cell arteritis)
- Neoplasms (e.g., meningioma)
- Ischemic stroke (due to reperfusion injury)
- CNS infections (e.g., HSV encephalitis)
- Septic emboli
- Coagulopathy (e.g., hemophilia, anticoagulant use)
- Stimulant use (e.g., cocaine and amphetamines; possibly also caffeine)
- Traumatic: : see traumatic brain injury

References:[3][4][5]
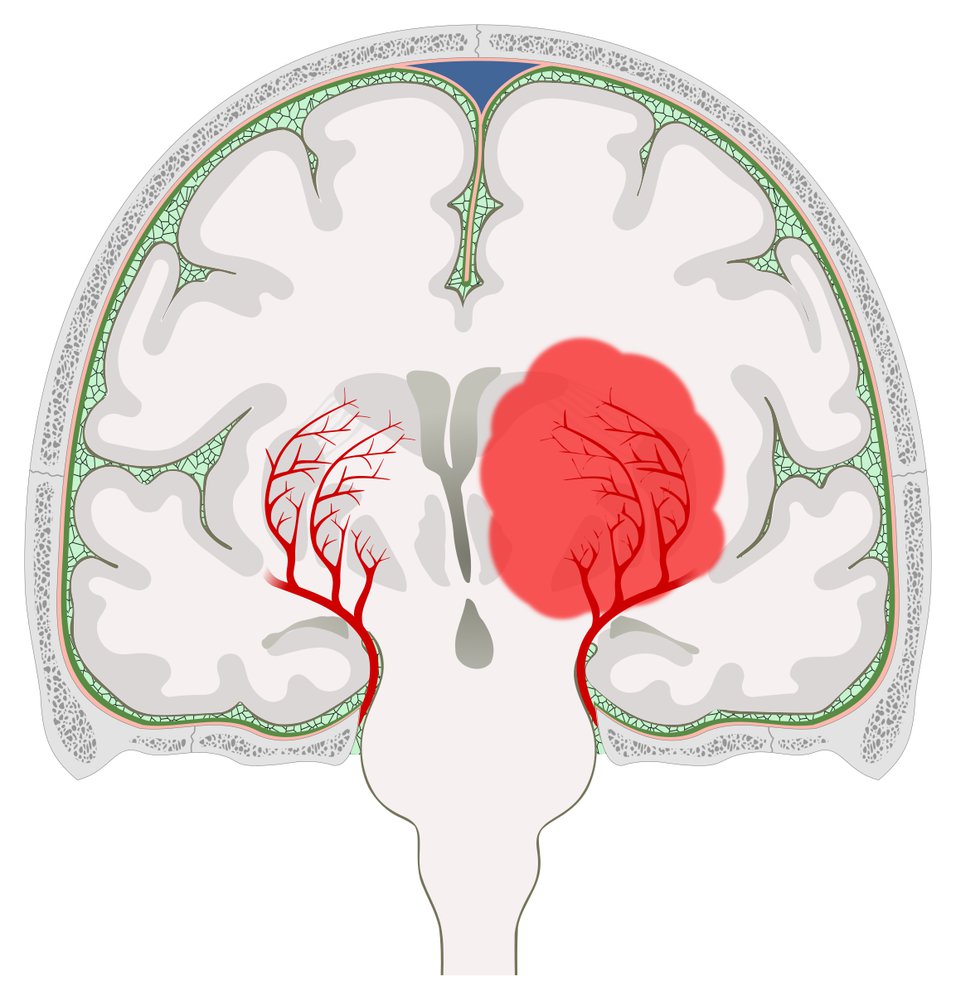
Hemorrhage in the region of the left basal ganglia causing a midline shift to the right
The basal ganglia are supplied by the lenticulostriate arteries, which arise from the middle cerebral artery. Hemorrhage from a lenticulostriate artery (e.g., due to poorly controlled hypertension or rupture of a Charcot-Bouchard microaneurysm) leads to a basal ganglia hemorrhage.
© AMBOSS
Pathophysiology
-
Nontraumatic mechanisms of hemorrhage
-
Chronic arterial hypertension → lipohyalinosis of lenticulostriate vessels (which supply the basal ganglia) and/or formation and rupture of Charcot-Bouchard microaneurysms → lacunar strokes (ischemia) of the basal ganglia
- Putamen most commonly affected
- Other locations: thalamus (second most common) and infratentorial parts of the brain (e.g., pons, cerebellum)
- Cerebral amyloid angiopathy: deposition of β-amyloid peptides in vessel walls → focal damage with formation of microaneurysms → rupture → recurrent lobar intracerebral hemorrhage
- Structural abnormalities (e.g., vascular malformations) → exposure of parts of the abnormal vascular segment to excessive strain → rupture
- Venous outflow obstruction and stimulant use (e.g., cocaine) → acute arterial hypertension
- Coagulopathies: impaired hemostasis → vascular microtrauma
- Inflammatory tissue necrosis → damage to vessels
-
Chronic arterial hypertension → lipohyalinosis of lenticulostriate vessels (which supply the basal ganglia) and/or formation and rupture of Charcot-Bouchard microaneurysms → lacunar strokes (ischemia) of the basal ganglia
- Traumatic: blunt or penetrating injury → damage to vessels
Clinical features
-
Headache
- Absent in small hemorrhages
- Most common in cerebellar and lobar hemorrhages [2][6]
-
Focal neurologic signs and symptoms may occur, depending on the location and size of the hemorrhage (see “Stroke symptoms by affected vessel” and “Stroke symptoms by affected region”) [2]
- Putaminal hemorrhage: contralateral hemiparesis or hemiplegia with less severe contralateral hemisensory loss; eyes deviate toward the side of the hematoma
- Thalamic hemorrhage: contralateral hemiparesis, contralateral hemisensory loss, decreased consciousness, wrong way eyes
- Course
- Symptoms typically progress gradually over minutes to a few hours
- Focal deficits worsen with expansion of the hematoma
-
Late: symptoms of increased ICP
- Nausea and vomiting
- Confusion and loss of consciousness
- Bradycardia
- Fixed pupils
Management
For the approach to patients with suspected traumatic ICH, see “Management of traumatic ICH.”
Initial evaluation [7][8][9]
Consider the sudden onset of focal neurological deficits a vascular event until proven otherwise and evaluate patients as promptly as possible (preferably within the so-called “golden hour”). [10][11][12]
- Perform an ABCDE survey.
- Initiate neuroprotective measures: These take precedence over diagnostics if they cannot be performed in parallel.
- Take a focused history, perform a neurological examination, and measure the GCS score.
-
Order immediate diagnostic studies.
- Neuroimaging: CT head without contrast or MRI head
- Laboratory studies: coagulation panel, platelets, and POC glucose
- Admit or urgently transfer the patient to a neurocritical care unit.
- Urgent consultations
- Neurosurgery: to evaluate if urgent operative intervention is indicated
- Neurology
- Hematology: if the patient is taking antiplatelet agents or anticoagulants
Patients with signs of brain herniation should be evaluated immediately for neurosurgical intervention!
Monitoring
- All patients should receive:
- Continuous cardiac telemetry
- Blood pressure (BP) monitoring
- Continuous pulse oximetry
- Hourly POC glucose monitoring
- Consider:
- An arterial line
- ICP monitoring (see “Acute stabilization” for indications)
- Continuous EEG monitoring
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
Acute stabilization
Acute stabilization should begin immediately after symptom onset, in parallel with diagnostic measures, with the goal of reducing hematoma expansion and limiting secondary brain injury. [7]
-
Airway management
- Immediately initiate basic airway maneuvers for airway compromise, e.g., signs of partial airway obstruction.
- Intubate if airway protective reflexes are lost.
- Intubation of patients with high ICP can be very risky and requires a specialized approach.
-
Standard neuroprotective measures
- Provide supplemental O2 as needed to maintain target SpO2 > 94%.
- If mechanical ventilation is required: maintain long-term normocapnia (PaCO2 35–45 mm Hg). [13]
- Maintain normoglycemia (see also “Treatment of hypoglycemia” and “Management of hyperglycemia in critically ill patients”). [7][13]
- Maintain normothermia: e.g., prevent neurogenic fever.
-
Blood pressure management in ICH: The optimal approach is unclear. [7][14][15][16][17];
- If systolic BP is > 220 mm Hg, promptly lower to 140–180 mm Hg; , e.g., using nicardipine AND/OR labetalol
- If systolic BP is 150–220 mm Hg and no contraindications to antihypertensive agents: Consider BP lowering on an individual basis in consultation with a specialist.
- Alternative antihypertensive agents include: [9][18]
- ACE inhibitors, e.g., enalapril or ARBs
- Furosemide
- Hydralazine
- Avoid systemic hypotension (e.g., MAP < 65 mm Hg).
-
Anticoagulation reversal
- Stop all anticoagulants and antiplatelet agents.
- Administer reversal agents as soon as possible to patients with an INR > 1.4 to reduce the risk of hematoma expansion.
- Platelet transfusion in intracranial bleeding: only for severe thrombocytopenia [7]
-
ICP management
- Considering invasive ICP monitoring if:
- The patient's GCS score is ≤ 8
- Significant intraventricular hemorrhage or hydrocephalus is present
- There is evidence of transtentorial herniation
- Consider measures to maintain ICP < 20 mm Hg and a cerebral perfusion pressure of 60–70 mm Hg: e.g., head elevation to 30°, hyperosmolar therapies for ICP management (mannitol, hypertonic saline), placement of an external ventricular drain or VP shunt for hydrocephalus [8]
- Avoid corticosteroids. [19]
- Considering invasive ICP monitoring if:
Remember to stop all anticoagulants and antiplatelet medication, including aspirin, in patients with ICH.
Platelet transfusion is not routinely indicated in patients with normal platelet counts taking antiplatelet agents (e.g., aspirin, clopidogrel). [7][20][21]
Diagnostics
| Approach to ICH diagnostics [7][9][13] | ||
|---|---|---|
| Time interval from initial presentation | Laboratory studies | Imaging |
| Within the first hour |
|
|
| Hours to days |
|
|
Characteristic neuroimaging findings [24]
-
Hematoma within the cerebral parenchyma (i.e., intraaxial lesion)
- Typical locations
- Supratentorial: lobar, or within the thalamus or basal ganglia
- Infratentorial: in the cerebellum or brainstem
- The density of the hematoma varies depending on the imaging modality used and age of the hematoma.
- Typical locations
| Variation in ICH density on imaging over time [25][26] | ||
|---|---|---|
| Time since ICH | Hematoma density | |
| CT without contrast | MRI (T2 weighted) | |
| Hyperacute (< 24 hours) | Hyperdense | Hyperintense |
| Acute (1–3 days) | Hyperdense with fluid level and hypodense perifocal edema | Hypointense with a hyperintense border |
| Early subacute (> 3 days to 1 week) | Hyperdense becoming isodense | Hypointense |
| Late subacute (weeks to months) | Isodense or hypodense | Hyperintense |
| Chronic (> months) | Hypodense | Hypointense |
-
Additional possible features
- Midline shift and/or mass effect; (if significant, this should raise suspicion for impending herniation)
- Intraventricular extension [9]









Angiography findings
Angiography may be performed to assess for signs of further bleeding and structural abnormalities in patients with suspected underlying pathology (e.g., patients aged < 55 years and those without risk factors for ICH). [7]
-
CTA spot sign [27]
- Definition: localized area of enhancement visible within an intracerebral hemorrhage only after administration of IV contrast
- Implication: indicates active hemorrhage; is a predictor of hematoma expansion [7][27][28]
- Aneurysms or other vascular lesions

")


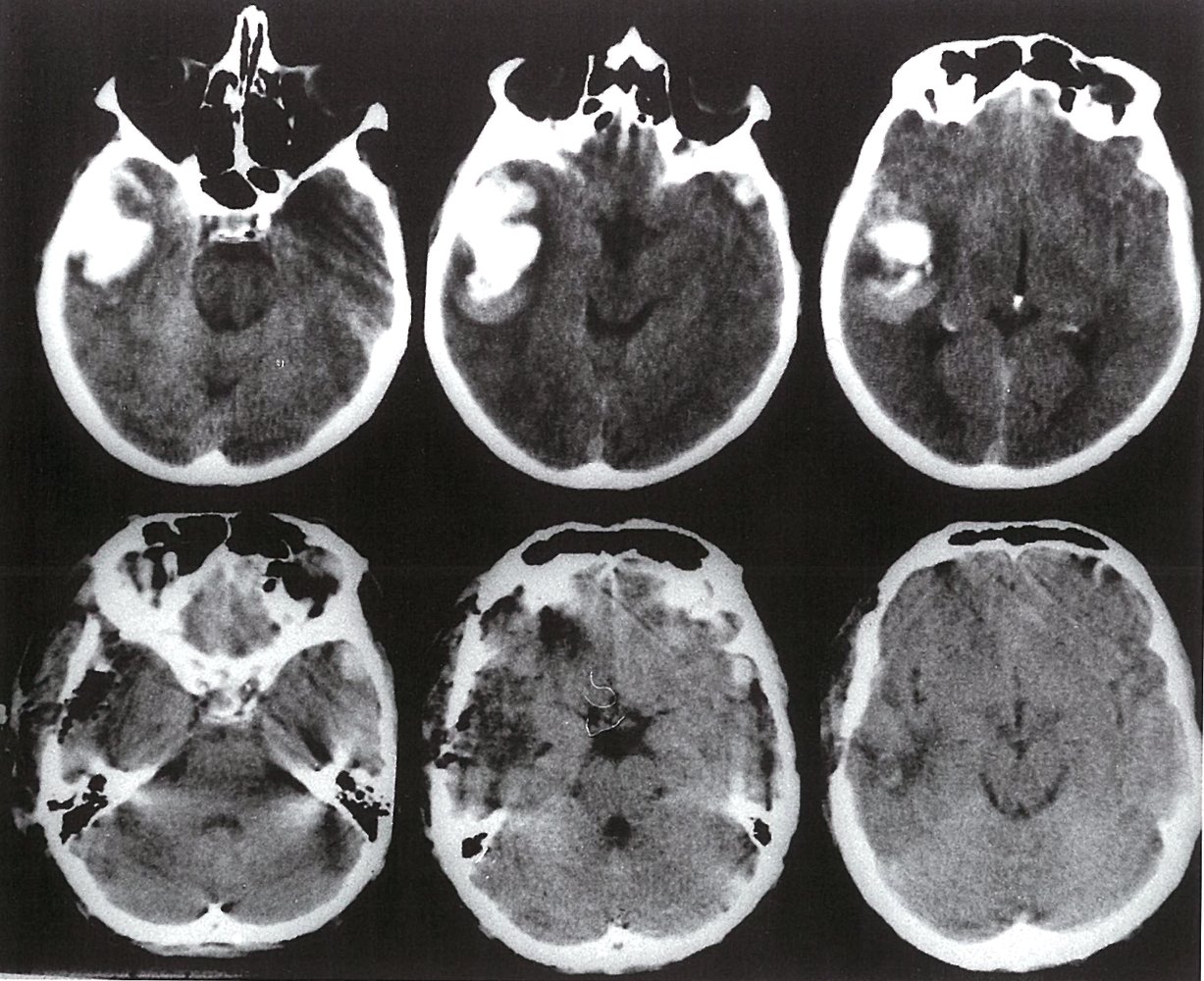
Series of cranial CTs (noncontrast; axial section; from left to right, caudal to cranial views)
Top series: before trephination (burr hole procedure)
An intraparenchymal hyperdensity (circled in green) consistent with an intracerebral hematoma is visible in the right temporal lobe.
Bottom series: after trephination
The hematoma has been evacuated through a burr hole created in the right temporal bone. Note the hypodense air pockets (circled in red). This is expected after trephination, and the air will resorb with time. (The mastoid air pockets visible bilaterally in the bottom two images on the left are physiological.)
Source: © IMPP

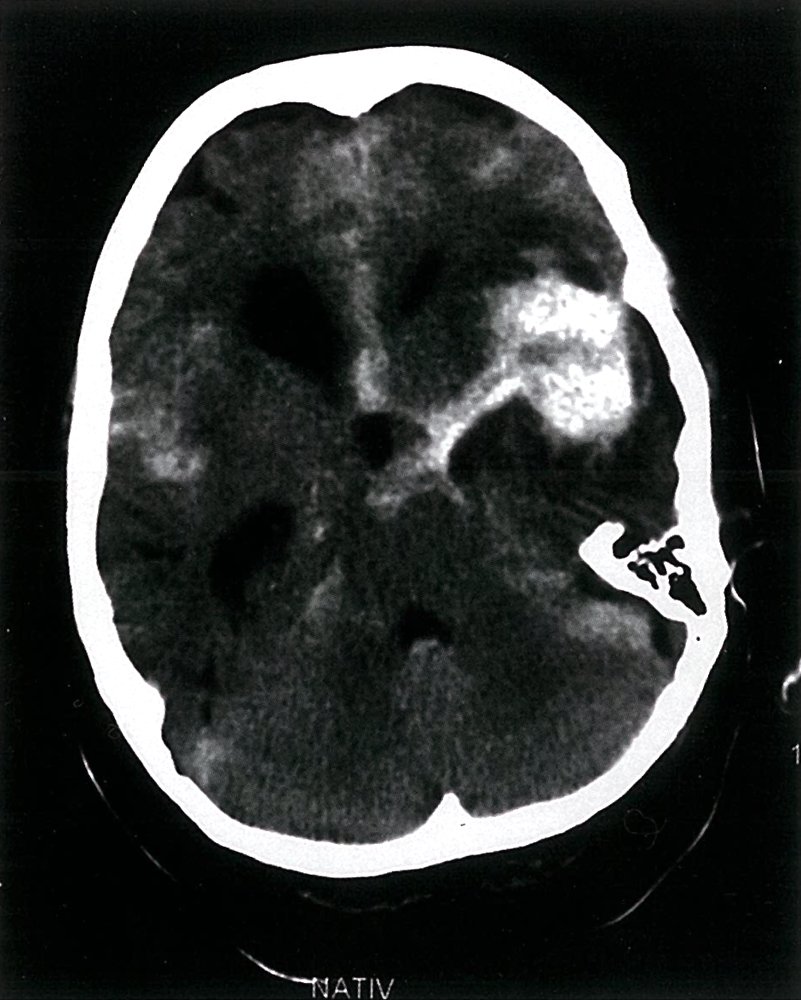
CT head (without contrast; axial plane)
A large hyperdense hematoma (green overlay) in the posterior aspect of the left cerebral hemisphere is accompanied by hypodense edema (red overlay), effacement of the occipital horn of the left lateral ventricle, and midline shift (dashed line and arrowheads).
ROH: right occipital horn
Source: © IMPP
CT head (without contrast; axial plane)
A rounded area of high attenuation (1) in the left frontoparietal region indicates intracerebral hemorrhage from a ruptured left middle cerebral artery aneurysm. Extensive subarachnoid hemorrhage is present in the basal cisterns (2), interhemispheric fissure (3), right Sylvian fissure (4), left frontal lobe fissures (5), and posterior fossa (6). Ventricular dilatation (green overlay) is the result of obstruction of CSF drainage.
Source: © IMPP
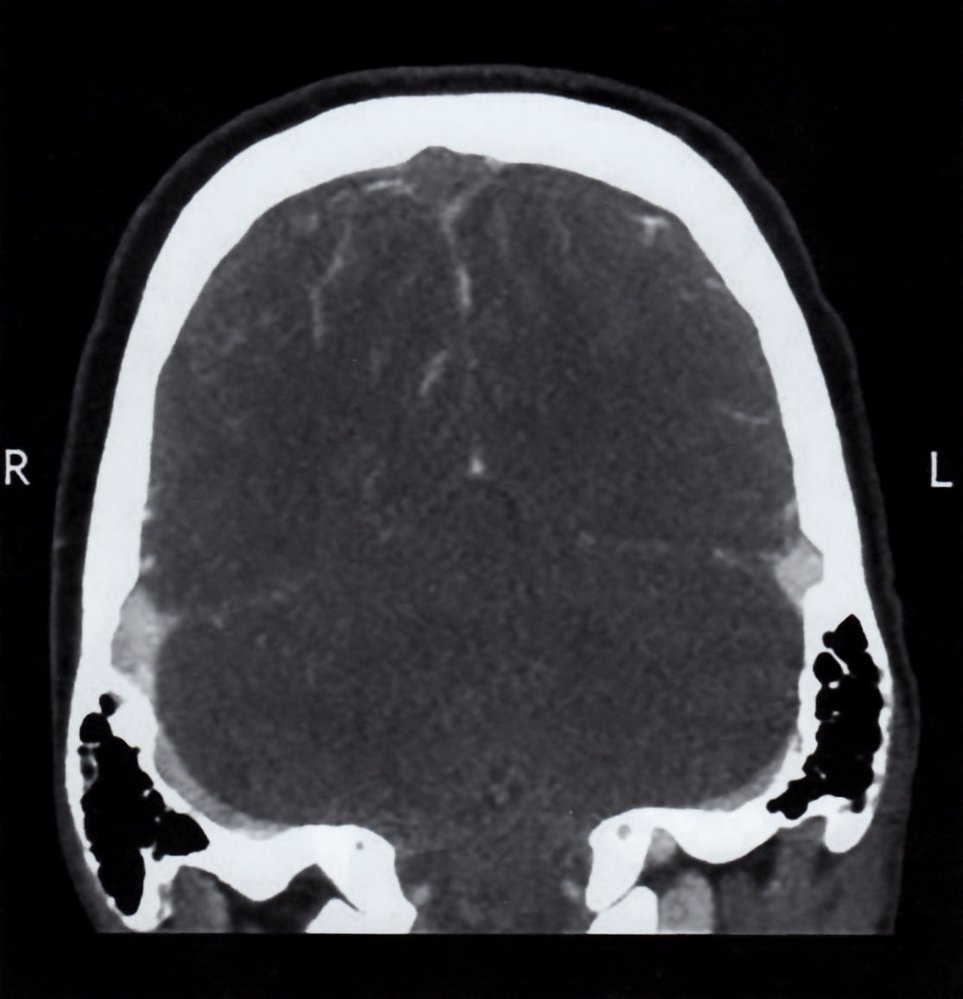
CT head (with IV contrast; coronal section; venous phase)
There is a contrast filling defect within the superior sagittal sinus (red overlay), which is hypodense with hyperdense borders (empty delta sign). The transverse sinuses (blue overlay) are hyperdense, which is their normal appearance.
This appearance is suggestive of a sinus vein thrombosis in the superior sagittal sinus.
Source: © IMPP
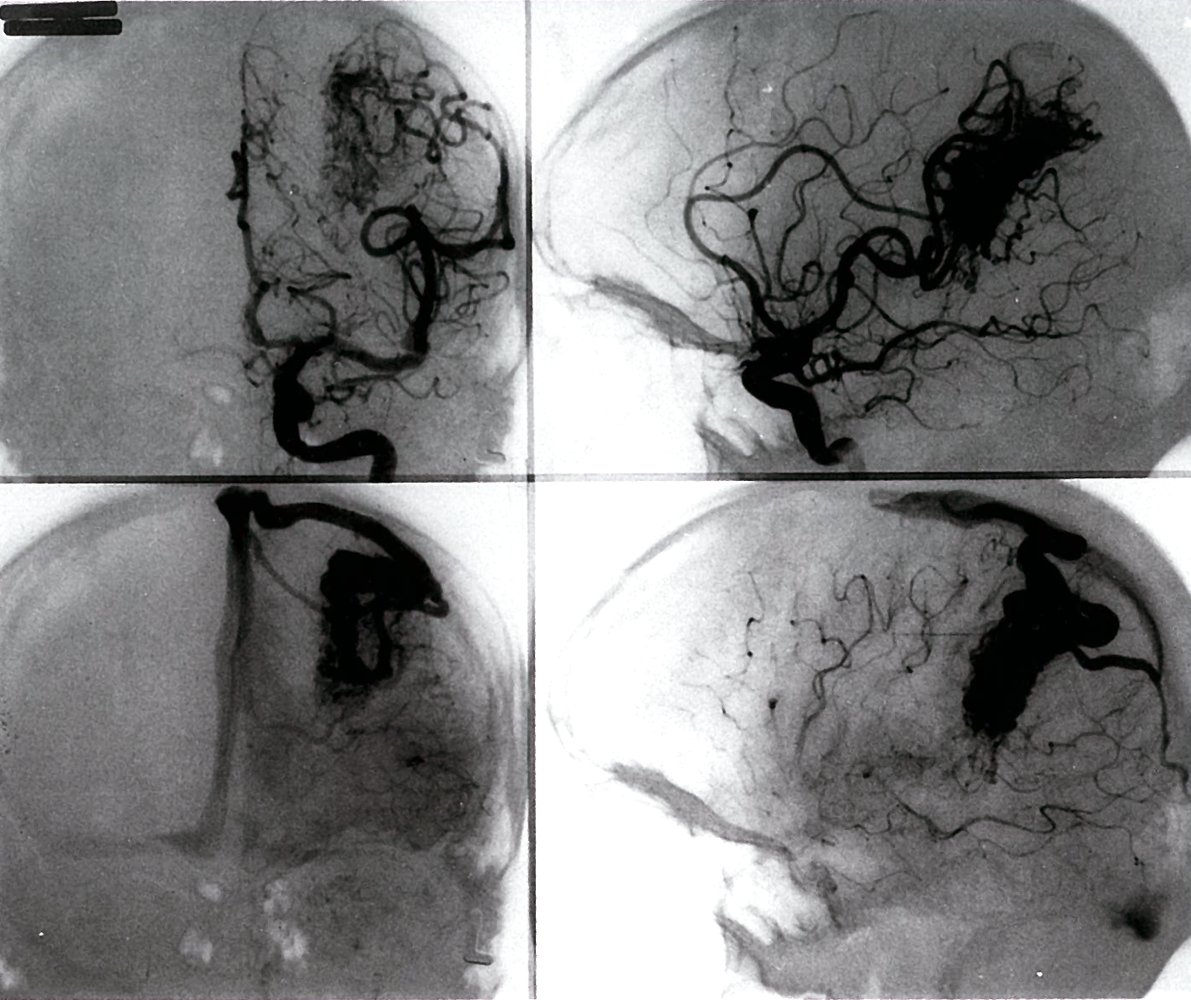
Cerebral angiography
Top left: arterial phase, coronal section
Top right: arterial phase, sagittal section
Bottom left: venous phase, coronal section
Bottom right: venous phase, sagittal section
A large vascular malformation (red overlay) is visible in the area of the temporal lobe. Since the malformation is clearly visible during both arterial and venous phases, it can be identified as arteriovenous.
Source: © IMPP
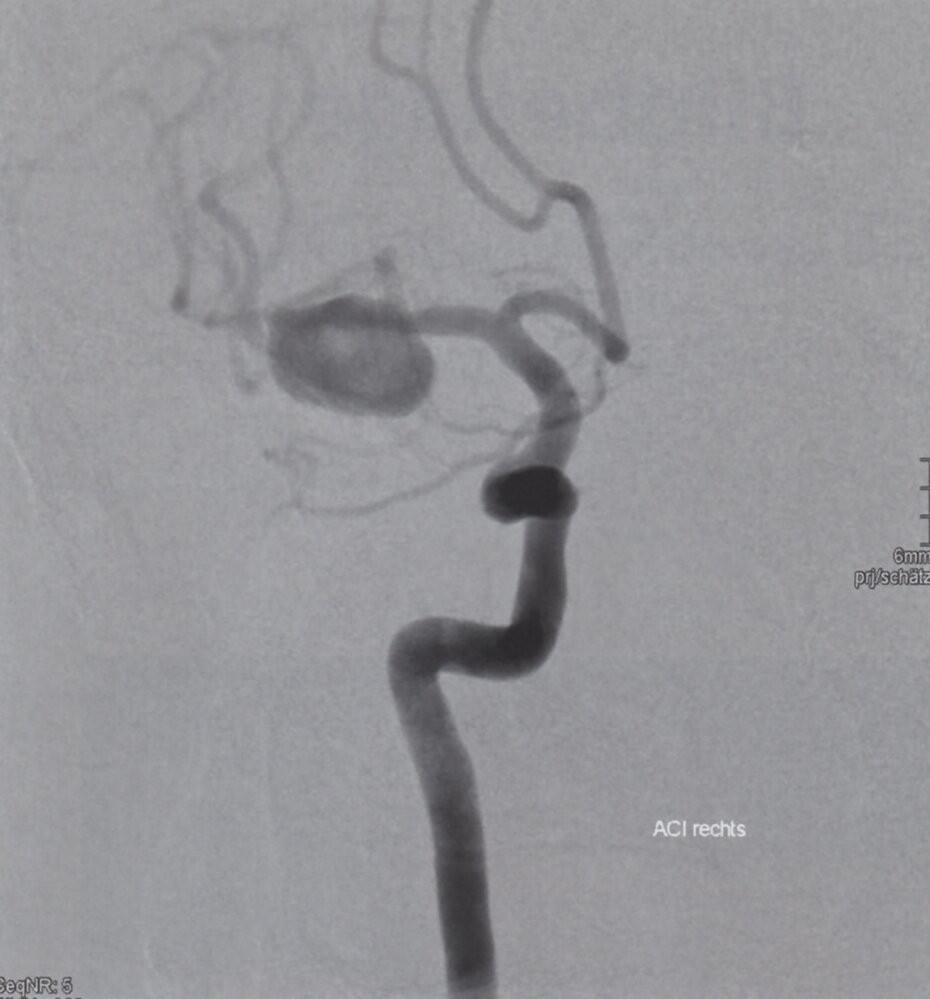
Digital subtraction angiography (right middle cerebral artery; AP view; arterial phase)
A large saccular aneurysm (green overlay) arises from the right middle cerebral artery (MCA) close to the bifurcation of the internal carotid artery (ICA).
Source: © IMPP
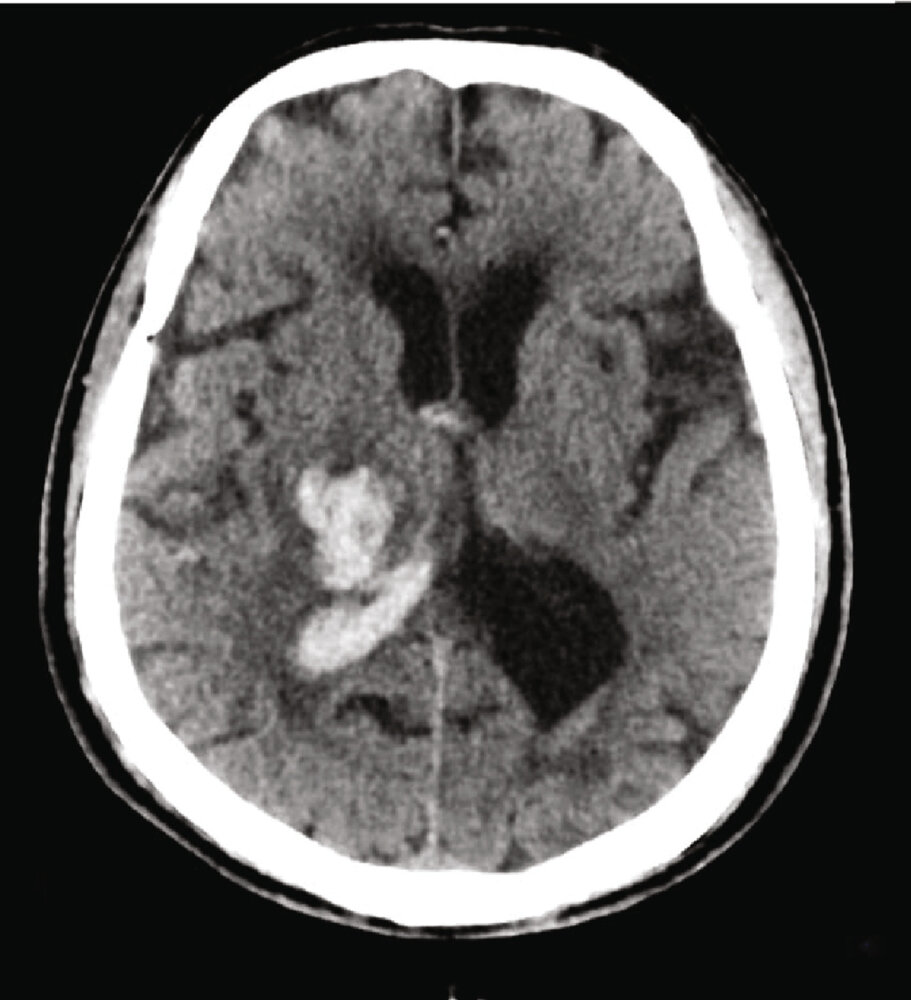
CT head (without contrast; axial plane) of an older adult
Hyperdense hemorrhage (blue overlay) involving the right thalamus extends to the posterior limb of the right internal capsule. Intraventricular hemorrhage (yellow overlay) is also present. Mass-effect has caused a slight midline shift.
Prominent sulci and ventricles are consistent with cerebral atrophy.
Green overlay: internal capsule; red line: midline; T: thalamus
Source: “Fig 4 A1, In: Different Effects of Hematoma Expansion on Short-Term Functional Outcome in Basal Ganglia and Thalamic Hemorrhages” by Deng L, Chen K, Yang L, Deng Z, Zheng H, Hindawi, licensed under CC BY 4.0. Modifications: image cropped; removed "A1". The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
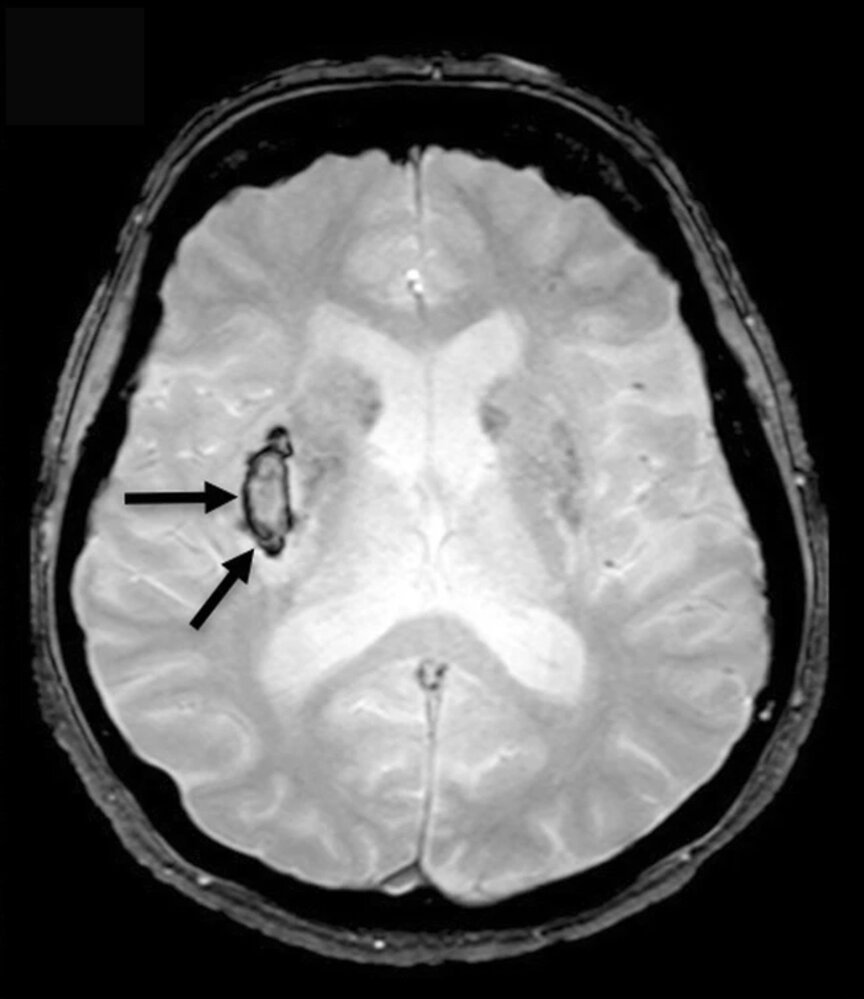
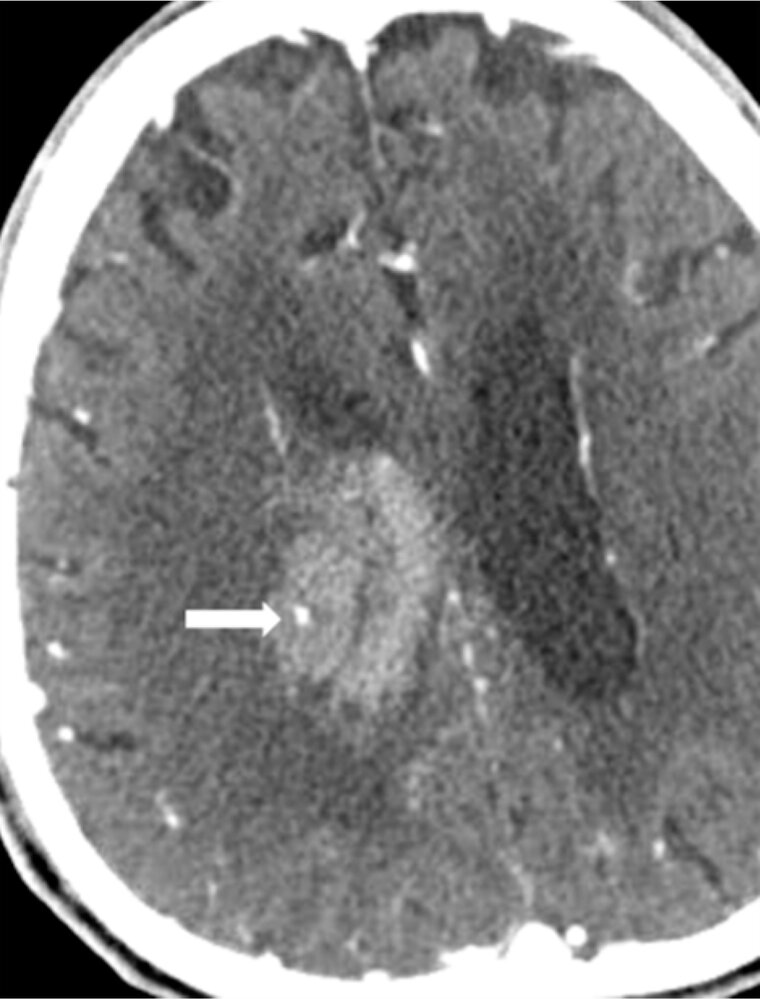
MRI head (T2 with gradient-recalled echo-weighted imaging (GRE); axial plane) of a patient with left-sided hemiplegia and homonymous hemianopsia
A slightly hyperintense lesion with a hypointense periphery (arrows) is seen in the area of the right basal ganglia.
These findings are consistent with a hyperacute intracerebral hemorrhage. The hypointense border, which results from deoxygenated hemoglobin, is a characteristic feature. In contrast to oxygenated hemoglobin (which is the main component of a hyperacute hemorrhage), oxygen-deficient hemoglobin has a paramagnetic effect, which leads to a signal decrease in the gradient-echo sequence.
Source: “Fig. 2, in: Magnetic resonance imaging of arterial stroke mimics: a pictorial review” by Adam G, Ferrier M, Patsoura s, Gramada R, Meluchova Z, Cazzola V, et al., Insights Imaging, licensed under CC BY 4.0. Modifications: Image was cropped, letter "D" was removed..
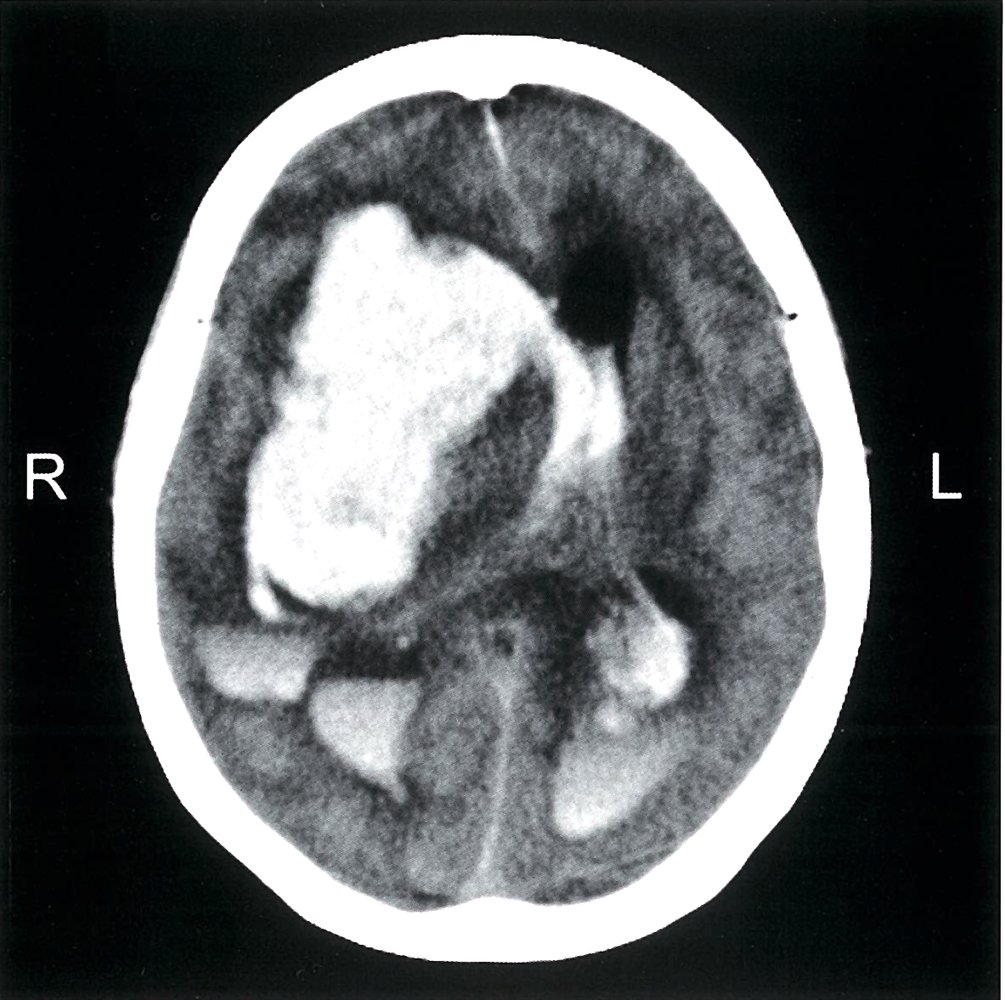
Noncontrast CT of the head (axial section)
The large hyperdensity (green overlay) in the region of the right basal ganglion indicates a massive intracerebral hemorrhage that has caused a midline shift (red line) to the contralateral side. There are focal areas of cerebral edema, identifiable as hypointense (black) areas in the perihemorrhagic area. The hemorrhage has extended into the lateral ventricles (red overlay), which appear enlarged (dotted white outline), indicating an obstruction to CSF drainage by the hemorrhage.
Blood, being denser than CSF, has settled in the posterior horns of the lateral ventricles (red overlay with white arrows) and the edematous parenchyma (green overlay with white arrowheads), as these areas are dependent fluid-filled portions in the supine position.
Source: © IMPP
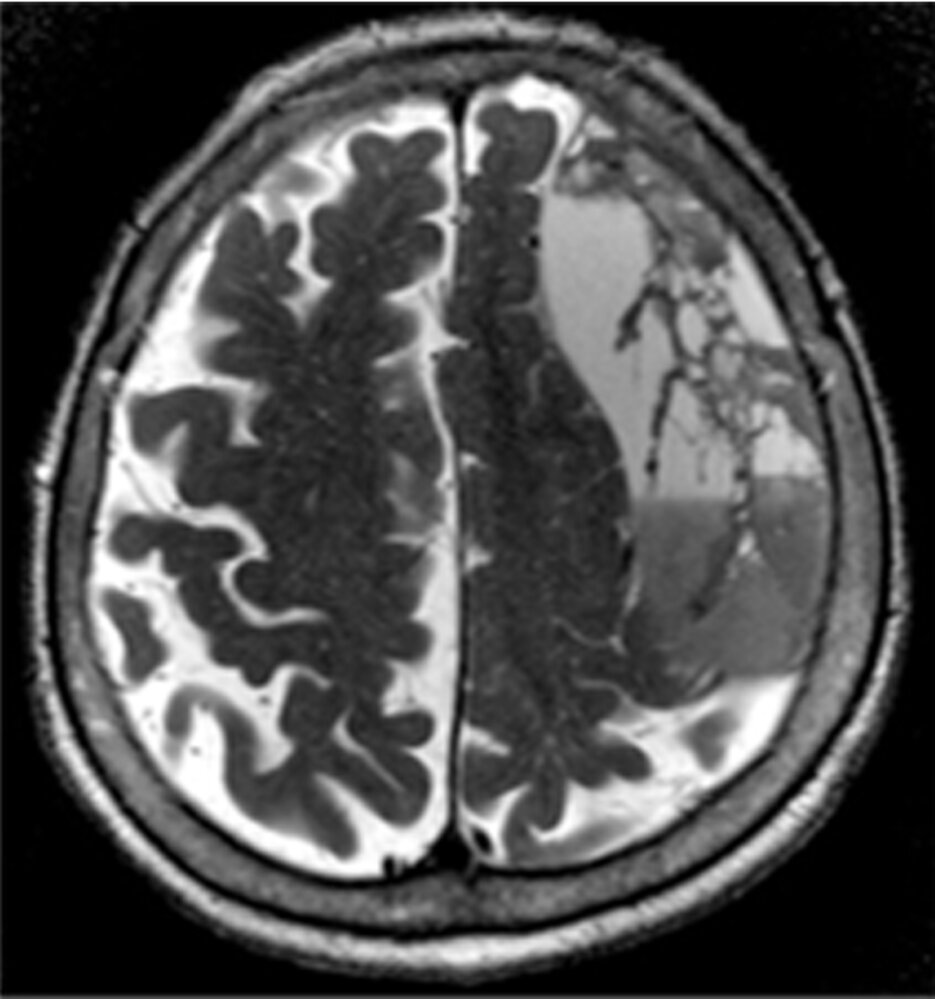
MRI head (T2 weighted; axial plane) of an 86-year-old patient with word-finding difficulties and generalized weakness after two falls (at 2 months at 1 month before presentation).
A large space-occupying lesion with heterogeneous signal intensity can be seen in the left high frontal region, shifting the midline to the contralateral side (red lines and arrow).
In the context of the patient's two falls, these findings are consistent with a chronic subdural hematoma (hypointense parts of the lesion; green overlay) with additional subacute hemorrhage (hyperintense parts of the lesion; red overlay).
Source: “Fig. 1 D, in: Use of Subdural Evacuating Port System Following Open Craniotomy with Excision of Native Dura and Membranes for Management of Chronic Subdural Hematoma” by Cage T, Bach A, Mcdermott M, Cureus, licensed under CC BY 3.0. Modifications: Image was cropped, letter "D" was removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
Click on the overlay icon below the taskbar on the left to toggle the overlay on and off.
CT head (without contrast; brain and bone windows; axial plane) of a 47-year-old patient after head trauma
Brain window images show multiple sites of parenchymal contusion in the frontal lobes (green overlay). Additional hemorrhage involves the left basal ganglia and internal capsule (yellow overlay). Scattered areas of subarachnoid hemorrhage (examples indicated by blue overlay) are present, and a subdural hematoma (red overlay) along the right cerebral convexity has caused mass effect with contralateral shift (dashed white line) of the midline. Hemorrhage extends along the falx cerebri, which appears hyperdense and thickened (especially dorsally).
Bone window images show a calvarial fracture (green overlay) that extends from the frontal bone into the sagittal suture. Zygomatic (red circle) and nasal bone (green circle) fractures are also seen, and there is extensive hemosinus (example indicated by hatched green overlay).
Created by: Nándor Faluhelyi. Organization providing image: University of Pécs, Medical School. Further notes: Our great thanks to Nándor Faluhelyi (University of Pécs, Medical School) for kindly providing this case.
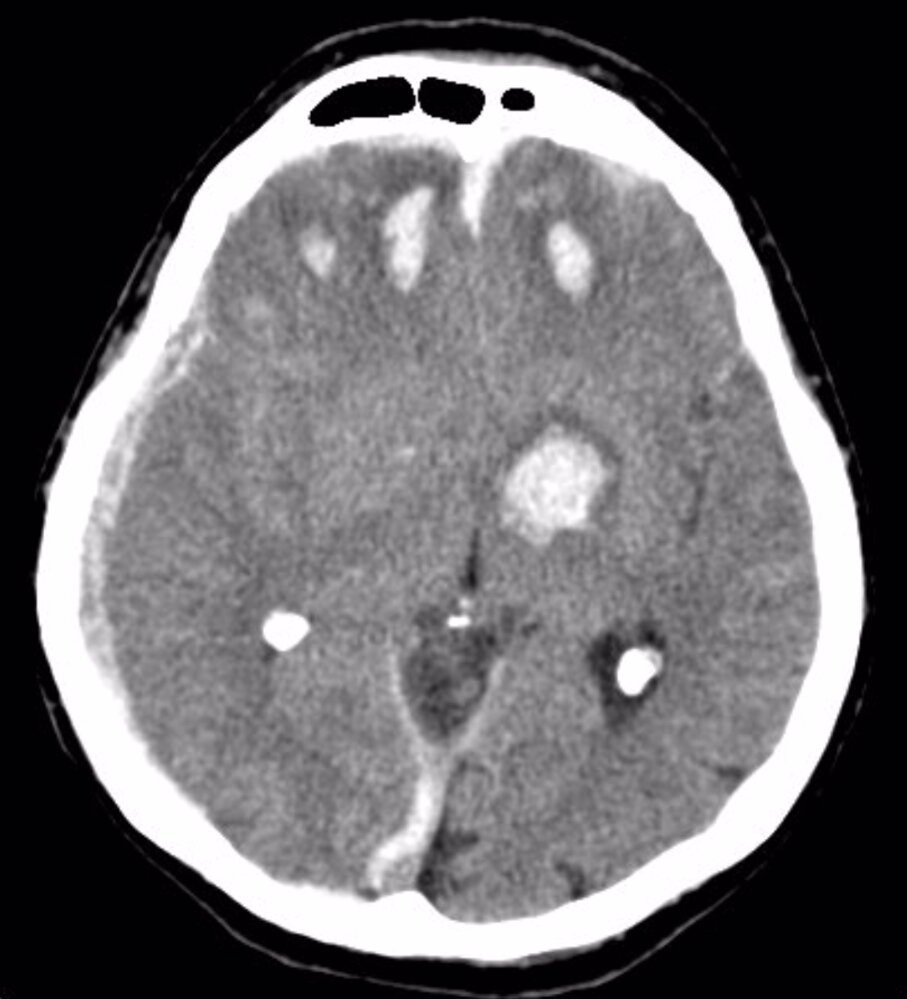
CT angiography head (second phase; axial plane)
A hyperdense area representing a hematoma (red overlay) is visible in the right basal ganglia and produces mass effect on the right lateral ventricle. The hematoma was seen on a precontrast study (first phase, not shown), but the dot-like hyperdensity within it (arrow; spot sign) was only visible postcontrast (second phase). The spot was not continuous with a normal enhanced blood vessel on multiplanar formatted images.
Contrast extravasation presenting as a positive spot sign indicates active bleeding and predicts hematoma expansion.
Source: “Fig. 4, in: Correlation between Spot Sign and Intracranial Hemorrhage Expansion on Dual-Phase CT Angiography” by Kim H, Goo JH, Kwak HS, Hwang SB, Chung GH, MDPI, licensed under CC BY 4.0. Modifications: Image was cropped. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
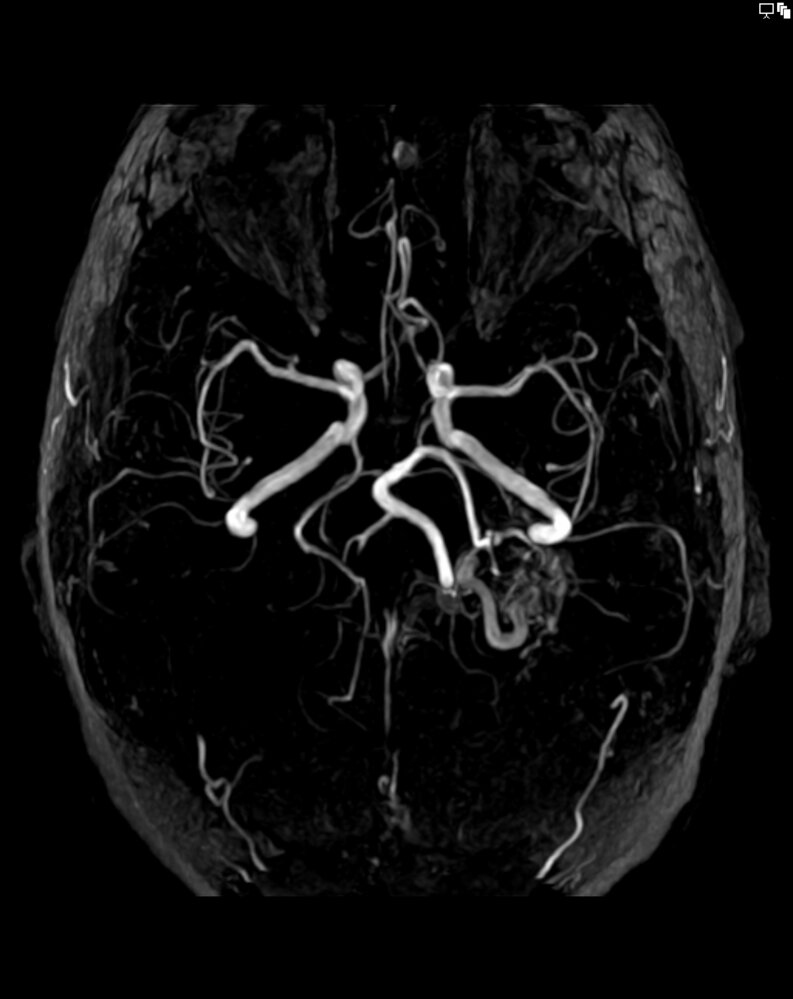
MR angiography head (time-of-flight (TOF); rotated maximum intensity projection (MIP))
A tangle of blood vessels (nidus, green overlay) is visible. It is supplied by an enlarged left posterior cerebral artery (red overlay) and drained by an enlarged vein (blue overlay).
The findings are consistent with an arteriovenous malformation.
Source: “001 Arteriovenous Malformation MRT TOF MIP 09.png” by Hellerhoff, Wikimedia Commons, licensed under CC BY 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
{kind=link}
Treatment
Approach
- Most patients are managed conservatively, with treatment focused on prevention of secondary brain injury.
- Patients should be screened for common complications.
- Select patients may benefit from neurosurgical intervention.
Detection and management of complications
| Common complications following spontaneous ICH [7] | |
|---|---|
| Complication | Screening and management |
| Dysphagia [29] |
|
| Seizures |
|
| Cardiac abnormalities |
|
| Electrolyte abnormalities |
|
| Venous thromboembolism (VTE) |
|
| Hematoma expansion |
|
Prophylactic anticonvulsants are not recommended in patients with ICH. [7]
Surgical management [7]
Neurosurgical consultation is advised for acute ICP management (see “Acute stabilization”) and definitive management. Evacuation of the hematoma may be appropriate depending on the size, location, and associated clinical features of the ICH.
Hematoma evacuation
- Can be performed using standard craniotomy or minimally invasive surgical techniques [7][36]
-
Hematoma evacuation is recommended in patients with infratentorial hemorrhage who have any of the following: [7]
- Large hematoma (> 3 cm)
- Declining neurological status
- Hydrocephalus
- Signs of brain herniation (e.g., Cushing triad)
- Consider in patients with supratentorial hemorrhage and a declining GCS score or an initial GCS score of 10–13. [37]
Decompressive craniotomy
- Decompressive craniotomy may be performed alone or in combination with hematoma evacuation.
- Consider in patients with supratentorial hemorrhage and any of the following: [7]
- Refractory elevated ICP
- Large hematoma with a significant midline shift
- GCS score ≤ 8
Reducing subsequent stroke risk
- Manage hypertension and address lifestyle risk factors.
- Provide lipid-lowering therapy for ASCVD.
- Statin therapy increases the risk of recurrent hemorrhagic stroke but is nonetheless typically indicated. [38]
- PCSK9 inhibitors can be considered as an alternative. [39]
- Avoid long-term use of NSAIDs and use SSRIs with caution. [40]
Individuals often have overlapping risk factors for both ischemic stroke and hemorrhagic stroke; assess recurrence risk with a thorough history and examination, laboratory studies, and possibly imaging. [40]
Management of traumatic ICH
The management of traumatic ICH is similar to the management of spontaneous ICH, with some modifications.
-
Diagnostics [41]
- Follow the management approach for TBI and exclude concurrent injuries.
- TBI diagnostics include CT head without contrast and additional imaging as needed.
-
Management [8][10][41]
- Focuses on the prevention of complications in brain injuries
- Early surgical intervention can improve outcomes; consult neurosurgery as soon as possible. [42]
- Recommendations for neuroprotective measures include seizure prophylaxis for severe TBI.
- Follow-up neuroimaging is usually indicated; timing depends on injury severity.
- For details, see “Management of moderate and severe TBI.”
Click on the overlay icon below the taskbar on the left to toggle the overlay on and off.
CT head (without contrast; brain and bone windows; axial plane) of a 47-year-old patient after head trauma
Brain window images show multiple sites of parenchymal contusion in the frontal lobes (green overlay). Additional hemorrhage involves the left basal ganglia and internal capsule (yellow overlay). Scattered areas of subarachnoid hemorrhage (examples indicated by blue overlay) are present, and a subdural hematoma (red overlay) along the right cerebral convexity has caused mass effect with contralateral shift (dashed white line) of the midline. Hemorrhage extends along the falx cerebri, which appears hyperdense and thickened (especially dorsally).
Bone window images show a calvarial fracture (green overlay) that extends from the frontal bone into the sagittal suture. Zygomatic (red circle) and nasal bone (green circle) fractures are also seen, and there is extensive hemosinus (example indicated by hatched green overlay).
Created by: Nándor Faluhelyi. Organization providing image: University of Pécs, Medical School. Further notes: Our great thanks to Nándor Faluhelyi (University of Pécs, Medical School) for kindly providing this case.
Differential diagnoses
See “Differential diagnoses of stroke.”
The differential diagnoses listed here are not exhaustive.
Complications
- Elevated ICP and brain herniation
- Intraventricular hemorrhage → hydrocephalus
- Recurrent hemorrhage
- Vasospasm and cerebral ischemia
- Dysphagia; : can lead to aspiration of food and pneumonia
- Seizures
- Hydrocephalus
- SIADH
- Deep vein thrombosis
- See “Complications of stroke.”
We list the most important complications. The selection is not exhaustive.
Prognosis
- 30-day mortality ranges from 25% to 50%. [44][45]
- Patients aged > 65 years and those with large hematomas and low GCS scores (≤ 11) typically have poor outcomes. [44][45]
- The ICH score is used to assess the severity of bleeds, and, in conjunction with other features, to estimate the patient's prognosis. [7]
| ICH score [46][47] | ||
|---|---|---|
| Variable | Findings | Points |
| GCS score | 3–4 | 2 |
| 5–12 | 1 | |
| 13–15 | 0 | |
| ICH volume | ≥ 30 cm3 | 1 |
| < 30 cm3 | 0 | |
| Intraventricular hematoma | Yes | 1 |
| No | 0 | |
| ICH of infratentorial origin | Yes | 1 |
| No | 0 | |
| Patient age | ≥ 80 years | 1 |
| < 80 years | 0 | |
Total ICH score: 0–6 Predicted 30-day mortality
|
||
The ICH score was designed to assess ICH severity and aid clinical communication; it should not be used in isolation to determine prognosis!
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
Prevention
See ”Primary prevention of stroke.”
Related One-Minute Telegram
- One-Minute Telegram 122-2025-2/3: Lower the pressure, not the perfusion: intensive BP management after intracerebral hemorrhage
- One-Minute Telegram 100-2024-3/3: Blood pressure management in undifferentiated stroke: one size does not fit all
Interested in the newest medical research, distilled down to just one minute? Sign up for the One-Minute Telegram in “Tips and links” below.
External Resources
References
- Kasper DL, Fauci AS, Hauser S, et al. "Harrisons Principles of Internal Medicine ". McGraw-Hill Medical Publishing Division. 19. (2016). ISBN: 9780071802154
- Berlit P. "Diagnosis and treatment of cerebral vasculitis". Ther Adv Neurol Disord. 3(1). :29–42. (2010)
- Chen M. "Stroke as a Complication of Medical Disease". Semin Neurol. 29(2). :154-162. (2009)
- Daroff RB, et al. "Bradley's Neurology in Clinical Practice". Elsevier. ISBN: 9780323287838
- Delcourt et al. "Intracerebral hemorrhage location and outcome among INTERACT2 participants". Neurology. 88(15). :1408–1414. (2017)
- Hemphill JC, Greenberg SM, Anderson CS et al. "Guidelines for the Management of Spontaneous Intracerebral Hemorrhage". Stroke. 46(7). (2015)
- Balami JS, Buchan AM. "Complications of intracerebral haemorrhage". Lancet Neurol. 11(1). :101-118. (2012)
- Carney N, Totten AM, O’Reilly C, et al. "Guidelines for the Management of Severe Traumatic Brain Injury, Fourth Edition". Neurosurgery. 80(1). :6-15. (2016)
- Claude Hemphill J, Lam A. "Emergency Neurological Life Support: Intracerebral Hemorrhage". Neurocrit Care. 27(S1). :89-101. (2017)
- American College of Surgeons and the Committee on Trauma. "ATLS Advanced Trauma Life Support". American College of Surgeons. (2018). ISBN: 9780996826235
- E. Brooke Lerner, Ronald M. Moscati. "The Golden Hour: Scientific Fact or Medical "Urban Legend"?". Academic Emergency Medicine. 8(7). :758-760. (2001)
- Rogers FB, Rittenhouse KJ, Gross BW. "The golden hour in trauma: Dogma or medical folklore?". Injury. 46(4). :525-527. (2015)
- De Oliveira Manoel AL, Goffi A, Zampieri FG, et al. "The critical care management of spontaneous intracranial hemorrhage: a contemporary review". Crit Care. 20(1). (2016)
- Hays A, Diringer MN. "Elevated troponin levels are associated with higher mortality following intracerebral hemorrhage.". Neurology. 66(9). :1330-4. (2006)
- Mu J, Ni C, Wu M, et al. "A Retrospective Study on Risk Factors for Urinary Tract Infection in Patients with Intracranial Cerebral Hemorrhage". BioMed Research International. 2020. :1-7. (2020)
- Morotti A, Goldstein JN. "Diagnosis and Management of Acute Intracerebral Hemorrhage.". Emerg Med Clin North Am. 34(4). :883-899. (2016)
- Aguilar MI, Brott TG. "Update in intracerebral hemorrhage.". The Neurohospitalist. 1(3). :148-59. (2011)
- Macellari F, Paciaroni M, Agnelli G, Caso V. "Neuroimaging in intracerebral hemorrhage.". Stroke. 45(3). :903-8. (2014)
- Wada R, Aviv RI, Fox AJ, et al. "CT Angiography “Spot Sign” Predicts Hematoma Expansion in Acute Intracerebral Hemorrhage". Stroke. 38(4). :1257-1262. (2007)
- Peng W-J, Reis C, Reis H, Zhang J, Yang J. "Predictive Value of CTA Spot Sign on Hematoma Expansion in Intracerebral Hemorrhage Patients". BioMed Research International. 2017. :1-9. (2017)
- Rabinstein AA. "Optimal Blood Pressure After Intracerebral Hemorrhage". Stroke. 49(2). :275-276. (2018)
- Divani AA, Liu X, Di Napoli M, et al. "Blood Pressure Variability Predicts Poor In-Hospital Outcome in Spontaneous Intracerebral Hemorrhage". Stroke. 50(8). :2023-2029. (2019)
- Boulouis G, Morotti A, Goldstein JN, Charidimou A. "Intensive blood pressure lowering in patients with acute intracerebral haemorrhage: clinical outcomes and haemorrhage expansion. Systematic review and meta-analysis of randomised trials". Journal of Neurology, Neurosurgery & Psychiatry. 88(4). :339-345. (2017)
- Minhas JS, Moullaali TJ, Rinkel GJE, Anderson CS. "Blood Pressure Management After Intracerebral and Subarachnoid Hemorrhage: The Knowns and Known Unknowns". Stroke. 53(4). :1065-1073. (2022)
- Dastur CK, Yu W. "Current management of spontaneous intracerebral haemorrhage". BMJ. 2(1). :21-29. (2017)
- Cook AM, Morgan Jones G, Hawryluk GWJ, et al. "Guidelines for the Acute Treatment of Cerebral Edema in Neurocritical Care Patients". Neurocrit Care. 32(3). :647-666. (2020)
- Baharoglu MI, Cordonnier C, Salman RA-S, et al. "Platelet transfusion versus standard care after acute stroke due to spontaneous cerebral haemorrhage associated with antiplatelet therapy (PATCH): a randomised, open-label, phase 3 trial". The Lancet. 387(10038). :2605-2613. (2016)
- Al-Shahi Salman R, Law ZK, Bath PM, Steiner T, Sprigg N. "Haemostatic therapies for acute spontaneous intracerebral haemorrhage". Cochrane Database Syst. Rev.. 2018(4). (2018)
- Fogelholm R, Murros K, Rissanen A, Avikainen S. "Long term survival after primary intracerebral haemorrhage: a retrospective population based study.". J Neurol Neurosurg Psychiatry. 76(11). :1534-8. (2005)
- Safatli D, Günther A, Schlattmann P, et al. "Predictors of 30-day mortality in patients with spontaneous primary intracerebral hemorrhage". Surg Neurol Int. 7(19). :510. (2016)
- Hemphill JC 3rd, Bonovich DC, Besmertis L, Manley GT, Johnston SC. "The ICH score: a simple, reliable grading scale for intracerebral hemorrhage.". Stroke. 32(4). :891-7. (2001)
- Greenberg MS. "Handbook of Neurosurgery". Thieme Medical Publishers. (2020). ISBN: 9781684201372
- Kasper DL, Fauci AS, Hauser SL, et al. "Harrison's Principles of Internal Medicine". McGraw-Hill Education. (2015). ISBN: 9780071802161
- Joundi RA, Martino R, Saposnik G, et al. "Dysphagia screening after intracerebral hemorrhage". International Journal of Stroke. 13(5). :503-510. (2017)
- Junttila E, Vaara M, Koskenkari J, et al. "Repolarization abnormalities in patients with subarachnoid and intracerebral hemorrhage: predisposing factors and association with outcome.". Anesth Analg. 116(1). :190-7. (2013)
- Hasegawa K, Fix ML, Wendell L, et al. "Ischemic-appearing electrocardiographic changes predict myocardial injury in patients with intracerebral hemorrhage.". Am J Emerg Med. 30(4). :545-52. (2012)
- Sandhu R, Aronow WS, Rajdev A, et al. "Relation of cardiac troponin I levels with in-hospital mortality in patients with ischemic stroke, intracerebral hemorrhage, and subarachnoid hemorrhage.". Am J Cardiol. 102(5). :632-4. (2008)
- Koivunen R-J, Haapaniemi E, Satopää J, et al. "Medical Acute Complications of Intracerebral Hemorrhage in Young Adults". Stroke Res Treat. 2015. :1-7. (2015)
- Farr S, Toor H, Patchana T, et al. "Risks, Benefits, and the Optimal Time to Resume Deep Vein Thrombosis Prophylaxis in Patients with Intracranial Hemorrhage". Cureus. (2019)
- Ovesen C, Havsteen I, Rosenbaum S, Christensen H. "Prediction and Observation of Post-Admission Hematoma Expansion in Patients with Intracerebral Hemorrhage". Front Neurol. 5. (2014)
- De Oliveira Manoel AL. "Surgery for spontaneous intracerebral hemorrhage". Crit Care. 24(1). (2020)
- Gregson BA, Mitchell P, Mendelow AD. "Surgical Decision Making in Brain Hemorrhage.". Stroke. 50(5). :1108-1115. (2019)
- Diener HC, Hankey GJ. "Primary and Secondary Prevention of Ischemic Stroke and Cerebral Hemorrhage". J Am Coll Cardiol. 75(15). :1804-1818. (2020)
- Sanz-Cuesta BE, Saver JL. "Lipid-Lowering Therapy and Hemorrhagic Stroke Risk". Stroke. 52(10). :3142-3150. (2021)
- Greenberg SM, Ziai WC, Cordonnier C, et al. "2022 Guideline for the Management of Patients With Spontaneous Intracerebral Hemorrhage: A Guideline From the American Heart Association/American Stroke Association". Stroke. 53(7). (2022)
- Walls R, Hockberger R, Gausche-Hill M. "Rosen's Emergency Medicine". Elsevier Health Sciences. (2018). ISBN: 9780323354790
- Kvint S, Gutierrez A, Blue R, Petrov D. "Surgical Management of Trauma-Related Intracranial Hemorrhage—a Review". Curr Neurol Neurosci Rep. 20(12). (2020)