Summary
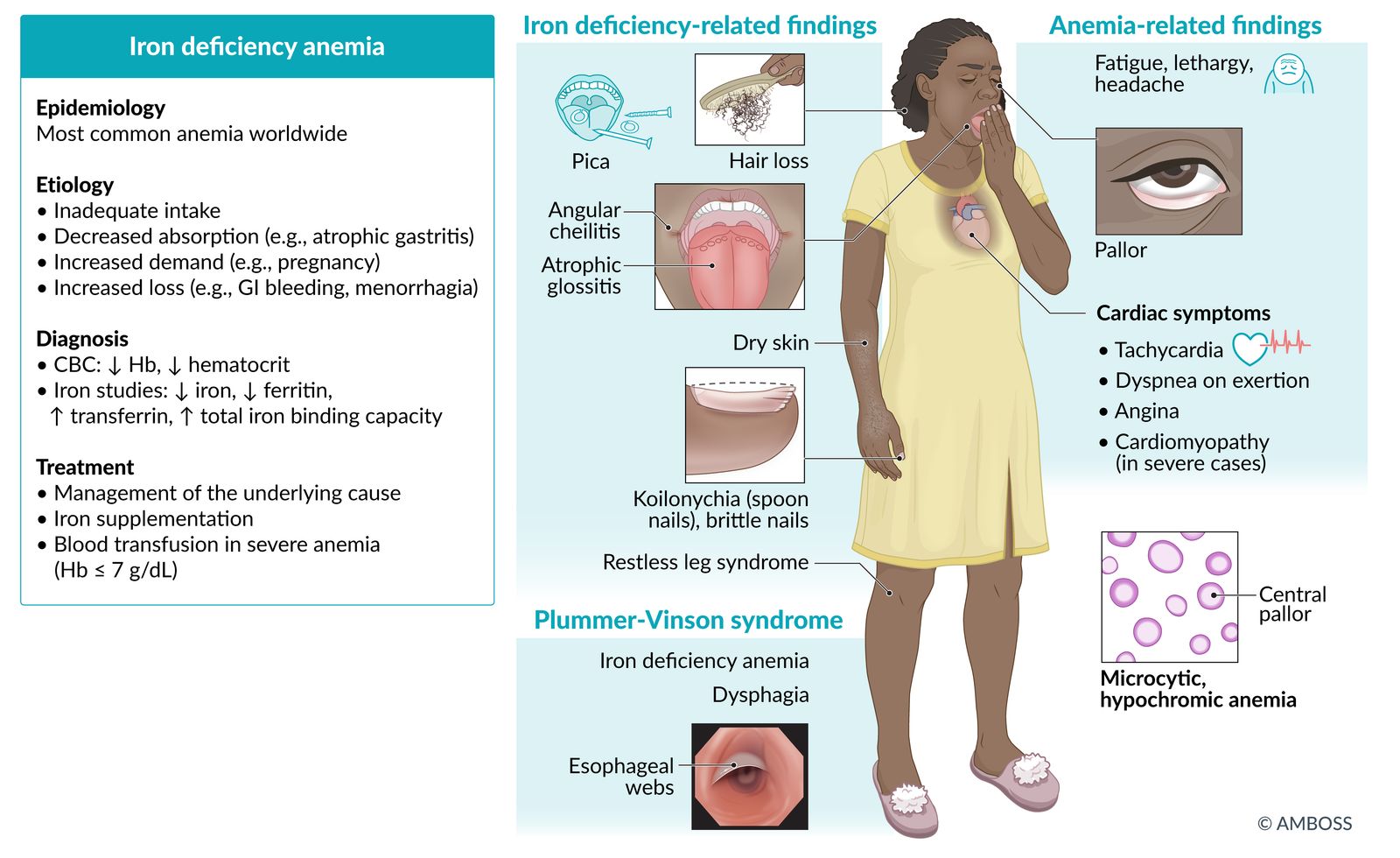
Iron deficiency anemia (IDA) is the most common form of anemia worldwide and is caused by inadequate intake, decreased absorption (e.g., atrophic gastritis, inflammatory bowel disease), increased demand (e.g., during pregnancy), or increased loss (e.g., gastrointestinal bleeding, menorrhagia) of iron. Prolonged deficiency depletes iron stores in the body, resulting in decreased erythropoiesis and anemia. Symptoms are nonspecific and include fatigue, pallor, lethargy, hair loss, brittle nails, and pica. Routine screening is only recommended for certain groups. IDA typically manifests as hypochromic, microcytic anemia, but it may also be normocytic. If diagnostic confirmation is needed, a low ferritin level indicates an iron deficiency, but additional iron studies may be necessary. Once IDA is confirmed, the underlying cause must be determined. In adults, this typically involves a gastroscopy and colonoscopy or, in women with abnormal uterine bleeding, a gynecologic workup. In children, a thorough history and review of symptoms, including a comprehensive dietary history, can help direct any further diagnostic evaluation. Patients with anemia severe enough to cause cardiopulmonary instability, or pregnant patients with a Hb < 6 g/dL, require blood transfusions. All other patients can be managed with oral or parenteral iron supplementation.
See also “Anemia.”

© AMBOSS
Epidemiology
- Most common form of anemia worldwide [1]
- ∼ 3% of the general population in the US is affected. [2]
- African American and Mexican American populations in the US are at increased risk.
-
Prevalence is highest in: [3]
- Children up to 5 years of age (see “IDA in children and adolescents”)
- Adolescent and premenopausal adult females (due to menstrual blood loss)
- Pregnant women (see “IDA in pregnancy”)
Epidemiological data refers to the US, unless otherwise specified.
Etiology
Based on age [1][4]
The most common causes of IDA in different age groups include:
-
Older adults > 50 years
- Resource-rich countries: colon polyps/carcinoma
- Resource-limited countries: hookworm infections, e.g., Ancylostoma duodenale, Necator americanus
-
Adults < 50 years
- Female individuals: menorrhagia, pregnancy (see “IDA in pregnancy”)
- Male individuals: peptic ulcer disease
- Children: See “Risk factors for pediatric IDA.”
In resource-rich countries, adults aged > 50 years who present with IDA should have colon polyps/carcinoma ruled out as a potential underlying etiology.
Based on underlying mechanism [4][5][6]
Iron losses
- Bleeding
-
Gastrointestinal bleeding
- Occult gastrointestinal malignancy (e.g., colon cancer)
- Hookworm infestation (e.g., Ancylostoma spp., N. americanus)
- Peptic ulcer disease
- Increased risk with NSAID use [7]
- Menstruation, particularly for individuals with heavy menstrual bleeding
- Hemorrhagic diathesis (e.g., hemophilia, von Willebrand disease)
-
Gastrointestinal bleeding
- Meckel diverticulum
- Dialysis-dependent renal failure
- Frequent blood donation
Decreased iron intake
- Chronic undernutrition
- Cereal-based diet
- Strict vegan diet [1]
Decreased iron absorption
- Achlorhydria/hypochlorhydria (e.g., due to autoimmune or Helicobacter pylori infection-induced atrophic gastritis)
- Inflammatory bowel disease, celiac disease
- Surgical resection of the duodenum
- Bariatric surgery
Increased demand
- Pregnancy
- Lactation
- Growth spurt
- Erythropoietin (EPO) therapy
Pathophysiology
- Iron deficiency → ↓ binding of iron to protoporphyrin (last reaction in heme synthesis) → ↓ production of hemoglobin
- For more information about the different physiological roles of iron and associated laboratory parameters, see “Iron” in “Trace elements” and “Iron studies” in “Laboratory medicine.”
Clinical features
- Frequently asymptomatic
- Fatigue, lethargy
- Pallor (primarily seen in highly vascularized mucosa, e.g., the conjunctiva)
- Cardiac: tachycardia, angina, dyspnea on exertion, pedal edema, and cardiomyopathy in severe cases
- Brittle nails, koilonychia (spoon-like nail deformity) , hair loss
- Pica, dysphagia
- Angular cheilitis: inflammation and fissuring of the corners of the mouth [8]
- Atrophic glossitis: erythematous, edematous, painful tongue with loss of tongue papillae (smooth, bald appearance)
- IDA can be associated with Plummer-Vinson syndrome (triad of iron deficiency anemia, postcricoid dysphagia, and upper esophageal webs) [9]


")

References:[1][10]

The conjunctiva appears pale, possibly indicating anemia.
Source: "ID#: 6900", CDC/ Dr. Lyle Conrad, Centers for Disease Control and Prevention licensed under Public Domain

Fingers (A) and thumb (B) of the right hand of a 22-year-old female patient presenting with weakness, weight loss, and reduced appetite
The nails are centrally concave and bend upwards distally, resulting in a characteristic spoon shape.
The most common cause of koilonychia is iron deficiency anemia, as was the case here.
Source: “Fig 1 (A & B), In: Spoon nails: still seen in today's world” by Moiz B, Wiley Online Library, licensed under CC BY 4.0. Modifications: part C of image cropped.

Multiple linear cracks of the epidermis (circled), approx. 0.5 cm in length, are located at the corner of the mouth. The occurrence of these fissures is called angular cheilitis and has many possible causes, e.g., iron deficiency, mechanical irritation, or infection.
Source: “Angular Cheilitis” by James Heilman, MD, Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}
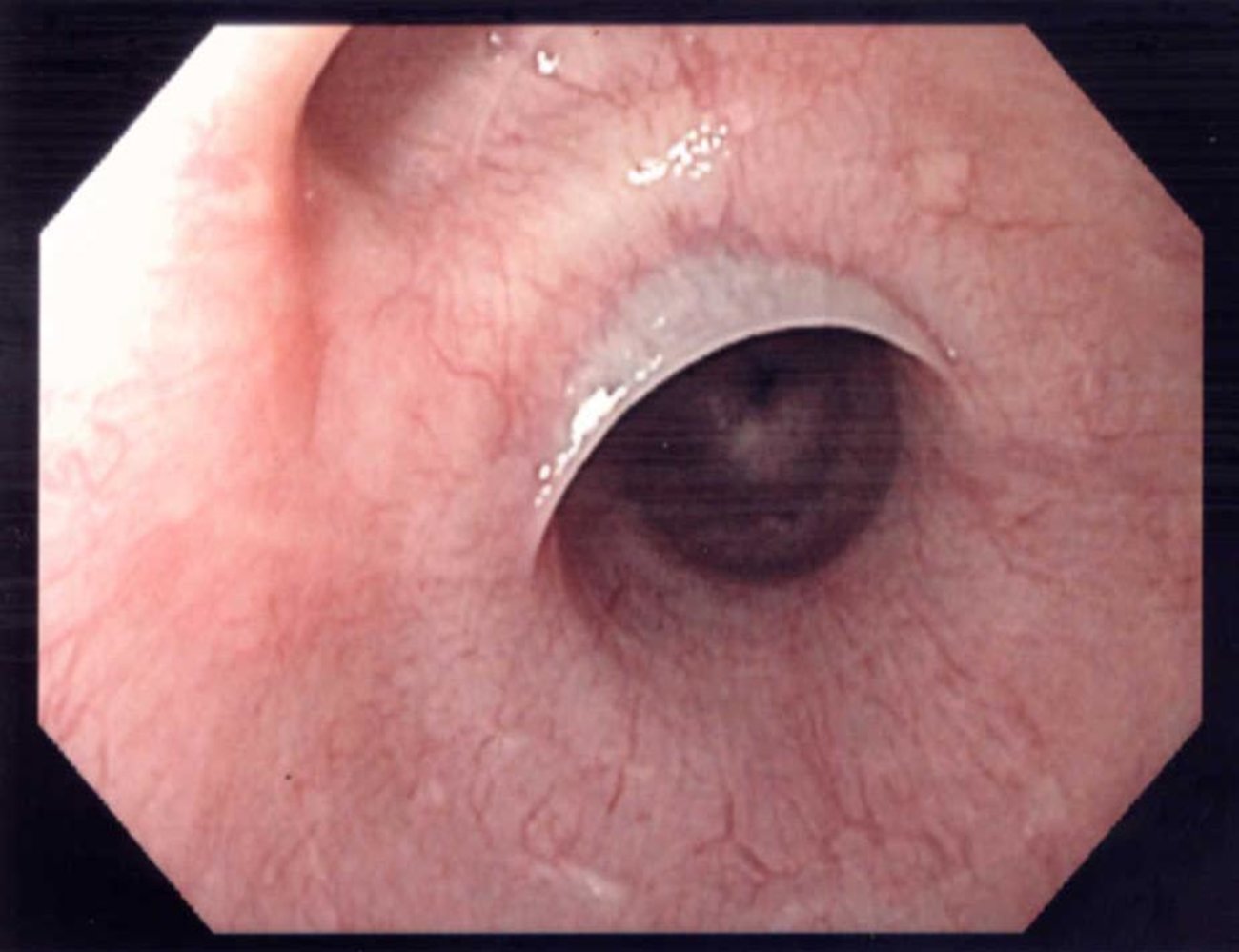
Endoscopic view of the esophagus
A thin, semilunar membrane (esophageal web; blue overlay) projects into the esophageal lumen. Esophageal webs usually occur in the upper esophagus and do not involve the muscle layer.
Cervical esophageal webs, iron deficiency anemia, and dysphagia form the classic triad of findings in Plummer-Vinson syndrome.
Source: “Endoscopic image of esophageal web” by Samir, Wikimedia Foundation, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
© AMBOSS
Screening
Indications [1][11]
- Recommendations for screening vary between medical bodies. [1][11][12][13][14]
- Consider screening in the following circumstances:
- Individuals with a history of IDA.
- Individuals with risk factors for IDA
- Anticipated high blood loss surgery [15]
- Infants and children (see “IDA in children”)
- Pregnant individuals (see “IDA in pregnancy”)
Method [11]
- Measure capillary or venous Hb level (with a Hb or CBC test).
- Assess whether Hb levels match the WHO definition of anemia.
- In patients with anemia, verify capillary samples with a venous CBC and proceed to diagnostic studies for IDA.
Recommended intervals [11]
- Nonpregnant women:
- With any risk factor for IDA (excluding menstruation) or previous IDA: annually [11]
- Without risk factors for IDA (excluding menstruation): every 5–10 years
- Pregnant individuals and children: See “Special patient groups.”
- Men with risk factors for IDA or previous IDA: periodically [1][11]
Screening for IDA is not recommended in asymptomatic men and postmenopausal women if they have no risk factors. [1]
Diagnosis
Approach

-
Initial investigations
- Routine studies: CBC (± blood smear) to check Hb and Hct
- Iron studies: to confirm the diagnosis of iron deficiency
- Evaluation for underlying causes of iron deficiency: recommended in the majority of patients
-
Empiric iron therapy can be initiated if:
- The patient's history points to a clear explanation for IDA (e.g., history of multiple blood donations or inadequate nutritional iron intake)
- No pathology is found in a young, otherwise healthy patient after the initial investigations
- Advanced studies (e.g., capsule endoscopy, angiographic or scintigraphic studies): Consider in older symptomatic patients with negative initial workup and no response to empiric iron therapy. [16]
Routine studies [1][16][17]
-
CBC
-
↓ Hemoglobin: The WHO definition of anemia is a hemoglobin level less than two standard deviations below the mean (adjusted for age and sex), i.e.: [1][17]
- Men: < 13 g/dL
- Nonpregnant women: < 12 g/dL
- Pregnant women: depends on trimester; see “Diagnostic Hb levels for anemia during pregnancy.”
- Children: See “IDA in children and adolescents.”
- ↓ Hematocrit
- ↑ Platelet count (reactive thrombocytosis) [18][19]
-
↓ Hemoglobin: The WHO definition of anemia is a hemoglobin level less than two standard deviations below the mean (adjusted for age and sex), i.e.: [1][17]
-
Red blood cell indices [16]
- RBC: initially normal (decreased with prolonged deficiency)
-
Mean corpuscular volume
- Typically ↓ (microcytic)
- May be normal (normocytic)
- Children: age-specific lower limit of normal for MCV values is (70 + age in years)
-
Mean corpuscular hemoglobin
- Typically ↓ (hypochromic)
- May be normal (normochromic)
- Normal or ↓ reticulocyte count
-
Red cell distribution width (RDW)
- Increases in established IDA
- Can help distinguish IDA from anemia of chronic disease and certain types of thalassemia (in which the RDW is usually normal) [20]
- See also “Serum laboratory findings in microcytic anemia.”
- Peripheral blood smear: : anisocytosis and hypochromasia (increased zone of central pallor) [21]



Diagnosis of iron deficiency [1][4][17][22]
-
Iron studies
-
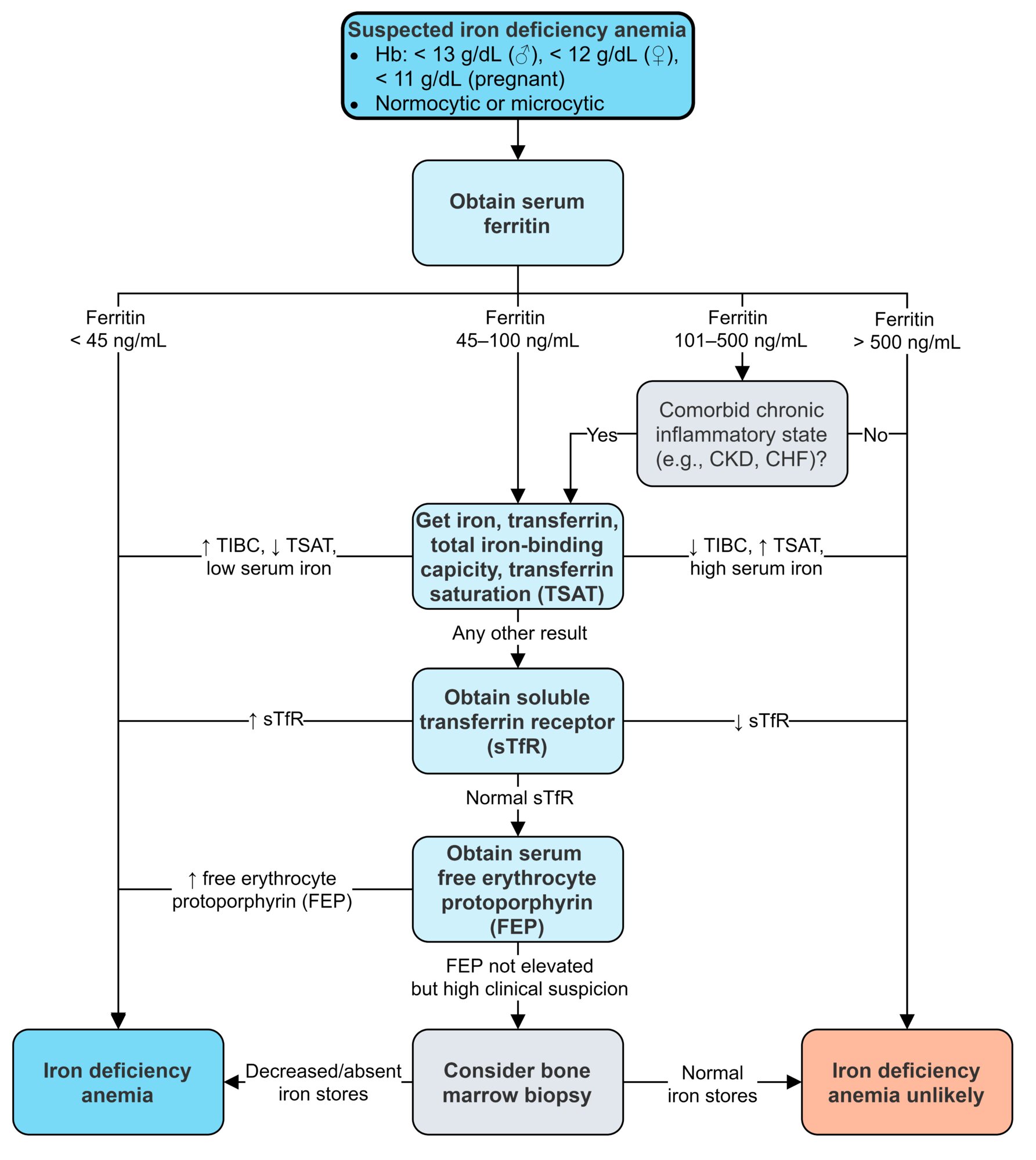
Best initial test: ↓ serum ferritin [1]
- < 45 ng/mL: IDA highly likely [11][22]
- 45–100 ng/mL: Consider further evaluation (e.g., transferrin, TSAT).
- Comorbid chronic inflammatory conditions, CKD, CHF: further evaluation even if ferritin is normal
- Further evaluation
- ↓ Serum iron [1]
- ↑ Serum transferrin and total iron binding capacity (TIBC)
- ↓ Transferrin saturation (TSAT) [4][17]
- ↑ Serum soluble transferrin receptor (sTfR) [21]
- Additional tests to consider
- Serum free erythrocyte protoporphyrin: elevated
- EPO: normal or elevated [23]
-
Best initial test: ↓ serum ferritin [1]
-
Bone marrow biopsy [1][21]
- Gold standard, but only indicated in patients with suspected IDA and equivocal iron studies.
- Findings: decreased or absent stainable iron stores [16]
In combination with an elevated TIBC, low ferritin and iron levels are diagnostic of iron deficiency anemia.
Increased ferritin does not rule out iron deficiency anemia. It can be increased in response to simultaneous inflammation.
Evaluation for underlying cause [1][22]
| Evaluation for underlying causes of iron deficiency [16][22] | ||
|---|---|---|
| Suspected etiology | Indications | Studies |
| Gastrointestinal pathologies |
|
|
|
|
|
| Gynecologic pathologies |
|
|
| Renal pathologies |
|
|
| Pulmonary pathologies |
|
|
© AMBOSS
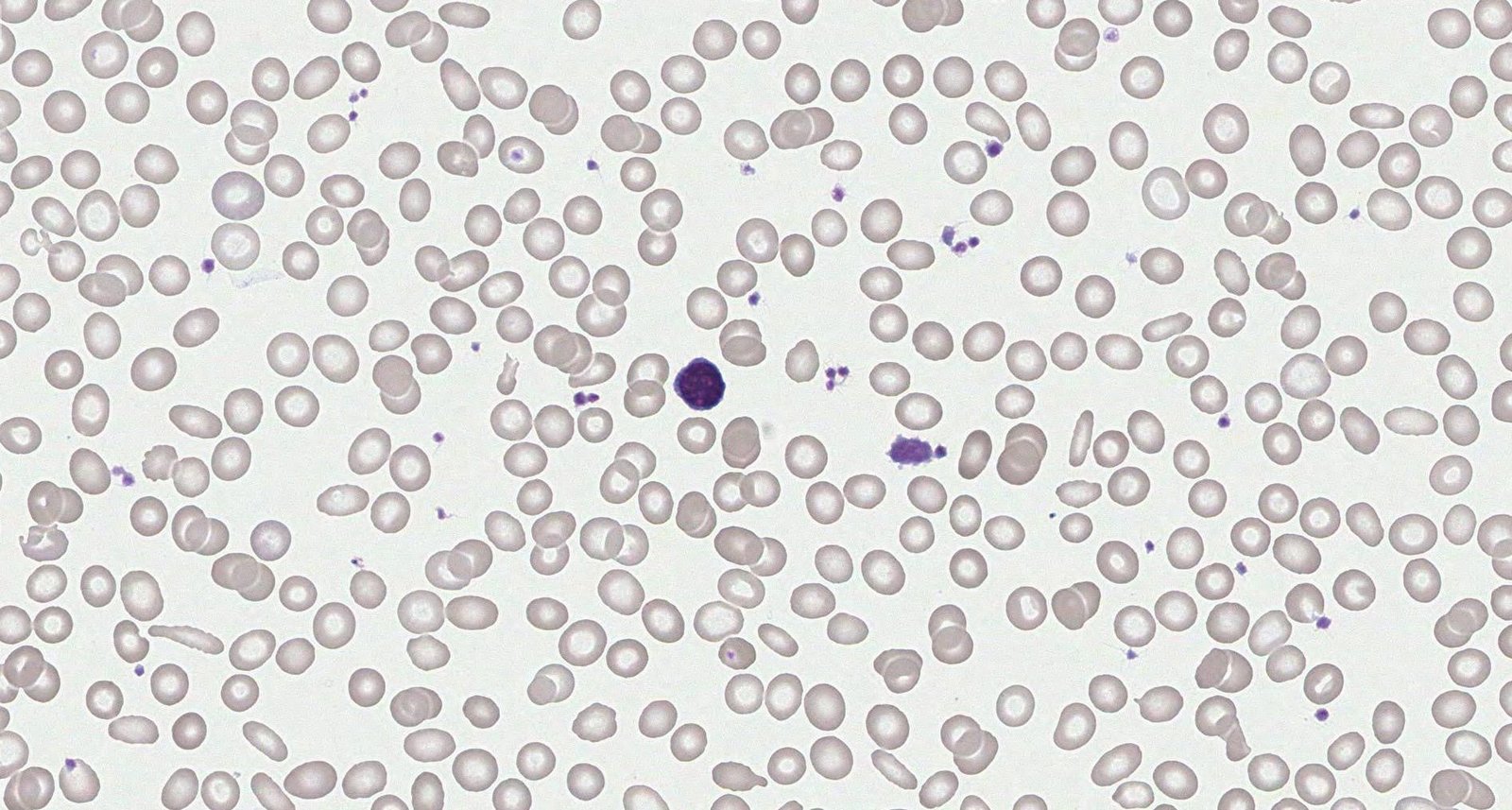
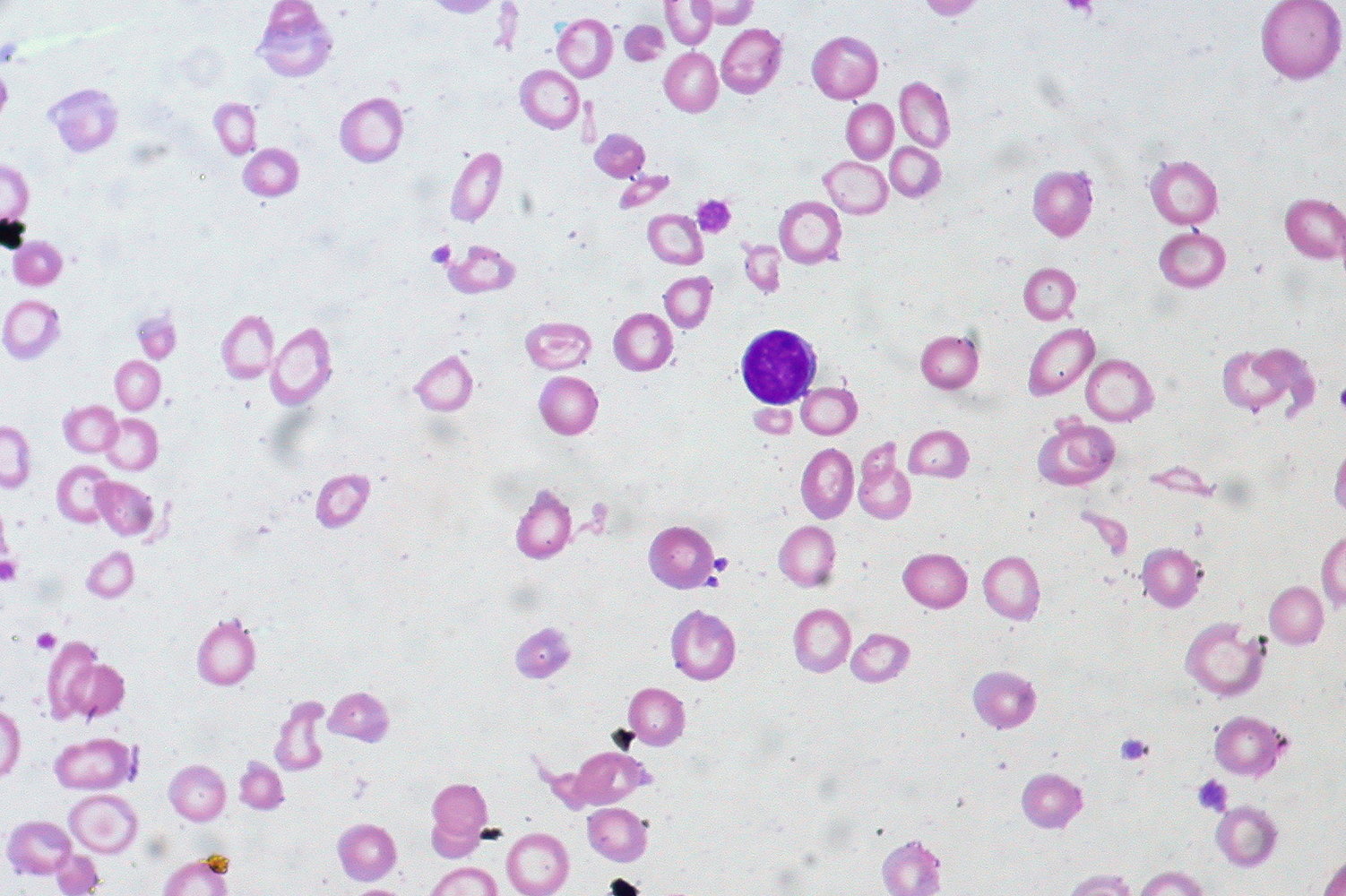
Photomicrograph of a peripheral blood smear (May-Grunwald-Giemsa stain)
Erythrocytes with different sizes (anisocytosis) and, in some instances, abnormal shapes (poikilocytosis, examples indicated by green overlays) are shown. Many erythrocytes have an increased zone of central pallor. There is a lymphocyte in the center of the image (large purple cell, red overlay) and multiple platelets throughout (smaller purple cells, examples indicated by black arrowheads).
These findings are characteristic of iron deficiency anemia.
Click on the Smartzoom button to view the entire specimen through a virtual microscope.
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: PD Dr. Alberto Perez Bouza
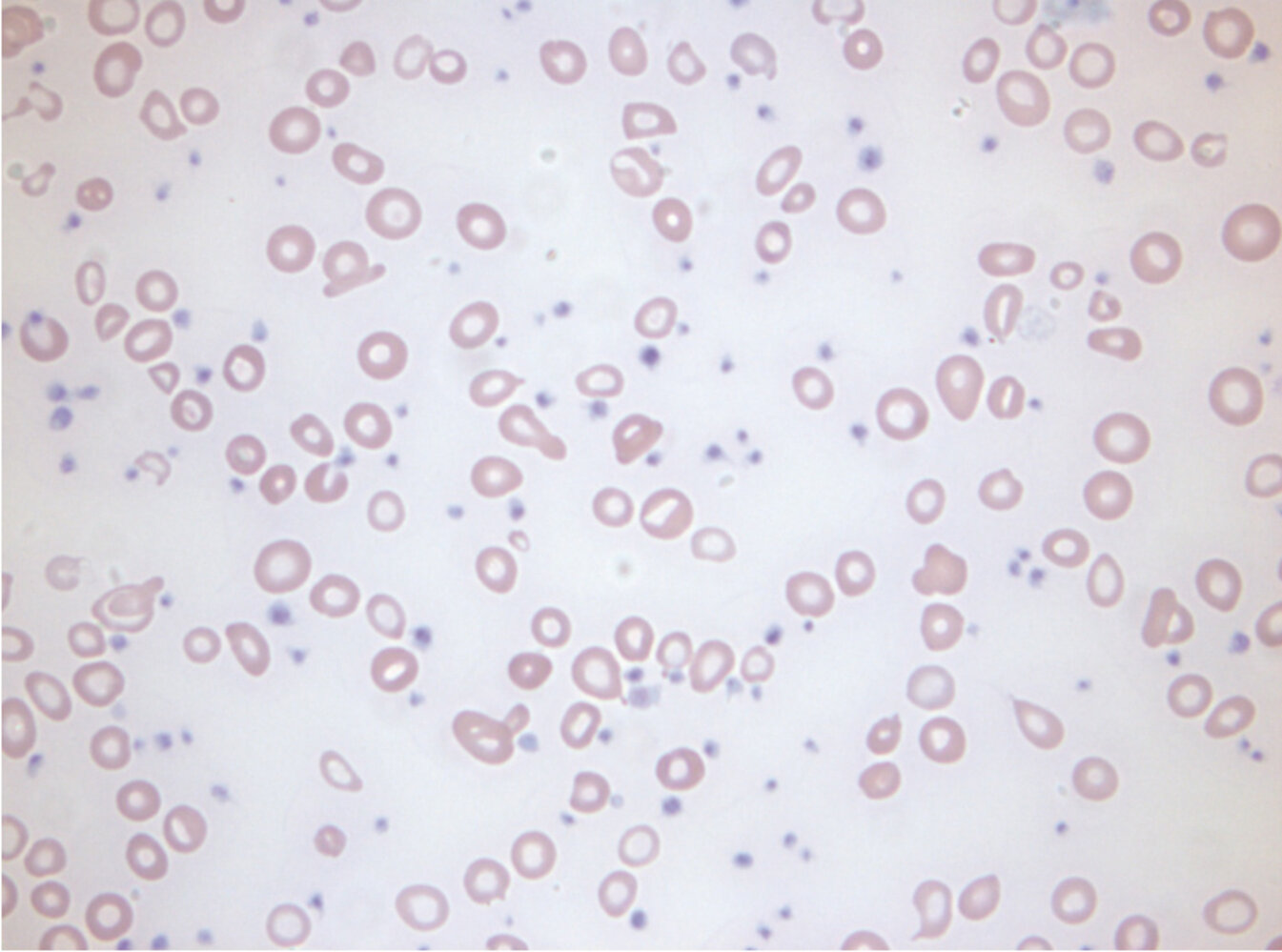
Photomicrograph of a peripheral blood smear
Most of the red blood cells are small (microcytic) and contain a central zone of pallor (hypochromasia; examples indicated by blue overlay). There are also cells with abnormal morphology (poikilocytosis; examples indicated by arrow-heads).
In the center of the image, a distinctly basophilic lymphocyte (example indicated by yellow overlay) is visible, which can be used to compare cell sizes.
These findings are characteristic of iron deficiency anemia.
Source: “Iron-deficiency Anemia, Peripheral Blood Smear” by Ed Uthman, Flickr, licensed under CC BY 2.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
Treatment
Treatment of the underlying condition
Examples include:
- Abnormal uterine bleeding: e.g., hormonal therapy (OCPs), tranexamic acid, gynecologic surgery
-
GI pathology
- H. pylori eradication therapy
- GI bleeding: e.g., polypectomy, treatment of GI malignancy (e.g., colon cancer)
- See also “Treatment” in “PUD,” “IBD,” “Celiac disease.”
- Hookworm infection: antihelminthics
- Malnutrition or malabsorption: Identification and treatment of underlying causes (e.g., eating disorders) and nutritional supplementation
Dietary modifications for IDA
-
Encourage the consumption of:
- Iron-rich foods (especially heme iron) to meet the recommended daily dietary iron intake [25]
- Foods with vitamin C (to enhance oral iron absorption) [26]
-
Counsel patients to limit intake of substances that reduce iron absorption. [1][17]
- Select foods, e.g., tea, cereals, dairy products, some soy products [27]
- Select medications, e.g., calcium, antacids, PPIs
- See “Prevention of IDA in children” for the additional dietary recommendations for infants and children.
Iron therapy
Oral iron therapy is effective, inexpensive, and is typically the initial treatment for most patients with IDA. Parenteral iron therapy is beneficial in certain cases.
| Iron therapy for iron deficiency anemia | ||
|---|---|---|
| Oral iron therapy | Parenteral iron therapy [1][17] | |
| Indications |
|
|
| Dosage and administration [17] |
|
|
| Adverse effects [1][30] |
|
|
Blood transfusion [32][33]
See “Transfusion” for further information.
-
Consider pRBCs in:
- Hemodynamically unstable patients with anemia
- Severe anemia (Hb ≤ 7 g/dL)
- Select patients with Hb ≤ 8 g/dL
- Avoid pRBCs in: hemodynamically stable patients with mild or moderate IDA.
Ongoing management of IDA [1][4]
- Obtain monitoring studies to assess response to treatment. [1][17]
- Check CBC:
- Monthly until in normal range
- Then every 3 months for one year
- Then repeat once after another year
- Adequate response: After one month, hemoglobin should have increased by ≥ 1 g/dL.
- Reticulocyte count may also be used for monitoring. [21]
- Check CBC:
- Patients receiving oral iron therapy: Continue treatment for 3–6 months to replenish iron stores. [1][4][17]
Differential diagnoses

See "Diagnosis" in “Anemia.”
-
Normocytic anemia
- Acute blood loss anemia
- Occult bleeding
- Anemia of chronic disease
- Hemolytic anemia
- Chronic kidney disease
- Aplastic anemia
-
Microcytic anemia
-
Thalassemia
- Laboratory studies reveal hemolysis: ↓ haptoglobin, ↑ indirect bilirubin, ↑ reticulocytes
- Confirmed on Hb-electrophoresis
- Mentzer index (MCV/RBC ratio): a ratio < 13 suggests thalassemia; a ratio > 13 suggests IDA
- Sideroblastic anemia: Serum ferritin levels and transferrin saturation levels are normal or increased.
-
Lead poisoning (esp. in children)
- Erythrocytes show characteristic basophilic stippling on peripheral smear.
- High levels of lead in blood
- Anemia of chronic disease (may co-exist with IDA): Serum ferritin levels and transferrin saturation levels are usually normal.
-
Thalassemia
| Iron deficiency anemia | Anemia of chronic disease | |
|---|---|---|
| Ferritin | ↓ | Normal to ↑ |
| Iron | ↓ | normal to ↓ |
| Transferrin/TIBC | ↑ | Slightly ↓ |
| Transferrin saturation | ↓ | Normal to slightly ↓ |
| RDW | ↑ | normal |
| Soluble transferrin receptor (sTfR) | ↑ | normal |
References:[34]
The differential diagnoses listed here are not exhaustive.
© AMBOSS
Complications
- Heart failure
- Increased infections
- Restless leg syndrome
-
In pregnancy:
- Increased maternal and neonatal mortality
- Preterm labor
- Low birth weight
-
In children:
- Developmental delay
- Low educational attainment
We list the most important complications. The selection is not exhaustive.
Prevention
See also “Special patient groups” for additional recommendations for children and pregnant individuals.
Recommended daily dietary intake of iron [11][35]
- The recommended daily intake of iron is calculated based on age, sex, and, in female individuals, gynecologic history (i.e., menstruation, pregnancy, breastfeeding).
- Most individuals achieve adequate intake through the consumption of iron-rich foods, e.g.:
- Red meat
- Legumes
- Dark green leafy vegetables
- Iron-fortified foods (including fortified formula for infants)
- Vitamin supplements are indicated in individuals unable to consume the recommended amount of iron-rich foods or who have risk factors for IDA.
| Recommended daily iron intake [36] | ||
|---|---|---|
| Age | Male individuals | Female individuals |
| ≤ 6 months |
|
|
| 7–12 months |
|
|
| 1–3 years |
|
|
| 4–8 years |
|
|
| 9–13 years |
|
|
| 14–18 years |
|
|
| 19–50 years |
|
|
| ≥ 51 years |
|
|
The National Academy of Medicine (formerly known as the Institute of Medicine) recommends that vegetarians consume almost twice the recommended daily dietary intake of iron because nonheme iron is not as easily absorbed as heme iron. [39]
Special patient groups
Certain patient groups are at increased risk of both developing IDA and complications resulting from it.
Iron deficiency anemia in children and adolescents
Rapid periods of growth increase the body's demand for iron, putting children and infants at risk of anemia. Children who develop anemia have a higher risk of developmental delay and infections. [4]
Risk factors for pediatric IDA [11][26][27]
- Prematurity [40]
- Small for gestational age (i.e., low birth weight)
- Poor dietary intake of iron-fortified or iron-rich foods, e.g.:
- Exclusively breastfed infants > 4 months of age not receiving iron prophylaxis
- Early (i.e., < 12 months of age) and excessive (> 700 mL (> 24 oz) per day) intake of nonfortified cow's milk
- Restrictive diets: malnutrition (mainly in resource-limited countries), eating disorders (including pica), picky eating
- GI bleeding (e.g., Meckel diverticulum)
- Heavy menstrual bleeding
- Intellectual disability
- Low socioeconomic status, including living in areas with a high prevalence of IDA
IDA is a risk factor for pediatric lead toxicity. [26]
Cow's milk has a very low concentration of iron and also disrupts iron absorption. [41]
Clinical features
- Clinical features of IDA in children are similar to those in adults.
- Commonly asymptomatic [42]
- Young children can present with irritability or pica. [42]
- Children with anemia have an increased risk of infections and developmental delay. [4]
Screening [12]
- Guidelines on screening children for IDA vary regarding which children to screen and the frequency of screening.
- Screen children with risk factors for pediatric IDA at set intervals. [12][27][43]
- Consider screening all infants at the 12-month well-child visit. [12]
- Method [27]
- Obtain a Hb level (capillary or venous).
- Assess whether Hb levels meet criteria for anemia (see “Diagnosis”).
- Next steps: If anemia is present, verify capillary samples with venous samples and proceed to diagnostics studies.
Diagnostics [12][27]
- Serum CBC to confirm anemia (according to the WHO definition of anemia).
- < 6 months of age: varies depending on age [44]
- 6–59 months: < 11 g/dL
- 5–11 years: < 11.5 g/dL
- 12–14 years: < 12.0 g/dL
-
Iron studies to confirm a diagnosis of IDA (recommended for most patients), e.g.: [1][27]
- ↓ serum ferritin with a normal C-reactive protein (CRP) [27]
- ↓ reticulocyte hemoglobin content (CHr) [27]
- ↑ soluble transferrin receptor [45]
In children with mild microcytic or normocytic anemia and a history of poor dietary iron intake, IDA can be presumed and empirically treated. The diagnosis can be confirmed with either a 1 g/dL increase in hemoglobin concentration after 1 month of iron therapy or with confirmatory testing for IDA. [27]
Management [1][4][26]
-
Severe anemia
- Consult hematology.
- Significant symptoms (e.g., hemodynamic compromise): PRBC transfusion, admission
- All other patients: IV iron or 3–6 mg/kg/day of oral elemental iron [26][46][47]
- Mild or moderate anemia: 3–6 mg/kg/day of oral elemental iron [1][4]
- See “Treatment for IDA” for more information on:
- Evaluation for underlying causes of IDA
- Dietary modifications for iron deficiency
- Ongoing management of IDA
Prevention of IDA in children [11][26]
- All children: Encourage the recommended daily dietary intake of iron. [26][27]
- Ensure formula or breastmilk until 12 months of age. [26][48]
- At around 4–6 months of age, introduce age-appropriate iron-rich foods (e.g., iron-fortified cereal, pureed meats).
- At ≥ 12 months of age, limit low-iron milk (e.g., cow's milk) to 470–710 mL (16–24 oz) per day.
- In children with risk factors for pediatric IDA, start iron supplementation, e.g., in: [11][26][27]
- Term breastfed infants ≥ 4 months of age: 1 mg/kg/day of elemental iron until there is an adequate intake of iron-rich foods (e.g., iron-fortified cereal) [26][27]
- Premature infants have increased iron requirements, e.g., 2–4 mg/kg/day, in the first year of life; tailor iron supplementation to their specific needs. [26][27]
- Children living in regions with a high prevalence of IDA : Consider oral iron supplementation. [37]
Do not introduce low-iron milk (e.g., cow's milk) before 12 months of age. [27]
Do not routinely start iron prophylaxis in children who receive frequent blood transfusions, because of the risk of iron overload. [27]
Iron deficiency anemia in pregnancy
Iron deficiency anemia in pregnancy is associated with preterm labor, low birth weight, and increased mortality for both the mother and neonate. Diagnostic Hb levels for anemia during pregnancy should be used when assessing for IDA as there is an expected physiological decrease in hemoglobin during pregnancy because of increased plasma volume (known as dilutional anemia). [4][13]
Epidemiology
- 30–50% of pregnant individuals worldwide have an iron deficiency. [31][49]
- IDA is the most common type of anemia during pregnancy. [31]
Etiology
- Increased fetal iron requirements for RBC production and fetoplacental growth
- Increased RBC mass [50]
- See also “Etiology of IDA.”
Clinical features
- Clinical features of IDA do not significantly differ in pregnant individuals.
- For effects on the fetus, see “Complications” below.
Screening for IDA in pregnancy [13][14][51]
- Recommended screening times: [13][14]
- First prenatal visit and again at 24–28 weeks' gestational age
- Consider screening once during each trimester.
- Method: Obtain a CBC to assess for diagnostic Hb levels for anemia during pregnancy.
- Next steps: If anemia is present, proceed to diagnostics.
Diagnostics [4][13]
- Routine studies
- CBC ± blood smear to confirm anemia (if not already obtained during screening) [13][14][21]
- Iron studies to confirm the diagnosis of IDA (recommended), e.g., ferritin level < 30 ng/mL [1][13]
-
Diagnostic Hb levels for anemia during pregnancy [13]
- First trimester: Hb < 11 g/dL
- Second trimester: Hb < 10.5 g/dL
- Third trimester: Hb < 11 g/dL
In pregnant individuals with nonsevere microcytic or normocytic anemia and nothing to suggest an alternative cause of anemia, IDA can be presumed and empirically treated. The diagnosis is confirmed with an appropriate increase in hemoglobin concentration within 2–4 weeks of initiating iron therapy or with confirmatory testing for IDA. [1][13][52]
Management [11][13][47]
- Severe anemia (< 7 g/dL)
- Consult hematology and OB/GYN. [13][47]
- Significant symptoms (e.g., hemodynamic compromise) or Hb < 6 g/dL: PRBC transfusion, admission [13]
- Asymptomatic patients: parenteral iron therapy (avoid in the first trimester) or oral iron therapy [13]
- For asymptomatic mild or moderate anemia (Hb ≥ 7 g/dL): 60–120 mg/day of oral elemental iron [29]
- See “Treatment for IDA” for more information on:
- Iron therapy for IDA
- Evaluation for underlying causes of IDA
- Dietary modifications for iron deficiency
- Ongoing management of IDA
Complications [4]
- Increased risk of adverse maternal/fetal outcomes (e.g., low birth weight, neonatal anemia, premature labor)
- Impaired fetal neurodevelopment
Prevention [13][53]
- Encourage patients to consume the recommended daily dietary intake of iron (i.e., 27 mg). [11][13]
- Consider routine supplementation with low-dose iron (i.e., 27 mg/day) starting at the first prenatal visit. [11][13][14]
Avoid iron supplements in pregnant individuals with conditions that increase iron levels in the body (e.g., hemochromatosis) without first consulting the patient's hematologist. [13]
External Resources
- 2024 USPSTF Recommendation Statement: Screening and Supplementation for Iron Deficiency and Iron Deficiency Anemia During Pregnancy
- 2021 ACOG Practice Bulletin: Anemia in Pregnancy
- 2020 AGA Clinical Practice Guidelines on the Gastrointestinal Evaluation of Iron Deficiency Anemia
- 2015 Clinical Practice Guidelines From the AABB: Red Blood Cell Transfusion Thresholds and Storage
- 2010 AAP Diagnosis and Prevention of Iron Deficiency and Iron-Deficiency Anemia in Infants and Young Children
- US Preventive Services Task Force recommendations (Anemia)
References
- Short MW, Domagalski JE. "Iron deficiency anemia: evaluation and management". Am Fam Physician. 87(2). :98-104. (2013)
- Miller JL. "Iron deficiency anemia: a common and curable disease". Cold Spring Harb Perspect Med. 3(7). (2013)
- Laura Percy, Diana Mansour. "Iron deficiency and iron-deficiency anaemia in women's health". The Obstetrician & Gynaecologist. 19(2). :155-161. (2017)
- Camaschella C. "Iron-Deficiency Anemia". N Engl J Med. 372(19). :1832-1843. (2015)
- Institute of Medicine (US) Committee on Use of Dietary Reference Intakes in Nutrition Labeling. "Dietary Reference Intakes, Guiding Principles for Nutrition Labeling and Fortification". National Academies Press. (2003). ISBN: 9780309091329
- Anderson GJ, McLaren GD. "Iron Physiology and Pathophysiology in Humans". Springer Science & Business Media. (2012). ISBN: 9781603274852
- Sostres C, Gargallo CJ, Lanas A. "Nonsteroidal anti-inflammatory drugs and upper and lower gastrointestinal mucosal damage". Arthritis Res Ther. 15(Suppl 3). :S3. (2013)
- "Angular Cheilitis". http://research.omicsgroup.org/index.php/Angular_cheilitis. [2017-02-28]
- Novacek G. "Plummer-Vinson syndrome". Orphanet J Rare Dis. 1(36). (2006)
- Khan Y, Tisman G. "Pica in iron deficiency: a case series". J Med Case Reports. 4. :86. (2010)
- Caligiuri M, Levi MM, Kaushansky K, et al. "Williams Hematology, 9E". McGraw-Hill Education / Medical. (2015). ISBN: 9780071833004
- Ning S, Zeller MP. "Management of iron deficiency". Hematology Am Soc Hematol Educ Program. 2019(1). :315-322. (2019)
- Mhadgut H, Galadima H, Tahhan HR. "Thrombocytosis in Iron Deficiency Anemia". Blood. 132(Supplement 1). :4985-4985. (2018)
- Dan K. "Thrombocytosis in iron deficiency anemia.". Intern Med. 44(10). :1025-6. (2005)
- Van Vranken M. "Evaluation of microcytosis.". Am Fam Physician. 82(9). :1117-22. (2010)
- Johnson-Wimbley TD, Graham DY. "Diagnosis and management of iron deficiency anemia in the 21st century". Therap Adv Gastroenterol. 4(3). :177-184. (2011)
- Ko CW, Siddique SM, Patel A, et al. "AGA Clinical Practice Guidelines on the Gastrointestinal Evaluation of Iron Deficiency Anemia". Gastroenterology. 159(3). :1085-1094. (2020)
- "Recommendations to prevent and control iron deficiency in the United States. Centers for Disease Control and Prevention". https://www.ncbi.nlm.nih.gov/pubmed/9563847. [1998-04-01]
- Camaschella C. "Iron deficiency: new insights into diagnosis and treatment". Hematology. 2015(1). :8-13. (2015)
- Loukas A, Hotez PJ, Diemert D, et al. "Hookworm infection". Nat Rev Dis Primers. 2(1). (2016)
- Killip S, Bennett JM, Chambers MD. "Iron deficiency anemia". Am Fam Physician. 75(5). :671-678. (2007)
- "Dietary guidelines for Americans 2020-2025". https://www.dietaryguidelines.gov/sites/default/files/2021-03/Dietary_Guidelines_for_Americans_2020-2025.pdf. [2020-12-01]
- American Academy of Pediatrics. "Pediatric Nutrition". American Academy of Pediatrics. (2019). ISBN: 9781610023603
- Baker RD, Greer FR. "Diagnosis and Prevention of Iron Deficiency and Iron-Deficiency Anemia in Infants and Young Children (0–3 Years of Age)". Pediatrics. 126(5). :1040-1050. (2010)
- Auerbach M, Adamson JW. "How we diagnose and treat iron deficiency anemia". Am J Hematol. 91(1). :31-38. (2015)
- American College of Obstetricians and Gynecologists' Committee on Practice Bulletins—Obstetrics. "Anemia in Pregnancy: ACOG Practice Bulletin, Number 233". Obstet Gynecol. 138(2). :e55-e64. (2021)
- Siu AL. "Screening for Iron Deficiency Anemia in Young Children: USPSTF Recommendation Statement". Pediatrics. 136(4). :746-752. (2015)
- AFP. "Screening for Iron Deficiency Anemia and Iron Supplementation in Pregnant Women to Improve Maternal Health and Birth Outcomes: Recommendation Statement". Am Fam Physician. 93(2). :133-6. (2016)
- Muñoz M, Gómez-Ramírez S, Bhandari S. "The safety of available treatment options for iron-deficiency anemia". Expert Opin Drug Saf. 17(2). :149-159. (2017)
- Breymann C, Auerbach M. "Iron deficiency in gynecology and obstetrics: clinical implications and management.". Hematology Am Soc Hematol Educ Program. 2017(1). :152-159. (2017)
- Carson JL, Guyatt G, Heddle NM, et al. "Clinical Practice Guidelines From the AABB: Red Blood Cell Transfusion Thresholds and Storage". JAMA. 316(19). :2025. (2016)
- Callum JL, Waters JH, Shaz BH, Sloan SR, Murphy MF. "The AABB recommendations for the Choosing Wisely campaign of the American Board of Internal Medicine". Transfusion. 54(9). :2344-2352. (2014)
- Scholl TO. "Maternal iron status: relation to fetal growth, length of gestation, and iron endowment of the neonate". Nutr Rev. 69. :S23-S29. (2011)
- Ekhard E Ziegler. "Consumption of cow's milk as a cause of iron deficiency in infants and toddlers". Nutr Rev. 69. :S37-S42. (2011)
- Kliegman RM, Geme JS. "Nelson Textbook of Pediatrics, 2-Volume Set". Elsevier. :3623-3633. (2019). ISBN: 9780323529501
- "Recommendations for Preventive Pediatric Health Care". https://web.archive.org/web/20230126132131/https://downloads.aap.org/AAP/PDF/periodicity_schedule.pdf. [2022-07-01]
- Widness JA. "Pathophysiology of Anemia During the Neonatal Period, Including Anemia of Prematurity". NeoReviews. 9(11). :e520-e525. (2008)
- Proytcheva MA. "Diagnostic Pediatric Hematopathology". Cambridge University Press. (2011). ISBN: 9781107377448
- Speckert M, Ramic L, Mitsakakis N, Liebman M, Leung EW. "Management of Severe Iron Deficiency Anemia in the Pediatric Emergency Department: A Comparison of IV Iron Vs Transfusions". Blood. 138(Supplement 1). :2011-2011. (2021)
- "Haemoglobin concentrations for the diagnosis of anaemia and assessment of severity.". https://apps.who.int/iris/bitstream/handle/10665/85839/WHO_NMH_NHD_MNM_11.1_eng.pdf?sequence=22&isAllowed=y. [2011-01-01]
- "Recommended Drinks for Children Age 5 & Younger". https://web.archive.org/web/20230614172704/https://www.healthychildren.org/English/healthy-living/nutrition/Pages/recommended-drinks-for-young-children-ages-0-5.aspx. [2022-05-13]
- WHO. "Guideline Daily Iron Supplementation in Infants and Children". World Health Organization. (2016). ISBN: 9789241549523
- "Dietary supplement fact sheet: Iron". https://web.archive.org/web/20230524150010/https://ods.od.nih.gov/factsheets/Iron-HealthProfessional/. [2022-04-05]
- Institute of Medicine (US) Panel on Micronutrients. "Dietary Reference Intakes for Vitamin A, Vitamin K, Arsenic, Boron, Chromium, Copper, Iodine, Iron, Manganese, Molybdenum, Nickel, Silicon, Vanadium, and Zinc". National Academies Press. (2001). ISBN: 9780309072793
- Burke R, Leon J, Suchdev P. "Identification, Prevention and Treatment of Iron Deficiency during the First 1000 Days". Nutrients. 6(10). :4093-4114. (2014)
- Pawlak R, Berger J, Hines I. "Iron Status of Vegetarian Adults: A Review of Literature". Am J Lifestyle Med. 12(6). :486-498. (2016)
- "Intermittent iron and folic acid supplementation during pregnancy in malaria-endemic areas". https://www.who.int/elena/titles/intermittent_iron_pregnancy_malaria/en/. [2019-02-11]
- Sanghavi M, Rutherford JD. "Cardiovascular Physiology of Pregnancy". Circulation. 130(12). :1003-1008. (2014)
- US Preventive Services Task Force, Nicholson WK, Silverstein M, et al. "Screening and Supplementation for Iron Deficiency and Iron Deficiency Anemia During Pregnancy: US Preventive Services Task Force Recommendation Statement.". JAMA. (2024)
- "Clinical Preventive Service Recommendation Iron Deficiency Anemia". https://web.archive.org/web/20230613212953/https://www.aafp.org/family-physician/patient-care/clinical-recommendations/all-clinical-recommendations/iron-deficiency-anemia.html. [2023-01-01]
- Igbinosa I, Berube C, Lyell DJ. "Iron deficiency anemia in pregnancy". Curr Opin Obstet Gynecol. Publish Ahead of Print. (2022)
- Siu AL. "Screening for Iron Deficiency Anemia and Iron Supplementation in Pregnant Women to Improve Maternal Health and Birth Outcomes: U.S. Preventive Services Task Force Recommendation Statement". Ann Intern Med. 163(7). :529-536. (2015)
- Lin Y. "Preoperative anemia-screening clinics". Hematology. 2019(1). :570-576. (2019)